


A Personalized Remote Video-Feedback Universal Parenting Program: A Randomized Controlled Trial
[Un programa personalizado de parentalidad a distancia mediante feedback por v├şdeo: un ensayo controlado aleatorizado]
Maria Beatriz M. Linhares, Elisa R. P. Altafim, Cláudia M. Gaspardo, and Rebeca C. de Oliveira
University of São Paulo, Brazil
https://doi.org/10.5093/pi2021a9
Received 22 March 2021, Accepted 9 August 2021
Abstract
The randomized controlled trial examined the efficacy of a personalized remote video feedback parenting program to improve parenting and child behavior outcomes. Ninety-two mothers of 2-6-year-old children were randomly allocated into the intervention group (n = 50) and waiting-list control group (n = 42). The Strengthening Bonds preventive program was performed to improve positive parenting. The mothers participated in one in-person group session. During six weeks, the mothers received, via smartphone, remote personalized video feedback about their mother-child interactions in a play situation. Parenting was the primary outcome, and child behavior was the secondary one. Pre- and post-intervention assessments were performed. The generalized estimating equation analysis showed no significant results in the intention-to-treat (ITT). In the treatment-on-the-treated (TOT), there were statistically significant effects of the intervention decreasing mothers’ coercive parenting practices and child behavior problems. The structural equation model analysis showed that the intervention-induced reductions in children’s behavior problems were mediated by improvements in coercive practices. There was a direct effect of the intervention to improve the parental sense of competence. Despite the null findings in the ITT analysis, the TOT analysis showed promising results to strengthen positive parenting behaviors and beliefs and reduce child behavior problems.
Resumen
El ensayo controlado aleatorizado analizó la eficacia de un un programa personalizado de parentalidad a distancia mediante feedback por vídeo dirigido a mejorar la parentalidad y el comportamiento de los niños. Se distribuyó aleatoriamente a 92 madres de niños de entre 2 y 6 años de edad en el grupo de intervención (n = 50) y un grupo control de lista de espera (n = 42). Para mejorar la parentalidad positiva se utilizó el programa preventivo Strengthening Bonds, en el que las madres participaron en una sesión de grupo presencial. Durante seis semanas recibieron por teléfono móvil feedback en vídeo personalizado sobre su interacción madre-hijo durante el juego. El resultado primario fue la conducta parental, y el resultado secundario la conducta del niño. Se llevaron a cabo mediciones preintervención y posintervención. El análisis de ecuaciones de estimación general no tuvo resultados significativos en los análisis por intención de tratar (AIT). En los análisis por protocolo (APP) hubo efectos significativos, reduciendo las prácticas parentales coercitivas de las madres y los problemas de conducta de los niños. El análisis de modelos de ecuaciones estructurales reveló que la disminución de los problemas de conducta de los niños producida por la intervención era mediada por la mejora en las prácticas coercitivas. La intervención tenía un efecto directo en la mejora del sentimiento de competencia parental. A pesar de la falta de resultados del AIT, el APP dio resultados prometedores en cuanto a la mejora de las conductas y creencias parentales positivas y en la reducción de los problemas de conducta de los niños.
Keywords
Video feedback strategy, Parenting, Child behavior, Early childhood developmentPalabras clave
Estrategia de feedback por v├şdeo, Parentalidad, Comportamiento del ni├▒o, Desarrollo temprano en la infanciaCite this article as: Linhares, M. B. M., Altafim, E. R. P., Gaspardo, C. M., & Oliveira, R. C. D. (2022). A Personalized Remote Video-Feedback Universal Parenting Program: A Randomized Controlled Trial. Psychosocial Intervention, 31(1), 21 - 32. https://doi.org/10.5093/pi2021a9
linhares@fmrp.usp.br Correspondence: linhares@fmrp.usp.br (M. B. M. Linhares).Early childhood development intervention is a substantial investment to reduce inequalities in human development caused by poverty, violence, poor parental care, and limited learning opportunities (Black et al., 2017; Engle et al., 2011; Grantham-McGregor et al., 2007). Developmental neuroscience shows that early biological and psychosocial experiences affect brain development (Walker et al., 2011). The risk factors for child development include family stress, exposure to violence, child abuse or neglect, and limited community resources (Black et al., 2017). However, it is essential to note that these negative impacts of risks are modifiable, and potential loss is preventable (Jolly, 2007; Leijten et al., 2019). The responsive relationships at early ages contribute effectively to the brain’s development and plasticity and the cognitive, language, and socio-emotional development of children (Fisher et al., 2016; Jeong et al., 2020). Achieving the 2030 Sustainable Development Goals (United Nations, 2015) involves implementing parenting programs that promote positive and responsive relationships between parents and children, ensuring adequate health, security and safety, responsive caregiving, and early learning opportunities for young children (Black et al., 2017; World Health Organization, 2009). Nurturing care may attenuate the negative impact of low socioeconomic status on the brain development of children (Hanson et al., 2015; Pavlakis et al., 2015), which is sensitive to children’s needs, responsiveness, emotional support, appropriate stimulation playing and exploring, and protection from adversities (Black & Aboud, 2011). Parenting encompasses broad global styles and domain-specific dimensions (Smetana, 2017). First, the pattern-based approach includes the following styles: authoritarian, authoritative, and permissive-indulgent. The authoritative style is characterized by warmth, responsiveness, consistency, and enforcement of boundaries; the authoritarian style is characterized by detrimental coercive and harsh discipline (Baumrind, 1967). Physical discipline, yelling, expressing disappointment, and shaming are hallmarks of authoritarian parenting (Smetana, 2017) and coercive discipline (Eddy et al., 2001). Multiculturally, quality mother-child interactions predict balanced positive parental discipline and vice versa (Pastorelli et al., 2016). Also, positive parent-child engagement reduces the impact of coercion in decreasing child behavior problems in early childhood (Sitnick et al., 2015). Second, a developmental parenting approach highlights interactive behaviors and beliefs based on every family’s assumption (Roggman et al., 2008). Focusing on mother-child interactions, the synchronicity component promotes child development through dynamic adaptation and temporal reciprocity of behaviors (Leclère et al., 2014). The dyadic synchrony interactions of children and their caregivers represent a significant achievement of close dyadic relationships, a developmental milestone, even changing the structure and function throughout early child development (Harrist & Waugh, 2002). Responsive relationships, including warmth, sensitive responsiveness, and adaptability, are crucial to promoting secure and healthy child development (Juffer et al., 2018; McFadden & Tamis-Lemonda, 2013). Sensitive parenting is linked with maternal emotional regulation and cognitive control, which, in turn, is a key component of protective parenting with a low risk of engagement in maltreatment practices (Crandall et al., 2015). Also, in the belief and feeling systems, the parental sense of competence represents parents’ self-confidence in supporting children’s development (Grusec & Danyliuk, 2014). The sense of competence is a key active ingredient that increases supportive parenting and decreases negative parental discipline (Dekovi et al., 2010). An enabling environment includes family support as proximal providers of nurturing and nutrition and mental and physical benefits to child growth and development (Jeong et al., 2020; Singla et al., 2015). Parenting programs effectively reduced child behavior problems (Kaminski et al., 2008; Leijten et., 2019; Thomas et al., 2017) through strengthening caregivers’ skills, such as positive parent-child interactions and emotional communication (Kaminski et al., 2008). A meta-analysis of parenting strategies for preventing and treating child behavior problems showed that positive reinforcement and nonviolent discipline techniques (e.g., applying logical consequences) reduced disruptive child behavior (Leijten et., 2019). Parenting intervention programs with video feedback strategy have shown a cumulative effect on parenting and child development over the last 70 years of research on the theoretical frameworks of attachment, psychoanalytic, and social learning theories (Fukkink, 2008). The interventions were planned, on the one hand, for parents’ interactive behaviors and sensitivity training based on a pedagogical approach (Juffer et al., 2017, 2018) and, on the other hand, for parental behaviors and attitude based on psychotherapy purposes (Fukkink, 2008; Steele et al., 2014). Parents record videos interacting with their children and later are invited to watch and reflect on their interaction observed in the video with guidance (Balldin et al., 2018). Video feedback intervention promotes sensitive parenting and positive discipline with firm limits (Juffer et al., 2017), even in six short-term intervention sessions (Juffer et al., 2018). A parenting program adopted an efficient coaching strategy to strengthen familial interactions, focusing on parents’ emotional regulation (Lunkenheimer et al., 2007). The video coaching strategy effectively promotes emotional regulation, responsiveness, and attachment in young mothers of infants (Crugnola et al., 2018) and enhances maternal sensitivity and less intrusiveness (Alvarenga et al., 2020). Some programs include a video feedback strategy using recorded videos analyzed by experts to offer positive parenting orientations and strengthen parent-child positive interactions, discipline with sensitivity, attachment, and child development (Fisher et al., 2016; Juffer et al., 2017; Moss et al., 2018). The video feedback strategy allows mothers to self-observe their behaviors, increasing the generalization of learning for new and similar situations (Steele et al., 2014). Parent awareness has been shown to provoke self-confidence impacting parenting behavior, with the feeling of “this is going the right way” (Roggman et al., 2008). It is important to note that the literature uses both the terms “video coaching” and “video feedback,” but there is no distinction between these strategies in the interventions. Parenting programs have been delivered individually, in groups, and self-directed online (Sanders et al., 2019). Technology-based parenting interventions have successfully improved parenting outcomes, such as parent knowledge, behavior, and self-efficacy (Corralejo & Rodríguez, 2018), and parenting knowledge and observed language-supportive parenting behaviors with positive change in an infant’s language behaviors (Feil et al., 2020). Self-administered approaches (e.g., interactive online programs, mobile phones, or tablet-based apps) allow parents more flexibility (Corralejo & Rodríguez, 2018), significantly increase the potential reach of parenting interventions, and reduce delivery costs and logistical barriers to program access (Corralejo & Rodríguez, 2018; Sanders et al., 2019). Intervention strategies for remote delivery include the use of mobile phones, video calls, and smartphone apps (Harris et al., 2020) and mothers of children with neurodevelopmental problems sending videos to a therapist and receiving messages in response (Stockwell et al., 2019). Mobile phones are a beneficial and inexpensive technology in a parenting intervention program to improve communication with high-risk families, reduce child behavior problems, maternal stress, and depression (Carta et al., 2013). As highlighted in the meta-analysis of Fukkink (2008), interventions with video feedback previously demonstrated that parents were more skilled in interacting with their children and had more positive perceptions of young children’s families, showing equal effectiveness in behavioral-oriented and psychotherapeutic programs. Besides, according to Van Ijzerdoorn and Bakermans-Kranenburg (2017), evidence-based parenting interventions are still relatively scarce. Then, video feedback is an effective strategy for improving parenting and child outcomes, but there was a modest use of this remote format in the studies. Despite advances in technology-based delivery of parenting programs, to the best of our knowledge, there are no programs analyzed in the literature that have used animated videos, that give examples of positive parenting, and that explain essential concepts of mother-child interactions, combined with individualized video-recording of mothers interacting with their children. Moreover, studies on video feedback programs predominantly had assessed mother-child interaction outcomes and no other parenting dimensions, such as parenting practices and parental self-perception of mothers. Also, despite numerous randomized controlled trials of parenting interventions in low- and medium-income countries (Jeong et al., 2020; Knerr et al., 2013), there is a lack of studies designed for parenting programs involving any type of digital delivery. In this sense, there is a scarcity of evidence-based and well-established parenting programs to be implemented at population level on a large sustainable scale. The scope of the current study was about the central strategy of remote video feedback to deliver contents about positive parenting. Then, the present study aimed to: (i) examine the efficacy of the Strengthening Bonds program, which is an innovative, remote, personalized video feedback universal program to develop and strengthen positive parenting and to reduce child behavior problems; (ii) examine the direct and indirect effects of the intervention in a single model pathway, aiming to understand better the mechanisms of “how” the Strengthening Bonds intervention affects parenting and child behavior outcomes. The present study proposed to perform a confirmatory analysis of a previous pilot study (Linhares, Altafim, Gaspardo, & Oliveira, 2019). The first hypothesis was that the Strengthening Bonds program will improve parenting by enhancing mothers’ positive interactive behavior, parenting practices, and parental sense of competence. The second hypothesis was that the Strengthening Bonds program will decrease child behavior problems. The third hypothesis was that the Strengthening Bonds program will improve mothers’ positive parenting, which, in turn, will act as a mediation effect reducing child behavior outcomes. This study has been reported following the CONSORT statement (Moher et al., 2010) that offers guidance for the transparent reporting of randomized controlled studies. The current study compiled 31 items of 37 items of the CONSORT statement, and six were not applicable for this RCT study. Study Design We conducted an RCT with a waiting-list control group and blinded assessment analysis of the video records [RCT register number, RBR-2mgzhvz]. Ethical Aspects This study was approved by the Ethical Board of Hospital of Clinics of the Ribeirão Preto Medical School of the University of São Paulo before data collection. Sample The sample comprised 92 adult mothers and their 2-to-6-year-old children of both genders from families living in a city in the Southeast of Brazil (low-to medium-income country) that were randomly allocated into two groups: an intervention group (IG, n = 50) and a waiting list control group (CG, n = 42). The random allocation sequence and assignment of participants to intervention and control groups were performed by the second author of the study using a web-based randomization strategy (htpp://www.randomizer.org). The randomization aimed at assigning mothers to the IG considered a minimum of two mothers in blocks, stratified by sites. The eligible participants were recruited from public schools (three sites) and family health centers (two sites). The following three ways recruited the eligible participants in the schools: invitation of mothers during meetings for parents; consultation of the lists of children who attended the inclusion criteria of the study; and sending messages via school schedules of children. In the family health center, the recruitment of eligible participants was performed using the records of the families of the community area covered by this center. The sample size was estimated to compare the means between two samples (IG vs. CG), considering a 5% probability of type-I errors (α = 5%) and a 20% probability of type-II errors (b = 80%), with a two-point difference in parenting practice scores (ACT Raising Safe Kids Evaluation Questionnaire communication scale), estimated from the data of a previous RCT study (Altafim & Linhares, 2019). In this previous RCT parenting study, the final sample comprised 81 mothers. The estimated sample of the present study was 31 mothers, in each group, with at least 62 mothers. The inclusion criteria were primary female caregivers of children who might be biological mothers or had legal custody of 2-to-6-year-old children. The exclusion criteria were the following: children with disabling mental or physical illnesses; mothers with apparent cognitive impairment, which would lead to an impaired understanding of assessment instructions; and mothers who participated in some other type of specific intervention program aimed at strengthening mother-child interactions or parenting practices. Figure 1 shows the flowchart of the study sample composition. Figure 1 Flowchart of the Sample 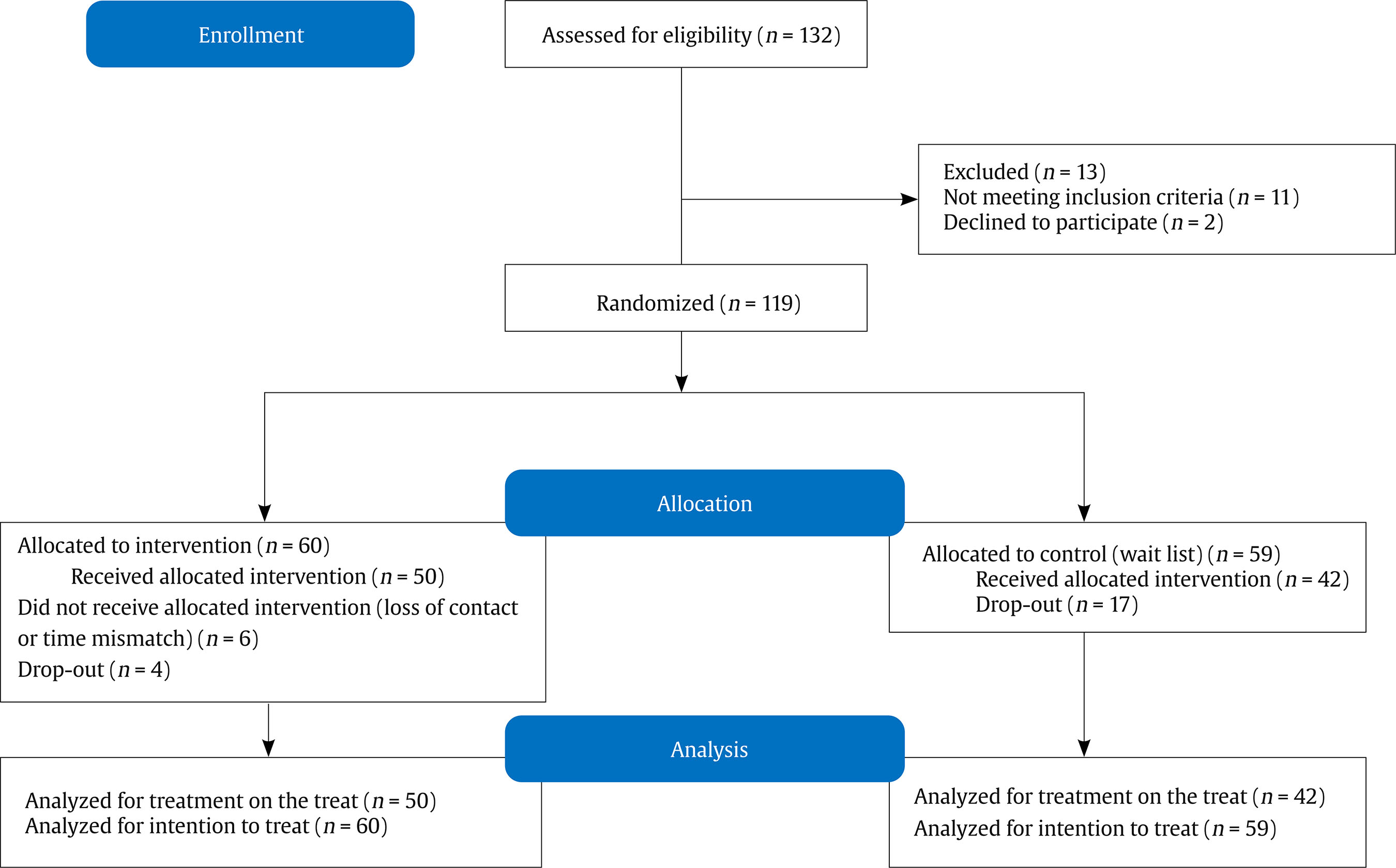 The initial sample of 132 mothers of 2 to 6-year-old children was assessed for eligibility criteria. Eleven mothers did not meet the inclusion criteria and two mothers declined to participate in the study. Then, 119 mothers were randomized into two groups (randomization in blocks of each site), allocating 60 mothers in the IG and 59 in the CG. Six mothers did not complete the intervention in the IG, and four mothers dropped out of the study, leaving 50 mothers. In the CG, in turn, 17 mothers dropped out of the study in the waiting period. The comparison between the sample in the study (in-sample, n = 92) and the sample out of the study (out-sample, n = 27) showed no statistically significant differences in the main sociodemographic variables, including children’s age (in-sample, mean = 3.39 years; out-sample, mean = 3.04 years; p = .15), children’s gender (in-sample, girls = 51%; out-sample, girls = 33%; p = .13), mother’s age (in-sample, mean = 32.42 years; out-sample mean = 31.44 years; p = .52), maternal schooling (in-sample, mean = 12.35 years; out-sample, mean = 11.96 years, p = .41), and socioeconomic level (in-sample, low = 65%; out-sample, low = 65%; p = 1.00). Instruments and Measures The parenting variables (maternal interactive behavior, parenting practices, and parental sense of competence) were the primary outcomes of the study, and the child behavior was the secondary one. Observational assessment of maternal interactive behavior. An expert researcher trained two observer research assistants to apply an observational coding system to analyze maternal interactive behavior. Parenting interactions with children: Checklist of observations linked to outcomes (PICCOLO; Roggman et al., 2013). This tool measures parenting interactions in an observational situation, focusing on four domains: affection, responsiveness, encouragement, and teaching. The total score indicates the maternal global interactive skill, ranging from 0 to 58 points. Higher scores indicate more positive maternal interactive behaviors with their children. In the PICCOLO scale, the manual’s recommendations were also followed, with training in 10 dyads different from the sample study (Roggman et al., 2013). Reliability tests (kappa coefficient) were performed aimed at evaluating the inter-rater agreement, with the following results: affection (91.50%, κ = .83), responsiveness (91.10%, κ = .83), encouragement (85.7%, κ = .72), and teaching (88.25%, κ = .76). Maternal report questionnaire of parenting outcomes Parenting and Family Adjustment Scale (PAFAS; Sanders et al., 2014; Santana, 2018). This tool evaluates the parenting practices and adjustment of the caregiver and family. In the present study, we used the parenting scale (parent-child relationship, positive encouragement, parental inconsistency, and coercive parenting subscales) exclusively. The total scores of the parental inconsistency and positive encouragement subscales range from 0 to 9, and the coercive parenting and parent-child relationship subscales range from 0 to 12. The higher the score, the better the parenting practices, except parental inconsistency and coercive parenting, for which the opposite holds. Parental Sense of Competence Scale (PSOC; Gibaud-Wallston & Wandersman, 1978; Ohan et al., 2000). This tool measures the beliefs, values, and skills perceived by mothers about “being a mother.” The total score ranges from 17 to 68 points; the higher the score, the higher the sense of parental competence. Maternal report questionnaires of child behavior outcome Strengths and Difficulties Questionnaire (SDQ; Fleitlich et al., 2000; Goodman, 1997). The SDQ is a screening tool for total behavioral problems (0-40 score), specifically internalizing problems (emotional symptoms and relationship problems) and externalizing problems (conduct problems and hyperactivity). The higher the total score, the greater the indication of behavioral problems. Maternal report questionnaires of sociodemographic variables Sociodemographic questionnaire (developed by the authors). Information about children’s age, gender, racial designation, mother’s age, racial designation, and schooling. Criteria for Economic Classification of Brazil. Association of Market Research Companies (CECB; Associação Brasileira de Empresas de Pesquisa, 2014). Assessment of the socioeconomic level of the families was based on an ordinal scale that represents very low (D/E), low (C), medium (B), and high (A) levels. The score range is from 0 to 46. Procedure Intervention: The Strengthening Bonds Program [“Fortalecendo laços”]. Strengthening Bonds is a personalized remote video feedback universal preventive parenting program to develop and strengthen positive parenting and reduce child behavior problems. The program has an implementation guide with the main steps of the program to aim to guarantee its fidelity. In Step 1, a systematic observational session in which the facilitator recorded a 10-min video of each mother playing with their children in two different situations: free-play and structured-play situations. In Step 2, after the dyadic observational session, a group of mothers (maximum of 10) was formed to participate in one 90-min structured face-to-face session. In this one, the facilitator explained the concepts of parenting, child development, and positive interactions to the mothers and clarified how they could avoid negative interactions with their children. The concepts addressed in the session included explanations about parenting, the negative impact of child maltreatment and coercive practices, and positive (responsiveness, reciprocity, and adaptive directivity) and intrusive interactions, illustrated with mock videos, facilitator explanations, group activities, and role play. In Step 3, the personalized video feedback was customized for each mother using the video records of the mother-child interactions by a team of three editors using the iMovie software in the laboratory. In this process, six videos were edited, including two mixed parts, as the following: (i) animated part with characters explaining the positive dimensions of mother-child interactions, that is standard for all the mothers; (ii) individualized tailored videos, including clips of the video record with positive feedback messages presented through subtitles and emojis. The personalized video feedback focused on responsiveness, reciprocity, and adaptive directivity dimensions of mother-child interactions. Each dimension had two videos summing the six videos. Also, the subtitles were chosen by the editors from a predefined list of potential subtitles, which was recommended in the implementation guide of the program. In Step 4, the edited videos were uploaded to YouTube using the unlisted option. Each mother received the six personalized videos edited with positive feedback via WhatsApp (each per week). During these six weeks, the facilitators contacted the mothers, interacting with them via WhatsApp messages to ensure that they watched the videos and obtained their spontaneous opinions and comments about the program. Also, statistics provided by YouTube were used to monitor whether the videos had been watched. The Strengthening Bonds program constitutes a short intervention to improve parenting outcomes through a responsiveness and supportiveness approach using remote video feedback via WhatsApp. The intervention recognizes and encourages mothers’ responsive interactions, identifying the parents’ everyday activities with their children and encouraging them to use those interactions to support their development. The emphasis on maternal responsiveness, reciprocity, and adaptive directivity strengthens parental practices and beliefs, observing and offering contingent comments using subtitles and emojis in personalized videos. The individualized, tailored edited videos follow the “feedforward strategy,” proposed by Dowrick (1999) and adopted by Smith et al. (2013), in which positive behaviors are reinforced, in contrast to pointing out ineffective parenting behaviors. Data Collection First, the family health centers’ and schools’ staff participated in one in-person sensitization session, mediated by the program’s facilitators (two psychologists), to discuss the principal dimensions and examples of mother-child interactions. Second, the mothers were invited to participate in the study and, after they signed the informed consent, the first in-person group session of mothers was scheduled. In this session, the pre-intervention assessment was performed to collect the maternal report measures (PSOC, ACT, PAFAS, and SDQ). In the SDQ evaluation, if the mother had more than one child, she had to choose the child to worry about her/his behavior. Third, an observational 10-min session was performed to video record the mother-child interactions using a tablet, equally divided into free-play situations (i.e., toys, such as little animals, cooking toys, and building blocks) and structured situations (i.e., puzzles). The recorded video was used to baseline evaluation of the maternal interactive behavior (pre-intervention assessment). Finally, the post-intervention assessment was performed. This evaluation comprised a second observational session of mother-child interactions (free- and structured-play situations) and the maternal report in the same questionnaires used in the pre-intervention assessment. It is important to highlight that the video recording of the mother-child interaction session was used to evaluate the maternal interactive behavior and select clips of it for edition the personalized videos of intervention. Both groups were assessed using the same procedures in two different moments, as the following: in the intervention group, pre-and post-intervention period, and the control group, pre- and post-waiting period. After the waiting period, the control group also received the same intervention program, which was previously done with the intervention group. This is ethical care in RCT- waiting list control group design. All data collection was performed by three research assistants (psychologists), who were previously trained in all instruments for the assessments. The three expert principal developer-researchers supervised and coordinated the training and data collection (first, second, and fourth authors). The data collection of the present study was carried out from April 2019 to June 2020. Despite the emergence of the COVID-19 pandemic in 2020, all the interventions (face-to-face group sessions and six remote video feedbacks) and the majority of the post-intervention assessment were performed, leaving 22 of the 92 mothers to be assessed during the period of social isolation due to the pandemic context. Of these 22 mothers, all answered the self-reported questionnaires, and ten mothers sent the videos to the facilitator via mobile phone. However, we did not receive videos from 12 of these 22 mothers (55%). There were no significant statistical differences between the groups of mothers who sent the videos (in-group) and the group of mothers who did not (out-group) in the main sociodemographic variables (mother’s age: in-group mean = 32.54 years, out-group mean = 32.09 years, p = 0.80; maternal schooling: in-group mean = 12.45 years, out-group mean = 12.04 years, p = .41; socioeconomic level: in-group low = 62%, out-group low = 74%, p = .32; children’s age: in-group mean = 3.38 years, out-group mean = 3.43 years, p = .78; children’s gender: in-group boys = 52%, out-group boys = 39%, p = .34. Data Analysis The observational data of maternal interactive behavior was coded using all the coding systems by two expert researchers, who were blinded for the moment of assessment (pre-intervention and post-intervention) and groups (IG and CG). The third author coordinated the coding analysis. The dataset was organized and double-checked. First, statistical descriptive data analysis was performed, using mean and standard deviation for continuous variables and percentages for categorical variables. Second, between-group comparisons were performed to examine the sociodemographic characteristics (IG vs. CG; in-sample vs. out-sample) and the outcome variables at baseline (pre-intervention assessment), using Student’s t-test for continuous variables and chi-square for categorical variables. Third, the generalized estimating equation (GEE) was used to test the first and second hypotheses, analyzing the estimated parameters of a generalized linear model with the possible unknown correlation between outcomes. The GEE was conducted with the intention-to-treat (ITT) strategy, including all randomized participants with dropouts (n = 119). Subsequently, we performed the analysis including only the participants who completed the intervention and assessments (n = 92), the treatment-on-the-treated (TOT) strategy. The study of Fidler et al. (2008) recommended that both analyses have to be performed, considering that the ITT explains whether the intervention made a difference and the TOT explains what the effects were likely to be if the mothers had been exposed to the intervention. Assuming an exchangeable correlation structure, the GEE was performed to examine mean differences between groups in continuous variables of parenting outcomes (parenting practices, parental sense of competence, maternal interactive behavior) and child behaviors over two-time (pre-and post-intervention). Initially, the time was entered as a continuous covariate in all models, and subsequently, we examined the adjusted models for socioeconomic status and mother’s schooling. Standardized effect sizes (Cohen’s d) were calculated using marginal means from endpoint assessments of all outcomes (insignificant effect < 0.19, small effect = 0.20-0.49, medium effect = 0.50-0.79, large effect = 0.80-1.29). Table 1 Sociodemographic Characteristics of the Sample 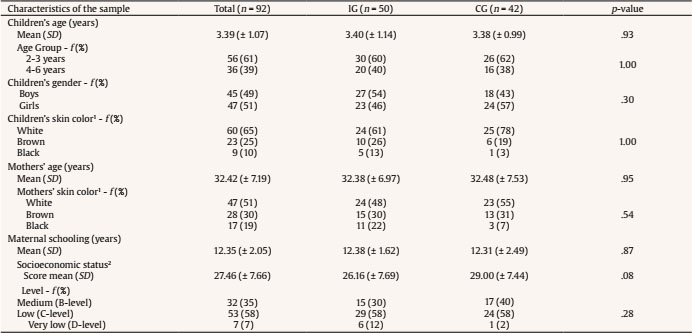 Note. SD = standard deviation; f = frequency; % = percentage. IG = intervention group; CG = control group. 1Brazilian classification of race, according to the Brazilian Institute of Geography and Statistics, IBGE, https://www.ib ge.gov.br/en/institutional/the-ibge.html . 2Criteria for economic classification of Brazil. Association of Market Research Companies (CECB). The score range is from 0 to 46. Assessment of the socioeconomic level of the families was based on an ordinal scale that represents very low (D/E), low (C), medium (B), and high (A) levels; in the between-group comparison, we analyzed B level vs. C plus D levels. Finally, we performed a structural equation model (SEM) to test the second hypothesis, examining the direct and indirect effects in a single model pathway, aiming to better understand the mechanisms of how the intervention affects parenting outcomes and child behavior. In the SEM, we included the IG as the predictor, parenting (post-intervention) as mediators, and child behavior problems (post-intervention) as outcomes. Child sex was used as a control variable to predict child behavior problems. Error covariances between the mediators and between the outcomes were also included. The pathway was considered statistically significant at p < .05. In keeping with field standards, we reported the p of the unstandardized coefficient. The pathways were considered statistically significant at p < .05. We considered model fit to be adequate based on the root mean square error of approximation (RMSEA) of ≤ .06, comparative fit index (CFI) of ≥ .95, and standardized root mean square residual (SRMR) of ≤ .08 (Hu & Bentler, 1999). All analyses of the study were conducted using STATA software (14.1 version). The significance level adopted in the study was 5%. Sociodemographic Characteristics of the Sample Table 1 shows the main sociodemographic characteristics of the IG and CG groups. There were no statistically significant differences between the two groups for mothers’ and children’s characteristics. In both groups, children’s mean age was three years, predominantly between 2 and 3 years. In both groups, the mothers were young adults with 12 years of schooling, on average. In both groups, the children’s and mother’s racial designation was primarily white, and families’ socioeconomic level was predominantly low income. Descriptive Data of the Main Outcomes Table 2 presents the descriptive data (mean and standard deviation) of the primary outcomes (maternal interactive behavior, maternal parenting practices, and parental sense of competence) and secondary outcome (child behavior) at the baseline (pre-intervention assessment). There were no statistically significant differences between-group comparisons for all outcomes at baseline; then, both groups are similar at the beginning of the RCT study. Table 2 Descriptive Data of the Parenting and Child Behavior Outcomes at Baseline (pre-intervention assessment) 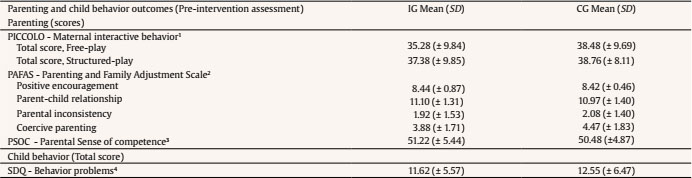 Note. IG = intervention group; CG = control group; SD = standard deviation; 1PICCOLO = Parenting Interactions with Children: Checklist of Observations Linked to Outcomes (range 0-58); 2PAFAS = Positive Encouragement and Parental Inconsistency (range 0-9), and Parent-child Relationship and Coercive Parenting (range 0-12); 3PSOC (range 17-68); 4SDQ = Strengths and Difficulties Questionnaire (range 0-40); 1IG (n = 50) / CG (n = 42); 2IG (n = 48) / CG (n = 38). There were no statistically significant differences between groups in all the outcomes. Strengthening Bonds Program’s Efficacy Findings First, considering the intention-to-treat GEE analysis, which included the 27 dropout participants in the entire sample analysis (n = 119), there were no statistical differences between groups in parenting behavior outcomes (parental practices, maternal interactive behavior, maternal sense of competence) and child behaviors outcomes. Second, Table 3 presents the treatment-on-the-treated GEE analysis, including the 92 participants who completed the study with the intervention and assessments concluded. In the treatment-on-the-treated, there were statistically significant effects of the intervention for decreasing mothers’ coercive parenting practices (d = -0.54, medium effect size) and child behavior problems (d = -0.43, small effect size), when adjusting for socioeconomic status and mother’s years of schooling. The treatment-on-the-treated without the adjustment showed a decrease only for mothers’ coercive parenting practices. Additionally, there were no statistically significant effects of the intervention on the other mothers’ parenting practices (parent-child relationship, positive encouragement, parental inconsistency, parental sense of competence, and maternal interactive behavior). Table 3 Strengthening Bonds Program’s Effects on Parenting and Child Behavior Outcomes (GEE Analysis) 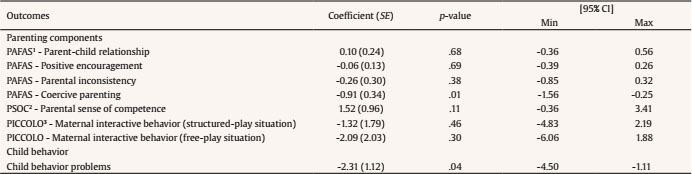 Note. min = minimum; max = maximum; SE = standard error. 1PAFAS = Parenting and Family Adjustment Scales; 2PSOC = Parenting Sense of Competence Scale; 3PICCOLO = Parenting Interactions with Children: Checklist of Observations Linked to Outcomes. Results adjusted for socioeconomic status score and mothers’ years of schooling. Third, Table 4 shows, in the treatment-on-the-treated GEE analysis, the marginal means and standard error of the primary outcomes (maternal interactive behavior, maternal parenting practices, and parental sense of competence) and secondary outcome (child behavior), the IG and CG in pre- and post-intervention assessments. Table 4 Parenting and Child Behavior Outcomes of the IG and CG, in the Pre-and Post-intervention Assessments (Marginal Means and Standard Errors of GEE Analysis) 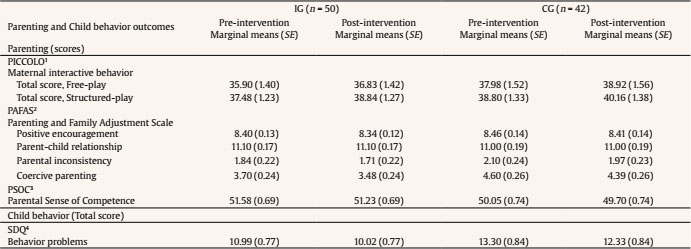 Note. IG = intervention group; CG = control group; SE = standard error; 1PICCOLO = Parenting Interactions with Children: Checklist of Observations Linked to Outcomes (range 0-58); 2PAFAS, Positive Encouragement and Parental Inconsistency (range 0-9), and Parent-child Relationship and Coercive Parenting (range 0-12); 3PSOC (range 17-68); 4SDQ = Strengths and Difficulties Questionnaire (range 0-40). GEE analysis adjusted by socioeconomic level and maternal schooling. Strengthening Bonds Program’s Mediation Model (Table 5) Table 5 Strengthening Bonds Program’s Mediation Model (SEM Analysis, direct effects)  Note. SE = standard error. *p ≤ .05, **p ≤ .01. The results of the SEM model revealed adequate overall model fit, RMSEA < .001, SRMR = .011, CFI = 1.00, χ2(2) = 0.242, and χ2/df = 0.121. Within this model, several significant direct pathways were found (Figure 2 and Table 5). The paths from the IG to mothers’ coercive parenting practices and sense of competence were statistically significant, suggesting that the IG presented a higher maternal sense of competence and fewer coercive practices. The path from coercive practice to children’s behavior problems was significant and positive, showing that children of mothers who reported less coercive practices presented fewer behavior problems. The indirect effect of the intervention on children’s behavior problems through coercive practices was confirmed (b = -1.21, SE = 0.57, p = .03). Figure 2 Strengthening Bonds Program’s Mediation Model (SEM Analysis). 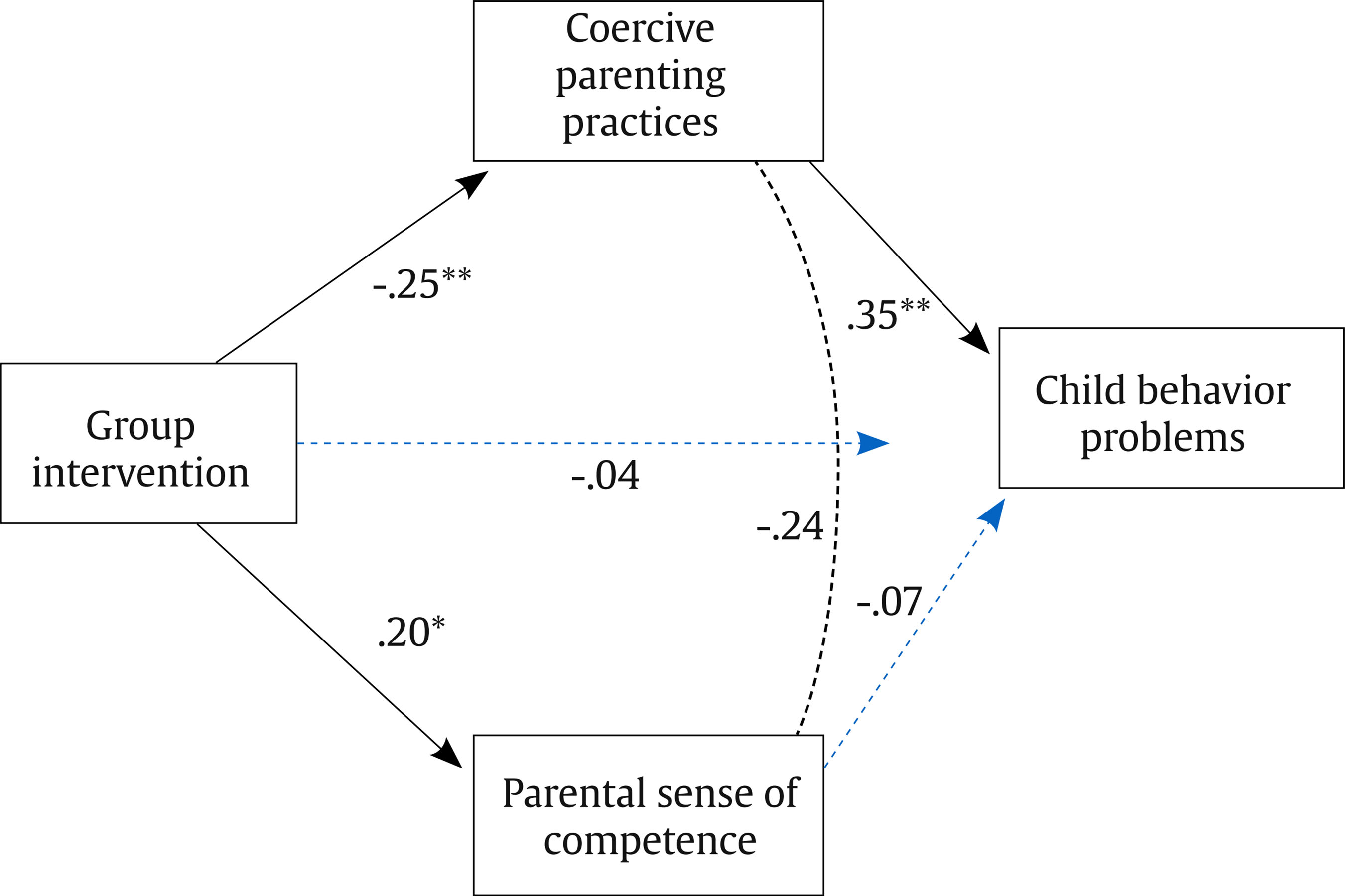 Note. Black lines represent significant pathways, dashed lines indicate significant correlation, and gray lines indicate non-significant pathways. All path coefficients are standardized (direct effects). *p < .05, **p < .01. Initially, it is important to highlight that the present study showed a high adherence rate, specifically in the intervention group (83%), encouraging the application of the Strengthening Bonds program. This rate is higher than a previous study (66%) with a face-to-face group parenting program with a similar sample (Altafim & Linhares, 2019). Therefore, our finding corroborates the literature that emphasizes that self-administered and technology approaches are more flexible and increase parenting interventions’ potential reach (Corralejo & Rodríguez, 2018; Sanders et al., 2019). The Strengthening Bonds adopted a hybrid methodology (one face-to-face meeting and six videos and messages sent via smartphone), allows the mothers to participate by themselves anytime, and share the videos with other family members. Regarding answering the hypothesis of the present study, firstly, we performed the intention-to-treat analysis, including all the participants to impute data of the dropout in the generalized estimating equation. As pointed out by Gupta (2011), this analysis maintains prognostic balance generated from the original random treatment allocation, estimating the treatment effect in a generally conservative way. The findings of the ITT analysis did not show statistically significant results, revealing any effects of the program when considering all the participants of the initial sample. It is important to note that the intention-to-treat analysis might suggest that an intervention does not affect, while in reality the intervention can be effective in participants who fully adhered to the study protocol (Tripepi et al., 2020). While the intention-to-treat analysis maintains comparability of participants in the different groups generated from the original random treatment allocation, in the per-protocol analysis it is not possible to distinguish whether the intervention effect is due solely to adherence or due to the characteristics of compliant participants (Tripepi et al., 2020). Then, the treatment-on-the-treated analysis includes the per-protocol population, which is defined as a subset of the intention-to-treat population who completed the study without any major protocol violations (Gupta, 2011). In this case, it is recommended a complementary method can be used to investigate the effect of the intervention on those participants who completed the trial (Tripepi et al., 2020). Then, in the present study, besides the intention-to-treat analysis, we also performed the treatment-on-the-treated one. We considered that it is an important decision based on the controversies identified in the literature. Although the controversy about whether to use an intention-to-treat or a per-protocol approach has subsided mainly in favor of support for the first one, there is still considerable ambiguity about the intention-to-treat analysis. As pointed out by Polit and Gillespie (2010), the advocacy of intention-to-treat analysis highlights that not removing the non-compliant participants to maintain the balance of randomization is relevant to guarantee methodological care. However, opponents of intention-to-treat analysis argued that it is not sensible to include in the intervention group people who did not receive the intervention, affirming that the per-protocol analysis would test the true efficacy of the intervention. The intention-to-treat analysis answers the question “What is the effect of assigning an intervention to a group of participants?”. In a complementary way, the treatment-on-the-treated analysis considers only patients who strictly adhere to the protocol and completed the intervention, providing an answer to the following question: “What is the effect of receiving an intervention in a group of participants who finished the trial?” (Tripepi et al., 2020). In the present study, differently from the null findings of the intention-to-treat analysis, the treatment-on-the-treated analysis showed statistically significant results of the effects of the program on strengthening positive parenting behaviors and beliefs and reducing child behavior problems. Then, we found promising findings in the treatment-on-the-treated analysis of cases that effectively participated in the program. There were main effects of the short-term remote personalized video feedback parenting program (Strengthening Bonds) on reducing maternal negative parenting practices and child behavior problems. Interestingly, the first hypothesis was confirmed regarding the Strengthening Bonds program’s direct effect on some parenting outcomes examined. We detected lower mothers’ coercive practices and children’s behavior problems in the intervention group, in this case, adjusted for socioeconomic level and mother’s years of schooling. The first hypothesis was then confirmed exclusively for negative parental discipline practices, not for positive ones. There were no effects of the Strengthening Bonds program intervention on other mothers’ parenting practices in the generalized estimating equation analysis. Investment in positive parenting practices constitutes a great accomplishment of preventive intervention programs in early childhood development, especially when reducing negative parenting practices, as demonstrated in the present study. Together with reasonable levels of control, parental warmth combines to produce positive child outcomes (Grusec & Danyliuk, 2014). Coercive parenting and abusive parenting are negative qualities associated with extraversion temperament, physical and emotional abuse, hostility, rejection, and punitive discipline (Gölcük & Berument, 2019). Coercive, harsh, and authoritarian discipline overlapped, showing intrusiveness, restrictiveness, and strict obedience (Gölcük & Berument, 2019). Coercion and related risks have been associated with both rigidity (low variability) and inconsistency (high variability) in parenting and dyadic behavior, requiring the cycle of coercion to be broken (Lunkenheimer et al., 2016). Then, the cyclical relation between harsh or coercive parenting that provokes child behavior problems could break through positive parenting practice interventions during early childhood (Sitnick et al., 2015). Therefore, the Strengthening Bonds program could act as a protective factor by decreasing coercive practices and strengthening positive mother-child interactions. Unexpectedly, we found no impact on mothers’ interactive behaviors. However, it is important to highlight that considering the interactive behavior pattern exhibited in the pre-intervention assessment, mothers presented a high-positive interaction pattern with their 2-6-year-old children, examined through the PICCOLO assessment. This absence of changes could be explained as follows: at baseline, mothers presented positive interactive behaviors in both groups and observational situations (free- and structured-play), exhibiting a high profile of positive interactions. Consequently, the first hypothesis was partially confirmed due to the “ceiling effect” in both groups at the start- and end-time points, which is not conducive to changes. In the ceiling effect, most values obtained for a variable approach the upper limit of the scale with slight variance. Thus, in our study, the effect of the intervention on maternal interactive behavior did not show significant results of between- and within-group comparisons because there was no variability in the data. Another explanation for this absence of changes in maternal interactive behaviors could be attributed to the positive characteristics of the sample study, as mothers had a medium educational level and a low rate of child behavior problems. Maternal years of education represent a relevant socioeconomic status variable that positively impacts responsive caregivers of 2-year-old children (Scherer et al., 2019). Also, a multicultural study revealed that the more prosocial behaviors of school-age children, the more reciprocal parental relationships with warmth and involvement (Pastorelli et al., 2016). These characteristics could be personal protective factors that facilitated positive interactive behavior in our sample study at the baseline. Regarding the second hypothesis, the Strengthening Bonds program directly affected decreasing child behavior problems but not increasing prosocial behavior. It is important to note that this behavior presented a high score in the pre-intervention assessment in both groups, indicating the ceiling effect’s presence. Behavior problems in early childhood, such as oppositional and aggressive behavior at 2-5 years, is a robust predictor of school-age children’s behavior problems, such as to conduct problems at 7.5-8.5 years (Smith et al., 2014). A child’s negative behaviors have been linked with coercive parent-child interactions (Lunkenheimer et al., 2016). Then, optimal strategies must be implemented to reduce coercion in a child’s trajectory to prevent undesirable future maladaptation. In the present study, investment in reinforcing responsive, reciprocal, and interactive directive behavior of mothers with their children, using the remote video feedback strategy, positively impacted child behavior contributing to protection against coercive parent-child interactions. Our finding is similar to a previous intervention using a face-to-face video feedback strategy focused on parents’ sensitive and firm discipline in target at-risk parents and vulnerable 0-6-year-old children (Juffer et al., 2017). The mechanism of reducing coercive parenting and child behavior problems could be explained by better maternal emotional and cognitive control regulation processes (Crandall et al., 2015). Finally, the third hypothesis fully confirmed that there are mediational effects that support a better understanding of the mechanism of Strengthening Bonds program’s impacts on parenting and behavior outcomes. The program showed direct effects of improving mothers’ sense of competence and decreasing coercive parenting practices. In turn, this maternal negative practice reduced children’s behavior problems. Therefore, on the one hand, the program showed a direct impact on mothers’ beliefs about their parental role related to self-confidence in their performance. On the other hand, coercive practices mediated the impact of the intervention on total child behavior problems. Interestingly, the mechanism detected in our study was similar to a previous study of a family-centered short intervention (three sessions) individually tailored and supported by multi-informants, which was delivered at home (Sitnick et al., 2015). In this study, positive parent engagement affected the reduction of coercive negative parenting, which, in turn, reduced child behavior problems at an early age. The undesirable coercive control practices of authoritarian parents were related to more negative parent-child relationship indicators than was the extensive use of firm and confronting control (rationally demanding) by directive parents or authoritative parents later in adolescence (Sorkhabi & Middaugh, 2014). The present findings are similar to the findings of a previous study on a face-to-face parenting group program that showed reductions in children’s internalizing and externalizing behavior problems mediated by parenting improvements (Altafim et al., 2021). Then, the parenting practice of mothers’ emotional and behavioral regulation was the intervention core mechanism that also includes coercive parenting. The Strengthening Bonds program’s primary emphasis is on reinforcing responsive and reciprocal parenting of mothers acting to enhance the self-perceptions of positive aspects and, inversely, to reduce demanding, coercive, and authoritarian parenting. Then, we move beyond the central question of “Does the program work?” to “How does the program work?” and analyze the mechanisms of the effect of multiple variables taken together. The developmental parenting intervention proposed by Roggman et al. (2008) highlighted that when mothers felt secure, valued, and satisfied they recognized their source of competence and their role with their children. The findings of the present study showed an impact on “overt” parenting practices as well as the sense of competence, which is a “covert” belief and feeling schema. Our results are similar to the previous findings of the impact of the Home-Start program, which enhanced maternal sense of competence, and, in turn, increased supportive parenting and decreased negative discipline (inconsistency, negative control, and harsh parenting) (Dekovi et al., 2010). The parental sense of competence could explain the mechanisms of changes and effects of preventive intervention programs. Dekovi et al. (2010) highlighted that when mothers are motivated, they are more persistent in attaining goals and more consistent in their interactive behavior with children. Finally, it is important to highlight some aspects of the key strategy of the Strengthening Bonds program. The personalized video feedback strategy of holding the mirror up for mothers could build their parental self-awareness and parenting representations in this innovative program. Also, the remote video feedback allowed the mothers to review by themselves, at any time they wanted to, and review the videos with their child and other family members to share learning about positive interaction behaviors. As noted by Fukkink (2008), the remote video feedback strategy has an advantage over live-video feedback. The facilitators need to perform the slow motion and freezing image of the videos to give feedback about mother-child interactions. Furthermore, in the Strengthening Bonds program’s methodology, the dosage of six sessions seems sufficient to show positive effects on parenting outcomes, impacting the child’s behaviors. As pointed out by Bakermans-Kranenburg et al. (2003), less is more in parenting programs, based on the finding that fewer sessions were more effective than extensive treatments. In conclusion, the present study showed that the Strengthening Bonds intervention reduced maternal negative coercive practices and child behavior problems, in this case, adjusted for socioeconomic level and mother’s years of schooling. Also, examining the mechanisms of the intervention’s effect, we detected a direct effect for improving mothers’ sense of competence and decreasing coercive parenting practices. This practice mediated the reduction of children’s behavior problems. The strong aspect of the current study is the video feedback intervention based on mother-child interactions using innovative, edited, mixed-personalized, and animated videos sent quickly via WhatsApp to mothers. A great advance has been made in using this specific innovation via mobile phones, inexpensive technology for improving communication with mothers. Finally, this study added to the scientific literature findings of an RCT design parenting study that applied an innovative and original methodology. Also, we used generalized estimating equation analysis to manage missing data in the two longitudinal time points of the study. Despite the strengths of the present study, we also note some limitations. First, the recruitment of the sample study was interrupted by the COVID-19 pandemic, with a situation of social isolation and distancing, and school closures. There was also a negative impact on the final sample composition, which did not allow very socially vulnerable families. Second, there was a dropout of study participants, mainly in the waiting-list control group; however, no significant differences were detected in the in- and out-samples. Third, some videos of mother-child interaction observation session assessments were not obtained to compare pre-and post-intervention moments because of the barriers imposed by social isolation during the pandemic. However, a generalized estimating equation analysis was adopted to reduce missing data on the database. Finally, this study focused exclusively on mothers from one city in Brazil; therefore, new studies are necessary for other social-cultural contexts in order to generalize the findings. The present study has important implications for researchers and practitioners, suggesting that this innovative program is an effective remote strategy that impacts parenting and child behavior outcomes. Individually tailored interventions, including feedforward communication with mothers, could be a potential strategy for universal preventive parenting programs. The program is low-cost and uses inexpensive technology that facilitates sustainable large-scale implementation in public services. Strengthening Bonds is a flexible short-term intervention that could be easily incorporated in a “modular way” in other standard-care programs implemented in public services, such as home-visit programs to promote positive parenting and early child development. The concept of modularity was proposed in the design and application of therapeutic protocols because it offers numerous potential advantages in terms of efficiency (reusability of modules and ease of updating or reorganizing protocols) and effectiveness (e.g., greater adaptability for applied contexts) (Chorpita et al., 2005). The Strengthening Bonds program could assume a flexible combination with other packages of program modalities aimed at obtaining synergic effects to improve parenting and child development and behavior outcomes. Additionally, the innovation strategy of personalized videos could be easily adapted for mothers of other countries. Future studies with the Strengthening Bonds program intervention should clarify what the program precisely entails considering the highlights and recommendations previously found in the scientific literature. Future directions for parenting interventions studies with remote video feedback should explore multi-problem families, as highlighted by Fukkink (2008), for example, by focusing on parent level (e.g., maternal depression), child-level (e.g., behavior problems), and family level (e.g., familial cohesion relationship problems). Also, the Strengthening Bonds program could maintain the core remote video feedback strategy and adapt features of the materials to examine their effectiveness in improving parenting outcomes in the father-target population. Furthermore, to clearly understand more socially vulnerable families and target populations (e.g., maternal mental health symptoms, emotional and behavioral dysregulation, history of childhood adversities, and children with clinical behavior problems) they should be examined in future research using the Strengthening Bonds program. This would enable us to move beyond considering whether the program works to how it works and for whom it fits best, based on person- and place-based factors, as strongly recommended in the IDEAS impact framework of Frontiers of Innovation (see Center on the Developing Child https://developingchild.harvard.edu/innovation-application/innovation-approach/guiding-principles/xxxprecision). Future studies should design larger trials focusing more extensively on the moderator and mediation analysis in prospective-longitudinal design studies using the Strengthening Bonds program and several time-point assessments from a multifaceted developmental perspective. As noted by Smetana (2017), the role of parenting beliefs moderating links between parenting and child adjustment should be examined, allowing a more complex model analysis of the main mechanism processes. As highlighted by Gardner et al. (2010), the moderator and mediator variables should be considered in a parenting intervention’s effectiveness trial. Also, a component analysis of content and strategies of the program, as performed in the meta-analytic study of Kaminski et al. (2008), could be useful in future studies. Conflict of Interest The authors of this article declare no conflict of interest. Acknowledgments The authors want to thank all the mothers and children who took part in the present study. Cite this article as: Linhares, M. B. M., Altafim, E. R. P., Gaspardo, C. M., & de Oliveira, R. C. (2021). A personalized remote video-feedback universal parenting program: A randomized controlled trial. Psychosocial Intervention, 31(1), 21-32. https://doi.org/10.5093/pi2021a9 Funding: The Strengthening Bonds (RCT study) was supported by the Laboratory of Innovation for Early Childhood Development [I-Lab Primeira Infância], an initiative of the Center of Science for Early Childhood [Núcleo de Ciência pela Infância]. The funders had no role in the design and conduct of the study, collection, management, analysis and interpretation of the data, and preparation, review, or approval of the manuscript. |
Cite this article as: Linhares, M. B. M., Altafim, E. R. P., Gaspardo, C. M., & Oliveira, R. C. D. (2022). A Personalized Remote Video-Feedback Universal Parenting Program: A Randomized Controlled Trial. Psychosocial Intervention, 31(1), 21 - 32. https://doi.org/10.5093/pi2021a9
linhares@fmrp.usp.br Correspondence: linhares@fmrp.usp.br (M. B. M. Linhares).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
Send






