


School-based Psychosocial Interventions’ Effectiveness in Strengthening Refugee and Migrant Adolescents’ Mental Health, Resilience, and Social Relations: A Four-country Cluster Randomized Study
[La eficacia de las intervenciones psicosociales centradas en la escuela para potenciar la salud mental, la resiliencia y las relaciones sociales de adolescentes refugiados y migrantes: un estudio de grupos aleatorizados en cuatro países]
Caroline Spaas1, Sameh Said-Metwaly1, 2, Morten Skovdal3, Nina Langer Primdahl3, Signe Smith Jervelund3, Per Kristian Hilden4, Arnfinn J. Andersen4, Marianne Opaas4, Emma Soye5, Charles Watters5, An Verelst6, Ilse Derluyn6, Hilde Colpin1, and Lucia De Haene1
1KU Leuven University, Belgium; 2Damanhour University, Egypt; 3University of Copenhagen, Denmark; 4Norwegian Centre for Violence and Traumatic Stress Studies, NKVTS, Oslo, Norway; 5School of Education and Social Work, University of Sussex, UK; 6Ghent University, Belgium
https://doi.org/10.5093/pi2023a12
Received 4 January 2023, Accepted 30 May 2023
Abstract
School-based psychosocial interventions are increasingly put forward as a way to support young refugees’ and migrants’ well-being and mental health in resettlement. However, the evidence on these interventions’ effectiveness remains scarce and scholars denounce particular gaps in the evidence to date, pointing to a lack of large-scale, controlled studies and studies including social outcome measures. This cluster randomized study aims to strengthen the evidence base on school-based psychosocial interventions for refugee and migrant youth by assessing the effect of two interventions, Classroom Drama and Welcome to School, on youth’s mental health, resilience, and social relations in Belgium, Denmark, Norway, and the United Kingdom. Multilevel analyses were conducted separately for the two interventions (Classroom Drama, n = 307, ages 11-19; Welcome to School, n = 251, ages 11-23), using separate no-treatment control groups. Our analyses indicated a significant main, positive effect of Classroom Drama on perceived family support, and an effect on perceived support from friends that was moderated by country: in the United Kingdom, the intervention group reported an increase in perceived friend support, whereas the control group reported a decrease. Furthermore, baseline resilience moderated the effect of the Classroom Drama intervention on behavioral difficulties and well-being. No effects of Welcome to School on any of the outcome variables were found. Overall, this study provides novel, nuanced evidence on school-based psychosocial interventions for refugee and migrant adolescents.
Resumen
Cada vez se proponen más las intervenciones psicosociales centradas en la escuela como ayuda al bienestar de jóvenes refugiados y migrantes en su realojamiento. No obstante hay pocas pruebas sobre la eficacia de tales intervenciones y los expertos denuncian fallas en dichas pruebas hasta el momento debido a la falta de estudios controlados a gran escala que incluyan medidas de los resultados sociales. El presente estudio de grupos aleatorizados pretende potenciar la base de pruebas sobre intervenciones psicosociales centradas en la escuela con jóvenes refugiados y migrantes analizando el efecto de dos intervenciones, “El drama en el aula” y “Bienvenido al colegio”, en la salud mental, la resiliencia y las relaciones sociales de los jóvenes en Bélgica, Dinamarca, Noruega y el Reino Unido. Se efectuaron análisis multinivel por separado para las dos intervenciones (“El drama en el aula”, n = 307, edad entre 11 y 19 años; “Bienvenido al colegio”, n = 251, edad entre 11 y 23 años) con grupos de control sin tratamiento separados. Los análisis mostraron un efecto positivo principal significativo de “El drama en el aula” en el apoyo familiar percibido y un efecto en el apoyo percibido de los amigos moderado por el país: en el Reino Unido el grupo de intervención presentó un aumento del apoyo percibido de los amigos, mientras que en el grupo control disminuyó. Además la resiliencia básica moderaba el efecto de la intervención de “El drama en el aula” en las dificultades conductuales y en el bienestar. No se apreció efecto de “Bienvenido al colegio” en ninguna de las variables resultado. En términos generales el estudio supone un inédito y detallado aval de las intervenciones psicosociales centradas en la escuela en el caso de adolescentes refugiados y migrantes.
Keywords
School-based psychosocial intervention, Refugee youth and adolescents, Migrant youth and adolescents, Mental health, Social relationsPalabras clave
Intervención psicosocial centrada en le escuela, Jóvenes y adolescentes refugiados, Jóvenes y adolescentes migrantes, Salud mental, Relaciones socialesCite this article as: Spaas, C., Said-Metwaly, S., Skovdal, M., Primdahl, N. L., Jervelund, S. S., Hilden, P. K., Andersen, A. J., Opaas, M., Soye, E., Watters, C., Verelst, A., Derluyn, I., Colpin, H., & Haene, L. D. (2023). School-based Psychosocial Interventions’ Effectiveness in Strengthening Refugee and Migrant Adolescents’ Mental Health, Resilience, and Social Relations: A Four-country Cluster Randomized Study. Psychosocial Intervention, 32(3), 177 - 189. https://doi.org/10.5093/pi2023a12
Correspondence: caroline.spaas@kuleuven.be. (C. Spaas).
High levels of global conflict and poor socio-economic and environmental conditions are driving the migration of a rising number of young refugees and migrants to and within Europe (European Commission, 2022; European Parliament, 2020; Palik et al., 2020). European host societies hold a key responsibility to promote the well-being and positive development of these young refugees, forcibly displaced due to war, conflict, or persecution (United Nations, 2022), and of their migrant peers relocating because of economic or social reasons (e.g., Douglas et al., 2019; Vaghri et al., 2019). Reflecting on adequate support for this population, scholars and policymakers are increasingly turning their attention to school-based psychosocial interventions. However, the evidence regarding this form of care needs to be further expanded (e.g., Tyrer & Fazel, 2014). In this context, this paper undertakes the systematic study of two school-based psychosocial intervention programs in four European countries. Throughout the following paragraphs, we first situate the need for psychosocial care for young refugees and migrants. We continue to present central arguments for locating psychosocial care in schools and address the current gaps in research on school-based psychosocial interventions. This preludes the description of our study, its design and results, and, finally, a discussion of its findings. Young Refugees and Migrants: An At-risk Population in Need of Psychosocial Support Migration is often identified as a risk factor for mental health, particularly in adolescence, when migration-related life changes concur with stark developmental transformations (e.g., Rousseau & Frounfelker, 2019). Central adolescent developmental tasks, such as identity formation, can be profoundly interrupted by experiences of uprooting, relocation, and navigating complex processes of social and cultural change in multi-ethnic resettlement contexts (e.g., Pacione et al., 2013). In this context, a substantial and growing body of studies documents the at-risk mental health of young refugees and migrants resettled in Europe (e.g., Dimitrova et al., 2016; Kouider et al., 2014; Spaas, Verelst, et al., 2022). Research on the mental health of refugee adolescents univocally describes high rates of post-traumatic stress disorder (PTSD; between 19 and 52.7%; Kien et al., 2019) and a broad range of internalizing and externalizing behavioral difficulties (e.g., Hodes & Vostanis, 2019). While research on non-refugee migrants is somewhat less conclusive (e.g., Rousseau & Frounfelker, 2019), a growing number of studies document also their vulnerable mental health status. Recent scholarly reviews point to an increased prevalence of internalizing mental health problems in migrants (Dimitrova et al., 2016; Kouider et al., 2014), and two other recent European studies describe elevated rates of PTSD-symptomatology in migrant children and adolescents, much like in their refugee counterparts: compared to 10% in general child and adolescent populations, 32.8% (Kevers, Spaas, Colpin, et al., 2022) and 32.4% (Spaas, Verelst, et al. 2022) of migrant children and adolescents participating in these studies showed to experience high levels of post-traumatic stress. In all, this body of research indicates that young refugees and migrants could benefit from the development and provision of psychosocial support in resettlement communities. Determinants of Young Refugees’ and Migrants’ Mental Health: Targeting Host Societal, Structural, and Relational Factors in Psychosocial Care The range of mental health difficulties experienced by young refugees and migrants, as well as the proportion of youth who do not develop mental health issues, have piqued research interest in identifying the risk and protective factors that influence mental health after migration (Scharpf et al., 2021). Understanding these risk and protective factors is crucial in comprehending refugee and migrant youth’s predicament and in designing and providing appropriate care for them (e.g., Reed et al., 2012). Throughout the literature on the mental health of young refugees and migrants, scholars often consider its determinants related to the different stages of migration, looking at pre-migration, peri-migration, and post-migration risks and protective factors (e.g., Reed et al., 2012; Rousseau & Frounfelker, 2019). Here, research on pre- and peri-migration adversity (e.g., exposure to war and collective violence, experiences of deprivation, family separation) as well as protective factors (e.g., personal resources, parental availability) is complemented by an emphasis on the central role of resettlement experiences (e.g., the detrimental mental health impact of daily stressors, experiences of social isolation and discrimination versus the protective influence of feelings of social support and belonging in resettlement) in explaining refugee and migrant adolescents’ mental health (e.g., Beiser & Hou, 2016; Frounfelker et al., 2020; Spaas, Verelst, et al., 2022; Verelst et al., 2022). Scholarly work on resilience equally draws attention to host societal and relational resources shaping positive mental health outcomes after adversity in the lives of young refugees and migrants (e.g., Ungar, 2013; Ungar & Liebenberg, 2011). Here, scholars have broadened individualized perspectives on resilience, toward a socio-ecological, dynamic understanding of resilience as “the quality of the interactions between systems [individuals] and the resources they need to do well.” (Ungar et al., 2019, p. 616). This uncovering of the role of host societal, structural, and relational dynamics in refugees’ and migrants’ well-being shapes scholarly consensus that mental health promotion is intrinsically intertwined with the fostering of social resources, social support, and social inclusion in resettlement (e.g., Kevers, Spaas, Derluyn, et al., 2022; Measham et al., 2014; Ungar et al., 2019). This consensus, in turn, has spurred the development of psychosocial care interventions that are embedded in the social ecologies of refugees and migrants and aim to strengthen their social relationships as a crucial determinant of individual mental health. Schools in particular, situated at the intersection of individual, family, community, and socio-cultural ecologies, are considered in a key position to provide psychosocial support in resettlement (e.g., Bennouna et al., 2019; Fazel & O’Higgins, 2020; Kevers, Spaas, Derluyn, et al., 2022; Kronick, 2018; Rousseau & Guzder, 2008; Tyrer & Fazel, 2014). School-based Psychosocial Interventions for Refugee and Migrant Adolescents Several arguments support the growing emphasis on the potential of school-based psychosocial interventions in promoting refugee and migrant adolescents’ well-being. First, providing psychosocial care within schools, as low-threshold spaces little imbued with institutional distrust and mental health-related stigma, can alleviate some of the barriers to accessing care that young refugees and migrants are known to experience (e.g., Colucci et al., 2015; Fazel et al., 2016; Peñuela-O’Brien et al., 2022). Second, the unique value of school-based psychosocial interventions lies in their potential to engage with refugee and migrant adolescents’ everyday social realities in promoting mental health. Indeed, scholars point to the centrality of schools as a developmental context in resettlement and herewith also emphasize the myriad of ways in which school-based relations play a role in refugee and migrant adolescents’ mental health (e.g., Schachner et al., 2018). Positive relations with peers and teachers at school, for example, are related to better mental health outcomes in refugee and migrant adolescents and can even counteract post-migration stressors of social isolation, discrimination, and exclusion (e.g., Kia-Keating & Ellis, 2007; Schachner et al., 2018). Third, schools often form a bridge between refugee and migrant adolescents’ family context and the host society (Fazel & O’Higgins, 2020; Rousseau et al., 2007; Spaas, Verbiest, et al., 2022). Here, scholars delineate the role of positive parent-school partnerships and collaborations in promoting adolescents’ mental health and adaptation in resettlement (Georgis et al., 2014; Roubeni et al., 2015). Emerging studies also show that school-based interventions might improve family relationships and interactions between families and schools, known to play an important role in the well-being of refugee and migrant children (e.g., Nadeau et al., 2017; Spaas, Verbiest, et al., 2022). Taken together, these arguments have inspired the development of school-based psychosocial interventions that engage with school-based social relations in aiming to support the mental health of refugee and migrant adolescents. Examples include classroom creative expression programs (e.g., Rousseau et al., 2007; Rousseau et al., 2004), participatory interventions aimed at enhancing safe, positive peer interactions and social relationships in multi-ethnic schools (e.g., Watters et al., 2021), classroom discussion programs focused on fostering positive relations in the classroom (e.g., Tuk & de Neef, 2020a), and multi-tier interventions combining preventive strategies targeting school-based relations, parent and community outreach with specialized mental health treatment located in the school context (e.g., Ellis et al., 2013). For all these interventions, the development of a solid scientific evidence base is still ongoing. Although a seminal body of studies provides promising evidence on the improvement of young refugees’ and migrants’ mental health through different types of school-based psychosocial interventions (e.g., Charbonneau et al., 2022; Tyrer & Fazel, 2014), other existing studies reveal important challenges as well as more complicated or mixed results (e.g., Bennouna et al., 2019; Rousseau et al., 2014). Overall, research on school-based interventions remains rather scarce and scholars identify several issues that need to be addressed when furthering the evidence base. First, scholars delineate the need for more controlled studies, preferably with larger sample sizes (n >100) than those featured in research to date (e.g., Sullivan & Simonson, 2016; Tyrer & Fazel, 2014). Second, scholars are furthermore called on to embrace the potential complexity of findings surrounding school-based interventions’ effectiveness (e.g., Sullivan & Simonson, 2016), to look not only at positive intervention outcomes, but to take into consideration that interventions might also elicit more nuanced or even negative outcomes, increasing, for example, youth’s awareness of their mental health difficulties, or exacerbating suffering in some youth (e.g., Rousseau et al., 2014). Third, scholars call for researchers to adopt a broader scope in assessing interventions’ effectiveness, suggesting that future research not only looks at individual mental health symptomatology as a central study outcome but also at interventions’ impact on the social processes they wish to affect (Kevers, Spaas, Derluyn, et al., 2022; Tyrer & Fazel, 2014). While interventions are increasingly designed from the perspective of this contextual understanding of mental health, intervention effectiveness research does not yet seem to have fully adopted this contextualized perspective in its aims. Indeed, only a small number of effectiveness studies to date have measured school-based psychosocial interventions’ impact on social determinants of young refugees’ and migrants’ mental health (e.g., Bal & Perzigian, 2013). However, based on the limited evidence for school-based psychosocial interventions’ effectiveness to date, it appears meaningful to broaden our perspective on interventions’ effectiveness, from an understanding of effectiveness as the reduction of individual symptomatic functioning to a more contextualized, systemic understanding of interventions’ impact on important social relations in the lives of young refugees and migrants. Indeed, a Belgian study that did take social outcome measures into account showed the positive impact of a school-based creative expression program on the safety of classroom social relations in multi-ethnic classrooms (Kevers, Spaas, Derluyn, et al., 2022). Another study on a school-based child-parent therapy program conducted with migrant children and their parents in the United States showed the intervention’s potential in improving both child-parent relations and children’s mental health (Ceballos & Bratton, 2010). This suggests that considering school-based psychosocial interventions’ impact on refugee and migrant adolescents’ social realities can provide novel and meaningful insight into interventions’ effectiveness, beyond a mere focus on their potential to reduce symptoms of individual psychopathology. This study aimed to contribute to the existing evidence base on school-based psychosocial interventions while addressing these gaps identified by scholars in the field. Thereto, we implemented two school-based psychosocial interventions, Classroom Drama and Welcome to School, in four European countries. Adhering to a cluster randomized design in two samples of 307 (Classroom Drama) and 251 (Welcome to School) adolescents, we examined the interventions’ effectiveness. Thereby, we paid attention not only to the effect of the interventions on young refugees’ and migrants’ mental health, but also to their potential impact on young people’s resilience and social relations, both in school and at home. Rooted in existing literature, as well as the design and aims of the two interventions, we hypothesized both interventions to be effective in improving refugees’ and migrants’ mental health, supporting their resilience, and promoting more positive social relations. Research Context This study forms part of the larger RefugeesWellSchool (RWS), a European Horizon2020 study investigating the effectiveness of different school-based psychosocial interventions in schools in six European countries through mixed quantitative and qualitative research methodologies. The present study concerns a quantitative evaluation of Classroom Drama (CD) (Equipe Théâtre Pluralité d’Erit, 2010), implemented in Belgium, Denmark, and the UK, and of Welcome to School (WTS) (Pharos, 2015; Tuk & de Neef, 2020a), implemented in Belgium, Denmark, and Norway. The implementation of the interventions and data collection within the RWS study occurred between January 2019 and October 2020. As such, the study was heavily affected by the outbreak of the Covid-19 pandemic and related public health measures, including the international closing of schools from March 2020 onward. This method section provides further detailed descriptions of the way Covid-19-related school closures impacted both the delivery of the interventions and the process of data collection in all four countries. Study Setting and Design In each country, schools were recruited based on their numbers of refugee and migrant newcomers, as well as their geographical location to maximize potential sample size and accommodate for feasible assessment and implementation of the intervention. In Belgium, Denmark, and Norway, schools were recruited relying on a combination of contacting schools through close collaboration with national and municipal educational departments, snowball sampling, and contacting schools directly. In the UK, due to the country’s decentralized educational system, schools were targeted and contacted directly by the research team. In Belgium, Denmark, and Norway the implementation of interventions targeted schools providing reception education to refugee and migrant newcomers. Reception education takes place in the first or first two years of newcomers’ introduction into the national educational system, focusing on host country language acquisition and integration (for a detailed description of the Norwegian educational system for refugee and migrant newcomers, see de Wal Pastoor, 2015). Here, all participating classes thus consisted solely of recently arrived refugee and migrant students. In the UK, CD was implemented in a multi-ethnic school receiving large numbers of refugee and migrant newcomers. In the class in which the intervention was implemented the majority of students were refugee and migrant newcomers, and a minority of students were second or third-generation migrants. While all students in the participating class received the intervention, only refugee and migrant newcomers were included in the assessments surrounding the intervention, as they made up the target population of the study. A cluster randomized design with pre- and post-test measurements was realized using schools as the unit of clustering in Norway and classes as clusters in Belgium, Denmark, and the UK. In Belgium, Denmark, and the UK, classes within schools were randomly assigned to either the intervention or no-treatment control condition. The potential risk for contamination between classes/conditions within schools was considered small, as the classes involved in the study did not share teachers. As an added measure of certainty, teachers in the intervention condition were requested not to exchange with their colleagues in control classes about the unfolding of the intervention in their classroom. In Norway, however, classes within schools did share the same teachers, and thus there existed a considerable risk of contamination between intervention and control classes. Therefore, in Norway, schools were randomly allocated to either the intervention or no-treatment control condition, and within each school, classes were selected to participate in the study, based on their interest to be part of it. An overview of the resulting randomized design is comprehensively presented in Figure 1. Figure 1 Overview of Cluster-Randomization in Belgium, Denmark, Norway, and the United Kingdom. 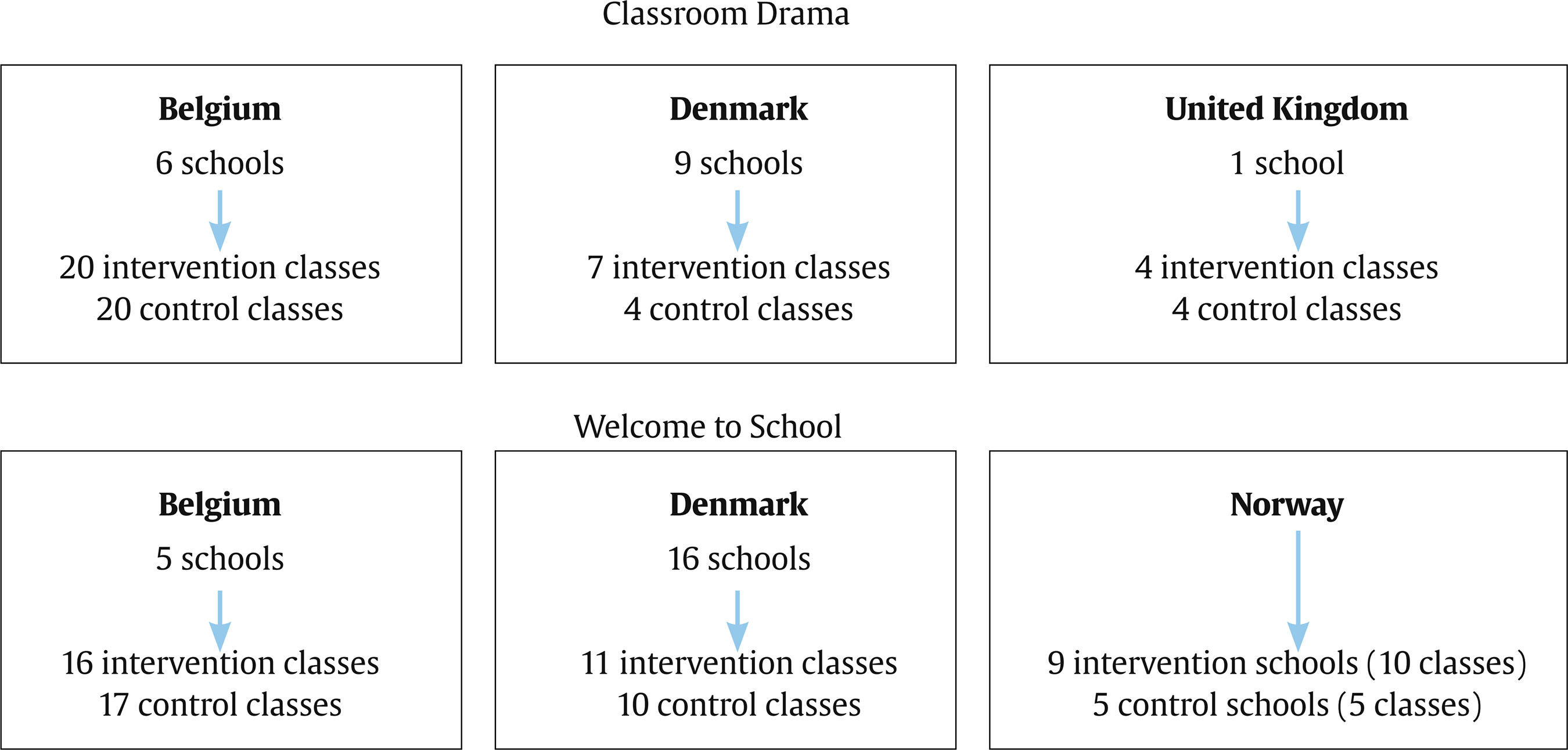 Participants In all schools, students were provided with information on the project through classroom-level information sessions, guided by the different research teams and students’ teachers. Corresponding to ethical guidelines for accessing and establishing trustful research relationships with refugee and migrant communities (e.g., de Smet et al., 2021), students were provided with tailored and exhaustive information on the study, using written information sheets in 22 languages and visual support through a PowerPoint presentation with images explaining the main aspects of the study. For students who needed it, professional interpreters were present during the information sessions in Belgium and Norway. In Denmark and the UK, students’ showed less need for translation, and students who did need additional help were provided with translation from an Arabic-speaking member of the research team (Denmark) or their peers (both in Denmark and the UK). In compliance with ethical standards on informed consent procedures with minors, additional consent of parents was sought for students below the nationally defined age for individual consent. Through close collaboration with school teams, we relied on a combination of strategies to reach out to parents, for example, introducing our study to parents at parent-teacher conference nights and organizing school-based collective information sessions about our study. Older participants could decide on their own participation and were given a complementary informed consent form for their parents only if they wanted to discuss their participation with their parents. All participants were assured they could withdraw from the study without an explanation. Both with adolescents and their parents, informed consent was thus approached as an active, relational, and iterative process, engaging with participants as true partners in the research process, as such supporting human agency and autonomy (e.g., Hugman et al., 2011). By its design, this study thus relies on separate samples for examining the effectiveness of the CD and WTS intervention. The two samples were composed of participants who completed both pre-test and post-test assessments. Covid-related school closures heavily affected our study, interrupting some of the ongoing interventions (cf. infra) and assessments and causing disproportionally high drop-out rates (> 65% drop-out in some contexts) in Belgium (for CD and WTS), Denmark (for WTS), and Norway (for WTS). Whereas pre-test assessment was realized with a total of 619 participants for CD (n intervention = 304, n control = 315), the final CD sample, thus including only participants who completed both pre- and post-test assessment, consisted of 307 participants (n Belgium = 105, n Denmark = 85, n UK = 117), aged 11 to 19 (mean age =14.27), of which 27.2% identified as female. Of the 307 participants, 146 were in the intervention group and 161 were in the control group. Participants’ migration motive, as indicated on a self-report demographic questionnaire, was used to distinguish participants who migrated because of reasons of war or persecution, ‘refugees’, from those who migrated because of other motives (e.g., work or education), ‘migrants’. Using this criterion, 30.8% of participants were categorized as refugees and 69.2% of participants in the CD sample were categorized as migrants. The sample was heterogeneous in terms of countries of origin, with participating youth being born in 58 different countries. Youth were mainly born in Syria (n = 42, 13.7%), Afghanistan (n = 23, 7.5%), Italy (n = 21, 6.8%), Somalia (n = 14, 4.6%), and Spain (n = 9, 2.9%). Participants in the CD sample had lived in their respective host countries between one and 13 years (mean = 1.97). For WTS, pre-test assessment was realized with 650 participants (n intervention = 411, n control = 239). The final sample for this study, including participants who completed both pre- and post-test assessment, consisted of 251 participants (n Belgium = 82, n Denmark = 69, n Norway = 100). Participants were between 11 and 23 years of age (mean = 15.07), and 47.3% of them identified as female. Of these 251 participants, 146 were in the intervention group and 105 were in the control group. Relying on the same method of categorization employed in the CD sample, 32.2% of the participants in the WTS sample were categorized as refugees and 67.8% as migrants. Like the CD sample, the WTS sample was heterogeneous in terms of countries of origin, with participants born in 46 different countries. Most youths were born in Syria (n = 36, 14.3%), Eritrea (n = 19, 7.6%), Afghanistan (n = 16, 6.4%), Pakistan (n = 8, 3.2%), and Romania (n = 7, 2.8%). Participants in this sample had lived in their respective host countries between one and five years (mean = 1.46). Interventions Classroom Drama The Classroom Drama (CD) intervention, developed in Montréal, Canada (Equipe Théâtre Pluralité d’Érit, 2010), is a nine-week series of drama workshops in which refugee and migrant adolescents in multi-ethnic schools engage in the construction of group stories, supporting identity and meaning-making in the aftermath of migration. The intervention engages with themes of migration, identity, exclusion, and cultural adaptation in the host society, aiming to support adolescents in establishing bridges between past and present life experiences and foster both adolescents’ well-being and the quality of classroom social relations. The CD intervention is facilitated by an external team of creative and/or drama therapists that enters the classroom and shapes the workshops using group rituals, improvisation exercises, and elements from Augusto Boal’s Theater of the oppressed (e.g., Boal, 1985) and Jonathan Fox and Jo Salas’ Playback theatre (e.g., Salas, 1999). While the intervention has been widely internationally implemented, it has only been systematically researched in a handful of studies. The findings of a Canadian pilot study (Rousseau et al., 2007) suggested CD had a promising impact on the adjustment of adolescent newcomers, whereby adolescents reported lower levels of perceived impairment by emotional and behavioral symptoms after receiving the intervention. The intervention had no significant impact on self-reported levels of mental health symptomatology, or self-reported levels of self-esteem. A Canadian randomized-control study (Rousseau et al. 2014) revealed more complex findings. In this study, CD was not associated with better mental health outcomes in first-generation refugee and migrant adolescents and was even related to higher levels of perceived impairment by symptoms in second-generation migrant youth (Rousseau et al., 2014). Last, a qualitative study of the intervention in Denmark described its potential to build social capital in classrooms (Dähne et al., in press). In the context of the WhatsApp project, CD was implemented in a total of 31 classes (N = 31) in Belgium, Denmark, and the UK. In Belgium, the intervention was led by a total of 18 therapists making up different creative teams, each composed of one drama/creative therapist and one drama teacher. These teams facilitated the workshop in a total of 20 newcomer classes in six schools (n = 20). In Denmark, a total of seven newcomer classes in seven schools (n = 7) received the intervention that was carried out by a team of two drama therapists. In the UK, the implementation of CD was equally done by a team of two drama therapists and targeted four classes in a multi-ethnic school (n = 4). As training, in all three countries, creative teams were provided with the intervention manual (Equipe Théâtre Pluralité d’Érit, 2010) and introduced to its content during a day-long meeting and exchange with the research teams. Afterward, the teams shaped the workshop based on the intervention manual but were allowed some degrees of therapeutic and creative freedom to adapt the workshops according to the themes and dynamics prevalent in each of the classrooms receiving the intervention. In all countries, the creative teams worked side-by-side, closely together with the classroom teachers in providing the intervention. Implementation of CD in Denmark occurred between January and May 2019, and in the UK between February and May 2019. Implementation fidelity was monitored through the use of checklists that had to be completed by both the creative teams and teachers surrounding each intervention session. In their checklists, creative teams were asked to report on their planning of each session and to reflect back on the sessions’ effective conduct. Filled in after each session, teachers’ checklists monitored the course of sessions, by asking questions such as “Was the classroom a safe space during the session?”; “Were students engaged in the session?”; “What themes arose during the session?”. In addition, regular contact between the research teams, teachers, and creative teams was maintained throughout the implementation process. In Belgium, the implementation of CD started in January 2020 but was halfway interrupted when schools closed in March 2020 due to the outbreak of the Covid-19 pandemic. In response to this interruption of the intervention, the Belgian research team, in close collaboration with the creative teams, developed three videos for students involved in the intervention. In the first video, the creative teams emphasized their connection with students and their proximity to them during the period of confinement. The second video built on intervention processes that were underway before schools closed and invited students to participate in the development of a group assignment based on creative and group dynamic exercises central to CD. A third and final video presented students’ responses to the second video which had been integrated by the creative teams to form a final creative product of the intervention. All videos were shared with students in collaboration with their teachers and creative teams and through the use of online school and social media platforms (e.g., Facebook, Instagram, Whatsapp). While some students explicitly responded to the videos and their invitation to participate in the development of a shared creative product, other students were never reached. Response rates to the videos in all classes ranged from zero to almost 30%, reflecting a general loss of connection and the difficulties experienced by many refugee and migrant youth to engage with their schooling during the period of home confinement (e.g., Primdahl et al., 2021). Welcome to School The second intervention evaluated in this study was Welcome to School (WTS), developed by Pharos Refugees and Health Knowledge Centre (the Netherlands; Pharos, 2015). The WTS intervention constitutes a group discussion program that brings together refugee and migrant students under the guidance of their classroom teacher. WTS provides teachers with a manual and students with a WTS workbook that allows them to engage in weekly classroom group discussions aimed at supporting students’ well-being through fostering social support and cohesion in the classroom. In its original form, WTS consists of a total of 21 weekly sessions in which students are invited to share experiences and engage in group discussions on themes of migration, identity, culture, and social relations. The classroom discussions are facilitated by the classroom teacher and supported through the combined use of both verbal exercises and non-verbal activities (e.g., role-playing and drama exercises, drawing, and photo collages). Within the framework of the RWS project, the intervention was shortened to 14 weekly sessions to accommodate the project’s timeline (Tuk & de Neef, 2020a, 2020b). This shortening of the program was done in close collaboration with the original intervention developers, the different research teams, and school actors in participating schools in Belgium, Denmark, and Norway. Scholars have pointed to WTS’ potential in strengthening refugee and migrant adolescents’ well-being through fostering social support in school (e.g., Ingleby & Watters, 2002). WTS was implemented in a total of 39 newcomer classes in 24 schools (N = 39) in Belgium (n classes = 16, n schools = 5), Denmark (n classes = 13, n schools = 10), and Norway (n classes = 10, n schools = 9). In all countries, teachers were provided with the intervention materials (Welcome to School teacher manual and Welcome to School student workbook) and invited for a meeting with the research teams in which the intervention and materials would be further introduced. However, only in Norway did the teacher prefer to participate in such a meeting and familiarize themselves with the materials together with the research teams. In Belgium and in Denmark, after seeing the materials, teachers indicated that they felt comfortable enough to start implementing the intervention. As with CD, teachers were provided with checklists to allow for the monitoring of implementation fidelity in each class. Checklists had to be completed after each session and inquired into the planning and conduct of each session, with questions such as “How did the session go?”; “Was the classroom a safe space during the session?”; “Were students engaged in the session?”; or “What themes arose during the session?”. Covid-19-related school closures affected the implementation of WTS, planned in all three countries during the spring of 2020. Most schools and classes were about halfway implementing WTS when schools closed. All three national research teams discussed the possibility of an online continuation of the intervention with schools and teachers but in none of the countries, such a scenario was deemed feasible. The Belgian research team collaborated with WTS teachers to create a short video expressing their support and continued connection to the intervention that was sent to all students receiving the intervention. One school in Norway and five classes in Belgium provided a closing WTS session after schools reopened in June 2020. Overall, both CD and WTS thus constituted preventive psychosocial care interventions, which aim to engage young people in topics related to identity, social relations, migration, and daily experiences in the host society. It is important to note that these interventions were not meant to directly address traumatic experiences in youth, though working around the aforementioned themes might for some adolescents touch upon or elicit traumatic life stories and experiences. For these cases, we provided guidelines and support to teachers and creative teams to ensure that young people receive adequate care, and put a follow-up plan in place should the interventions reveal in some youth a need for specialized trauma or mental health care. Figure 2 Timelines Underlying National Intervention Implementation and Assessments. 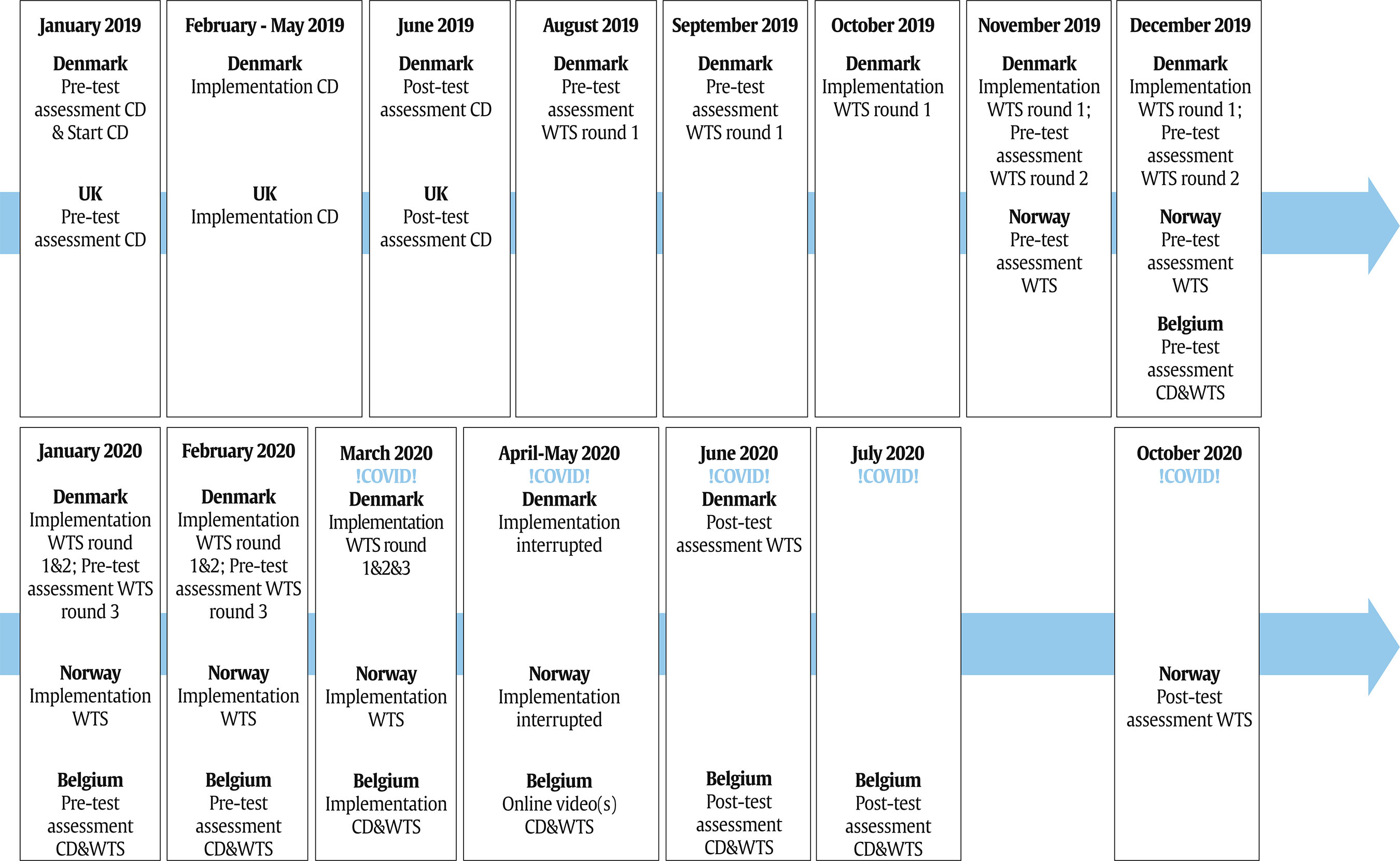 Procedure Participants completed self-report questionnaires at two points in time, preceding (pre-test) and after (post-test) the implementation of the interventions. All questionnaires had been translated and back-translated into a total of 22 languages. Pre-test assessment in all four national contexts was conducted in the classroom, supported by the different national research teams and classroom teachers, and in Belgium and Norway also by professional interpreters. In Denmark and the UK, students showed no need for additional assistance from professional interpreters in filling out the (translated) questionnaire. Questionnaires were completed either on paper (in Belgium preceding both CD and WTS, and in Denmark preceding the implementation of CD) or online, using LimeSurvey software (LimeSurvey Project Team/Carsten Schmitz, 2012) (in Norway, the UK, and Denmark preceding the implementation of WTS). Post-test assessments that took place before Covid-19-related school closures were conducted again in the classroom, using LimeSurvey (in Denmark and the UK following CD). Following the interrupted implementation of CD in Belgium and WTS in all three countries, questionnaires were completed through LimeSurvey by students at home (Belgium and Denmark) or at school (Norway), through links provided by the research teams in collaboration with students’ classroom teachers. In Belgium, the post-test online assessment included audio translations of the questionnaire in six languages (Arabic, Pashto, Dari, Kurmanji, Turkish, and Somali) that were integrated into LimeSurvey to support students who at pre-test showed to need extensive support from professional interpreters in completing the questionnaire. In Denmark and Norway, the research teams assessed that adding audio translations was not necessary for the youth in their sample. Post-test assessments took place immediately after the implementation of the interventions. In Norway (WTS) and Belgium (CD & WTS), though due to the closing of schools more time passed between the last session of the interventions and the post-test assessment. Figure 2 was designed to support readers’ insight into the different national timelines underlying the implementation of both interventions, the pre- and post-test assessments, and the impact of Covid-19-related school closures on the study in each of the national contexts. Measures The self-report questionnaire completed by participating students was composed of the following scales. Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997; 2001) The SDQ was used to measure emotional and behavioral difficulties. This 25-item self-report measure has been well-validated, translated into over 40 languages, and extensively used with culturally diverse study populations (Bourdon et al., 2005; Goodman, 2001). Participants scored each item on a three-point Likert scale with 0 = not true, 1 = somewhat true, and 2 = certainly true. Summing up their scores, we calculated total mental health difficulties scores (range 0-40) as well as two subscale scores (internalizing and externalizing behavioral difficulties, range 0-20; Goodman et al., 2010). Children’s Revised Impact of Events Scale-8 (CRIES-8; Perrin et al., 2005) The CRIES-8 was administered to measure participants’ self-reported symptoms of post-traumatic stress (PTSS). The CRIES-8 was developed for use with eight- to 18-year-old children and adolescents and consists of eight items inquiring about PTSS of intrusion and avoidance. Participants scored each item on a four-point Likert-scale with 0 = not at all, 1 = rarely, 3 = sometimes, and 5 = often. The total score of the measure ranges between zero and 40. The CRIES-8 has demonstrated good validity and internal consistency (Magalhães et al., 2018) and has furthermore shown its value as a screening measure for PTSD in refugee children and adolescents (e.g., Salari et al., 2016). Well-being was assessed using one item “How would you rate your overall well-being?”, with the following answer options and corresponding scoring: very bad = 1, bad = 2, normal = 3, good = 4, and very good = 5 (see also Spaas, Verelst, et al., 2022). Brief Child and Youth Resilience Measure (CRYM-12; Liebenberg et al., 2013) The CRYM-12 aims to assess participants’ resilience through 12 items inquiring about the availability and participants’ trust in the availability of individual-, peer-, family-, school-, and community-level resources. The CRYM was developed through a mixed-method design aimed at gaining an in-depth understanding of both common and unique factors of resilience across cultures. The measure has good content-related validity and is generally accepted to constitute a culturally sensitive measure of resilience (e.g., Ungar & Liebenberg, 2011). Participants scored each item on a five-point Likert-scale with 1 = not at all, 2 = a little, 3 = somewhat, 4 = quite a bit, and 5 = a lot. Multidimensional Scale of Perceived Social Support (MSPSS; Zimet et al., 1988) Two subscales of the MSPSS were used to assess participants’ perceptions of the adequacy of social support they received from friends and family. The MSPSS has previously shown good reliability and validity when administered to adolescents in diverse settings (e.g., Chou, 2000). Participants scored each item on a four-point Likert scale with 1 = not at all, 2 = a little, 3 = quite a bit, and 4 = a lot. Psychological Sense of School Membership (PSSM; Goodenow, 1993) The PSSM measures participants’ self-reported sense of school belonging. The PSSM has previously been used and validated in research with young refugees (Kia-Keating & Ellis, 2007). Within the framework of this study, a shortened version of the PSSM was used, with nine items inquiring into participants’ perceptions of feeling accepted, included, and treated well in school. All items were scored on a five-point Likert scale with 1 = not at all true, 2 = a bit true, 3 = more or less true, 4 = very true, and 5 = completely true. Brief Perceived Ethnic Discrimination Questionnaire (PEDQ) The Exclusion and Discrimination Subscale of the PEDQ was used to assess participants’ experiences of perceived discrimination. The PEDQ has previously been shown to possess good psychometric qualities and to be reliable when used with adolescent and culturally diverse study populations (Brondolo et al., 2005). Participants scored each item on a four-point Likert-scale with 1 = never, 2 = sometimes, 3 = often, and 4 = always. Participants could also withhold from answering in case they did not know the answer to an item or felt uncomfortable answering it (answering option “I don’t know”/”I don’t want to answer”). Within the whole of studies conducted through RWS project, the different scales were proved to be reliable and valid for use with the participant sample under study (Spaas, Verelst, et al., 2022; Verelst et al., 2022). In these studies, Cronbach’s alpha reliability values for all measures were estimated between .71 and .94, indicating acceptable internal consistency (Nunnally & Bernstein, 1994). Analyses Quantitative data analyses were performed using the software R (version 4.2.0) and started with descriptive analyses to obtain a summary of the data for the whole samples and the data per country in each sample. Next, using the package lmerTest (Kuznetsova et al., 2017), a series of three-level random intercept linear regression models, using the restricted maximum likelihood (REML) procedure, were fitted to the data. These models assessed the effect of each intervention on each outcome, relying on adolescents’ score difference (post-test score minus pre-test score) and taking into account shared variance among adolescents in the same school or class (Peugh, 2010). Country was not modeled for as an additional level since the study design with only three countries per intervention precluded reliable estimation and meaningful interpretation of cluster variance at this level (Gelman & Hill, 2006). Based on an unconditional model (i.e., a model without any predictors), the intraclass correlation coefficient (ICC) was estimated at the school and classroom level for each outcome to explore the amount of between-group variance at each level. ICC estimates exceeding .05 suggest substantial between-group variance. However, even in cases with a low ICC estimate, we relied on multilevel regression rather than ordinary regression to maintain consistency in reporting the results and avoid potentially biased estimates due to ignoring the nested structure of the data (Bliese et al., 2018). To assess the effect of the interventions on each outcome, we added predictors to the unconditional models using a two-step approach: (i) a model (Model 1) including a dummy-coded group variable (0 = control group, 1 = intervention group) and (ii) a model (Model 2) including the intervention group variable and the following covariates: country (0 = Belgium, 1 = Denmark, 2 = Norway or UK), age, gender, reason for migration (0 = migrant, 1= refugee), time in country, and proportion of intervention sessions completed (to control for differences in intervention delivery due to school closures). Finally, we fitted three additional models per outcome, including interactions between the group and baseline scores of mental health symptomatology (SDQ and CRIES total baseline scores, Models 3 and 4 respectively) and resilience (CYRM total baseline score, Model 5), as well as another model including the interaction between the group and country (Model 6). The goal of these model estimations was to explore whether the intervention effect on each outcome was perhaps moderated by participants’ baseline mental health or resilience (Nunes et al., 2011) or the country context in which the intervention was implemented. Continuous predictors were grand mean-centered in all regression models. Cohen’s d effect size was computed for significant effects involving the group using the package Effect Size (Ben-Shachar et al., 2022). Interpretation of these effect sizes followed Cohen’s (1992) guidelines, whereby 0.20 is small, 0.50 is medium, and 0.80 is large. Post hoc multiple comparisons with Tukey adjustment were conducted for significant group-by-country interactions using the package Emmeans (Length, 2018). Ethical Considerations Ethics approval for the RefugeesWellSchool project was granted by Ghent University’s Ethics Commission and all countries involved ensured additional ethics approval from their respective national or university’s Ethics Commissions. Descriptive statistics for the experimental and control groups in each intervention on the pre-test and post-test scores for each outcome variable are provided in Table 1. Due to significant differences identified between the two control groups of CD and WTS in the outcome variables, separate analyses were conducted for the two interventions. Across all the outcome variables, the percentage of missing data varied between 2.28% and 21.82% in the CD dataset and between 3.18% and 18.73% in the WTS dataset. The missing data were imputed by chained equations implemented in the package Mice (Van Buuren & Groothuis-Oudshoorn, 2011). Twenty imputations were performed (following the rule that the number of imputations should approximate the percentage of missing data), incorporating all covariates involved in the analysis models to avoid introducing bias in the results (White et al., 2011). Analyzing these imputed datasets yielded results comparable to our initial analyses of the unimputed datasets. This indicates that the missing data were not significantly biasing our results, and we, therefore, report on the unimputed datasets. In the CD analyses, ICC estimates ranged from < .01 to .26 for schools and from < .01 to .16 for classes within schools. In the WTS analyses, ICC estimates ranged from < .01 to 0.08 for schools and from < .01 to .15 for classes within schools. Table 1 Means and Standard Deviations of Pre-Test and Post-Test Scores of the Outcome Variables in the Classroom Drama and Welcome to School Sample 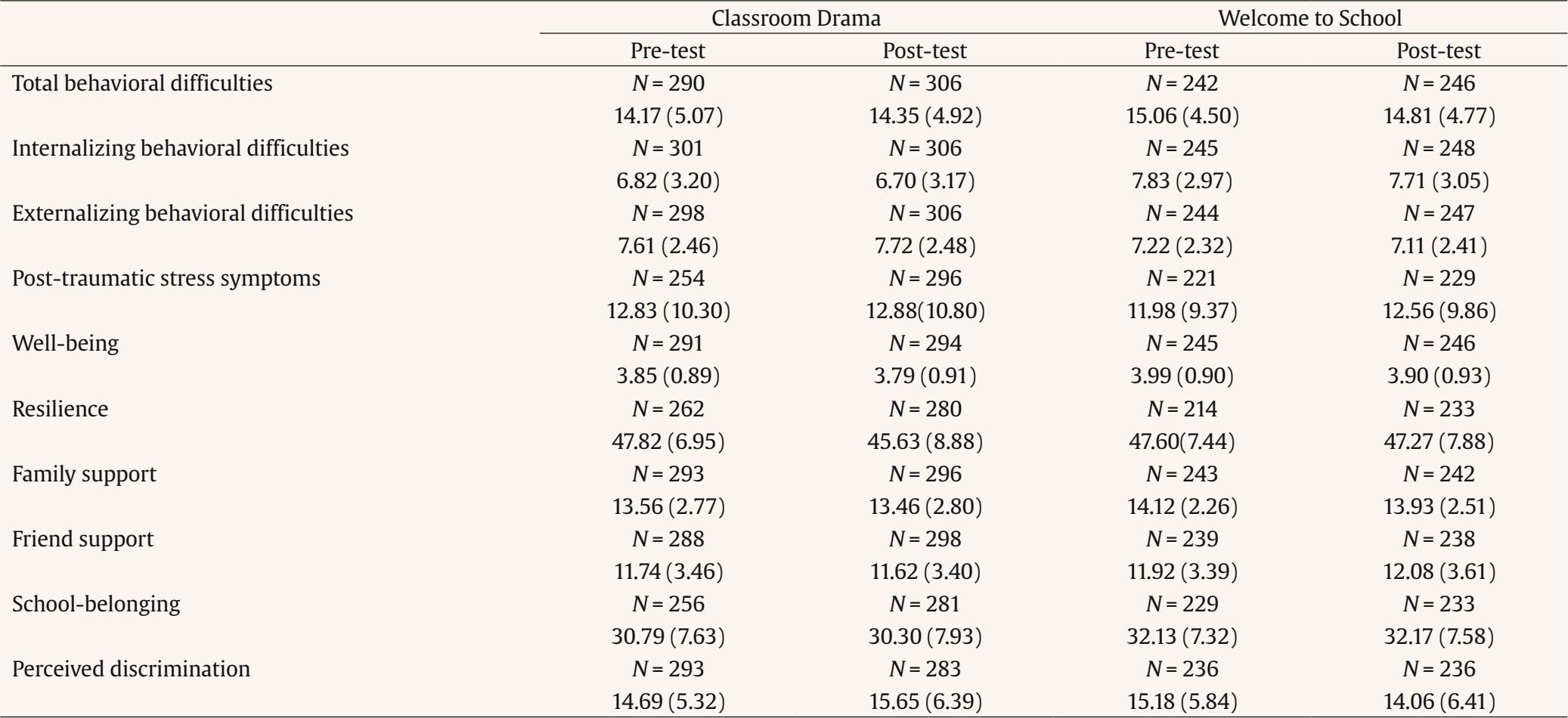 Note. Mean (SD); minimum and maximum scores: total behavioral difficulties: 0-40; internalizing and externalizing behavioral difficulties: 0-20; post-traumatic stress symptoms: 0-40; well-being: 1-5; resilience: 12-60; family and friend support: 4-16; school-belonging: 9-45; perceived discrimination: 9-36. Classroom Drama In order to reflect on the clinical significance of participants’ mental health difficulties at baseline, participants’ scores were categorized using cutoff scores employed in large population-based surveys. For PTSS the cut-off scores for clinical range were applied (Perrin et al., 2005). According to this classification, for participants completing all items of the CRIES-8 a sum score above 17 corresponds to a clinical level of symptomatology, indicating a high probability of meeting the criteria for PTSD diagnosis (American Psychiatric Association, 2013). For total, internalizing and externalizing behavioral difficulties, cut-offs were calculated based on the 90th percentile of a large-scale British population survey (Youth in Mind, 2018). Based on these categorizations, 14.1% of participants in the CD sample reported high levels of behavioral difficulties and 34.3% scored above the clinical cut-off for PTSD at baseline. Figure 3 Interaction Plot of the Group-by-Country Effect for Friend Support. 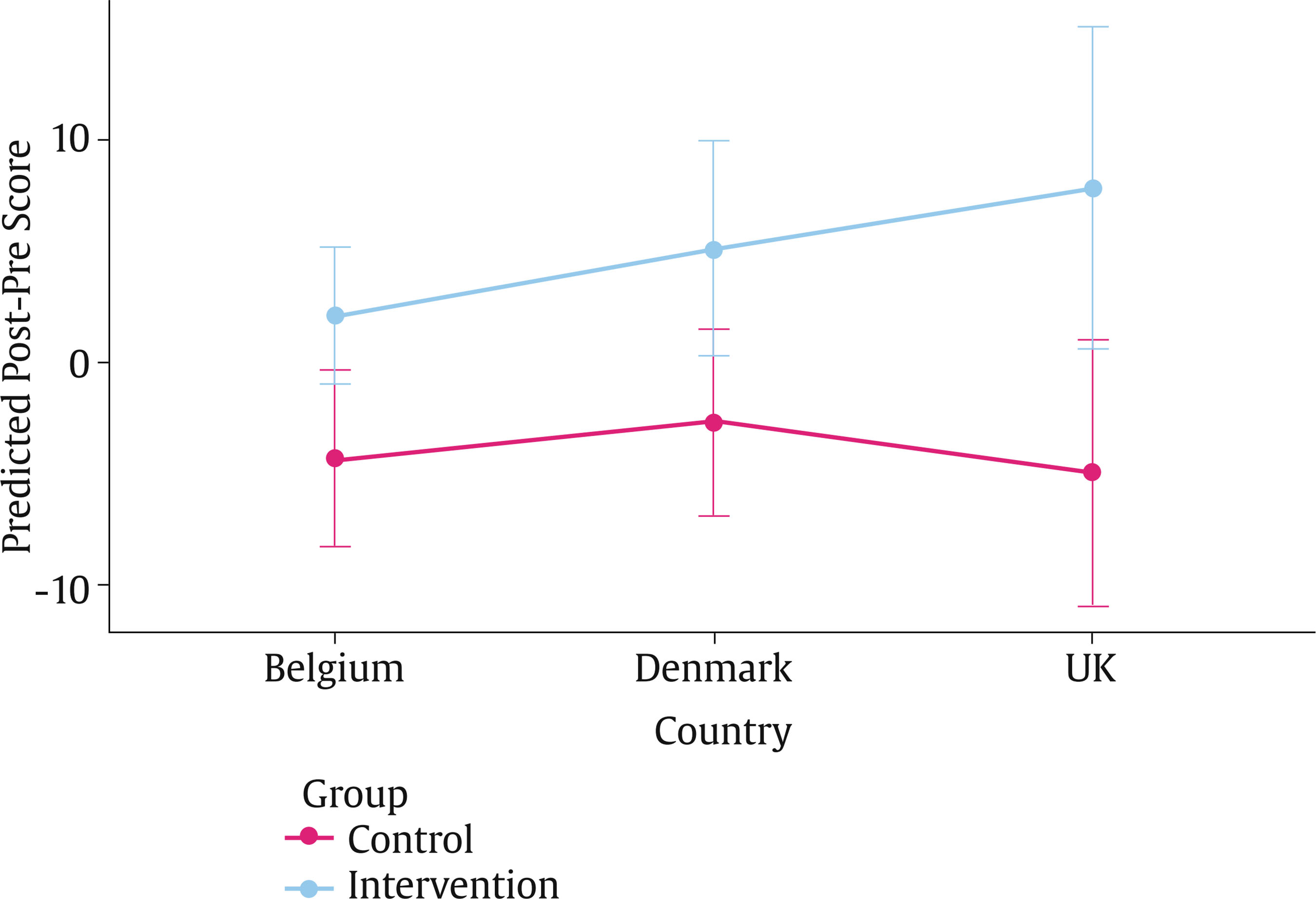 In Supplementary materials, Table S1 presents the parameter estimates and corresponding standard errors for all multilevel models for each outcome. With regard to the outcomes of social relations, significant effects were found for the group variable on “family support”. Model 2 suggested an increase in “family support” in the intervention group (β = 2.03, p = .07) compared with a decrease in the control group (β = -1.52, p = .12), yet both changes were not statistically significant. Similar trends were observed for the effect of the group variable on “family support” in Model 3 (β = 1.86, p = .10 for the intervention group, and β = -1.45, p = .14 for the control group) and Model 6 (β = 1.96, p = .15 for the intervention group, and β = -1.23, p = .30 for the control group). The corresponding effect size was small in Models 2 and 3 (d = 0.4 and 0.38 respectively) and medium in Model 6 (d = 0.75). In addition, the group-by-country interaction in Model 6 was significant for “friend support”. Post-hoc analysis detected a significant, large difference (d = 1.19) between the intervention group and the control group in the UK in “friend support” (t = 3.10, df = 27, p = .04), in that the intervention group showed a non-significant increase (mean difference = 7.70, p = .06) whereas the control group showed a non-significant decrease (mean difference = -5.13, p = .06). Figure 3 illustrates this group-by-country interaction. No other statistically significant differences were identified in other countries. Model 6 also revealed a significant group-by-country interaction for school belonging, though post hoc analysis did not detect any significant pairwise differences. No significant main effects of the group variable on the different mental health outcomes were found. Yet, Model 5 revealed a significant group by baseline resilience interaction for some outcomes. Specifically, higher baseline resilience was associated with a larger increase in the “total” (β = 0.23, p = .003) and “internalizing” (β = 0.14, p = .004) behavioral difficulties in the control group, compared with a non-significant change in the intervention group (β = 0.02, p = .83 for the “total” behavioral difficulties and β = 0.01, p = .82 for “internalizing”). The corresponding effect sizes were small (d = -0.33 for the “total” behavioral difficulties and d = -0.30 for “internalizing”). Furthermore, higher baseline resilience was associated with a greater decline in “well-being” in the control group (β = -0.04, p = .004), compared with a non-significant change in the intervention group (β = 0.01, p = .64). The corresponding effect size was also small (d = 0.39). Welcome to School Population research-based clinical classification of participants’ mental health at baseline followed the same categorization as in the CD sample. In the WTS sample, 17.6% of participants reported high levels of behavioral difficulties and 33.9% scored above the clinical cut-off for PTSD at baseline. In Supplementary materials, Table S2 presents the parameter estimates and corresponding standard errors for all multilevel models for each outcome. No significant main or interaction effects of the group variable on any of the outcomes of mental health or social relations were found. Although Model 6 revealed a significant group-by-country interaction for “externalizing behavioral difficulties”, no significant pairwise differences were detected in the post hoc analysis. In light of increasing scholarly and policy emphasis on school-based psychosocial interventions to support refugee and migrant youth, this study used a cross-country, cluster randomized design to examine the effectiveness of the CD and WTS intervention in fostering young refugees’ and migrants’ mental health and social relations. Herewith, this study set out to strengthen the evidence base on school-based psychosocial interventions for refugees and migrants, while answering to scholarly call for the use of more robust study designs including both mental health and social outcomes in the development of this evidence base (e.g., Tyrer & Fazel, 2014). In accordance with previous studies, our study confirms the mental health vulnerability of young refugees and migrants. The young people in our study reported elevated levels of mental health difficulties, compared to levels reported by their peers in population-based studies (e.g., Lukaschek et al., 2013; Wright et al., 2020). These high levels of baseline mental health difficulties are in line with previous European studies of the mental health of young refugees and migrants (e.g., Dimitrova et al., 2016; Kevers, Spaas, Colpin, et al., 2022; Kien et al., 2019; Spaas, Verelst, et al., 2022) and confirm the need for psychosocial care for this population. Studied in Belgium, Denmark, and the UK, for CD, a significant main effect of the intervention on perceived family support was found: whereas the control group on average reported a decrease in family support, the intervention group reported increased levels of perceived support from family members. By focusing on working around themes and (family) stories of migration and exile, the CD intervention might have positively altered youth’s perceptions of their family relations, or instead, promoted supportive interactions between young people and their family members through facilitating intra-family communication on central life experiences of migration and exile. Indeed, previous scholarly work points to the important role of family relations and family processes of trauma communication in young refugees’ and migrants’ well-being. Studies, for example, emphasize the protective nature of family support and balanced communication surrounding life experiences of migration and exile for children’s development, mental health, and processes of post-trauma restoration in resettlement (e.g., De Haene & Rousseau, 2020; Kevers et al., in press; Reed et al. 2012; Scharpf et al., 2021). While our study did not engage in an exploration of the working mechanisms underlying the effect of the intervention on family support, the effect does suggest a positive influence of the intervention that might extend beyond the school context into refugees’ and migrants’ homes. However, the intervention’s effect on family support should not be overestimated, as the effect size was rather small and the effect was not significant in those models testing interaction with baseline resilience. The study also showed that the effect of the CD intervention on perceived friend support was not significant, yet this effect was found to be moderated by country. In the UK, the intervention group reported an increase in perceived friend support, whereas the control group reported a decrease in perceived friend support. This finding suggests that, in the UK context, the intervention might have succeeded in promoting a positive classroom atmosphere where refugee and migrant youth felt supported by their peers, an atmosphere that perhaps countered stressors negatively impacting perceived levels of support from friends in the control group. Potentially interesting to take into account here is the fact that only in the UK context CD was implemented in a multi-ethnic school context other than that of reception education. Here, CD might have succeeded in shaping dynamics of support between newcomer students and students who have resided in the host country for a longer period of time. Findings from a previous qualitative study on CD also suggest that the intervention has the potential to promote social capital in the classroom (Dähne et al., in press), and another mixed-method study on a similar intervention implemented with refugee and migrant children in multi-ethnic primary schools showed that the intervention improved the quality of classroom social relations (Kevers, Spaas, Derluyn, et al., 2022). Taken together, this evidence suggests that school-based creative interventions might have the potential to promote positive peer interactions and social support in the classroom, known to be important determinants of refugees’ and migrants’ mental health in resettlement (e.g., Schachner, 2018). Aside from its effect on family support, the CD intervention did not have any significant main effect on the other outcomes. Previous investigation of this intervention in Canada similarly reported no significant effects of the intervention on youth’s mental health symptomatology (internalizing and externalizing behavioral difficulties and PTSS) but did find a beneficial impact of CD on perceived impairment by their symptoms, a measure not included in our study (Rousseau et al, 2007). Perhaps CD mostly succeeded in promoting supportive relations as potential protective factors that could influence youth’s mental health indirectly. In this case, an effect of the intervention on mental health outcomes might take longer to unfold than captured by the timeline of our study. Nevertheless, the current study did show that baseline resilience moderated the effect of the CD intervention on the total and internalizing behavioral difficulties as well as its effect on well-being. Higher baseline resilience was found to be related to an increase in the total and internalizing behavioral difficulties in the control group versus a non-significant change in the intervention group. It was also found to be related to a decrease in well-being in the control group versus a non-significant change in the intervention group. It is possible that experiencing safety within the school and research context might have fostered in highly resilient participants a more open disclosure of difficult experiences between pre- and post-test assessment. Indeed, findings from focus group research with some of the participants suggest they mobilized school-based and research relations to address difficult experiences, such as discrimination, within the framework of the larger RWS study (Spaas, Verelst, et al., 2022). In this case, the increased reporting of symptoms in the control group might not represent increased psychosocial suffering between pre- and post-test assessment, but rather form an indication of underreporting of symptoms at pre-test assessment. Indeed, scholarly literature highlights the complexities of self-reporting psychological suffering and stressful life experiences, such as discrimination, in research with refugee and migrant communities (e.g., Spinhoven et al., 2006). Alternatively, rooted in socio-ecological perspectives on resilience (e.g., Ungar, 2011) we propose that it could also be that participants describing themselves as highly resilient at baseline fared more poorly over time because they were faced with novel stressors with which the resources they possessed did not align (e.g., discrimination). Relatedly, those with lower levels of resources might have been familiar with a broader variety of previous adverse life experiences, instigating a ‘steeling effect’ that supported coping with current adversity (e.g., Rutter, 2012). In all possible scenarios, the observed interaction effects potentially suggest that, for those with higher levels of resilience at baseline, the intervention might have succeeded in mitigating the detrimental impact of stressful life experiences on mental health and well-being, perhaps through fostering social support. Studied in Belgium, Denmark, and Norway, the WTS intervention did not show to have an effect on any of the outcomes of mental health or social relations. The implementation of the WTS intervention was interrupted by the Covid-19-related school closures in all country contexts, rendering the impossibility of completing the intervention the most important explanation for the lack of effects found. Precisely because of the impact of the Covid-reality on the study and perhaps also on participants’ well-being and social relations, irrespective of the intervention (e.g., Hodes, 2022), it does not seem indicated to put forward alternative hypotheses explaining the absence of intervention effects in our study. A previous study on WTS demonstrated a positive dose-response effect of the intervention on emotional behavioral difficulties in refugee and migrant youth (Brunak et al., 2022). These findings suggest the intervention has potential in supporting young refugees’ and migrants’ mental health, but future systematic studies remain needed to further develop the evidence base on WTS. Overall, this study generates modest, preliminary evidence on the effect of the CD intervention in fostering social support from family and friends and a potential buffering effect of the intervention on the well-being and mental health of youth with the highest levels of resilience at baseline. It provides an argument for taking into account outcome measures of social relations in the evaluation of school-based interventions for refugee and migrant youth. Understanding interventions’ effectiveness in improving youth’s social relations is of particular relevance given the growing body of scholarly work that emphasizes the central role of school-based and host society relations in shaping young refugees’ and migrants’ well-being and mental health in resettlement (e.g., Schachner et al., 2018; Spaas et al., 2022; Spaas, Verelst, et al., 2022). Strengths, Limitations, and Future Research This study has various strengths and answers to several of the previously identified gaps in the scholarly literature on school-based interventions for refugee and migrant youth. First, as one of few existing studies to include outcome measures of young refugees’ and migrants’ social relations (e.g., Bal & Perzigian, 2013; Kevers, Spaas, Derluyn, et al., 2022), this study provided nuanced, new insight into school-based intervention’s effectiveness by uncovering the impact of the CD intervention on central social determinants of refugee and migrant mental health, namely social support from family and friends. Second, the cluster randomized design and relatively large sample size of this study lend often-called-for robustness to its findings and its contribution to the evidence base on school-based psychosocial interventions for refugees and migrants (e.g., Tyrer & Fazel, 2014). Third, equally fostering the study’s robustness are its multilevel analyses that accounted for contextual level differences on the levels of schools and classrooms, while also considering potential baseline-treatment interactions and country-level interaction effects in assessing the interventions’ effectiveness. Fourth, the use of iterative and tailored informed consent procedures, translated research materials, and cross-culturally validated and translated questionnaires, as well as the collaboration with professional interpreters throughout the study correspond to central ethical-methodological guidelines on fostering autonomy and agency of refugee and migrant participants in research practices (e.g., de Smet et al., 2021). Fifth, the research teams’ commitment to developing strong and positive relations with and between school actors and creative teams supported the careful monitoring of the implementation of CD and WTS and, in Belgium, even allowed for the realization of brief intervention-related videos shared with participants after their schools closed in March 2020. While it is unlikely these short videos represented actual intervention doses, post-intervention focus groups with participants suggested that participants who successfully received and watched the videos experienced being cared for during home confinement and “not forgotten” by their teachers and the creative teams. Overall, we believe this study enriches the existing scholarly evidence base on school-based psychosocial interventions by uncovering one intervention’s potential for fostering young refugees’ and migrants’ social relations and mental health. However, the limitations of our study should equally be noted. A first and clear limitation of this study concerns the extent to which it was impacted by the outbreak of the Covid-19 pandemic and the ensuing school closures between the spring and summer of 2020. The Covid reality led to an interruption of ongoing interventions in some study sites, altered the timing and procedure of planned assessment in several country contexts, and also caused a significant drop-out of participants. This drop-out and the study’s lower final sample size reduced the power of the study. Furthermore, as our analysis included only data on participants assessed at two time points, this study perhaps excluded some of the most vulnerable refugee and migrant youth who experienced barriers engaging with school through internet-based home learning (e.g., Hodes, 2022). Also, the pandemic and experiences of home confinement themselves might have negatively impacted participants’ mental health and social lives (e.g., Hodes, 2022), thus yielding a potentially confounding influence on the central outcomes of this study. A second limitation of our study lies in the heterogeneity of procedures and timelines underlying the study designs in each of the four countries. While attempted to control for in the analyses, differences in recruitment strategies, type of school settings, randomization procedures, the timing of intervention implementation and assessments might have weakened the study’s overall rigor and influenced its results. Third, while our sample was of considerable size compared to similar studies with our study population (e.g., Tyrer & Fazel, 2014), a larger sample would have ensured higher analytical power, particularly in the post hoc analyses. Last, the study’s outcomes and conclusions apply only to the countries and particular school settings in which the data were collected and cannot readily be generalized to refugee and migrant youth in alternative school settings or elsewhere in the world. Therefore, it is important to note that this study exclusively involved high-income countries, while low- and middle-income countries host the largest populations of refugees worldwide (UNHCR, 2022). As emerging research on school-based interventions in these countries shows promising results (e.g., Charbonneau et al., 2022; Sullivan & Simonson, 2016), future school-based intervention research could meaningfully engage in an exploration of the way context and intervention mechanisms operate and interact to support refugee and migrant minors around the world (e.g., Sullivan & Simonson, 2016). We recommend future studies continue to include outcome measures on youth’s social relations in their designs, meaningfully broadening their focus on understanding school-based intervention effectiveness in supporting the well-being of refugee and migrant youth beyond an emphasis on individual mental health symptomatology. In light of the complexity of our findings, we believe that future studies could also benefit from an integration of rigorous quantitative and qualitative methodologies to develop a further in-depth understanding of school-based interventions’ potential in caring for young refugees and migrants resettling in Europe. While CD could still benefit from additional research in larger samples, using mixed methodologies, the WTS intervention surely requires further evaluation, as the incompletion of the intervention in all countries limited our study’s potential to make reliable statements on its effectiveness in supporting refugee and migrant youth. Conflict of Interest The authors of this article declare no conflict of interest. Acknowledgments We are foremost grateful to all the young people and school partners with whom we were privileged to collaborate throughout this study. We want to thank Dr. Philip Jefferies at Dalhousie University for his readiness to reflect with us on our findings concerning resilience. Cite this article as: Spaas, C., Said-Metwaly, S., Skovdal, M., Langer Primdahl, N., Smith Jervelund, S., Kristian Hilden, P., Andersen, A. J., Opaas, M., Soye, E., Watters, C., Verelst, A., Derluyn, I., Colpin, H., & De Haene, L. (2023). School-based psychosocial interventions’ effectiveness in strengthening refugee and migrant adolescents’ mental health, resilience, and social relations: A four-country cluster randomized study. Psychosocial Intervention, 32(3), 177-189. https://doi.org/10.5093/pi2023a12 Funding: This project has received funding from the European Union’s Horizon 2020 research and innovation program under grant agreement No 754849. Supplementary data Supplementary data are available at https://doi.org/10.5093/pi2023a12 |
Cite this article as: Spaas, C., Said-Metwaly, S., Skovdal, M., Primdahl, N. L., Jervelund, S. S., Hilden, P. K., Andersen, A. J., Opaas, M., Soye, E., Watters, C., Verelst, A., Derluyn, I., Colpin, H., & Haene, L. D. (2023). School-based Psychosocial Interventions’ Effectiveness in Strengthening Refugee and Migrant Adolescents’ Mental Health, Resilience, and Social Relations: A Four-country Cluster Randomized Study. Psychosocial Intervention, 32(3), 177 - 189. https://doi.org/10.5093/pi2023a12
Correspondence: caroline.spaas@kuleuven.be. (C. Spaas).
Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
Send






