


Implementation Factors that Predict Positive Outcomes in a Community-based Intervention Program for at-Risk Adolescents
[Factores de implementaciĂłn que predicen resultados positivos en un programa de intervenciĂłn comunitaria para adolescentes en situaciĂłn de riesgo psicosocial]
Chloe GarcĂa-Poole, Sonia Byrne, and MarĂa-JosĂ© Rodrigo
Universidad de La Laguna, Tenerife, Spain
https://doi.org/10.5093/pi2019a4
Received 17 August 2018, Accepted 19 January 2019
Abstract
This study examines the impact of the Building My Future program's implementation variables on attendance rate and on changes in personal, problem-solving, and community competencies. The program is run by local Social Services from Castile and Leon, Spain, and offers opportunities for adolescents to propose and carry out youth-led activities in their community. Data were accumulated from 356 participants, the majority experiencing negative psychosocial conditions, attending a total of 32 groups from 2013 to 2016. Using binary logistic regression and hierarchical linear regression analyses, results showed that having a facilitator with less professional experience, attending larger groups, having a high level of family involvement, and performing fewer modules and fewer extra activities predicted higher attendance rates and more positive task orientation, self-concept, social realization, and problem-solving competencies. Being younger, from an urban area, and having a facilitator with less professional experience predicted a higher score in community integration. These findings reveal that several program implementation components can contribute to the program's development and effectiveness and can also be considered across multiple programs in this field of practice.
Resumen
Este estudio examina la influencia de las variables de la aplicación del programa “Construyendo mi futuro” en el índice de asistencia y el cambio en competencias personales, de resolución de problemas y comunitarias. El programa se ofrece desde los Servicios Sociales de Castilla y León, España, brindando oportunidades para que adolescentes propongan y lleven a cabo actividades en su comunidad. Se recogieron datos de 356 participantes, la mayoría en situación de riesgo psicosocial, que asistieron a un total de 32 grupos desde el año 2013 hasta el año 2016. Mediante análisis de regresión logística binaria y regresión jerárquica lineal, los resultados indican que tener un facilitador con menos experiencia (más joven), asistir a grupos más grandes, disfrutar de un alto nivel de participación familiar y realizar menos módulos y menos actividades adicionales predecían un mayor índice de asistencia. Estas variables predijeron además una mayor orientación hacia la tarea y cambios positivos en autoconcepto, realización social y resolución de problemas. El hecho de ser joven, de zona urbana y tener un facilitador con menor experiencia profesional predecía una mayor puntuación en integración comunitaria. Estos resultados nos revelan cómo determinados componentes de la aplicación del programa pueden contribuir al desarrollo y a la eficacia del mismo, pudiendo igualmente ser considerados en otros muchos programas en este ámbito de intervención.
Keywords
Evidence-based community program, Adolescence, Implementation components, Attendance rate, Positive youth development.Palabras clave
Programa comunitario basado en evidencias, Adolescencia, Componentes de implementaciĂłn, ĂŤndice de asistencia, Desarrollo juvenil positivo.Cite this article as: GarcĂa-Poole, C. , Byrne, S. , & Rodrigo, M. (2019). Implementation Factors that Predict Positive Outcomes in a Community-based Intervention Program for at-Risk Adolescents. Psychosocial Intervention, 28, 57 - 65. https://doi.org/10.5093/pi2019a4
Correspondence: cgarciap@ull.edu.es (C. GarcĂa-Poole).Programs offered by community organizations (as well as school and family interventions) are especially needed to support adolescents in families experiencing negative psychosocial conditions, such as adolescents whose parents have low educational backgrounds, poverty, lack of social support, inter-parental violence, or substance abuse (Council of Europe. 2006). Adolescents living under these circumstances have been found to present lower levels of personal, social, and community competencies as well as poorer health-related lifestyles, poorer mental health, and more substance use and criminal behaviour compared to their peers (Aebi, Giger, Plattner, Metzke, & Steinhausen, 2014; García-Poole, Byrne, & Rodrigo, 2017; Lee & Vandell, 2015; Robinson et al., 2011; Rodrigo et al., 2006). Furthermore, cumulative adversity has also been found to affect the timing and sequence of adolescence to adulthood transition events (Lee, Wickrama, O'Neal, & Prado, 2017); therefore, it is important for adolescents facing difficult circumstances in a scenario of economic, family, school, or community risk factors to be offered additional support by social services in order to transition successfully into adulthood. Intervention programs for adolescents have usually aimed at reducing single problematic risk-taking behaviours such as alcohol and drug use, aggression, or sexual risk (Catalano, Hawkins, Berglund, Pollard, & Arthur, 2002; Hale, Fitzgerald-Yau, & Viner, 2014). Over the last two decades, there has been an increasing use of evidence-based intervention programs, based on the Positive Youth Development framework, aimed at strengthening competencies for better adjustment results and more sustained improvements in problematic areas in children and adolescents (Eichasa, Kurtines, Rinaldi, & Farr, 2018; Lerner et al., 2013; Lerner, 2004; Lerner & Lerner, 2006; Roth & Brooks-Gunn, 2016; Vandell, Larson, Mahoney, & Watts, 2015). The Positive Youth Development framework is informed by developmental theories of resilience, plasticity, and competency building, replacing the deficit view of adolescents as ‘problems to be managed' for a more positive view of adolescents as ‘resources to be developed' (Lerner et al., 2013; Roth & Brooks-Gunn, 2003; Schwartz, Chan, Rhodes, & Scales, 2013). This perspective recognizes that preventing problem behaviours is not all that is needed to prepare youth for their future, and that adolescents must be provided with opportunities for positive growth. These opportunities include caring and supporting relationships with adults, challenging experiences, skill-building activities, social bonding and engagement, prosocial standards, and positive behaviour acknowledgment (Ince, Yperen, & Valkestijn, 2014; Zarrett & Lerner, 2008). With the rise of the Positive Youth Development framework, risk avoidance and competency promotion views of development are being better understood as coexisting ideas (Catalano et al., 2004, 2002; Ciocanel, Power, Eriksen, & Gillings, 2017; Dixon, Schoonmaker, & Philliber, 2000; Gavin, Catalano, David-Ferdon, Gloppen, & Markham, 2010; Hale et al., 2014; Morgan & Ziglio, 2007; Schwartz, Pantin, Coatsworth, & Szapocznik, 2007). Schools are increasingly offering a variety of activities aiming to increase personal and social competences as well as preventing undesired behaviours. However, programs offered in formal settings during school or after school hours often fail to engage adolescents who are already experiencing school failure, dropout, or have started showing delinquent behaviour (Kremer, Maynard, Polanin, Vaughn, & Sarteschi, 2015). It is also more difficult to reach older youth with after-school programs as they tend to be drawn to more independent and unsupervised activities (Badura et al., 2018; Mahoney, Vandell, Simpkins, & Zarret, 2009; Sipe, Ma, & Gambone, 1998). Therefore, programs that are embedded in the neighbourhood or community (e.g., at recreational centres or local youth spots) may have better chances to reach at-risk adolescents and provide them with an array of activities that suit them better (Ince et al., 2014; Ungar, 2011). However, for many community-based organizations, adopting the perspective of working on a variety of key developmental competencies still remains a challenge (Sardiñas et al., 2017). Community services can play an important role giving opportunities to increase positive development and reduce adolescent risk, as the activities that take place in a community provide a unique normative system, expectations, goals, and relationships with adults and peers (Cicognani, Albanesi, & Zani, 2008; Eccles & Gootman, 2002; Flanagan, Kim, Collura, & Kopish, 2015; Rogoff, Baker-Sennett, Lacasa, & Goldsmith, 1995). The Building My Future program (in Spanish Construyendo mi futuro; Rodrigo et al., 2006), is a psycho-educational and community-based intervention program that aims to promote personal, social, and community competencies in adolescents. Throughout its modules, the ‘big three' effective features of positive development promotion are present: 1) positive and sustained adult-youth relationships, 2) activities that build important life skills (e.g., decision making and time management during a volunteering action), and 3) opportunities for participation and leadership in valued community activities, for example, planning and serving as the leader in a volunteering action (Lerner, 2004). During the program, adolescents propose activities following a youth-led approach, allowing them to display multiple assets, make decisions, and achieve their project goals. Facilitators help to put into action the chosen activities by facilitating contact with community resources, as well as emphasizing the planning of each action, the selection of strategies, and the reflection on the achievements made. The program is structured yet flexible, open to taking on different types of activities proposed and arranged by the group of participants (e.g., nature excursions, city walks, handicraft work, or collaborations with mental health associations). These action projects are embedded in the work sessions of five modules: 1) ‘Creating our group', 2) ‘Getting to know our surroundings', 3) ‘Making our surroundings better', 4) ‘Clarifying my future', and 5) ‘Boosting our relationships'. Following the Positive Youth Development framework and the Council of Europe's Recommendation, the program is being widely implemented in the local social services of the Spanish Autonomous Region of Castile and Leon, in coordination with the region's community resources, as part of the family preservation services targeting families with psychosocial risk. The enrolment strategy consists of offering a pre-intervention fun and appealing leisure activity which aims to hook up and motivate participants to attend to the following sessions of the program. This pre-intervention activity is advertised through different community resources (web pages, schools, town hall centres, etc.), enabling non-at-risk adolescents to participate as well. The selection of the pre-intervention activity considers the context and interests of the potential participants, examples being an adventure camp or music encounter. The program is offered during the academic year (from October to June), with adolescents generally attending the group activities at least once a week. A previous evaluation study of the types of activities performed during the program has found that performing group dynamics as a pre ‐intervention activity, carrying out creative activities, volunteering, excursions, and games, but no sports, and meeting up with associations were related to the most positive competence changes in at ‐risk groups, whereas non ‐at ‐risk groups that mainly participated in amusing activities experienced a decrease in their competence scores (García-Poole, Byrne, & Rodrigo, 2018). As found in a recent review, many studies have found positive outcomes of intervention programs on adolescents' developmental assets (Roth & Brooks-Gunn, 2016). However, less is known about the conditions that assure the correct implementation of group-based community programs, leaving practice fields with ‘the paradox of non-evidence-based implementation of evidence-based programs' (Drake, Gorman, & Torrey, 2002, cited in Fixsen, Naoom, Blase, Friedman, & Wallace, 2005, p. 35). Evaluating the quality of implementation is critical to understand which factors make a program work when applied in real-life conditions (Durlak & DuPre, 2008; Ibrahim & Sidani, 2015). Within the field of social work, the shift toward the use of evidence-based community practices is a relatively recent phenomenon (Santiago, Soska, & Gutierrez, 2017), and therefore the evaluation work involving testing for implementation factors is even less frequent. The present study tries to fill this gap by analysing several implementation factors (facilitator and group characteristics, family involvement, and adherence to the program's curriculum) and their contribution to multiple program outcomes (attendance rate and personal, social, and community competences), since most studies have focused on single implementation components and single outcomes (Carroll et al., 2007; Durlak & DuPre, 2008; Kutash, Cross, Madias, Duchnowski, & Green, 2012). We have selected different implementation and outcome components that are relevant for group-based interventions, following Berkel, Mauricio, Schoenfelder, and Sandler's (2011) comprehensive model, which distinguishes between facilitator (e.g., professional experience) and participant behaviors (e.g., attendance) during the implementation of preventive programs and suggests that different dimensions of implementation can jointly influence program outcomes. The implementation dimensions analysed in this study have also been highlighted when evaluating group-based interventions with families at psychosocial risk (Rodrigo, 2016), such as group characteristics (size and composition); the facilitator's professional experience, which may affect the skill with which material is delivered and the interaction with participants; the level of family involvement in the program, which may suggest a positive program-parent-child relationship with family support and quality involvement from the facilitator; and the level of adherence to the program's curriculum: dosage, and engagement in extra activities that were not included in the program's design. We are aware that the list of implementation components is not exhaustive, though we believe that they are relevant across multiple programs and may be helpful for practitioners working in the field of community practice with adolescents (social services, juvenile points, associations, etc). Two research questions were addressed in this study. First, we aimed to examine which implementation components best predict the attendance rate of the Building My Future program. We selected attendance rate as our focus outcome, and not as a predictor, aiming to discover implementation components that could be increasing participation, as drop-out rates are usually high in at-risk families (Baker, Arnold, & Meagher, 2011). Second, we wished to examine which of the implementation components predict positive outcomes in the adolescents' competencies after participation in the program. We examined personal competencies, coping strategies, and community competencies. We expected that the implementation factors under control of the facilitator would have a stronger effect than individual sociodemographic variables when predicting attendance and positive competence outcomes (Álvarez, Rodrigo, & Byrne, 2016; Gagnon et al., 2015). Establishing which components predict attendance and competence changes in this community-based intervention can add knowledge and improve the quality of implementation among practitioners working with adolescent groups in the community. Participants and Procedure Primary caregivers of all participants gave informed consent and the procedures were approved by the Committee for Research Ethics and Animal Welfare at the University of La Laguna. Participants were 356 adolescents (55% girls) who attended the Building My Future program in 18 local social services of the Autonomous Region of Castile and Leon, Spain. Each participant only attended one edition (year) of the program. Data was accumulated from three separate editions of the program, from 2013 to 2016. Participants came from urban areas (53%) and rural areas (47%), with an average age of 14.6 (SD = 1.6) and a range from 11 to 18 years of age. A total of 32 groups were included: six groups with no psychosocial risk (n = 68) and 26 mixed groups with and without psychosocial risk (n = 288). Adolescents with psychosocial risk were referred to the program by social service workers as part of the family's case plan, whereas the rest of participants were invited to participate on a more voluntary basis (through advertising, civic centers, and friends). The flow of participants through the stages of this study is depicted in Figure 1, and the sociodemographic and implementation characteristics of the sample can be seen in Table 1. Figure 1 Flowchart of Participants. 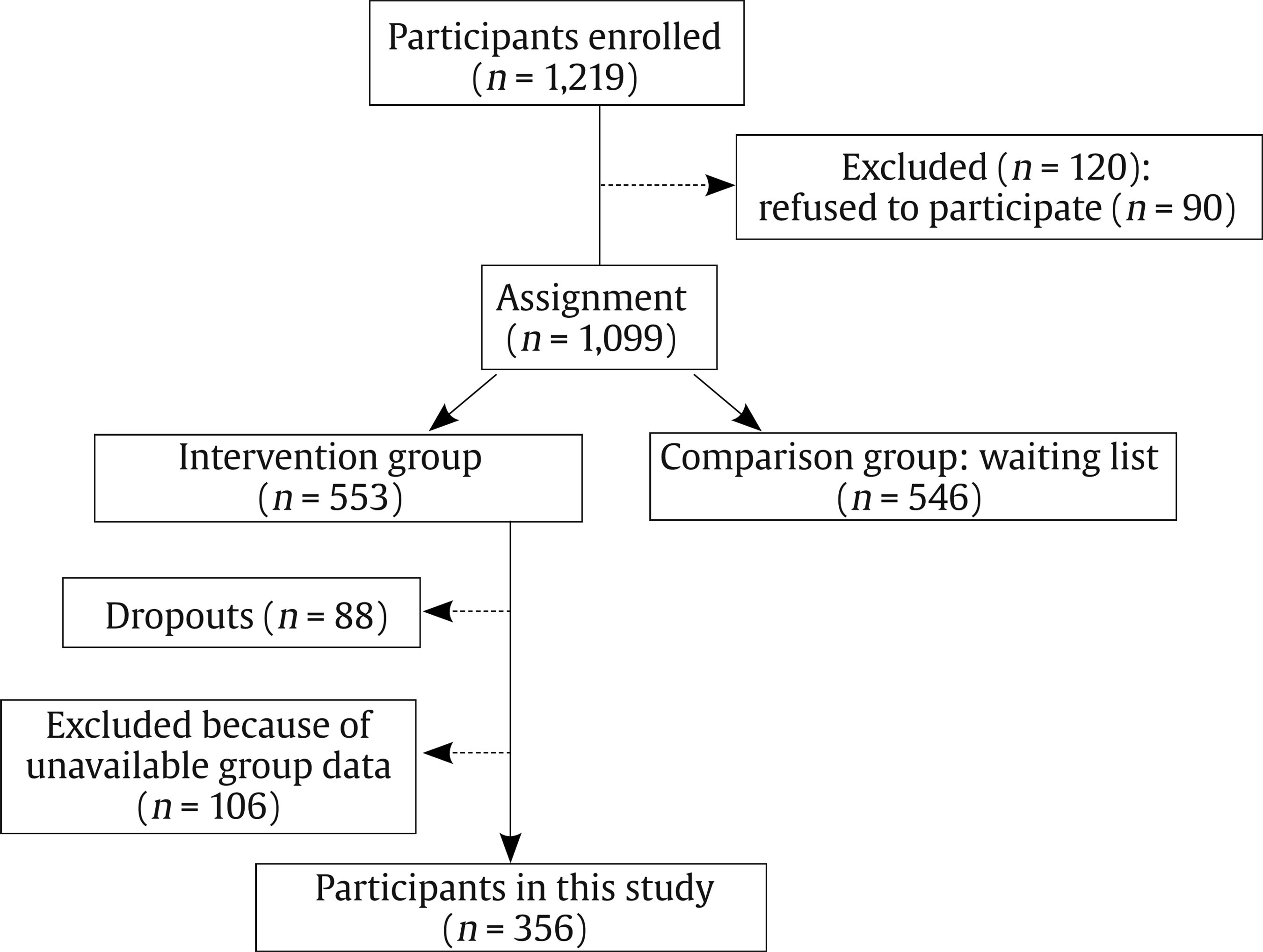 Table 1 Descriptive Data of Participants' Sociodemographic and Implementation Variables  The Building My Future team of experts provided an intensive 25-hour training program for the group facilitators (social educators and social workers) in the capital of the Autonomous Region of Castile and Leon. This training program covered the core principles, methods, and evaluation of the program, as well as guidance on how to implement it successfully. Once the program had started (after the pre-intervention enrolment activity), two warm-up sessions were necessary to create a group feeling and to establish the group roles. Part of the first session was also used for participants to complete the pre-test questionnaires. The post-test questionnaires were completed during the last session, within a week of the program completion. Each set of questionnaires together with the group implementation datasheets were sent by the program coordinators to the university team, where all material was collected, organized, and entered into a database to be analysed. Measures and Instruments Personal information datasheet. Each adolescent participating in the program filled out a personal information datasheet during the first session of the program, which gathered the following sociodemographic variables: sex (0 = girl, 1 = boy), age, and residential area (0 = rural, 1 = urban). Facilitator's datasheet. The facilitator of each group filled out a datasheet with information related to the following implementation components: group size (number of participants); group risk status (participants' psychosocial risk status was identified and labelled by the social service workers using a normalized measure of negative psychosocial conditions such as parental violence, substance use, poverty or lack of access to resources, and then the group was identified according to its participants statuses as 0 = without risk, 1 = mixed: with and without risk); group nationality (0 = only Spanish, 1 = mixed nationalities); facilitator's years of professional experience working with adolescents; family involvement in the group (the level of family involvement during the program was informed by the facilitator with an open response and responses were categorized by consensus as: 0 = none/low involvement – e.g., ‘families were not involved during the program' –, 1 = medium involvement – e.g., ‘families were contacted by phone and informed about the activities' -, and 2 = high involvement – e.g., ‘families took part in program activities'); number of modules (1-5); and number of extra activities. A total of 32 datasheets were analysed, and this group data was assigned to each individual member of the corresponding group. The variables mentioned above in the adolescents' personal information datasheet and the facilitator's datasheet were used as predictors of the following outcome measures: Group attendance rate. The facilitator of each group also included in the facilitator's datasheet the number of adolescents who started the program and the number of adolescents who did not finish the intervention. The attendance rate was calculated as the percentage of adolescents in each group that completed the intervention (total number of participants attending at the start minus those who did not finish the intervention), independently from the number of modules and activities that were carried out, as some facilitators chose to implement the program partially. The group attendance rate (in percentage) was then assigned to the participants of each corresponding group. To proceed with the binary logistic regression analyses, group attendance was divided into two categories. As the average percentage of group attendance was 80%, participants in groups with 80% attendance or higher were classified as high group attendance, and participants in groups with lower than 80% of attendance were classified as low group attendance. Self-concept and social realization questionnaire. We used the Self-Concept and Social Realization Questionnaire (in Spanish AURE; De Mendoza, Medina, & Hernández, 2005), originally validated with Spanish adolescents (α = .91). The instrument has a total of 42 items, comprising three factors: 1) self-concept (16 items, α = .89, ω = .90, GLB = .93 in this study), as the positive evaluation of one's personal qualities; 2) task-oriented strategy (13 items, α = .89, ω = .88, GLB = .92 in this study), which includes the need to be efficient and to enjoy facing the challenges that one is involved in while performing tasks; and 3) empathy and social realization (10 items, α = .84, ω = .85, GLB = .90 in this study), which involves the capacity to enjoy caring relationships and concern about other people's problems. Each item is presented using Osgood's semantic differential scale (Osgood, Suci, & Tannenbaum, 1957) where two statements are opposed and must be rated (e.g., “I feel good about myself”, 1 2 3 4 5, “I feel uncomfortable with myself”). Scores nearer to 1 represent higher levels of competence, so all scores in this instrument were inverted for easier understanding. Coping scale for children and youth. A reduced version of the Coping Scale for Children and Youth (CSCY; Brodzinsky et al., 1992) was used, originally validated in the USA (α = .80 for assistance seeking, α = .80 for cognitive-behavioural problem solving, α = .81 for cognitive avoidance, and α = .73 for behavioural avoidance). The instrument has a total of 29 items, with responses rated on a five-point scale going from 1, never, to 5, always. Before rating these items, adolescents were asked to describe a recent specific problem and to bear it in mind while answering the rest of the questionnaire. This instrument includes four different factors: 1) assistance seeking (4 items, α = .60, ω = .63, GLB = .67 in this study), which involves interpersonal problem solving, such as getting advice or sharing feelings with another person such as a family member or a friend; 2) cognitive behavioural problem solving (8 items, α = .76, ω = .76, GLB = .81 in this study), such as making plans to solve problems and then following them; 3) cognitive avoidance (11 items, α = .83, ω = .83, GLB = .84 in this study), involving putting the problem out of one's mind; and 4) behavioural avoidance (6 items, α = .66, ω = .66, GLB = .73 in this study), consisting of reducing tension by indirect means such as avoiding people that remind you of the problem. Perceived community support questionnaire. We applied the Community Participation and Community Integration subscales of the Perceived Community Support Questionnaire (PCSQ; Gracia, Herrero, & Musitu, 2002), originally validated with Spanish population (α = .75 for community integration, and α = .85 for community participation). We used a total of 11 items with responses rated on a five-point scale going from 1, strongly disagree, to 5, totally agree. The two factors of community support measured were: 1) community integration (5 items, α = .67, ω = .67, GLB = .67 in this study), measuring the sense of belonging to a community or neighbourhood; and 2) community participation (6 items, α = .73, ω = .75, GLB = .81 in this study), measuring the level of involvement in the community's social activities. Data Analysis To examine which implementation components best predict the group attendance rate, a binary logistic regression analysis was run. In Step 1, we introduced the adolescents' sociodemographic variables: sex, age, and residential area. In Step 2 we included group and facilitator variables: group size, group psychosocial risk-status, group nationality, and the facilitator's years of experience. In Step 3 we included the remaining implementation variables: family involvement level, number of modules carried out, and number of extra activities performed. To interpret the global significance of the model, at each step we examined the F statistic, the values for the adjusted R2 (AdjR2), and the change in R (ΔR2), as well as the specific contribution of each variable to the total variance explained by the model through the odds ratio (OR), and the regression coefficient (B). Second, to examine which of the implementation components predict positive outcomes in the adolescents' competencies after participating in the program, hierarchical linear regression analyses were run separately for each of the post-test competence scores: self-concept, task-oriented strategy, empathy and social realization, assistance seeking, problem solving, cognitive avoidance, behavioural avoidance, community participation, and community integration. To help with the interpretation, the predictor variables included in the regression model were standardized (Tabachnick & Fidell, 2007). In each regression model, we included the pre-test centered competence scores as a predictor at Step 1, to control for the initial level of competence and find out what the remaining predictors were adding to the explanation of the post-test variance. The pre-test centred competence scores were calculated by subtracting the average of the participant's pre-test scores from each of the participant's pre-test scores, helping us to interpret the direction of gain between the pre-test and post-test scores when looking at beta values. The hierarchical regression models were carried out using a stepwise forward procedure. In Step 1 we included the pre-test centred scores, and in the following three steps we included the remaining implementation variables as mentioned previously for the attendance rate. To interpret the global significance of the model, at each step we examined the F statistic, the values for the adjusted R2 (AdjR2), and the change in R (ΔR2), as well as the specific contribution of each variable to the total variance explained by the model through the significance and the value of the squared semi-partial correlation (rs2). All analyses were conducted using SPSS 21 statistical software, assuming a confidence level of 95% for Type I error. Components Predicting Group Attendance Table 2 Binary Logistic Regression Analysis of Sociodemographic and Implementation Variables on Group Attendance Rate (N = 356) 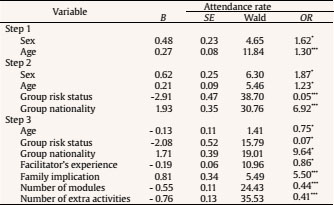 Table 2 represents a summary of the binary logistic regression analysis of the sociodemographic and implementation variables on group attendance. The model was significant in all three steps: Step 1, c2(3) = 24.14, p ≤ .001; Step 2, c2(4) = 65.22, p ≤ .001; and Step 3, c2(3) = 102.14, p ≤ .001, explaining 56% of the variance. Transforming the odds ratios into percentages to intuitively interpret the results, (OR – 1)* 100, at Step 3, groups with mixed nationalities were found to have 864% higher odds of having high group attendance than those with only Spanish members (OR = 9.64) and groups with greater family involvement were found to have 450% higher odds of having high group attendance than groups with low family involvement (OR = 5.50). On the other hand, each additional year of age in the participants reduced by 25% the odds of having high group attendance (OR = .75); groups with mixed psychosocial risk had 93% lower odds of having high group attendance compared to non-at-risk groups (OR = .07); each additional year of facilitator experience reduced the odds of having high group attendance by 14% (OR = .86); and each additional module and each additional activity reduced the odds of having high group attendance by 56% (OR = .44) and 59% (OR = .41), respectively. Components Predicting Post-test Competencies Results of the hierarchical regression analysis on the predictive capacity of the sociodemographic and implementation factors on post-test personal competencies can be seen in Table 3. The regression model for self-concept was significant in all four steps, explaining 52% of the variance in Step 4, F(11, 344) = 10.76, p ≤ .001. After controlling for the pre-test performance (38% of the variance), a significant increase in the variance was found in Step 2 and in Step 3. Being a boy (rs2 = .15) and having a facilitator with fewer years of experience (rs2 = -.19) significantly contributed to predicting a higher score in self-concept at the post-test. Table 3 Regression Models Controlling Pre-test Competence Measures of Sociodemographic and Implementation Variables on Adolescents’ Post-test Personal Competences (N = 356) 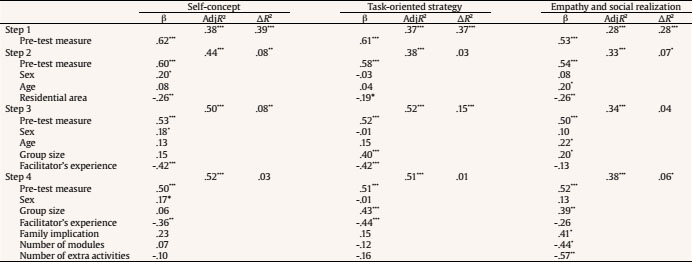 The regression model for task-oriented strategy was significant in all four steps, explaining 52% of the variance in Step 3, F(8, 347) = 13.53, p ≤ .001. After controlling for the pre-test performance (37% of the variance), a significant increase was found in Step 3. Being in a larger group (rs2 =.35) and having a facilitator with fewer years of experience (rs2 = -.26) significantly contributed to predicting a higher score in task-oriented strategy at the post-test. The regression model for empathy and social realization was significant in all four steps, explaining 38% of the variance in Step 4, F(11, 344) = 6.64, p ≤ .001. After controlling for the pre-test performance (28% of the variance), a significant increase was found in Step 2 and in Step 4. Being in a larger group (rs2 = .22), with a high level of family involvement during the program (rs2 = -.20), and performing fewer modules (rs2 = .17) and fewer extra activities (rs2 = .23) predicted a higher score in empathy and social realization at the post-test. Results of the hierarchical regression analysis on the predictive capacity of the sociodemographic and implementation factors on post-test problem-solving competencies can be seen in Table 4. The regression model for assistance seeking was significant in all four steps, explaining 41% of the variance in Step 4, F(11, 344) = 7.12, p ≤ .001. After controlling for the pre-test performance, that in Step 1 explained 35% of the variance, no significant increases were found in Step 2, 3 or 4, yet Step 4 explained the highest percentage of the variance. Being in a larger group (rs2 = .19) and performing fewer modules (rs2 = -.16) and fewer extra activities (rs2 = -.19) significantly contributed to predicting a higher score in assistance seeking at the post-test. Table 4 Regression Models Controlling Pre-test Competence Measures of Sociodemographic and Implementation Variables on Adolescents’ Post-test Problem-solving Competences (N = 356) 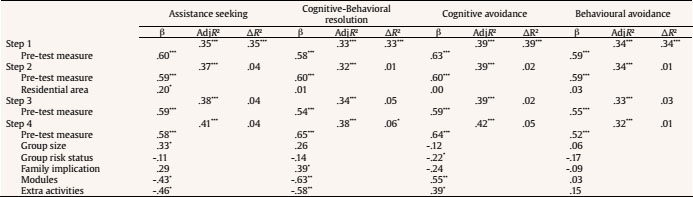 The regression model for cognitive-behavioural problem solving was significant in all four steps, explaining 38% of the variance in Step 4, F(11, 344) = 6.49, p ≤ .001. The pre-test performance on its own explained 33% of the variance, and a significant increase was found in Step 4. Having a higher level of family involvement (rs2 = .18) and performing fewer modules (rs2 = -.23) and fewer extra activities (rs2 = -.22) significantly contributed to predicting a higher score in cognitive-behavioural problem solving at the post-test. The regression model for cognitive avoidance was significant in all four steps, explaining 42% of the variance in Step 4, F(11, 344) = 7.55, p ≤ .001. After controlling for the pre-test performance in Step 1, explaining 33% of the variance, no significant increases were found in Step 2, 3 or 4. Being in a mixed risk group (rs2 = -.16) predicted a lower score in Cognitive Avoidance, whilst performing more modules (rs2 = .21) and more extra activities (rs2 = .16) predicted higher scores in Cognitive Avoidance at the post-test. The regression model for behavioural avoidance was significant in all four steps, with Step 1 explaining 34% of the variance, F(1, 354) = 65.85, p ≤ .001. Only the pre-test measure was a significant predictor for post-test behavioural avoidance (rs2 = .59). Results of the hierarchical regression analysis on the predictive capacity of sociodemographic and implementation variables on participant's community competencies can be seen in Table 5. The regression model for community participation was significant in all four steps, yet only the pre-test performance was a significant predictor of the post-test score, explaining 21% of the variance, F(1, 354) = 27.72, p ≤ .001. Table 5 Regression Models Controlling Pre-test Competence Measures of Sociodemographic and Implementation Variables on Adolescents’ Post-test Community Competences (N = 356) 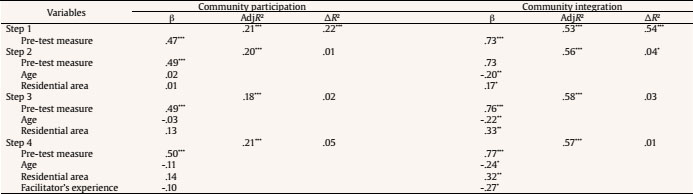 The regression model for community integration was significant in all four steps, explaining the highest percentage of the variance (58%) in Step 3, F(8, 347) = 17.89, p ≤ .001. The pre-test performance on its own explained 53% of the variance, yet a significant increase was found in Step 2 and in Step 3. Being younger (rs2 = -.16), from an urban area (rs2 = .18), and having a facilitator with fewer years of experience (rs2 = -.14) predicted a higher score in post-test community integration. The present study evaluates the impact of implementation components on program outcomes such as attendance rate and changes to personal, problem-solving, and community competencies. Results showed a substantial variability in the attendance rate and in the patterns of change in adolescent competencies that were partially explained by several implementation components reported by the facilitators. As expected, higher rates of attendance were predicted by participants' younger ages and less psychosocial risk. While younger adolescents' daily activities can still be strongly supervised by their families, older adolescents seek more independence, which may be causing their lower attendance (Furstenberg, Cook, Eccles, Elder, & Sameroff, 1999; Zimmer-Gembeck & Collins, 2006). At-risk adolescents are also known to attend organized activities such as theatre, music, or sports clubs less frequently (Theokas & Bloch, 2006), therefore more of an effort needs to be made in order to engage them into the program, even when involving a flexible curriculum. Other implementation components such as forming groups with mixed nationalities conducted by young facilitators, involving families in the program, and carrying out one to two modules without any extra activities contributed to the higher rates of attendance. Extra activities were not included in the program's design and may be increasing its length, thus impacting on the rate of attendance. In turn, mixing nationalities may be making the program more appealing to adolescents, as during this developmental period adolescents are in search of new experiences and may be attracted by the idea of meeting peers from different cultures (Arasaratnam, Banerjee, & Dembek, 2010). What is more, mixing nationalities can be empowering for Spanish adolescents as they help others integrate into their culture, while the program may also help foreign adolescents settle better into the community while making new friends. We recommend for these controllable implementation components to be especially taken into account in order to promote attendance in future editions, especially with older participants and adolescents with psychosocial risk. The facilitator's lower experience, which is related to being younger, was one of the implementation components that predicted the highest number of positive competence outcomes: self-concept, task-oriented strategy, and community integration. Younger facilitators are closer to the participants' ages, are more personally available, and are more likely to serve as positive role models for the adolescents. When aiming to improve adolescents' task orientation, and empathy and social realization, the size of the group is important. Larger groups are more effective at task orientation since participants were encouraged to take on planned community actions and had to distribute the plan into individual or subgroup tasks to achieve their project goal. It could be that larger groups were able to distribute the main action into smaller units, and that each adolescent found it easier to concentrate and accomplish their individual and/or subgroup tasks. Large groups were also more effective at improving participants' empathy and social realization. This may be due to adolescents exchanging more experiences and getting to know a greater variety of people in these groups (Alvarez, Rodrigo, & Byrne, 2016). Having a shorter program with high family involvement is also key when working on adolescents' empathy and social realization (Duerden, Witt, & Harrist, 2013), as adolescents must see that there is coherence between what the community is offering (the program) and what their families approve of. Large groups are also positive when working on problem-solving strategies to promote assistance seeking. It could be that in larger groups adolescents have more peers to choose from to share their problems and ask for help. High family involvement during the program also promotes cognitive and behavioural problem solving, whilst shortening the program and not overloading the adolescents with extra activities can be beneficial for both of these problem-solving strategies. Adolescents in mixed-risk groups predicted low post-test cognitive avoidance, a positive outcome that could mean that they are admitting having problems, an important starting point from which to continue working on further problem-solving strategies. Evidence documents that youth from disadvantaged families or communities participate in fewer organized activities, such as music lessons or hobby clubs, and for less time (Theokas & Bloch, 2006; Wimer et al., 2006). A community program aimed especially at this population can be an efficient way to counteract this deficit. Based on the results from this study, we consider that an optimal implementation strategy could be to place at-risk adolescents with peers from other countries, in large groups, with young facilitators; to get their families involved; and to make the program shorter, not only to promote their attendance but also to obtain the best results. Our study reveals that shortening the program to include fewer modules and having fewer extra activities predicts the highest number of positive competence outcomes in empathy and social realization, assistance seeking, cognitive-behavioural problem solving, and (less) cognitive avoidance. A recent study has also found that a short intensive youth development program offered adolescents more developmental experiences than longer conventional school activities (Bash, 2015). A short yet intensive community program provides adolescents with a unique social context and can initiate or sustain a positive developmental pathway with fewer negative experiences than longer school activities. As for the high number of extra activities, these could be overloading the participants, or they could be used in replacement of other important activities designed in the modules. The type of leisure activities performed during the current program influenced the positive outcomes achieved, as shown in a previous study (García-Poole et al., 2018). Organized group dynamics such as presentation games, rather than unorganized activities such as hanging out in overnight stays, were associated with a positive competence change profile. Finally, in relation to community competencies, young adolescents, residence in urban areas, and the use of less experienced (younger) facilitators predicted a high sense of community integration after the program. This is a positive finding, as urban individuals are typically found to be less community orientated (Prezza & Costantini, 1998). In this case, group composition and adherence to the program design did not contribute to the community outcomes. It is also possible that community competencies were not very self-evident for the adolescents, and that during the program facilitators did not emphasize the improvements made to their sense of belonging to the community or to their level of involvement in the community's social activities. A recommendation for both facilitators and adolescents would be to emphasize the contributions that their action projects can have to the community. Several limitations of this study are noteworthy. First, the measures of attendance rate, psychosocial risk status, and level of family involvement were group measures, and as such, were not able to capture the inter-variability between the members of each group. It was considered that asking the facilitators for this amount of specific information could potentially lead to overload, as they were already engaged in action projects with the participants and taking part in a major evaluation process. Second, the list of implementation measures is limited and could be complemented with information provided by the participants on quality of delivery. Third, data were collected by the group facilitators and not by independent researchers, which may introduce biases such as social desirability. Furthermore, the fact that a large number of participants were excluded from the analysis because of missing group data may introduce biases to the results, as this could indicate a variation in the facilitators' organization and overall program implementation. Fourth, even though the program is flexible and can be suited for most communities, the fact that this study was carried out in Spain can limit the generalizability of the findings. Finally, we do not have any follow-up data that show that our results are sustained over time. In conclusion, the findings from this study have shown that variations in the implementation conditions of the Building My Future program can affect adolescents' attendance rate and competencies, helping practitioners make informed decisions on future interventions. A future research agenda should be considered to overcome some of the limitations of this study, following a multidimensional model of implementation components. Quality of delivery can be better explored and reported on by independent researchers and participants, as well as further information should be given on participant dropout. Finally, other important outcomes related to these competences could be explored, such as health-related lifestyle profiles. Cite this article as: García-Poole, C., Byrne, S., & Rodrigo, M. J. (2019). Implementation factors that predict positive outcomes in a community-based intervention program for at-risk adolescents. Psychosocial Intervention., 28, 57-65. https://doi.org/10.5093/pi2019a4 Funding: This research was supported by Spanish Ministry of Education, Culture, and Sport grants (FPU13/00063) and by the Spanish Ministry of Economy and Competitiveness, under Research Project (PSI2012-32879). REFERENCES |
Cite this article as: GarcĂa-Poole, C. , Byrne, S. , & Rodrigo, M. (2019). Implementation Factors that Predict Positive Outcomes in a Community-based Intervention Program for at-Risk Adolescents. Psychosocial Intervention, 28, 57 - 65. https://doi.org/10.5093/pi2019a4
Correspondence: cgarciap@ull.edu.es (C. GarcĂa-Poole).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Imprimir
Imprimir Enviar
Enviar






