


Humanization, Adaptation to Change, and Mental Health in Teachers in Three European Countries
[Humanizaci├│n, adaptaci├│n al cambio y salud mental en docentes de tres pa├şses europeos]
María M. Molero1, África Martos1, María C. Pérez-Fuentes1, Begoña M. Tortosa1, Maria Sisto1, María M. Simón1, and José J. Gázquez2
1University of Almer├şa, Spain; 2Universidad Aut├│noma de Chile, Providencia, Chile
https://doi.org/10.5093/ejpalc2024a2
Received 1 September 2023, Accepted 21 November 2023
Abstract
Background: The aim of this study was to explore the relationships between humanization, adaptability to change, and mental health in European teachers (Spanish, Portuguese, and Italian teachers), as well as the relationship between humanization and mental health in teachers through the analysis of the mediating role of adaptability to change. Method: A cross-sectional descriptive study was conducted with teachers from three European countries (Spain, n = 263; Portugal, n = 344; and Italy, n = 287). The Healthcare Professional Humanization Scale (HUMAS), General Health Questionnaire (GHQ-28), and the Adaptation to Change Questionnaire (ADAPTA-10) were administered. Results: In all three countries, negative associations were observed between humanization and the presence of problematic symptoms. With respect to the adaptability to change factors, humanization showed negative associations with the emotional factor and positive associations with the cognitive-behavioral factor. Comparative mean analysis revealed differences in humanization, the emotional factor of adaptability to change, and the presence of problematic symptoms. Finally, the mediation models showed the absence of a direct effect in the relationship between humanization and the presence of GHQ-28 symptomatology when it was mediated by the emotional factor (Spanish and Portuguese sample). In the Italian sample, the direct effect of humanization-GHQ-28 symptomatology was significant, with a smaller proportion of the indirect effect of the emotional factor acting as a mediator. On the other hand, when considering the cognitive-behavioral factor as a mediator, the same result was obtained for all three countries: a negative direct effect between humanization and GHQ-28 symptomatology, with no mediation by the cognitive-behavioral factor. Conclusions: The need to improve training in humanization competencies lies in the potential protective function that these competencies can have on the mental health of teachers.
Resumen
Antecedentes: El objetivo del trabajo fue explorar la relación entre humanización, capacidad de adaptación al cambio y salud mental en docentes europeos (españoles, portugueses e italianos) y la relación entre humanización y salud mental en docentes mediante el análisis del rol mediador de la capacidad de adaptación al cambio. Método: Se realizó un estudio descriptivo transversal con docentes de tres países europeos (España, n = 263, Portugal, n = 344 e Italia, n = 287). Se administró la Healthcare Professional Humanization Scale (HUMAS), el General Health Questionnaire (GHQ-28) y el Cuestionario de Adaptación al Cambio (ADAPTA-10). Resultados: En los tres países se obervó una asociación negativa entre humanización y la presencia de sintomatología problemática. Con los factores de adaptación al cambio la humanización presentó una asociación negativa con el factor emocional y positiva con el cognitivo-conductual. Del análisis comparativo de medias se obtuvieron diferencias en humanización, el factor emocional de adaptación al cambio y la presencia de sintomatología problemática. Finalmente, los modelos de mediación mostraron la ausencia de un efecto directo en la relación entre humanización y la presencia de sintomatología GHQ-28 cuando esta se encontraba mediada por el factor emocional (muestra española y portuguesa). En la muestra italiana fue significativo el efecto directo de la humanización-sintomatología GHQ-28, con menor proporción del efecto indirecto del factor emocional actuando este como mediador. Por otro lado, tomando como mediador el factor cognitivo-conductual, se obtuvo el mismo resultado para los tres países: un efecto directo negativo entre la humanización y la sintomatología GHQ-28, no estando este mediado por el factor cognitivo-conductual. Conclusiones: La necesidad de mejorar la formación en competencias de humanización reside en la potencial función protectora que pueden ejercer sobre la salud mental de los docentes.
Keywords
Humanization, Adaptation to change, Mental Health, Teachers, EuropePalabras clave
Humanizaci├│n, Adaptaci├│n al cambio, Salud mental, Docentes, EuropeCite this article as: Molero, M. M., Martos, Á., Pérez-Fuentes, M. C., Tortosa, B. M., Sisto, M., Simón, M. M., & Gázquez, J. J. (2024). Humanization, Adaptation to Change, and Mental Health in Teachers in Three European Countries. The European Journal of Psychology Applied to Legal Context, 16(1), 17 - 25. https://doi.org/10.5093/ejpalc2024a2
Correspondence: amm521@ual.es (Á. Martos).
Teachers may possess certain psychological characteristics that contribute to the enhancement of the quality of their job performance. In teachers, professionals whose interaction with students is direct and continuous, specific personal resources (such as adaptability to change, emotional intelligence, social skills, empathy, and self-efficacy) have been observed to enable them to better cope with the psychophysical stress and exhaustion generated in the teaching-learning process (Carter et al., 2016; Izquierdo et al., 2022; Klassen & Chiu, 2011; Molero et al., 2019). Presently, the educational field is reemphasizing the importance of student-centered attention to improve education quality (Hall & Saunders, 1997). Building upon this theoretical framework, we understand that for educational practices to be humanized, teachers must possess specific personal resources. In fact, teachers advocating for humanized practices are those who exhibit certain psychological characteristics that contribute to enhancing their performance quality and continually work to create learning environments that better combat stress and psychophysical exhaustion while addressing the needs of every student (Carter et al., 2016; Molero et al., 2019; Molero et al., 2023). However, the high demands of the educational context and the changes brought about by Covid-19 have caused teachers difficulties in adapting to new changes, whether in terms of behavioral, cognitive, or emotional functioning, hindering humanized educational practices (Bjorklund, 2015; Lacolino et al., 2023). Within adaptation, uncertainty and teachers’ ability to tolerate it arise. This stressor is capable of producing mental health disturbances such as anxiety and depression (Molero et al., 2022; Soriano et al., 2019), which in turn dehumanize education (Salazar, 2013). Currently, humanization is very much present in the educational context and has been accepted among teachers, countering dehumanization in education (Freire, 1970; Salazar, 2013). The construct of humanization is defined as a set of personal, social, and emotional competencies that facilitate professional work and enable an active role in professional performance, respecting, attending to, and caring for the human being (Freire, 1970; Pérez-Fuentes, Herrera-Peco, et al., 2019). Among the personal competencies that define humanization are self-efficacy, understood as the ability of the education professional to deal with difficult and stressful situations (Guo et al., 2011; Yoo, 2016). It also involves the ability to manage and express one’s emotions, implying confronting situations that require tailored action in relation to the context and the individual, thereby improving the quality of professional attention (Pérez-Fuentes, Herrera-Peco, et al., 2019). Expectations related to self-efficacy depend on job achievements, experiences, and emotional states (Bandura, 1997; Williams, 1995). This ability is closely related to teachers’ mental health, emotional intelligence, and self-esteem because these are associated with an individual’s capacity to relate and communicate with those in their environment (Von Münchhausen et al., 2021). Additionally, it is common for teachers to possess social skills due to their ability to relate to others assertively and empathetically (Bar-on, 2006; Gardner, 1983; Goleman, 1996), increasing their capacity to adapt to changes and job performance (Lown et al., 2016; Srivastava & Das, 2016). Emotional understanding, is defined as an individual’s ability to process emotional information in their work environment (Miao et al., 2017). Humanization in the education professional requires an optimistic disposition, implying motivation, and generating positive future expectations that aid in coping with difficult and stressful situations that can impact professionals’ mental health (Dymecka, et al., 2023; Segerstrom et al., 2017). Thus, optimism maintains a close relationship with increased physical and psychological health and motivation (Carver & Scheier, 2014; Seligman et al., 2007). Humanization is focused on improving physical, emotional, and mental attention directed toward students, teachers, and families, as these are indispensable agents in the context of educational humanization (Carter et al., 2016; Freire, 1970; Pérez-Fuentes, Herrera-Peco, et al., 2019). From this perspective, humanization aids in the integral development of the human being, with the student becoming the center and assuming an active role, alongside the teachers (Hall & Saunders, 1997; Pérez-Fuentes, Molero, et al., 2019; Zhang et al., 2021). The goal of humanization in the educational context is to ensure exquisite attention to students, thus meeting their needs, and ensuring job commitment to improve the quality of education (Carter et al., 2016; Klassen and Chiu, 2011; Zhang et al., 2021), considering that the primary objective of teachers should be to enhance the teaching-learning process (Schneider et al., 2014), involving education-involved agents such as students and families in the process (Núñez et al., 2019; Vanderburg et al., 2022). Furthermore, it is essential that students and their families are convinced that they are receiving adequate attention (Núñez et al., 2019), and it has been demonstrated that teachers’ mental health is one of the main aspects to consider in order to cope with the psychological demands required by changes in their teaching and to deal with the stress generated in the teaching-learning process (Paris & Alim, 2017). In fact, in a sample of teachers, high levels of stress and anxiety have been negatively related to humanized educational practices (Harmsen et al., 2018). In other studies, the ability to adapt to change has been positively related to teachers’ mental health (Sharplin et al., 2011). It can be deduced from this that humanized and student-centered educational practices require good mental health among education professionals, especially in situations of high psychosocial stress (such as significant changes or high job demands), where mental health levels are altered and affect the quality of teaching (Rajendran et al., 2020). The literature shows that unfavorable mental health among teachers can lead to adverse situations for both students and teachers themselves. In other words, unfavorable mental health among teachers could lead to stress, anxiety, job dissatisfaction, emotional exhaustion, and even depression (Akbaba, 2014; Rajendran et al., 2020). However, good mental health among teachers could lead to higher levels of job commitment and motivation. Training to care for mental health is an effective way to reduce exhaustion and improve job satisfaction and commitment (Klassen & Chiu, 2011; Paris & Alim, 2017). To facilitate teachers’ mental well-being enhancement in a qualitative and significant manner, it is essential to commence with the contributions of positive psychology, which centers its focus on the development of personal resources that counteract stress and exhaustion (Bakker et al., 2012). Some authors propose that specific personal resources, such as adaptability to change, which is in turn linked to humanization and mental health (Aslam, 2016), enhance occupational commitment. Teachers who possess adaptation strategies to address changes and the pressures of teaching are more adept at mitigating exhaustion, stress, and anxiety (Bowles & Arnup, 2016; Johnson et al., 2014; Kearney, 2016; Mansfield et al., 2014; Mansfield et al., 2014; Naidoo & Wagner, 2020). Concerning mental health, a limited capacity to adapt to changes among teachers has been associated with increased levels of anxiety and stress due to the challenge these professionals encounter in distancing themselves and managing the emotions and tensions stemming from their job performance. Conversely, a high capacity to adapt to changes has been correlated with enhanced mental well-being (Hogan & White, 2021). After scrutinizing the empirical results of the most pertinent studies related to the subject of this investigation, the main objectives were: (1) to explore the relationships between humanization, adaptability to change, and mental health among teachers from three European countries: Spain, Portugal, and Italy; (2) to scrutinize the association between humanization and mental health in teachers by analyzing the mediating role of adaptability to change. In light of these objectives and drawing upon prior empirical evidence, the following research hypotheses were formulated: (I) humanization exhibits a positive association with the cognitive-behavioral factor and a negative association with the emotional factor of adaptability to change; (II) humanization is negatively related to the presence of problematic symptomatology for mental health (somatic symptoms, anxiety and insomnia, social dysfunction, and depression); (III) the presence of somatic symptoms, anxiety and insomnia, social dysfunction, and depression is positively related to the emotional factor and negatively related to the cognitive-behavioral factor of adaptability to change; (IV) the impact of humanization on the presence of negative symptomatology is mediated by the emotional and cognitive-behavioral factors of adaptability to change; and (V) the relationships between humanization, adaptability to change, and mental health are analogous across the three countries. Table 1 Sociodemographic Characteristics of the Study Samples 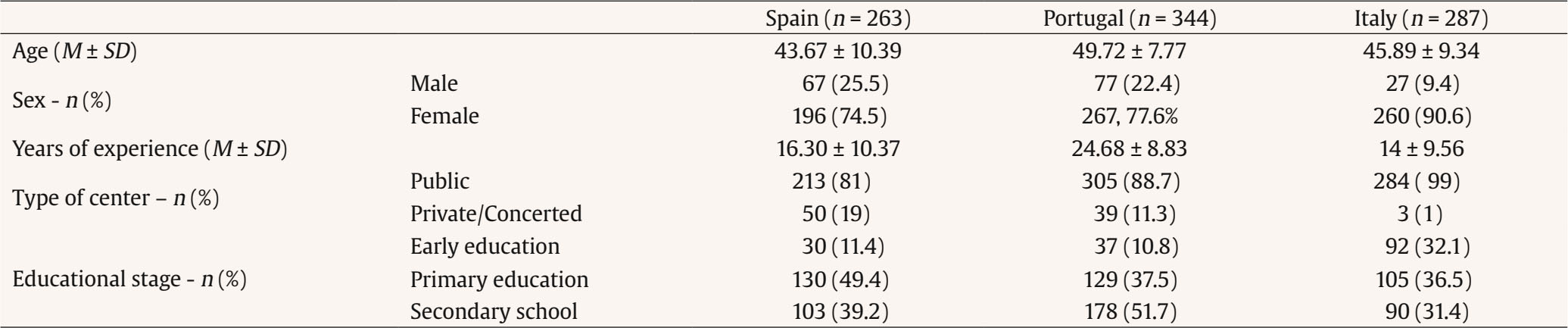 Participants This quantitative study employed a cross-sectional descriptive design and followed the STROBE guidelines for cross-sectional studies (Vandenbroucke et al., 2007). The sample consisted of a total of 894 teachers from three European countries (Spain, n = 263; Portugal, n = 344; Italy, n = 287), with a majority of female participants (Spain, 74.5%; Portugal, 77.6%; Italy, 90.6%). All descriptive data of the sample are presented in Table 1. Instruments Healthcare Professional Humanization Scale (HUMAS; Pérez-Fuentes, Herrera-Peco, et al., 2019) This scale analyzes a professional’s humanization competencies focused on improving care. It consists of 19 items which measure professional competencies or attitudes: dispositional optimism, sociability, emotional understanding, self-efficacy, and affection. McDonald’s (1999) omega was calculated to estimate the reliability of each of the subscales: dispositional optimism (Spain, ω = .67; Portugal, ω = .83; Italy, ω = .78), sociability (Spain, ω = .79; Portugal, ω = .78; Italy, ω = .88), emotional understanding (Spain, ω = .77; Portugal, ω = .77; Italy, ω = .87), self-efficacy (Spain, ω = .71; Portugal, ω = .73; Italy, ω = .89), and affection (Spain, ω = .71; Portugal, ω = .75; Italy, ω = .76). The omega for the complete scale was .79 for Spanish sample, .86 for the Portuguese sample, and .88 for the Italian sample. General Health Questionnaire (GHQ-28; Goldberg & Hillier, 1979) The Spanish version of the questionnaire (Lobo et al., 1986) was applied. It evaluates four dimensions of mental health: somatic symptoms, anxiety and insomnia, social dysfunction, and depression. The GHQ-28 is composed of 28 items, with four answer choices. The Likert-type scale correction method was used, attributing a value of 0 to 3 to each answer choice. For each of the subscales, the reliability values are as follows: somatic symptoms (Spain, ω = .88; Portugal, ω = .92; Italy, ω = .86), anxiety and insomnia (Spain, ω = .89; Portugal, ω = .92; Italy, ω = .90), social dysfunction (Spain, ω = 0.74; Portugal, ω = .85; Italy, ω = .81), and depression (Spain, ω = .85; Portugal, ω = .94; Italy, ω = .88). Change Adaptation Questionnaire (ADAPTA-10; Pérez-Fuentes et al., 2020) The ADAPTA-10 consists of 10 items with response options on a five-point Likert scale. It provides information about the capacity for change adaptation, specifically in two factors: an emotional factor related to anxiety and discomfort that may arise in response to change and a cognitive-behavioral factor related to the ability to control, manage, and act in different situations. McDonald’s (1999) omega was calculated to estimate the reliability of subscales: emotional factor (Spain, ω = .79; Portugal, ω = .86; Italy, ω = .84) and cognitive-behavioral factor (Spain, ω = .76; Portugal, ω = .71; Italy, ω = .86). Procedure A meticulous process of translation and adaptation of the questionnaires used in the countries was followed to ensure their cultural appropriateness and linguistic understanding by Portuguese and Italian participants, following the guidelines outlined by Muñiz et al. (2013). This translation and adaptation process ensured that the instruments were suitable for use in different countries, allowing for precise and meaningful data collection within the cultural and linguistic context. In addition, informed consent was obtained from all participants before their participation in the study. The research was approved by the Committee of Bioethics of the University of Almería with reference UALBIO2020/046. Data Analysis Firstly, as preliminary analyses, descriptive statistics and a correlation matrix were presented for each sample in the study (Spain, Portugal, and Italy). Cronbach’s alpha coefficients were calculated to assess the reliability of the measurement scales used in the study. An acceptable internal consistency was determined with values above .70 indicating reliable and consistent measurement of the constructs under investigation (Cronbach, 1951). Additionally, McDonald’s (1999) omega coefficient was calculated for each scale and study sample, following the recommendations of Ventura-León and Caycho-Rodríguez (2017). Then, a multivariate analysis (MANOVA) was conducted to test if there were significant differences between the three countries, considering the set of dependent variables (humanization, emotional and cognitive-behavioral factors of change adaptation, and the four dimensions of GHQ-28). The partial eta-squared coefficient (ηp2) was used as a measure of effect size, following the criteria established in Cohen’s (1988) classic work, where an effect is considered small when ηp2 = .01, medium when ηp2 = .06, and large when ηp2 = .14. Finally, to examine the role of each of the change adaptation factors in the relationship between humanization and mental health, latent mediation models were computed for each country using maximum likelihood (ML) estimation, specifying two pathways of association for humanization in the presence of negative symptoms: a direct effect and an indirect effect through the emotional and cognitive-behavioral factors of change adaptation. The lavaan package (Rosseel, 2012), integrated in JASP v.0.16.3 (JASP Team, 2022), was used for this purpose. Model fit was evaluated using the following indices: the chi-square/degrees of freedom ratio (χ2/df), which is considered optimal with values < 3 (Iacobucci, 2010; Kline, 2005) and acceptable < 5 (Bentler, 1989); the CFI, TLI, and GFI indices, which should provide values > .95 for optimal fit and > .90 for acceptable fit, according to Hu and Bentler (1999); and RMSEA, which considers values < .06 as optimal and < .08 or very close as acceptable. Humanization, Change Adaptation, and Mental Health: Descriptive Statistics and Correlations As shown in Table 2, humanization in the samples of teachers is negatively associated with the presence of somatic symptoms, anxiety and insomnia, social dysfunction, and depression. Regarding the factors of change adaptation, humanization maintains negative correlations with the emotional factor and positive correlations with the cognitive-behavioral factor. This pattern of associations is consistent across all three study samples. Table 2 Correlations, Descriptive Statistics, and Alphas for the Samples of Spain, Portugal, and Italy 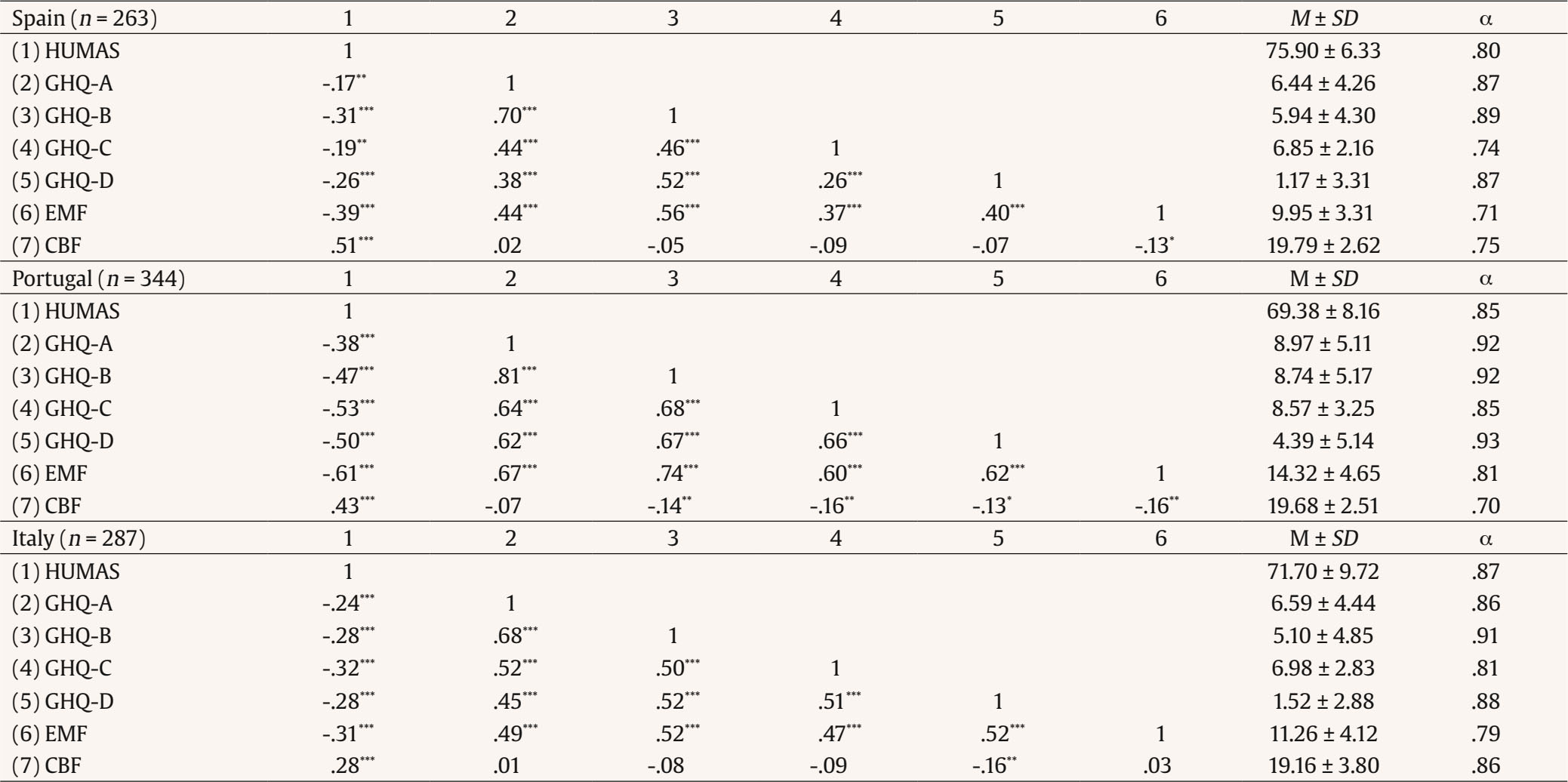 Note. HUMAS = humanization; GHQ-A = somatic symptoms; GHQ-B = anxiety and insomnia; GHQ-C = social dysfunction; GHQ-D = depression; EMF = emotional factor of adaptation to change; CBF = cognitive-behavioral factor of adaptation to change; M = media; SD = standard deviation; α = Cronbach’s alpha. *p < .05, **p < .01, ***p < .001. In contrast, the associations between the emotional factor of change adaptation and the presence of problematic symptoms are positive in all cases, maintaining this trend in all three analyzed samples. However, in the cognitive-behavioral factor, some variations in associations among the three countries were observed:
Subsequently, a MANOVA was conducted to assess the differences between the countries under study, considering the set of dependent variables. The Box’s M-test for homogeneity of covariance matrices (p < .05) rejects the null hypothesis that assumes the equality at the population level of the covariance matrices generated for each group of the independent variable. This is why the Pillai’s trace statistic was used for the multivariate contrast, which is more robust in case of violating the assumption. In this case, the multivariate contrast showed that there are differences between the means of the three countries considering this linear combination of the set of dependent variables (Pillai’s trace = .272, F = 19.93, p < .001; ηp2 = .14). The Levene test (p < .05) indicated that the groups were not homogeneous (rejecting the null hypothesis about equal variances), so univariate analyses (ANOVA) were conducted using the Games-Howell statistic for post hoc tests. In humanization, significant differences were found between the countries (F = 47.25, p < .001, η p2 = .09). Post hoc tests revealed that the Spanish sample (M = 75.90) had a significantly higher score (p < .001) compared to the Italian (M = 71.69) and Portuguese samples (M = 69.37). Figure 1 Humanization and Mental Health in Spanish Sample (Model S1: Emotional Factor as Mediator, and Model S2: Cognitive-Behavior Factor as Mediator) 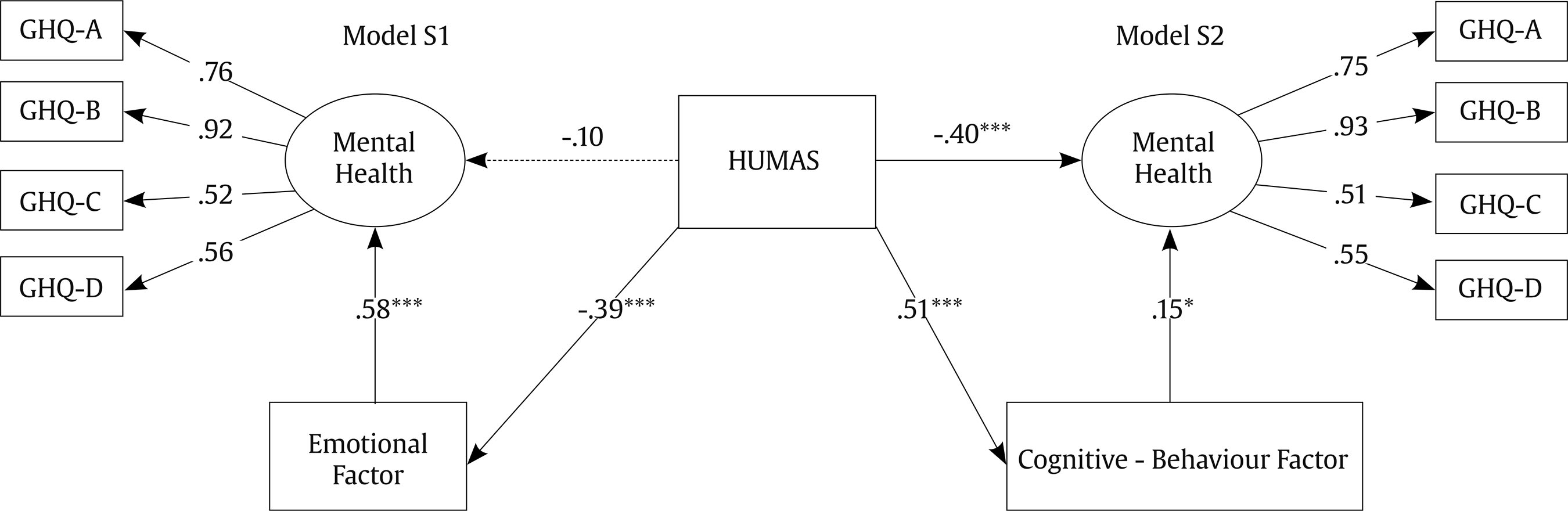 Note. HUMAS = humanization; GHQ-A = somatic symptoms; GHQ-B = anxiety and insomnia; GHQ-C = social dysfunction; GHQ-D = depression. *p < .05, **p < .01. All standarized estimates. Regarding the change adaptation factors, differences were also detected between the countries, specifically for the emotional factor (F = 91.18, p < .001, ηp2 = .17). In the case of the cognitive-behavioral factor (F = 3.61, p < .05, ηp2 = .01), the differences, although statistically significant, had a small effect size. Post hoc tests showed that both the Portuguese sample (M = 14.32) and the Italian sample (M = 11.26) obtained significantly higher means than the Spanish sample (M = 9.95) in the emotional factor of change adaptation. Finally, significant differences between the countries were also found for each of the GHQ-28 dimensions: somatic symptoms (F = 29.19, p < .001, ηp2 = .06), anxiety and insomnia (F = 49.59, p < .001, ηp2 = 0.10), social dysfunction (F = 36.13, p < .001, ηp2 = .07), and depression (F = 67.96, p < .001, ηp2 = .13). Post hoc tests showed that the Portuguese sample significantly differed from the mean scores obtained by the other two countries, with Portugal having higher mean scores in terms of somatic symptoms (M = 8.97), anxiety and insomnia (M = 8.73), social dysfunction (M = 8.57), and depression (M = 4.39). Humanization in the Promotion of Mental Health in Teachers: The Mediating Role of Change adaptation Spanish Sample The S1 and S2 models (Figure 1), which correspond to the Spanish sample of teachers, both showed good fit in both cases (Table 3). Table 3 Regression Coefficients and Models Fit Indices (Spanish Sample) 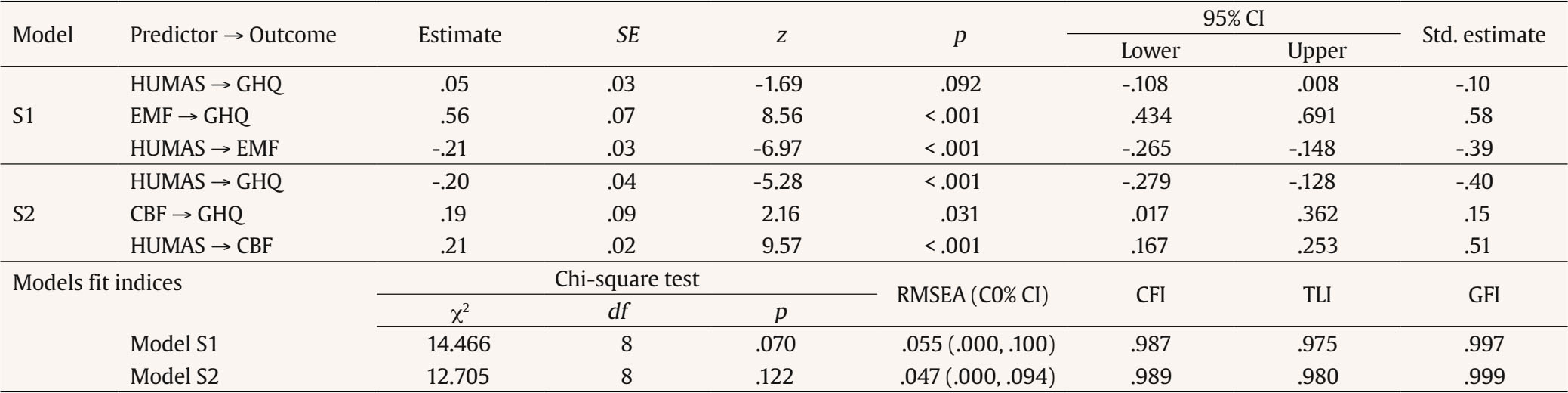 Note. SE = standard error; CI = confidence intervals; Std. estimate = standardized estimate; RMSEA = root mean square error of approximation; CFI = comparative fit index; TLI = Tucker-Lewis index; GFI = goodness of fit index; HUMAS = Humanization; GHQ = negative symptoms to mental health; EMF = emotional factor; CBF = cognitive-behavior factor. In Model S1, there was no significant direct effect of humanization on the presence of GHQ-28 symptomatology. However, considering the total effect of humanization on GHQ-28 symptomatology (estimate = -.17, SE = .03, z = -4.98, p < .001, 95% CI [-.232, -.101], std. estimate = -.33) and taking into account the magnitude of the indirect effect (estimate = -.12, SE = .02, z = -5.40, p < .001, 95% CI [-.158, -.074], std. estimate = -.23), we can conclude that the proportion (indirect/total = .70) of this effect mediated by the emotional factor falls between .429 and .968. In Model S2, humanization had a negative direct effect on the presence of GHQ-28 symptomatology. Furthermore, considering the total effect of the model (estimate = -.16, SE = .03, z = -4.94, p < .001, 95% CI [-.229, -.099], std. estimate = -.32), and taking into account the magnitude of the indirect effect (estimate = .04, SE = .02, z = 2.10, p < .05, 95% CI [.003, .077], std. estimate = .08), we can conclude that the proportion (indirect/total = -.24) of this effect mediated by the cognitive-behavioral factor was not statistically significant (-.488, .001). Portuguese Sample Models P1 and P2 (Figure 2), corresponding to the sample of Portuguese teachers, showed acceptable fit in both cases (Table 4). Figure 2 Humanization and Mental health in Portuguese Sample (Model P1: Emotional Factor as Mediator, and Model P2: Cognitive-Behavior Factor as mediator). 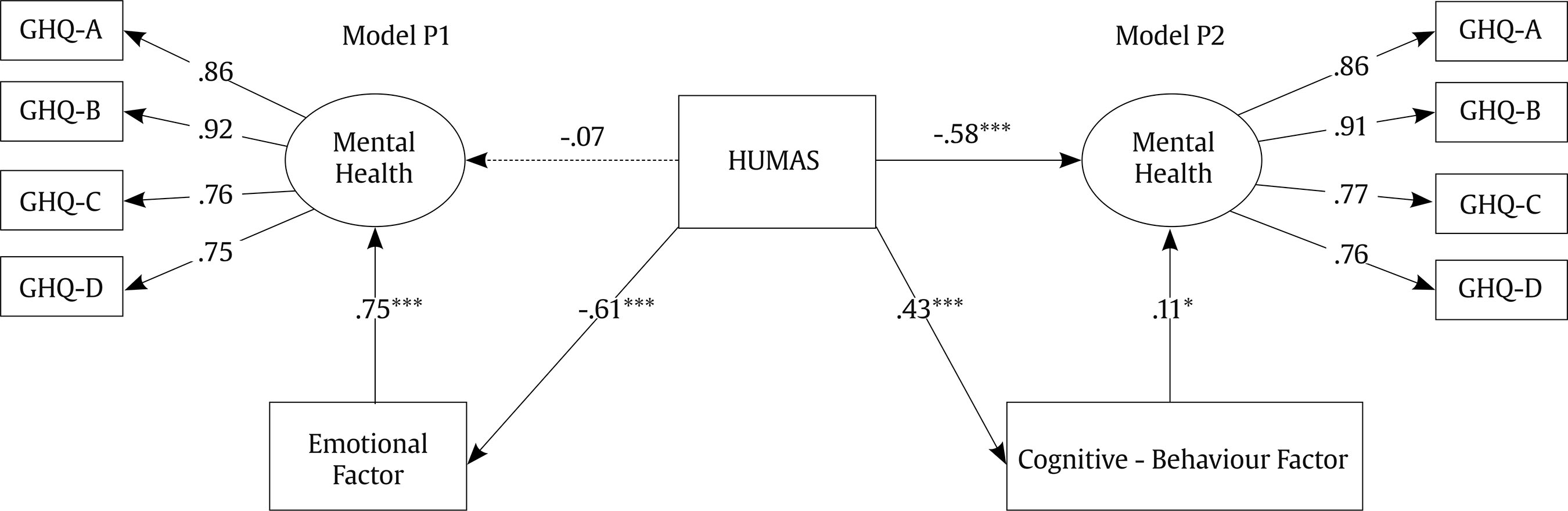 Note. HUMAS = humanization; GHQ-A = somatic symptoms; GHQ-B = anxiety and insomnia; GHQ-C = social dysfunction; GHQ-D = depression. *p < .05, **p < .01. All standarized estimates Table 4 Regression Coefficients and Models Fit Indices (Portuguese Sample)  Note. SE = standard error; CI = confidence intervals; Std. estimate = standardized estimate; RMSEA = root mean square error of approximation; CFI = comparative fit index; TLI = Tucker-Lewis index; GFI = goodness of fit index; HUMAS = Humanization; GHQ = negative symptoms to mental health; EMF = emotional factor; CBF = cognitive-behavior factor. In Model P1, no significant direct effect of humanization on the presence of GHQ-28 symptomatology was observed. However, considering the total effect of humanization on the presence of GHQ-28 symptomatology (estimate = -.29, SE = .03, z = -10.45, p < .001, 95% CI [-.341, -.234], std. estimate = -.53), and taking into account the magnitude of the indirect effect (estimate = -.25, SE = .02, z = -10.31, p < .001, 95% CI [-.297, -.202], std. estimate = -.46), we can conclude that the proportion (indirect/total = .87) of this effect mediated by the emotional factor falls between .712 and 1.023. In Model P2, humanization had a significant direct negative effect on the presence of GHQ-28 symptomatology. Furthermore, considering the total effect of the model (estimate = -.29, SE = .03, z = -10.52, p < .001, 95% CI [-.344, -.236], std. estimate = -.54), and examining the indirect effect, taking into account that in this case, a marginal indirect effect was obtained (estimate = .02, SE = .01, z = 1.93, p = .053, 95% CI [-.304, .050], std. estimate = .05), we can conclude that the proportion (indirect/total = -.08) of this effect mediated by the cognitive-behavioral factor did not turn out to be statistically significant (-.173, .003). Italian Sample The models I1 and I2 (Figure 3), corresponding to the sample of Italian teachers, showed acceptable fit in both cases (Table 5). Figure 3 Humanization and Mental Health in Italian Sample (Model I1: Emotional Factor as Mediator, and Model I2: Cognitive-Behavior Factor as Mediator). 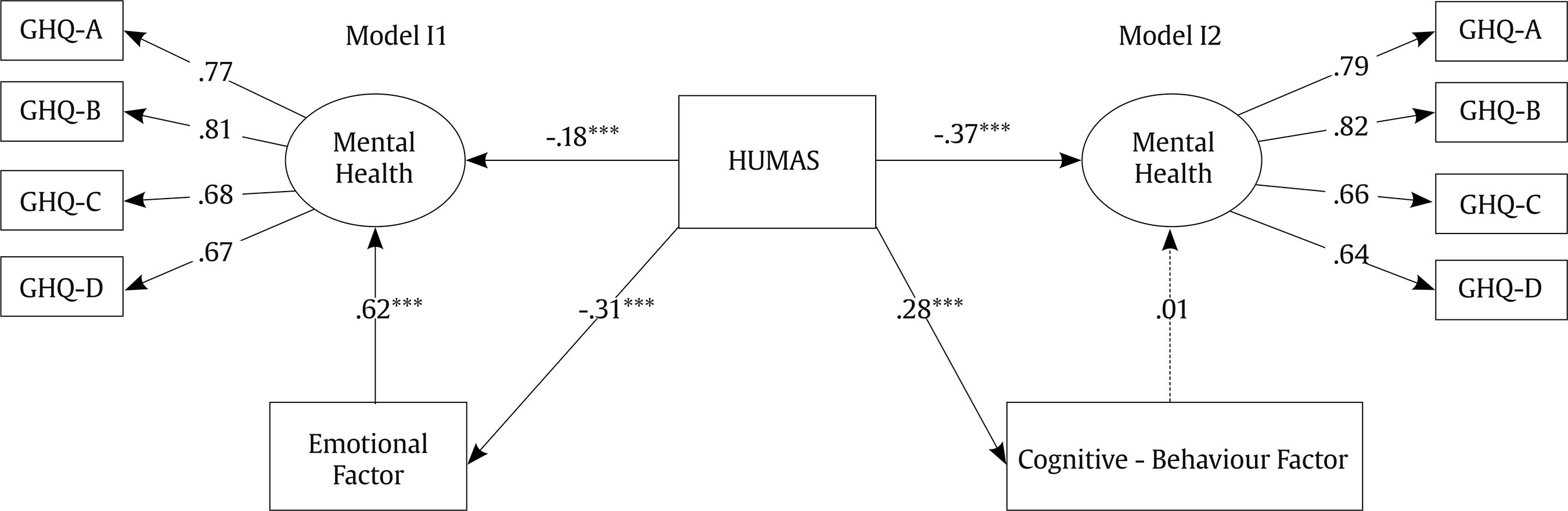 Note. HUMAS = humanization; GHQ-A = somatic symptoms; GHQ-B = anxiety and insomnia; GHQ-C = social dysfunction; GHQ-D = depression. ***p < .001. All standarized estimates. Table 5 Regression Coefficients and Models Fit Indices (Italian Sample) 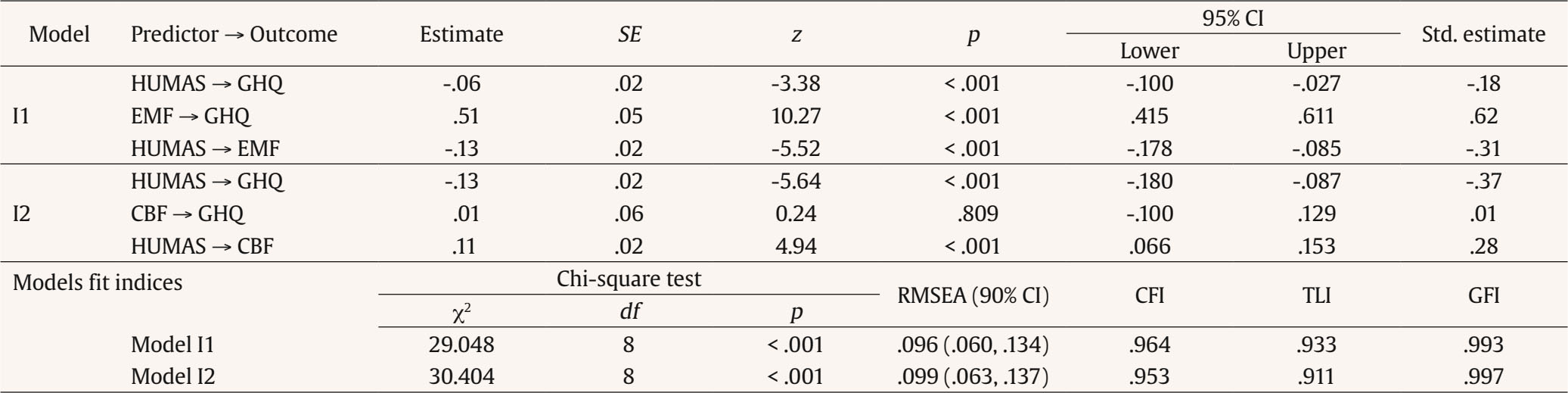 Note. SE = standard error; CI = confidence intervals; Std. estimate = standardized estimate; RMSEA = root mean square error of approximation; CFI = comparative fit index; TLI = Tucker-Lewis index; GFI = goodness of fit index; HUMAS = Humanization; GHQ = negative symptoms to mental health; EMF = emotional factor; CBF = cognitive-behavior factor. In model I1, a direct negative effect of humanization on the presence of GHQ-28 symptomatology was observed. Furthermore, considering the total effect of humanization on the presence of GHQ-28 symptomatology (estimate = -.13, SE = .02, z = -5.86, p < .001, 95% CI [-.175, -.087], std. estimate = -.37), and taking into account the magnitude of the indirect effect (estimate = -.07, SE = .01, z = -4.86, p < .001, 95% CI [-.095, -.040], std. estimate = -.19), we can conclude that the proportion (indirect/total = .51) of this effect mediated by the emotional factor lies between .331 and .699. On the other hand, in model I2, humanization had a direct negative effect on the presence of GHQ-28 symptomatology. Furthermore, the total effect of the model was considered (estimate = -.13, SE = 0.02, z = -5.79, p < .001, 95% CI [-.177, -.087], std. estimate = -.36), and the indirect effect was examined (estimate = .002, SE = .01, z = 0.24, p = .810, 95% CI [-.011, .014], std. estimate = .004). We can conclude that the proportion (indirect/total = -.01) of this effect mediated by the cognitive-behavioral factor was not statistically significant (-.107, .084). The present study provides valuable insights into the relationships between humanization, the ability to adapt to change, and mental health in teachers from three European countries. The results confirm the importance of humanization in the educational context. Humanization, defined as a set of personal, social, and emotional competencies that facilitate student-centered care (Freire, 1970; Pérez-Fuentes, Herrera-Peco, et al., 2019), showed positive associations with teachers’ mental health in all three countries. This supports the idea that humanization not only enhances the emotional well-being of teachers but could also contribute to better job performance and, ultimately, higher-quality education (Carter et al., 2016; Molero et al., 2019; Molero et al., 2023). The study also identified the capacity for adaptation to change as a relevant factor in the relationship between humanization and mental health (Sharplin et al., 2011). The capacity for adaptation to change was analyzed considering its two components: the emotional and the cognitive-behavioral. While the emotional component of adaptation to change mediated the relationship between humanization and mental health in all three samples, the cognitive-behavioral component did so only in the Spanish sample. These results suggest that the ability to manage emotions and stress associated with change is key in protecting the teachers’ mental health (Akbaba, 2014; Rajendran et al., 2020). Furthermore, the ability to control and act in changing situations seems to have a stronger effect on Spanish teachers. These differences may reflect cultural variations in the perception and management of change in the educational environment. The differences observed among teachers in Spain, Portugal, and Italy in terms of humanization, adaptation to change, and mental health are noteworthy. For instance, Spanish teachers scored significantly higher in humanization compared to teachers from the other two countries. Additionally, the Portuguese and Italian samples scored higher on the emotional component of adaptation to change, while Spanish teachers showed lower scores in this component. These differences highlight the need to address education and teacher well-being taking into account the cultural and contextual specificities of each country. Furthermore, they may indicate that interventions aimed at improving teachers’ mental health should be adapted to the specific characteristics of each population. Finally, it is important to note that this study was based on cross-sectional data, which limits our ability to establish causal relationships between variables. Future research could employ longitudinal or experimental designs to more accurately examine how humanization and adaptation to change influence teachers’ mental health over time. Additionally, the sample was limited to teachers from three European countries, which restricts the generalizability of the results on a global scale. It would be valuable to replicate this study in other regions and cultures to better understand the differences and similarities in the relationship between humanization, adaptation to change, and mental health in teachers. Practical Applications and Future Lines of Research This study underscores the importance of promoting humanization as a key approach to enhance teachers’ mental health. Educational institutions can develop training and educational programs to help teachers acquire emotional management and adaptation to change skills. Therefore, the need to offer training and support in emotional management and adaptation to change as effective strategies to protect teachers’ mental health is highlighted. These findings are particularly relevant at a time when teachers have faced exceptional challenges due to the COVID-19 pandemic, and we are currently observing its consequences. Future research can employ longitudinal or experimental designs to examine the causal relationships between humanization, adaptation to change, and teachers’ mental health over time. Additionally, further studies could explore specific interventions that promote humanization and adaptation to change in the educational context and assess their impact on teachers’ mental health. Conclusions This study highlights the importance of humanization and adaptation to change in promoting teachers’ mental health. The results suggest that improving humanization and providing support for emotional management and adaptation to change could be crucial in safeguarding the mental health of European teachers. However, cultural differences should be taken into account when addressing these issues. These findings have significant implications for the development of interventions and support programs aimed at teachers in various educational settings. Conflict of Interest The authors of this article declare no conflict of interest. Cite this article as: Molero, M. M., Martos, A., Pérez-Fuentes, M. C., Tortosa, B. M., Sisto, M., Simón, M. M., & Gázquez, J. J. (2024). Humanization, adaptation to change, and mental health in teachers in three european countries. European Journal of Psychology Applied to Legal Context, 16(1), 17-25. https://doi.org/10.5093/ejpalc2024a2 Funding: This publication is part of the I+D+i PID2020-119411RB-I00 funded by MCIN/AEI/10.13039/501100011033/ and FEDER “Una manera de hacer Europa”. References |
Cite this article as: Molero, M. M., Martos, Á., Pérez-Fuentes, M. C., Tortosa, B. M., Sisto, M., Simón, M. M., & Gázquez, J. J. (2024). Humanization, Adaptation to Change, and Mental Health in Teachers in Three European Countries. The European Journal of Psychology Applied to Legal Context, 16(1), 17 - 25. https://doi.org/10.5093/ejpalc2024a2
Correspondence: amm521@ual.es (Á. Martos).
Copyright © 2026. Colegio Oficial de la Psicología de Madrid





 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
The European Journal of Psychology Applied to Legal Context is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License








