


Contribution of Brain Cortical Features to the Psychological Risk Profile of Juvenile Offenders
[La contribuci├│n de las caracter├şsticas corticales al perfil de riesgo psicol├│gico de los delincuentes juveniles]
Iván Padrón1, 2, Daylin Góngora3, Iván Moreno4, María José Rodrigo1, 2, and Ana M. Martín5
1Instituto Universitario de Neurociencia (IUNE), Universidad de La Laguna, Santa Cruz de Tenerife, Spain; 2Departamento de Psicolog├şa Evolutiva y de la Educaci├│n, Universidad de La Laguna, Santa Cruz de Tenerife, Spain; 3Departamento de Ciencias M├ędicas B├ísicas, Universidad de La Laguna, Santa Cruz de Tenerife, Spain; 4Departamento de Psiquiatr├şa, Hospital Universitario de Canarias, Santa Cruz de Tenerife, Spain; 5Departamento de Psicolog├şa Cognitiva, Social y Organizacional, Universidad de La Laguna, Santa Cruz de Tenerife, Spain
https://doi.org/10.5093/ejpalc2022a9
Received 11 February 2022, Accepted 27 May 2022
Abstract
Objectives: This study contributes to the neuroscience of offending behavior by addressing two aims: a) to examine differences in the cortical features in a group of male serious juvenile offenders (21 OG), versus controls (28 CG), both ranging from 18 to 21 years old; and b) to determine to what extent the differential cortical features and the risk psychological profile discriminate between the two groups. Method: Besides cortical measures, demographics, executive functioning, childhood trauma, psychopathic traits, psychopathological symptoms, and antisocial and delinquent behavior were assessed. Results: Whole-brain analysis of the cortical mantle identified increased cortical thickness in the cluster comprising the right middle temporal gyrus and a smaller surface area in the lateral orbitofrontal cortex for the OG compared to the CG. The discriminant function correctly classified 100% of cases of the CG and 94.7% of the OG. Right temporal cluster, childhood trauma, callousness and symptoms of interpersonal sensitivity, psychoticism, depression, phobic anxiety, and obsessive-compulsive behavior contributed to the OG. In turn, the lateral orbitofrontal cluster, psychopathic traits of grandiosity, unemotionality, and thrill seeking, and working memory contributed to the CG. Conclusions: The increased right middle temporal gyrus of the OG could be indicative of impaired brain development in social cognition processes since it appeared in combination with the higher risk profile. The reduced orbitofrontal cortex could be indicative of immature brain development in emotional control processes since it appeared in combination with the normative psychological profile in adolescence. Based on these novel findings, areas of potential improvement for research and intervention are suggested.
Resumen
Objetivos: Este estudio contribuye a la neurociencia de la conducta delictiva abordando dos objetivos: a) examinar las diferencias en las características corticales en un grupo de delincuentes juveniles de sexo masculino (21 GD), frente a los controles (28 GC), ambos con edades comprendidas entre los 18 y los 21 años; y b) determinar hasta qué punto las características corticales diferenciales y el perfil psicológico de riesgo discriminan entre los dos grupos. Método: Además de las medidas corticales, se evaluaron los datos demográficos, el funcionamiento ejecutivo, el trauma infantil, los rasgos psicopáticos, los síntomas psicopatológicos y el comportamiento antisocial y delictivo. Resultados: El análisis del manto cortical de todo el cerebro mostró un mayor grosor cortical en el clúster que comprende la circunvolución temporal media derecha y una menor superficie en la corteza orbitofrontal lateral para el GD con respecto al GC. La función discriminante clasificó correctamente el 100% de los casos del GC y el 94,7% del GD. El clúster temporal derecho, el trauma infantil, la insensibilidad y los síntomas de sensibilidad interpersonal, psicoticismo, depresión, ansiedad fóbica y comportamiento obsesivo-compulsivo contribuyeron al GD. Por su parte, el clúster orbitofrontal lateral, los rasgos psicopáticos de grandiosidad, impasibilidad y búsqueda de emociones y la memoria de trabajo contribuyeron al GC. Conclusiones: La alteración temporal media derecha del GD podría ser indicativa de un desarrollo cerebral alterado en los procesos de cognición social, ya que este rasgo cortical apareció en combinación con el perfil de mayor riesgo. La reducción en el área orbitofrontal podría ser indicativa de un desarrollo cerebral inmaduro en los procesos de control emocional, ya que apareció en combinación con el perfil psicológico normativo en la adolescencia. A partir de estos hallazgos novedosos, se proponen áreas posibles de mejora para la investigación y la intervención.
Keywords
Cortical thickness, Cortical surface area, Juvenile offenders, Childhood trauma, PsychopathyPalabras clave
Grosor cortical, ├ürea de superficie cortical, Delincuentes juveniles, Trauma infantil, Psicopat├şaCite this article as: Padrón, I., Góngora, D., Moreno, I., Rodrigo, M. J., & Martín, A. M. (2022). Contribution of Brain Cortical Features to the Psychological Risk Profile of Juvenile Offenders. The European Journal of Psychology Applied to Legal Context, 14(2), 93 - 103. https://doi.org/10.5093/ejpalc2022a9
ammartin@ull.edu.es Correspondence: ammartin@ull.edu.es (A. M. Mart├şn).Most adolescents who commit crime desist as they become adults (Moffitt, 2018). The peak of criminal behavior in relation to age is 17-18 years old (Farrington et al., 2012), and spontaneous desistance occurs in early adulthood (Doherty & Bersani, 2018). The highest percentage of crimes are perpetrated by a small proportion of young offenders who continue to offend into midlife and beyond (Baglivio et al., 2020). Developmental Criminology explains this evidence by relating criminal behavior to an individual’s development along the life course. Research carried out from this perspective has focused on variations in criminal behavior over time, the factors related to its onset, maintenance, and desistance, and the risk and protective factors associated with this development (Morizot & Kazemian, 2015). Evidence provided by this line of research has led to the disclosure of different criminal careers (Farrington, 1986) and delinquent profiles (Moffitt, 1993). Moffitt (1993) distinguishes between two qualitatively different delinquent profiles: those whose antisocial activity is limited to adolescence and those whose activity persists throughout their life. Life-course-persistent delinquents commit a wide range of crimes, including violent ones, whereas adolescence-limited delinquents commit crimes that are less serious, nonviolent, and more related to adolescent defiance attitudes (Farrington & Ttofi, 2015). Different risk factors have been proposed for each delinquent type (Moffitt, 2006; Moffitt et al., 2001). Life-course-persistent criminal behavior has been associated with exposure to early life adversity (Moffitt, 2018; Moffitt et al., 2002), psychopathy (McGee & Moffitt, 2019; Moffitt, 1993), and neurodevelopmental deficits (Moffitt, 1990), which are not observed in the adolescence-limited delinquents. Research on exposure to adverse childhood experiences has shown that the number, severity, and diversity of adverse experiences that children are exposed to have an impact on their future maladaptive behaviors, including depression (Allwood et al., 2011), anxiety (Tatar et al., 2012), aggressive behavior (Ford et al., 2012), delinquency in general (Baglivio et al., 2015), and offenses related to child-to-parent violence in particular (Nowakowski-Sims & Rowe, 2017; see reviews by Jaffee, 2017 or Teicher & Samson, 2013). At this point, it is worth noting that the relationship between offending behavior and psychopathology is complex (Grisso, 2008). The percentage of youth with mental health needs in the juvenile justice system is higher than in the community and seems to be increasing (Fazel et al., 2008). However, this percentage should not be explained in terms of a causal relationship but rather as a spurious one in which exposure to adverse childhood experiences plays a central role (Colins & Grisso, 2019). Early traumatic experiences promote, among other effects, irritability, impulsiveness, or substance use, which are risk factors for juvenile delinquency, characteristics that are currently used to assign diagnoses of mental disorders such as depression, traumatic stress, attention deficit disorder, or substance use disorders (Colins & Grisso, 2019). The second risk factor pointed out by Moffitt (McGee & Moffitt, 2019; Moffitt, 1993), psychopathy, has been consistently associated with criminal behavior (Marques et al., 2022), and this association has been documented across the life course (Farrington & Bergstrøm, 2022). Psychopathy is defined as a personality construct that involves “self-regulation problems, a manipulative, exploitative, and selfish interpersonal style, and reduced conscience illustrated by reduced empathy, remorse, or guilt” (DeLisi et al., 2021, p. 1). The classical conceptualization of psychopathy (Cleckley, 1988; Hare, 2003) distinguishes among ten personality traits that cluster in three dimensions: affective, interpersonal, and behavioral (Cooke & Michie, 2001). The affective dimension of psychopathy, callousness-unemotionality, has long been associated with an earlier onset of conduct problems (Brandt et al., 1997), with the severity and stability over time of these problems, and with delinquent behavior (Frick et al., 2014). The third risk factor of offending behavior identified by Moffit (1990) is neurodevelopmental deficits. These deficits have been associated with specific functions related to some brain features (Casey et al., 2022). The bulk of the research connecting offending behavior and brain functioning has focused on executive functioning. Differences between offenders and non-offenders, or between different types of offenders, have been stated in relation to planning, cognitive flexibility, and inverse learning (Broche-Pérez & Cortés-González, 2015). Also, impaired performance in working memory, decision making, risk-taking behavior (Syngelaki et al., 2009), and inhibition of interference (Borrani et al., 2015) has been found for young offenders. Meta-analyses with adults (Morgan & Lilienfeld, 2000; Ogilvie et al., 2011) and juvenile offenders (Gil-Fenoy et al., 2018) have concluded that offender performance is impaired in neuropsychological tasks that involve executive functions. However, Borrani et al. (2019), in comparing adult and young offenders, concluded that the latter display more neuropsychological disorders than the former in planning, inhibition, and cognitive flexibility. At this point, it is worth noting that there are differences in the size of the effect for adult and young, violent, and non-violent offenders (Meijers et al., 2015; Meijers et al., 2017), and that institutionalization may reduce self-control and attention even after only a three-month prison stay (Meijers et al., 2018). Also, some studies have been criticized because the offender and control groups sometimes differed in age, education level, diagnoses of psychopathological disorders, and number of risk factors in relation to both delinquency and psychopathology (Moreira et al., 2020). Even considering these cautions, the studies on executive functioning cited above, taken as a whole, suggest that some types of offenders, especially among young offenders, have delayed development of the prefrontal cortex. However, research relating offender behavior and brain neuroanatomical features is scarce. The Present Study The main aim of this study is to fill this gap by assessing whether there are differences in the cortical features of a group of young offenders when compared to a control group matched in age and with a similar sociodemographic profile. The cortical measures include overall gray matter volume, more specific measures of cortical thickness, which is a measure of the density of the neurons in the cortex layer, surface area of cortex regions, and cortical folding or gyrification, which reflects the amount of cortex folded within the sulci of the brain versus that found outside the sulci (Rakic, 2009; Raznahan et al., 2011). Cortical thickness and surface area each have their own cellular mechanism and genetic underpinning, thus providing unique and complementary information on the cortex (Chen et al., 2013). During adolescence, the brain undergoes a remarkable number of changes in grey and white matter volume, connectivity, myelination, and synaptic pruning that continue into early adulthood (Paus et al., 2008; Spear, 2010; Tamnes et al., 2017). These changes are related to the increases in risky and antisocial/offending behavior that occur more frequently during this period of the lifespan than in adults over 25 (Fairchild, 2011; Steinberg, 2008). A second objective of the study is to determine to what extent the differential cortical features and the risk psychological profile discriminate between the two groups. On one hand we have the cortical features of both groups and on the other hand we have two risk factors associated by Moffitt (1993) with life-course-persistent delinquents: exposure to adverse childhood experiences and psychopathy. Psychopathology is also measured, given its relationship with early traumatic experience. Self-report measures of antisocial and violent behavior of individuals from both groups are used. Evidence has largely shown that experiencing child maltreatment is associated with vulnerability to mental health needs, such as depression, bipolar disorder, anxiety, and post-traumatic stress disorders over the course of the lifetime (see reviews by Jaffee, 2017; Teicher & Samson, 2013). The exposure to early life adversity that challenges adolescent and adult functioning is also associated with life-course-persistent antisocial and criminal behavior (Moffitt, 2018; Moffitt et al., 2002). What is new here is to examine which is the respective contribution of certain brain cortical features and the psychological risk profile to the discrimination between the two groups. By addressing these two objectives, we can contribute to a relevant research question applied to the case of juvenile offenders, that is, the extent to which the presence of antisocial/offending behavior in the transition from late adolescence to early adulthood (18 to 21 years old) could be a signal of brain immaturity mainly observed in areas that develop late (i.e., control and social cognition areas) or a signal of an impaired brain development that is more likely to be accompanied by a psychological risk profile. The distinction between immature or defective brain developments in the transition to early adulthood could be influential in reinforcing early-year prevention and juvenile justice policies, as well as in clinical practice. Concerning the first objective, neural models of decision making in social contexts have signaled the late development of cognitive control areas (e.g., dorsolateral prefrontal cortex [DLPFC], anterior cingulate cortex [ACC], and orbitofrontal cortex [OFC]) involved in goal-directed decision-making processes and top-down emotion regulation, as well as social cognition areas (bilateral temporoparietal junction [TPJ], bilateral middle temporal gyrus [MTG], right medial prefrontal cortex [MPFC]) related to the ability to interpret the mental states of others (Blakemore & Robbins, 2012; Crone & Dahl, 2012). In this vein, two studies comparing participants in late adolescence (17-18 years old) and early adulthood (21-22 years old) in a decision-making task in social situations found that late adolescents need to employ more neural resources than early adults in the right DLPFC and the right TPJ in risk situations (Rodrigo et al., 2014). Furthermore, when choosing the dangerous option (e.g., taking a drug) and experiencing the emotion of regret after receiving a negative result (e.g., feeling very bad), early adults as compared to adolescents show a further engagement in regions related to social cognition (bilateral MTG), harm avoidance emotion (insula), and action monitoring areas (inferior frontal gyrus and presupplementary cortex). These further activations place them in a better position to learn more about the negative consequences of risky behaviors and to reduce them in the future (Rodrigo et al., 2018). Neuroanatomical evidence in juvenile offenders is still scarce and heterogeneous, involving different categories such as antisocial and violent behavior, conduct disorder and psychopathic tendency, different structural measures using voxel-based morphometry (volume) and surface-based morphometry analyses (cortical thickness, surface area, and folding index), and varied age ranges. Several studies in youths with conduct problems related to controls reported smaller grey matter volume in the ventromedial, orbitofrontal, and dorsolateral prefrontal cortex, anterior and posterior cingulate cortex, and temporal cortex regions supporting executive function, motivation, and affect regulation (see meta-analysis by Rogers & De Brito, 2016). A review of cross-sectional studies in adolescents with conduct disorders reported lower cortical thickness in the right superior temporal gyrus, reduced surface area in the orbitofrontal cortex (OFC), and increased cortical folding in the insula relative to healthy controls (Fairchild & Smaragdi, 2018). However, cortical thinning is not always the tendency, since individual rates of change in psychopathic tendency from ages 9 to 18 have been correlated with thicker cortex measurements in the superior temporal gyrus, middle temporal gyrus, inferior temporal gyrus, parahippocampal gyrus, and posterior cingulate gyrus, particularly in males (Yang et al., 2015). Finally, 45-year-old adults from a large longitudinal birth cohort with a life-course-persistent antisocial trajectory were found to have thinner cortex and smaller surface area measurements than non-antisocial individuals in brain regions including the ventromedial prefrontal and orbitofrontal cortices, superior temporal gyrus, and posterior cingulate cortex (Carlisi et al., 2020). In our study, we expected that reductions in volume, cortical thickness, surface area, and gyrification would be more likely to be found in the ventromedial, orbitofrontal, and dorsolateral prefrontal cortex, anterior and posterior cingulate cortex, and temporal cortex regions supporting executive control, affect regulation, and social cognition processes. However, although there could be overlaps in differential areas observed in adolescents and adults, the neural signature of early juvenile offenders may involve some differences in the target areas and direction of effects. The second objective involves the combination of the differential brain areas obtained and the variables of the psychological risk profile. We evaluated a wide range of psychological variables, such as executive functioning, exposure to childhood adversity, psychopathic traits, psychopathological symptoms, and self-reported antisocial and delinquent behaviors. We selected two measures of executive functioning tapping cognitive flexibility and working memory (Diamond 2013) that have been well related to antisocial behavior in juvenile offenders (see a meta-analysis by Ogilvie et al., 2011). Likewise, measurements of exposure to childhood adversity, psychopathic personality traits, and various psychopathological disorders were included because of their direct or indirect relationship to antisocial and delinquent behavior (Moffitt, 2018; Moffitt et al., 2002). Assessments of antisocial and delinquent behavior were also performed to compare the deviation features of the offender and control groups. Next, we examined the combination of the differential brain areas and those psychological risk variables that best discriminate between the two groups. In this way we could examine the specific contribution of each brain measure and risk psychological variable to the group classification. Evidence from differential brain measures occurring in combination with variables of a higher risk profile (i.e., psychopathology symptoms, delinquent behavior) may support the hypothesis of defective brain development, whereas brain measures associated with a lower risk profile (i.e., impulsivity) may support immature brain development. Participants Forty-nine early adults (21 offender group, OG, and 28 control group, CG) of the scanned sample of 52 participated in the experiment (scan data from three juvenile offenders were eliminated for technical problems). The inclusion criteria for participants in the OG were to be over 18 years of age and have committed a serious violent crime for which they were serving a judicial measure. These crimes included robbery, theft by violence, bodily injury, family violence, reckless driving, and drug trafficking. All of them had also other previous criminal records. Participants in the OG were in an open regime at the moment of the study, after having served their sentence in semi-confinement in a prison for youth or in an educational living group (a social facility in the community). Participants in the CG did not have criminal records of any kind and were selected to match the participants of the OG in sex, age, educational level, and neighborhood. All participants had normal or corrected-to-normal vision and were right-handed according to the Edinburgh Handedness Inventory (Oldfield, 1971). The sociodemographic profile of individuals in both groups did not differ significantly, whereby the two groups can be considered comparable. With regard to sex and age, they were all males in their transition from late adolescence to young adulthood, with a range of age from 18 to 21 years old, CG: M (SD) = 18.75 (0.89); OG: M (SD) = 18.65 (0.93); t(47) = 0.71, p > .05. Participants also did not differ by level of education (only primary, secondary, and post-secondary educational level, χ2(2) = 4.932, p < .09. They lived mainly in urban areas, as opposed to rural areas, χ2(1) = 9.169, p > .05. In the selection process it was assured that none of participants had abused drugs on a continuous basis or had been diagnosed with any mental illness. However, as it was hypothesized a relationship between adversity, occurring during childhood, and adolescence, a psychopathological symptoms screening was administered to both groups and the outputs were reported in the result section. Measures Executive Tasks Wisconsin Card Sorting Test® (WCST). The 64-card version downloaded from Mueller (2011) and validated by Piper et al. (2012) is a test of mental flexibility and set shifting that takes approximately 10 minutes to administer. Subjects were instructed to match each card that appeared to one of four reference cards, without being told the matching criteria. They were given feedback on whether their response was correct or not, discovering by trial and error the sorting rule, which also changed periodically. The dependent measure was the percentage of the total number of trials with perseverative errors. A perseverative error was defined as the number of times the participant persisted in making an incorrect sorting choice that was previously correct. Verbal Working Memory. The Spanish adaptation of the Siegel and Ryan’s (1989) sentence memory test was administered. The task consists of the auditory presentation of a sentence with the last word missing and that the participant must complete. For example: the evaluator says “The planes land at the ...” and the participant must complete the sentence, for example, “airport”. Once the participant has completed the sentences, he is asked to say the words that he used to complete the sentences in the same order. The task has five levels and three trials per level. The first level has two phrases and the fifth level five. At each level the participant has three trials to carry out the task. The score is given by the last level with the maximum number of words retained. In studies with Spanish samples adequate validity and reliability indices of this test have been obtained (Hernández et al., 2012). Self-report Questionnaires Childhood Trauma Interview (CTI; Fink et al., 1995). This is a semi-structured interview for the retrospective assessment of adversity occurring during childhood and adolescence. Participants were asked about the seven domains of adversity from birth through the age of 18 and characterized each adversity on its emotional impact ranging from 1 (minimal), 3 (moderate) to 5 (severe impact): separation from caregiver/loss of caregiver; neglect by caregiver; emotional abuse; physical abuse; seeing violence at home; sexual abuse and assault; bullying or harassment by peers (added for this study). Overall mean was calculated as a final score. Youth Psychopathic Traits Inventory (YPI; Andershed et al. 2002). The YPI is composed of 50 items that assess psychopathic traits in adolescents older than 12. Participants are asked to answer on a 4-point Likert scale, from 1 (does not apply at all) to 4 (applies very well). The scale structure involves 10 factors of 5 items each, related to three dimensions: the grandiose-manipulative dimension, the callous-unemotional dimension, and the impulsive-irresponsible dimension. The grandiose-manipulative dimension includes four factors: dishonest charm, grandiosity, lying, and manipulation. the callous-unemotional dimension contains three factors: callousness, unemotionality, and remorselessness. last, the impulsive-irresponsible dimension consists of three factors: impulsivity, thrill seeking, and irresponsibility. The YPI has been adapted to Spanish by Hilterman et al. (2006), and Orue and Adershed (2015) have provided evidence of validity and reliability for a short version. Cuestionario de Conductas Antisociales y Delictivas [Antisocial and Delinquent Behavior Questionnaire A-D] (Seisdedos, 1988). This measures criminal and non-criminal antisocial behavior of adolescents from 11 to 19 years of age. The questionnaire includes a wide range of behaviors grouped in two subscales of 20 items each: antisocial behavior and delinquent behavior. Participants are asked to answer yes (1) if they have carried out the behavior described in the item, or no (0) if otherwise. Seisdedos (1988) provides evidence of reliability and validity for this questionnaire. Symptom Assessment-45 Questionnaire (SA-45; Davison, et al., 1997). This consists of a 45-item self-report of psychopathological symptoms derived from the Symptom Check List-90 (SCL-90; Derogatis et al., 1973). SA-45 is a brief, yet thorough, measure of symptomatology that has the same structure of the SCL-90, and it is often used as a screening tool. This questionnaire includes nine scales of five items each that assess the same dimensions as the SCL-90: somatization, obsession-compulsion, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism. Participants are asked to answer each item on a Likert-type scale from 0 (not at all) to 4 (very much). The SA-45 has been adapted to Spanish by Sandín et al. (2008), providing evidence of its reliability and validity. Brain Structural Measures MRI Structural Image Acquisition. High-resolution T1-weighted MPRAGE anatomical volumes were acquired on a General Electric 3T scanner located at the University Hospital’s Magnetic Resonance Service for Biomedical Research at the University of La Laguna. A total of 180 contiguous 1 mm sagittal slices were acquired with the following parameters: repetition time = 4.7440 ms, echo time = 1.9080 ms, field of view = 256 × 256 mm2, in-plane resolution = 1 mm × 1 mm, flip angle = 20°. Cortical Parcellation. The anatomical images were aligned automatically by the ACPCDETECT program (Ardekani & Bachman, 2009), which is a module of the Automatic Registration Toolbox (ART). The program takes a 3D T1-weighted structural MRI of the human brain as input and automatically detects the mid-sagittal plane (MSP), then detects the anterior commissure and posterior commissure intersection points, and finally detects eight additional landmarks (the so-called Orion landmarks) on the MSP. This information is used to tilt-correct the input volume into a standard orientation. Each realigned-T1 was submitted to FreeSurfer v6.0.0 (http://surfer.nmr.mgh.harvard.edu/) (Dale et al., 1999; Fischl et al., 2001; Fischl et al., 2002; Fischl, van der Kouwe, et al., 2004), where the function recon-all performed tissue classification and anatomical labeling. The output was visually inspected and the cases with some defects were corrected (ex: no-brain tissue included). Using the aparcstats2table function, the following statistics were extracted for the cortical measures according to the Desikan-Killiany atlas (Desikan et al., 2006): mean thickness (mm), surface area (mm2), volume (mm3), and folding index extracted for the differential cluster analyses. Surface-Based Morphometry. Cortical thickness (CT), surface area (SA), folding index, and gray matter volume (GMv) measures were obtained. Surface cortical reconstruction included: motion correction, skull tripped, automated transformation into Talairach space, subcortical white matter, deep gray matter volumetric structure segmentation, triangular tessellation of the white surface (corresponding to the grey/white matter boundary) and pial surface (corresponding to the pia mater), and automated topology correction and surface deformation that optimally place the (inner) white surface and the (outer) pial surface (Dale et al., 1999). Some deformations included surface inflation and a high-dimensional nonlinear registration to a spherical atlas. The individual white and pial surfaces created by FreeSurfer were displayed in Freeview to visually evaluate if they accurately follow the grey and white matter boundaries as recommended in the freesurfer pipeline (http://surfer.nmr.mgh.harvard.edu/fswiki/fstutorial/troubleshootingdata). FreeSurfer also provided an averaged brain in MNI standard space that was used to match surfaces across participants and compare results. The segmentation and deformation algorithms produce representations of the CT that is the average of the closest distance from the white to the pial surface and from the pial to the white surface at each vertex on the tessellated surfaces. The SA is computed at the white surface (SAw) and measured at each vertex as one-third of the area of each triangle that meets the vertex; in other words, it is the sum of the area of all the triangles that meet the vertex divided by three (Winkler et al., 2012). Besides, the surface area was also computed at the pial surface (SAp). The measure maps were smoothed using a 15 mm with a full-width at half maximum (FWHM) Gaussian filter. Clusterwise correction for multiple comparisons was performed using pre-computed z Monte Carlo simulation, including a vertex-wise/cluster forming threshold of 2.3 (p = .005), cluster-wise p-value < .05, and adjusting p-value for two hemispheres. For the SAp the cluster forming threshold allowed was 2 (p = .01). Statistical Analysis All statistical analyses were performed with the SPSS v.25 package (IBM Corp., New York, NY, USA). With the purpose of carrying out a discriminant analysis, we first performed group comparison (one-way ANOVAs) with the full set of child adversity, clinical, and behavioral assessment variables. Given the large number of variables that have factorial scores from the same instruments, these comparisons allowed us to select those showing group differences for the further phase. Then, we carried out the discriminant analysis to determine the lineal combination of cortical measures, executive variables, child adversity, and clinical (psychopathic and psychopathological measures) and behavioral measures (antisocial and delinquent behavior) that reliably distinguished between CG and OG. We also added the cortical measures which were mean thickness (mm), surface area (mm2), volume (mm3), and folding index extracted for the differential cluster analyses. In addition to obtaining the discriminant function with the typical and structure coefficients, we also continued with the predictive and classificatory part of the discriminant analysis to know how well can be predicted from the set of variables to which group a particular case belongs. Procedure A project describing the study was submitted to the government authority responsible for implementing the judicial measures applying to adolescents in the research setting. After authorization was obtained, the project was submitted to the heads of the entities responsible for implementing the legal measures. The technical staff of those entities were asked to select participants who had the characteristics described in the participant section. They were also requested to collaborate in obtaining the informed consent of the young people and their legal guardians, and to ensure that the data collection interfered as little as possible with the functioning of the center and with the youths’ daily activities. Participants of the CG were contacted on an incidental basis, through the participants of the OG, to be sure that they came from the same neighborhood and shared a similar social background. Participants of this group were chosen to match participants of the OG in all their characteristics except of having had criminal records. In the interviews with participants of both groups, they were informed of the objectives of the project, and the anonymity and confidentiality of the information they provided was reiterated. Participants first underwent standardized executive, clinical psychometric testing, and then took part in a neuroimaging session, in the same day. Participants filled out the psychometric tests in a counterbalanced order. Reading comprehension was generally good in both groups. Only in few cases the participants asked the meaning of a specific word or sentence, and the technical staff gave them a synonym or an alternative wording, assuring that they had understood its meaning. After filling in the tests, the participants entered the MRI laboratory and were prepared for the scanning session with the instruction to remain still and relaxed but not fall asleep. The scan session lasted 12 minutes without any presentation of stimuli. Finally, each participant received €35 at the end of the whole session and a pen drive with the scanned brain image for their participation. The technical staff did not know about the assignment of the participant to the control or the offender groups. The study protocol was approved by the Human Research Ethics Committee of the University of [masked for review] to protect the participants’ rights according to the Declaration of Helsinki. Group Comparison in Child Adversity, Clinical, and Behavioral Assessment Variables Groups comparisons were carried out by ANOVA. Concerning executive functions, all participants were within the normal range of cognitive and verbal abilities within the cut-off values of ±2 SD in the two screening tests: (a) the Wisconsin Card Sorting Test of executive functioning (perseverative errors), M = 16.09, SD = 6.3; and (b) the Working Memory-Sentences Test of verbal memory span (first error appearance), M = 3.05, SD = 0.65. Comparatively, control participants in the working memory task showed the first error after remembering 3.25 items, whereas participants in the offender group failed after 2.85 items retained (see Table 1). No statistically significant difference was found in the Wisconsin Card Sorting Test in the percentage of perseverative sorting errors when the card category was shifted. The groups differed significantly in most psychological risk variables related to child adversity, psychopathy, psychopathology, and antisocial behavior/delinquency, as shown in Table 1. The OG had experienced more negative events and a more severe impact of childhood trauma than the CG. Specifically, moderate to extreme impact was observed in loss of the main caregiver (40%, 10.7%), neglect (15%, 0%), emotional abuse (35%, 10.7%), physical abuse (30%, 10.7%), eyewitnessing violence at home (30%, 0%), sexual abuse (0%, 0%), and bullying (10%, 14%). Table 1 Means, Standard Deviation and Contrast Statistics for the Control Group and the Offender Group in Executive, Child Adversity, Clinical, and Behavioral Variables  *p ≤ .05, **p ≤ .01, ***p ≤ .001 In relation to psychopathy, the OG scored higher on callousness, whereas the CG scored higher on grandiosity, unemotionality, and thrill seeking. The OG scored higher than the CG in psychopathological symptoms such as depression, interpersonal sensitivity, obsessive-compulsive behavior, psychoticism, and phobic anxiety. They also reported being engaged in a greater number of antisocial and delinquent behaviors. Differential Cortical Features in Control and Offender Groups For our first aim, we analyzed the cortical features that differed significantly between the two groups using ANOVA. A significant increment in the cortical thickness of the right middle temporal cluster was found in the OG as compared to the CG (CG: M = 2.74, SD = 0.11; OG: M = 2.89, SD = 0.15; F(1, 47) = 14.25; p < .001, d =1.14), as shown in Table 2 and Figure 1. Table 2 Differential Cortical Thickness (CT) and Differential Surface Area Estimated at the Pial Surface Area in Control and Offender Groups  Figure 1 Decreased Cortical Thickness in Control Group Versus Offender Group in One Cluster Comprising the Right Middle Temporal Gyrus. Background Brain Image Represents the Lateral View of the Right Hemisphere of the Inflated FreeSurfer Fsaverage Brain. 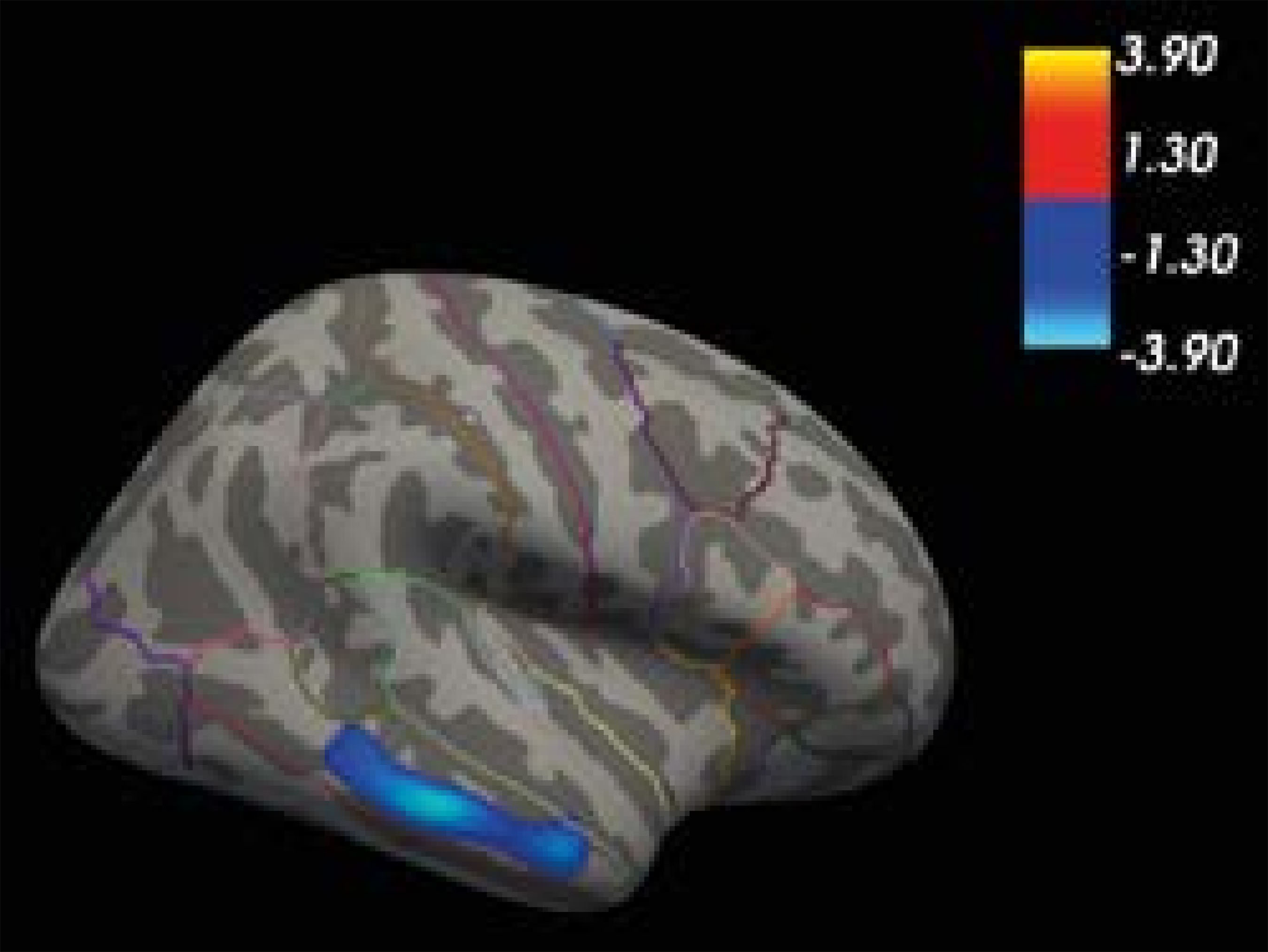 With respect to surface area (SA), there was no statistically significant difference computed at the white surface area (SAW). There was a statistically significant difference at the pial surface area (SAP) on the right lateral orbitofrontal cluster, with the offenders scoring lower than the controls (CG: M = 2896.71, SD = 277.74; OG: M = 2636.68, SD = 325; F(1, 47) = 8.63, p < .01; d = 0.86), as shown in Table 2 and Figure 2. Figure 2 Surface Area Estimate at the Pial Surface Area in the Offender versus Control Group in One Cluster Comprising the Lateral Orbitofrontal Gyrus. 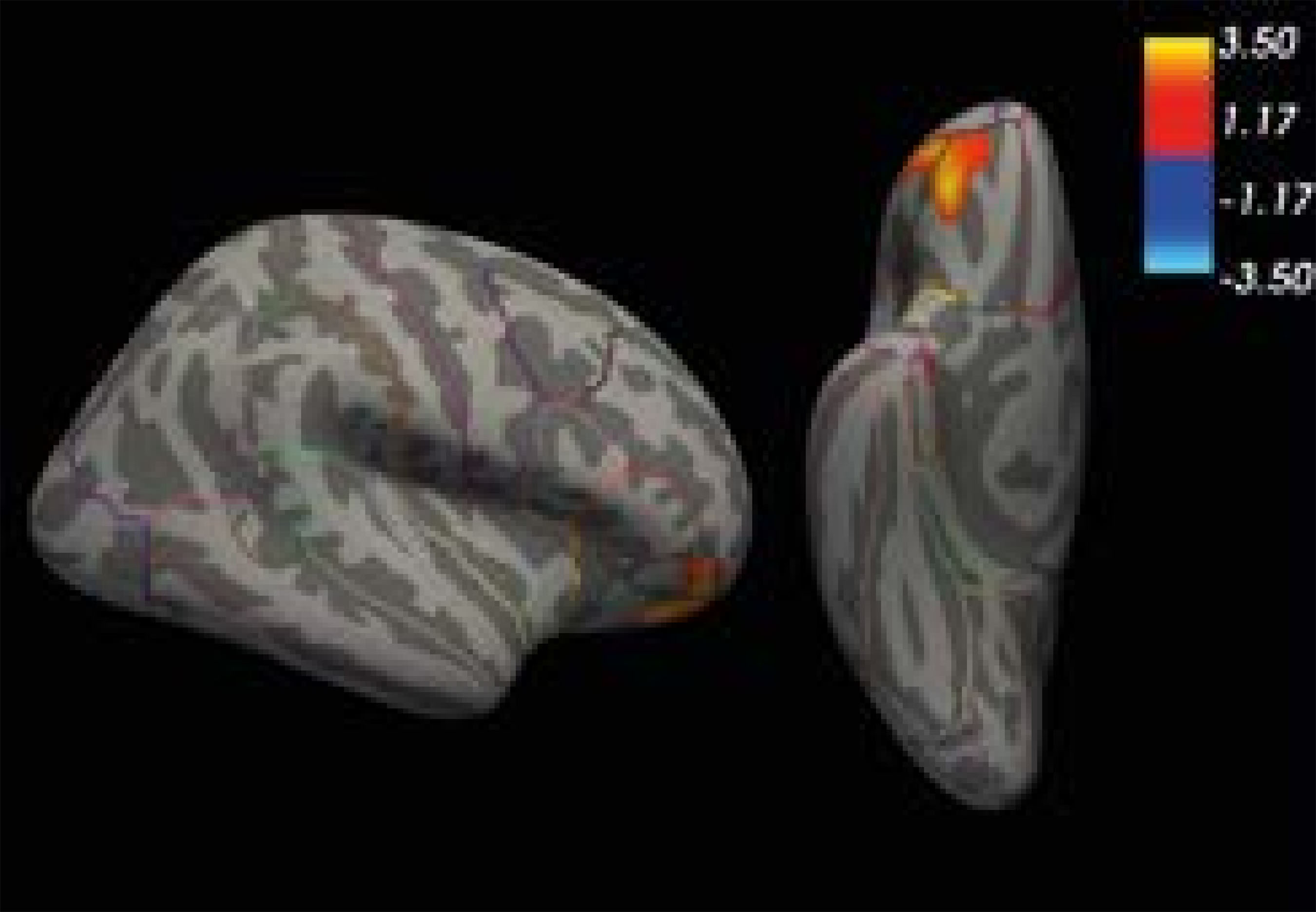 Background brain image represents the lateral view of the right hemisphere of the inflated FreeSurfer Fsaverage Brain. There were no statistically significant group differences in gray matter volume or in the folding index. Discriminant Analysis with Differential Cortical Features, Executive, Clinical, and Behavioral Measures For our second aim, we carried out a discriminant analysis to determine the combination of differential cortical features found in CT (right middle temporal cluster) and SA (right orbitofrontal cluster) that distinguishes between OG and CG. We also included in the same analysis the psychological risk variables: working memory, childhood trauma, psychopathic traits, psychopathological symptoms, and antisocial and delinquent behavior. A statistically significant function was obtained: Wilks’ lambda = .233, χ2(15) = 54.65, p < .001; canonical correlation = .876, with a non-significant Box’s M test that fulfills the assumption of equality of covariance matrices (p = .359), even with different sample sizes. To guarantee the robustness and reproducibility of the results, leave-one-out cross validations and bootstrap tests were also performed. The discriminant function correctly classified 100% of the control group and 94.7% of the offender group; bootstrap split = 0 was 97.9%. Cross validation yielded 86% and 68.4%, respectively; bootstrap split = 0 was 78.7%. A combination of 15 variables significantly contributed to the discriminant function: right middle temporal cluster (CT), lateral orbitofrontal cluster (SA), working memory, childhood trauma (CTI), grandiosity (YPI), unemotionality (YPI), callousness (YPI), thrill seeking (YPI), depression (SA-45), interpersonal sensitivity (SA-45), anxiety (SA-45), psychoticism (SA-45), obsessive-compulsive (SA-45), antisocial behavior, and delinquent behavior (see Table 3). The typical coefficients indicate the unique contribution of each variable in predicting group assignment, whereas the structure coefficients indicate the correlation between each variable and the discriminant score of the function. The negative and positive values of the coefficients were associated respectively to the centroids of the CG and of the OG (the attribution of the signs to the groups was arbitrary). As shown in Table 3, the variables that characterized the CG were the area in right orbitofrontal cluster, psychopathic traits such as grandiosity, unemotionality, and thrill seeking, and good working memory. The variables that characterized the OG group were delinquent behavior, childhood trauma, cortical thickness in right temporal cluster, antisocial behavior, psychopathological symptoms of interpersonal sensitivity, psychoticism, depression, phobic anxiety, and obsessive-compulsive, and the psychopathic trait of callousness. Comparing the typical and structural coefficients, the two cortical features, childhood trauma, and antisocial behavior contributed highly and equally well to the group assignment and the discriminant function. Moderate and similar contributions were found in psychoticism, depression, unemotionality, thrill seeking, and obsessive-compulsive symptoms. Working memory mostly contributed to the classification, whereas delinquent behavior, grandiosity, interpersonal sensitivity, callousness, and phobic anxiety mostly contributed to the discriminant function, suggesting that their contributions were made through their potential relation to other variables (i.e., antisocial behavior, depression). Table 3 Typical and Structure Coefficients of the Discriminant Function Analysis for the Control and Offender Groups on Cortical Features, Working Memory, Child Adversity, Clinical, and Behavioral Variables 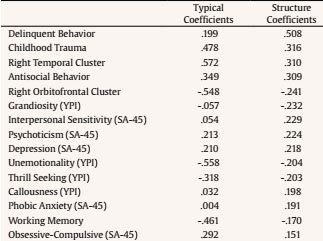 Note. Centroids of the function: CG = -1.463, OG = 2.156. This study focuses on the third risk factor associated by Moffitt (1990) with life-course-persistent offenders: neurodevelopmental deficits. Our findings may be also coherent with integrated theories of crime (e.g., Farrington, 2005) and other criminal life-course theories (e.g., Sampson & Laub, 1993), all in debt to Gottfredson and Hirschi’s (1990) general theory of crime. However, the exclusive focus of this last theory on self-control, setting aside the contribution of other factors to continuity in offending, asked for further formulations aimed to fill these gaps (Lilly et al., 2010). Moffitt’s (1990) model was one of them in stating that offending is characterized by either continuity or change, and by neuropsychological deficits, tied to brain anatomical structures that have their origin in early life experiences and that are related to psychological traits that place children and youth at risk for antisocial conduct. Based on her formulation, this study aimed to examine more specifically distinctive brain features in a variety of neuroanatomical measures and psychological risk measures to determine their classificatory value between juvenile offenders and controls. With respect to the psychological risk profile, we found that the offender group versus the control group had a higher exposure to traumatic experiences (Moffitt, 2018; Moffitt et al., 2002), showed affective psychopathic traits (McGee & Moffitt, 2019; Moffitt, 1993), and were more likely to engage in antisocial and delinquent behavior, in line with the characteristics proposed by Moffitt (1990) for life-course-persistent criminal behavior. They also reported symptoms of various psychopathological disorders frequently found in individuals with early traumatic experiences (see review by Jaffee, 2017; Teicher & Samson et al., 2013), and poor working memory, which has been proposed as connecting offending behavior and brain functioning (Borrani et al., 2019; Gil-Fenoy et al., 2018; Morgan & Lilienfeld, 2000; Ogilvie et al., 2011). For our first aim, we found significant group differences in two structural features of the neocortex: cortical thickness and surface area. Cortical thickness increased in the offender group compared to the control group in one cluster comprising the right middle temporal gyrus. This is a typical social cognition area, along with the temporoparietal junction and right medial prefrontal cortex, related to the ability to interpret the mental states of others, and that undergoes late development (Blakemore & Robbins, 2012; Crone & Dahl, 2012). The relevance of social cognition areas is in line with the behavioral evidence that adolescents’ risky decisions appear to be highly sensitive to the presence of socio-emotional cues (e.g., peers), as demonstrated by their increased risk-taking behavior in social contexts as compared to adults (Gardner & Steinberg, 2005; Steinberg, 2008). We also found smaller surface area in the lateral orbitofrontal cortex in offenders versus control participants; this is an executive control area involved in goal-directed decision-making processes and top-down emotion regulation of limbic areas (i.e., amygdala, hippocampus), especially under threatening or risky situations (Buchheim et al., 2013), that also suffers late development (Blakemore & Robbins, 2012; Crone & Dahl, 2012). The fact that two different temporal and frontal regions are involved, rather than being restricted to the frontal cortex, suggests that brain structure features in juvenile offenders may be more widespread than originally thought (Fairchild et al., 2016). With respect to the direction of the effects, cortical thinning in the superior temporal gyrus has usually been found in adolescents, youths, and adults with conduct problems and antisocial behavior (Fairchild & Smaragdi, 2018). However, in support of our finding of a thicker cortex in the superior temporal gyrus, similar measures of the middle temporal gyrus and inferior temporal gyrus have also been found in male adolescents showing increases in the psychopathic tendency from ages 9 to 18 (Yang et al., 2015). The disparity in the target categories under study (conduct problems, antisocial behavior, psychopathic traits) reinforces the relevance of performing a wide assessment of psychological risk variables to help interpret the directionality of the result. There is greater consensus in the evidence supporting a smaller lateral orbitofrontal area in our offenders compared to controls, as this has also been found in adolescents, youths, and adults with conduct problems and antisocial trajectories (Carlisi et al., 2020; Fairchild & Smaragdi, 2018), revealing deficits in the executive mechanisms of control associated with the commission of antisocial behavior. For our second aim, the results indicated that both cortical measures and most of the psychological risk measures were very good at classifying the participants into the offender and control groups, being the two cortical features, the experience of childhood trauma and engaging in antisocial behavior, the ones that contributed highly and equally well to the discriminant function and the group assignment. Specifically, greater cortical thickness in the right temporal cluster, exposure to childhood trauma, the psychopathological symptoms of interpersonal sensitivity, psychoticism, depression, phobic anxiety, and obsessive-compulsive behavior, as well as antisocial and delinquent behavior, contributed to the offender group. Evidence has largely shown that experiencing child maltreatment is associated with vulnerability to psychiatric disorders over the course of the lifetime (see reviews by Jaffee, 2017; Teicher & Samson et al., 2013). Exposure to early life adversity that challenges adolescent and adult functioning is also associated with life-course-persistent antisocial and criminal behavior (Moffitt, 2018; Moffitt et al., 2002). Among the psychopathic traits, only callousness, the most severe form of affective psychopathy, contributed to the offender group profile. Juveniles scoring high in psychopathy have empathic arousal deficits towards others’ suffering, while their capacity to understand intentionality in social interactions is not impaired, with this dissociation leading to callous disregard for the rights and feelings of others (Cheng et al., 2012). The presence of a callous trait designates an important subgroup that is at particularly high risk of showing severe and persistent antisocial behavior (Blair, 2013; Frick et al., 2014). In turn, the lateral orbitofrontal area, working memory, and psychopathic traits, such as grandiosity, unemotionality, and thrill seeking, contributed to distinctively define the control group profile. Evidence has shown that the lateral orbitofrontal area, subserving goal-directed decision-making processes and top-down emotion regulation, is associated with good working memory performance that warrants flexible behavior whenever previous experiences and different potential outcomes need to be integrated in the context of the currently available information, supporting efficient reasoning, problem-solving, and planning (Diamond, 2013; Niendam et al., 2012). Affective psychopathic traits of uncaring and unemotionality, as well as the behavioral trait of thrill or sensation seeking, have been related in middle school males with no history of criminal offence to low physiological arousal using a resting heart rate measure (Kavish et al., 2017). Although low heart rate has been considered as an unequivocal risk factor for both the perpetration of and exposure to violence (Raine, 2015), it is also likely that juveniles may experience this low level of arousal as a lack of emotion or caring. They also would require greater stimulation to increase their heart rates to a high level of arousal, which could explain thrill-seeking behavior. In fact, a relative lack of consideration for others’ needs and feelings, as well as a high degree of sensation seeking, have been considered two main features of normative adolescence that drive them to risky behavior (Steinberg, 2008). Consistently with that, these psychopathic features contributed to defining the psychological profile in the control group in the present study, confirming that many of the risk factors associated with juvenile delinquents (e.g., impulsivity, thrill seeking, irresponsibility) may be due more to the fact that they are adolescents than to the fact that they are offenders (Vaughn et al., 2022). The main limitation of this study, the small sample size, prevents us from drawing definite conclusions about brain differences in cortical features, even though the clusters were identified in regions that fit our hypotheses. This limitation stems from the difficulties involved in accessing offender samples, having them come voluntarily to the MRI laboratory located in a hospital, and getting them to follow a complex procedure, even when they are paid for their participation. We acknowledge that additional research with larger samples is needed to replicate our findings. Furthermore, the results are based on cross-sectional neuroimaging data and thus require extension by longitudinal designs involving repeated assessments of brain structure to claim causal relationships. Despite these limitations, this study also has several strengths to highlight, such as the detailed characterization of the sample, the use of multiple surface-based metrics in addition to a global volumetric measure, the use of whole-brain analyses, strict threshold criteria, and controlling for multiple comparisons to reduce the probability of type I errors. The fact that the sample was restricted to males also means that the present findings are arguably easier to interpret than those obtained with mixed-sex samples. The study also benefits from the assessment of homogeneously aged groups, which limits confounds associated with age-related variations in brain structure typically found in developmental studies. Summing up, this study provides preliminary evidence of distinctive cortical features in the temporal and frontal cortices and of psychological risk variables, such as childhood trauma, psychopathic traits, psychopathological symptoms, and antisocial and delinquent behavior, that characterize the profile of juvenile offenders compared to controls, both transitioning from late adolescence to early adulthood. The selected group of factors with high discriminative power provides new insights into the neural and psychological profile of youths who engage in violent antisocial behaviors. In this sense, our findings may help contribute to the crucial hypothesis that immature or defective brain developments may be linked to the commission of violent acts. We can tentatively suggest that the increased right middle cluster could be indicative of defective brain development in social cognition processes, since this distinctive feature appeared in combination with the higher risk profile of childhood trauma, psychopathological symptoms, psychopathic callousness, and antisocial and delinquent behavior. In turn, the smaller lateral orbitofrontal area could be more indicative of immature brain development in cognitive and emotional control processes, since it appeared in combination with the lower risk profile of grandiosity, unemotionality, and thrill-seeking traits that characterize participants in the control group. These preliminary results may have practical implications because the combined use of brain imaging and psychological measures has the potential to improve assessment and intervention practices within the health care and juvenile justice systems. First, the importance of childhood trauma in our sample reinforces the need for prevention programs focusing on early intervention to reduce child exposure and the negative impact of toxic social environments. These might include video training interventions exposing mothers to their interactions with the child to improve their sensitivity and responsiveness to the child’s emotional expressions of their needs that result in healthier infant attachment (Mountain et al., 2017). From a broader view, early relational health is a multidimensional concept that emphasizes the importance of the earliest relational experiences and caregiver-child interactions in building lifelong health, early learning, social-emotional capacities, self-regulation, and resilience (Metzler & Willis, 2020). Therefore, careful screening for early traumatic experiences in juvenile offenders is a good practice to identify and better understand the possible deficits that are present in their psychological profile. Second, the potential comorbidity of various psychopathological symptoms observed in juvenile offenders may suggest the need to adopt a transdiagnostic perspective that seeks to identify the core psychological and neurobiological processes underlying multiple forms of psychopathology, eventually leading to more effective assessment and integrated treatment protocols (Lahey et al., 2016). Exposure to trauma in childhood is a powerful trigger associated with increased risk of many types of psychopathologies, including internalizing (major depression, dysthymia, generalized anxiety disorder, posttraumatic stress disorder, panic disorder, and phobia) and externalizing (conduct disorder, oppositional defiant disorder, alcohol and drug dependence, antisocial personality disorder) factors (McLaughlin et al., 2020). Important transdiagnostic mechanisms linking early trauma exposure and psychopathologies include social information processing and emotional processing. These areas are presumably affected in juvenile offenders, given the alterations in temporal and frontal areas reported in this study. For instance, young adults reporting a history of moderate to severe childhood abuse exhibit preferential attention to angry over happy faces and increased sensitivity in the detection of angry expressions at lower levels of emotional intensity, accompanied by hostile attribution towards the intention of others that leads them to aggressive responding (McLaughlin et al., 2020). In turn, emotion regulation difficulties, rumination, low emotional awareness, difficulty discriminating between cues that predict threat versus safety, and reduced social skills, associated with impaired executive control are all predictors of psychopathology (Snyder et al., 2015). Therefore, it is important to emphasize interventions targeted at improving emotion regulation strategies to treat chronic stress-related pathologies coupled with maladaptive emotional, cognitive, and behavioral responses (Renna et al., 2020). Similarly, interventions that improve social information processing, such as those that focus on training interpersonal problem-solving skills, have been shown to be the most effective for offender rehabilitation (Mathys, 2017). These programs focus on skills such as causal, consequential, and means-end thinking, as well as critical reasoning, value training, perspective taking, and empathy (Polaschek et al., 2019). The ability to adequately resolve interpersonal problems is also a protective factor against antisocial and other maladaptive behaviors (Lösel & Bender, 2003), which becomes essential when adolescents make decisions in risky situations involving their peers. In summary, this transdiagnostic approach may be useful in informing the development of integrative interventions that address the brain alterations and psychological deficits seen in this population, rather than treating risk factors one at a time. Conflict of Interest The authors of this article declare no conflict of interest. Cite this article as: Padrón, I., Góngora, D., Moreno, I., Rodrigo, M. J., & Martín, A. M. (2022). Contribution of brain cortical features to the psychological risk profile of juvenile offenders. The European Journal of Psychology Applied to Legal Context, 14(2), 93-103. https://doi.org/10.5093/ejpalc2022a9 References |
Cite this article as: Padrón, I., Góngora, D., Moreno, I., Rodrigo, M. J., & Martín, A. M. (2022). Contribution of Brain Cortical Features to the Psychological Risk Profile of Juvenile Offenders. The European Journal of Psychology Applied to Legal Context, 14(2), 93 - 103. https://doi.org/10.5093/ejpalc2022a9
ammartin@ull.edu.es Correspondence: ammartin@ull.edu.es (A. M. Mart├şn).Copyright © 2026. Colegio Oficial de la Psicología de Madrid





 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
The European Journal of Psychology Applied to Legal Context is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License








