


Motivational Strategies in Interventions for Intimate Partner Violence Offenders: A Systematic Review and Meta-analysis of Randomized Controlled Trials
[Las estrategias motivacionales en las intervenciones con agresores de pareja: Revisión sistemática y meta-análisis de ensayos controlados aleatorizados]
Faraj A. Santirso1, Gail Gilchrist2, Marisol Lila1, and Enrique Gracia1
1University of Valencia, Spain; 2National Addiction Centre, Institute of Psychiatry, Psychology and Neuroscience, KingÔÇÖs College London, UK
https://doi.org/10.5093/pi2020a13
Received 20 October 2019, Accepted 9 June 2020
Abstract
Previous research suggests that the inclusion of motivational strategies in interventions for intimate partner violence (IPV) offenders could increase their effectiveness. This review evaluated the effectiveness of interventions for IPV offenders that includes motivational strategies to reduce physical and psychological IPV, treatment dropout, official recidivism to IPV offending, and to increase intervention attendance dose. The present systematic review and meta-analysis were conducted using PRISMA guidelines. The following databases were searched from 1983 to 2018 for randomized controlled trials (RCTs) of interventions for IPV offenders that incorporated motivational strategies for adult participants that included men and included IPV behaviors as outcomes: Cochrane Collaboration, MEDLINE, EMBASE, PsycINFO and CINAHL. A total 1,134 studies were identified, 12 RCTs were included in the narrative review and 7 in the meta-analysis. Results indicated that IPV interventions that incorporated motivational strategies were significantly more effective in increasing the intervention dose and reducing dropout than interventions without motivational strategies. IPV offenders receiving interventions with motivational strategies were 1.73 times less likely to intervention dropout compared to those in interventions without such strategies. For physical and psychological IPV and official recidivism (e.g., rearrests, police record), evidence favored interventions with motivational strategies, although not significantly. These findings have important practical implications, especially considering the high dropout rates in IPV offender programs and the link between dropout and higher rates of recidivism.
Resumen
La investigación previa sugiere que la inclusión de estrategias motivacionales en las intervenciones con agresores de pareja podría incrementar la efectividad de estas intervenciones. Esta revisión evaluó la eficacia de las intervenciones en agresores de pareja, que incluye las estrategias motivacionales para reducir la violencia física y psicológica contra la pareja, el abandono de la intervención y la reincidencia oficial, así como para aumentar la dosis de asistencia a las intervenciones. Tanto la revisión sistemática como el meta-análisis se llevaron a cabo siguiendo las recomendaciones PRISMA. Se examinaron las siguientes bases de datos desde 1983 hasta 2018, con objeto de localizar ensayos controlados aleatorizados (ECA) de intervenciones para agresores de pareja que incluyeran estrategias motivacionales, en las que los participantes fueran hombres mayores de edad y que incluyeran como variables de resultado conductas de violencia contra la pareja: Cochrane Collaboration, MEDLINE, EMBASE, PsycINFO y CINAHL. Se identificaron 1,134 estudios, incluyéndose 12 ECAs en la revisión narrativa y 7 en el meta-análisis. Los resultados indicaron que las intervenciones para agresores de pareja que incorporan estrategias motivacionales eran significativamente más efectivas en incrementar la dosis de intervención y reducir el abandono de la intervención que las que no incluían estrategias motivacionales. Los agresores que participaron en intervenciones con estrategias motivacionales tenían 1.73 veces menor probabilidad de abandonar el tratamiento, en comparación con aquellos que participaron en intervenciones sin tales estrategias. En cuanto a la violencia física y psicológica contra la pareja y la reincidencia oficial (e.g., arrestos reiterados, denuncias policiales), la evidencia, aunque no es significativa, favorece las intervenciones con estrategias motivacionales. Estos resultados tienen importantes implicaciones prácticas, especialmente si se tiene en cuenta las altas tasas de abandono de la intervención que se producen en los programas de intervención con agresores de pareja y la relación existente entre abandono de la intervención y mayores tasas de reincidencia.
Keywords
Intimate partner violence, Motivational strategies, Systematic review, Meta-analysis, Randomized controlled trialPalabras clave
Agresores de pareja, Estrategias motivacionales, Revisión sistemática, Meta-análisis, Ensayo controlado aleatorizadoCite this article as: Santirso, F. A., Gilchrist, G., Lila, M., & Gracia, E. (2020). Motivational Strategies in Interventions for Intimate Partner Violence Offenders: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Psychosocial Intervention, 29(3), 175 - 190. https://doi.org/10.5093/pi2020a13
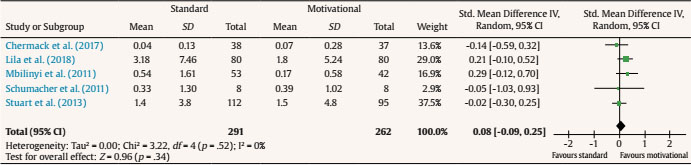
Marisol.Lila@uv.es Correspondence: Marisol.Lila@uv.es (M. Lila).Intimate partner violence (IPV) against women is a widespread public health problem with serious consequences on victims’ physical and psychological health, their children, and the wider society (Campbell, 2002; Ellsberg et al., 2008; Gracia, Rodríguez et al., 2020; Guedes et al., 2016; Martín-Fernández et al., 2019, 2020; Okuda et al., 2011; Vilariño et al., 2018; World Health Organization, 2013). Given the importance and complex nature of IPV, prevention and intervention strategies need to be targeted at different levels (i.e., individual, relational, contextual, and socio-cultural levels; Gracia, 2014; Gracia et al., 2008; Gracia, Lila, et al., 2020; Heise, 2011; Jewkes, 2002; Jewkes et al., 2015; World Health Organization, 2002). IPV offender intervention programs are one of the main treatment approaches aimed at preventing further violence (Cannon et al., 2016; Price & Rosenbaum, 2009; Voith et al., 2018). However, meta-analyses focused on the effectiveness of IPV offender intervention programs have shown small effect sizes (Arias et al., 2013; Babcock et al., 2004; Cheng et al., 2019; Eckhardt et al., 2013; Feder & Wilson, 2005; Gondolf, 2004; Smedslund et al., 2011). Research has identified a number of factors explaining the modest effectiveness of IPV offender intervention programs. High levels of attrition, low motivation to change, lack of acceptance of responsibility, low working alliance, and limited engagement in treatment activities are among these factors (Gerlock, 2001; Martín-Fernández, Gracia, Marco, et al., 2018; Saunders, 2008; Stuart et al., 2007). Levels of attrition are high in IPV offender intervention programs, ranging from 15% to 58% (Babcock et al., 2004; Bennett et al., 2007; Daly & Pelowski, 2000; Feder & Wilson, 2005; Jewell & Wormith, 2010; Olver et al., 2011; Rondeau et al., 2001). This is an important concern and challenge for the reduction and prevention of IPV, since program dropout is associated with higher recidivism rates (Bennett et al., 2007; Chen et al., 1989; Coulter & VandeWeerd, 2009; Dutton et al., 1997; Gondolf, 2000; Taft et al., 2001). Additionally, IPV offenders typically show low levels of motivation to change at the intake phases of IPV offender programs (Carbajosa, Catalá-Miñana, Lila, & Gracia, 2017; Carbajosa, Catalá-Miñana, Lila, Gracia, et al., 2017; Crane et al., 2015; Zalmanowitz et al., 2013). This is an important issue, because IPV offenders in the most advanced stages of change are more likely to complete the treatment (Eckhardt et al., 2004; Levesque et al., 2000; Scott, 2004; Scott & Wolf, 2003). Furthermore, IPV offenders are characterized by their tendency to deny and minimize their violent behavior, as well as to blame the victims (Heckert & Gondolf, 2000; Henning & Holdford, 2006; Lila et al., 2014; Martín-Fernández, Gracia, & Lila, 2018). A large number of IPV offenders are court-mandated to attend these intervention programs instead of receiving a custodial sentence (Eckhardt et al., 2013; Price & Rosenbaum, 2009). Consequently, they may not be purely voluntary and self-motivated participants to attend, as they are ‘forced’ to undergo an intervention that they often feel is useless or unfair (Eckhardt et al., 2013; Lila et al., 2018; Stuart et al., 2007). Finally, some studies have suggested that IPV offender intervention programs often use confrontational approaches that can limit the development of positive treatment processes, such as working alliance and engagement in treatment activities, limiting the effectiveness of the intervention (Murphy & Baxter, 1997; Taft et al., 2003). Several authors point out that the inclusion of motivational strategies, such as stages-of-change-based treatments, strengths-based treatments, motivational interviewing, and retention techniques, could overcome some of these limitations, increasing the effectiveness of interventions for IPV offenders (Babcock et al., 2016; Feder & Wilson, 2005). Thus, motivational strategies, with proven evidence among other populations resistant to change (such as people with alcohol and drug disorders), are increasingly being incorporated into IPV offender intervention programs with promising results (Babcock et al., 2004; Eckhardt et al., 2013; Lee et al., 2004; Morrel et al., 2003; Musser et al., 2008; Saunders, 2008; Scott et al., 2011; Taft et al., 2001). The ‘stages of change’ model, or the Transtheoretical Model of behavioral change (TTM; Prochaska & DiClemente, 1982; Prochaska et al., 1992), emphasizes that individuals proceed through a series of stages in preparing for, accomplishing, and maintaining behavior change (Prochaska & Velicer, 1997). Closely related to TTM, the Motivational Interviewing Techniques (MITs; Miller & Rollnick, 2002) assumes that participants arrive at interventions at different levels of readiness to change and focus on mobilizing a client’s intrinsic motivation (Murphy & Maiuro, 2009). Finally, retention techniques (e.g., telephone calls about appointments and after missed sessions) are focused on maintaining participants within the intervention program (Taft & Murphy, 2007; Taft et al., 2003). This body of research suggests potential benefits of incorporating motivational strategies into interventions for IPV offenders to increase its effectiveness. Therefore, the aim of this review was to rigorously assess the effectiveness of interventions for IPV offenders that includes motivational strategies in reducing physical and psychological IPV, treatment dropout, official recidivism to IPV offending (e.g., rearrests, police records), and in increasing intervention attendance dose. Only randomized controlled trial studies (RCTs) were included to obtain a precise effect size and to prevent possible confounding factors, as well as to ensure the replicability of the results (Ioannidis, 2015). RCTs are the gold standard for making comparisons between different interventions (Lilienfeld et al., 2018), since they afford enhanced control over different causes of spurious therapeutic efficacy, such as regression to the mean, spontaneous remission, or selection bias (Lilienfeld et al., 2014). As far as we are aware, this is the first systematic review and meta-analysis focusing on the effectiveness of motivational strategies in interventions for IPV offenders that has considered evidence only from RCTs. This systematic review and meta-analysis were undertaken in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) recommendations (Moher et al., 2009) and registered with the International Prospective Register of Systematic Reviews (PROSPERO 018: CRD42018110107). Search Strategy A systematic search of the literature was carried out in Cochrane Collaboration, MEDLINE, EMBASE, PsycINFO and CINAHL, covering the period from 1983 to August 2018; 1983 was selected as the start date for the search as this was when first publication about motivational interviewing was published (Miller, 1983). The search strategy included combining terms for randomized controlled trials, IPV interventions, and motivational strategies (see Appendix). Given the different nomenclatures used for IPV and motivational strategies, we first carried out a thesaurus search from Cochrane Collaboration, CINAHL, PsycINFO, Emtree terms in EMBASE, and Mesh terms in Medline to include all related terms in the search strategy. Search terms used included terms related to intimate partner violence (e.g., abuse, batterer, domestic, dating, and marital) and motivational strategies (e.g., motivational interviewing, motivational enhancement therapy, motivational intervention), and the Cochrane Highly Sensitive Search Strategy (Lefebvre et al., 2011) was used for identifying RCTs. Forward and backward searches of all relevant records were conducted by performing electronic searches for further relevant articles by the first author of any identified study. Eligibility Studies were eligible if (1) they were published during the 1983-2018 period; (2) the sample consisted of adult participants; (3) the sample included men; (4) they were RCTs; (5) the intervention incorporated motivational strategies; and (6) outcome/s included any IPV behaviors. No language restrictions were applied. Manuscripts were independently assessed for eligibility in two stages. Firstly, GG and FS independently assessed all titles and abstracts against eligibility criteria. Secondly, full-text articles of potentially eligible manuscripts were independently assessed (GG and FS), and disagreements were solved through discussions and consensus with additional reviewers (EG or ML). Figure 1 Flowchart. 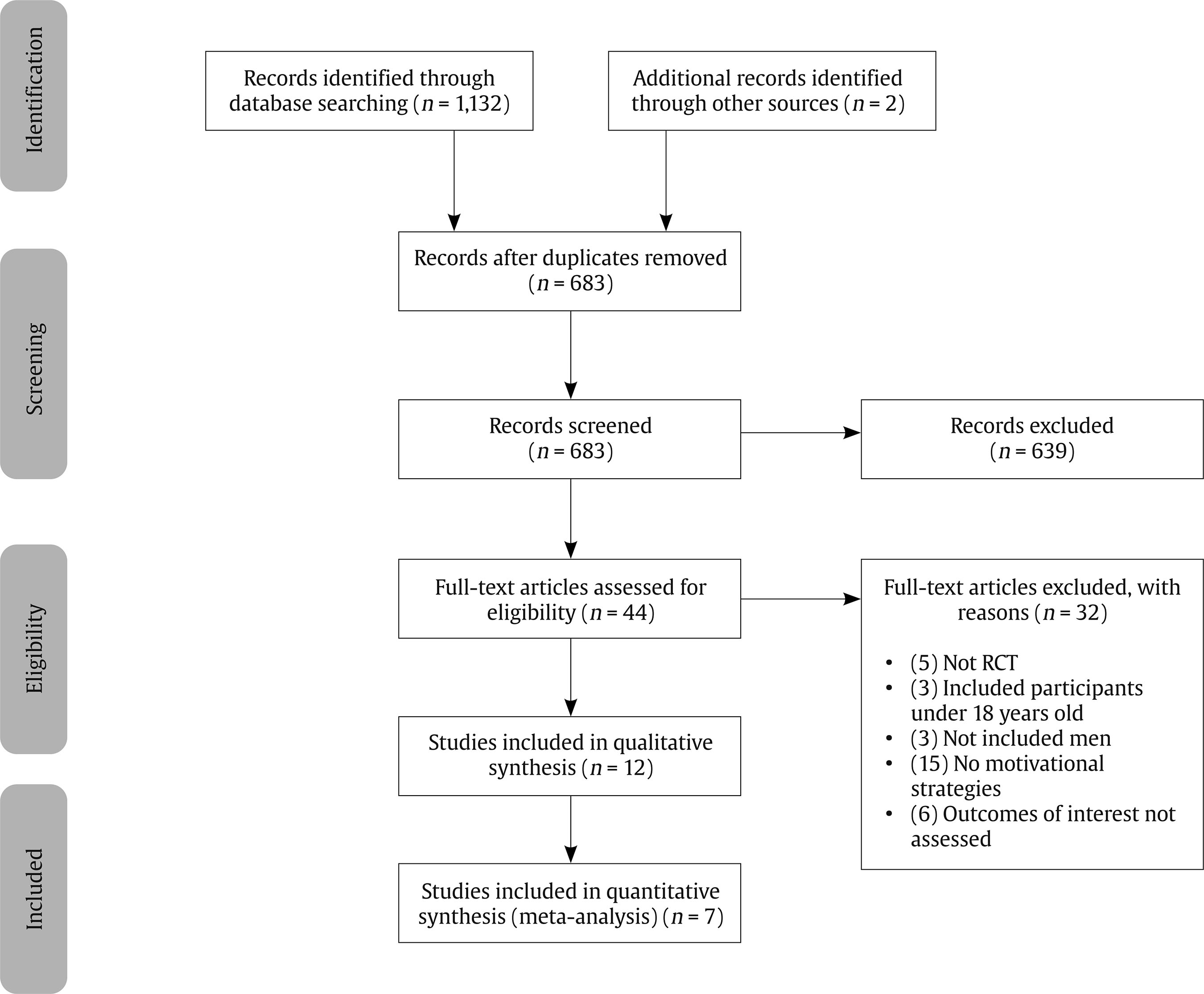 Data Extraction FS and GG independently extracted data from all included studies by following the Template for Intervention Description and Replication (TIDIeR; Hoffmann et al., 2014). Specifically, information around the intervention approach and goals, materials and procedures followed, intervention providers, frequency and duration of the intervention, delivery mode, setting and modifications made were extracted. In addition, outcome assessments and results were compiled. These data were verified by a third reviewer (EG or ML) and differences resolved through discussion. Assessment of Methodological Quality The methodological quality of trials was assessed using the Cochrane Risk of Bias tool (Higgins et al., 2011): 1) random sequence generation, 2) allocation concealment, 3) blinding of participants and personnel, 4) blinding of outcome assessment, 5) incomplete outcome data, and 6) selective reporting bias. Two authors (FS and GG) independently assessed trials’ methodological quality. Disagreements were resolved through discussion with other authors (EG or ML). Statistical Analysis The main summary measures were the standardized mean difference (SMD) and odds ratios (OR) depending on the nature of the variable (continuous or dichotomous). For each RCT, the corresponding 95% CIs for the assessed outcome were retrieved or calculated (Bland & Altman, 2000). Data entry and statistical analysis were carried out using Review Manager Software, version 5.3. When data from more than one follow-up period were reported, data from the latest period were included in the meta-analysis. The degree of heterogeneity (I2) was calculated to determine whether RCTs included in the meta-analysis were consistent. I2 of 25% was considered low, 50% moderate, and 75% high (Higgins et al., 2003). Study Selection Database searches resulted in 1,132 records and two additional ones were identified through other sources (Figure 1). Following the removal of duplicates, 683 articles were retained for title and abstract screening. In total, 639 abstracts were excluded as they did not meet the eligibility criteria and 44 manuscripts were selected for full text review. Thirty-two manuscripts were excluded because the intervention did not include motivational strategies (n = 15), outcomes of interest were not assessed (n = 6), they were not RCTs (n = 5), the sample was composed exclusively of women (n = 3), or the sample included offenders under the age of 18 (n = 3). The remaining 12 trials (see Table 1) were included in the qualitative synthesis and are marked with an “*” in the References section. Of these, five trials were excluded from the meta-analysis. One trial was excluded because it did not fully report the outcomes of interest (Alexander et al., 2010). The other four trials were excluded from the meta-analysis to favor comparability: two were couples-based therapy (Bahia 2016; Woodin & O’Leary, 2010), one incorporated motivational strategies in both conditions (Kraanen et al., 2013), and one trial used two different delivery intervention formats for each condition of the same intervention (individual intervention vs. group intervention; Murphy et al., 2017). Therefore, meta-analyses in this study included seven trials. Table 1 Summary of Trials 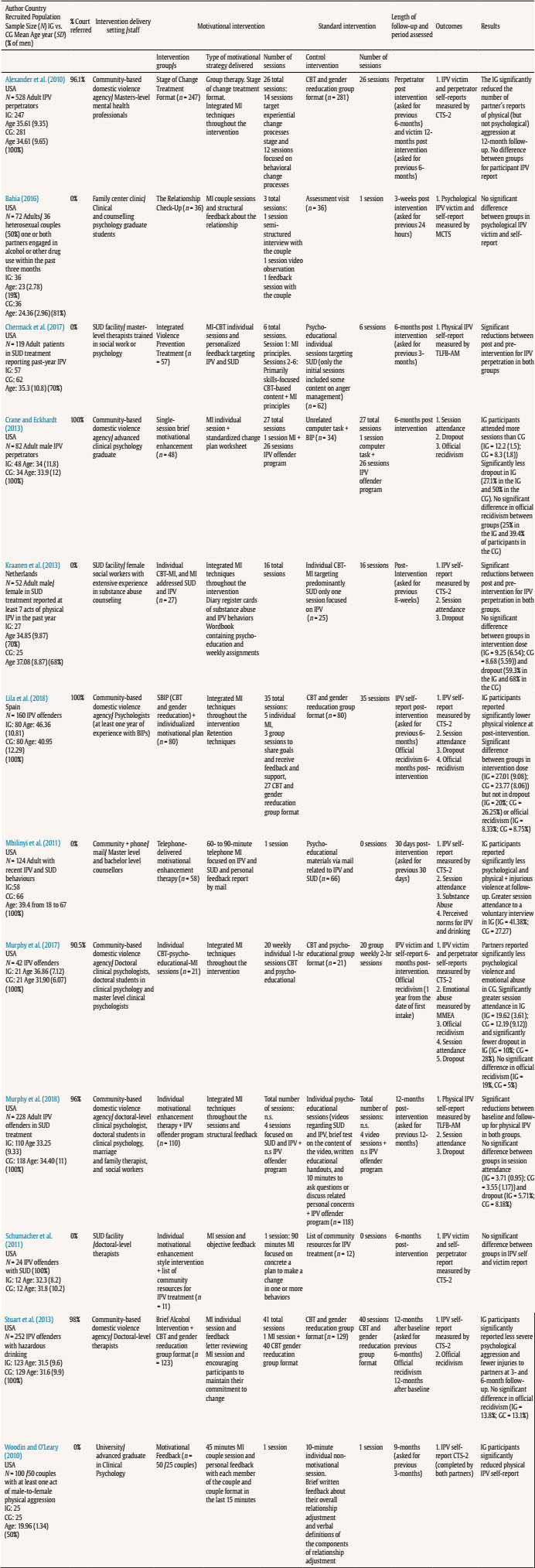 Note. CBT = cognitive behavioral therapy; CG = control group; CTS-2 = Revised Conflicts Tactics Scale; IG = intervention group; IPV = intimate partner violence; MMEA = Multidimensional Measure of Emotional Abuse; MCTS = Modified Conflict Tactics Scale; MI = motivational interviewing; n.s. = not specified; SUD = substance use disorder; TLFB-AM = Time Line Follow Back-Aggression Module. The 12 trials selected for the narrative review evaluated 1,733 participants, 844 in intervention groups (IG) and 889 in control groups (CG). Only seven trials were included in the meta-analyses, including 989 participants: 488 in intervention groups (IG) and 501 in control groups (CG). Most of the trials were conducted in the USA (n = 10; Alexander et al., 2010; Bahia, 2016; Chermack et al., 2017; Crane & Eckhardt, 2013; Mbilinyi et al., 2011; Murphy et al., 2017; Murphy et al., 2018; Schumacher et al., 2011; Stuart et al., 2013; Woodin & O’Leary, 2010), one in the Netherlands (Kraanen et al., 2013), and one in Spain (Lila et al., 2018). Quality and Publication Bias Assessment A summary of authors’ judgements about each risk of bias item for each included trial is described in Figure 2. Six trials (50%) met at least three criteria. None of the trials satisfied all criteria. Concerning random sequence generation, nine of 12 trials (75%) described a random component in the sequence generation. In one trial (8.3%) assignation was constrained by IPV offenders’ work schedules (Alexander et al., 2010), so its risk of bias was considered high. Knowledge of allocation concealment was not properly described except for two trials that reported a suitable method to conceal allocation (Kraanen et al., 2013; Stuart et al., 2013). Four trials (33.3%) reported no or incomplete blinding of participants and personnel (Alexander et al., 2010; Bahia, 2016; Murphy et al., 2018; Woodin & O’Leary et al., 2010). In the remaining eight trials (66.7%), the blinding of participants and personnel scores indicate that the risk is unclear due to inadequate description. Three trials (25%) ensured blinding of outcome assessment (Alexander et al., 2010; Murphy et al., 2018), or the outcome measurement was not likely to be influenced by lack of blinding (Crane & Eckhardt, 2013). Two trials reported no blinding of outcome assessment (Bahia, 2016; Woodin & O’Leary, 2010). The information provided was insufficient to assess detection bias of the remaining seven trials (58.3%). An intention-to-treat analysis was used in eight trials (66.7%; Chermack et al. 2017; Crane & Eckhardt, 2013; Kraanen et al. 2013; Lila et al., 2018; Murphy et al., 2017; Murphy et al., 2018; Stuart et al. 2013; Woodin & O’Leary, 2010). Regarding selective reporting, two trials (16.6%) were assessed as high risk because one or more outcomes of interest in the review were incompletely reported and, consequently, they could not be entered in the meta-analysis (Alexander et al., 2010; Woodin & O’Leary, 2010). In four trials (33.3%), information available was insufficient to judge the reporting bias (Bahia, 2016; Chermack et al., 2017; Kraanen et al., 2013; Murphy et al., 2018). Figure 2 Risk of Bias for Included Trials 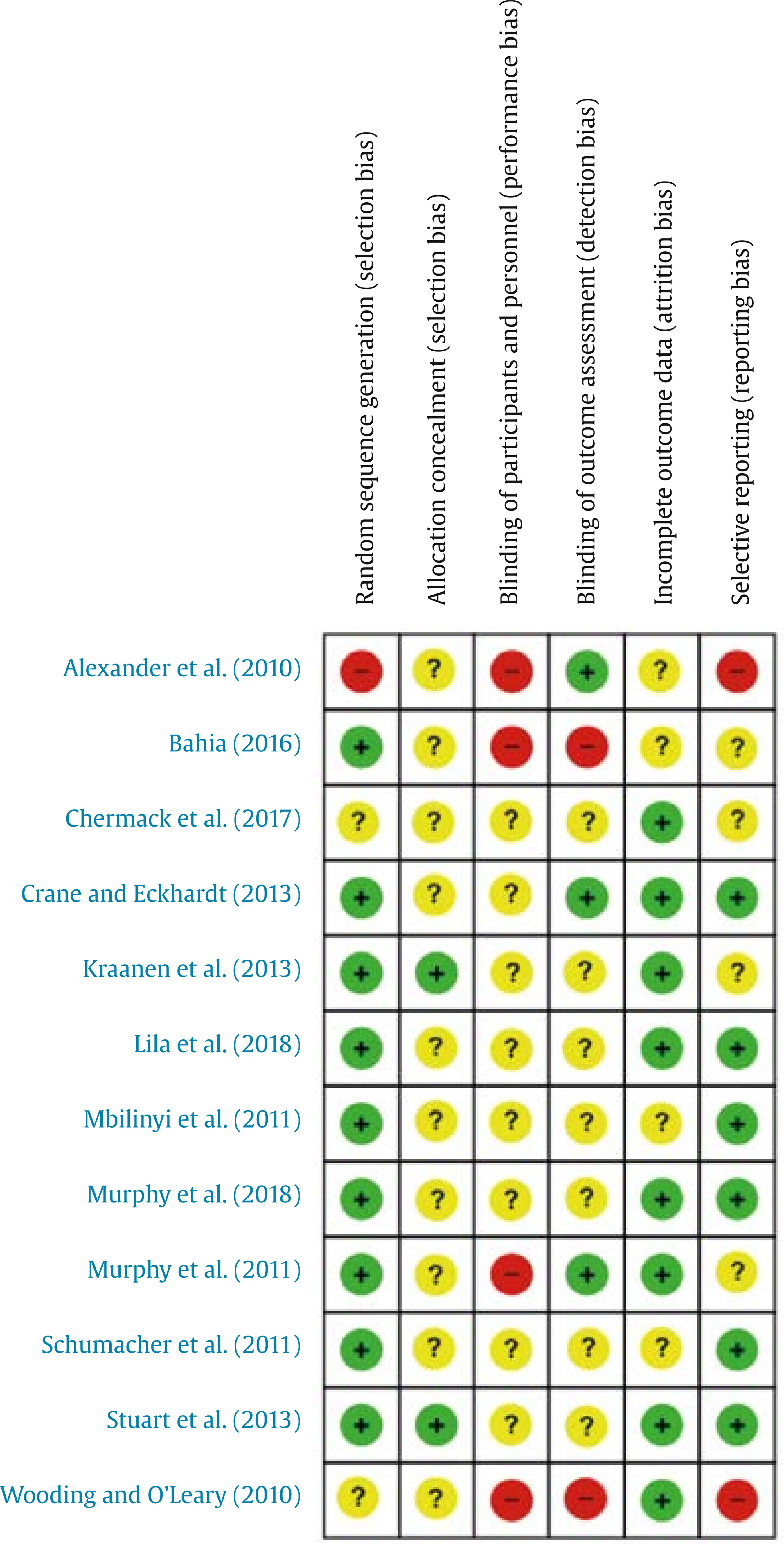 Qualitative Analysis The majority of trials recruited exclusively male IPV offenders (eight trials, 66.7%; Alexander et al., 2010; Crane & Eckhardt, 2013; Lila et al., 2018; Mbilinyi et al., 2011; Murphy et al., 2017; Murphy et al., 2018; Schumacher et al., 2011; Stuart et al., 2013). Four trials (33.3%) recruited both male and female IPV offenders, including 50% male (Bahia, 2016; Woodin & O’Leary, 2010), 69.2% male (Kraanen et al., 2013), and 70% male (Chermack et al., 2017). In seven trials (58.3%) participants also met criteria for substance use disorder (SUD; Bahia 2016; Chermack et al., 2017; Kraanen et al., 2013; Mbilinyi et al., 2011; Murphy et al., 2018; Schumacher et al., 2011; Stuart et al., 2013). Half of the reviewed trials included court-referred participants, ranging from 90.5% to 100% of the sample (Alexander et al., 2010; Crane & Eckhardt, 2013; Lila et al., 2018; Murphy et al., 2017; Murphy et al., 2018; Stuart et al., 2013), while the other half included only “voluntary” participants who had not been court-mandated (Bahia 2016; Chermack et al., 2017; Kraanen et al., 2013; Mbilinyi et al., 2011; Schumacher et al., 2011; Woodin & O’Leary, 2010). The intervention delivery setting was: community-based domestic violence agencies (Alexander et al., 2010; Crane & Eckhardt, 2013; Murphy et al., 2017; Murphy et al., 2018; Stuart et al. 2013), substance abuse facilities (Chermack et al. 2017; Kraanen et al., 2013; Schumacher et al., 2011), family center clinic (Bahia, 2016), university (Lila et al., 2018; Woodin & O’Leary, 2010), and community + phone/mail (Mbilinyi et al., 2011). In five trials (41.7%), the intervention was delivered by graduate-level professionals, either psychologists (Bahia 2016; Crane & Eckhardt, 2013; Lila et al., 2018; Woodin & O’Leary, 2010) or social workers (Kraanen et al., 2013). In two trials (16.7%), master-level mental health professionals delivered the intervention (Alexander et al., 2010; Chermack et al., 2017). In one study (8.3%) both graduate and master counsellors delivered the intervention (Mbilinyi et al., 2011). In four trials (33.3%) the intervention was conducted by doctoral-level professionals, either clinical psychologists (Murphy et al., 2017; Murphy et al., 2018) or therapists (without specifying background; Schumacher et al., 2011; Stuart et al., 2013). The content of the intervention in seven (58.3%) trials exclusively addressed IPV (Alexander et al., 2010; Bahia, 2016; Crane & Eckhardt, 2013; Lila et al., 2018; Murphy et al., 2017; Schumacher et al., 2011; Woodin & O’Leary, 2010) and five interventions (41.7%) targeted both IPV and SUD (Chermack et al., 2017; Kraanen et al., 2013; Mbilinyi et al., 2011; Murphy et al., 2018; Stuart et al., 2013). Five interventions for IPV offenders were delivered to individuals (Chermack et al., 2017; Kraanen et al., 2013; Mbilinyi et al., 2011; Murphy et al., 2018; Schumacher et al., 2011), four were delivered to groups (33.3%; Alexander et al., 2010; Crane & Eckhardt, 2013; Lila et al., 2018; Stuart et al., 2013), and two (16.7%) were couples-based interventions (Bahia, 2016; Woodin & O’Leary, 2010). In one trial (8.3%; Murphy et al., 2017) the motivational intervention was delivered individually to the intervention group and the standard intervention was delivered to the control group in a group format. Multiple motivational strategies were used in the RCTs. MITs (Miller & Rollnick, 2002) were included in all RCTs, most of them incorporating a personalized feedback to participants about their behaviors of interest (Bahia, 2016; Chermack et al., 2017; Mbilinyi et al., 2011; Murphy et al., 2018; Schumacher et al., 2011; Stuart et al., 2013; Woodin & O’Leary, 2010). Alexander et al. (2010) carried out an intervention based on stages of change, in which the first 14 sessions where focused on precontemplation and contemplation stages with an approach based on experiential change processes activities, and the following 12 sessions focused on advanced stages of change based on behavioral change process. Bahia (2016) delivered a couple-based intervention consisting of a semi-structured interview to identify areas of strength and strain in the relationship and build rapport, a couple video observation task, and a feedback session. Chermack et al. (2017) implemented six individual motivational interview-cognitive behavioral therapy (MI-CBT) sessions, with the first session focusing on MITs and enhancing motivation to change, and the remaining sessions being primarily skills-focused. Crane and Eckhardt (2013) carried out a single individual MI prior to entry into the IPV offender intervention program, and a standardized worksheet to reflect the change plan at the end of the interview. Kraanen et al. (2013) integrated MITs over the 16 sessions of the program and implemented diary register cards of SUD and IPV behaviors, as well as a workbook containing psychoeducation and weekly assignments. Lila et al. (2018) implemented five individual MI and three group sessions where participants shared their goals, and retention strategies and participants’ personal goals were reinforced throughout the program. Mbilinyi et al. (2011) conducted a single telephone MI and a personal feedback report by mail. Murphy et al. (2017) delivered 20 individual CBT-psycho-educational-MI sessions. Murphy et al. (2018) carried out four MIs prior to entry into the IPV offender program and included a personalized assessment feedback. Schumacher et al. (2011) implemented a MI session and provided a list of community resources for IPV treatment. Stuart et al. (2013) carried out a MI session prior to entering the program and delivered feedback letters reviewing the MI session. Finally, Woodin and O’Leary (2010) proposed a MI couple session divided into three parts: with the couple, with each member of the couple (in which they received personal feedback), and finally with the couple again. We found a high heterogeneity in terms of duration of the intervention. Six (50.0%) trials were long-term programs (Alexander et al., 2019; Crane & Eckhardt, 2013; Kraanen et al., 2013; Lila et al., 2018; Murphy et al., 2017; Stuart et al., 2013), with the number of sessions ranging from 16 (Kraanen et al., 2013) to 40 (Stuart et al., 2013). Three (25.0%) were short-term programs (Bahia, 2016; Chermack et al., 2017; Murphy et al., 2018), with the number of sessions ranging from three (Bahia, 2016) to six (Chermack et al., 2017). Finally, three interventions (25.0%) were carried out in a single session (Mbilinyi et al., 2011; Schumacher et al., 2011; Woodin & O’Leary, 2010). Regarding control groups, three trials (25%) compared IPV intervention programs with added motivational strategies against those without motivational strategies. Among them, the approach used was CBT and gender re-education group format (Alexander et al., 2010; Lila et al., 2018), and CBT and psycho-educational format (Murphy et al., 2017). Three trials (25%) compared pre-entry IPV offender program interventions that include motivational strategies against those comprised by non-motivational strategies, such as unrelated computer tasks (Crane & Eckhardt, 2013), no intervention (Stuart et al., 2013), or four individual psycho-educational sessions focused on IPV and SUD, written educational handouts, and 10 minutes to ask questions or discuss related personal concerns (Murphy et al., 2018). In two trials (16.7%) the control group was composed of interventions focused predominantly on SUD (Chermack et al., 2017; Kraanen et al., 2013). Two trials (16.7%) based control interventions on providing prevention materials; Schumacher et al. (2011) offered a list of community resources for IPV treatment, and Mbilinyi et al. (2011) sent psycho-educational materials via mail. In Woodin and O’Leary’s (2010) trial each partner in the control group received 10-minutes of non-motivational feedback sessions and a brief written feedback about overall relationship adjustment. In Bahia’s (2016) trial, couples in the control group received an assessment session only. Among trials comparing interventions of more than one session per condition, most (87.5%) included the same number of sessions in both groups (Alexander et al., 2010; Chermack et al., 2017; Crane & Eckhardt, 2013; Kraanen et al., 2013; Lila et al., 2018; Murphy et al., 2017; Murphy et al., 2018), except for Stuart et al. (2013), where the number of sessions was lower in the control intervention than in the motivational intervention. There was considerable heterogeneity across RCTs in the duration of time participants who were followed-up. The follow-up varied depending on the outcome considered. In two trials, the baseline/first intake was considered the reference point for reporting the follow-up time period; specifically, the follow-up was up to 12 months after the date of first intake (Murphy et al., 2017), and 12 months after baseline (Stuart et al., 2013). All other trials considered post-intervention as the starting point, with a follow-up time period from immediately post intervention (Kraanen et al., 2013), three weeks post intervention (Bahia, 2016), one-month post intervention (Mbilinyi et al., 2011), six months post intervention (Chermack et al., 2017); Crane & Eckhardt, 2013; Lila et al., 2018; Schumacher et al., 2011), nine months post intervention (Woodin & O’Leary, 2010), and 12 months post intervention (Alexander et al., 2010; Murphy et al., 2018). Regarding the assessment period participants were asked about, the most frequent was whether any of the IPV behaviors had occurred in the last 3 months (Chermack et al, 2017; Murphy et al. 2018; Stuart et al. 2013; Woodin & O’Leary, 2010). Two trials (16.7%) asked for reports of exceptionally short periods of time, such as Mbilinyi et al. (2011), who asked for the previous 30 days, and Bahia (2016), who asked for the past 24 hours. Regarding the main outcomes analyzed in RCTs, physical IPV was assessed in all trials except in Bahia’s (2016) and in Crane and Eckhardt’s (2013) studies. All trials used the Conflict Tactics Scales-Revised (CTS-2; Straus et al., 1996) or tools based on the same scale (Chermack et al., 2017; Murphy et al., 2018). These tools were semi-structured interviews to identify specific days in which physical assault and injurious behaviors occurred. Psychological IPV was assessed in nine RCTs (75.0%; Alexander et al. 2010; Bahia, 2016; Kraanen et al., 2013; Lila et al. 2018; Mbilinyi et al., 2011; Murphy et al., 2017; Stuart et al., 2013; Schumacher et al., 2011; Woodin & O’Leary, 2010). All trials used CTS-2 except for Bahia (2016), who used an alternative tool based on the same scale. Only one study included the Multidimensional Measure of Emotional Abuse (MMEA; Murphy et al., 1999) to measure emotional abuse (Murphy et al., 2017). Only two trials (16.7%; Alexander et al., 2010; Murphy et al., 2017) obtained victim reports about both physical and psychological IPV. Injuries resulting from IPV were assessed in three RCTs (25.0%; Kraanen et al., 2013; Murphy et al., 2017; Stuart et al., 2013) using the CTS-2. Dropout and intervention doses were assessed in five trials (41.7%; Crane & Eckhardt, 2013; Kraanen et al., 2013; Lila et al., 2018; Murphy et al., 2017; Murphy et al., 2018). Official recidivism (i.e., rearrests, police records) was assessed in four trials (33.3%; Crane & Eckhardt, 2013; Lila et al., 2018; Murphy et al., 2017; Stuart et al., 2013). In three trials, IPV specific recidivism was assessed (Lila et al., 2018; Stuart et al., 2013; Murphy et al., 2017). However, Crane and Eckhardt (2013) were unable to assess IPV-specific recidivism due to the low rate of IPV events, and therefore considered any new police record as recidivism (including IPV and non IPV events). The follow-up assessment period for official recidivism varied across RCTs. Crane and Eckhardt (2013) collected recidivism data six months after the first pre-intervention session, Lila et al. (2018) six months after completing the intervention, Stuart et al. (2013) twelve months following the baseline assessment, and Murphy et al. (2017) twelve months from the date of first intake. Trial Authors’ Findings and Conclusions Integrated motivational strategies throughout IPV offender intervention program. Alexander et al. (2010) found a significant reduction for the motivational intervention group in the number of partner reports of physical violence 12 months post intervention (p < .01), but not in psychological violence. No differences in participant self-reported violence during follow-up were found (Alexander et al., 2010). Chermack et al. (2017) found a significant reduction in total violence reported by participants in both conditions at 6-month follow-up compared with the baseline. Kraanen et al. (2013) found a significant reduction in IPV perpetration in participants in both treatment conditions after the intervention. Those in the motivational intervention group received a higher mean intervention dose (mean ± SD: IG = 9.25 ± 6.54, CG = 8.68 ± 5.59, p = .89) and a lower proportion of intervention dropout was reported (IG = 59.3%, CG = 68%, p = .51), but these differences were not statistically significant (Kraanen et al., 2013). Lila et al. (2018) reported significant reductions in physical violence at post-treatment in the motivational group (p < .05). Moreover, participants from the motivational group received a significantly higher mean intervention dose (mean ± SD: IG = 27.01 ± 9.08, CG = 23.77 ± 8.06, p < .01) and a lower proportion dropped out of the intervention (IG = 20%, CG = 26.25%, p = .15) and official recidivism at 6 month post intervention (IG = 8.33%, CG = 8.75%, p = .64) (Lila et al., 2018). Murphy et al. (2017) showed less psychological and emotional violence reported by partners six months after the intervention in participants from control intervention (CBT and psychoeducational 20 group weekly 2-hour sessions). A lower proportion of participants in the motivational group dropped out of the intervention (IG = 10%, CG = 28%, p = .03) and received a significant higher mean intervention dose (mean ± SD: IG = 19.62 ± 3.61, CG = 12.19 ± 9.12, p = .001) (Murphy et al., 2017). There were no significant differences in official recidivism at 12 month from the date of first intake between motivational and control groups (IG = 19%, CG = 5%) (Murphy et al., 2017). Figure 3 Self-reported Physical IPV.  Motivational intervention prior to entry in IPV offender program. Crane & Eckhardt (2013) found that participants in the motivational intervention received a non-statistically significant higher mean intervention dose (mean ± SD: IG = 8.34 ± 9.89, CG = 12.24 ± 10.18, p = .09) and a significantly lower proportion dropped out of the intervention than those from the control group (IG = 27.1%, CG = 50%, p = .04). Moreover, motivational intervention participants showed a reduction in official recidivism at 6 months post intervention (IG = 25%, CG = 39.4%), although this difference did not reach statistical significance. Similarly, Stuart et al. (2013) found that those in motivational intervention reported less severe psychological violence and fewer injuries to partners at three- and six-month follow-up (for all, p < .04). However, there were no significant differences between groups in physical IPV and official recidivism at 12 months following the baseline (IG = 13.8%, CG = 13.1%) (Stuart et al., 2013). Murphy et al. (2018) showed that both groups had a significant reduction in physical violence from baseline through 12-month follow-up. Those in the motivational intervention group received a higher mean intervention dose (mean ± SD: IG = 3.71 ± 0.95, CG = 3.55 ± 1.17, p = .27) and a lower proportion dropped out than those from the control group (IG = 5.71%, CG = 8.18%, p = .31), but these differences were not statistically significant (Murphy et al., 2018). Single session interventions. Mbilinyi et al. (2011) reported a significant reduction in psychological and physical plus injurious violence for participants in the motivational intervention group. In addition, these participants showed higher attendance to a voluntary interview (IG = 41.38%, CG = 27.27) (Mbilinyi et al., 2011). Schumacher et al. (2011) found no differences in IPV reported by victims or self-reported by offenders between groups. Couple-based interventions. Bahia et al. (2016) reported no significant differences in psychological violence reported by victims or self-reported by offenders between groups. Woodin and O’Leary (2010) found a significant reduction in self-reported IPV in the motivational group. Meta-analysis The main outcomes analyzed in the meta-analysis were physical and psychological IPV, intervention dropout, intervention dose, and official recidivism. Injuries resulting from IPV were not included in the meta-analysis as only one trial measured this outcome (Stuart et al., 2013). Results for the outcomes analyzed are showed in Figures 3-7. Figure 4 Self-reported Psychological IPV.  Figure 5 Dropout.  Figure 6 Intervention Dose.  Figure 7 Official Recidivism. 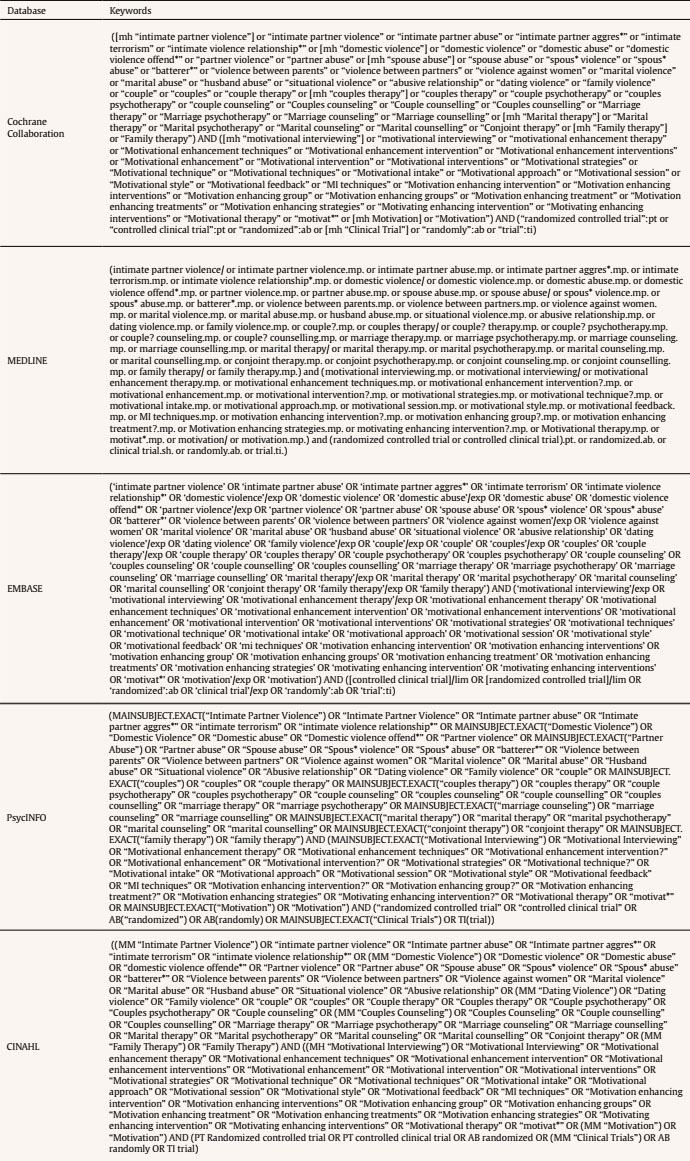 Physical IPV. Data from trials carried out by Murphy et al. (2018) and Woodin and O’Leary (2010) could not be included in the meta-analysis due to the lack of data for comparison (means and standard deviations were not reported in the manuscript). The meta-analysis with self-reported physical IPV as outcome included 553 participants from five trials (Chermack et al., 2017; Lila et al., 2018; Mbilinyi et al., 2011; Schumacher et al., 2011; Stuart et al., 2013). It is worth noting that Mbilinyi et al. (2011) included results of self-reported physical and injurious IPV combined, so in the present meta-analysis this measure was considered as an indicator of physical violence. Only Alexander et al. (2010) examined victim-reported physical IPV, so this outcome was not included in the meta-analysis. IPV offenders allocated to receive motivational interventions showed a non-significant reduction in the occurrence of physical IPV compared to those allocated to control interventions (SMD = 0.08, 95% CI [-0.09, 0.25]) (Figure 3). Heterogeneity was low (I2 = 0%). Consequently, no further analysis of the heterogeneity was conducted. Psychological IPV. Four trials with a total of 478 participants (Lila et al., 2018; Mbilinyi et al., 2011; Schumacher et al., 2011; Stuart et al., 2013) were included in the meta-analysis with self-reported psychological IPV as the outcome. Only one trial examined victim-reported psychological IPV (Alexander et al., 2010), so this outcome was not included in the meta-analysis. IPV offenders allocated to receive motivational interventions showed no difference in psychological IPV occurrence compared to those allocated to interventions without motivational strategies (SMD = 0.09, 95% CI [-0.21, 0.38]) (Figure 4). Moderate heterogeneity (I2 = 53%) was reported. No further analysis of heterogeneity was conducted. Dropout. Three trials with a total of 455 participants were included in the meta-analysis with intervention dropout as outcome (Crane & Eckhardt, 2013; Lila et al., 2018; Murphy et al., 2018). IPV offenders receiving motivational interventions were significantly more likely to complete the intervention, compared to interventions without motivational strategies (OR = 1.73, 95% CI [1.04, 2.89]) (Figure 5). Heterogeneity was low (I2 = 0%). Intervention dose. Three trials with a total of 449 participants were entered into the meta-analysis with intervention dose as an outcome (Crane & Eckhardt, 2013; Lila et al. 2018; Murphy et al., 2018). IPV offenders allocated to receiving motivational interventions significantly attended a higher number of sessions than those allocated to interventions without motivational strategies (SMD = 0.27, 95% CI [0.08, 0.45]) (Figure 6). Heterogeneity was low (I2 = 0%). Official recidivism. Three trials with a total of 492 participants were included in the meta-analysis with official recidivism (i.e., rearrests, police records) as outcome (Crane & Eckhardt, 2013; Lila et al., 2018; Stuart et al., 2013). In the motivational intervention, 35 participants out of 251 (13.9%) were rearrested on one or more occasions at follow-up, compared with 40 participants out of 241 (16.6%) in the intervention without motivational strategies. Evidence favored motivational interventions, although not significantly (OR = 1.46, 95% CI [0.76, 2.80]) (Figure 7). Heterogeneity was low (I2 = 33%), so no further analysis of heterogeneity was conducted. A systematic review and meta-analysis of the effectiveness of motivational strategies in interventions for IPV offenders was conducted. Different outcomes were compared (i.e., self-reported physical and psychological IPV, dropout, intervention dose and official recidivism). Twelve trials were included in the qualitative analysis and seven trials in the meta-analysis. Results from the meta-analysis indicated that interventions for IPV offenders that included motivational strategies were significantly more effective in reducing dropout and increasing intervention dose than interventions without motivational strategies. For official recidivism and self-reported physical and psychological IPV, evidence favored motivational interventions, although results did not reach statistical significance. Concerning dropout and intervention dose, all analyzed trials found greater reductions in dropout and increases in the number of intervention sessions attended among offenders participating in motivational interventions compared to those in interventions without motivational strategies (Crane & Eckhardt, 2013; Lila et al., 2018; Murphy et al., 2018). Intervention dropout rate was 15.02% in interventions that included motivational strategies versus 20.72% in interventions without these strategies. This means that dropout rate was 1.73 times greater amongst interventions for IPV offenders without motivational strategies compared to those that included them. It is noteworthy that lower dropout in motivational intervention groups was also found in Crane and Eckhardt’s (2013) trial, that incorporated only a single motivational interviewing session prior to the delivery of a standard IPV offender program. However, in Crane and Eckhardt’s (2013) study, improvements in initial treatment compliance in the motivational condition tended to dissipate over time. It is possible that interventions with more motivational strategies could lead to more durable gains, suggesting that the majority of trials with integrated motivational strategies delivered throughout the duration of the intervention program maintained these effects with large follow-up periods of at least six months (Alexander et al., 2010; Chermack et al., 2017; Kraanen et al., 2013; Lila et al., 2018; Murphy et al., 2017). Lundahl et al. (2010) conducted a systematic review of the effectiveness of motivational interviewing on SUD, gambling, health-related behaviors, and engagement in treatment and found similar results, that is, the greater the dose of motivational strategies received, the better the outcomes. This body of evidence highlights the importance of incorporating motivational strategies to significantly increase treatment compliance among IPV offenders (Miller & Rollnick, 2002; Musser et al., 2008; Soleymani et al., 2018). These findings have important practical implications, especially considering high dropout rates in IPV offender programs and the link between dropout and higher rates of recidivism reported (Jewell & Wormith, 2010; Lila et al., 2020; Lila et al., 2019; Olver et al., 2011; Stoops et al., 2010). For example, Lila et al. (2019) analyzed official recidivism from an IPV offender program and found that dropout was the most predictive variable of official recidivism. Regarding official recidivism, two trials in the current meta-analysis favored motivational intervention (Crane & Eckhardt, 2013; Lila et al., 2018), and one trial reported inconclusive evidence (Stuart et al., 2013). Considering these three trials, the rate of recidivism was 1.46 times greater in IPV offenders from standard interventions compared to those from motivational interventions, although results did not reach statistical significance. One possible explanation for this result could be the low level of official recidivism rates among participants in both conditions. Of the 492 participants analyzed, only 75 were rearrested on one or more occasions at follow-up. Arrests are low base-rate events limiting the power of our analysis. Police reports as an index of IPV recidivism could be also problematic and may not appropriately reflect reality. Many acts of IPV do not result in law enforcement intervention and, therefore, are likely to greatly underestimate IPV actual frequency (Velonis et al., 2016). As Babcock et al. (2004) pointed out, official reports could be inaccurate and some crimes may not appear on criminal records (e.g., crimes committed outside of the state or local jurisdiction, violence incidents in which adjudication was deferred), and there is a certain disparity in which types of crimes research considered as recidivism. For example, in our meta-analysis, three trials considered only IPV-specific new police records (Lila et al. 2018; Murphy et al., 2017; Stuart et al., 2013), while another (Crane & Eckhardt et al., 2013) considered any new police report. Nevertheless, arrest records are the most objective data available on IPV recidivism and the most commonly used objective recidivism measure (Babcock et al., 2004; Gondolf, 2004; López-Ossorio et al., 2016). Despite the lack of statistical significance in official recidivism results in this meta-analysis, the role of motivational strategies in lowering attrition and recidivism has been stressed in previous systematic reviews on IPV offender programs’ effectiveness (Babcock et al., 2004; Eckhardt et al., 2013). Regarding physical IPV reported by offenders, the meta-analysis indicates that two trials favored motivational intervention (Mbilinyi et al., 2011; Lila et al., 2018), two trials favored control intervention (Chermack et al., 2017; Schumacher et al., 2011), and one trial showed inconclusive evidence (Stuart et al., 2013). Two trials favored motivational intervention (Lila et al., 2018; Mbilinyi et al, 2011) on psychological IPV reported by offenders, and two trials favored control intervention (Schumacher et al., 2011; Stuart et al., 2013). Overall, although reduction in psychological IPV was in the expected direction across all included studies, the difference was not large enough to be significant. Reliance on self-reported perpetrators IPV behavior still presents complex issues (Babcock et al. 2004). Despite the fact that the use of reliable and well-validated instruments and the guarantee of confidentiality reduces the risk of biased data (Babor et al., 2000), the court-mandated nature of some IPV offender programs may cause participants to associate program staff with probation personnel and to adapt their responses accordingly (Crane & Eckhardt et al., 2013). In our meta-analysis, the percentage of court ordered participants in the sample measuring outcomes for physical and psychological IPV were 60% and 73%, respectively. Previous studies showed that such participants were more likely to minimize the severity of assaults than their victims (Heckert & Gondolf, 2000). In fact, Alexander et al. (2010) found that motivational interventions favor a significant reduction in the number of partner reports of physical violence, but not a significant reduction in self-reported violence. Finally, based on this systematic review and meta-analyses, the following recommendations for future trials can be made. Longer follow-up periods are necessary to appropriate assess persistence of change (Alexander et al., 2010; Soleymani et al., 2018). Also, it is important to accurately report follow-up start point. For example, some trials used the date of first intake or baseline assessment as the start of the follow-up period. However, there may be a substantial delay between the in-take and the actual initiation of the intervention program. Using post treatment as reference point could help improve comparability of study results. A clear definition of dropout criteria is also important. Indicating the number of participants who leave the program before it ends (i.e., dropout) provides more accurate information than, for example, stablishing a pre-defined percentage of participation as criteria. Additionally, one way to strengthen overall validity of IPV offender program outcomes would be data triangulation, such as using information from perpetrators, current or ex-partners, and police records (Heckert & Gondolf, 2000). This review is not without limitations. We have only considered RCTs in our study. Although it is a strength of our study to use the gold standard to evaluate interventions effectiveness (Lilienfeld et al., 2018), we are aware of difficulties of and downsides to the use of RCT in the field of IPV offender treatment (Lilley-Walker et al., 2018), what explain in part the low number of RCTs found. Relatedly, the low number of studies included in the meta-analysis implies that the results should be considered with caution. Also, the outcomes considered (men’s self-reported physical and psychological IPV or official recidivism) to report change in behavior or effectiveness could raise concerns about whether we are measuring IPV offender treatment ‘success’ too narrowly without accurately reflecting relevant changes in any controlling or coercive behaviors, repeating victimization, or whether women/children feel safer (Arbach & Bobbio, 2018; Dobash et al., 1999; Hester & Westmarland, 2005). Also, self-report measures of physical and psychological IPV can be vulnerable to participants’ distortions and social desirability biases (Eckhardt et al., 2012; Gracia et al., 2015; Santirso et al., 2018). In addition, methodology of studies presented considerable heterogeneity in terms of duration, intervention format, follow-up duration, or methods used to evaluate outcomes. Finally, some studies included mixed samples of men and women and court referred and non-court referred participants, without reporting disaggregated data. This may have influenced results. Despite these limitations, this review points to the potential benefits of integrating motivational strategies into IPV offender programs to increase intervention adherence and reduce dropout. Also, sustained integration of motivational strategies throughout the delivery of IPV intervention program could lead to more substantial gains than the use of a single session motivational strategy, increasing long-term effects of these programs (Lila et al., 2018; Santirso et al., 2020). Additionally, matching the appropriate intervention with participants’ readiness to change could help to improve the effectiveness of these programs (Begun et al., 2003; Eckhardt et al., 2004; Levesque et al., 2008). Alexander et al. (2010) and Murphy et al. (2017) illustrated that participants who are less ready to change at intake were more likely to benefit from interventions that included motivational strategies. Also, therapists who use motivational strategies tend to minimize their confrontational style, develop a more collaborative therapeutic alliance, and find less resistance from participants (Alexander et al., 2010; Stuart et al., 2007). In contrast to a more coercive approach, motivational strategies may help IPV offenders to overcome ambivalence about change, helping them to find their own reasons to change and promoting offenders efficacy in obtaining their goals and, more generally, increasing IPV offender program effectiveness. Conflict of Interest The authors of this article declare no conflict of interest. Cite this article as: Santirso, F. A., Gilchrist, G., Lila, M., & Gracia, E. (2020). Motivational strategies in interventions for intimate partner violence offenders: A systematic review and meta-analysis of randomized controlled trials. Psychosocial Intervention, 29(3), 175-190. https://doi.org/10.5093/pi2020a13 Funding: This work was supported by the Spanish Ministry of Health, Consumption and Social Services, National Drugs Plan (PND2018/021). Faraj A. Santirso was supported by the FPU Program of the Spanish Ministry of Science, Innovation and Universities (grant number FPU15/00864). References References with an asterisk refer to articles included in the meta-analysis. |
Cite this article as: Santirso, F. A., Gilchrist, G., Lila, M., & Gracia, E. (2020). Motivational Strategies in Interventions for Intimate Partner Violence Offenders: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Psychosocial Intervention, 29(3), 175 - 190. https://doi.org/10.5093/pi2020a13
Marisol.Lila@uv.es Correspondence: Marisol.Lila@uv.es (M. Lila).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
Send






