


Effectiveness Evaluation of a Violence Prevention Parenting Program Implemented at Large Scale: A Randomized Controlled Trial
Elisa Rachel P. Altafim and Maria Beatriz M. Linhares
RibeirĂŁo Preto Medical School, University of SĂŁo Paulo, Brazil
https://doi.org/10.5093/pi2025a6
Received 9 July 2024, Accepted 22 January 2025
Abstract
Parenting programs can enhance positive parenting, reduce harsh parenting, and positively impact children’s development. This two-arm randomized controlled trial examined the effectiveness of the parenting program, the ACT Action Program - Raising Safe Kids, on parenting practices (primary outcomes), parental sense of competence, stimulation activities, and children’s behaviors (secondary outcomes) in low-income families. The sample consisted of 1,310 caregivers and their 0-to-6-year-old children from 17 municipalities in a Brazilian state, with the majority receiving cash transfers (governmental monetary support for families facing vulnerabilities). The caregivers were randomly allocated into the intervention (IG, n = 639) or waitlist control (CG, n = 671) groups. The IG participated in the ACT Program during an 8-week-in-person group session to strengthen positive parenting, and the CG in the usual care. The caregivers answered the questionnaires administered by the facilitators in the pre-intervention (after the randomization) and the post-intervention (at the end of the program), using the following tools: ACT Scale, Parenting and Family Adjustment, Parental Sense of Competence, UNICEF’s Multiple Indicator Cluster Survey, home stimulation activities, and the Strengths and Difficulties Questionnaire. The analysis used the MANOVA followed by the two-way mixed ANOVA for repeated measures. Results showed that compared to GC, the IG significantly increased emotional and behavioral regulation practices, parental sense of competence, and caregivers’ home stimulation and decreased parental inconsistency, coercive practices, and children’s behavior problems in the post-intervention. The program was effective in improving positive parenting and decreasing child behavior problems when implemented at a large scale in a policy system.
Keywords
Parenting program, Violence prevention, Early childhood, Scaling up, Low incomeCite this article as: Altafim, E. R. P. and Linhares, M. B. M. (2025). Effectiveness Evaluation of a Violence Prevention Parenting Program Implemented at Large Scale: A Randomized Controlled Trial. Psychosocial Intervention, 34(2), 63 - 77. https://doi.org/10.5093/pi2025a6
Correspondence: altafim.elisa@gmail.com (E. R. Pisani Altafim) and linhares@fmrp.usp.br (M. B. Martins Linhares)., Correspondence: altafim.elisa@gmail.com (E. R. Pisani Altafim) and linhares@fmrp.usp.br (M. B. Martins Linhares).Violence against children is a huge problem with the violation of children’s rights, requiring high priority worldwide. Approximately 300 million children aged between 2 and 4 years old regularly face violent practices from their caregivers (World Health Organization [WHO, 2020]). In Low-and-Middle-Income countries (LMIC), several social vulnerabilities, such as low socioeconomic status and low educational level, exacerbate the violence against children (Cerna-Turoff et al., 2021). Evidence from a study of young children in 49 LMICs shows that corporal punishment, including spanking, is likely to harm their development and well-being, needing public policies to protect children (Cuartas, 2021). In Brazil, 84% of violence against children is provoked by their caregivers (Linhares et al., 2023). Violence is a toxic stress event with a great risk for the intergenerational cycle of violence that negatively impacts later parenting behaviors and practices (Savage et al., 2019). Early childhood development is a critical period in the life cycle, with high brain plasticity and great learning potential, requiring social protection, family support, and violence prevention (Daelmans et al., 2017). Given the high prevalence of parenting practices using physical punishment and the associated high likelihood of harm to children, it is critical that social policies and parenting programs address the issue (Heilmann et al., 2021). The INSPIRE framework recommends seven strategies to end violence against children, focusing on governmental, civil society, and private sector actions by the 2030 Sustainable Development Goals (WHO, 2018). The seven strategies are the following: implementation and enforcement of laws, norms and values, safe environments, parent and caregiver support, income and economic strengthening, response and support services, and education and life skills. Then, strategies including parent and caregiver support and income and economic strengthening through cash transfers could be an effective initiative. Considering that poverty disrupts child development (Grantham-McGregor et al., 2007) and is a predictor of child maltreatment reporting (Kim & Drake, 2023), cash transfers could be a strategy to be implemented with low-income families, promoting investment in human capital (Arriagada et al., 2018). The Federal Unified Registry in Brazil shows that 55% of children 0-to-6-year-old live in poverty, depending on the cash transfer programs (Martins & Gomes, 2024). Cash transfers provided for women combined with parenting programs improve positive parenting and reduce child maltreatment (WHO, 2018) and might be crucial in breaking the cycle of detrimental parenting behaviors and improving children’s mental health over successive generations (Rothenberg et al., 2023). A randomized controlled trial (RCT) in the Philippines combining a group-based parenting program from 120 families receiving cash transfers reduced child maltreatment and dysfunctional parenting while improving positive parenting (Lachman et al., 2021). However, scientific evidence integrating cash transfer and parenting programs remains limited (Arriagada et al., 2018), requiring further investigation to optimize cash transfers with multisectoral interventions to achieve sustainable development goals (Little et al., 2021). Parenting programs conducted early in children’s lives can reduce adverse childhood experiences (e.g., neglect and abuse) and positively impact children’s cognitive and socioemotional development, brain structure and function, and health (Britto et al., 2017). Furthermore, family stimulation activities (e.g., reading, playing, and singing) improved children’s development in LMICs, underscoring the need for additional research into parenting interventions (Cuartas et al., 2023). A meta-analysis highlights that harsh parenting consistently leads to increased internalizing and externalizing symptoms in children across diverse regions and ethnic groups, emphasizing the need for solutions such as parenting programs to promote positive parenting (Pinquart, 2021). Therefore, parenting programs are a powerful preventive strategy to prevent violence against children (Baker-Henningham et al., 2023), and more RCTs in LMIC are required (Branco et al., 2022). A systematic review shows that the ACT Raising Safe Kids Program (ACT Program) is one of the few parenting programs that addresses specific content on violence and explicitly states its purpose as preventing violence against children (Branco et al., 2022). The INSPIRE (WHO, 2018) recommended the ACT Program as a universal preventive evidence-based parenting program for caregivers up to 8-year-old children, developed by the American Psychological Association (Silva, 2011). This group-based program, grounded in social learning theory, has a low implementation cost (Knox & Dynes, 2020), effectively strengthens positive parenting practices, and mitigates coercive and aggressive practices (Altafim et al., 2024; Pontes et al., 2019). RCTs using the ACT Program, performed in the United States of America (Knox et al., 2013; Portwood et al., 2011) and Brazil (Altafim & Linhares, 2019), demonstrated an increase in positive parenting practices and a decrease in harsh and coercive parenting. Also, there was an improvement in parental sense of competence (Lotto et al., 2022) and a reduction in children’s internalizing and externalizing behavior problems (Altafim & Linhares, 2019). The validation of the ACT Program theory of change showed that the intervention had a positive effect directly on parenting practices, which mediated the reduction of children’s behavior problems, mainly through parental practice with emotional and behavioral regulation (Altafim et al., 2021). However, despite the robust scientific evidence base of the positive effects of the ACT Program on parenting and children’s behavior, there is a gap in the literature about the effectiveness of the program implemented at a large scale, considering that the range of the previous sample size was from 10 to 369 caregivers (Altafim et al., 2024). The great challenge of parenting programs concerns the transition of science to practice and policy approach to achieve sustainability in public policies in the “real world” (Lansford et al., 2022). Existing evidence on large-scale parenting intervention is scarce and there is no guarantee that programs with efficacy in small trials will maintain the effects when scaled up (Arriagada et al., 2018). The interventions should have standard evidence of efficacy with rigorous trials and effectiveness under “real-world” conditions before being ready for dissemination or transitioning to scale (Flay et al., 2005). As shown by a systematic review of parenting interventions, there is a gap in large-scale RCTs with direct measurement of the effects of programs on parenting, with the largest study analyzed involving 464 participants (Backhaus et al., 2023). This review identified only one RCT carried out on a large scale involving 17 counties but without precision in the number of families served and using outcomes from official records (Prinz et al., 2009). Furthermore, as shown by systematic reviews, there is a gap in RCTs evaluation parenting programs in LMIC (Backhaus et al., 2023; Branco et al., 2022). Therefore, it is necessary to acquire findings about the scaling implementation of parenting programs in a public policy system with workers at the frontline in services that usually attend to vulnerable families, especially those receiving income transfers. It is also still necessary to validate the outcomes of the ACT Program to examine its effectiveness in an implementation in a natural setting. The Present Study The current study was developed in the State of Ceará, Northeast Brazil. In 2019, research in this state showed that 49% of 6,447 caregivers reported believing in the necessity of using physical punishment to raise their children (Venancio, 2022). The state government planned several strategies to promote early childhood development (ECD) and prevent violence against children, aiming to support families with young children in vulnerable situations. The ACT Program was selected to be integrated into this government ECD initiative in some municipalities to first test its effectiveness and subsequently expand it to other municipalities. The ECD government program focuses primarily on families receiving federal and state-level cash transfer benefits; however, it is not exclusive to these families. The cash transfer consists of monthly governmental monetary support for families facing vulnerabilities. Therefore, the present RCT study was carried out in the context of a broad initiative, including the ACT Program, with the following steps: (i) sensitization and articulation of the stakeholders at a state-level government to implement the program as a sustainable policy; (ii) organization of core teams at municipality-level; (iii) capacity building professionals as ACT facilitators; (iv) implementation the program with socially vulnerable families. Therefore, the purpose of the present study was to examine the effectiveness of the ACT Program, delivered at a large scale in the public policy system, in improving positive parenting practices and reducing negative practices in very low-income families. As secondary outcomes, the study aimed to examine the program’s effectiveness in improving home stimulation activities and parental sense of competence and decreasing children’s behavior problems. Then, aiming to evaluate the intervention outcomes, the hypotheses of the study were the following: H1) there will be significant positive effects of the intervention on primary parenting outcomes, such that the intervention group will show greater improvements in positive parenting practices and greater reductions in negative parenting practices from pre- to post-intervention compared to the control group; and H2) there will be significant positive effects of the intervention positive effects on the secondary outcomes, such as the intervention group showing greater improvements in home stimulation activities, parental sense of competence, and prosocial behaviors, and greater reductions in behavior problems from pre- to post-intervention compared to the control group. Study Design, Ethics, and Protocol The study is a two-arm randomized controlled trial with a waiting-list control group (usual care), with assessments performed in the pre-intervention (after the randomization) and the post-intervention (at the end of the program). The procedure followed the CONSORT Reporting Checklist (See Supplementary Material). Figure 1 Flow Diagram for the Randomized Controlled Trial.  The study protocol, including methodology and procedures, was first approved prospectively in May 2021 by the Ethics Committee of the Ribeirão Preto Medical School of the University of São Paulo and, in sequence, registered in the Brazilian Registry of Clinical Trials (ReBEC; RBR-5gbhw5w). The caregivers voluntarily signed the Informed Consent Form at the beginning of the study before the data collection. Sample The inclusion criteria of the participants established in the study considered caregivers who performed the parental role daily with 0-to-6-year-old children (e.g., biological- or stepmothers or fathers, grandmothers, or others). The families were recruited predominantly in the Social Assistance public services of 17 municipalities of the Ceará state (Northeast of Brazil), and few of these municipalities had an intersectoral context with Social Assistance Services allied with educational and health areas. Professionals invited the caregivers that were routinely attended by ECD social protection initiatives, primarily low-income families registered in the federal- and state-level cash transfer programs (Bolsa Família and Cartão Mais Infância Ceará). These caregivers and their children represent an at-risk population living under social vulnerabilities, facing inequalities, and exposure to adverse events. The professionals delivering the program, trained as ACT Program facilitators, were government employees working in these services. They were responsible for identifying and inviting families in these contexts, particularly those receiving cash transfers, though not exclusively. The state-level cash transfer program required caregivers to participate in social service programs. The ACT Program was offered as an option; however, participation was voluntary, not mandatory or conditional. The sample size was estimated to compare means between two groups (intervention vs. control), targeting a 5% probability of type I errors (α = .05) and an 80% power to detect type II errors (β = .20). The calculation considered multiple outcomes, including parenting practices (ACT Scale; communication, positive discipline, and emotional regulation) and child behavior (prosocial behavior and internalizing and externalizing problems), based on data from a preliminary RCT (Altafim & Linhares, 2019). The estimated sample size required for these multiple outcomes was 564 mothers per group, totaling 1,128 caregivers. The sample size exceeded the power analysis estimate to account for potential attrition and enable the analysis of multiple instruments, ensuring robust results. Figure 1 shows that the professionals registered 1,571 caregivers for enrollment in the study. Of these, 17 declined to participate, and 38 were excluded because two professionals did not follow the randomization procedure, resulting in 1,516 that were randomized. These 1,516 participants were randomly divided into an intervention group (IG, n = 769) and a control group (CG, n = 747). However, 206 participants withdrew from the study, with 130 withdrawing from the IG and 76 from the CG. As a result, the final sample consisted of 1,310 participants, with 639 caregivers in the IG and 671 in the CG. The CG was a usual care waiting-list group, where caregivers and children received the standard care protocols from Social Assistance services for families and educational centers in their municipalities. The Social Assistance services usually provide support for all families, including meetings to strengthen the affective bonds between children and families and financial benefits (e.g., cash transfer). These usual care services did not offer a structured and manualized parenting program for violence prevention. The final sample comprised 1,310 family primary caregivers with at least one 0-to-6-year-old child living in Brazil, a middle-income Country. Randomization Procedure The randomization of groups was stratified in blocks by each facilitator of each site by the software application (App) entitled ACT - Ceará, which was customized for the present study. In this App, the professional registered each participant. Upon reaching a minimum of six caregivers, the App randomly distributes the number of participants between the intervention and the control groups using a programming function. If the number of registered participants were odd, the IG would receive one more participant than the CG. The App generates a list informing the group (IG or CG) of each participant. Through the App and block randomization by facilitators, it was possible to maintain a continuous flow of participants entering the study, starting from group formation. Then, after the conclusion of the randomization process for each block, the data collection started with pre-intervention assessments of those participants. Instruments and Measures Parenting Practices (Primary Outcomes) ACT Scale (Silva, 2011; 3-factor ACT Scale, Portuguese-Brazilian version). This self-report Likert scale featured in the ACT Evaluation and Instrument Guide (Silva, 2011) comprises 15 items based on the three-factor model identified through a validation study (Altafim et al., 2018). These factors include emotional and behavioral regulation (seven items; score range = 7 to 35), positive discipline (five items; score range = 5 to 25), and communication (three items; score range = 3 to 15), where higher scores indicate more effective parenting practices within these dimensions. The three-factor model of the ACT Scale (Altafim et al., 2018) produces three distinct scores, but it does not provide an overall composite score. The internal consistency coefficients for the present sample were emotional and behavioral regulation (α = .71), communication (α = .54), and positive discipline (α = .81). Parenting and Family Adjustment Scales (PAFAS; Sanders et al., 2014; Portuguese-Brazilian version by Correia et al., 2024). The present study used this self-report focus in the Parenting Scale, with the following three dimensions: parental inconsistency (three items; score range = 0-9) and coercive parenting (four items; score range = 0-12), where higher scores signify more dysfunctional practices and positive encouragement (three items; score range = 0-9), with higher scores indicating better parenting practices. The internal consistency coefficients for the present sample were as follows: parental inconsistency (α = .53), coercive parenting (α = .68), and positive encouragement (α = .81). Therefore, in the present study, three PAFAS scale scores were used. Parental Sense of Competence and Home Stimulation Activities (Secondary Outcomes) Parental Sense of Competence Scale (PSOC; Gibaud-Wallston & Wanderman, 1978). The present study used the Frontiers of Innovation version of the scale translated into Portuguese-Brazil with the authors’ authorization. All 17 items of the original instrument were scored on a four-point Likert scale (from strongly disagree to strongly agree), generating the final score ranging from 17 to 68. Higher scores indicate a higher parental sense of competence. The internal consistency coefficient for the present sample was α = .60. The instrument generates a single score. Home Stimulation Activities. To assess home stimulation activities, the item of the UNICEF’s Multiple Indicator Cluster Survey (MICS6; UNICEF, 2020) Questionnaire for Children Under Five, the Early Childhood Development module was used. This module captures adult-child interactions in six home stimulation activities (e.g., reading, telling stories, and playing) over the preceding three days. The final stimulation scores represent the activities reported by caregivers, ranging from 0 to 6. The higher scores indicate greater home stimulation. The internal consistency coefficient for the current sample was α = .63. The instrument generates a single score. Children’s Behaviors (Secondary Outcomes) Strengths and Difficulties Questionnaire (SDQ; Brazilian versions P2-4 and P4-16). It is a caregiver report instrument, translated and validated for Brazil (Fleitlich et al., 2000), employing a 3-point Likert-type scale, grouped into three subscales: internalizing problems (10 items) and externalizing problems (10 items), where higher scores indicate more behavior problems, and the prosocial scale (5 items), where higher scores reflect greater capacity (Goodman et al., 2010). The internalizing and externalizing scales generate a total difficulties score, which is used for screening child behavior as normal, at-risk, and clinical, based on cutoff points (Fleitlich et al., 2000). Internal consistency scores for the SDQ scales in this study sample were the following: total difficulties, α = .78; internalizing, α = .64; externalizing, α = .70; and prosocial, α = .67. The instrument generates four scores that were used in the present study (total difficulties, internalizing, externalizing, and prosocial). Characterization of the Sample Sociodemographic Questionnaire. Includes the Brazil Economic Classification Criterion from the Brazilian Association of Research Companies (Associação Brasileira de Empresas de Pesquisa [ABEP, 2019]), which measures the socioeconomic score, including questions about the number of electronic items in the household, household head education level, and the use of public services (e.g., piped water and paving at the street). The questions generate a score ranging from 0 to 100, subdivided into socioeconomic levels from A to E. The higher the score, the higher the socioeconomic level. Also, the questionnaire included complementary questions about children’s age and sex, as well as mothers’ age, schooling level, marital status, self-declared skin color, and number of children. Procedure Data Collection The initial schedule for data collection was set for 18 months between 2021 and 2022 and needed adjustment due to the pandemic period. Therefore, the data were collected from March 2022 to June 2023 by trained professionals (e.g., social workers, psychologists, and educators) from the public system of the cities of the Ceará state and mostly from Social Protection and Educational Services. The professionals were previously trained and certified as ACT facilitators and trained in the instruments for assessment used in the present study. The data collection schedule was the following: two sessions for the assessment phase (pre- and post-intervention), one preparatory session, and eight sessions for the intervention with the ACT-Raising Safe Kids Program. Facilitators read the questionnaires and scales applied for caregivers during the interview in both phases, which were the following: ACT, PAFAS, PSOC, MICS, and SDQ. The sociodemographic questionnaires were applied only in the pre-intervention. These questionnaires were included in the App ACT-Ceará, developed and customized for the present study. Data collection was performed during the COVID-19 pandemic when physical contact was allowed. The local and leading team of investigators monitored and supervised all data collection to guarantee the fidelity of the intervention and assessments. The facilitators had the support of a team functioning in their respective municipalities composed of a coordinator (logistic role) and a supervisor (technical role) to implement the ACT Program. Intervention Procedure The ACT-Raising Safe Kids Program, an in-group psychoeducational universal preventive program performed weekly in eight highly interactive sessions lasting around 120 minutes, provides structured materials, including the facilitator manual, assessment questionnaires, a booklet for parents, and motivational interviews (Silva, 2011). The ACT Program has a Brazilian-Portuguese version developed by the American Psychological Association that was previously culturally adapted and validated for Brazil (Altafim et al., 2016; Pedro et al., 2017). The sessions include group activities, didactic presentations, discussions, and role-play. The booklet for parents includes short messages discussed during the sessions, serving as reminders to take home. The sessions were conducted by a facilitator and a co-facilitator, certified by master trainers, to ensure fidelity in implementing the program. The ACT Program covers the following topics: (i) children’s development and behaviors; (ii) types of violence against children and strategies to prevent it; (iii) managing caregivers’ anger and other emotions; (iv) supporting and understanding children’s emotions; (v) electronic media monitoring and use regulation; (vi) positive discipline and parenting styles; (vii) disseminating knowledge about ACT to family members and the community. These contents are presented in a reflexive strategy, inclusive participant responsiveness, and with non-judgments and non-stigmatization. The program is free of charge for the families. Each caregiver’s dosage of the ACT Program was measured by the number of sessions they participated in a maximum of eight sessions. Core Implementation Components of the Intervention The implementation of the ACT intervention with the families in the municipalities followed some core components, as recommended by Fixsen et al. (2009): (i) local staff selection of practitioners from the Social Protection Services, with graduation academic qualification, experience with families and child development, and basic skills with groups; (ii) capacity building of the professionals following the theory and methodology of the program, including evaluation of the professionals’ performance to guarantee the fidelity to the curriculum and strategies, and the quality of the delivery with the families; (iii) core group trained in each municipality, including facilitators, supervisors (psychologists), and coordinators of logistic of implementation; (iv) coaching and consultation by technical assistants (specialists in the ACT Program) during the practical training and the implementation with the families; (v) monitoring all the implementation process by the coordinators of the project (authors) and their team, including local visiting in the sites; (vi) administrative and organizational support system by governments at municipal- and state-levels; (vii) financial support for the training and implementation by foundations. Capacity Building of ACT Facilitators The capacity building of ACT facilitators was done following the American Psychological Association’s requirements, comprising two parts: Theoretical Workshop and Practical Training. The Theoretical Workshop presented and discussed the curriculum, specific instructions, strategies, role-play, and group dynamics. Practical training refers to delivering the ACT Program to caregivers in the groups. Specifically, in the sixth session, the professional video recorded the session, and the professional performance was evaluated by the master trainers, aiming to guarantee the fidelity of the program. The theoretical workshop was conducted online by two ACT master trainers (authors) due to the social distancing during the COVID-19 pandemic, and it was adapted for four days (16 hours). The practice consisted of the in-person application of the ACT Program with a group of caregivers. These professionals received additional support through optional online meetings for supervision and clarification with two psychology specialists who participated in the training together with the master trainers and are experts in the ACT Program, each with over four years of experience as ACT facilitators. For the certification process, the professionals video-recorded the sixth session as proposed by the American Psychological Association and sent it to the master trainer for evaluation. Only certified professionals participated in the data collection of the present study. Data Analysis Initially, the data collected via the App-ACT Ceará were exported to an Excel sheet and double-checked for accuracy by two research assistants. Then, the data were imported into the Statistical Package for Social Sciences (SPSS, version 29.0, Chicago, IL, USA) for statistical data analysis. All randomized caregivers who concluded the intervention were included in the analysis independently of the number of sessions to avoid bias in the randomization process. The dataset and its structure were prepared by independent team members not involved in the data analysis. Secondly, descriptive statistical analyses were conducted. Thirdly, the statistical analysis used MANOVA and ANOVA, which are objective statistical methods, minimizing the risk of bias or interference. The MANOVA was performed to assess the multivariate time-by-group interaction effects on the scores of the instruments with multiple constructs (ACT, PAFAS, and SDQ). Fourthly, for instruments with significant group-by-time interactions identified in the MANOVA, a two-way mixed-design ANOVA (general linear model for repeated measures) was conducted. This ANOVA assessed changes within groups (pre- to post-intervention) and between groups (IG vs. CG) over time. This analysis was also applied to both instruments with single variables (MICS and PSOC). Fifthly, when significant interactions between groups and time were identified, further within-group comparisons were conducted using repeated measures ANOVA to compare the outcomes from pre- to post-intervention in each group (IG and CG), and the effect sizes for each group were calculated. The effect size, measured as partial eta squared (η²), was used to assess the magnitude and practical relevance of significant findings, interpreted according to Cohen’s benchmarks for η² = .01 for a small effect size, .059 for a medium effect size, and .138 for a large effect size (Portney & Watkins, 2008). Finally, a complementary analysis was conducted to compare the post-intervention scores for outcomes that demonstrated an interactive effect, assessing whether the intervention group exhibited significantly higher mean scores compared to the control group, using an independent samples t-test. The statistical significance level for all tests was set at 5% (p < .05). Sample Sociodemographic Characteristics The main sociodemographic characteristics of the completers’ participants (CP; n = 1,310) were similar to those of the dropout participants (DP; n = 206). The between-group comparisons (t-test or chi-square test) showed no statistically significant differences between these groups regarding the children’s age and sex, kinship with the child, number of children aged from 0 to 6 years, receiving cash transfer marital status, and monthly family income. There was a unique statistical difference between groups in the caregivers’ age, in years, CP, mean age = 31.61 (± 7.72) and DP, mean age 30.13 (± 8.34) and p = .01, and in the percentage of adolescent caregivers (CP = 2% and DP = 7% and p < .001). Then, the younger caregivers dropped out of the study more than the older ones. Table 1 Sociodemographic Characteristics of the Sample (n = 1,310) 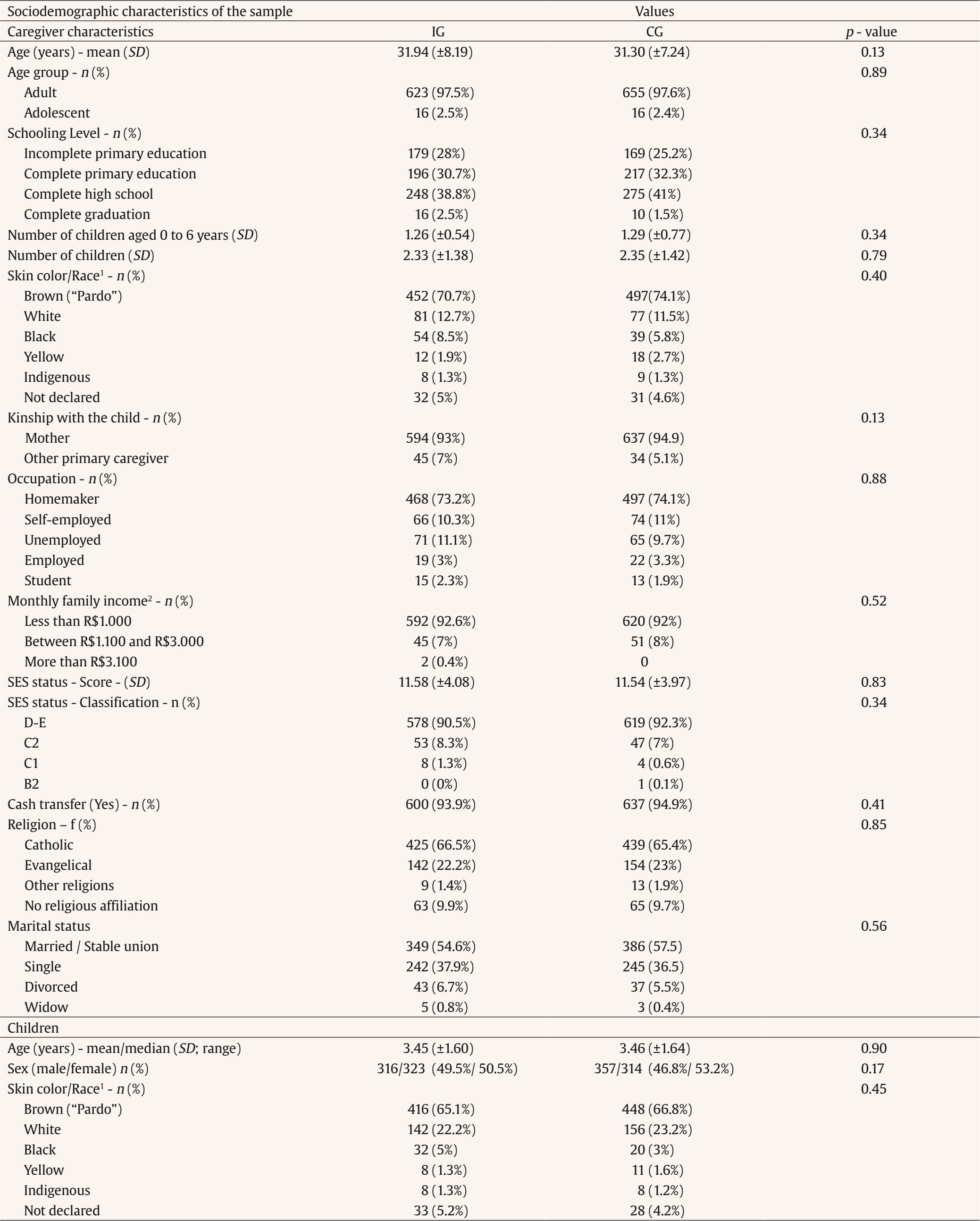 Note. n = number of participants; % = percentage; SD = standard deviation; 1Brazilian classification of race, according to the Brazilian Institute of Geography and Statistics, IBGE; SES = socioeconomic status, according to Brazilian Association of Research Companies (ABEP). ABEP Classification: C1 = 23 to 28 points, average income of R$ 3,276.76; C2 = 17 to 22 points, average income of R$ 1,965.87; D-E = 0 to 16 points, average income of R$ 900.60; 2R$ = Brazilian currency, U$ 1 = R$ 5.04. Table 1 shows no statistically significant differences between the two groups (IG and CG) regarding the sample sociodemographic characteristics. The caregivers were predominantly adult mothers with self-declared brown skin color, stable union relationships, at least completed elementary education, and were homemakers. Most caregivers were from a very low socioeconomic status with a monthly income of up to R$1,000.00 Brazilian reais (approximately U$198.41) and received cash transfers. The children in the sample had a similar distribution among boys and girls, with an average age of three years old and most with declared brown skin color. Parenting and Children’s Behaviors Outcomes at Baseline In the pre-intervention, there were no statistically significant differences between IG and CG across all parenting (ACT, PAFAS, PSOC, and MICS scores) and children’s behaviors (SDQ scores) variables. Then, both groups were similar in the caregivers’ parenting and child behavior outcomes at baseline. Dosage of the Intervention The IG received a high dose of the ACT Program, considering that 70% of participants attended seven or eight sessions, 15% six sessions, 11% between five or four sessions, and only 4% fewer than four meetings. According to the monitoring and facilitators’ reports, the data was not contaminated, with the participation of families from the CG in the intervention. Parenting Outcomes Parenting Practices (Primary Outcomes) The MANOVA revealed a significant multivariate effect of group and time interaction on the dependent variables of the ACT Scale, (Wilks’ Λ = .99, F(3, 1306) = 5.015, p = .002, indicating that the combined dependent variables (Emotional/Behavioral Regulation, Positive Discipline, and Communication) were significantly influenced by the time-by-group interaction. There was also a significant multivariate effect of group and time interaction on the dependent variables of the PAFAS Scale, Wilks’ Λ = .98, F(3, 1306) = 7.545, p < .001, indicating that the combined dependent variables (parental inconsistency, coercive practices, and positive encouragement) were significantly influenced by the time-by-group interaction. As seen in Table 2, for the primary outcomes, there were significant interactions between groups (IG and CG) and time (pre- and post-intervention) in parenting for the caregivers’ emotional and behavioral regulation, F(1, 1308) = 13.78, p < .001, parental inconsistency, F(1, 1308) = 17.52, p < .001, coercive practices, F(1, 1308) = 12.59, p < .001. There was also a marginal interaction and differences between time for positive discipline (p = .059). The within-group comparisons from pre- to post-intervention showed statistically significant increases in emotional and behavior regulation (p < .001, η² = .045) and positive discipline (p = .001, η² = .016) in the IG caregivers, both with a small effect size. Conversely, the CG did not exhibit significant changes in these measures (behavioral regulation, p = .435 and positive discipline, p = .535). Additionally, the IG demonstrated a significant decrease in parental inconsistency (p < .001, η² = .067) and coercive practices (p < .001, η² = .098) from pre- to post-intervention, both with medium effect sizes. In the CG, there were no significant changes in parental inconsistency (p = .28), but there was a significant decrease in coercive practices, with a small effect size (p < .001, η² = .021). There was no significance on the interaction between groups and time for communication and positive encouragement; in both scales in pre-intervention assessments, the caregivers presented high scores, considering the maximum scores of these scales. Table 2 Mother’s Parenting Outcomes in the ACT Intervention and Control Groups, in the Pre-and Post-intervention Moments 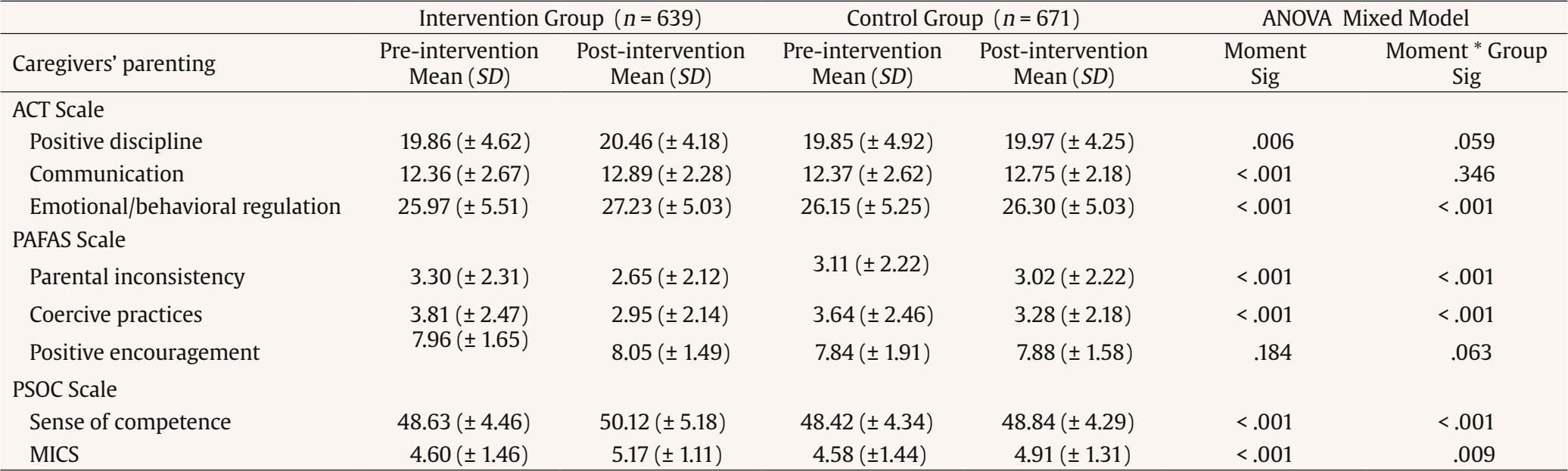 Note. SD = standard deviation; Sig = significance; Moment*Group – interaction effect. In the ACT Scale, the total score on the Positive Discipline scale can range from 5 to 25, Communication from 3 to 15, and Emotional/Behavioral Regulation from 7 to 35; for all the scales, higher scores indicate better parenting practices; PAFAS = Parenting and Family Adjustment Scale. On PAFAS Scale, the total score for the Parental Inconsistency and Positive Encouragement factors can range from 0 to 9, and the factors of Coercive Practices can range from 0 to 12. In Parental Inconsistency and Coercive Practices scales, the higher the score, the more dysfunctional the parenting practices related to these aspects. In Positive encouragement, the higher the score, the better the parenting practice; PSOC = Parenting Sense of Competence Scale. In the PSOC Scale, the total score ranges from 17-68; the higher, the better the result; MICS = UNICEF’s Multiple Indicator Cluster Survey, assessing six home stimulation activities (e.g., reading, telling stories, and playing), with scores ranging from 0 to 6, where higher scores indicate greater home stimulation. The between-group comparison analysis of the post-intervention assessment showed significantly higher scores in emotional and behavioral regulation (p < .001) and positive discipline (p < .001) in IG compared to CG and lower scores in parental inconsistency (p = .002) and coercive practices (p = .005). In summary, the ANOVA interaction effects between group and time indicated that the intervention effectively improved emotional and behavioral regulation and positive discipline, and reducing parental inconsistency and coercive practices. Statistically significant changes in emotional and behavioral regulation, positive discipline, and parental inconsistency were observed only in the IG, with no significant differences in the CG. Although both groups showed a reduction in coercive practices, the IG exhibited a greater magnitude of change (effect size) from pre- to post-intervention compared to the CG. Additionally, all the parenting outcomes showed better mean scores in the IG than the CG in the post-intervention. Figure 2 shows the interaction effects of parenting outcomes. Figure 2 Mean Scores of the Parenting Outcomes of IG and CG Groups (pre- and post-intervention).  Parental Sense of Competence and Home Stimulation Activities (Secondary Outcomes) The ANOVA mixed method showed significant interactions between groups (IG and CG) and time (pre- and post-intervention) in the parental sense of competence, F(1, 1308) = 14.23, p < .001) and caregivers’ home stimulation, F(1, 1308) = 6.87, p = .009. Both groups (IG and CG) exhibited significant statistical differences from pre- to post-intervention regarding the parental sense of competence and home stimulation. However, the magnitude of these differences varied, showing that the IG presented a medium effect size (parental sense of competence, p < .001, η² = .062; home stimulation, p < .001; η² = .108), while the CG exhibited a small effect size (sense of competence, p < .001, η² = .009; home stimulation, p < .001, η² = .041). The between-group comparison analysis of the post-intervention assessment showed significantly higher scores in parental sense of competence (p < .001) and home stimulation (p < .001) in IG compared to CG. Table 3 Children’s Behavior Difficulties and Prosocial Behavior in the ACT Intervention and Control Groups, in the Pre-and Post-intervention Moments  Note. SDQ = Strengths and Difficulties Questionnaire; SD = standard deviation; Sig = significance; Moment*Group = interaction effect; the total difficulties score range from 0 to 40; externalizing and internalizing behavior problems range from 0 to 20; the higher scores indicate more behavior problems; the Prosocial Behavior subscale ranges from 0-10: the higher the score, the greater capacity. In summary, the ANOVA interaction effects between group and time indicated that the program was effective in enhancing parental sense of competence and home stimulation activities. While both groups demonstrated improvements in these outcomes, the IG showed greater change (effect size) from pre- to post-intervention compared to the CG. Additionally, both outcomes showed better mean scores in the IG than the CG in the post-intervention. Children’s Behaviors Outcomes (Secondary Outcomes) The child behavior measure was conducted with children from 2 years old, considering the instrument restriction for age. The MANOVA revealed a significant multivariate effect of group and time interaction on the dependent variables of the SDQ, Wilks’ Λ = .98, F(4, 1135) = 4.56, p = .001, indicating that the combined dependent variables (total difficulties, internalizing, externalizing and prosocial behaviors) were significantly influenced by the time-by-group interaction. As seen in Table 3, significant interactions were observed between groups (IG and CG) and time points (pre- and post-intervention) for child behaviors regarding total difficulties, F(1, 1138) = 14.27, p < .001, and externalizing, F(1, 1138) = 12.84, p < .001, and internalizing difficulties, F(1, 1138) = 8.46, p = .004. Within-group comparisons indicated significant reductions in total difficulties, externalizing, and internalizing problem scores from pre- to post-intervention in both groups. However, the magnitude of change differed between them. The IG exhibited medium effect sizes for total difficulties (η² = .113) and externalizing behaviors (η² = .093), while the CG showed small effect sizes for total difficulties (η² = .019) and externalizing behaviors (η² = .009). For internalizing problems, both groups displayed small effect sizes, but the effect was higher in the IG (η² = .056) compared to the CG (η² = .008). Figure 3 shows the interaction effect of child outcomes. The child’s prosocial behavior did not show an interaction between groups (IG and CG) and time point (pre- and post-intervention); however, there was a statistically significant difference in time, F(1, 1138) = 10.27, p = .001, showing that both groups improved over time (pre- to post-intervention). The between-group comparison analysis of the post-intervention assessment showed significantly lower scores for child total difficulties (p = -.047) and externalizing behavior problems (p = .036), in IG compared to CG. There was no significant difference for child internalizing behavior problems. In summary, the ANOVA interaction effects between group and time showed that the program was effective in decreasing total behavior and externalizing problems. While both groups showed reductions in these outcomes, the IG exhibited a greater magnitude of change (effect size) from pre- to post-intervention in comparison to the CG, and the post-intervention mean scores were lower for the IG. Figure 3 Mean Scores of the Child Outcomes of IG and CG Groups (pre- and post-intervention). 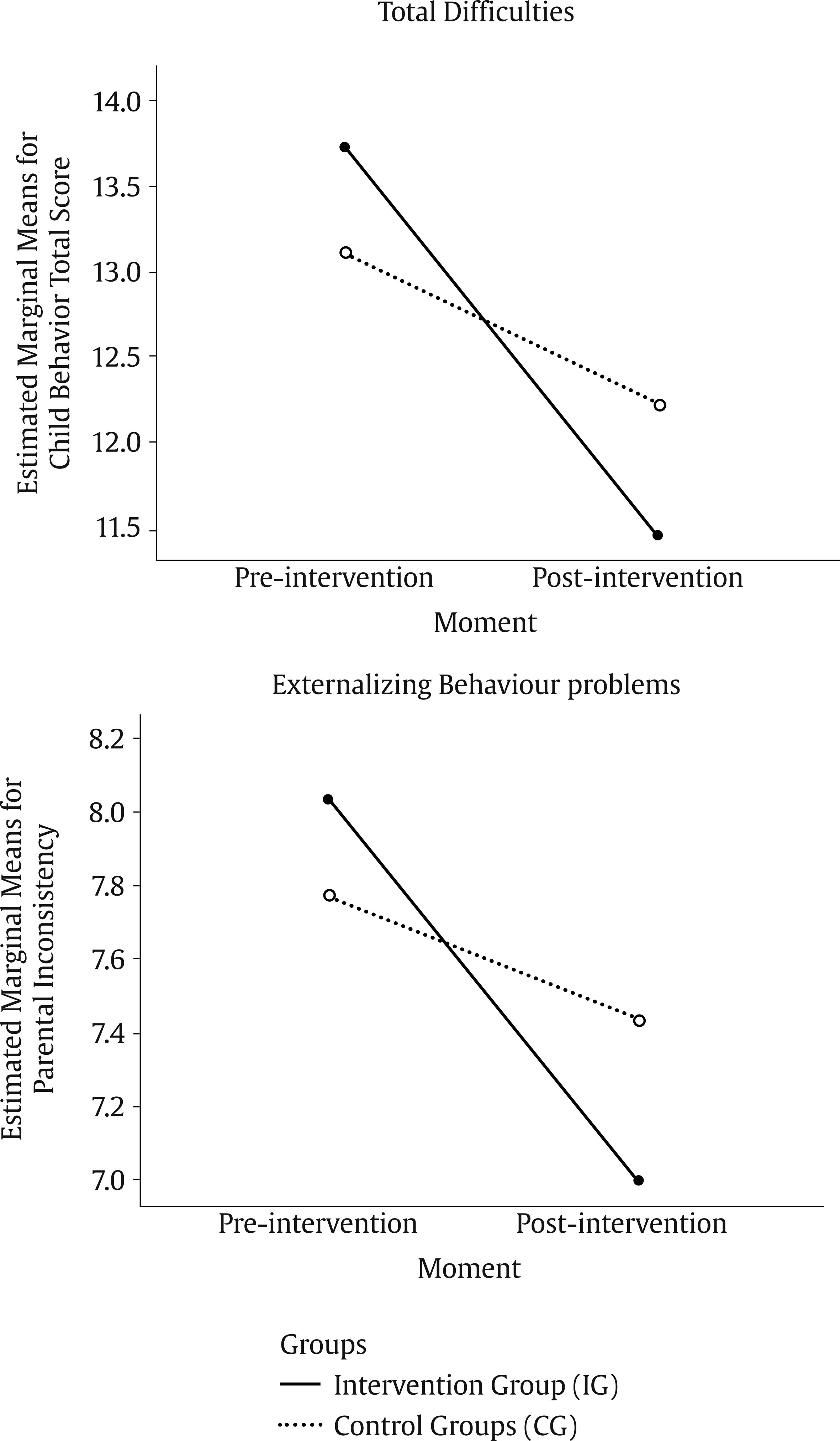 As far as we know, this is the first RCT study of the ACT Program implemented at a large scale within the public policy system for attending to vulnerable families and involving the largest number of cities and participants in a collaboration between the state and its municipalities. Previous ACT studies involved fewer participants; the most extensive study included 339 caregivers across eight US cities but was not RCT (Weymouth & Howe, 2011), while in Brazil an RCT protocol involved 369 caregivers from a single city (Murray et al., 2019). The study also represents a significant advancement in the literature on parenting programs, addressing the notable gap in large-scale studies (Arriagada et al., 2018) and LMICs (Backhaus et al., 2023; Branco et al., 2022). The present RCT confirmed the hypotheses of the ACT Program’s positive effects on the primary outcomes, showing improvements in positive parenting practices (emotional and behavioral regulation and positive discipline) and reductions in negative parenting practices (parental inconsistency, coercive practices) from pre- to post-intervention in the IG compared to the CG. Also, the intervention had positive effects on the secondary outcomes, revealing improvements in home stimulation activities, parental sense of competence, and reductions in children’s behavior problems from pre- to post-intervention in the IG compared to the CG. The hypotheses of intervention effects on communication and positive encouragement parenting practices and children’s prosocial behavior were not confirmed. Focusing on the current outcomes of the ACT Program in the context of its implementation at a large scale, the present study confirmed the ACT theory of change tested in a previous study (Altafim et al., 2021). It shows the ACT Program’s positive effects on improving parenting practices and reducing children’s behavioral difficulties. Furthermore, the current study goes beyond adding evidence of the ACT Program in other components of parenting, reducing coercive and parental inconsistency practices and improving parental sense of competence and caregivers’ home stimulation. All these positive changes after the intervention are significant considering that the characteristics of the sample of the present study were families living in poverty conditions, experiencing iniquities, with high risk for violence, which is a well-known risk for child development and mental health problems. These findings about the positive effects of the ACT Program to increase caregivers’ emotional and behavioral regulation practices and parental sense of competence, and a decrease in parental inconsistency and coercive practices were found in previous studies, specially developed in Brazil and the USA, but with small samples sizes and not implemented at large scale (Altafim et al., 2024). Positive parenting with emotional and behavioral regulation is a vital component of the ACT curriculum that reduces children’s behavior problems (Altafim et al., 2021). The literature reveals that maternal self-regulation is linked to less internalizing (Zimmer-Gembeck et al., 2022) and externalizing symptoms (Zurynski et al., 2023). Although the findings showed a marginal interactive effect for positive discipline, the within-group analysis also demonstrated that the IG improved while the control group did not change. Additionally, the findings showing a reduction of coercive parenting, including physical punishment, is essential to reducing children’s behavior problems. As seen in a previous review, physical punishment is related to increases in child behavior problems over time (Heilmann et al., 2021). The findings showing an improvement in caregivers’ home stimulation after the program is also an advance of the current study since this variable was not evaluated in previous ACT studies. Providing stimulation to create learning opportunities that promote child development at early ages is a relevant component of parenting and nurturing care and is related to better child development outcomes (Cuartas et al., 2023). The study reached families of very low socioeconomic status and showed high adherence to the ACT Program, with 85% of the intervention group completing most program sessions (six or more). Even though the previous ACT studies showed its effects on families of different socioeconomic levels (Altafim et al., 2024; Pedro et al., 2017), adherence to the program was significantly lower among mothers with low socioeconomic status, 51% in C-level compared to those with medium socioeconomic status, 79% in B-level (Pedro et al., 2017). Thus, this study represents a significant contribution by successfully retaining families with very low incomes. However, the analysis of the complete and dropout participants revealed that younger mothers, particularly adolescents, were likelier to drop out of the study. This finding suggests that younger caregivers face specific challenges that hinder engagement, highlighting the need for age-appropriate strategies and enhanced support to reduce attrition and increase participation. A previous ACT study with a sample exclusively of adolescents and young women who became pregnant during adolescence found a high dropout rate and recruitment difficulties, which may indicate a characteristic of this participant group (Santos et al., 2024). The intervention dosage was adequate, with most participants enrolled in almost all ACT sessions. The dosage and fidelity are critical in determining the main effects of the outcomes (Parker et al., 2020). The good engagement in the program could be attributed to several variables, such as the combination of a cash transfer program and the link with social protection services, the program’s content, caregivers` motivation to change, facilitators’ strategies, implementation monitoring, and others. Most part of the participants in the current study received cash transfers from federal- and state-level programs, which could be an incentive for caregivers to participate in programs offered by the government. This finding indicates that linking the program to a cash transfer program could effectively reach and retain families in parenting programs. As previously highlighted, combining parenting programs and cash transfers has synergic effects for change (Arriagada et al., 2018; Landsford, 2022). The study found similar results in reducing negative and dysfunctional parenting and improving positive parenting as in a previous RCT in an Asian middle-income country offering group-based parenting programs for families receiving cash transfers but with a smaller sample (Lachman et al., 2021). Despite existing recommendations to combine cash transfers with parenting programs (WHO, 2018), research demonstrating the effectiveness of this combination remains scarce on a large scale (Arriagada, 2018), especially in LMIC (Little et al., 2021). Therefore, the current study represents an advancement in the literature. Additionally, the program implementation in the Brazilian Northeast region presents a unique context to explore its effects on a large scale, regarding that this region has the highest concentration of low-income families enrolled in the federal cash-transfer program named “Bolsa Família” (Martins & Gomes, 2024). The study participants were predominantly female caregivers’ mothers, who usually care for and support children. In Brazil, most beneficiaries of the Federal Government’s transfer programs are women, the family heads (Martins & Gomes, 2024). The fathers’ poor engagement in the parenting program observed in the current study is commonly detected in other studies as a great challenge for practitioners and service providers (Lechowicz et al., 2019). The current study had several strengths. The innovation is related to implementing the ACT Program at a large scale in a “real world” setting with very low-income families mostly inserted in cash transfer programs. The study was designed to evaluate a low-cost, evidence-based parenting program that is effective on a large scale with families under adverse conditions. The program is specifically oriented to violence prevention and recommended by INSPIRE as an effective strategy to end violence against children (WHO, 2018). Innovative findings showed that the ACT Program is culturally sensitive in strengthening positive parenting, reducing negative parenting practices and decreasing child behavior problems in low-income families in middle-income countries. The study is the first to assess the ACT Program in families from an Indigenous community included in the sample. Therefore, the study’s findings advance the generalizability of the ACT Program’s effects by evaluating a previously unexamined population – very low-income families on a large scale – and finding the same results as previous studies conducted in Brazil and other countries (Altafim et al., 2024). Also, the RCT comprises the data collection performed by the frontline workers under supervision, but independent investigators did the data analysis and interpretation of the results. The use of professionals in the data collection reduced the study costs and facilitated large-scale evaluation, as seen in a previous ACT study (Portwood et al., 2011). Finally, the ACT Program implementation used previous principles of implementation science (Baker-Henningham et al., 2023), as follows: (i) design programs for scale, (ii) learning cycles for quality improvements, (iii) plan strategies to guide government agency, (iv) provide high-quality training and supervision, (iv) monitoring of implementation, (v) flexibility modes, and (vi) plan for program sustainment. The role of facilitators is crucial for the sustainability of programs and services and for maintaining the long-term effects, but staff turnover could be a barrier to implementation (Zurynski et al., 2023). The present study also has some limitations. Firstly, most of the sample was predominantly female caregivers, with low enrollment from fathers; then, the findings could be generalized carefully for all caregivers. Secondly, the evaluation was based exclusively on reports using one informant that could bias answers to the questionnaire. However, a previous RCT evaluating the ACT intervention demonstrated that a second informant had a similar perception of change in a child’s behavior to their caregiver participating in the program (Altafim & Linhares, 2019). Furthermore, as demonstrated by a systematic review and meta-analysis, most RCTs on parenting interventions use self-report data (Backhaus et al., 2023). Thirdly, the RCT included a short-term post-intervention evaluation without follow-up. Even though previous RCTs have shown that improvements in parenting (Portwood et al., 2011) and children’s behavior persist after three to four months (Altafim & Linhares, 2019), verifying follow-up data in a large-scale study is necessary. Finally, the data collectors were the facilitators, which did not allow blind conditions to be guaranteed; however, this procedure made it possible to carry out a large-scale study with low resources. This aspect is fundamental because there is a shortage of RCTs with large samples (Backhaus et al., 2023). Furthermore, as a methodological care, the facilitators did not have access to the participants’ scores of the instruments to avoid potential differential treatment, and all the data analysis was conducted after the end of data collection. The study presents practical implications by contributing with an efficacious intervention to prevent violence against children, capacity-building workers to scale up the program, improving public services, and spreading family benefits. The study demonstrated that the ACT Program is a short intervention that could be used as a modular strategic intervention aligned with standard programs implemented in the Social Protection Assistance Services and the educational context. The modularity principle facilitates implementing interventions at a large scale (Center on the Developing Child - Harvard University, 2016; Parker et al., 2020). Based on the current RCT findings, the ACT Program could be linked to cash transfer programs that benefit vulnerable families with children at an early age. The ACT Program includes a session about spreading its contents in families and communities, contributing to improving the ecosystem of violence prevention against children. Therefore, the stakeholders could have an effective parenting program with a low cost, delivered in-group, in a short period to implement in their policy systems, contributing to breaking the intergenerational cycle of violence. However, evidence at large scale is insufficient to sustain the program in the policy system, requiring a long-term workforce and engagement of the governments with actions to continue. At the end of the present study, the researchers offered a report for each municipality, showing how to maintain the ACT Program in their services. Future studies should address new questions. Firstly, a follow-up study is necessary to better understand the duration of the effects of the intervention in the medium-term. Secondly, fathers’ engagement should be examined to determine if some adaptation will be necessary in the ACT Program to enhance adherence and engagement. Thirdly, disaggregated analysis by ethnicity, gender, marital status, and region variables could be used to understand better if the ACT Program has a differential effect on the families. Fourthly, evaluation of the outcomes comparing families with and without cash transfers could be explored. Finally, the implementation outcomes associated with the findings of this RCT study could be examined. As highlighted by Rodrigo (2016), the large-scale implementation outcomes to measure the quality of an evidence-based parenting program in family services is necessary to guide the best practices, examining the factors related to the implementation and for whom and under conditions the program presents positive outcomes. The context, process, and participant response in implementing family support programs are relevant factors for the sustainability of the programs in the “real world” (Byrne et al., 2023). Then, the implementation measures could add complementary information on the outcomes of the ACT parenting program on families. The current RCT confirmed the ACT theory of change, demonstrating positive effectiveness in a scaling policy system, adding information on improvements in emotional and behavioral regulation practices, positive discipline, parental sense of competence, and caregivers’ home stimulation and decreased parental inconsistency, coercive practices, and children’s behavior problems in families living under high adverse social conditions. Therefore, the ACT showed effectiveness when implemented in the “real world” and is ready for broad dissemination in the public policy system. Conflict of Interest The authors of this article declare no conflict of interest. Acknowledgements We acknowledge all the team members involved in the ACT Ceará initiative. We also acknowledge the families that agree to participate in the study, the professionals who implement the parenting program with the families, and the agreement of the governments at municipal and state levels (Ceará State and Programa Mais Infância Ceará) to perform the study in public services. We are also grateful for all the support of the Institute for Valorization of Education and Research of the State of São Paulo (IVEPESP). We recognize the crucial support of the funders. Cite this article as: Altafim, E. R. P., & Linhares, M. B. M. (2025). Effectiveness evaluation of a violence prevention parenting program implemented at large scale: A randomized controlled trial. Psychosocial Intervention 34(2), 63-77. https://doi.org/10.5093/pi2025a6 Funding Fundação Maria Cecília Souto Vidigal, Porticus, and Van Leer supported the research, and the National Council for Scientific and Technological Development supported MBML (CNPq, Process 310726/2021-2). The funders had no involvement in the design, data collection, analysis, data interpretation, decision to publish, and writing or review the manuscript. Supplementary Material CONSORT Harms 2022 Integrated into CONSORT 2010 Items Checklist of Information to Include when Reporting a Randomised Trial 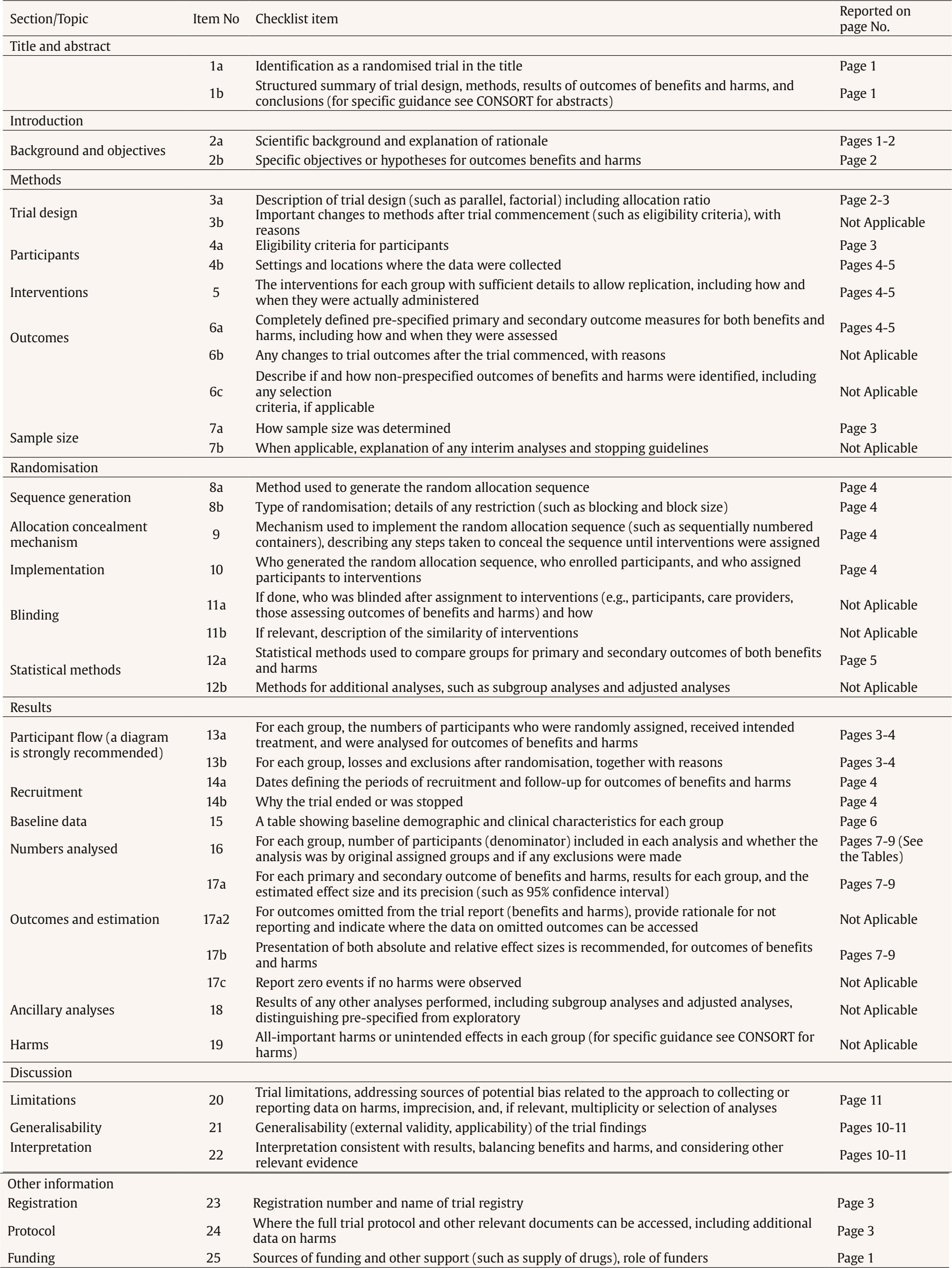 Note. Adapted from Schulz (2010) to integrate items of CONSORT Harms 2022 (Junqueira 2022) [https://creativecommons.org/licenses/by/2.0/]. CONSORT items 1b, 2b, 6a, 11a, 12a, 13a, 14a, 16a, 17a, 17b, 18, 20 and 24 of were modified to incorporate elements relevant to the reporting of harms. Two new items were added (item 6c and 17a2). Please see the CONSORT Harms 2022 statement for additional details (Junqueira 2022). |
Cite this article as: Altafim, E. R. P. and Linhares, M. B. M. (2025). Effectiveness Evaluation of a Violence Prevention Parenting Program Implemented at Large Scale: A Randomized Controlled Trial. Psychosocial Intervention, 34(2), 63 - 77. https://doi.org/10.5093/pi2025a6
Correspondence: altafim.elisa@gmail.com (E. R. Pisani Altafim) and linhares@fmrp.usp.br (M. B. Martins Linhares)., Correspondence: altafim.elisa@gmail.com (E. R. Pisani Altafim) and linhares@fmrp.usp.br (M. B. Martins Linhares).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
Send






