


Virtual Reality-based Cognitive Intervention for Enhancing Executive Functions in Community-dwelling Older Adults
[IntervenciĂłn cognitiva con realidad virtual para mejorar las funciones ejecutivas de las personas mayores que viven en la comunidad]
Pattrawadee Makmee and Peera Wongupparaj
Cognitive Science and Innovation Research Unit, College of Research Methodology and Cognitive Science, Burapha University, Thailand
https://doi.org/10.5093/pi2022a10
Received 4 February 2022, Accepted 22 April 2022
Abstract
With the rapid growth of the older population globally, it is anticipated that age-related cognitive decline in the prodromal phase and more severe pathological decline will increase. Moreover, currently, no effective treatment options for the disease exist. Thus, early and timely prevention actions are promising and prior strategies to preserve cognitive functions by preventing symptomatology from increasing the age-related deterioration of the functions in healthy older adults. This study aims to develop the virtual reality-based cognitive intervention for enhancing executive functions (EFs) and examine the EFs after training with the virtual reality-based cognitive intervention in community-dwelling older adults. Following inclusion/exclusion criteria, 60 community-dwelling older adults aged 60–69 years were involved in the study and randomly divided into passive control and experimental groups. Eight 60 min virtual reality-based cognitive intervention sessions were held twice a week and lasted for 1 month. The EFs (i.e., inhibition, updating, and shifting) of the participants were assessed by using standardized computerized tasks, i.e., Go/NoGo, forward and backward digit span, and Berg’s card sorting tasks. Additionally, a repeated-measure ANCOVA and effect sizes were applied to investigate the effects of the developed intervention. The virtual reality-based intervention significantly improved the EFs of older adults in the experimental group. Specifically, the magnitudes of enhancement were observed for inhibitory as indexed by the response time, F(1) = 6.95, p < .05, ηp2 = .11, updating as represented by the memory span, F(1) = 12.09, p < .01, ηp2 = .18, and the response time, F(1) = 4.46, p = .04, ηp2 = .07, and shifting abilities as indexed by the percentage of correct responses, F(1) = 5.30, p = .03, ηp2 = .09, respectively. The results indicated that the simultaneous combined cognitive-motor control as embedded in the virtual-based intervention is safe and effective in enhancing EFs in older adults without cognitive impairment. Nevertheless, further studies are required to investigate the benefits of these enhancements to motor functions and emotional aspects relating to daily living and the well-being of older populations in communities.
Resumen
Ante el rápido crecimiento de la población mayor a nivel mundial se prevé un aumento del deterioro cognitivo propio de la edad en la fase prodrómica y un mayor deterioro patológico. Además no hay en la actualidad opciones eficaces de tratamiento de la enfermedad. Por tanto, las medidas preventivas tempranas y puntuales suponen estrategias prometedoras para preservar las funciones cognitivas al evitar que la sintomatología aumente el deterioro de las funciones asociado a la edad de personas mayores sanas. El presente estudio tiene como obejetivo desarrollar una intervención cognitiva basada en la realidad virtual para mejorar las funciones ejecutivas (FE) y examinarlas tras el entrenamiento de intervención cognitiva con realidad virtual en personas mayores que viven en su domicilio. Teniendo en cuenta criterios de inclusión y exclusión se contó para el estudio con 60 personas mayores de entre 60 y 69 años que vivían en su domicilio, a los que se asignó aleatoriamente a un grupo de control pasivo y a un grupo experimental. Se realizaron ocho sesiones de 60 minutos de intervención cognitiva con realidad virtual dos veces por semana durante un mes. Las FE (i.e., la inhibición, actualización y cambio) de los participantes se evaluaron mediante tareas informatizadas estandarizadas, i.e., Go/NoGo, amplitud de dígitos hacia delante y hacia atrás y clasificación de cartas de Berg. Además, se utilizó un ANCOVA de medidas repetidas y el tamaño del efecto para medir el efecto de la intervención desarrollada. La intervención con realidad virtual mejoró significativamente las funciones ejecutivas de los mayores del grupo experimental. En concreto se observaron más mejoras en inhibición, reflejada en el tiempo de respuesta, F(1) = 6.95, p < .05, ηp2 = .11, actualización, representada por la amplitud de memoria, F(1) = 12.09, p < .01, ηp2 = .18, y el tiempo de respuesta, F(1) = 4.46, p = .04, ηp2 = .07, y las habilidades de cambio, como refleja el porcentaje de respuestas correctas, F(1) = 5.30, p = .03, ηp2 = .09, respectivamente. Los resultados indican que el control cognitivo-motor combinado simultáneamente, tal y como se aplica en la intervención virtual, es seguro y eficaz para conseguir aumentar las funciones ejecutivas de personas mayores sin deterioro cognitivo. No obstante, se necesitan más estudios para investigar los beneficios de estas mejoras en las funciones motoras y los aspectos emocionales de la vida cotidiana, así como el bienestar de las personas mayores que viven en la comunidad.
Keywords
Nonpharmacological cognitive, intervention, Inhibition, Shifting, Updating, A short-term interventionPalabras clave
IntervenciĂłn cognitiva no farmacolĂłgica, InhibiciĂłn, Cambio, ActualizaciĂłn, IntervenciĂłn a corto plazoCite this article as: Makmee, P. & Wongupparaj, P. (2022). Virtual Reality-based Cognitive Intervention for Enhancing Executive Functions in Community-dwelling Older Adults. Psychosocial Intervention, 31(3), 133 - 144. https://doi.org/10.5093/pi2022a10
peera.wo@go.buu.ac.th Correspondence: peera.wo@go.buu.ac.th (P. Wongupparaj).The proportion of older adults has been increasing in the majority of countries (Shetty, 2012; World Health Organization, 2021). The number of older adults outnumbered younger children in several countries, suggesting an increase in the pace of population aging (United Nations Report, 2019b; World Health Organization, 2021). Furthermore, the increase in the share of older adults aged over 60 years was projected to approximately double between 2015 and 2020 (12%-22%) (Livingston et al., 2020; World Health Organization, 2021). Additionally, improved and adequate access to healthcare systems is related to an increase in life expectancy at older ages (Hao et al., 2020; United Nations Report, 2019a). Nonetheless, with the rapid growth of the older population globally, it is anticipated that age-related cognitive decline in the prodromal phase (i.e., mild cognitive impairment) and more severe pathological decline will increase (i.e., dementia or Alzheimer’s disease) (Jia et al., 2020; Livingston et al., 2020; Nguyen et al., 2019b) due to increased risk and accessibility of cognitive screening tests for older adults (Thabtah et al., 2020; van Dalen et al., 2022). Another warning sign of the aging population is that it is projected to include 152 million older adults with dementia by 2050 (Editorial, 2017). The most recent data have indicated that the prevalence of neurodegenerative diseases will double in Europe and triple globally by 2050 (Scheltens et al., 2021). Multiple and progressive symptom manifestations of mild cognitive impairment and dementia are characterized by a decline from a previously attained cognitive level; however, in dementia, the profound decline also affects social functioning and daily living (Livingston et al., 2017; Mitchell, 2015). Furthermore, the enormous burden of dementia on patients, families, and society costs approximately $818 billion – $1 trillion annually (Editorial, 2017; Levey, 2021). Dementia has been regarded as a progressive, inexorable, and incurable illness (Levey, 2021; Mitchell, 2015). Meanwhile, arduous research has been undertaken to seek more effective therapeutic interventions for patients with dementia (Cummings, 2004). Nevertheless, currently, no effective treatment options for the disease exist (Yiannopoulou & Papageorgiou, 2020). Thus, promoting healthy cognitive functions has been a necessity for reducing individual and societal burdens related to impaired cognition in older adults (Alves et al., 2013). On the basis of the current evidence, it is concluded that early and timely preventative actions are promising strategies to delay the onset of cognitive impairment and dementia (Grande et al., 2020; Livingston et al., 2020). There has been growing interest in enhancing cognitive functions in older adults via cognitive and brain interventions (Meltzer et al., 2021; Nguyen et al., 2019b; Wollesen et al., 2020). It is also evident that pure cognitive training and cognitive training with additional physical activity can be effective for leading stronger long-term effects on several aspects of cognitive functioning in healthy older adults (Gavelin et al., 2021; Rahe et al., 2015; Reijnders et al., 2013). Further, cognitive training can enhance cognitive self-efficacy (Goghari & Lawlor-Savage, 2018) as well as reliable neural effects in healthy older adults (Duda & Sweet, 2020). Consequently, various cognitive functions have been used as targets for training programs, i.e., memory, reasoning, processing speed (Rebok et al., 2014), cognitive plasticity (Nguyen et al., 2019a), and executive functions (EFs) (Mowszowski et al., 2016). Specifically, it is plausible that EFs might be the first cognitive functions to decline in older adults, and EF dysfunction was generally disproportionally higher than other cognitive impairments (Reuter-Lorenz et al., 2021). EFs have been considered as important and high-level cognitive processes for the successful completion of basic and complex daily activities in older adults (Ferguson et al., 2021). To carry out everyday functioning, older adults demand executive functioning to be able to independently perform complex, self-serving, and goal-directed behaviors, while ignoring irrelevant information (Bell-McGinty et al., 2002; Veríssimo et al., 2022). The key components of EFs include inhibition, updating/working memory (WM), and shifting/cognitive flexibility (Miyake & Friedman, 2012). Additionally, EFs have been found to decline in the 30s (at the earliest), especially WM, inhibitory control, and planning (Ferguson et al., 2021). Moreover, cognitive training aiming at enhanced EFs yields a reduction in functional decline and immediate and long-term improvements in cognitive performance during everyday activities (Nguyen et al., 2019b; Willis et al., 2006). Furthermore, in longitudinal studies, EF improvement in older adults shows protective effects (or cognitive reserve) against cognitive decline (Holtzer et al., 2012; Ihle et al., 2020; Oosterman et al., 2021). Accordingly, several commercially available cognitive games have focused on enhancing EFs of older adults without cognitive impairment (Bonnechère et al., 2020). Additionally, combined physical and cognitive interventions on EFs in older adults have been widely investigated and the results have suggested positive outcomes for delaying the decrease of EFs (Guo et al., 2020). Nevertheless, previous studies have suggested a combination of physical exercise and cognitive training was not significantly more effective than each training alone (Gavelin et al., 2021; Guo et al., 2020). Expectedly, combined intervention should improve EFs, everyday functioning, and well-being; however, the varying results have suggested that the combined training did not yield expected synergic effects (Desjardins-Crépeau et al., 2016; Fraser et al., 2017). An interesting avenue in the investigation of synergetic effect would be to consider the effect of simultaneous (instead of sequential) cognitive and physical activities (e.g., cognitive motor functions) on cognitive functions using technology-based platforms in older adults (e.g., virtual reality) (Dermody et al., 2020; Desjardins-Crépeau et al., 2016; Wollesen et al., 2020; Zhu et al., 2021). VR has several applications for improving (or training) older adults. Although exposure to VR application may result in symptoms of motion sickness for some people (e.g., eye fatigue, headaches, and nausea) (Park et al., 2019), its advantages include a secure environment, high ecological validity, and an inexpensive aid to support active aging (Appel et al., 2020; Kim et al., 2021; Syed-Abdul et al., 2019). A previous study revealed the acceptance (or positive perception) of older adults toward using VR (Mascret et al., 2020), namely, they perceived the VR to be useful, an enjoyable experience, and easy to use (Mascret et al., 2020; Syed-Abdul et al., 2019). Additionally, several studies have implemented the VR intervention in clinical settings with children and adolescent populations, but there have been fewer studies focusing on the older adult population (Skurla et al., 2021). Moreover, the effectiveness of the VR-based intervention on cognitive functions in older adults has remained underinvestigated. Additionally, the extant literature on the VR-based training has been generated from high-income countries; therefore, it remains unclear if this emerging technology can be translated to other regions of the world (Skurla et al., 2021). Accordingly, the present study aimed to investigate the effectiveness of the VR-based cognitive intervention for enhancing EFs in older adults living in communities. Study Design and Participants The pretest-posttest control group design (Edmonds & Kennedy, 2017) was applied at the Brain Stimulation and Development Center, College of Research Methodology and Cognitive Science, Burapha University in Thailand. In this design, participants were randomly assigned to passive control (nonintervention) and experimental groups. The dependent variables (i.e., EFs) were assessed twice (i.e., pretest and posttest measurement) for both groups. The initial EFs scores of the participants were recorded for comparison to the posttraining scores. The older adults living in communities aged 60-69 years from Chonburi province in the Eastern region of Thailand were invited to participate in the study. Subsequently, the interested individuals were assessed according to inclusion and exclusion criteria for hearing, vision, cognitive functions, and a history of brain injury and psychiatric disorders. All participants had normal hearing and vision. Additionally, these participants had normal cognitive function as being assessed by the Mini-Mental Status Examination-Thai version (MMSE-Thai) (Muangpaisan et al., 2015) and no history of brain injury and psychiatric disorders. During the training, four participants in the experimental group did not complete the VR-based cognitive intervention due to illness (i.e., nausea and oculomotor effects). In total, 60 eligible older adults were randomly and equally assigned to the passive control (n = 30) and experimental (n = 30) groups. All participants were fully informed of the purpose of the study, and written informed consent was obtained from all participants. The protocol of this study was approved by Burapha University-Institutional Review Board (BUU-IRB: HUU003/2564). The study was conducted according to the Guideline for Good Clinical Practice and the Declaration of Helsinki (World Medical Association, 2013). The participants received $30 for their participation and travel costs. The protocol of this project was approved by Burapha University-Institutional Review Board (BUU-IRB: HUU003/2564). Written informed consent was obtained from all participants. VR-Based Cognitive Intervention To enhance EFs of older adults, the VR-based cognitive intervention was developed according to the extant literature suggesting the strong links between EFs, visuospatial WM (Brown et al., 2012; Miyake et al., 2001; Wang et al., 2018), and visuomotor adaptation (Li et al., 2021; Stirling et al., 2013) in an aging population. Furthermore, the VR content was developed to fulfill six psychological processes (i.e., sensory memory, encoding, planning, movement control, active manipulation, and adaptation). Additionally, the analysis, design, development, implementation, and evaluation (ADDIE) model is a common instructional system design to develop the instructional and evaluate the VR system (Kim, 2021; Yu et al., 2021). Thus, the ADDIE model was utilized as an important phase for improving the VR learning environment and performance of the participants in the study. The VR immersive environment was delivered to each participant using an Oculus Quest head-mounted display (HMD) with a refresh rate of 72 Hz, a resolution of 1440 x 1600 per eye, and USB-C 3.0 connectivity controllers (see Figure 1A). The software used in the VR-based cognitive intervention was built in the Unity3D game engine. The VR system operated on a PC (CPU: AMD FX (tm)-6100 six-core; processor: 3.30 GHz; RAM: 128 GB DDR4; GPU: NVIDIA GeForce; GTX1050: 2GB GDDR5 128-bit memory; Microsoft Windows 10 64-bit OS). Additionally, two wireless joystick controllers (see Figure 1B) were applied to perform involving touching, selecting, grabbing, grouping/categorizing, and arranging animated objects in several environments. Figure 1 (A) Participant in the Experimental Group Wore HMD, Sat 100 cm in front of the Computer Screen, and was Supervised by a Well-trained Research Assistant; (B) Wireless Joystick Controllers; and (C) Eight Elderly VR Characters with Four Men and Women. 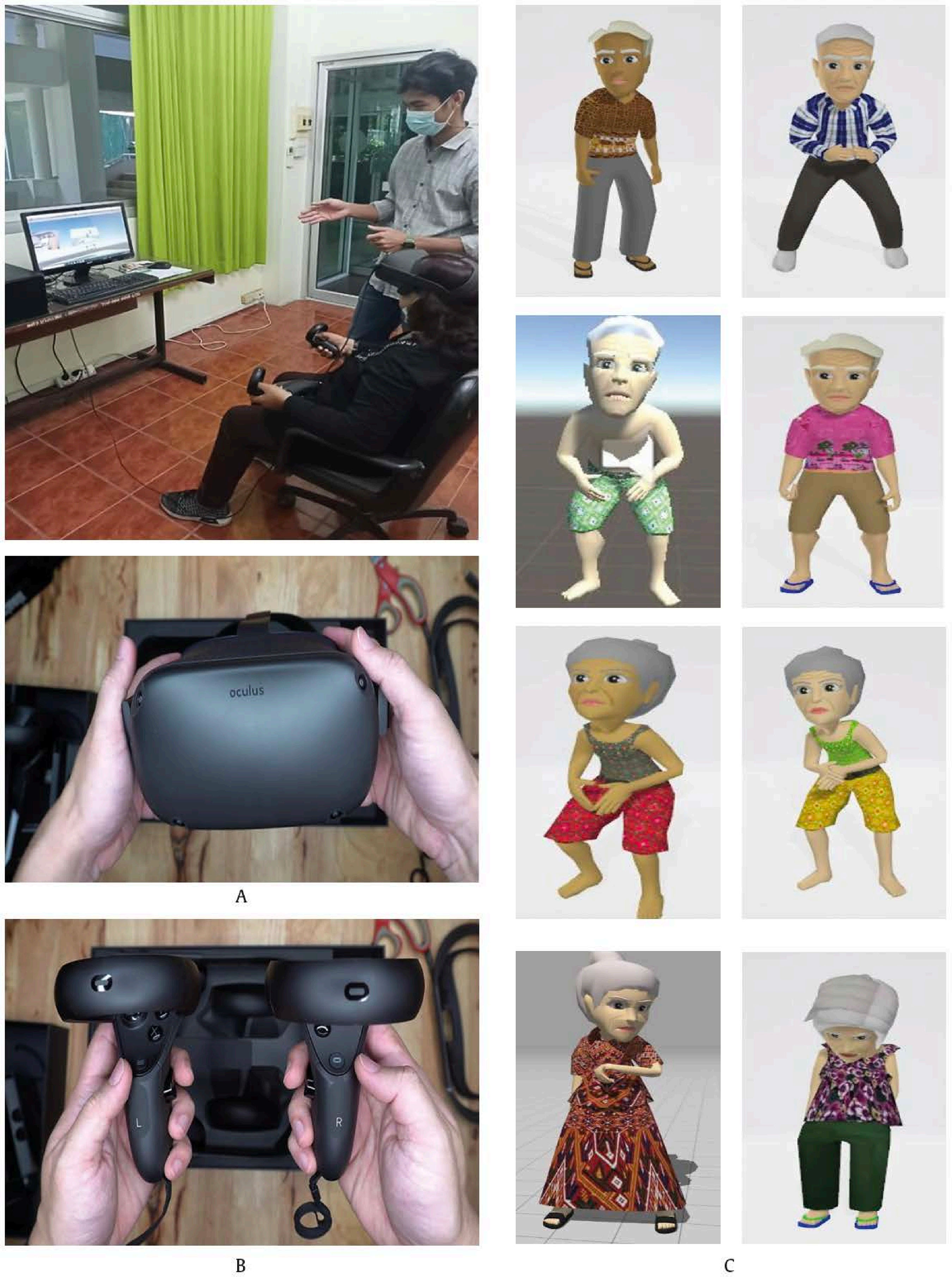 In Figure 1A participants in the experimental group wore HMD, sat 100 cm in front of the computer screen, and were supervised by well-trained research assistants, Figure 1B presents wireless joystick controllers, and in Figure 1C eight elderly VR-characters with four men and women appear. Before starting the intervention, participants were allowed to select a character out of eight models (see Figure 1C). VR scenarios (places, sounds, and objects) were designed (see Figure 2) according to the findings of a focus group with five older adults. Table 1 reports the places, objects, activities, and total session lengths of the VR experiences. The motion sickness was assessed for all participants by using an interview questionnaire. Two older adults (6.67%) reported mild motion sickness during the first session; thus, a short break was allowed to alleviate their symptoms. The experimental group received the VR training in the form of two 60 min sessions on a weekly basis for 4 weeks. After 4 weeks of training, the computer-based tests of EFs were used to assess the participants in both the control and experimental groups, and the posttest scores were compared with the pretest score. Table 1 Summary of the VR-based Cognitive Intervention for Older Adults 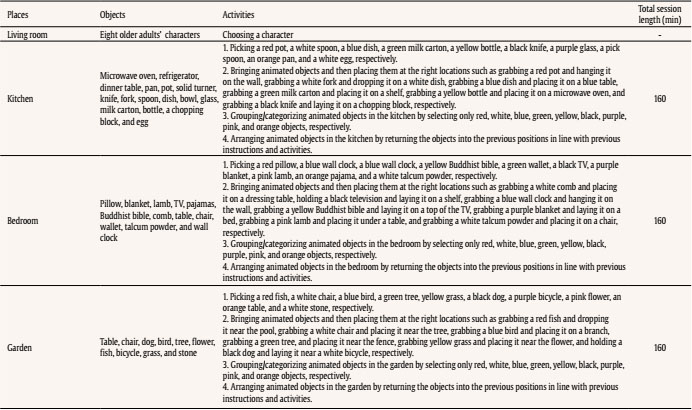 Figure 2 Screenshots of VR Kitchen (Upper Panel), Garden (Middle Panel), and Bedroom Scenarios (Lower Panel).  Measures All participants completed three standardized EF assessment tests (i.e., Go/noGo, Forward/backward digit span, and Berg’s Card Sorting) in the lab during the pretraining and posttraining sessions, approximately 30 days apart. The three EF tests were implemented using the Psychology Experiment Building Language Test Battery-version 2 (Mueller & Piper, 2014; Piper et al., 2012). Inhibition The Go/noGo test was used to index the inhibitory control as a central component of EFs (Diamond, 2013). The Go/noGo test has been reported in several studies to gauge the effective inhibition of a prepotent response in older adults (Falkenstein et al., 2002; Hong et al., 2016; Najberg et al., 2020). During the test, participants were required to watch a sequential presentation on a computer screen of letters (i.e., P or R) and respond to a target letter by pressing a button on a computer keyboard. A single letter (P or R) was presented in one of the 2 x 2 arrays with four stars for a duration of 500 ms with an interstimulus interval (ISI) of 1,500 ms. The Go/noGo test was composed of two conditions: the P-Go condition with 160 trials and the R-Go condition with 160 trials (see Figure 3, left panel). For the P-Go condition, participants were asked to respond by pressing the right shift key on the keyboard in response to the target letter “P” but to withhold their response to the nontarget letter “R.” The proportion of the target vs. nontarget letters was 80:20. Subsequently, a second reversal condition (R-Go) was administered requiring participants to respond to the target letter “R” but to withhold the response to the nontarget letter “P.” The ratio and the number of trials were identical to the P-Go condition. Together, the two conditions are composed of 320 trials with a mean response accuracy (RA) in percentage and a mean response time (RT) in ms used as the primary outcomes. The duration of the Go/noGo test was approximately 8 min. Updating Forward and backward digit span tests were applied to tax abilities to update and manipulate information in the WM (Nyberg & Eriksson, 2015; Wager & Smith, 2003). Forward and backward digit span tests (FDS/BDS) uniquely reflect passive and active updating of information, respectively (Waris et al., 2015). The FDS represents as a pure measure of attention, while the BDS relies more upon WM skills (Cullum, 1998; Cullum & Larrabee, 2010). The updating WM reflects a core of EFs, in which it is responsible for the reviewing of incoming information, elimination of extraneous information, and replacement of discarded information with more relevant content (Daucourt et al., 2018). The digit span tests were divided into two conditions, namely, the FDS/BDS tests. The FDS/BDS tests were reported to measure updating abilities of EFs in older populations (Fisk & Sharp, 2004; Grogan et al., 2018; Heinzel et al., 2014). During the tests, strings of digits of increasing length, beginning with three and ending with ten, were presented on the computer screen. Each length of digit list consisted of two trials, with ISI of 1,000 ms and intertrial stimulus of 1,500 ms (see Figure 3, middle panel) and each trial of which was scored 0 or 1 point. Participants were asked to repeat by pressing the target numbers on the computer keyboard in forward or backward orders. If participants failed to repeat both trials or obtained scores of 0 on both trials of the same block of digit, the tests were immediately terminated. No time limit was placed on the participants. The primary outcomes were the number of trials completed correctly or memory span and the total response time in minutes. The duration of the FDS/BDS tests was approximately 14 min in total. Figure 3 Screenshot of PEBL’s Go/noGo (Left Panel), Forward/Backward Digit Span (Middle Panel), and Berg’s Card Sorting Tests (Right Panel). 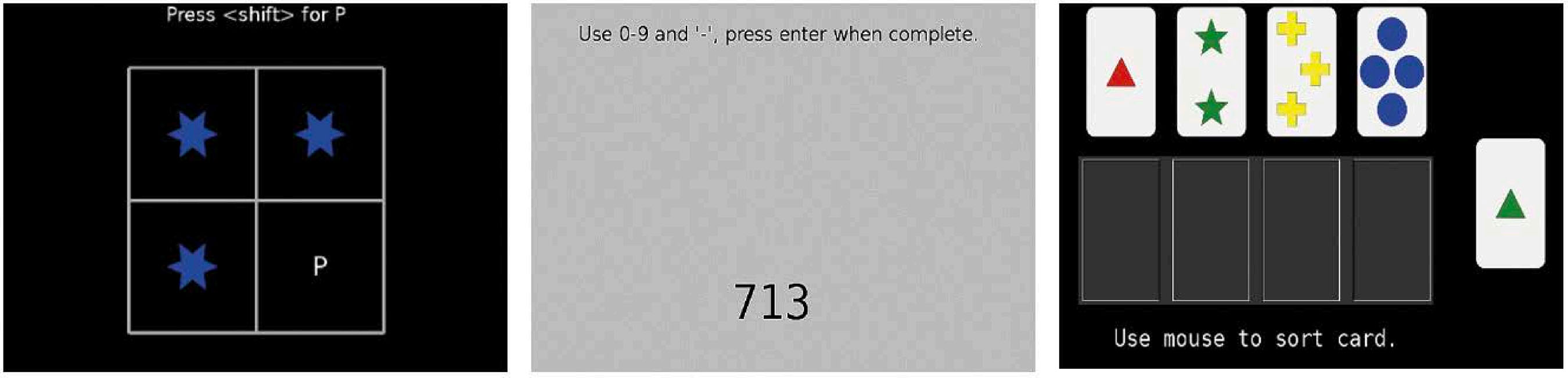 Shifting Berg’s Card Sorting Test (BCST) was used to measure the EF features-switching task. The shifting/switching ability is often regarded as a key aspect of EFs, reflecting the ability to modify attention and behavior in coping with changing demands and circumstances (Rabinovici et al., 2015). The BCST-like card-sorting tests have been widely used to index the shifting ability in older adults (Gamboz et al., 2009; Lange et al., 2016; Ridderinkhof et al., 2002). During the test, participants were presented with a 64-card deck displayed on a computer screen. Each stimulus card contained a different combination of one red triangle, two green stars, three yellow crosses, and four blue circles (see Figure 3, right panel). Participants were required to sort a card into piles by using a computer mouse and determine the underpinning classification rule by trial and error. The feedback was provided after each card was sorted. Once the participants achieved card matching for 10 consecutive cards, the classification rule was changed (Fox et al., 2013; Piper et al., 2015). No time limit was imposed on the participants. The percentage of correct responses, percentage of perseverative errors, and the number of trials to complete the first category were used as the primary outcomes (Gunner et al., 2012; Miranda et al., 2020). The duration of the BCST was approximately 12 min. Data Analysis Descriptive (i.e., mean, standard deviation, skewness, kurtosis, and effect size) and inferential statistics (i.e., chi-square test, independent t-test, and a repeated-measures ANCOVA were used to (i) summarize information concerning sex, age group, level of education, health status, and the EFs parameters; (ii) examine the normality assumption of dependent variables across the EFs parameters; and (iii) test the within- and between-group differences, respectively. Additionally, the group x time interaction was investigated to examine the pattern of change for the groups (Tabachnick & Fidell, 2001). Partial eta squared ηp2) was calculated to estimate the effect sizes or magnitudes of differences for the EF enhancement from the pretraining to the posttraining and between the posttraining of the control and experimental groups. The calculated ηp2 values of .01, .06, and .17 can be interpreted as small, moderate, and large effects, respectively (Lakens, 2013). Additionally, descriptive and inferential statistics were performed using IBM SPSS Statistics 27.0 (SPSS Inc., Chicago, Illinois, USA). Sixty community-dwelling older adults were recruited and equally and randomly assigned to the control (n = 30) and experimental groups (n = 30). The mean age of all participants was 65.87 ± 4.18 years (min 60 - max 77), 63% were female, and 100% were Thais. The mean year of education was 6.16 ± 4.11 years (min 1 – max 18). The majority of participants were healthy (73%), the rest had hypertension and type II diabetes (27%). Accordingly, no significant difference was found between two groups in terms of sex (χ2 = 3.52, p = .06), year of education (t = 1.91, p = .06), and health status (χ2 = 0.09, p = .77). Nonetheless, the mean age differed between the two groups (67.30 ± 4.86 and 64.43 ± 2.79 for the control and experimental groups, t = −2.80, p =.01), so that this variable was used as a covariate in the model. No missing data were found. Table 2 indicates mean, SD, min-max, and skewness and the kurtosis values for the control and experimental groups across several parameters of EF tests. The normality assumption was tested to obtain accurate results for multivariate analysis. Specifically, the pretest scores for parameters of the Go/noGo, FDS/BDS, and BCST revealed a normal distribution as indexed by the skewness and kurtosis values (Brown, 2006). The skewness values ranged from 0.12 to -2.58 and the kurtosis values ranged from -0.01 to 6.43. The posttest scores for parameters of the same tests indicated the normal distribution. The skewness and kurtosis values were not greater than -3 - 3 and -10 - 10, respectively (i.e., -0.07 - 2.75 and ± 0.04 - 9.70) (Brown, 2006). Table 2 Participant Characteristics of the Control and Experimental Groups across Outcome Measures 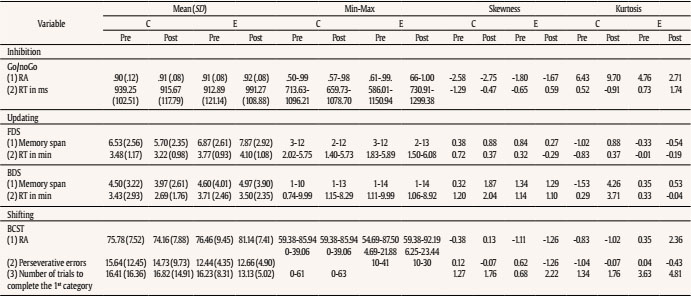 Note. C = control; E = experimental. For the Go/noGo test, an ANCOVA revealed no main and interaction effects for RA, F(1, 57) = 0.22, p = .64, ηp2 = < .01; F(1, 57) = 1.47, p = .23, ηp2 = .03. The significant interaction effect for group x time was found for RT, F(1, 57) = 6.95, p = .01, ηp2 = .11, suggesting that the posttest of the experimental group was significantly higher than those of the control group and the effect size was moderate (see Table 3 and Figure 4A). Figura 4 Significant Interaction Effects for (A) Go/NoGo: RA, (B) FDS: Memory Span, (C) FDS: RT, and (D) BCST: Percentage of Correct Responses, with Age as a Covariate in the Model. 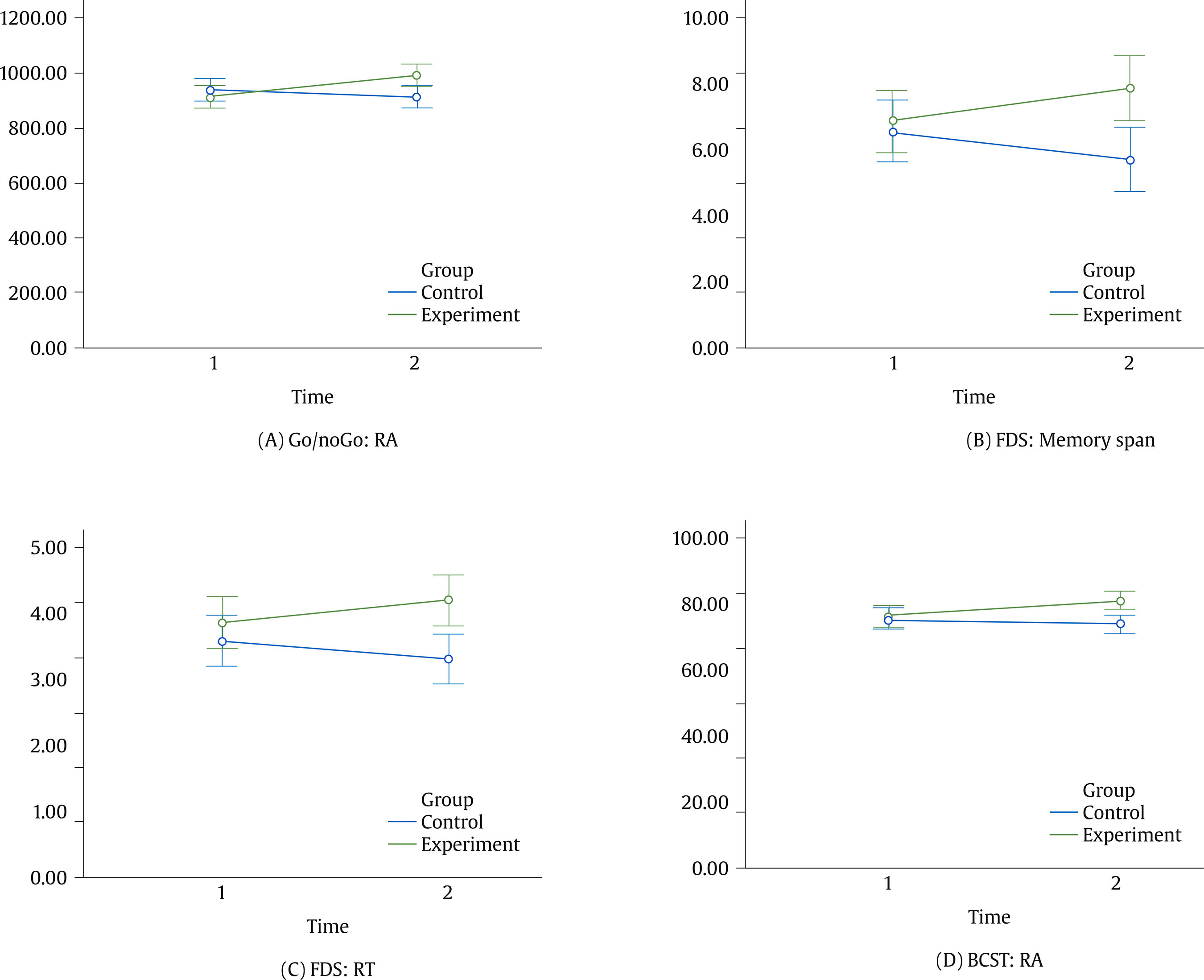 For the FDS test, the interaction effects were evident for both memory span and RT. The interaction effect of group x time for memory span was statistically significant, F(1, 57) = 12.09, p < .01, ηp2 = .18, indicating that the posttest of the experimental group was significantly greater than those of the control group and the effect size was large (see Table 3 and Figure 4B). Similarly, the significant interaction effect of group x time was also found for RT, F(1, 57) = 4.46, p = .04, ηp2 = .07, revealing that the posttest of the experimental group was significantly higher than those of the control group and the effect size was moderate (see Table 3 and Figure 4C). Table 3 ANCOVA Results for Outcome Measures 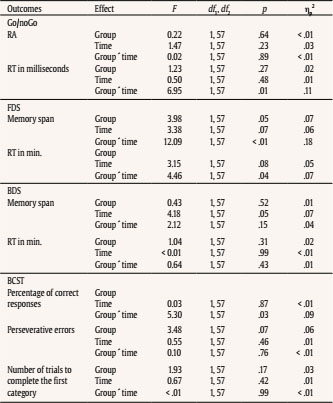 Note. Age as a covariate; significant differences in bold font. Although the pretest and posttest of the BDS test indicated a downward trend for memory span, F(1, 57) = 4.18, p = .05, ηp2 = .07, the main and interaction effects were not evident for two parameters of the BDS test, Groupmemory span: F(1, 57) = 0.43, p = .52, ηp2 = .01; Group x Timememory span: F(1, 57) = 2.12, p = .15, ηp2 = .04; GroupRT: F(1, 57) = 1.04, p = .31, ηp2 = .02; TimeRT: F(1, 57) = < .01, p = .99, ηp2 = < .01; Group x TimeRT: F(1, 57) = 0.64, p = .43, ηp2 = .01. Finally, only RA differed significantly between groups for posttest of the BCST, F(1, 57) = 5.30, p = .03, ηp2 = .09 (see Table 3). Figure 4D indicates that the posttest for RA was significantly greater than those of the control group, and the effect size was moderate. In line with previous studies, this study addresses the research gaps on the VR-based cognitive intervention in older adults living in communities. Specifically, limited evidence exists to demonstrate the combined cognitive motor training using VR technology in older adults, especially in developing countries (Seifert & Schlomann, 2021; Skurla et al., 2021). Additionally, the effectiveness of an intensive and short-term cognitive intervention on the enhancement of EFs has been underinvestigated in healthy older adults (Muñoz et al., 2022). Thus, this study aimed to investigate the EF enhancement from participating in VR-based cognitive intervention in older adults. The visuospatial WM and visuomotor adaptation were inputted and utilized as multimodal domains for enhancing EFs in the intensive VR activities. The participants in the control and experimental groups were comparable in sex, year of education, and health status. The mean year of education for both groups was approximately 6 years, and this number is higher than those of older adults in other developing countries (Jin et al., 2022; Lu & Lou, 2022). Moreover, a higher level of education may increase positive attitude toward or adoption of VR technology in older adults (Huygelier et al., 2019). Motion sickness or cybersickness occurred during and after exposure to the VR intervention for the first session, but it was well tolerated (i.e., 6.67% withdrawals). This finding aligns with the recent review, indicating approximately 4%-5% cybersickness withdrawals across different stimuli and HMDs (Caserman et al., 2021). Previously, evidence has suggested the support of enhancing cognitive functioning in healthy older adults by using cognitive-based trainings (Gavelin et al., 2020; Sanjuán et al., 2020). Nevertheless, despite the diversity among applied cognitive interventions in healthy older adults, the VR-based intervention has not been widely adopted for boosting EFs (Kim et al., 2021). EFs (i.e., inhibitory control, WM, and attentional flexibility) has been linked with daily activities since these functions include the ability to evaluate, organize, plan, perform, and achieve goals as well as the capacity to flexibly adapt to changed circumstances (Diamond, 2013; Lezak, 1982). Thus, cognitive and functional decline might be prevented or delayed via an effective intervention targeting multiple domains of executive functioning. The current findings highlighted that the benefits of the multiple domains of the VR-based cognitive intervention enhance key aspects of higher cognitive functions (i.e., multidimensional EFs). To the best of our knowledge, this study is the first to highlight the positive outcomes of the VR-based intervention on EF performances in older adults without cognitive impairment. Particularly, these findings suggest the greater effects on the training group for inhibition, updating, and shifting abilities. The inhibitory control, as a key process of EFs, was impaired in older age according to the inhibitory deficit hypothesis wherein older adults are less able to ignore irrelevant thoughts and actions in comparison with young adults (Rey-Mermet & Gade, 2018). The eight-week intervention increased processing speed as measured using RT for the Go/noGo test. These findings are contrary to previous studies in that cognitive training induced a faster RT for the Go/noGo test in older adults (Schroder et al., 2020; Wilkinson & Yang, 2015). Consequently, it is plausible that older adults in the training group have greater recruitment of attentional control systems and this may increase the speed of cognitive processing (Campbell et al., 2020). Similarly, the VR-trained older adults may adopt a more cautious approach when performing the inhibition task (Shao & Lee, 2014). The FDS and BDS were used to index updating abilities of older adults. The FDS score reflects passive updating capacity, but the BDS score indicates active updating capacity (Waris et al., 2015). This study demonstrated an improved memory span and reduced cognitive processing of older adults in the experimental group. Nevertheless, the null effect was found for the BDS. These findings align with previous studies in that the FDS test was less sensitive to decline because of aging (Sun et al., 2005) but more sensitive to change because of cognitive training than those of the BDS test (Borella et al., 2013). Likewise, previous studies also suggested the FDS score showed less g-loaded measures and implies a major environment influence (i.e., practice and training effects) (Bartels et al., 2010; Ganzach, 2016; Roediger & Karpicke, 2006; te Nijenhuis & van der Flier, 2013; Wongupparaj et al., 2017). The FDS and BDS tests measures share cognitive processing in that the FDS reflects the passive updating processing, but the BDS requires beyond mere storage of representation (i.e., manipulation and processing) (Bopp & Verhaeghen, 2005). Specifically, the BDS is fundamentally a more attentionally demanding test than the FDS (Coalson et al., 2010; Wongupparaj et al., 2017). Therefore, a longer period of the intervention may accordingly benefit more complex cognitive functions (i.e., active updating of WM). The VR-based training showed an improved shifting ability of older adults in the experimental group as indexed by the percentage of correct response (i.e., RA). These results align with the previous study in that the correct response was improved after the training (Grönholm-Nyman et al., 2017). The null effects for other shifting parameters (i.e., perseverative errors and the number of trials to complete the first category) may reflect a slower update of the cognitive function relating to schema thresholds within the basal ganglia and a decline in sensitivity to feedback (Caso & Cooper, 2021). In sum, the present results highlighted the benefits of the VR-based cognitive intervention for enhancing EFs of older adults. The underlying mechanism of the training on EFs may reflect the effectiveness of the current VR protocol wherein it was developed according to the initial findings of the pilot study in older adults. The training activities also focused on two EF-related constructs (the visuospatial WM and visuomotor adaptation) and complied with the ADDIE model. Moreover, the indirect effects of the use of VR environments may be influential as indicated in previous studies suggesting the positive effects of VR intervention on participants in terms of increasing engagement and motivation (Makransky et al., 2019; Mouatt et al., 2020), enhancing ecological validity (Bauer & Andringa, 2020), improving embodied cognition (Peeters & Segundo-Ortin, 2019), and stimulating multisensory integration for learning (Bauer & Andringa, 2020). It is evident that the VR-based intervention showed a powerful real-life impact and a good stability of results over time, similar to that of the classical evidence-based treatments (Morina et al., 2015; Opri et al., 2012). Further, the VR therapeutic technique demonstrated several potential clinical uses, and it might also be considered for routine use in rehabilitation (Geraets et al., 2021; Tennant et al., 2020; Triegaardt et al., 2020). Nonetheless, much of the research with technologies behind the VR-based trainings and interventions is still in the intervention development phase. Building on the promising results of the current study, further studies will begin to observe intervention efficacy studies in terms of specific components of the intervention, dosing, frequency of intervention, intensity, number of repetitions, and measurement tool (Proffitt & Lange, 2015; Ridout et al., 2021). Finally, this study comprises several limitations that deserve comment. First, this study excluded the follow-up; thus, the middle- and long-term effects of the VR-based intervention were unobserved. Second, there was no subgroup analysis on sex for the VR-based intervention. Third, emotional and well-being-related effects of the VR-based intervention should also be further investigated. Beside cognitive effects, the intervention based on emotional and well-being aspects can yield positive outcomes for aging adaptation and quality of life of older adults (Delhom et al., 2020). Fourth, further study should also evaluate motor functions of the VR-trained older adults as the efficacy of the VR-based intervention. The findings of this study can provide stronger support for the VR-based intervention on cognitive abilities in older adults without cognitive impairment, especially in a higher cognitive function (i.e., EFs). Additionally, the current findings support the generalization of the effectiveness of VR training in developing countries. Nevertheless, future research should therefore continue to utilize the VR-based cognitive intervention in tandem with other treatment modes, brain stimulation, or traditional rehabilitation in older patients. Given the immediate beneficial training effects of several EF parameters, further studies should investigate middle- and long-term training periods and the benefits resulting from the VR-based cognitive intervention. Conflict of Interest The authors of this article declare no conflict of interest. Acknowledgments The authors would like to sincerely thank the research assistants of this project, that is, Miss Chanmeardey Chiv, Mr Oussa Em, Miss Wanvipha Hongnaphadol, and Miss Natthapat Thammasittivate. Funding: This research is funded by National Research Council of Thailand (NRCT 367-2563), and it is part of the research project entitled ‘Development of a virtual reality program for enhancing executive functions in the elderly’. This research is partially supported by the Cognitive Science and Innovation Research Unit (CSIRU), College of Research Methodology and Cognitive Science, Burapha University. Cite this article as: Makmee, P. & Wongupparaj, P. (2022). Virtual reality-based cognitive intervention for enhancing executive functions in community-dwelling older adults. Psychosocial Intervention, 31(3), 133-144.https://doi.org/10.5093/pi2022a10 |
Cite this article as: Makmee, P. & Wongupparaj, P. (2022). Virtual Reality-based Cognitive Intervention for Enhancing Executive Functions in Community-dwelling Older Adults. Psychosocial Intervention, 31(3), 133 - 144. https://doi.org/10.5093/pi2022a10
peera.wo@go.buu.ac.th Correspondence: peera.wo@go.buu.ac.th (P. Wongupparaj).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
Send






