


Evidence-based Interventions Targeting Remand Prisoners: A Systematic Review and Meta-analysis
[Intervenciones basadas en la evidencia dirigidas a reclusos en prisión preventiva: revisión sistemática y meta-análisis]
Joana Andrade1, Rui A. Gonçalves1, Catarina Abrunhosa1, and Andreia de Castro-Rodrígues2
1University of Minho, Braga, Portugal; 2William James Center for Research, ISPA, Lisbon, Portugal
https://doi.org/10.5093/ejpalc2024a5
Received 30 March 2022, Accepted 9 January 2024
Abstract
Background/Aim: Official data show that nearly three million people are awaiting trial in prison. Despite this group representativeness, few interventions have been developed and assessed for these prisoners, even though literature has been showing that they present specific vulnerabilities. Nevertheless, no previous literature review had covered this topic. Considering this, the present review aims to gather evidence on the programs focused on this population, analyzing their intervention targets and their effectiveness. Method: The search identified a total of 7,143 studies. After removing the duplicates, 2,199 were screened using the title and abstract, according to the inclusion criteria. The full-text screening comprehended 45 articles, of which 37 were excluded. This resulted in 8 studies for inclusion in the final analysis, of which four were pharmacological studies. Results: Overall, meta-analysis results exhibited that treatment of remand prisoners (RPs) has an extraordinarily large positive effects, exceeding 92%. Our study confirmed that RPs would benefit from treatment, and therefore intervention programs should be established. Conclusions: Besides, our findings underlined the scarce resources to address the difficulties of the remand population, reinforcing the importance of assessing these individuals’ needs to develop effective responses to them.
Resumen
Introducción/Objetivo: Los datos oficiales muestran que casi tres millones de personas se encuentran en prisión a la espera de juicio. A pesar de la representatividad de este grupo, se han desarrollado y evaluado pocas intervenciones para estos presos, a pesar de que las publicaciones científicas han venido demostrando que presentan vulnerabilidad específica. Sin embargo, ninguna revisión anterior de la literatura había abordado este tema. Teniendo esto en cuenta, la presente revisión pretende reunir evidencias sobre los programas dirigidos a esta población, analizando sus objetivos de intervención y su efectividad. Método: La búsqueda identificó un total de 7,143 estudios. Tras eliminar los duplicados, se seleccionaron 2,199 mediante el título y el resumen, de acuerdo con los criterios de inclusión. El cribado del texto completo comprendió 45 artículos, de los cuales 37 fueron excluidos. Esto dio lugar a 8 estudios para su inclusión en el análisis final, de los cuales 4 eran estudios farmacológicos. Resultados: En general, los resultados del meta-análisis mostraron que el tratamiento de los presos preventivos tiene enormes efectos positivos, superiores al 92%. Nuestro estudio confirmó que los presos preventivos se beneficiarían del tratamiento, por lo que deberían establecerse programas de intervención. Conclusiones: Los resultados subrayan los escasos recursos que hay para abordar las dificultades de la población en prisión preventiva, reforzando la importancia de evaluar las necesidades de estos individuos para desarrollar respuestas efectivas a las mismas.
Keywords
Remanded prisoners, Pre-trial detention, Interventions, Systematic review, Meta-analysisPalabras clave
Presos preventivos, Arresto antes del juicio, Intervenciones psicolĂłgicas, RevisiĂłn sistemática, Meta-análisisCite this article as: Andrade, J., Gonçalves, R. A., Abrunhosa, C., & Castro-Rodrígues, A. D. (2024). Evidence-based Interventions Targeting Remand Prisoners: A Systematic Review and Meta-analysis. The European Journal of Psychology Applied to Legal Context, 16(1), 49 - 59. https://doi.org/10.5093/ejpalc2024a5
Correspondence: joana.rm.andrade@gmail.com (J. Andrade).
The Use of Pre-trial Detention Detention on remand is widely used all over the world. Although pre-trial detention (PTD) should be the exception, not the norm (Levin & Haugen, 2018), official data show that there are nearly three million remand prisoners (RPs) throughout the world (Walmsley, 2020). Indeed, statistical information from 2021 revealed that at least 47 countries had more than half of the prison population untried (Walmsley, 2020). In some jurisdictions, the rates of inmates awaiting trial exceed the number of sentenced prisoners (SP) (Ortiz, 2015; United Nations Office on Drugs and Crime [UNODC, 2018]). PTD is a utilitarian and risk-oriented order that should be applied as a measure of last resort and without violating the presumption of innocence (Martufi & Peristeridou, 2020). However, the legislative grounds for PTD could vary from place to place (Baughman, 2017), which makes it difficult to compare rates across different countries. Following the Portuguese law (similarly among democratic countries), PTD is foreseen in the Code of Criminal Procedure for situations where other enforcement measures are considered less appropriate. Official data from May 2021 indicated that there were 2,208 RPs in Portugal (about 19.5% of the total prison population) (see https://dgrsp.justica.gov.pt). Moreover, official records show that from 2015 to 2020 the percentage of RPs has increased despite the total prison population decrease (J. A. Moreira & Martins, 2019). The Portuguese Penal Code, particularly article 202, states that prison detention should be considered when: a) the alleged offense is punished with a sentence that could be longer than five years and is presumed to have been committed intentionally; b) the alleged offense corresponds to a violent crime; c) the alleged offense could be a terrorist act or corresponds to a highly organized crime that could be sentenced longer than three years; d) there is evidence of aggravated crimes that were committed with intent and the sentence could be longer than three years; and e) it concerns a person who has entered illegally in the national territory, or against whom extradition or expulsion proceedings are in progress. The use of PTD is widely known to have many undesirable consequences for the criminal justice system, society, and inmates (Baughman, 2017), which underlines the importance of applying it only when another measure seems inefficient. Since criminogenic effects for individuals seem to start at the pre-trial stage (Dobbie et al., 2018), it may presume that the pejorative consequences of being labelled as a prisoner tend to occur even if the defendant will not be found guilty. RPs’ Conditions and The Importance of Developing Responsive Interventions Within the prison setting, PTDs are usually perceived as criminals as those condemned, even though they were not yet found guilty. Previous studies underlined the lack of responses for RPs’ needs, particularly concerning mental health care (Ruddell, 2006; Weinrath et al., 2019), as well as a higher tendency to provide ill treatment to this group (Open Society Justice Initiative, 2011). Despite this, when compared to SP, RPs usually reported lower levels of well-being (Cumming & Wilson, 2009; Ruddell, 2006; Tweed et al., 2021), higher levels of mental disorder (Cumming & Wilson, 2009; Ruddell, 2006; Tweed et al., 2021), and a high tendency for prison suicide (Cumming & Wilson, 2009; Zhong et al., 2021). According to the evidence, the most common cause of death in jails is suicide (Berman & Canning, 2022; Fazel et al., 2008; World Health Organization [WHO, 2000]). Inmates are known to be one of the risk groups to show suicidal behaviors since they are in a vulnerable situation resulting from a combination of stressors, including psychological and environmental factors (WHO, 2000). Also, data about the prevalence of prison deaths worldwide have shown a higher incidence among RPs (Berman & Canning, 2022; Boren et al., 2019; Sarre et al., 2006; WHO, 2000; Zhong et al., 2021). In Portugal, the mortality rates within prison walls are one of the highest in Europe. Furthermore, according to the existing data, two-thirds of these deaths – either suicides or homicides – occur to RPs (Carvalho et al., 2016). Besides, it should be borne in mind that these statistics do not include non-suicidal self-injuries (N. C. Moreira & Gonçalves, 2012). Non-suicidal self-injuries are also highly prevalent in this population (Favril, 2019), which is easily understood since increased levels of negative emotional distress are a risk factor for non-suicidal self-injury behaviors (Selby et al., 2019). Moreover, evidence also displayed that when mental illness problems are left untreated among the inmate population, this tends to result in an increased risk of disturbance behaviors and disciplinary violations (Ruddell, 2006; Veysey & Bichler-Robertson, 2002). It is important to note that imprisonment itself represents a risk of developing mental health problems due to the inmates’ deprivation and exposition to undesirable conditions. The group of inmates awaiting trial could be presumed to have even more difficulties due to the uncertainty of their future (Duthé et al., 2013). Besides, often, these individuals do not have the same opportunities as those sentenced. Since their detention is presumably temporary, they tend not to have equal opportunities inside the prison (Schönteich, 2018), in terms of access to education, training, and work opportunities (Open Society Justice Initiative, 2011). This lack of positive opportunities might contribute to the difficulties felt during their detention. As a result, this deprivation could enhance feelings of segregation and insecurity by RPs. Most research conducted with the prison population focused on convicted inmates, and as a result most interventions are applied mainly to SP. Even though some studies had explored the RPs’ needs, the truth is that little has been done to address these issues in terms of intervention (HM Inspectorate of Prisons, 2012; Ruddell, 2006). Indeed, the penal system continues to be characterized by a lack of responses for this group. Also, beyond RPs’ difficulties being usually different, they were not found guilty yet, and it may be inadequate to include them in reintegration programs. Thus, the development of appropriate interventions that fit RPs’ particular situations and address their specific needs should be stressed. Considering the literature gap regarding interventions targeting RPs, a systematic review and meta-analysis was designed to assess the efficacy of the programs focused on this population. First, it was intended to understand to what extent RPs are included in prison interventions, treatments, and therapies. Besides, it was aimed to assemble these efforts in order to identify the intervention targets and understand how effective they show to be. Inclusion/Exclusion Criteria This review followed the guidelines of the PRISMA statement (Page et al., 2021). The eligibility criteria of the studies for inclusion were a) studies that describe interventions that targeted RPs (including male, female, young, and adults on remand) and b) written in English. As exclusion criteria we defined a) interventions that included sentenced prisoners, b) non-empirical studies (such as reviews, conference papers, editorials, and books), and c) studies that describe pharmacological or non-psychological interventions. No limits were set concerning the year of publication. Besides, since unpublished articles might lack scientific rigor, we include only published articles to ensure higher levels of robustness in our results. This study was conducted at Psychology Research Centre (UID/PSI/01662/2013), University of Minho, and it was approved by the University of Minho Ethics Commission (CEICSH 051/2021). All procedures performed were in accordance with the tenets of the Declaration of Helnsiki. Search Strategy The search was performed in three electronic databases (PubMed, Web of Science, and Scopus) using the combination of the following key terms: (“Pretrial” OR “Pre-trial” OR “Preventive det*” OR “Remand*” OR “Awaiting trial”) AND (“intervention*” OR “program*” OR “therap*” OR “treatment*”), by title, abstract, and keywords. Since no previous systematic reviews exist regarding interventions for RPs, we included in the search all the studies up to December 2021, this month included. The only limit used was the language (only English articles). Study Selection and Coding Procedures Once we removed the duplicates, two independent researchers read the titles and abstracts. Manuscripts accepted for full-text reading were coded in a data extraction sheet according to the following key topics: reference information (e.g., author, year, type of manuscript), study characteristics (e.g., design, country, sampling strategy), sample description (e.g., gender, age), and intervention data (e.g., type of intervention, theoretical model, eligibility, intervention target and content description, length of delivery, dropout rates, and outcomes/results). Missing characteristics were coded as “not available”. All these stages of searching, selecting, and coding procedures as well as quality assessment of included studies were developed by two independent researchers, following the best practices recommendations (Siddaway et al., 2019). Quality Assessment One of the crucial stages of systematic reviews is the critical quality assessment of included studies. In this review, we used the Mixed Method Appraisal Tool (MMAT; Hong et al., 2018). The MMAT is a tool to be used to appraise the quality of empirical research based on five criteria. Each study was rated as weak, moderate, or strong, depending on the met/unmet criteria. A total of 7,413 articles resulted from the search (Figure 1). After removing the duplicates, we analyzed 2,199 studies’ titles and abstracts. From these, full-text screenings included a total of 45 papers, of which 37 were excluded for the following reasons: 17 did not describe any intervention, 17 were not applied to remand prisoners, and 3 were not limited to the RPs. The final analysis included only 8 studies (Table 1), which corroborate the idea that RPs are usually a group neglected from interventions in prison. Figure 1 PRISMA Flowchart. 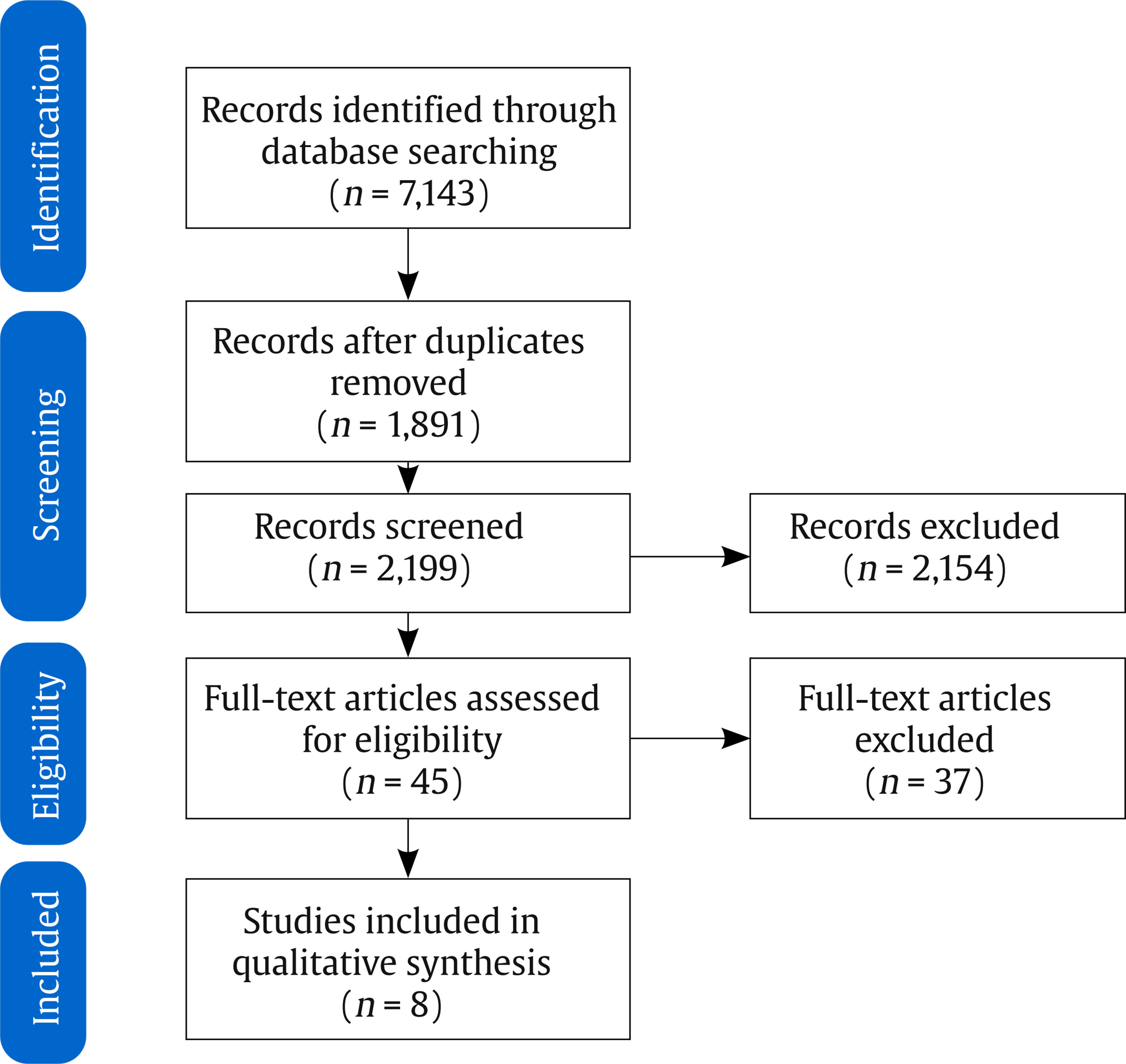 Table 1 Summary of the Psychological Interventions Included 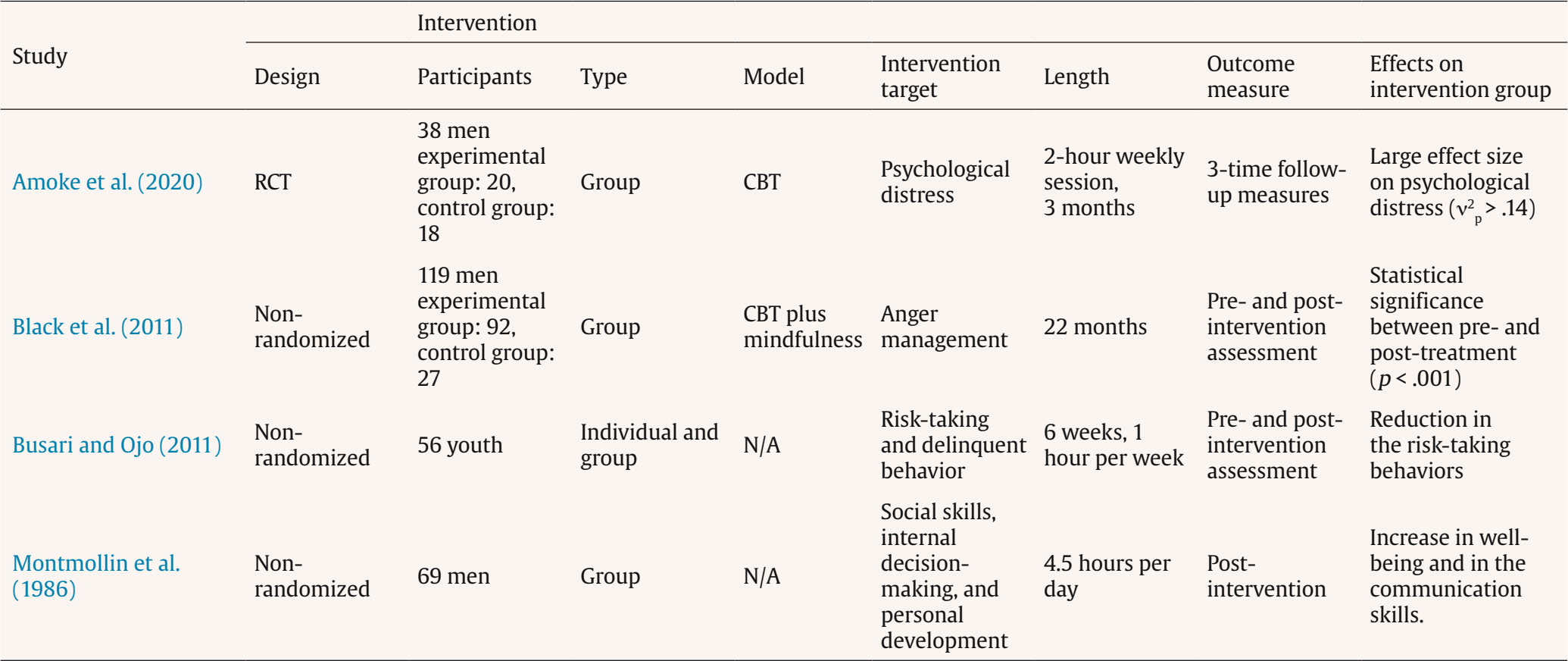 Characteristics of Included Studies Four studies described psychological interventions (Amoke et al., 2020; Black et al., 2011; Busari & Ojo, 2011; Montmollin et al., 1986), while the others are pharmacological (Favrod-Coune et al., 2013; Jeanmonod et al., 1991; Mitchell et al., 2020; Schwartz et al., 2020). The studies included took place in Nigeria (Amoke et al., 2020), UK (Black et al., 2011), USA (Busari & Ojo, 2011), USA (Mitchell et al., 2020; Schwartz et al., 2020), and Switzerland (Favrod-Coune et al., 2013; Jeanmonod et al., 1991; Montmollin et al., 1986). Only one study targeted youth on remand (Busari & Ojo, 2011), while the others refer to interventions targeting adult respondents. Regarding the study designs, three were randomized control studies (RCT; Amoke et al., 2020; Johnson et al., 2020; Johnson et al., 2017; Mitchell et al., 2021), while the others were non-randomized quantitative studies. Quality Assessment and Risk of Bias The quality assessment measured by Hong et al. (2018) showed that seven out of the eight studies presented acceptable quality. The RCT conferred all the criteria of excellence. One non-randomized study showed four out of five quality criteria, while the other three presented three. Besides, one of the included studies did not show satisfactory quality, having less than half of the criteria present (i.e., had only two out of the five criteria of excellence). It should be noted that when it was not possible to ascertain that a criterion was present, researchers coded it as “can’t tell”, which equates to an unmet criterion. Concretely, the RCTs (Amoke et al., 2020; Mitchell et al., 2020; Schwartz et al., 2020) presented: randomization appropriately performed (criterion 1), no differences between the groups at the baseline (criterion 2), acceptable complete data without any dropout rate (criterion 3), blinded conditions were ensured (criterion 4), and all participants adhere to assigned intervention (criterion 5). Regarding the study of Black et al. (2011), the measurements were appropriate regarding both the outcome and intervention (criterion 2), the confounders were accounted for in the analysis (criterion 4), and the intervention was administered as intended, meaning that participants were treated according to the planned intervention (criterion 5). Despite this, the study failed to gather a representative sample of the population (criterion 1), as well as in obtaining complete outcome data (criterion 3), considering the high rates of non-compliance and dropout. The study of Busari and Ojo (2011) showed adequate measurements (criterion 2) and complete outcome data (criterion 3), and during the study period the intervention was administered as intended (criterion 5). However, the study miscarried on aggregate a representative sample of the population (criterion 1), as well as on account of confounding factors (criterion 4). The study of Montmollin et al. (1986) had appropriate measurements (criterion 2), and the assigned intervention followed the initial (criterion 5). Nonetheless, the work did not include a representative sample (criterion 1), did not show acceptable outcome data (criterion 3), and did not indicate methods to control confounders (criterion 4). The study of Favrod-Coune et al. (2013) exhibited appropriate measurements (criterion 2) and acceptable outcome data (criterion 3), indicated methods to control confounders (criterion 4), and during the research the intervention was administered as planned (criterion 5). Despite this, the paper failed to aggregate a representative sample of the population (criterion 1). Finally, the study conducted by Jeanmonod et al. (1991) presented appropriate measurements (criterion 2), had methods to control confounders (criterion 4), and administrated the intervention as intended (criterion 5). However, the findings cannot be generalized (criterion 1) and there were no complete outcome data since a significant part of the participants did not contribute to all measures (criterion 3). Psychological Interventions Description Considering the modality of intervention, all psychological interventions included in this review (Amoke et al., 2020; Black et al., 2011; Busari & Ojo, 2011; Montmollin et al., 1986) described group interventions. The targets of interventions were psychological distress (Amoke et al., 2020), anger management (Black et al., 2011), risk-taking and delinquent behavior (Busari & Ojo, 2011), and social skills, internal decision-making, and personal development (Montmollin et al., 1986). Two interventions (Amoke et al., 2020) followed the cognitive behavior therapy (CBT) principles (see Beck, 2020). Concretely, participants worked on their emotions, thoughts, and behaviors, identifying distorted beliefs and replacing them with alternative ways of thinking and behaving. Moreover, the study of Black et al. (2011) also included a component of mindfulness linked to the CBT session, integrating both techniques to manage daily situations. Besides, the studies of Montmollin et al. (1986) and Busari and Ojo (2011) did not adhere to a specific model. The first covered discussion groups, creative work, and social skills training, while the second described weekly and daily programs based on different intensive and multiple contacts. The length of interventions ranged between six weeks (Busari & Ojo, 2011) and 22 months (Black et al., 2011). A summary of psychological interventions is presented in Table 2. Table 2 Psychological Interventions’ Content 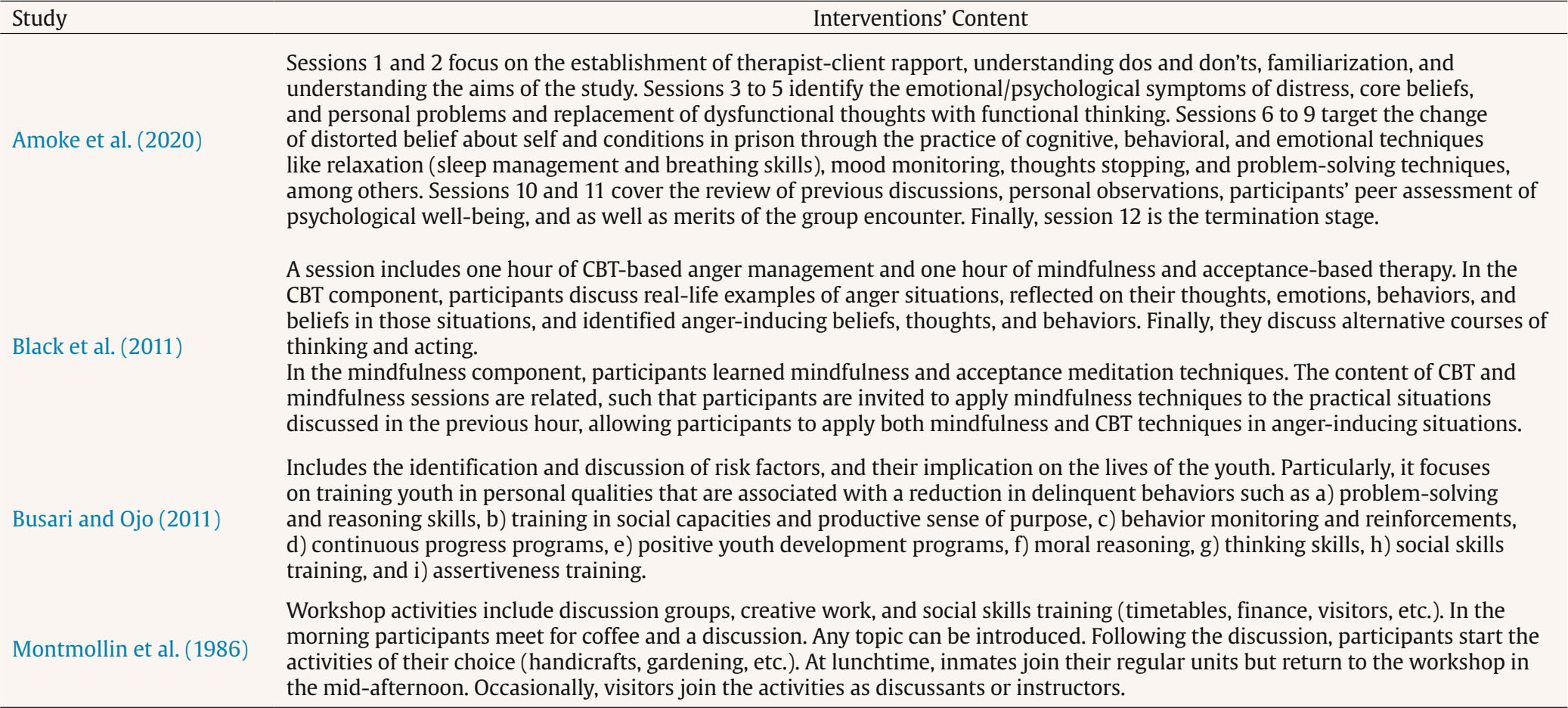 Psychological Intervention Outcomes The two psychological interventions that comprised an experimental and control group (Amoke et al., 2020) displayed that the group who participated in the treatment condition showed improvement during the intervention. In the study of Amoke et al. (2020), differences between pre- and post-intervention were assessed as measured by the PEDI (Perceived Emotional Distress Inventory), and the GHQ-12 (General Health Questionnaire). Black et al. (2011) used the STAXI-II (Spielberg Anger Expression Inventory-2). Both studies found a positive effect of the interventions, with the work of Amoke et al. (2020) showing a large effect size ( > .14) of the treatment and the study of Black et al. revealing a statistical significance difference between pre- and post-treatment (p < .001). Regarding the study of Busari and Ojo (2011), the researchers compare pre- and post-intervention reports (repeated measures design) using the TILQ (Transition to Independent Living Questionnaire), having found a reduction in delinquent behavior after the interventions. Finally, the work of Montmollin et al. (1986) only used post-intervention measures through a structured questionnaire that assessed both the inmates’ and the guards’ perceptions of the outcomes of the intervention. The results reported that participants reacted positively to the treatment setting, referring to the positive experience during the program. Pharmacological Interventions Description The intervention target of treatments that included the application of medication was drug abuse problems and in one case the sex-related HIV-risk behaviors associated with drug use (Mitchell et al., 2021). All studies applied a protocol of methadone maintenance treatment. One study included other prescribed drugs (buprenorphine, tramadol, and codeine) for a small portion of participants who refuse methadone (Favrod-Coune et al., 2013). Three studies applied the treatment during the individuals’ prison stay (Favrod-Coune et al., 2013; Mitchell et al., 2020; Schwartz et al., 2020), while the other prescribed methadone over 5-10 days in decreasing doses according to the standard practice of the prison medical services (Jeanmonod et al., 1991). Pharmacological Interventions Outcomes Two of the for pharmacological interventions included a control group (i.e., a group in treatment as usual) (Mitchell et al., 2021; Schwartz et al., 2020). Both studies conducted compare three conditions: a) group with methadone maintenance without counseling, b) group with methadone maintenance plus counseling, and c) group in treatment as usual that consisted of brief medically supervised withdrawal using methadone. The work developed by Mitchell et al. (2021) aimed to analyze the relative effectiveness of the three interventions in reducing drug use and sex-related HIV-risk behaviors. The results showed that there were no significant differences in post-release HIV drug and sex risk scores among the three groups. Regarding the study of Schwartz et al. (2020), which aimed to understand if there were differences between the three groups, the conclusions also revealed that there were no significant differences. The two groups assigned to initiate interim methadone treatment in jail had significantly higher rates of post-release treatment entry compared to the control group, but later treatment discontinuation diminished the potential impact of such treatment. The research conducted by Favrod-Coune et al. (2013) intended only to describe an opioid substitution treatment, and therefore any assessments were conducted. However, the study concluded that these types of treatment are feasible and safe in a pretrial setting. Finally, the study of Jeanmonod et al. (1991) was carried out in order to assess the effectiveness of the treatment offered in reducing or eliminating symptoms of opiate withdrawal in a remand prison setting. The results exhibited that there was a significant difference between withdrawal scores over time. Most participants felt that methadone had been effective in relieving symptoms, even though some participants had reported that the treatment period was too short or had not been effective. Besides, despite the general improvement, the symptomatic relief was incomplete for symptoms like insomnia and restlessness. Table 3 Summary of the Psychological Interventions Included 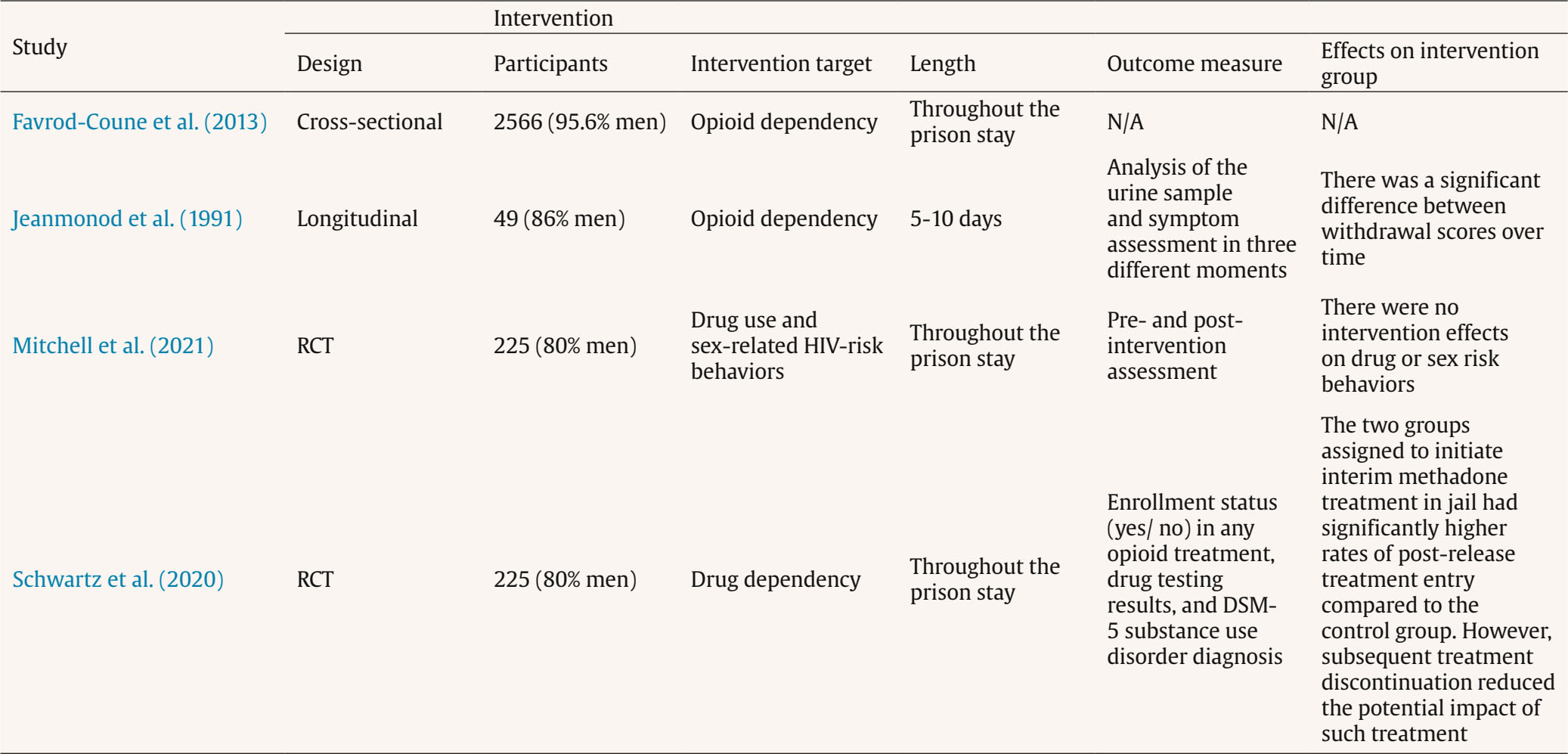 Table 4 Meta-analyses of the Treatment Effect of Remand Prisoners  Note. k = number of effect sizes; N = total sample size; dw = sample size weighted mean effect size; SDd = standard deviation of d; SDpre = standard deviation predicted for sampling error alone; SDres = standard deviation of d after removing sampling error variance; δ = mean true effect size; SDd = standard deviation of d; %Var = percent of observed variance accounted by artifactual errors; 95% CId = 95% confidence interval for d; 80% CIδ = 80% credibility interval for δ. Table 5 Meta-analyses of the Effect of Type of Treatment Moderator in Internalizing Mental Health Markers  Meta-analyses Global Effects The overall impact is summarized in Table 3. The findings revealed a positive (improvement in treatment markers), significant, Z = 69.58, p < .001, and more than large magnitude (δ > 1.20, an effect size above 92.4%, PSES = .924) mean true effect size (δ = 2.028) for the treatment of remand prisoners. However, the results are no generalizable to the population of studies (credibility interval has zero), i.e., negative effects may be obtained (the lower limit of the credibility interval is negative). Furthermore, this variability can be attributed to moderating factors, with the distribution of studies exhibiting heterogeneity (% var < 75%). Therefore, it is imperative to explore the moderators of this effect. Through a content analysis of the primary studies, the measurement of the effects, specifically internalizing and externalizing mental health markers, were identified as a key moderator to be examined. Treatment Effect on Internalizing Mental Health Markers A positive, significant, Z = 44.94, p < .001, generalizable (the minimum expected effect was 1.701 for 90% of the future studies), and more than large (δ > 1.20) mean true effect size (δ = 2.458) was observed in internalizing mental health problems (see Table 4). Furthermore, the observed effect size exceeded 95.9% of all possible true effects (PSES = .959). Nevertheless, heterogeneity was observed among studies (% var < 75%). This implies that while positive and significant effects are anticipated in the studies, noteworthy differences in treatment outcomes between studies might be observed. According to the treatment implemented, the moderators of the effects registered in the content analysis of the primary studies were: cognitive behavioral therapy and sociotherapeutic workshop. As displayed in Table 5, the results of the meta-analysis for the cognitive behavioral therapy determined a positive (clinical improvement in internalizing mental health problems), significant, Z = 12.02, p < .001, generalizable (the minimum expected effect for 90% of the population of studies was 1.367), and more than large (δ > 1.20, an effect size above 93.2%, PSES = .932) mean true effect size (δ = 2.113). However, despite the systematic positive impact, the distribution of the effects is heterogeneous inter studies in internalizing mental health problems (% var < 75%). As for the sociotherapeutic workshops the results revealed a positive (clinical improvement in internalizing mental health problems), significant, Z = 43.14, p < .001, generalizable (the minimum expected effect for 90% of the population of studies is 1.957), and more than large (δ > 1.20, an effect size above 96.5%, PSES = .965) mean true effect size (δ = 2.558). Nevertheless, similar to cognitive behavioral therapy, a heterogeneity distribution was observed inter studies. Comparatively, the effect of sociotherapeutic workshops was significantly larger, qs(N’ = 448) = .207, Z = 3.08, p = .001, than that of cognitive behavioral therapy. Treatment Effect on Externalizing Mental Health Markers A positive, significant, Z = 52.83, p < .001, generalizable (the minimum expected effect for 90% of the population of studies is 1.702), and more than large (δ > 1.20, an effect size above 90.0%, PSES = .900) mean true effect size (δ = 1.814) was observed in externalizing mental health problems (as depicted in Table 4). However, it is essential to note that these results might not be universally generalizable to the entire range of studies, as some treatments may yield negative effects on externalizing problems (indicated by the negative lower limit of the credibility interval, -0.984). The distribution of the studies is heterogeneous (% var < 75%), meaning that differences between studies are explained by moderators. In the primary studies review, the type of treatment was identified as a moderator to study: methadone and psychological therapy. Table 6 shows the effect of moderators in externalizing mental health markers. Methadone treatment yielded a positive (less externalizing mental health problems), significant, Z = 51.29, p < .001, and more than large (δ > 1.20, an effect size above 99.7%, PSES = .997) mean true effect size (δ = 1.962) of the treatment with methadone in externalizing mental health problems. However, this outcome may not be generalizable across all studies, as negative effects might also arise from this treatment (the lower limit of the credibility interval was negative, -0.838). Additionally, the distribution of the studies is heterogeneous (% var < 75%), where moderators accounted for both positive and negative effects. In the case of cognitive behavioral therapy, the results of the meta-analysis exhibited a positive (reduction of negative outcomes in externalizing mental health problems), significant, Z = 13.24, p < .001, and of a large magnitude (δ > 0.80, an effect size above 88.5%, PSES = .885) mean true effect size (δ = 1.066) of the cognitive behavioral therapy in externalizing mental health problems. Similarly, the generalizability of these results across the entire spectrum of studies is committed, as negative effects may be also observed (the lower limit of the credibility interval was negative, -0.464). Heterogeneity in the distribution of the studies was also observed (% var < 75%), suggesting differences between studies explained by moderators. Comparatively, the effects of methadone were significantly more positive (improvement in externalizing mental health problems) than those of cognitive behavioral therapy, qs(N’ = 1605) = .323, Z = 9.14, p < .001. Table 6 Meta-analyses of the Effect of Type of Treatment Moderator in Externalizing Mental Health Markers  A moderator was identified in the primary studies, specifically examined concerning the externalizing measure attributed to the treatment administered, focusing on drug use. The meta-analysis of psychological therapy on drug use (k = 3, N = 336) yielded non-significant effects (dw = 0.056, Z = 0.51, p = .610. Contrastingly, in the case of treatment involving methadone (k = 27, N = 3,467), a significant effect, dw = 1.763 95% CI [1.685, 1.841]. However, negative effects might be elicited by the application of methadone in treating drug use, as indicated by the negative lower limit of the 80% CIδ -0.933. Due to insufficient k values (k < 3) and an inadequate sample size (N < 300), other potential moderators could not be effectively investigated. Comparatively, significant more positive effects, qs(N’ = 3314) = .221, Z = 8.99, p < .001, were observed in internalizing mental health problems in comparison to externalizing mental health problems. RPs are a particularly at-risk population inside prisons in terms of mental disorder (Cumming & Wilson, 2009; Ruddell, 2006; Tweed et al., 2021), and suicide (Cumming & Wilson, 2009; Zhong et al., 2021). Hence, it is crucial to acknowledge their problems and the initiatives that have and are being made to minimize them. This article aims to gather evidence about the interventions that targeted this group of prisoners, identifying which programs have been developed and to what extent they showed effective results. According to the inclusion criteria previously described, this systematic review found only eight published papers that describe and assess an intervention on RPs. Despite this low result, this is not the first time a systematic review found a huge lack of research on a given topic (e.g., Dehghanniri & Borrion, 2021; Johnson et al., 2019; Maniglio, 2008; Whiteside et al., 2020). This expressive small number of articles supports the assumption that inmates awaiting trial are usually disregarded from the efforts to treat mental and emotional health disorders and adaptation problems within prisons (Duthé et al., 2013). Indeed, this result is not surprising since this particular group, due to the uncertainty of their stay, is often neglected from the intervention practices (HM Inspectorate of Prisons, 2012; Ruddell, 2006). Concerning the psychological interventions, we noticed that despite the low number, the target interventions were all different. This could reflect the heterogeneity of problems within this group. Indeed, several studies had reported a high tendency for comorbidity conditions in RPs (Barrett et al., 2020; Bebbington et al., 2017; Combs et al., 2019; Eytan et al., 2011). Even though epidemiological studies showed the prevalence of different types of disorders, we noticed that no intervention had targeted a particular disorder. Instead, psychological interventions were designed to address more general difficulties exhibited by the target population. Amoke et al. (2020) established psychological distress as the main target of the intervention. Indeed, previous works underlined the likelihood for inmates to present high levels of psychological distress, particularly during the first periods of incarceration (Elger, 2009; Gonçalves et al., 2016; Orjiakor et al., 2017). We can presume that RPs suffer even more than SP since they face the difficulties of prison adaptation and at the same time they need to deal with doubts about their future. Since psychological stress is a factor that could be linked to suicide attempts (Hayes, 2010; Liebling, 2007), it is important to address such issues to support the RPs’ adaptation. Moreover, the literature showed that psychological stress and self-harm behaviors are linked to a higher probability of misconduct in prison and to the display of violent behaviors (Vinokur & Levine, 2019). The study developed by Black et al. (2011) targeted precisely anger management. Previous research underlined that RPs are known to be the more violent and problematic group inside prisons (Værøy, 2011). Anger is sometimes a non-adaptative response for individuals struggling with mental disorders. In fact, anger behaviors are usually related to mental health problems (Bahrami et al., 2016; Rose et al., 2018), and cognitive-behavioral treatments are more likely to have positive effects on aggressive individuals (Lee & DiGiuseppe, 2018). Similarly, Busari and Ojo (2011) targeted risk-taking and delinquent behavior in a large spectrum, providing skills to increase pro-social and adaptative behaviors and trajectories. This program was developed for juvenile delinquents. Adolescence is a period when teenagers tend to engage in some risky conduct and, to some extent, these behaviors are considered normal (Christensen & Baker, 2020). Many studies had focused on delinquent trajectories and distinguished between adolescence-limited offenders from life-course-persistent offenders (see Mallet & Fukushima, 2019; Moffitt, 1993). It is critical to discontinue this deviant path, avoiding juveniles’ continuity of crime during adulthood. Indeed, researchers and practitioners have underlined the cost-effectiveness of intervention programs in youth (Christensen & Baker, 2020; Kratcoski et al., 2020), enhancing their likelihood to engage in prosocial behaviors. Besides, the intervention proposed by Montmollin et al. (1986) focused on social skills, internal decision-making, and personal development. Likewise, the authors targeted general skills to enhance the individuals’ adjustment. It is well-reported that the lack of social skills is linked to criminal and antisocial behavior (Lipsey et al., 2010; Mariano et al., 2017). Moreover, there is some evidence that correlates impulsivity and the tendency to exhibit emotion-driven behaviors to criminal and violent conduct (Bousardt et al., 2016; Meijers et al., 2017; Moore et al., 2017), thus emphasizing the role of internal decision-making and the ability to ponder and to inhibit disruptive behaviors. The current review showed that all psychological interventions were applied in group modality, even though one of them (Busari & Ojo, 2011) also included an individual component. Indeed, group interventions usually are the most cost-effective (Rath et al., 2010) since it allows a more resourceful use of therapists (Galik et al., 2013). It also allows some processes such as cohesiveness and modeling (Ezhumalai et al., 2018). Regarding the therapeutic model, two out of the four studies (Amoke et al., 2020; Black et al., 2011) were grounded in the cognitive-behavioral model. Besides, Black et al. (2011) also included a component of mindfulness. Cognitive-behavioral therapy is one of the most effective interventions to work with offenders (Bonta & Andrews, 2024; Landenberger & Lipsey, 2005). Indeed, this model had already been named the “gold standard” of psychological treatment (David et al., 2018). Previous research highlighted that people involved in criminal justice often had cognitive distortions and maladaptive schemas, and cognitive and behavioral techniques seem to be effective in inducing the process of change (Hofmann & Hayes, 2018). Moreover, we noticed that the remaining two studies (Busari & Ojo, 2011; Montmollin et al., 1986) did not specify any theoretical model underlying the programs, even though they applied some cognitive and behavioral techniques. These programs may not rely on a specific psychological model because they may not be designed only for psychologists. All studies that described a psychological intervention protocol have found positive effects of the interventions. These results showed that despite RPs represent a problematic group, their difficulties could be minimized if proper intervention is provided (Bonta & Andrews, 2024). Indeed, a previous systematic review noted that psychological interventions, particularly cognitive-behavioral therapies showed a positive effect on offenders’ treatment (Landenberger & Lipsey, 2005). As mentioned, RPs is a group with a high prevalence of mental disorders. The association between mental disorders and crime has been reported (Peay, 2011; Whiting & Fazel, 2020), and it seems to be essential to provide proper support and treatment to those involved in the criminal justice system. Considering the pharmacological interventions, we concluded that all of them target drug abuse problems, which is known to be a considerable problem among pre-trial detainees (Chow et al., 2018; Eytan et al., 2011; Mason et al., 1997; Scott et al., 2015). Indeed, drug-related disorders are very common among these individuals, and recent evidence showed that such conditions are frequently associated with other comorbid problems (Andrade et al., 2022). Given this, we consider that the findings of the present systematic review corroborate the notion that the developed interventions are not sufficiently inclusive of the broad of problems reported by RPs. Overall, meta-analysis results showed that treatment of RPs has an extraordinarily large positive effects, exceeding 92%. However, a comprehensive File Drawer Analysis (FDA = 2704 > 35; Rosenthal, 1979) revealed that when studies remain unpublished it skews the revised outcomes, effectively diminishing the effect to an insignificant level (Fandiño et al., 2021). To counter this and reverse the trend to a trivial effect, approximately 129 primary studies with non-effect are deemed necessary (Schmidt & Hunter, 2015). Additionally, there have been no significant, adverse, or minor effects observed with small sample sizes. This suggests that there is no proof indicating biased publication of research. Our study confirmed that RPs would benefit from treatment, and therefore intervention programs should be established. However, due to the limited evidence regarding the effectiveness of treatment for remand prisoners, most of them do not receive the benefit of such treatment, as it is not routinely implemented. Yet, it is important to note that the effectiveness of treatment might not apply universally to all aspects, as certain negative effects could be present. Findings indicate that these negative effects relate to externalizing mental health issues, not internalizing ones. Consequently, RPs consistently benefit from treatment when addressing mental health problems. Additionally, it was observed that treatments seem to be more beneficial for RPs dealing with internalizing mental health issues compared to those dealing with externalizing problems. Indeed, our results showed that significant, positive, and notably substantial effects were observed in cognitive behavioral therapy and sociotherapeutic workshops. However, these treatments were not standardized, resulting in heterogeneous effects across various studies and markers. Consequently, it remains challenging to examine the distinctions within these treatment methodologies and their impact across different indicators. Besides, positive effects were also found in externalizing mental health markers. These are robust predictors of recidivism (Goodley et al., 2022). Thus, externalizing mental health problems, mainly drug use, must be a target of the treatment with remand prisoners. In terms of the treatment technique, methadone and cognitive behavioral therapy exhibited a general positive effect in externalizing mental health markers, but both may also produce negative effects. The moderators of these contradictory effects could only be partially studied. In short, evidence was found for no-effects of cognitive behavioral therapy treatment in drug, whereas the treatment with methadone revealed a mean positive and more than large effect but negative effects may be made. It also important to pointed out that the focal points of the interventions primarily do not align with the criminogenic needs of RPs, except in cases related to drug use, which is considered a criminogenic need within the scope of the analysis. Notably, as these individuals have not been sentenced, penitentiary interventions are not mandated to address criminogenic needs. Rather, the interventions primarily target associated factors, such as externalizing mental health indicators linked with delinquent behaviors, and factors that serve as barriers to recidivism, identified as internalizing mental health indicators (Basanta et al., 2018; Becker et al., 2012). As our results indicated, the primary observed beneficial outcomes primarily centered around internal mental health indicators. Even though Bonta and Andrews (2024) introduced the R-N-R model, establishing that internal mental health issues are not directly linked to causing delinquency or relapse into criminal behavior, and therefore might not be the primary focus of treatment, it is important to note that mental health problems, which can emerge as an adverse consequence of imprisonment, play a dual role: they can act as a catalyst (albeit not the root cause) for relapse into criminal behavior and psychological adaptation, while also serving as a deterrent for recidivism, self-harm, and suicidal tendencies in correctional facilities (Basanta et al., 2018; Maruna, 2004). Furthermore, we consider it relevant to reflect on the reasons to exclude so many studies. Concretely, we acknowledged that 17 studies were excluded because they described community-based interventions. Therefore, it seems that intervention that targets individuals awaiting trial is more likely to be developed mainly for those who are diverted. Previous studies underlined the pertinence of diversion programs since they are an alternative to PTD that typically addresses the individuals’ difficulties (Camilletti, 2010). Moreover, it could be that these programs are cheaper than those within the jail context since they use community resources, conserving the justice system funds (Pierce-Danford & Guevara, 2013). We should underline that two studies were excluded because, despite having one first session in jail, the interventions were designed for jail inmates who were supposed to not be condemned to a prison sanction, and the consultation while incarcerated had only the aim to plan an intervention after release (Johnson et al., 2017; Johnson et al., 2014). These studies could reinforce the idea that intervention in prison might be more expensive and challenging, and supporting individuals after release could be a practical alternative to helping suspects. Besides, 17 studies were excluded because they failed in describing an intervention, and therefore they were not informative of the efforts developed to intervene if pre-trail detainees’ needs. Conclusion To our knowledge, this is the first systematic review looking at the psychological and pharmacological interventions targeting RPs. The results are relevant for the scope of literature, considering the gap on this issue and the urge to develop therapeutic efforts to address the needs and difficulties of inmates awaiting trial. Despite the reduced number of studies in this review, our results emphasized the positive effect of the interventions. Even though our findings are based on a small number of studies, which is very informative in itself, the eight interventions presented an acceptable quality, which gives confidence to our conclusions. We recommend that future research could develop, apply, and assess more interventions capable to support RPs’ needs. Also, although many effect sizes could be obtained, primary studies were scarce. Thus, future literature should increase on this topic and focused to the identification of the moderators of null and adverse effects. Besides, researchers should replicate the existing programs and control the effects of prisonization in the criteria to achieve more robust conclusions about their effects. Limitations While the present review offers critical findings, the study has the limitation of being based only on eight studies. As a result, at present, there is insufficient evidence to draw robust conclusions about how effective interventions that target RPs are shown to be. However, our findings offer the first comprehensive picture of the (lack of) evidence-based interventions for this particular group. This review is limited to the published English articles and, for that reason, we might not include valuable articles written in other languages. Furthermore, the prevalent application of repeated measures designs is a limitation, failing to account for the impact of the prison environment on criteria. Consequently, the effects ascribed to treatment may be influenced by the prison environment (e.g., restricting drug use or delinquent behaviors), possibly overestimating the treatment’s efficacy. Lastly, the utilization of non-standardized treatment techniques impedes an accurate estimation of the actual effectiveness of the administered treatments. Conflict of Interest The authors of this article declare no conflict of interest. Funding: This study has been funded by FCT – Fundação para a Ciência e a Tecnologia. Cite this article as: Andrade, J., Gonçalves, R. A., Abrunhosa, C., & de Castro-Rodrigues, A. (2024). Evidence-based interventions targeting remand prisoners: A systematic review andmeta-analysis. European Journal of Psychology Applied to Legal Context, 16(1), 49-59. https://doi.org/10.5093/ejpalc2024a5 References |
Cite this article as: Andrade, J., Gonçalves, R. A., Abrunhosa, C., & Castro-Rodrígues, A. D. (2024). Evidence-based Interventions Targeting Remand Prisoners: A Systematic Review and Meta-analysis. The European Journal of Psychology Applied to Legal Context, 16(1), 49 - 59. https://doi.org/10.5093/ejpalc2024a5
Correspondence: joana.rm.andrade@gmail.com (J. Andrade).
Copyright © 2026. Colegio Oficial de la Psicología de Madrid





 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
The European Journal of Psychology Applied to Legal Context is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License








