


User Violence and Psychological Well-being in Primary Health-Care Professionals
[La violencia de los usuarios y el bienestar psicológico en los profesionales de atención primaria de salud.]
Cecilia López-Garcíaa, José A. Ruiz-Hernándeza, Laura Llor-Zaragozab,Paloma Llor-Zaragozac and José Antonio Jiménez-Barberoa
aUniversidad de Murcia, Campus Mre Nostrum, Spain; bUniversidad Católica San Antonio de Murcia, Spain; cHospital General Morales Meseguer, Murcia, Spain
https://doi.org/10.5093/ejpalc2018a6
Received 3 February 2017, Accepted 23 September 2017
Abstract
It is estimated that one fourth of workplace violent incidents occur in the health sector. The aims of the present investigation are: a) to identify sociodemographic and work variables related to exposure to user violence in primary care professionals and b) to the impact of exposure to user violence on professionals’ psychological well-being, job satisfaction, and empathy. An empirical study with quantitative, descriptive, and transversal methodology was carried out with a sample of 574 professionals from 39 primary-care centers. The study revealed that variables of gender, professional tenure, continued training, and professional status are significantly associated with exposure to user violence. Likewise, the results that depending on professional status exposure to user violence, job satisfaction and professionals’ empathy have an impact on primary health-care workers’ General Health Questionnaire (GHQ) scores. In conclusion, exposure to non-physical user violence in primary-care professionals is associated with some sociodemographic and work characteristics.
Resumen
Se estima que una cuarta parte de los incidentes violentos laborales se producen en el ámbito sanitario. Los objetivos de la presente investigación son: a) identificar las variables sociodemográficas y laborales relacionadas con la exposición a la violencia de los usuarios en profesionales de atención primaria y b) analizar el impacto sobre el bienestar psicológico de los profesionales de la exposición a la violencia de los usuarios, la satisfacción laboral y la empatía. Se llevó a cabo un estudio empírico con metodología cuantitativa, descriptivo y transversal, con una muestra de 574 profesionales de 39 centros de atención primaria. Se observa que las variables de género, antigüedad en la profesión, formación continuada y categoría profesional se encuentran asociadas significativamente a la exposición a la violencia de los usuarios. Del mismo modo, se identifica que la exposición a las conductas violentas de los usuarios, la satisfacción laboral y la empatía de los profesionales influyen, dependiendo de la categoría profesional, en las puntuaciones de GHQ total de los trabajadores de atención primaria. En conclusión, la exposición a la violencia no física de los usuarios en los profesionales de atención primaria se asocia con ciertas características sociodemográficas y laborales.
Keywords
Aggression, Health staff,Job satisfaction, Primary health-care, Psychological well-being, Workplace violence
Palabras clave
Agresión, Personal sanitario, Satisfacción laboral, Atención primaria, Satisfacción laboral, Violencia laboral
Cite this article as: López-García, C., Ruiz-Hernández, J. A., Llor-Zaragoza, L., Llor-Zaragoza, P., & Jiménez-Barbero, J. A. (2018). User violence and psychological well-being in primary health-care professionals. The European Journal of Psychology Applied to Legal Context, 10, 57-63. https://doi.org/10.5093/ejpalc2018a6
Correspondence: Jaruiz@um.es (José A. Ruiz-Hernández).
Introduction The topic of workplace violence in the health-care setting is nowadays increasing persistently because, until recently, the severity and consequences of this problem were virtually unknown due to the underestimation and the few legal charges of violent behaviors, as in other areas where violence takes place (Cala, Trigo, & Saavedra, 2016; Contreras, & Cano, 2016; Mayorca Yancán, Lucena García, Cortés Martínez, & Lucerna Méndez, 2013). Workplace violence has been defined as “incidents in which workers suffer abuse, threats or attacks in work-related circumstances—including traveling to and from work—that endanger, implicitly or explicitly, their safety, well-being, or health” (International Labour Organization/International Council of Nurses/World Health Organization/Public Services International, ILO/ICN/WHO/PSI, 2002, p. 3) and, depending on its forms of expression, it can be classified as: a) verbal, psychological or non-physical violence, referring to verbal abuse, threats, ironic language, contemptuous looks, provocative or aggressive body language, and communication styles based on humiliation and intimidation; and b) physical violence, referring to physical intimidation and harm to persons, properties or furniture (ILO/ICN/WHO/PSI, 2002; Ureña, Romera, Casas, Viejo, & Ortega-Ruiz, 2015; Waschgler, Ruiz-Hernández, Llor-Esteban, & García-Izquierdo, 2013). In this study, we focus on the analysis of violent user behaviors of low and medium intensity towards the professionals of Primary Care (hereinafter PC), without considering aggressions performed by coworkers or superiors. Workplace violence is considered an important professional risk of psychosocial origin that is triggered by the confluence of various factors, which can be classified as follows: (a) patient factors – male sex, age, presence of physical alterations and pathologies, mental state, presence of psychopathology, patients’ perspective; (b) individual factors of health professionals, such as burnout or their attitudes; (c) environmental or organizational factors –type of room, such as emergency units, psychiatry and intensive care units, long-term care or geriatric centers, insufficient staff, assistential pressure, lack of privacy, a climate of tension; (d) factors related to treatment, such as changes or suspension of medication; and (e) factors of interaction and social factors (Ahmad, Al-Rimawi, Masadeh, & Atoum, 2015; Chapman, Styles, Perry, & Combs, 2010; El-Gilany, El-Wehady, & Amr, 2010; Llor-Esteban, García-Jiménez, Ruiz-Hernández, & Godoy-Fernández, 2016; Speroni, Fitch, Dawson, Dugan, & Atherton, 2014; Waschgler et al., 2013). Numerous studies (Da Silva et al., 2015; Galián-Muñoz, Ruiz-Hernández, Llor-Esteban, & López-García, 2016; Jaradat et al., 2016; Llor-Esteban, Sánchez-Muñoz, Ruiz-Hernández, & Jiménez-Barbero, 2017) have confirmed that workplace violence towards health professionals has important consequences for their psychological well-being, manifesting with symptoms of anxiety and/or depression, among others. El-Gilany et al. (2000) also found that mistrust, anger, job dissatisfaction, irritability, and anxiety are some of the most frequent consequences of workplace violence in PC professionals. Bernaldo-De-Quirós, Piccini, Gómez, and Cerdeira (2015) concluded that the health staff who has suffered some type of workplace violence present greater anxiety, emotional exhaustion, depersonalization, and higher levels of burnout than those who have not experienced any aggression. Likewise, variables such as empathy or job satisfaction have been associated with anxious and depressive symptoms, a frequent way of measuring psychological well-being. With regard to job satisfaction, various studies have reported its relation with psychological well-being in health professionals (Amati et al., 2010; Emmanuel Olatunde & Odusanya, 2015; Khamisa, Oldenburg, Peltzer, & Ilic, 2015; Ríos-Risquez, & Godoy-Fernández, 2008; Teles et al., 2014), such that job dissatisfaction has been associated with poorer psychological well-being. Regarding health professionals’ empathy, diverse investigations have shown its influence on their own psychological health, finding that higher scores in perspective taking—a central component of empathy—have been associated with higher psychological well-being (Shanafelt et al., 2005) and lower scores in the burnout dimension of emotional exhaustion (Lamothe, Boujut, Zenasni, & Sultan, 2014). Considering the theoretical framework of reference, the goals of the present study aim to: (a) identify the sociodemographic and job variables related to exposure to user violence in PC professionals and (b) analyze the impact of exposure to user violence on the professionals’ psychological well-being, job satisfaction, and empathy. MethodAn empirical study with quantitative, descriptive, and cross-sectional methodology was performed in the area of Primary Health Care. This study was approved by the Commission of Research Ethics of the University of Murcia and by the Managing Directors of the participant health areas. Participants The study population consisted of PC professionals who worked in various Health Areas of the Health Service of Murcia. Following the internal organization of PC centers, professionals were grouped into three collectives: doctors, nursing staff, and non-health staff who carry out support functions. We obtained a sample made up of 574 professionals from 39 PC centers. This sample represents 22.3% of the total PC staff of the Health Service of Murcia. Initially, a total 670 assessment protocols were handed out, as we estimated a 30% rate of non-response. The global response rate was 85.7%. The majority were women (68.1%), married or living with a partner (72.6%) and with a mean age of 49.6 years (SD = 8.4). Concerning working conditions, 82.6% of the participants had a permanent contract and a mean job tenure in the profession of 23.6 years (SD = 9.1). Moreover, 38.9% were doctors, 34% nursing staff, and 25.8% non-health staff. Table 1 shows the main socio-demographic and work data of the sample. Table 1 Socio-demographic and Job Characteristics of the Sample 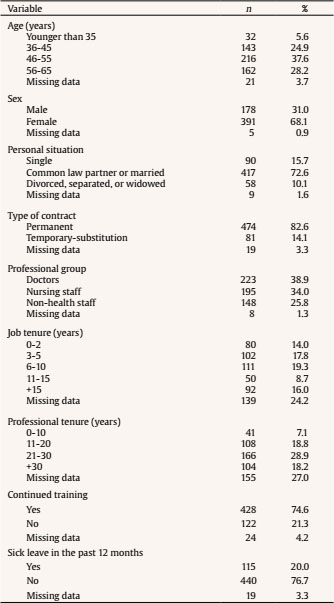 Instruments Together with a questionnaire designed ad hoc to collect socio-demographic and work data, the following scales that assess different psychosocial variables were used: Health-care Workers’ Aggressive Behaviour Scale -Users- Primary Healthcare Version (HABS-U-PHC; Ruiz-Hernández, López-García, Llor-Esteban, Galián-Muñoz, & Benavente-Reche, 2016). This instrument evaluates users’ hostile behaviors of low and medium intensity towards PC professionals. It is made up of 14 items about the violence suffered during the past year, rated on a 6-point Likert-type ranging from 1 (never) to 6 (daily), and explains 51.2% of the variance. Its items are grouped into two factors: Factor I (non-physical violence), with 11 items about users’ verbal and nonverbal violence, which explains 40.6% of the variance (α = .92) and Factor II (physical violence), consisting of 3 items that account for 10.6% of the variance (α = .68). Goldberg’s General Health Questionnaire 28-item version (GHQ-28; Goldberg & Hillier, 1979), using the Spanish adaptation by Lobo, Pérez-Echeverría, and Artal (1986). This questionnaire is a general measure of psychological well-being that is distributed in 4 subscales of 7 items each: psychosomatic symptoms (feelings of exhaustion, weakness, and bodily distress), anxiety/insomnia, social dysfunction (problems to perform and enjoy daily activities), and depressive symptomatology (thoughts and feelings of personal uselessness, sadness, hopelessness, and suicide). Each item has four response options on a Likert-type scale (from 0 to 3), where higher scores indicate worse psychological well-being. Values of Cronbach’s alpha of .92 for the total GHQ and between .74 and .90 for the subscales have been observed in this instrument (Waschgler, Ruiz-Hernández, Llor-Esteban, & Jimenez-Barbero, 2013). Overall Job Satisfaction (OJS; Warr, Cook, & Wall, 1979), adapted to Spanish by Pérez and Hidalgo (1995). This scale assesses job satisfaction and is made up of 15 items divided into two subscales: extrinsic satisfaction, which asks about the organization of work, such as the schedule, remuneration, physical conditions, relations between managers and workers, job stability, etc., and intrinsic satisfaction, which deals with job content, such as acknowledgment received for work, assigned responsibility, professional promotion, etc. (Berrios-Martos, Augusto-Landa, & Aguilar-Luzón, 2006). They are rated on a 7-point Likert-type response format ranging from 1 (very dissatisfied) to 7 (very satisfied), such that higher scores reflect greater satisfaction. For this instrument, values of Cronbach’s alpha of .87 for general satisfaction and of .70 and .84 for extrinsic satisfaction and intrinsic satisfaction, respectively, have been obtained (Waschgler et al., 2013). Jefferson Scale of Physician Empathy (JSPE; Hojat et al., 2002) using the adaptation of Alcorta-Garza, González-Guerrero, Tavitas-Herrera, Rodríguez-Lara, and Hojat (2005). This scale assesses empathy and consists of 20 items distributed in three factors: Factor I – perspective taking, which corresponds to the central element of empathy –, Factor II – compassionate care –, and Factor III – skill to put oneself in the patient’s place. These are specific components of the relationship with the patient. They are reverse-worded, such that high scores indicate less empathy, and vice versa. The Likert-type items are rated from 1 (totally disagree) to 7 (totally agree). In our investigation, the factor skill to put oneself in the patient’s place obtained low internal consistency (α = .47) so, statistically speaking, it was not used in this study. For this scale, values of Cronbach alpha between .76 and .84 were obtained (Ferreira-Valente et al., 2016; Jumroonrojana & Zartrungpak, 2013; Paro, Daud-Gallotti, Tibério, Pinto, & Martins, 2012). Procedure Considering the total of the 2,575 professionals from 74 PC centers, according to the data provided by the Health Service of Murcia, we estimated a sample size of 510 professionals with a 95% confidence level and an assumed error of ± 3%. To select the participants, we used two-stage cluster sampling. Firstly, the population was stratified by CP centers (clusters), and 39 centers were selected through simple random sampling. Subsequently, using a fixed ratio pattern, we randomly selected from the alphabetical listing of all the professionals from each center those who were numbered with multiples of three. Meetings were held with the coordinators of the selected health centers where they were informed about the study, and we distributed the research protocol in printed version. We programmed visits to the center to clarify possible doubts and collect the completed protocols. Participation was voluntary, ensuring strict confidentiality, and anonymity of the data collected. Data Analysis Data analysis was carried out using the SPSS (version 22.0) statistical package. We initially performed a descriptive analysis of the sample, and Student’s t-test and ANOVA were used to determine possible differences between exposure to user violence and the sociodemographic and job characteristics of the sample. To determine differences between the various professional groups and the variables of the study, we used ANOVA together with the post hoc Tukey test in the variables that met the assumption of variance homogeneity, and ANOVA by means of the robust Brown-Forsythe test, along with Games-Howel post hoc test in cases where the assumption was not met. We calculated the mean score and standard deviation of the scales used, and Pearson correlation coefficients as a function of the professional group among the variables of the study. We performed multiple linear regression analysis on total GHQ variable with the variables with which it showed a significant relation in order to develop a predictive model of psychological well-being in the different groups of PC professionals. ResultsWith regard to the sociodemographic characteristics of the sample, statistically significant differences were obtained between the factor of non-physical violence and sex and age variables. Women presented higher scores than men (t = -3.34, p = .001) and age correlated significantly and negatively with non-physical violence (r = -.14, p = .001), that is, younger practitioners reported more exposure. Regarding job variables, there were significant differences between non-physical violence and years of professional tenure (r = -.18, p < .000). In this sense, professionals with less job tenure presented higher scores in non-physical violence. Due to the relation between age and years of professional tenure variables, we studied their possible nesting, including them concurrently in a regression model of non-physical violence. The results showed that only professional tenure maintained its significant relation with non-physical violence (t = -2.45, p = .015). Taking into account the continued training variable, we observed that the professionals who do not receive such training presented higher scores in non-physical violence (t = -3.49, p = .001). With regard to type of contract and job tenure in the position, no significant relationships were observed with user violence. No significant differences were found in either of the two factors of user violence in the case of the sick leave variable in the past 12 months. We analyzed the relationship of professional group with the variables of the study (Table 2), finding significant differences in all variables, except for physical violence. Non-health staff presented significant higher mean scores than the rest of professional groups on the total GHQ scale (F(2, 555) = 5.58, p = .004), and significantly lower scores on extrinsic satisfaction (F(2, 485) = 6.25, p = .002) and perspective taking, F(2, 471) = 6.92, p = .001. Table 2 Relation between the Various Groups of PC Professionals and the Variables of the Study  Table 3 Mean, Reliability and Pearson Correlations between Variables by Professional Group 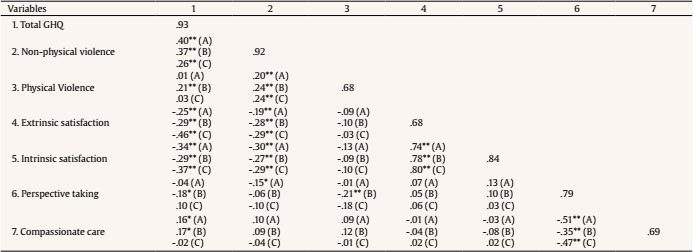 We also observed significant differences (p < .000) among the three professional groups in the variables of non-physical violence (Brown-Forsythe F(2, 295.6) = 43.72), intrinsic satisfaction (Brown-Forsythe F(2, 394.7) = 20.92), and compassionate care (Brown-Forsythe F(2, 344.2) = 24.87). The post hoc study (Table 2) indicated that non-health staff perceived the highest levels of non-physical user violence (M = 3.05, SD = 1.16), followed by doctors (M = 2.21, SD = 0.95), and, lastly, by nursing staff (M = 1.84, SD = 0.80). The nursing staff obtained the highest scores in intrinsic satisfaction (M = 27.12, SD = 6.88), whereas doctors obtained the highest scores in compassionate care (M = 43.54, SD = 5.06). Table 3 shows the Pearson correlations obtained between the variables of the study, taking into account the professional group. In doctors, the total GHQ scores correlated with non-physical violence (r = .40, p < .000), compassionate care (r = .16, p = .023), and extrinsic (r = -.25, p = .001) and intrinsic satisfaction (r = -.34, p < .000). In nursing staff, the total GHQ scores correlated significantly with all the variables, positively with both factors of violence and with the empathy factor of compassionate care, and negatively with subscales of job satisfaction and perspective taking. Lastly, in non-health staff, total GHQ scores correlated positively with non-physical violence (r = .26, p = .004) and negatively with extrinsic (r = -.46, p < .000) and intrinsic satisfaction (r = -.37, p < .000). Table 4 shows the model of stepwise multiple linear regression analysis obtained for global GHQ score, taking into account that variables were statistically significant in each professional group. In the case of doctors, the resulting model includes the variables of non-physical violence (β = .29, p < .000), Intrinsic satisfaction (β = -.29, p < .000), and compassionate care (β = .16, p = .020), and explains 24.3% of variance. In the case of nursing staff, the final model selected non-physical violence (β = .33, p < .000), intrinsic satisfaction (β = -.26, p = .002), and perspective taking (β = -.20, p = .015), and explained 24.5% of variance. With regard to non-health staff, only extrinsic satisfaction was significant (β = -.49, p < .000), explaining 23.2% of the variance. Table 4 Discussion and Conclusions Multiple Linear Regression Models for Total GHQ as a Function of Professional Group 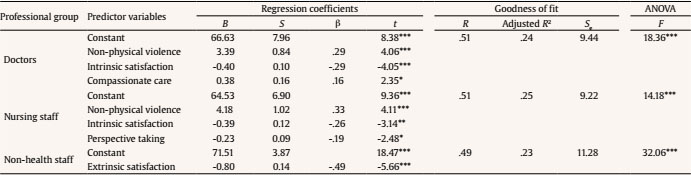 Taking into account the goals of the study, the results obtained indicate that PC professionals present significant differences in the scores of exposure to user violence as a function of their sociodemographic and job characteristics. In this sense, we observed that women report more exposure to non-physical violence than men, although in the literature consulted there is no homogeneity with regard to these results. Thus, some studies (Joa & Morken, 2012; Llor-Esteban et al., 2016) report more exposure to physical violence in men than in women, possibly because men feel less intimidated and less fearful and, therefore, expose themselves more to violent behaviors (Jansen, Middel, Dassen, & Menno, 2006). Alternatively, other studies (Fute, Mengesha, Wakgari, & Tessema, 2015; Ortells Abuyé, Muñoz Belmonte, Paguina Marcos, & Morató Lorente, 2013) report greater exposure to user violence in women, generally non-physical violence, as women may be considered easier targets of violence (Koritsas, Coles, Boyle, & Stanley, 2007). In other studies carried out in different health areas (Fisekovic-Kremic, Terzic-Supic, Santric-Milicevic, & Trajkovic, 2017; Galián-Muñoz, Llor-Esteban, & Ruiz-Hernández, 2014), no significant differences were obtained in exposure to user violence in relation to professionals’ gender. With regard to professional tenure, a negative relation was identified with non-physical violence, coinciding with the results of other studies carried out in the health area (Alameddine, Mourad, & Dimassi, 2015; El-Gilany et al., 2010; Fute et al., 2015; Galián-Muñoz, Llor-Esteban, & Ruiz-Hernández, 2012). Professionals with fewer years of professional experience present higher scores in non-physical violence, which can be attributed to their inexperience and lack of skills to prevent and properly deal with potentially troublesome situations with the users (Shields & Wilkins, 2009). In this regard, Whittington (2002) indicates that professionals with more than 15 years of job tenure show greater tolerance to patients’ violent behaviors, possibly due to the development of “professional wisdom” and an increase of confidence in dealing with aggressive patients. Moreover, it was found that professionals who do not receive continued training present higher scores in non-physical violence. A possible explanation is that professionals who do receive continued training have more action patterns to deal with, mediate in, and resolve troublesome situations with users than professionals who do not receive such a training. Various manuals for prevention of aggressions (Servicio Andaluz de Salud [Andalusian Health Service], 2004; Servicio Murciano de Salud [Health Service of Murcia], 2005) consider that Plans of Continued Training should contemplate instructing workers in general communication skills with the patients. Health professionals’ communication skills can help them feel safer and more competent and promote interpersonal relations with the patients (Leal-Costa, Tirado-González, Rodríguez-Marín, & van-der-Hofstadt-Román, 2016). No significant relationships were found with the physical violence factor, which may be conditioned by the small number of items that make up this factor and by the unusual behaviors described. Therefore, in future works, we will explore the inclusion of new items. With regard to the professional group, significant differences were obtained in the perception of non-physical violence. In our study, non-health staff holds a prominent place among the professions most exposed to non-physical user violence, followed by doctors and, finally, nursing staff. In the PC area, the group of non-health staff is recognized as vulnerable to patients’ violent behaviors. They are between the first and the last line of contact with users and, therefore, the ones who frequently receive patients’ demands and frustrations (Magin, Joyce, Adams, Goode, & Cotter, 2009). They usually perform most of their activity behind admission counters, which, following the recommendations of some protocols of prevention of aggressions (Servicio Canario de Salud [Canarian Health Service]; Health Service of Murcia, 2005), have installed some protection system, like glass partitions or a window. This measure minimizes physical aggressions towards this collective, as it is a physical barrier that prevents direct contact with non-health staff but, alternatively, it may produce an increase of non-physical violence because it hinders communication between professional and user (Blanquer Gregori, et al., 2003), forcing both speakers to raise their voices, which can trigger a troublesome situation. For this reason, it is not surprising that this professional group is the most exposed to non-physical user violence in the PC area. In this sense, Magin et al. (2009) carried out a qualitative research focused on this group, which highlights that PC receptionists are subject to considerably frequent workplace violence. However, in other studies (Da Silva et al., 2015; El-Gilany et al., 2010; Fisekovic-Kremic et al., 2017; Gascón et al., 2013; Magnavita & Heponiemi, 2012), it is considered that the professionals most exposed to user violence are doctors and nursing staff. It is difficult to make a comparison with other studies because we have analyzed the mean score of each variable as a function of the professional PC category. With regard to the exposure to violence, we cannot compare our results with other studies’ due to the novelty of the use of the HABS-U-PHC as the assessment instrument. With regard to the analyses carried out to predict the scores in psychological well-being (total GHQ), the predictors that were significantly associated vary as a function of the professional PC group. Non-physical violence is present in doctors and nursing staff, so a high exposure to non-physical troublesome situations with users directly impacts total GHQ scores of these professionals, implying a decrease or worsening of their psychological well-being. This outcome coincides with those obtained in numerous studies that reveal that workplace violence is associated with negative consequences in the psychological health of concerned professionals (Llor-Esteban et al., 2017; Magin et al. 2009). In this sense, Lam (2002) found that exposure to workplace aggressions is a risk factor of nursing staff’s mental health status, and Gerberich et al. (2004) observed that nurses who had been exposed to non-physical violence had more psychological consequences (frustration, anger, depression, fear, anxiety, etc.) than those exposed to physical violence. Intrinsic satisfaction is a predictor of psychological well-being (total GHQ) in the categories of doctors and nursing staff. In this case, the relation is inverted, that is, both groups of professionals consider that their score in psychological well-being (total GHQ) is influenced if they are dissatisfied with aspects related to the contents of their work. With regard to empathy, Factor I (perspective taking) inversely influences the scores in psychological well-being (total GHQ) of nursing staff and Factor II (compassionate care) directly influences the scores of GHQ total of doctors. In both cases, the results indicate that higher scores in empathy factors are related to lower scores in total GHQ scale, that is, it can be considered that greater empathy prevents psychological distress in PC professionals. These results are consistent with those obtained by Shanafelt et al. (2005), where higher scores in empathy were related to better psychological well-being. In the case of non-health staff, only extrinsic satisfaction is a predictor of their scores in psychological well-being (GHQ total). It is striking that being the professional group the one that has perceived more user violence, this variable does not influence their total GHQ scores. A possible explanation is the fact that these professionals have probably become familiar with non-physical user violence, incorporating it as part of their work. Therefore, it does not appear as a predictor of psychological well-being (GHQ total), which is only influenced in this professional group by their job satisfaction derived from their working conditions, such as wages, schedules, physical environment, etc. The present paper presents the typical limitations of retrospective studies. We relied on participants’ recall, which may not be accurate when trying to remember events that occurred previously. Unlike other studies on user violence, in our study, all professional categories present in PC centers participated proportionately. The field methodology used has generated a strong point in the study, – the high response rate (85.7%). The no-response rate was random, so it had no impact on the results. Likewise, the randomization procedure employed prevented self-selection bias. To conclude, the results of this study indicate that user violence, specifically non-physical violence, is related to certain sociodemographic and job characteristics of PC professionals. In this sense, the factors that contribute to the exposure to non-physical violence include being female, having less professional tenure, not receiving continued training, and belonging to the non-health professional category. This research intended to explore in more depth the relevance of certain variables for the psychological well-being of health care practitioners. There is evidence that user violence, job satisfaction, and professionals’ empathy influence their scores in psychological well-being, and these variables should be taken into account according to the professional PC category. References |
Cite this article as: López-García, C., Ruiz-Hernández, J. A., Llor-Zaragoza, L., Llor-Zaragoza, P., & Jiménez-Barbero, J. A. (2018). User violence and psychological well-being in primary health-care professionals. The European Journal of Psychology Applied to Legal Context, 10, 57-63. https://doi.org/10.5093/ejpalc2018a6
Correspondence: Jaruiz@um.es (José A. Ruiz-Hernández).
Copyright © 2024. Colegio Oficial de la Psicología de Madrid





 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
The European Journal of Psychology Applied to Legal Context is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License







