


Is the Self-reported Information by Male Sentenced of Violence against Women in the Intervention Phase Valid?
[¿Es válida la información reportada por sentenciados por maltrato contra la mujer en la fase de intervención?]
Ramón Arce1, Verónica Marcos1, Jéssica Sanmarco1, and Francisca Fariña2
1University of Santiago de Compostela, Spain; 2University of Vigo, Spain
https://doi.org/10.5093/apj2023a3
Received 30 May 2022, Accepted 13 October 2022
Abstract
The evaluation of the needs of convicts is a critical issue for the design of the intervention. Nonetheless, in the information reported by convicts in penitentiary evaluation, simulation (malingering) and dissimulation (denial of symptoms, social desirability, and both) must be suspected. Thus, a field study with the aim of estimating the prevalence rate of the distortions and its effects in the needs reported by convicts was designed. A total of 624 men convicted for intimate partner violence reported their needs in the MMPI-2 in the reception phase of a penitentiary intervention program. Results: tion consisting in denial of symptoms, .112 [.087, .137], social desirability, .223 [.190, .256], and the combination of both two, .120 [.095, .145]. The effects in denial of symptoms emerged in the information of less depressive (i.e., lack of interest in activities, excessive sensitivity, lack of sociability), paranoid (i.e., interpersonal sensitivity and perceptiveness), psychasthenic (i.e., general subjective distress and negative affect), schizoid (i.e., alienation, chaotic interpersonal relations, and disruptive cognitive processes), and hypomanic (i.e., hyperactivity, irritability, and sensation seeking) symptoms. Likewise, social desirability dissimulators detailed significantly less depressive, psychopathic (i.e., less general social maladjustment), paranoid, psychasthenic, schizoid, and hypomanic symptoms. Similarly, the whole dissimulators (combining denial of symptoms and social desirability responses) informed less depressive, psychopathic, paranoid, psychasthenic, schizoid, and hypomanic symptoms, and fewer problems of social introversion. Conversely, they related significantly more symptoms of hysteria (i.e., physical complaints). Distortions introduced by convicts in self-reports must be controlled to design effective correctional interventions.
Resumen
La evaluación de las necesidades de los sentenciados es clave para diseñar la intervención. No obstante, en la información facilitada por los sentenciados en proceso de evaluación penitenciaria ha de sospecharse simulación y disimulación (negación de síntomas, deseabilidad o ambas). Por ello, se diseñó un estudio de campo con el objetivo de estimar la tasa de prevalencia de distorsiones en las respuestas y sus efectos en las necesidades psicológicas informadas. Una muestra de 624 hombres sentenciados por violencia de género informaron de sus necesidades en el MMPI-2 en la fase de acogida de un programa de intervención penitenciario. Los resultados pusieron de manifiesto que las respuestas de los sentenciados eran coherentes y no estaban sujetas a simulación. No obstante, se observó una prevalencia significativa de disimulación consistente en negación de síntomas, .112 [.087, .137], deseabilidad social, .223 [.190, .256], y la combinación de ambas, .120 [.095, .145]. Los efectos de las distorsiones en la negación de síntomas se manifestaron en el informe de menos síntomas depresivos (i.e., ocultación de carencias en la sociabilidad), paranoides (i.e., ocultación de sensibilidad interpersonal), psicasténicos (i.e., ocultación de afecto negativo), esquizoides (i.e., ocultación de procesos cognitivos disruptivos) e hipomaníacos (i.e., ocultación de irritabilidad y búsqueda de sensaciones). Asimismo, los efectos de la deseabilidad se concretaron en el informe de menos de síntomas de depresión, psicopatía (i.e., menos inadaptación social), paranoia, psicastenia, esquizofrenia e hipomanía. Igualmente, los disimuladores que combinaron deseabilidad social y negación de síntomas manifestaron menos rasgos depresivos, psicopáticos, paranoides, psicasténicos e hipomaníacos, así como menos problemas de introversión social. Además, notificaron más histeria (i.e., quejas somáticas). Las distorsiones introducidas por los convictos en los auto-informes deben ser controladas para el diseño de intervenciones penitenciarias eficaces.
Palabras clave
Simulaci├│n, Maltratadores, Estilo de respuesta defensivo, Evaluaci├│n forense, Negaci├│n de s├şntomasKeywords
Malingering, Batterers, Defensiveness, Forensic evaluation, Denial of symptomsCite this article as: Arce, R., Marcos, V., Sanmarco, J., & Fariña, F. (2024). Is the Self-reported Information by Male Sentenced of Violence against Women in the Intervention Phase Valid?. Anuario de Psicolog├şa Jur├şdica, 34(1), 23 - 30. https://doi.org/10.5093/apj2023a3
Correspondence: ramon.arce@usc.es (R. Arce).In psychological evaluation, the clinician must suspect simulation1, understood as “the intentional production of false or grossly exaggerated physical or psychological symptoms, motivated by external incentives such as avoiding military duty, avoiding work, obtaining financial compensation, evading criminal prosecution, or obtaining drugs” (American Psychiatric Association [APA , 2013, p. 726]), when a combination of the following is noted: a) evaluations in medicolegal context; b) a marked discrepancy between the alteration manifested by the person and the objective data obtained from the clinical examination; c) lack of cooperation during the diagnostic evaluation and non-compliance with the prescribed treatment regimen; and d) the presence of antisocial personality disorder. Nevertheless, in the forensic setting, simulation must be suspected in any circumstance in which the evaluated person can obtain a benefit from presenting a psychological disorder, forcing a simulation differential diagnosis, such that if this cannot be ruled out the psychological evaluation is not valid as forensic evidence of charge (Arce, 2018) or in criminal insanity evaluations (Osuna et al., 2015). Additionally, in the forensic psychological evaluation not only should simulation be suspect, but, as the case may be, dissimulation2 and oversimulation3 (exaggeration of symptoms). Oversimulation is the exaggeration of a real psychological damage to obtain a benefit, generally economic, as in the case of compensation for the aftermath of a traffic accident. Meanwhile, dissimulation consists of reporting responses biased towards defensiveness. This includes the denial or concealment of symptoms – negative dissimulation – and the social desirability – positive dissimulation –, that is, the assumption of positive characteristics that are not present (fabricated) or the concealment of negative characteristics to convey a favorable image of oneself, being able to be conscious – impression management – or unconscious – self-deception – (Paulhus, 1984). Dissimulation must be suspected in the evaluation of populations in intervention for behavior problems or for violent behaviors (Molero et al., 2022; Nasaescu et al., 2020); of prison inmates (Arce et al., 2014; Martín et al., 2019; Redondo et al., 2022); in risk assessment (Jugl et al., 2021); and in the forensic evaluation of family courts (Arce et al., 2015; Baer & Miller, 2002). Overall, dissimulation is more difficult to classify correctly than simulation (Baer & Miller, 2002), because the task involves less cognitive activity of the individual and, consequently, less measure of the construct (validity) (Arce et al., 2015). These response biases, if they are systematic, constitute a serious measurement problem, since they support an interpretive hypothesis of the relationship between the variables that is different from the real one (Podsakoff et al., 2003). In sum, forensic evaluation requires a psychological diagnosis (variable according to judicial needs) and, at the same time, a differential diagnosis of distortion of responses (simulation, dissimulation and/or oversimulation). With this dual purpose, the traditional clinical evaluation is not valid, since it does not diagnose simulation (the diagnosis or suspicion of dissimulation and oversimulation do not exist in clinical setting; APA, 2013), due to the potentially devastating consequences of a false positive: deny a treatment to a sick person (it could lead to judicial responsibility), which may be a plea for help or of a phenomenological style to overreact and to be traumatized (Greene, 2011; Rogers, 2018). On the contrary, in the forensic psychological evaluation the undesirable outcome would be a false negative of simulation, dissimulation, or oversimulation. For the study and classification of response biases, both individual and population, a multi-method approach is required (Burchett & Bagby, 2014; Graham, 2011) comprising an interview, necessary for the forensic diagnosis and the establishment of causality (Arce, 2017), and a psychometric measure, with which to contrast –inter- measure consistency – the forensic diagnosis and the differential diagnosis of distortion of responses (Graham, 2011; Greene, 2011). The clinical-forensic interviews in use, i.e., the Structured Inventory of Reported Symptoms (SIRS; Rogers et al., 1992) and the Forensic-Clinical Interview (Vilariño et al., 2013), embrace measures of the distortion of the responses (i.e., detection strategies for simulation, dissimulation and oversimulation), but do not have sufficient validity (i.e., false positive diagnosis is no 0) for the differential diagnosis of simulation, dissimulation, or oversimulation in the forensic context. With this purpose, the psychometric evaluation is fundamental, being the MMPI-2 the reference instrument in forensic setting (Graham, 2011; Greene, 2011) and with superiority over its Restructured Form, the MMPI-2-RF (Fariña et al., 2017; Gancedo et al., 2020; Redondo et al., 2019; Rogers et al., 2003; Sharf et al., 2017). In this regard, the MMPI-2 has numerous scales (in the forensic context, not only the scales of the commercial version are taken, but also other additional ones) and indices that have been extensively studied, showing significant discriminative efficacy and a great magnitude in the classification of simulation and oversimulation (Gancedo et al., 2020; Rogers et al., 2003), as well as dissimulation (Baer & Miller, 2002; Fariña et al., 2017). The prodigality of scales and indices is necessary for two reasons. First, no scale or index by itself correctly classify the distortions of the responses, so the combination of scales and indices increase the validity of the approach to the control of false positives (forensic task; Fariña et al., 2014). Second, (over)simulation and dissimulation are not a unitary construct, but rather hide different strategies. Thus, (over)simulation can manifest itself in rare symptoms (Fp scale), quasi-rare (F and Fb scales), combination of symptoms (the family of F scales), severity of symptoms, or exaggeration of symptoms, i.e., overstimulation (the family of F scales). Hence, measures of all these strategies must be taken, combined in a measure of (over)simulation: infrequency (Gancedo, Sanmarco et al., 2021; Greene, 2011; Rogers, 2018; Vilariño et al., 2013). This (over)simulation measure is completed by the lack of consistency in the responses (APA, 2013), which are evaluated by the TRIN and VRIN scales, as well as the F-Fb index (Fariña et al., 2014; Greene, 2011). Conversely, dissimulation can manifest itself in denial or concealment of symptoms, which are evaluate by the K, L and S scales and the Gough index (Butcher & Han, 1995); and social desirability (only referring to the conscious impression management, since non-conscious self-deception is part of the personality of the evaluated person) measure by the L, MP, Od, and Wsd scales (Arce et al., 2015; Bagby & Marshall, 2004; Strong et al., 1999). Penitentiary intervention is aimed at addressing the criminogenic needs of inmates (i.e., inmate characteristics that contribute to the likelihood of recidivating) (Bonta & Andrews, 2017), such that if it is not adequately adjusted to the needs of each individual, it is not effective (Bonilla-Algobia & Rivas-Rivero, 2022; Moral-Jiménez & González-Sáez, 2020; Santirso et al., 2020) and can even be counterproductive (Arias et al., 2020). Hence, inmate needs are evaluated in the reception phase of the intervention with the aim of establishing the contents of the intervention programs based on the evaluation and adjusted to each case. This assessment relies almost exclusively on self-reports of moot reliability to prescribe treatment based on them. Thus, they are not consistent with other more reliable measures such as judicial or prison records (Expósito-Álvarez et al., 2021). In this state of the question, a field study with a sentenced population was designed to find out the rate of prevalence of distortions in the responses and their effects, where appropriate, on the reported psychological needs (Arce et al., 2014). Participants A total of 624 men between the ages of 18 and 78 (M = 41.87, SD = 12.12) serving a sentence of less than two years in prison, suspended by participation in a community penitentiary intervention program, participated in the study. All of them were gender-based primary offenders whose sentence was suspended by a voluntary participation in a community penitentiary program in application of L.O. 1/2004 (Ley Orgánica 1/2004, de 28 de diciembre, de Medidas de Protección Integral contra la Violencia de Género). The sentence suspension time was 5 years for 13 (2.1%), 4 years for 24 (3.8%), 3 years for 210 (33.7%), and 2 years for 377 (60.4%) of the batterers. Procedure and Design The sentenced persons were offered, under the protection of article 83 of L.O. 1/2015 (Ley Orgánica 1/2015 de 30 de marzo, por la que se modifica la Ley Orgánica 10/1995, de 23 de noviembre, del Código Penal), the suspension of the execution of the sentence in prison for participation in the Galician Re-Education Programme for Male Intimate-Partner Violence Offenders (Arce & Fariña, 2006, 2010). All participated voluntarily and signed the informed consent for the evaluation and intervention. In the reception phase, and after presenting the program and signed the acceptance form of participation, they were evaluated on the psychological adjustment. The order in which measures (i.e., assessment of psychological adjustment, risk assessment, assessment of cognitive skills, assessment of psychosocial skills) were administered to participants, was rotated, following a standard systematic rotation procedure (i.e., A, B, C, D, …...; B, C, D, …...; C, …...), in order to control the carry-over effect of the measurement variables in the subsequent ones (Arce et al., 2000). Measurement Variables Participants were administered the Spanish adaptation of the MMPI-2 (Butcher et al., 2019), the reference instrument for evaluation in forensic and penitentiary settings (Ackerman & Pritzl, 2011; Arce et al., 2015; Archer et al., 2006; Fariña et al., 2017; Graham, 2011; Greene, 2011; Redondo et al., 2019; Rogers et al., 2003). This instrument measures the psychological adjustment of the individual in 10 basic clinical scales: Hypochondriasis [Hs], Depression [D], Hysteria [Hy], Psychopathic Deviate [Pd], Paranoia [Pa], Psychasthenia [Pt], Schizophrenia [Sc], Hypomania [Ma], and Social Introversion [Si]. The Masculinity-Feminity scale was discarded since it did not measure psychological adjustment (Graham, 2011). This questionnaire includes also scales for the differential diagnosis of distortions in responses. With the measures and validity scales, 5 response manipulation profiles were constructed in which, due to the addition of various measures, the probability of a distortion of the responses is very high: inconsistent responses, infrequent responses (over-simulation), denial of symptoms (negative dissimulation), social desirability (positive dissimulation), and dissimulation (whole dissimulation: negative and positive dissimulation). The APA (2013) include as a criterion for the suspicion of simulation the lack of consistency in the responses (that is, in non-psychiatric populations it evaluates simulation). This is measured in the MMPI-2 (Greene, 2011) through the VRIN (variable response inconsistency) and TRIN (true response inconsistency) scales to which the |F-Fb| index has been added, which assesses the infrequency of symptoms in the first part of the instrument (up to item 370; included the basic clinical scales), and Fb which is the continuation of F in the second part (from item 370 onwards). As a criterion for the suspicion of a very high probability of inconsistency in the responses, two of these indicators (VRIN ≥ 9, TRIN ≥ 11; |F-Fb| > 11) have to classify the protocol as ‘inconsistent’ (Osuna et al., 2015). Simulation, which is measured through the infrequency of symptoms (Gancedo, Sanmarco et al., 2021; Greene, 2011; Rogers, 2018), that is, symptoms that rarely occurred in the general population, is evaluated with the scales F (Infrequency; items-symptoms-that are infrequently admitted by the normative population, < 10%), Fb (Back Infrequency scale; continuation of F on the back of the instrument); Fp (Uncommon psychopathology; items-symptoms-that are infrequently admitted by psychiatric inmates, < 20%), and the Gough index (i.e., F-K), being highly probable that the responses are distorted when two or more of the following criteria are met: F, Fb, Fp ≥ T66.45; and Gough index ≥ 30 (Arce et al., 2009; Rogers, 2018). Denial or concealment of symptoms (favorable report of psychopathology) is addressed with K (correction scale; people who create a favorable impression of themselves; denial of symptoms especially in somatization and histrionic disorders), L (lie; intent deliberate not to respond honestly and frankly, including denial of minor misconduct, honesty, aggressiveness, bad thoughts, and weakness of character), S (superlative; evaluates people who are superlative) scales and the Gough index (Butcher & Han, 1995). A protocol is classified as highly probable subject to denial of symptoms when two or more of the following criteria are met: K < 40, L ≥ 66.45, S ≥ 66.45, Gough index < -21 (Greene, 2011; Fariña et al., 2017). The social desirability in the responses (that was, the intentional handling of the responses in order to make a positive impression) is appreciated with the scales L, Mp (positive malingering; identifies self-favorable protocols of psychopathology), Od (other deception; update of Mp) and Wsd (Wigging’s social desirability scale; responses biased to appear socially desirable), and the classification as very highly probable impression management when two or more of the criteria are met: L, MP, Od, Wsd ≥ T66.45 (Arce et al., 2015). Data Analysis For the study of the prevalence rate of response distortion strategies, the observed probability was contrasted with a constant, a trivial probability (insignificant, .05; Fandiño et al., 2021), calculating the zeta score for the difference of the observed proportion with a constant. β was computed in order to know the power of the results, with 1-β being the probability associated with the correct refutation of the null hypothesis. The effect size was measured in odds ratio (OR) and the magnitude was quantified in terms of the effect incremental index (EII; Redondo et al., 2019) that estimates the increased probability over the constant due to the distortion strategy. As to compare the observed probabilities in the different strategies, 95% confidence intervals for the probabilities were computed: if confidence intervals overlap, the observed probabilities are equal, and if the confidence intervals do not overlap, the observed probabilities are significantly different (p < .05). A comparison of means with MANOVAs with the psychological adjustment measurement variables as dependent variables (r = .331, p < .001) and the group (distorted response pattern vs. undistorted response pattern) as a factor was applied. The analysis of variance is robust to the heterogeneity of variances when the groups are of equal size (i.e., Ngreater/Nlesser < 1.5), but when the assumption of homogeneity of variances is violated and the Ns are different, it could result in relevant deviations in the estimate of the associated probability (α) to F (Stevens, 1986). In multivariate F-test, the Pillai-Bartlett (V) trace is robust to the heterogeneity of variance (Olson, 1976), but in univariate F-tests, when the variability is greater in the larger group, F is conservative and vice versa. To address this contingency and have absolute certainty of the correct rejection of the null hypothesis, three safeguards were verified (Mayorga et al., 2020): a) that the theoretical F (Box’s conservative test, 3.841) was less than the empirical value of F; b) that the type II error – false acceptance of the null hypothesis – was greater than the type I error – false rejection of the null hypothesis – i.e., β/α > 1, being the result the number of times that the probability of a false negative than a false positive; and c) that the effect size, corrected for unequal Ns – the analysis of variance is robust to the heterogeneity of variance with equal Ns –, was > 0.20 (small). In all results with significant univariate F-tests (p < .05), these 3 requirements were met. The effect size for multivariate comparisons was estimated with η2p, interpreted in terms of the explained variance and quantified as the probability of superiority of the effect size (PSES; Gancedo, Fariña et al., 2021). For the difference of two means, a standardized mean difference, d, was calculated with the Hedges’ formula (when N1 ≠ N2), interpreting it in terms of the PSES. From d, the quantification of the increase (+) or decrease (-) in the distortions in the responses was estimated with an adaptation of the BESD (Rosenthal & Rubin, 1982), r (Gancedo, Fariña, et al., 2021). Finally, the error of the statistical model through the probability of an inferiority score (PIS; Fandiño et al., 2021) was calculated, which is an estimate of the probability that an individual in the group, in our case of distorted responses, obtained a lower score in the measurement variable than the mean of the group of non-distorted responses (that is, probability contrary to the classification of the statistical model). Ethical Issues The data were taken anonymized from the database of the Galician Re-Education Programme for Male Intimate-Partner Violence Offenders and were treated guaranteeing all the rights of convicted set forth in Penitentiary Spanish Law (Ley Orgánica 1/1979, de 26 de septiembre, General Penitenciaria) and according with the Spanish Data Protection Law (Ley Orgánica 3/2018, de 5 de diciembre, de Protección de Datos Personales y Garantía de los Derechos Digitales). Study of the Validity of the Protocols The protocols were scrutinized to identify whether they were subject to extreme acquiescence (TRIN T ≥ 80), a pattern of random responses (VRIN T ≥ 80; F, Fb or Fp T ≥ 120), or outliers (L rs > 12 or K rs > 29 i.e., 99.9 percentile), to eliminate them from the database (Fariña et al., 2014; Graham, 2011; Greene, 2011). Lack of collaboration (> 10 unanswered items or with double response; Graham, 2011) was also stated as a cause of invalidity of the protocols in forensic or prison evaluation. No protocol was removed for these reasons. Prevalence of Cases of Distorted Responses The results (see Table 1) showed a significantly negative rate (lower than normative, .05) of inconsistent responses among those convicted of intimate-partner violence, indicating that the responses of male convicted of intimate-partner violence were more consistent than the normative. Likewise, the response profiles of offenders were not uncommon, because the responses of these individuals do not include symptoms that rarely occur in the general (< 10%) or psychiatric (< 20%) population. In sum, in this evaluation context this population did not simulate or exaggerate psychopathology. On the contrary, the observed rates of denial of symptoms (negative dissimulation), social desirability (positive dissimulation), and whole dissimulation (combination or concealment of denial of symptoms and social desirability) have been registered significantly in this population, suggesting that the observed prevalence was not trivial. The magnitude of the effect of the distortions in the responses introduced by the subjects was moderate (OR ≈ 2.47) in whole dissimulation and denial of symptoms, and large (OR > 4.25) in social desirability, being the increase in the magnitude of the effect (EII) due to the conscious distortions in the responses of 55.4% in denial of symptoms, 58.3% in dissimulation, and 77.6% in social desirability. Comparatively, the prevalence of distorted responses in the direction of social desirability was significantly higher (the lower limit of the confidence interval for the observed prevalence is higher than the upper limit of denial of symptoms and dissimulation) than that of denial of symptoms and whole dissimulation. Table 1 Prevalence of Distorted Responses  Note. f(p) [95% CIp] = frequency(proportion) [95% confidence interval]; Z = zeta score for the comparison of the observed probability in the batterer population with a constant (.05; trivial effect); OR = odds ratio; 1EEI = effect incremental index. ***p < .001. As a consequence of these results, it was necessary to contrast what clinical symptoms they deny or conceal, and what positive characteristics report they did not present (social desirability), as well as to quantify the magnitude of the response distortions. Negative Dissimulation: Denial of Symptoms Knowing that prevalence rate of denial of symptoms was significant, the results showed that denial has significant effects on the self-reports of psychological adjustment, F(9, 605) = 8.39, p < .001, 1-β = 1.0, accounting for the 11.1% of the variance (η2p =.111), an effect size greater than 69.15% of all effect sizes (PSES = .6915). The univariate effects (see Table 2) exhibited that batterers classified as ‘denial of symptoms’ reported significantly less depressive (i.e., lack of interest in activities expressed as general apathy, physical symptoms such as sleep disturbances and gastrointestinal ailments, excessive sensitivity, and lack of sociability), paranoid (i.e., interpersonal sensitivity and perceptiveness), psychasthenic (i.e., general subjective distress and negative affect), schizoid – in non-psychiatric populations the Schizophrenia scale measures social alienation, not the positive symptoms of schizophrenia – (i.e., alienation, chaotic interpersonal relations, and disruptive cognitive processes), and hypomanic (i.e., hyperactivity, irritability, and sensation seeking) symptoms. They also warned of less social introversion (less personal discomfort in social situations, isolation, general maladjustment, and self-deprecation) than those in the non-denial of symptoms group. Finally, and contrary to the grouping criterion, the batterers in the denial of symptoms group reported significantly more symptoms of hysteria (i.e., complaints about muscular, gastrointestinal or cardiac problems, feelings of tension, anguish or fear). Nevertheless, this measure includes many items that imply a denial of problems in life or the absence of social anxiety (Greene, 2011) that, indeed, are related to denial of symptoms. Thus, the measure is reversed, and the results corroborated the validity of the inmate classification model. Table 2 Univariate Effects on the MMPI-2 Basic Clinical Scales for the Denial of Symptoms Desirability Factor. Between-subjects Effects 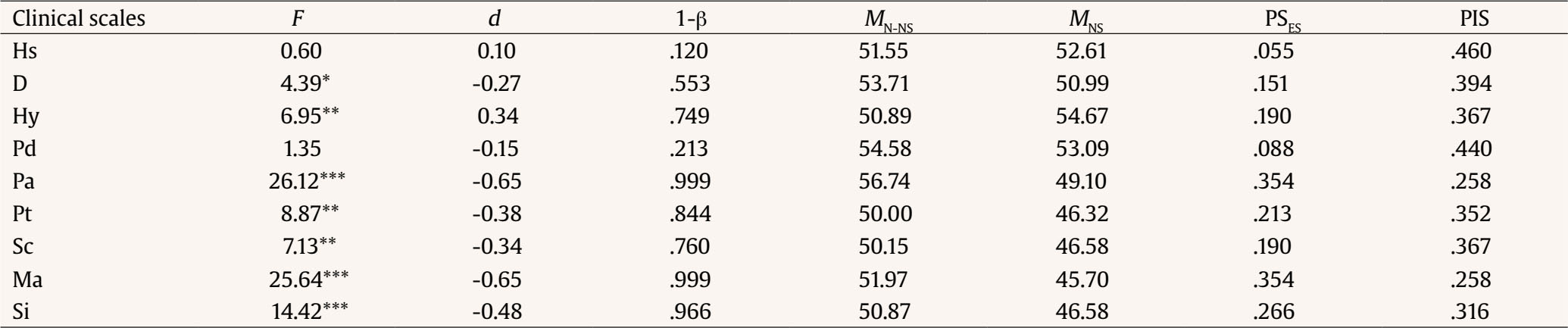 Note. df(1, 613); MN-NS = mean of the ‘not-denial of symptoms group’; MNS = mean of the ‘denial of symptoms group’. *p < .05, **p < .01, ***p < .001. Quantitatively, the batterers of the denial of symptoms group reported, on average, a 13.4% (r = -.134) fewer depressive symptoms; 30.9% (r = -.309) fewer paranoid symptoms; 18.7% (r = -.187) fewer symptoms of psychasthenia; 16.8% (r = -.168) fewer schizoid symptoms; 30.9% (r = -.309) fewer hypomanic symptoms; and 23.3% (r = -.233) fewer problems related to social introversion. Furthermore, the batterers of the denial of symptoms group assumed 16.8% (r = .168) more characteristics of hysteria (denial of problems in life or the absence of social anxiety). The magnitude of the effect (PSES) was greater (damage in mental health markers) than 15.1% of all possible in depression; than 19.0% in hysteria; than 35.4% in paranoia; than 21.3% in psychasthenia; than 19.0% in schizophrenia; than 35.4% in hypomania; and than 26.6% in social introversion. On the contrary, the probability (PIS) that the batterers of the denial of symptoms group obtained a score lower than the mean of the non-denial of symptoms group (error of the statistical model) was 39.4% in depression; 25.8% in paranoia; 35.2% in psychasthenia; 36.7% in schizophrenia; 25.8% in hypomania; and 31.6% in social introversion; while in hysteria, the probability that those in the non-denial of symptoms group had a lower score than those in the denial of symptoms group was of 36.7%. Positive Dissimulation: Social Desirability Based on previous findings supporting that the prevalence rate of social desirability in batterer responses was significant, the results displayed that the social desirability factor has significant effects on the self-reports of psychological adjustment, F(9, 612) = 10.88, p < .001, 1-β = 1.0, accounting for 13.8 % of the variance (η2p =.138), an effect size greater than 71.57% of all effect sizes (PSES = .7157). The univariate effects (see Table 3) revealed that batterers in the social desirability group reported significantly fewer depressive, psychopathic (i.e., general social maladjustment and absence of pleasant experiences), paranoid, psychasthenic, schizoid, and hypomanic symptoms. Table 3 Univariate Effects on the MMPI-2 Basic Clinical Scales for the Social Desirability factor. Between-subjects Effects 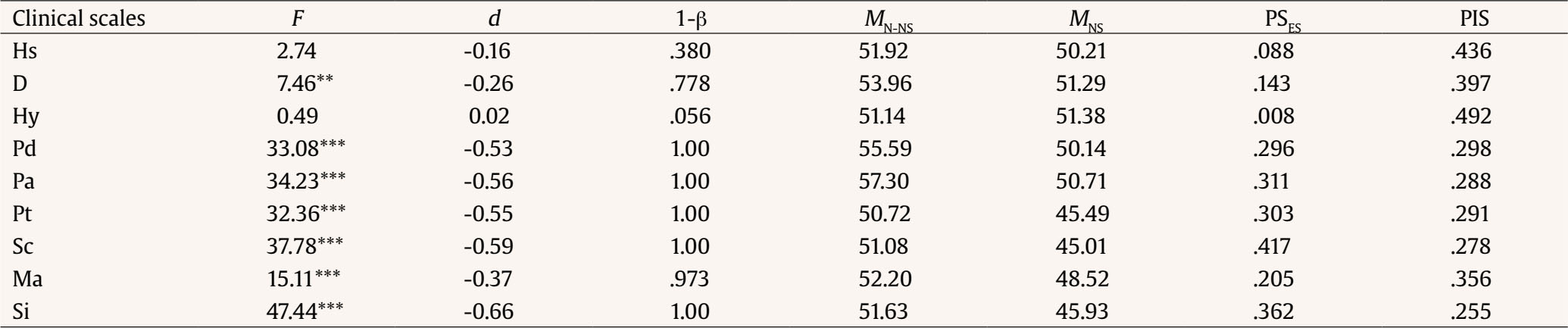 Note. df(1, 613); MN-DS = mean of the of ‘non-social desirability group’; MDS = mean of the ‘social desirability group’. **p < .01, ***p < .001. Similarly, they reported less social introversion than those of the group of non-social desirability. Quantitatively, the batterers of the group who distorted their answers in line with social desirability reported, on average, 12.9% (r = -.129) fewer depressive symptoms; 25.6% (r = -.256) fewer psychopathic characteristics; 27.0% (r = -.270) fewer paranoid symptoms; 26.5% (r = -.265) fewer psychasthenic symptoms; 28.3% (r = -.283) fewer schizoid symptoms; 18.2% (r = -.182) fewer hypomanic symptoms; and 31.3% (r = -.313) fewer problems related to social introversion than batterers of the non-social desirability group. The magnitude of the effect was greater (damage in mental health markers) than 14.3% of all possible in depression; than 29.6% in psychopathic deviation; than 31.1% in paranoia; than 30.3% in psychasthenia; than 41.7% in schizophrenia; than 20.5% in hypomania; and than 36.2% in social introversion. On the contrary, the probability (PIS) that the batterers in the social desirability group obtained a score lower than the mean of the social undesirability group (statistical model error) was 39.7% in depression; 29.8% in psychopathic deviation; 28.8% in paranoia; 29.1% in psychasthenia; 27.8% in schizophrenia; 35.6% in hypomania; and 25.5% in social introversion. Whole Dissimulation The results for the whole dissimulation factor (combination of denial or concealment of symptoms and social desirability) showed a significant effect on the self-reports of psychological adjustment, F(9, 614) = 9.92, p < .001, 1-β = 1.0, accounting for 12.7% of the variance (η2p =.127), an effect size greater than 70.54% of all effect sizes (PSES = .7054). The univariate effects (see Table 4) revealed that the batterers of the whole dissimulating group informed significantly fewer depressive, psychopathic, paranoid, psychasthenic, schizoid and hypomanic symptoms, and fewer problems of social introversion. In addition, they related significantly more symptoms of hysteria. Quantitatively, the batterers of the dissimulating group, on average, refer 14.0% (r = -.140) less of depressive symptoms; 17.2% (r = -.172); less of psychopathic characteristics; 30.5% (r = -.305) less of paranoid symptoms; 20.1% (r = -.201) less of symptoms of psychasthenia; 20.0% (r = -.200) less of schizoid symptoms; 31.3% (r = -.313) less of hypomanic symptoms; and 30.0% (r = -.300) less of problems related to social introversion. Additionally, the batterers of the group of dissimulating group assume 15.0% (r = .150) more characteristics of hysteria (denial of problems in life or the absence of social anxiety). The magnitude of the effect size was greater (i.e., damage in mental health markers) than 15.9% of all possible in depression; than 16.6% of all possible in hysteria; than 19.7% in psychopathic deviation; than 34.7% in paranoia; than 22.8% in psychasthenia; than 22.1% in schizophrenia; than 36.2% in hypomania; and than 34.7% in social introversion. On the contrary, the probability (PIS) that the batterers of the dissimulating group obtained a score higher than the mean of the non-dissimulating group (statistical model error) was of 39% in depression; of 36.3% in psychopathic deviation; 26.1% in paranoia; 34.1% in psychasthenia; 34.5% in schizophrenia; 25.5% in hypomania; and 26.4% in social introversion, while in hysteria the probability that those from the non-dissimulating group have a lower score under the mean of the dissimulators group was 38.2%. Table 4 Univariate Effects on the MMPI-2 Basic Clinical Scales for the Dissimulation Factor. Between-subjects Effects 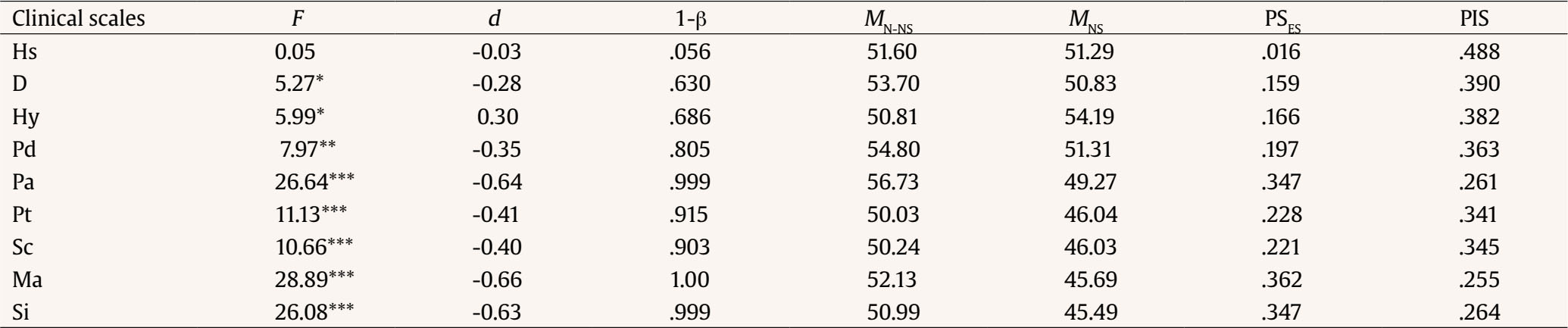 Note. df(1, 622); MN-D = mean of group of ‘non-dissimulators’; MD = mean of group of ‘whole dissimulators’. *p < .05, **p < .01, ***p < .001. The results of this research are subjected to limitations in their generalization. First, the evaluation was carried out in the reception phase in the penitentiary treatment, so its generalization to other moments of the process is not automatic. Thus, while it was expected that during the penitentiary intervention the response biases would be in the direction of dissimulation, motivated by obtaining penitentiary benefits or therapeutic success, during the judicial process a bias was expected in line with the simulation aimed at attenuation or exemption from criminal responsibility. Second, the results are not generalizable to other measurement instruments and subject classification criteria. Third, the magnitude of the effects cannot be generalized to other unmeasured criminogenic needs that may be the aim of penitentiary treatment. Having these limitations in mind, the following conclusions emerged from the results. First, the conscious distortions in the responses of those evaluated in penitentiary intervention are consistent, suggesting that batterers manipulate the responses in a stable way throughout the measure. Hence, the lack of consistency in the responses must be taken as a characteristic of the individual and not as a measure of deception (Osuna et al., 2015). Second, in the evaluation in the intervention phase, (over)simulation should not be systematically suspected (i.e., rare, quasi-rare symptoms, severity of symptoms, combination of symptoms, oversimulation; Rogers, 2018; Vilariño et al., 2013). Consequently, the information on deficiencies or needs must be taken, in general, as valid and, consequently, direct the intervention to them (Arce et al., 2014; Santirso et al., 2020). Third, in the evaluation of batterers in the intervention phase, dissimulation must be suspected, both referring to the denial or concealment of symptoms (non-criminogenic needs that are related to the criminal conduct but that are not the cause of it), as well as to social desirability (criminogenic needs, that are to say, causing the penalized conduct), or to a combination of both (whole dissimulation). Hence, the validity of the information self-reported by the batterers must be contrasted and complemented with other measures (Expósito-Álvarez et al., 2021). In sum, the validity of the measure is imperfect, understanding by imperfect validity that the results are not totally invalid, since not all subjects distort the responses (see the probability of cases contrary to the model; PIS). Fourth, manifested positive characteristics and unreported criminogenic needs (Bonta & Andrews, 2017) are those with the highest probability of bias being the self-report validity suspected. Failure to correct this bias will mean that the intervention does not focus on the needs of the individual and, henceforth, lost its effectiveness (Daffern et al., 2022). Fifth, there is also a systematic tendency to hide and deny clinical symptoms that, although they are not criminogenic needs (causal relationship with the criminal behavior), non-intervention on them is related to recidivism (Basanta et al., 2015). Sixth, the magnitude of the hidden or denied clinical symptoms, negative characteristics (e.g., denial of problems), and the invented positive characteristics range between approximately 1/5 and 1/3 of what is self-reported. In conclusion, the effects of distortions introduced by batterers in self-reports must be taken into account in the design of both effective correctional interventions and future research with offenders. Conflict of Interest The authors of this article declare no conflict of interest. Notes 1 This is the seminal scientific and judicial expression for intended fabrication of symptoms (Latin word with this significance) that was translated to English as malingering, feigning, feigning bad, faking, faking bad, overreporting, self-unfavorable reporting or even dissimulation. Some use them as synonymous, meanwhile others as a more specific definition of simulation (in any case, a simulation) and others as a non-intended (then it is not simulation). Thus, the correct and non-confusing expression for intended fabrication of symptoms is simulation. 2 The seminal scientific and judicial expression (Latin word antonymous of simulation meaning the concealment of symptoms or negative characteristics including the assumption of non-present property to hide its lack) for defensiveness, feigning good, faking good, underreporting, self-favorable reporting. 3 The seminal scientific and judicial expression (Latin word antonymous of simulation meaning the concealment of symptoms or negative characteristics including the assumption of non-present property to hide its lack) for defensiveness, feigning good, faking good, underreporting, self-favorable reporting. Funding: This research has been partially sponsored by a grant of the Consellería de Cultura, Educación e Ordenación Universitaria of the Xunta de Galicia (ED431B 2020/46), and by a grant of the Ministry of Science and Innovation of Spain (PID2020-115881RB-I00). Cite this article as: Arce, R., Marcos, V., Sanmarco, J., & Fariña, F. (2023). Is the self-reported information by male sentenced of violence against women in the intervention phase valid? Anuario de Psicología Jurídica, 34, 23-30. https://doi.org/10.5093/apj2023a3 References |
Cite this article as: Arce, R., Marcos, V., Sanmarco, J., & Fariña, F. (2024). Is the Self-reported Information by Male Sentenced of Violence against Women in the Intervention Phase Valid?. Anuario de Psicolog├şa Jur├şdica, 34(1), 23 - 30. https://doi.org/10.5093/apj2023a3
Correspondence: ramon.arce@usc.es (R. Arce).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






Herramientas:
 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Imprimir
Imprimir Enviar
EnviarALERTA POR E-MAIL
La Revista de Anuario de Psicología Jurídica está distribuida bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObra Derivada 4.0 Internacional.com








