


Dissonance-based Program for Eating Disorders Prevention in Mexican University Students
[Un programa de prevención de los trastornos de la conducta alimentaria basado en la técnica de disonancia cognitiva en alumnos universitarios mexicanos]
Claudia Unikel-Santoncini1, Concepción Díaz de León-Vázquez2, José Alberto Rivera-Márquez2, Ietza Bojorquez-Chapela3, and Enrique Méndez-Ríos1
1Ramón de la Fuente Muñiz National Institute of Psychiatry, Ciudad de Mexico, Mexico; 2Universidad Autónoma Metropolitana-Xochimilco, Ciudad de Mexico, Mexico; 3El Colegio de la Frontera Norte, Tijuana, Mexico
https://doi.org/10.5093/pi2018a17
Received 22 February 2018, Accepted 12 June 2018
Abstract
The purpose of this study was to identify changes in the risk of eating disorders after a one-year follow-up of a dissonance-based eating disorders prevention program. The Body Project was implemented in a sample of male and female university students: 133, 110, and 74 at baseline, post-test, and follow-up respectively, and we tested the change in disordered eating behaviors (DEB) over time, and by levels of variables that according to the theoretical model lie on the path between the intervention and DEB, with one-way MANOVA analyses of repeated measures for the associations between internalization of the esthetic thin ideal, depressive symptoms, and DEB. The average value of DEB was 5.23 at pre-test, 3.45 at post-test, and 2.80 at follow-up. The model with DEB at each time point, as dependent variables, and internalization of the esthetic thin ideal and depressive symptoms, as independent variables, showed a significant effect of internalization of the esthetic thin ideal, F(2, 136) = 7.66, p = .0011, while there was no significant effect of depressive symptoms, F(2, 136) = 0.45, p = .6191, indicating that the intervention exerted its effect on DEB via the former variable. The intervention proved to produce effects after a one-year follow-up. These findings support the implementation of universal prevention programs using dissonance-based techniques.
Resumen
El objetivo de este trabajo fue identificar los cambios en el riesgo de desarrollar trastornos de la conducta alimentaria después de un año de seguimiento de un programa de prevención basado en la técnica de la disonancia cognitiva para trastornos de la conducta alimentaria. El Body Project fue implementado en una muestra de estudiantes universitarios, hombres y mujeres: 133, 110 y 74 en el pre-test, post-test y seguimiento, respectivamente. Se comprueba el cambio en las conductas alimentarias de riesgo (CAR) a lo largo del tiempo y según las variables que, de acuerdo con el modelo teórico, se encuentran entre la intervención y las CAR, con un análisis MANOVA de medidas repetidas para las asociaciones entre interiorización del ideal estético de delgadez, los síntomas depresivos y las CAR. El valor promedio de las CAR en el pre-test fue 5.23, 3.45 en el post-test y 2.80 en el seguimiento. El modelo de las CAR como variable dependiente e interiorización del ideal estético de delgadez y los síntomas depresivos como variables independientes mostró un efecto significativo de la internalización del ideal estético de delgadez, F(2, 136) = 7.66, p = .0011, mientras que no hubo un efecto significativo de los síntomas depresivos, F(2, 136) = 0.45, p = .6191, lo que indica que la intervención tuvo un efecto en las CAR por vía de la variable antecedente. Se mostró que la intervención produce efectos después de un año de seguimiento. Este hallazgo sustenta la implementación de programas universales de prevención que utilicen la técnica de disonancia cognoscitiva.
Keywords
Eating disorders, Disordered eating behavior, Cognitive dissonance, Prevention, Youth.
Palabras clave
Trastornos de la conducta alimentaria, Conductas alimentarias de riesgo, Disonancia cognitiva, Prevención, Jóvenes.
Cite this article as: Unikel-Santoncini, C. , León-Vázquez, C. D. D. , Rivera-Márquez, J. A. , Bojorquez-Chapela, I. , and Méndez-Ríos, E. (2019). Dissonance-based Program for Eating Disorders Prevention in Mexican University Students. Psychosocial Intervention, 28, 29 - 35. https://doi.org/10.5093/pi2018a17
Correspondence: unikels@imp.edu.mx(C. Unikel-Santoncini).
Introduction Eating disorders (ED) are serious pathologies that tend to be chronic (Wonderlich et al., 2012), involve relapses (Herzog et al., 1999), and are associated with a high degree of comorbidity with other psychiatric pathologies. Around 56% of patients with anorexia nervosa and 94.5% with bulimia nervosa present at least one comorbid diagnosis described in the DSM-IV (Benjet, Méndez, Borges, & Medina-Mora, 2012; Hudson, Hiripi, Pope, & Kessler, 2007; Swanson, Crow, Le Grange, Swendsen, & Merikangas, 2011). ED are associated with multiple medical complications, including dermatological, endocrine, cardiovascular and pulmonary problems, electrolyte imbalance, and bone demineralization (Mitchell & Crow, 2006). Their mortality is among the highest for mental illness, one-fifth of which correspond to suicide deaths (Smink, van Hoeken, & Hoek, 2012). Treatment is often costly, time-consuming, and in many cases only partial recovery is achieved (Keel & Brown, 2010). Disordered eating behaviors (DEB) include all the manifestations of ED in similar form but with less frequency and intensity (Shisslak & Crago, 2001). Studies conducted on samples of university students in Mexico with ages 16 to 26 report a prevalence of DEB ranging from 7.9% (Morán, Cruz, & Iñárritu, 2009) to 18.9% (Alvarez et al., 2003) in women, and from 4.2% (Saucedo & Unikel, 2010) to 13% (Cruz-Bojorquez, Ávila-Escalante, Cortés-Sobrino, Vázquez-Arévalo, & Mancilla-Díaz, 2008) in men. Data from the National Health and Nutrition Survey 2012 (Encuesta Nacional de Salud y Nutrición - ENSANUT; Gutiérrez et al., 2012) representative for the population ages 10 to 19 shows that 33% of women and 29.6% of men mentioned at least one DEB in the previous three months. Furthermore, 1.9% of women and 0.8% of men are at risk of ED (Gutiérrez et al., 2012). Hence the importance of effective prevention programs to reduce the risk factors associated with the development of ED in young people, such as the internalization of the esthetic thin ideal (IATI), body image dissatisfaction, food restriction, and negative affect (Jacobi, Hayward, de Zwaan, Kraemer, & Agras, 2004; Polivy & Herman, 1987; Stice, 2001; Thompson & Stice, 2001). IATI has a moderate effect on the maintenance of bulimic symptoms (Stice, 2002; Thompson & Stice, 2001), while body dissatisfaction is one of the most powerful predictors of ED (Stice, Marti, & Durant, 2011). Evidence suggests that the risk of bulimic symptoms in subjects with high scores for depressive symptoms (DS) increases sevenfold (Jacobi et al., 2004). After a three-year follow-up, Jacobi et al. (2011) observed that a history of DS is the independent risk factor with the greatest ability to predict the development of an ED in female undergraduate students (area under the curve = 67.21). At the same time, chronic dietary practice increases the risk of binge eating, because calorie deficit is compensated and therefore associated with the onset of bulimia nervosa and negative affect (Stice, 2001). Prevention programs based on the Cognitive Dissonance Theory (Festinger, 1962), such as the Body Project (Stice, Rodhe, & Shaw, 2007), have proved effective in reducing both the risk factors associated with the development of ED and their symptoms (Stice, Marti, Spoor, Presnell, & Shaw, 2008; Stice, Rohde, Shaw, & Marti, 2012). The effects have been observed in adolescents and young women for at least six months, particularly in universal, selective, and indicated prevention programs (Stice, Black-Becker, & Yocum, 2013), when the intervention has been conducted by non-experts (Perez, Becker, & Ramirez, 2010) or by a peer-led team (Stice, Rohde, Shaw, Gau, & Jeff, 2017). The Body Project is based on the Dual-Pathway Model of Bulimic Pathology (Stice, 2001). This model is based on the idea that women’s IATI promotes body dissatisfaction because it is an unattainable ideal. On the other hand, high levels of pressure to be thin from family, peers, and the media promote body dissatisfaction through repeated messages that one is not thin enough. At the same time, body dissatisfaction triggers dieting or negative affect, consequently increasing the risk of binge eating and compensatory dietary behaviors, and therefore bulimic symptoms (Stice, 2001). The purpose of the Body Project is to reduce IATI through oral, written, and behavioral exercises focusing on potential health risks attributable to the obsession with achieving this ideal, which in turn leads to the reduction of DEB. According to the literature, the type of prevention with the greatest effect on ED targets at-risk women (Stice & Shaw 2004; Stice, Shaw, & Marti, 2007), achieving clinically significant improvement (Akers, Rodhe, Stice, Butryn, & Shaw, 2017). In Mexico, several selective prevention programs have been undertaken on adolescent girls using strategies such as media literacy (Rodríguez & Gómez- Peresmitré, 2007), cognitive dissonance (Pineda, Gómez-Peresmitré, & Méndez, 2010), and social skills (León, 2010). Results have been encouraging, with changes being observed in “concern with food” and “body weight”, “compulsive eating”, “body dissatisfaction”, and “ideal figure” when the study subjects were comparatively analyzed before the intervention and at three-month (Pineda et al., 2010) and six-month follow-up (León, 2010). Nevertheless, the Body Project has not been reported previously with Mexican populations. The purpose of this study was therefore to identify changes in the risk of ED after a one-year follow-up as a result of the implementation of a dissonance-based intervention for ED prevention, based on the following assumptions: 1) DEB reduces after intervention, 2) IATI has an effect on DEB, 3) IATI has an effect on depressive symptoms, 4) DS have an effect on DEB, and 5) IATI and DS have an effect on DEB. MethodSample This was a pre-experimental (Campbell & Stanley, 1995) pretest-posttest study without a control group, including a non-probabilistic sample comprising 133 subjects at baseline measurements (105 women and 28 men), 110 at posttest (88 women and 22 men), and 74 at a one-year follow-up (58 females and 16 males). All participants were students of a public university in Mexico City, who were not selected by sex or eating behavior risk levels. An oral invitation was made to professors imparting from first to fifth trimester students’ classes from Biological and Health Sciences, such as Human Nutrition, Biological and Pharmaceutical Chemistry, Biology, Veterinary, and Agronomy undergraduate courses. During the intervention, male and female students were evenly distributed (approximately 7 females per 3 males) in groups coordinated indistinctively by male or female facilitators. However, the reduced sample size of male participants did not allow for comparisons, due the disproportion observed between male and female students in the Human Nutrition undergraduate course, from which most of the students in the sample was drawn. Of the total sample, 17.2% (16.1% women and 21.4% men) did not answer the questionnaires at posttest because they failed to come into class on the day scheduled for data collection. A total of 44.3% of the students (44.7% women and 42.8% men) did not provide follow-up information after one year, for several reasons, including feeling that they had been singled out, exposed, forced to participate, or because they had dropped out of school or were repeating a course (oral communication). A comparison of students with complete and incomplete data at a one-year follow-up showed no statistically significant differences at baseline (p > .05) for DEB (ncompleters = 74, nnon completers = 59), mean = 4.6 and 5.2 respectively, IATI (ncompleters = 70, nnon completers = 63), mean = 27.6 and 29.1 respectively, and DS (ncompleters = 72, nnon completers = 135), mean = 26.3 and 24.0 respectively. Instruments Brief questionnaire to measure disordered eating behaviors (BQDEB). This questionnaire consists of 10 questions measuring concern over weight gain, practice of binge eating, as well as restrictive and purging behaviors in the three months prior to the data collection. Each question consists of four possible answers: never or almost never, sometimes, frequently (twice a week) and very frequently (more than twice a week) with 0 to 3 option score, where a higher score implies more eating behavior problems. The scale has a cut-off point of 10; scores of 10 or below are considered not at risk of DEB, whereas those above 10 are considered at risk of DEB. The scale has a reliability of .83 in female students from Mexico City (Unikel, Bojorquez, & Carreño, 2004) and of .80 in those from the State of Mexico (Unikel, Díaz de León, & Rivera, 2017). Attitudes towards body figure questionnaire. This questionnaire consists of 15 items measuring IATI. It has previously been validated in teenage female students and young adults, as well as in adolescent students from both Mexico City (Unikel, Gómez Peresmitré, & Aguilar, 2006) and the State of Mexico (Unikel et al., 2017). Each item has four possible answers: never or almost never, sometimes, frequently and always with 1 to 4 option scores. A higher score implies greater pathology. It has a cut-off point of 37 to determine at-risk cases. The reliability of the scale in women from Mexico City is .93 (Unikel et al., 2006). This scale was validated in male students at a public university, where a reliability of .89 was obtained (Díaz de León, 2013). The males’ version of this questionnaire was adapted by changing gender features in the syntax and modifying two questions: “Thin women are more feminine” to “Thin men are more attractive”, and “When you’re fat, men don’t approach you”, to “When you’re fat women don’t approach you”. Depressive symptoms (DS). The Center for Epidemiological Studies’ Revised Depression Scale - CES-R comprises 35 questions, with four response options to evaluate the previous week (slightly = 0-1 days, somewhat = 1-2 days, occasionally = 3-4 days, and usually = 5-7 days) and with a response option to evaluate the previous fortnight (almost every day = 10-14 days). This scale has been validated in Mexican school populations (González-Forteza, Jiménez-Tapia, Ramos-Lira, & Wagner, 2008), showing an adequate internal consistency value (α = .93). Self-reported body mass index (BMI). Self-reported body weight and height were used to estimate self-reported BMI. This index was classified according to the World Health Organization’s criteria: malnutrition ≤ 18.4 kg/m2, normal from 18.5 to 24.9 kg/m2, overweight from 25 to 29.9 kg/m2, and obesity ≥ 30 kg/m2 (WHO, 2013). There is evidence supporting the reliability of self-reported BMI in Mexican adult populations (Osuna-Ramírez, Hernández-Prado, Campuzano, & Salmerón, 2006) and in college students in Colombia (Martínez-Torres et al., 2013). Procedure In July 2012, the Board of the Biological and Health Sciences Division of the Metropolitan Autonomous University, Xochimilco Campus (Spanish acronym, UAM-X), in Mexico City, approved the research project from which the present study is derived. Before the Body Project workshop was given, authorization was requested from teachers of each class. Activities were carried out at dates and times that did not interfere with class hours previously agreed with teachers. Students were evaluated with a battery of tests at three different times: 1) before beginning workshop sessions, 2) at the end of the workshop, and 3) a year after the intervention. The average time for answering the questionnaires was 60 minutes. All participants were asked to sign an informed consent form stipulating the confidentiality of all data gathered, as well as their right to decline participation at any moment of the protocol. The intervention was conducted from 2012 to 2015, in groups of 20 mixed gender students, subdivided into 8 to 10 participants for the first four sessions and all together (up to 20 students) for the fifth session. Each group began and ended the intervention at different points during this period. The workshop was organized into five sessions, each lasting approximately two hours along five weeks. Unlike the original Body Project proposal, in this study the time allotted for each session was extended to enhance student participation. A fifth session was added to create a space to share the two last home works with the whole group: these are the letter to a younger self and the self-affirmation exercise. Two facilitators coordinated the sessions following the Body Project Facilitators Guide available on the Internet (www.bodyprojectsupport.org) and in the original publication (Stice, Rodhe et al., 2007). The only difference in the interventions for females and males was the use of the concept of the esthetic body thin ideal for the former and the esthetic muscular body ideal for the latter. The rest of the facilitator’s guide was followed strictly. The facilitator’s guide was designed to disseminate the program (Stice, Rodhe et al., 2007), with specific instructions for the accurate implementation of each workshop session, to enhance the effect of the intervention (Butryn, Rodhe, Marti, & Stice, 2014). A key aspect in guaranteeing the effectiveness of the intervention was the training of group facilitators. Project leaders (the first and second author of this paper), who are health professionals with extensive experience in coordinating the workshop, also acted as facilitators. Moreover, after participating in the workshop as respondents, some of the students expressed interest in becoming group facilitators. Facilitators training was carried out as follows: 1) participating in the workshop as subjects of the intervention, 2) participating as observers during the holding of the workshop by one of the project leaders and after having studied the facilitator’s guide, 3) participating as an assistant (i.e., co-facilitator) during the organization of the workshop by a more experienced peer, and 4) conducting the workshop as a co-facilitator with a less experienced peer. Project leaders determined when facilitators were ready to take over a group, ensuring constant supervision. Data Analysis Frequencies, percentages, and central tendency measures were estimated to describe the demographic characteristics of the sample. Mean scores on DEB over time were compared using repeated measures MANOVA tests. To assess the associations between variables that the Body Project intervention is expected to modify, and which in turn are expected to influence change in DEB, one-way MANOVA analyses of repeated measures, with “time” as the within subject factor were performed: 1) DEB as dependent variable (DEB), 2) DEB as dependent variable and internalization as independent variable (DEB = IATI), 3) internalization as independent variable and depression as dependent variable (DS = IATI), 4) DEB as dependent variable and depression as independent variables (DEB = DS), and finally 5) a two-way MANOVA analysis of repeated measures with “time” as the within subject factor, was performed to determine the effectiveness of the intervention with internalization and depression as independent variables and DEB as dependent variable (DEB = DS + IATI) (Figure 1). Missing values for DEB variables (3.75%), IATI (2.73%), and DS (11.12%) were imputed, measured on a Likert scale and regarded as continuous variables. A parametric method involving a normal multivariate distribution was used. Since the imputed variables did not follow a Monotone missing pattern, the Makov Chain Monte Carlo distribution was used instead, making it possible to estimate the mean vector and the variance and co-variance matrix. Figure 1 Theoretical Model. 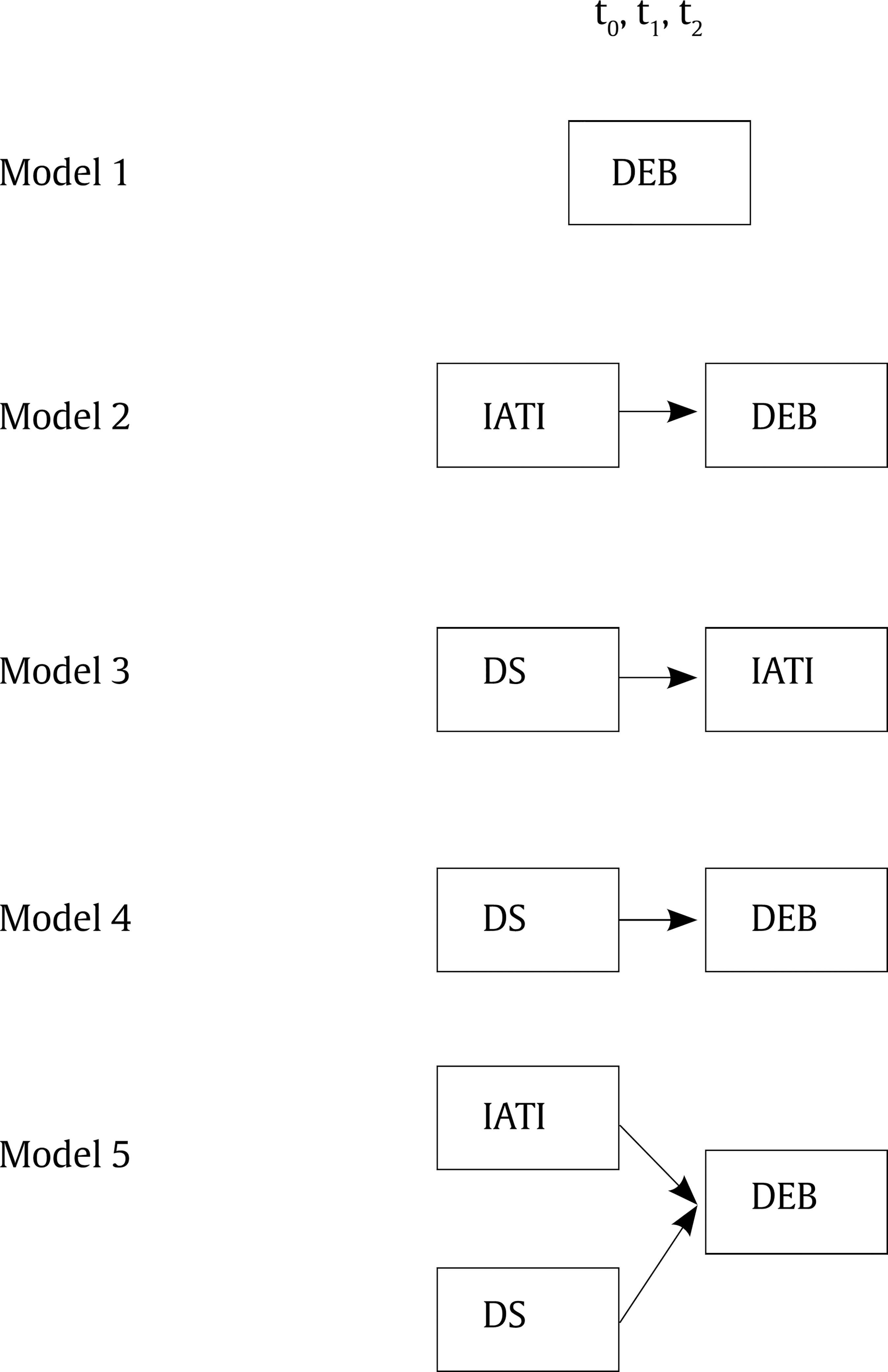 Note. DEB = disordered eating behaviors; IATI = internalization of the esthetic thin ideal; DS = depressive symptoms. For tests that involve only between subjects’ effects and their interactions, both the multivariate and univariate approaches give rise to the same tests. Tests for within subject effects and related interactions depend on the sphericity test. If Mauchly’s sphericity test is rejected, the significance is proved through the Greenhouse-Geisser and Huynh-Feldt-Lecoutre’s univariate test, otherwise Wilks’ lambda multivariate test is used. DEB and IATI were recoded into dummy variables using the cut-off scores of each (Unikel et al., 2004; Unikel et al., 2006), to classify subjects as at-risk or not-at-risk. In order to analyze the depressive symptoms scale, this sample’s mean values plus one standard deviation were used, considering subjects above this cut-off score as being at risk. Analyses were carried out in SAS 9.4 for Windows (SAS Institute Inc., 2013). ResultsThe sample consisted of women and men who, on average, were 22.4 ± 3.5 years old at pretest (t0), 22.2 ± 3.4 years at posttest (t1), and 23 ± 3.4 years at one-year follow-up (t2) (Table 1). Participants reported an average BMI of 22.9 (SD = 3.0). Table 1 Distribution of the Sample for Each Age Measurement 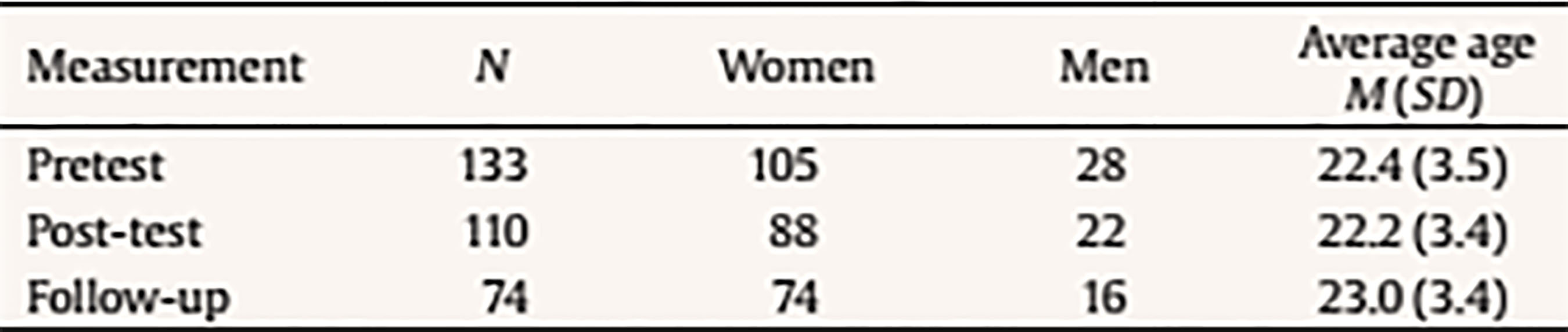 A MANOVA of repeated measures analysis showed that for DEB (Model 1) the average value in t0 was 5.23, which fell to 3.45 in t1, and 2.80 in t2. The analysis also showed that this difference in time was statistically significant, F(2, 140) = 20.31, p < .01, with a value of ή2 = 22%. Model 2 included IATI as an independent dichotomous variable and DEB in the three measurements as a dependent variable (Figure 2). Results showed a significant effect of time, F(2, 138) = 34.81, p < .01, with a value of ή2 = 33%. The interaction of time with IATI was also significant, F(2, 138) = 12.77, p < .01. The difference between the mean scores in the BQDEB in the groups with a high and low score by IATI was therefore 5.96 at t0, 4.33 at t1 and 1.13 at t2. This last value was statistically different from the two previous measurements (Table 2). Figure 2 Model 2: Changes in Disordered Eating Behaviors according toInternalization of the Esthetic Thin Ideal.  Table 2 Multiple Repeated Measures Analysis of Variance 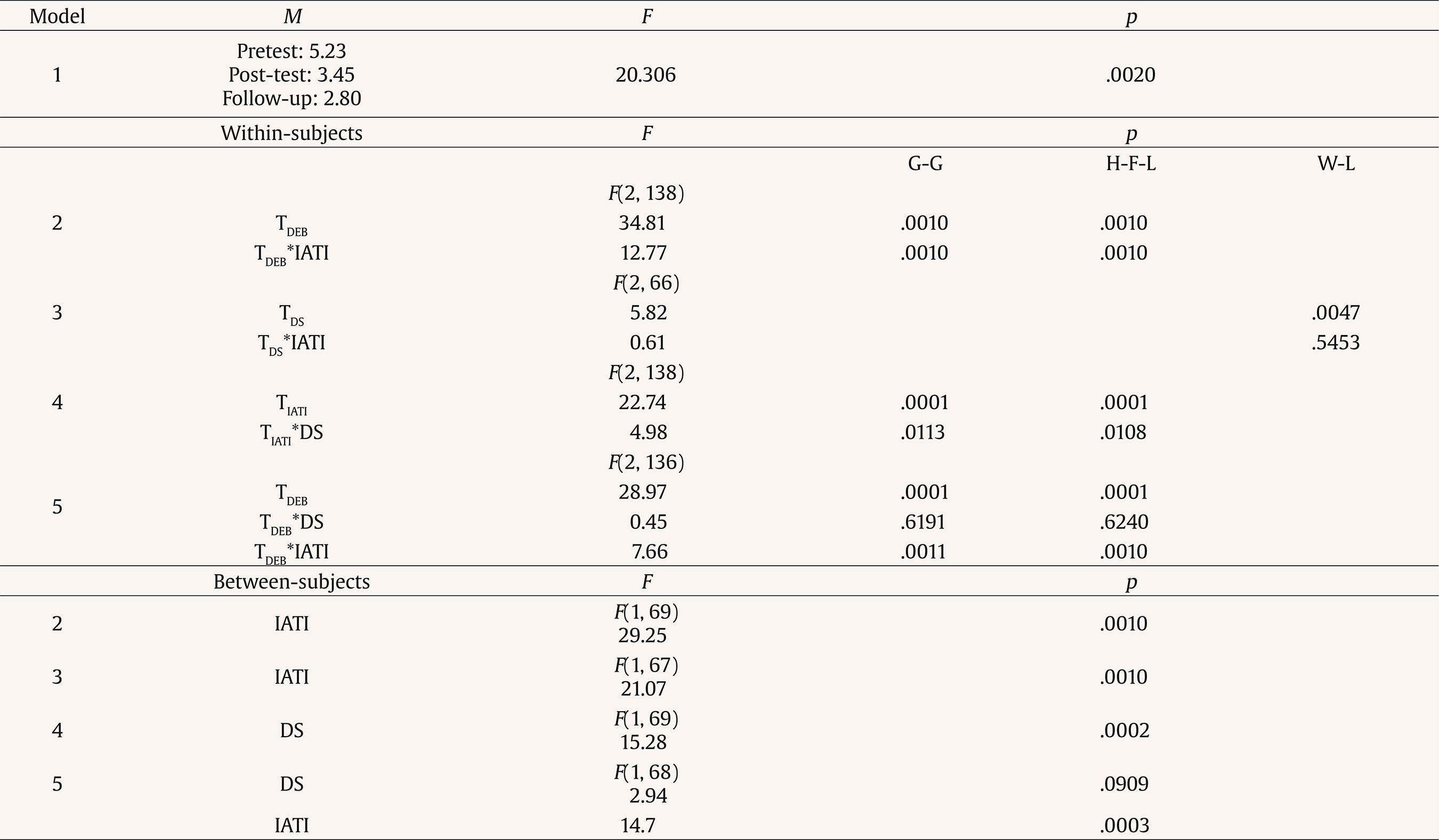 Note. T = time; IATI = internalization of esthetic thin ideal; DEB = disordered eating behaviors; DS = depressive symptoms; G-G = Greenhouse-Geisser; H-F-L = Huynh-FeldtLecoutre; W-L = Wilks’ Lambda. The third model included DS as dependent variable and IATI as an explanatory dichotomous variable (Figure 3). There was a statistically significant difference in t0, t1, and t2 mean values (Wilks’ Lambda, F = 5.88, p < .01) with ή2 = 15%, as well as for IATI (Wilks’ Lambda, F = 31.87, p = .0001), ή2 = 49%. The effect of time was significant (Wilks’ Lambda, F(2, 66) = 5.82, p < .01. Conversely, the interaction of time with IATI was not statistically significant. Figure 3 Model 3: Changes in Depressive Symptoms according to Internalization of the Esthetic Thin Ideal. 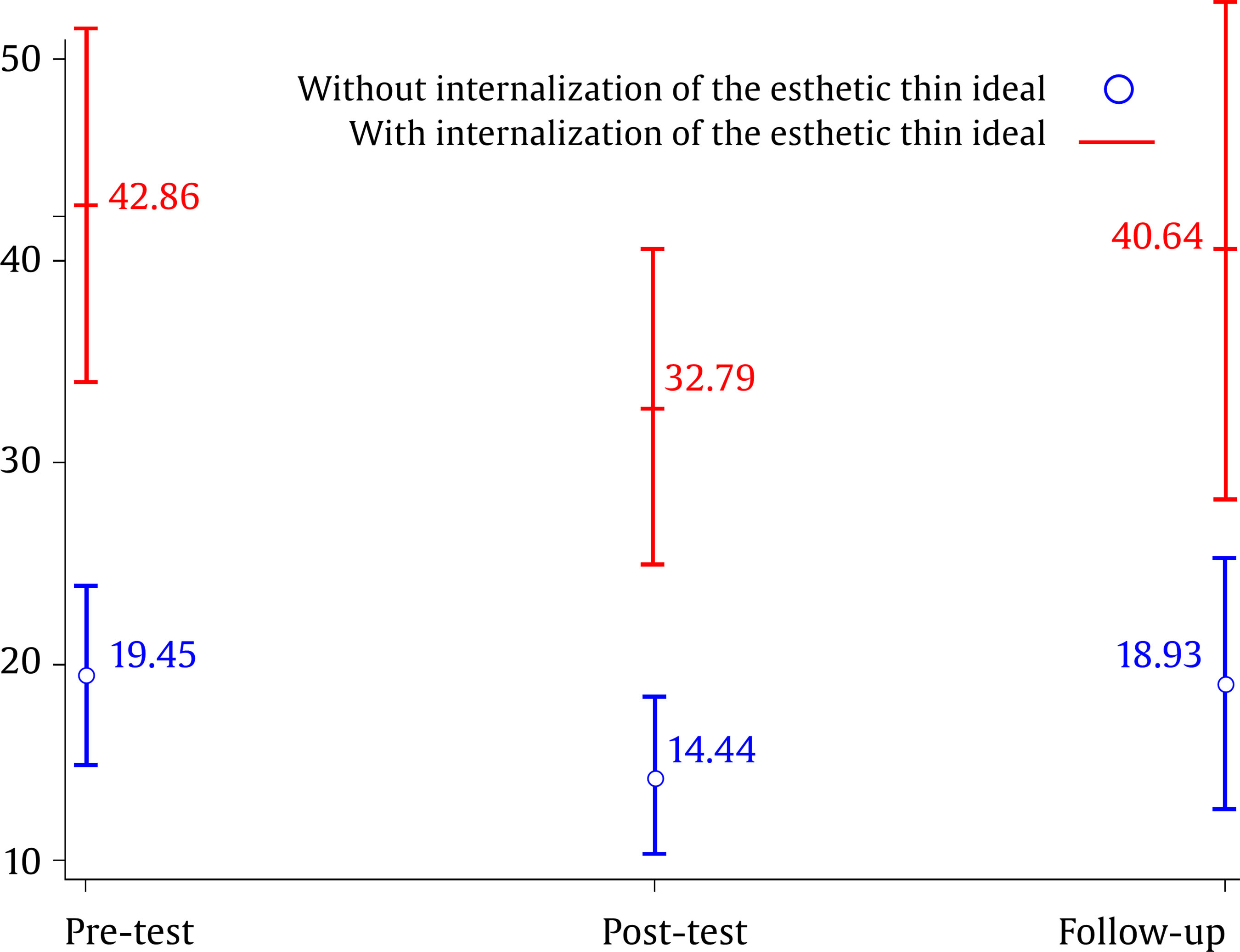 The fourth model was performed with DEB as the dependent variable and DS as the explanatory variable (Figure 4). The test showed a significant effect of time F(2, 138) = 22.74, p < .01, with values of ή2 = 24%. The interaction between time and DS was significant F(2, 138) = 4.98, p < .01. The difference between means in the DEB score between the groups with high and low levels of depressive symptoms was 5.09 at t0 (with ή2 = 20.43%), 3.54 at t1 (with ή2 = 13.03%), and 1.62 at t2 (with ή2 = 4.41%). Figure 4 Model 4: Changes in Disordered Eating Behaviors according to Depressive Symptoms. 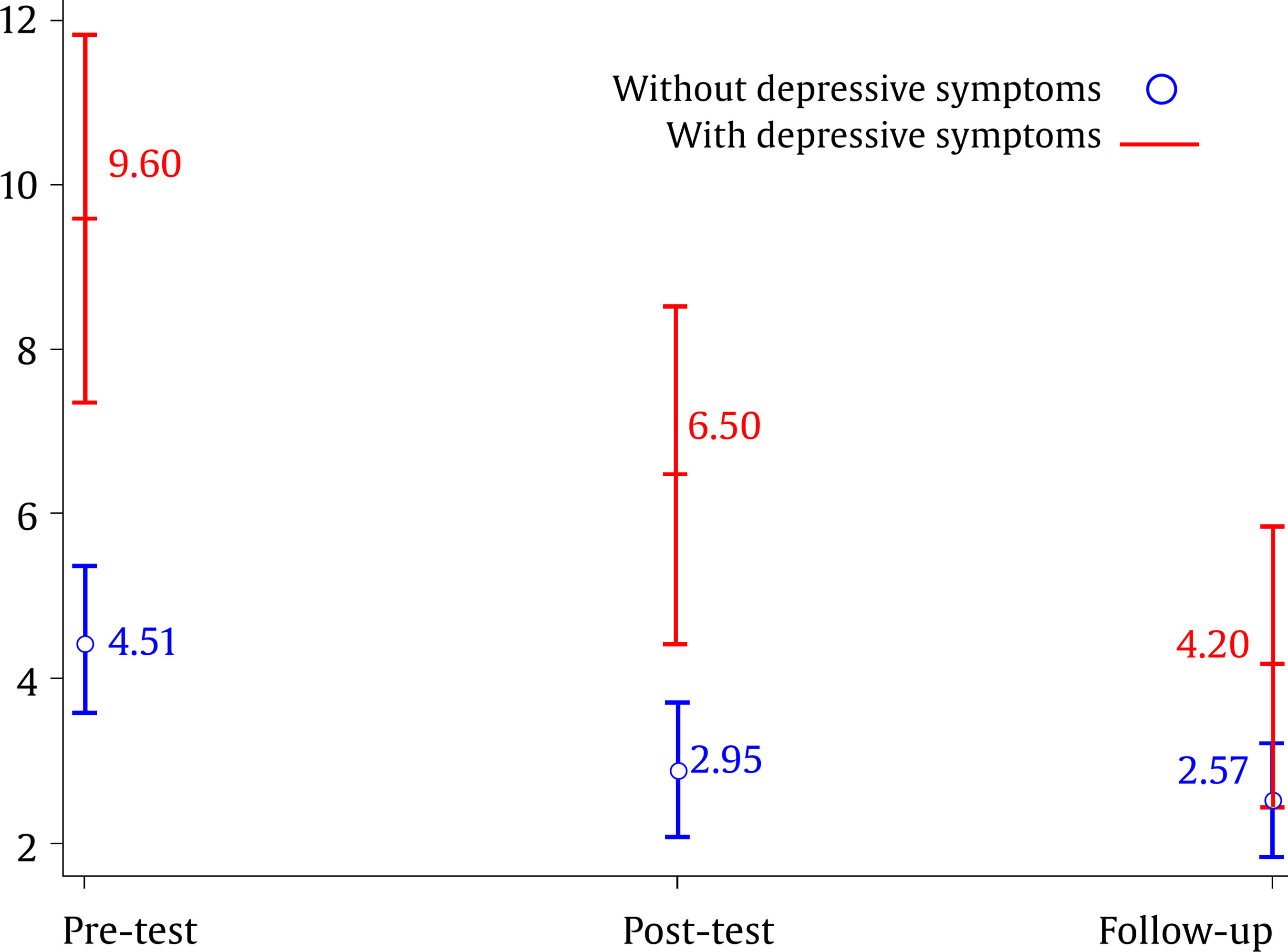 In the fifth model, the DEB score was considered as a dependent variable and both DS and IATI as explanatory variables (Table 2). The effect of time on DEB was significant, F(2, 136) = 28.97, p < .01. Conversely, time interaction with DS was not statistically significant, although the interaction of time with IATI was significant, F(2, 136) = 7.66, p < .01. The difference of the mean BQDEB score at t1 between the group with a high and low levels of IATI was 3.71, whereas at t2 it was 0.79. DiscussionThe results of this study show that the program achieved effects at one-year follow-up of the subjects in the reduction of DEB, IATI, and DS achieving the objectives proposed. The most recent systematic reviews and meta-analyses performed on ED prevention (Khanh-Dao, Barendregt, Hay, & Mihalopoulos, 2017; Watson et al., 2016) suggest that interventions based on media literacy are the most effective means of reducing ED risk factors for universal prevention schemes and that dissonance-based interventions are the most effective options for selective prevention. Nevertheless, our results confirm the importance of universal prevention interventions, in which the risk of stigmatizing is reduced and participation rates increased (Marchand, Stice, Rohde, & Black-Becker, 2011). Khahn-Dao et al. (2017) and Watson et al. (2016) did not include dissonance-based interventions in universal prevention, meaning that there are no data to prove their efficacy. Stice, Shaw et al. (2007) found a greater effect in subgroups with high risk of DEB in universal interventions, in comparison with low-risk subjects. In this study, results showed that when subjects with a high and low IATI were compared, the scores of both were matched at the low level at one-year follow-up. As the authors noted, a floor effect occurs in those with low scores, due to the low level of psychopathology. As for our second assumption, the esthetic thin ideal had an effect on DEB in time, which declined a year after the intervention was carried out. This coincides with what is proposed by Stice, Shaw, and Marti (2006) regarding the effect IATI has as a mediator in the reduction of DEB, proposed in the Dual-Pathway Model of Bulimic Pathology (Stice, 2001). Conversely, the third assumption was not significant, given that IATI did not have an effect on DS over time, although the literature shows that they constitute a significant risk factor for the development of ED (Jacobi et al., 2011). According to Killen et al. (1996), IATI works in conjunction with body dissatisfaction, dieting, and negative affect in the promotion of DEB. However, in our results, this relationship was not observed, probably because we did not use a specific measure for negative affect but, instead, a DS questionnaire. Although DS did have an effect on DEBs, as observed in the fourth model (fourth assumption), and statistical significance was found when the fifth assumption was included, where the interaction of both IATI and of DS on DEB was sought, the effect of DS was cancelled, leaving only IATI. A limitation in undertaking interventions for young people in Mexico is the lack of motivation of study subjects to participate voluntarily in research projects. Moreover, it is not part of Mexican research culture to reward college students’ participation financially, in kind, or with academic credits, as happens in other countries. Forcing students to participate would constitute ethical misconduct and mean that we were not working with volunteers. These difficulties have led us to propose prevention workshops as part of the range of academic activities offered to students, which yield positive results, as suggested in this study. At the same time, this has led to a high rate of attrition of the sample, since young people do not consider this type of long-term interventions to be of benefit to themselves or their community. It is essential to implement mechanisms that encourage the development of this type of research, considering the specific characteristics of Mexico’s institutions and the idiosyncrasy of the various population groups. However, a small group of students expressed interest in being trained as workshop facilitators and, subsequently, as coordinators of working groups and trainers of other young people who wish to be actively involved in the intervention. Stice et al.’s, (2017) findings, regarding the power of peer-led interventions, support our initiative to incorporate students as facilitators of the Body Project workshop. Regarding Mexican cultural adaptation of the Body Project, the main changes were related to the session format. We did not stick to the time scheduled as people tend to be very specific when talking about personal experiences; accordingly, we expanded sessions from one hour, as marked in the facilitators guide which was not enough, to two hours. In a previous experience with the Body Project we realized that people did not send the fourth session’s homework by email; therefore, a fifth session was incorporated to be sure students carried out the last homework. Other changes in content were related to examples that do not apply to Mexican culture, such as pertaining to a fraternity or being a cheerleader; we also used images of famous Mexican and Latin-American singers and actors. As we worked with mixed-gender groups, male and female images were used to carry out the first session definition and thin body-ideal exercise, in which men were asked to choose males images and women female ones. The rest of the program was carried out faithfully. The main limitation of the present study is the absence of a control group on a waiting list or a comparison with another intervention. Another limitation was a lack of more effective strategies to ensure a better response rate during follow-up to reduce the attrition of the sample. However, its main strength lies in the fact that this is the first-time evidence from the Body Project that has been provided for Mexico. It would be important for future studies to expand the size of the sample, particularly of male students, as well as including weight and height measures, in addition to those reported by the students themselves. In conclusion, the positive effect of IATI on DEBs after a year’s follow-up encourages us to continue with the Body Project and to test new hypotheses regarding dissonance-based prevention interventions on Mexican populations. Acknowledgements Thanks are due to Dr. Erik Stice for his permission to replicate the Body Project prevention programme and his encouragement to conduct this research, and to Dr. David Bisetto Pons for providing the Spanish version of the facilitator’s guide translated into Spanish for the research project “Risky Eating Behaviour Prevention among the Adolescent Population” at the University of Valencia, Spain, and permitting its use in a disinterested way. We are also grateful to the group facilitators: Fernanda Oropeza Aguirre, Verónica Hernández Valdez, Claudia Correa Ponce, Itzel Flores Gálvez, Eunice I. Alvarado Zapata, Verónica M. Hawley Luna, Luis Felipe Malváez Gómez, Héctor Rodrigo Vallejo Chavarría, Josué de Jesus Torres Celis, Laura Trinidad Rojas, Abril P. González Martínez, and Cinthya Paola Aguilar Vargas. Cite this article as: Unikel-Santoncini, C., Díaz de León-Vázquez, C., Rivera-Márquez, J. A., Bojorquez-Chapela, I., & Méndez-Ríos, E. (2018). Dissonance-based program for eating disorders prevention in Mexican university students. Psychosocial Intervention., 28, 29-35. https://doi.org/10.5093/pi2018a17 |
Cite this article as: Unikel-Santoncini, C. , León-Vázquez, C. D. D. , Rivera-Márquez, J. A. , Bojorquez-Chapela, I. , and Méndez-Ríos, E. (2019). Dissonance-based Program for Eating Disorders Prevention in Mexican University Students. Psychosocial Intervention, 28, 29 - 35. https://doi.org/10.5093/pi2018a17
Correspondence: unikels@imp.edu.mx(C. Unikel-Santoncini).
Copyright © 2024. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef Print
Print Send
Send






