


Sociodemographic Variables Most Associated with Suicidal Behaviour and Suicide Methods in Europe and America. A Systematic Review
[Las variables sociodemográficas más asociadas con el comportamiento suicida y con los métodos suicidas en Europa y América. Una revisión sistemática]
Inés Cano-Montalbán, Raúl Quevedo-Blasco
Mind, Brain and Behavior Research Center (CIMCYC), University of Granada, Spain
https://doi.org/10.5093/ejpalc2018a2
Received 24 July 2017, Accepted 9 October 2017
Abstract
This Systematic Review is thought to deepen the relation between sociodemographic variables most associated with suicidal behaviour and suicide methods in Europe and America. A research was made from articles and reviews published between 2005-2015 in PsycINFO, Medline, Web of Science Core Collection, Scopus, and SciELO. Thanks to it, we retrieved 5,222 records which were analysed against the inclusion (e.g., any design of the study, published in English or Spanish) and quality criteria, including 53 studies in the review. In these results it is noticeable how men (36% of the studies) and elderly (28% of the studies) commit suicide more frequently. Women (30% of the studies) and young people (17% of the studies) have more attempts and suicidal behaviour. The most commonly used methods among them hanging (24% of the studies), firearm (17% of the studies), and precipitation (6% of the studies); unemployment (17% of the studies), rural life (9% of the studies), a marital status other than marriage (15% of the studies), and low education (23% of the studies) are also closely associated with both suicide and suicidal behaviour. Consequently, important connections can be concluded when carrying out psychological autopsies, which should be taken into ac due to their clear implications in personal and material damage that must be elucidated judicially, clarifying the specific occurrence as suicide, homicide, or accident.
Resumen
Esta revisión sistemática tiene por objetivo profundizar en la relación entre las variables sociodemográficas más asociadas con el comportamiento suicida y los métodos suicidas en Europa y América. Se realizó una investigación a partir de artículos y revisiones publicadas entre 2005-2015 en PsycINFO, Medline, Colección Principal de Web of Science, Scopus y SciELO. Se recuperaron 5.222 registros, en los que se analizaron los criterios de inclusión (p. ej., cualquier diseño de estudio, publicado en inglés o español) y de calidad, incluyendo 53 estudios en la revisión. En estos resultados se observa que los hombres (36% de los estudios) y los ancianos (28% de los estudios) presentan unas tasas superiores de suicidio que las mujeres (30% de los estudios) y los jóvenes (17% de los estudios) tienen más intentos y conductas suicidas. Los métodos más utilizados son el ahorcamiento (24% de los estudios), las armas de fuego (17% de los estudios) y la precipitación (6% de los estudios); el desempleo (17% de los estudios), la vida rural (9% de los estudios), un estado civil distinto de matrimonio (15% de los estudios) y un nivel educativo bajo (23% de los estudios) también están estrechamente relacionados con el suicidio y el comportamiento suicida. Se puede concluir la importancia de realizar autopsias psicológicas, las cuales deberán tener en cuenta los factores analizados en este estudio y sus implicaciones judiciales, dilucidando la ocurrencia de suicidio, homicidio o accidente.
Keywords
Suicidal behaviour, suicide methods, sociodemographic variables, systematic review, Europe and America
Palabras clave
Comportamientos suicidas, métodos suicidas, variables sociodemográficas, revisión sistemática, Europa y América
rquevedo@ugr.es (R. Quevedo-Blasco)
Introduction
The World Health Organization (WHO) defined suicide in 1986 as “an act with lethal outcome, deliberately initiated and carried out by the subject, knowing or expecting its lethal denouement and through which it pretends to obtain the desired changes” (Ministerio de Sanidad, Política Social e Igualdad, 2012, p. 43). However, suicide is now considered a continuum, encompassing suicidal behaviours (SB): ideation (thinking about suicide, cognitions), plans (propose methods with which to carry out suicide), and attempts (potentially self-injurious conduct with no fatal outcome that may or may not result in injury, with evidence of intentionality of causing death), as well as consummate suicide (self-inflicted death with evidence of intentionality) (Ministerio de Sanidad, Política Social e Igualdad, 2012; WHO, 2014). Therefore, suicide also supposes both a big economic and a public health problem, being among the first fifteen causes of death in all ages and second and third in the groups of 10-24 and 15-44 years respectively, daily happening many more attempts which have not been consummated according to the Ministerio de Sanidad, Política Social e Igualdad (2012) . This report also states that, in the USA, the annual economic cost (both direct and indirect) reaches 25,000 million dollars. In Europe, the (also annual) costs are changeable. For example, in Ireland the cost has been around €835 million, in Scotland the estimated cost has been £1.08 billion (Centre for Suicide Prevention, 2010), and in England the cost has reached £1.45 million (Expert Platform on Mental Health, 2011). According to WHO (2014) , every year the suicide number exceeds 800,000, happening one each 40 seconds and adding around 804,000 suicide deaths around the world in 2012, with an annual worldwide rate of 11.4/100,000, the majority being men (15:8). Although psychological autopsies show that around 90% of people who commit suicide have mental disorders, the most usual being depression, substance abuse, psychotic disorder, personality disorder, and anxiety, among others (Ministerio de Sanidad, Política Social e Igualdad, 2012). Rodríguez-Carballeira et al. (2015) state that the psychological abuse group considered could lead to extreme behaviour in the so-called collective suicide; there are also other protection and risk factors (see for example, López-Ossorio, González Álvarez, Buquerín Pascual, García, & Buela-Casal, 2017). This paper focuses on some of them. If we look at suicide rates, countries with high income per inhabitant have a higher suicide rate than countries with lower income (WHO, 2014). Lithuania and Russia are the two countries on top of the list (51.6 and 43.1/100,000 respectively) contrasting with Azerbaijan and Philippines (1.1-2 and 2.1/100,000 respectively), which have the lowest rates. In Europe, where suicide is the tenth cause of death, the highest rates are located in Eastern Europe and in the Nordic countries, where differences according to gender have also been found, and with a rate of 4:1 in the West and 3:1-7.5:1 in the rest of the world, without differences in India or in China (Ministerio de Sanidad, Política Social e Igualdad, 2012). Regarding age, the majority of cases are under the age of 45, a fact that repeats in all continents, with the lowest rates in children under the age of 15 and increasing again in people over 70 years or older (WHO, 2014). Even so, in Europe cases in young people have multiplied by four (Ministerio de Sanidad, Política Social e Igualdad, 2012). Furthermore, it must not be forgotten that the previous information shows the importance of knowing the risk factors associated with these deaths in order to be able to evaluate and prevent the problem, as well as to promote an effective prevention policy. Therefore, the aim of this study is to analyse sociodemographic variables (sex, age, marital status, employment status, education, and place of residence) which are more closely related to suicidal behaviour (ideation, plans, and suicide attempts) and suicide, as well as the suicide method, in the general population in Europe and America. MethodDesign and Procedure This work focuses on a Systematic Review (SR) following the criteria by Perestelo-Pérez (2013). From April 19th to May 24th 2016, a bibliographic search of “articles” and “reviews” published between 2005 and 2015 (both years included) was carried out with PsycINFO, Medline, Web of Science Core Collection, Scopus, and SciELO databases. When we check these databases (and the types of documents) there may be biased publications, which could imply that some studies should be excluded because of their deficient statistic results or because of not being clinically meaningful. These studies will not take part in the databases that will be analysed. The key concepts which have been used were: < Selecting Criteria The criteria born in mind to select the studies were: - General population sample or psychology autopsy of death labelled as “suicide”. - Carried out in Europe, America (North and South) and published between 2005-2015 (both years included). - imagenes Data about suicide behaviours related to the variables sex, age (no age limit), marital status, employment state (employed or unemployed), education, suicide method, and/or residence area (rural or urban). - Without restricting the type of the design of the study. - Published either in English or in Spanish. - Works that were articles and reviews. - High (score between 15-23) or medium (score between 9-14) methodological quality (see Study Selection and Methodological Quality section). Study Selection and Methodological Quality In the studies, after examining titles and abstracts to check that they meet the selection criteria, we selected those who met some of the criteria. When this was not enough, the entire text was checked and in case of not fulfilling any of the previous criteria, the paper was removed. Finally, in the studies that were finally included, the methodological quality was evaluated through an adaptation of the Meta-analysis of Observational Studies in Epidemiology (MOOSE) by Stroup et al. (2000). This adaptation was created previously to its use so that the checklist was adjusted to the type of work which had been expected and that it was strict to guarantee the quality of the studies included. Moreover, when doubts were considered regarding criteria, there was a discussion in order to reach a conclusion. Studies were classified in three groups according to their quality: high (with a score between 15 and 23), medium (with a score between 9 and 14) or low (with a score between 0 and 8). Both low-quality studies and those medium or high quality which did not provide the expected data about the variables under study (outcomes procedures) were removed. Furthermore, for data extraction from all the works finally included they used a codification book where works were organized by title, authors, and year of publication along with all the information that was considered important or that could contribute something to the SR. ResultsSearch and Study Selection From the 5,222 articles and reviews, after removing duplicate articles (25), 115 (2.19%) were included once we checked that the “title” and/or “abstract” fulfilled any of the selection criteria. Fifty-three of them (1%) were excluded after a complete reading and once it was found that despite fulfilling some criteria they failed to comply with others (e.g., articles about suicide methods published between 2005-2015 but carried out in Asia). From those, 69% were high-quality, 24% were medium-quality, and 7% were low-quality studies. Once 4 low-quality works were removed along with 5 other studies that did not contribute enough information of the variables (outcomes), the final sample consisted of 53 (1%) articles and reviews (see Figure 1).
Characteristics of the Studies Most relevant characteristics of the articles and reviews included in this SR (references with asterisk) are specified in Table 1 (samples and interval of years analysed in each study) and Table 2 (variables and main results).
Table 1
Information to the Sample Display and Years in Which the Studies Were Analysed 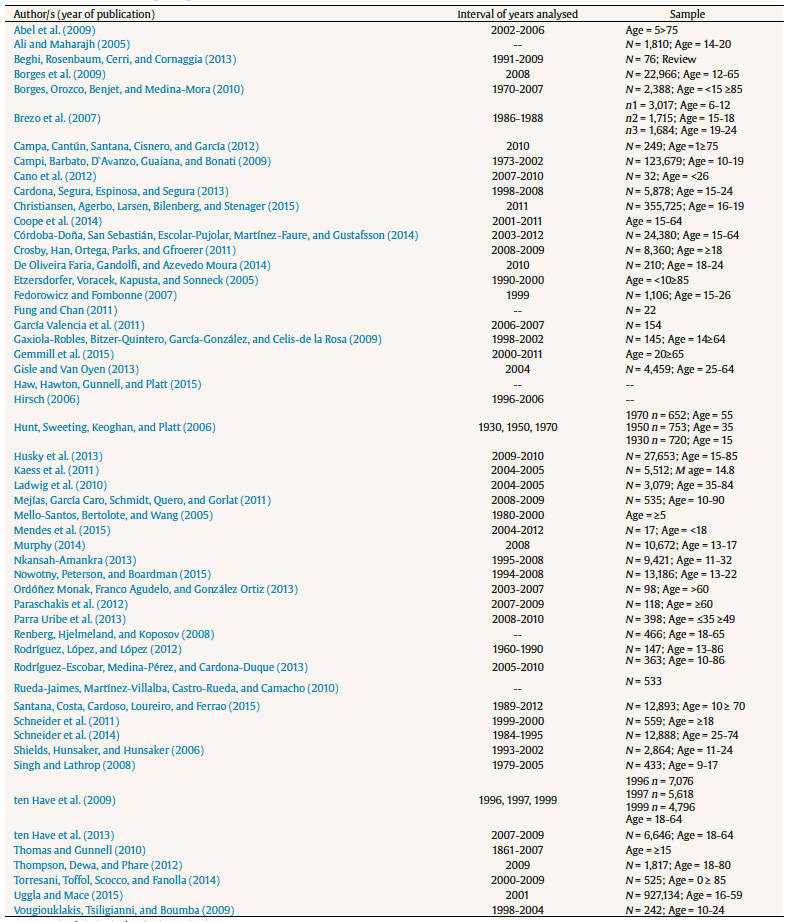
Table 2
Variables and Main Results of the Analysed Studies 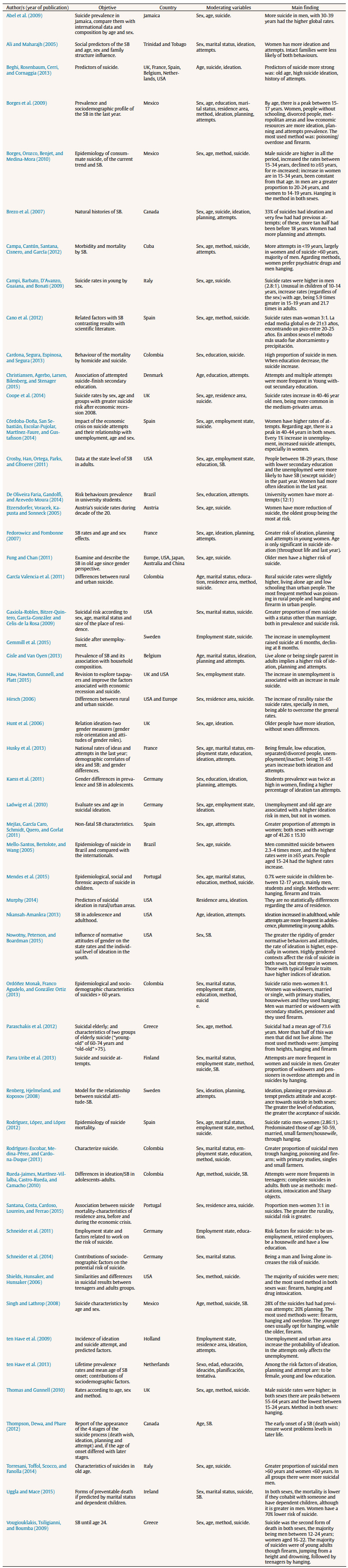
Analysis of the Studies From the 34 studies containing information about sex, 55.8% show a high rate of suicide in men and 47% a high ideation, planning, and attempt rates in women, the most frequent of them being the latter (18%), mainly because of the methods used by each one. As for education, according to the 14 studies, 85.7% indicate higher SB among those who have low education. Concerning residence area, 71.4% of the 7 studies share the fact that rurality is closely related to suicide (51.7%) and with the rest of SB (14.28%). Regarding marital status, 61.54% of the 13 studies show higher rates above all the SB in those with a marital status other than marriage; related to this and as far as age is concerned, we found that from the 27 works with this information, we can find more suicide (55.5%) than the rest of suicide behaviours (11.1%) in older people, contrasting with 26% and 33.3% that show more suicides and the rest of suicide behaviours respectively in younger people. One of the explanations to take a look at is that in the elderly it is easier to be a widow. Relating to the 12 studies regarding employment situation, the 75% show more suicide (33.3%) and the rest of the SB (41.6%) in those people who are unemployed. Lastly, but not least importantly, the most used methods are hanging (81.3%), firearm (56.3%), poisoning/overdose (43.7%), and jumping from a height (18.7%), according to 16 works with this information. Moreover, the relations between the variables will be commented in greater depth in the following section. Discussion and ConclusionThe goal of this SR was to analyse the relationships between the sociodemographic variables that are more closely related to the SB, as well as the way that is used to commit suicide among the general population in Europe and America. The outcomes concerning sex show that being a woman is more associated with suicide ideation, planning, and attempt, with a prevalence of the first and third variables (e.g., Husky, Guignard, Beck, & Michel, 2013; ten Have, van Dorsselaer, & de Graaf, 2013). Nevertheless, Hunt, Sweeting, Keoghan, and Platt (2006) found that in older people the ideation appeared to be the same in both sexes. On the other hand, being a man increased not only the frequency but also the risk of suicide (e.g., Coope et al., 2014; Gaxiola-Robles,Bitzer-Quintero, García-González, & Celis-de la Rosa, 2009). This distinction is due to the fact that men use suicide methods that are more lethal, such as hanging or firearms, so they manage to achieve suicide, implying 60-70% and 85-90% of these fatalities respectively, in contrast with 2% of psychiatric drugs used by women (Campa, Cantún, Santana, Cisnero, & García, 2012; Fung & Chan, 2011; Miller, Azrael, & Barber, 2012). In spite of this, autopsies have revealed that both genders use more frequently as suicide methods hanging, poisoning/overdose, and firearms (e.g., Borges et al., 2009; Paraschakis et al., 2012). There are also differences concerning rural areas and countries with low and medium outcomes, where poisoning/intoxication prevails due to the accessibility to pesticide residues used in farming, whereas in urban environments firearms are preferred. This latter suicide method affects 46% of suicide in USA because firearms are legal; this also applies to 18% of low-income countries, together with 50% of the suicides committed through hanging (García Valencia et al., 2011; Ministerio de Sanidad, Política Social e Igualdad, 2012; WHO, 2014). Regarding marital status, we find a greater probability of all SBs in people with a status other than marriage, the most common suicide being in single people, and ideation, planning, and attempts in separated/divorced/widowed people (e.g., Borges et al., 2009; Gaxiola-Robles et al., 2009; Rodríguez-Escobar, Medina-Pérez, & Cardona-Duque, 2013). Therefore, marriage seems to be a protective factor, with a risk of suicide 3.3 and 18.32 times higher among people who are widowers or separated/divorced, respectively (e.g., Fung & Chan, 2011; Gaxiola-Robles et al., 2009). These percentages decrease when people live in couple with children to take care of (Uggla & Mace, 2015). However, Rodríguez, López, and López (2012) found more suicide episodes among people who were married, even if it cannot be concluded that these outcomes were significant since the sample was distorted because of having high rates of married people. The suicide related to the marital status can be associated with age: although different studies show different rates, most of them are common in people of older age (e.g., Beghi, Rosenbaum, Cerri, & Cornaggia, 2013; Coope et al., 2014). In this group of people is more common to be a widower, and also other risk factors, such as chronical diseases (Fairweather-Schmidt, Anstey, Salim, & Rodgers, 2010), appear and they have a higher intentionality using methods which are more lethal (Ministerio de Sanidad, Política Social e Igualdad, 2012). Moreover, due to the increase of life expectancy and a greater accessibility to health services, the population seem to grow older showing a higher number of old adults, implying a rise in the rates of this group and making them more noticeable than the ones of the young people (Beautrais, Collings, Ehrhardt, & Henare, 2005). Despite the fact that some studies have shown more ideation, planning, and attempts among young people - especially the latter (e.g., Nkansah-Amankra, 2013; ten Have et al., 2013) -, other studies find higher rates of suicide in these people (e.g., Cano et al., 2012; Vougiouklakis, Tsiligianni, & Boumba, 2009). It seems that suicide ideation and attempts tend to appear in young adults, increasing the risk of suicide after puberty (Beautrais et al., 2005; Gisle & Van Hoye, 2013; Ministerio de Sanidad, Política Social e Igualdad, 2012). The disagreement among studies may be associated to the age of the sample collected and the fact that even if suicide has increased among older people, the rates of young people have been increasing over the last years (Ministerio de Sanidad, Política Social e Igualdad, 2012). Referring to education, an agreement exists, as it has been found that every SB occurs among people who have a low level of education - the lower the education the higher the suicide rate (e.g., Cardona et al., 2013; Husky et al., 2013). De Oliveira Faria, Gandolfi, and Azevedo Moura (2014) found more attempts among women studying at the university. Considering the employment situation as a matter to be studied, the rates of SBs are higher among unemployed and retirees/pensioners (e.g., Crosby, Han, Ortega, Parks, & Gfroerer, 2011; Schneider et al., 2011), and this could be associated with the fact that losing an employment or retiring may imply a stressfull situation, increasing the risk of suicide by 2-3 times (Ministerio de Sanidad, Política Social e Igualdad, 2012). Finally, rates are higher in all SBs in rural areas, where suicide is more frequent (Borges et al., 2009; Santana, Costa, Cardoso, Loureiro, & Ferrao, 2015) as there is a higher accessibility to tools and methods to commit suicide. However, according to Murphy (2014), when we refer to ideation, there are not differences regarding the area of residence. In spite of all the information obtained, this SR has the restriction of a possible publication bias, so for future research other journals which do not appear in the databases used should be taken into account. Furthermore, it was decided not to include psychopathological variables because the role of certain mental illnesses (e.g., depression or anxiety) is better known, and the results are more stable and clearer than other types of variables such as those chosen for this SR. Despite of the fact that these variables appear to be unconnected, this SR made the relationship between each of them and the SB clear, including the relationship between several of them. For the aforesaid, it would be advisable to expand the search with variables which, even if not closely associated with SB for future research, at least should provide important information as, for instance, sexual orientation, since different studies show that groups of Lesbians, Gays, Bisexuals, and Transsexuals have a higher risk of SB (Eisenberg & Resnick, 2006; Haas et al., 2010; Harris, 2013; Liu & Mustanski, 2012; Power et al., 2016). In view of all this, intervention and/or prevention plans (with instruments that detect, for example, psychological abuse; see Saldaña, Rodríguez-Carballeira, Almendros, & Escartín, 2017) can be set up and targeted at groups that are more frequently associated with SBs. Other aspect to be mentioned is that in the flow chart a number of duplicate studies can be found in lower amount than studies excluded because they did not meet the inclusion criteria. That is the reason why the search was focused, among other databases, on the Web of Science Core Collection, in addition to the use of specific search criteria rather than more generic ones. To conclude, the results show that men exceed women in consummated suicide, whereas in women the rest of SBs prevail, mainly attempts. In general, in both genders hanging, firearm use, and jumping from heights are more frequently used as a method of suicide. As for age, although consummated suicides are increasing among teenagers, they still prevail in older age (contrasting with ideation, planning, and attempts). Finally, unemployment, rurality, marital status other than marriage, and low education are associated with all SBs. These results should be taken into account when carrying out psychological autopsies, as they help to differentiate between actual suicides and possible homicides or accidents disguised as suicides. Being aware of clinical (characteristics of suicides/homicides), statistical (trends in space and time, related, for example, with the most common methods for committing suicide), and epidemiological (identification of risk factors) aspects is extremely important when carrying out such autopsies (Morales, 2006). Ruling out that there are no third persons involved (when it is not the case of a suicide) is a key factor in the legal field and during judicial proceedings. Furthermore, if we compare this SR with other recent publications (Franklin et al., 2017; Huang, Ribeiro, Musacchio, & Franklin, 2017; Ribeiro et al., 2016), we could find that this SR allows us to have relevant information in a single study regarding the variables that are more closely associated to suicidal behaviour (sex, age, marital status, employment status, residence area, education), the most commonly used suicide methods, and the relationship between all variables. In addition, the database used and the year range selected (ten years) allows us to have a very complete, comprehensive, and quality information. References |
rquevedo@ugr.es (R. Quevedo-Blasco)
Copyright © 2026. Colegio Oficial de la Psicología de Madrid





 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
The European Journal of Psychology Applied to Legal Context is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License








