


Active Aging Program in Nursing Homes: Effects on Psychological Well-being and Life Satisfaction
[El envejecimiento activo en residencias para personas mayores: su efecto en el bienestar psicolĂłgico y la satisfacciĂłn vital]
Cristina Buedo-Guirado, Laura Rubio, Cristina G. Dumitrache, and Juan Romero-Coronado
University of Granada, Spain
https://doi.org/10.5093/pi2019a18
Received 28 March 2019, Accepted 1 October 2019
Abstract
A great number of intervention strategies that provide opportunities to maintain physical, psychological, and social wellbeing have been carried out in order to promote active aging. Most of these strategies are aimed at people without physicalor cognitive dependence, while institutionalized older people have not been considered as a target group. The main objectiveof this study was to analyze the effect of an active aging program on the psychological well-being and life satisfaction ofinstitutionalized older people. A total of 141 participants with adequate psychomotor skills were selected (Mage = 85.50 years,SD = 8.47), and a quasi-experimental pretest-posttest design with a control group and an experimental group was used. Thecontrol group participated in the traditional limited active aging program offered in long-term care facilities – cognitivestimulation and physical activity – while the experimental group participated in a comprehensive active aging program. Afterthe intervention, participants from the experimental group showed improvements in the mean values of psychological wellbeing and life satisfaction, while no change was found in the control group. The improvements in psychological well-beingand life satisfaction were maintained 12 months later in the follow-up evaluation. This study suggests that the inclusionof a comprehensive active aging program in nursing homes, that comprises actions aimed at promoting empowerment,participation, and social openness, contributes to the maintenance of perceived well-being.
Resumen
Se ha implementado un gran número de estrategias de intervención para promover el envejecimiento activo basadasen el mantenimiento del bienestar físico, psicológico y social. Muchas de esas estrategias se han llevado a cabo conpersonas mayores sin dependencia física o cognitiva, mientras que las personas mayores institucionalizadas no hansido un grupo objetivo. El principal objetivo de este estudio fue analizar el efecto de un programa de envejecimientoactivo sobre el bienestar psicológico y la satisfacción vital de personas mayores institucionalizadas. Participó un grupo de141 personas mayores con adecuadas capacidades psicomotoras (Medad = 85.50 años, DT = 8.47), utilizándose un diseñocuasiexperimental pretest-postest con grupo control y grupo experimental. El grupo control participó en un programatradicional limitado de envejecimiento activo ofrecido en residencias (estimulación cognitiva y ejercicio físico) mientrasque el grupo experimental participó en un programa global de envejecimiento activo. Tras la intervención aumentó lapuntuación media de los participantes del grupo experimental en bienestar psicológico y satisfacción vital, mientras queno se observaron cambios en el grupo control, mejoras que se mantuvieron 12 meses después de la intervención. Esteestudio sugiere que la inclusión de un programa global de envejecimiento activo en residencias para personas mayores quecontemple medidas para impulsar el empoderamiento, la participación y la apertura social contribuye al mantenimientodel bienestar percibido.
Keywords
Psychological well-being, Life satisfaction, Nursing homes, Active agingPalabras clave
Bienestar psicolĂłgico, SatisfacciĂłn vital, Residencias, Envejecimiento activoCite this article as: Buedo-Guirado, C., Rubio, L., Dumitrache, C. G., & Romero-Coronado, J. (2020). Active Aging Program in Nursing Homes: Effects on Psychological Well-being and Life Satisfaction. Psychosocial Intervention, 29(1), 49 - 57. https://doi.org/10.5093/pi2019a18
lrrubio@ugr.es Correspondence: lrrubio@ugr.es (L. Rubio).As a consequence of the increase in life expectancy the improvement of the quality of life and well-being of the aging population has become an important goal. Bearing this in mind, the World Health Organization (2002) proposed the term of active aging, defining it as “the process of optimizing opportunities for health, participation, and security in order to enhance quality of life as people age” (p. 12). According to the WHO (2002), active aging implies maintaining autonomy, independence, and quality of life, and participating in all spheres of life, that is, participating in the social, civic, economic, and spiritual spheres of life (Caprara, 2008). Finally, lifelong learning is proposed as another component of active aging (WHO, 2015), given its positive implications during the entire life cycle and also at older ages (Fernández-Ballesteros, Molina, Schettini, & Del Rey, 2012). For Paúl, Teixeira, and Ribeiro (2017) active aging comprises different determinants, namely, availability and use of health and social services, behavioral and personal determinants, physical environment, and social and economic determinants. According to Paúl et al. (2017) the definition of active aging has been adopted by many countries that have developed their aging polices based on the recommendations made by the WHO. As Zaidi and Howse (2017) underline, this might be due to the fact that the active aging paradigm was proposed with the intention to mirror the values that should outline and support policies aimed at promoting well-being in later life. According to these authors, by maintaining health and functional ability we can maintain well-being and also ensure older adults’ engagement in social life and participation in productive activities. With respect to maintaining well-being, active aging promotes both subjective and psychological well-being. Subjective well-being can be defined as a positive orientation towards own life (Ní Mhaoláin et al., 2012), and includes several components, such as positive affective balance, with high positive affect and lower negative affect, and life satisfaction (Diener, 1984), defined as a global assessment that people carry out of their lives (Caprara, Steca, Alessandri, Abela, & McWhinnie, 2010). Marsillas et al. (2017) found that active aging, conceptualized as a higher-order construct that comprises physical, psychological, and social health, functional status, leisure activities, social participation, employment, and lifelong learning, is positively linked to life satisfaction and explained 27 percent of variance in life satisfaction. Previous studies have shown that the different components of active aging, such as health, lifelong learning, or social participation, are important life satisfaction correlates (Jenkins, & Mostafa, 2015; Karata & Duyan, 2008; Zhang & Zhang, 2015). Thus, active aging promotes life satisfaction, which is decisive for reducing the prevalence of disability and morbidity (Mendoza-Ruvalcaba & Arias-Merino, 2015; Woo, Leung, & Zhang, 2016). Furthermore, health or social participation are also linked to psychological well-being (Ho, 2017; Minagawa & Saito, 2015; Steptoe, Deaton, & Stone, 2015). Psychological well-being refers to the development of human potential and own capacities and to personal growth, and is an indicator of positive psychological functioning (Ryff, 1989). This perspective is based on the life span developmental theory that postulates that, by overcoming different developmental challenges, individuals achieve personal growth and psychological development (Ryff, 1989). A six-component structure of psychological well-being is considered in this research: self-acceptance, positive relationships with others, autonomy, environmental mastery, purpose in life, and personal growth (Ryff, 1989). On one hand, self-acceptance, purpose in life, and personal growth constitute positive attitudes towards oneself and allow us to ascertain how individuals perceive themselves and their decisions (Ryff, 1989). They could be indicators that individuals have a positive view of their past, which constitutes a source of learning. In a study by Windsor, Curtis, and Luszcz (2015) higher sense of purpose was associated with lower levels of disability, better cognitive functioning, a more positive assessment of self-rated health, and a lower level of depressive symptoms. On the other hand, autonomy and environmental mastery refer to the ability of being independent, to adjust one’s criteria and to control the available resources in order to satisfy one’s needs (Ryff, 1989). Thus, activities included in active aging programs might be in agreement with participants’ interests and motivations. Also, enjoyment of life and acceptance of change are the essential criteria for psychological well-being, mental health, and successful aging (Kasser & Ryan, 1999; Ryff, 1989). The positive relations dimension refers to individuals’ perception of available close social relations (Ryff, 1989). In this sense, establishing new social and meaningful social relations and maintaining social network prior to institutionalization are essential in nursing home interventions to promote well-being (Park, 2009). Under the paradigm of active aging, a wide range of activities and programs have been proposed, aimed at preserving the autonomy and independence of older people for as long as possible. These programs focus on promoting older adults’ well-being and on investigating factors that are related to active aging. Initiatives carried out to promote active aging include programs such as Vivir con vitalidad (Fernández-Ballesteros, Caprara, Iñiguez, & García, 2005), California Active Aging Community Grant Program (Hooker et al., 2005), Soy activo (Mendoza-Ruvalcaba & Arias-Merino, 2015), and Program for Active Aging and Community Engagement (Foy et al., 2013), which demonstrate improvement in domains such as physical and cognitive functioning, nutrition, and quality of life. Nevertheless, despite the aforementioned initiatives, a large sector of the older population has difficulty accessing the programs on offer, namely, institutionalized older people. On occasion, institutionalization is associated with a loss of physical and mental functionality, which is a barrier to active aging (Fernández-Mayoralas et al., 2015). Furthermore, it is rare for nursing homes to offer comprehensive and global active aging opportunities and the chance for residents to participate in society. In this respect, a recent systematic review of intervention programs aimed at improving well-being of institutionalized older people carried out in long-term care facilities shows that a large percentage of such interventions are limited active aging programs focused on improving physical or cognitive functioning (Van Malderen, Met, & Gorus, 2013) while they overlook social participation and lifelong learning domains. Likewise, a study on well-being in residential settings conducted by Ors and Maciá (2013) demonstrates that close relationships and relationships with family and social ties prior to admission were not covered after institutionalization; scheduled activities did not promote residents’ autonomy or initiative, nor did such actions generate sense of belonging to a group (Ors & Maciá, 2013). Participants also reported that they felt, to a certain extent, that they had been stripped of their personal or group initiative and demanded a program of activities more in line with their interests (Ors & Maciá, 2013). Another more recent study showed how institutionalized older people benefited emotionally from a healthy aging program (Jiménez, Izal, & Montorio, 2016). The group that participated in the healthy aging program had an increased level of affect balance and of positive affectivity, with high levels of happiness, and a decrease in the average negative affect score, with reduced levels of concern (Jiménez et al., 2016). Institutionalized people who maintain a high level of activity and participation have been found to usually have a greater level of cognitive functioning and a better perceived health status (Fernández-Mayoralas et al., 2015). Furthermore, taking into account that social participation is one of the cornerstones of active aging, it is vital for programs that promote active aging to be comprehensive and to include activities that encourage active participation of those living in care facilities, something that is not done in the active aging programs that are currently being applied in nursing homes. Besides this, active aging programs in residential settings are limited and usually are pilot tests that are not ultimately incorporated into residential facilities. Furthermore, no follow-up is made of results months after having carried out the intervention. It is therefore impossible to ascertain whether the observed effect last on the long term. Thus, as indicated by Caprara et al. (2013), more efforts should be devoted to designing and implementing intervention programs aimed at institutionalized older people. Based on this, the objective of this study was to analyze the impact of a comprehensive active aging program on the psychological well-being and life satisfaction of a sample of institutionalized older people, compared to a traditional limited active aging program, and, furthermore, to evaluate whether positive effects were maintained twelve months after having finalized the intervention. Participants The sample of this study consisted of 141 people with ages between 60 and 100 years-old, with a mean age of 85.50 (SD = 8.47). Due to the characteristics of this study, a non-probabilistic consecutive sampling was employed, in which participants were selected according to two inclusion criteria that were established at the outset: being physically capable of carrying out the activities (thus they were autonomous for performing activities that required the upper body even though they needed to use a wheelchair to get about) and maintaining the cognitive ability to answer to questions included in the instruments used in this study. Due to it, autonomous older people without disability or older people with disability caused by physical impairment (with limitations for example for washing or getting up from a seat) and with normal cognitive performance or with mild cognitive impairment took part in this study. In order to ascertain participants’ cognitive status, the Mini Mental State Examination (Folstein, Folstein, & McHugh, 1975; Lobo, Saz, & Marcos, 2002) was used. A minimum score of 20 points was needed for participants to take part in the study. All of the participants were institutionalized in a nursing home in the province of Madrid, Spain. This was a private nursing home with a capacity of 180 residents. Therefore, a 77.9% of the residents met the two inclusion criteria and were included in this study; the remaining 22.1% of the residents did not meet the inclusion criteria because they showed high cognitive impairment or physical limitations affecting the upper body or were bedridden. Regarding participants’ characteristics, the average time from their admission into the facility to the time of carrying out the project was 1.55 years (SD = 1.43). With regard to gender, 82.97% of the sample were women and 17.03% were men. The educational level was medium, only 2.1% was illiterate but could read and write, 41.8% of the participants had primary studies, 9.9% secondary studies, 16.3% high-school, and finally, 29.8% of the participants had college studies. Of the participants 25.5% were single, 17.7% were married, 5% divorced, and a high percentage were widowed (51.8%). The number of children oscillated between none and four (M = 2.30, SD = 1.33). In general, none of the participants had taken part in active aging activities or programs before their admission into the facility. Participants’ functional status had been assessed before institutionalization and the degrees of disability mentioned before were established according to the classification of the Spanish Act 39/2006, of 14th December, on the Promotion of Personal Autonomy and Care for Dependent Persons (Act 39/2006, 2006). According to this act, dependent individuals are classified according to their severity in three grades: grade I or moderate dependence, grade II or severe dependence, and grade III or extreme dependence. These grades refer to the limitations for carrying out basic daily-life activities that were caused either by cognitive or physical difficulties or both. In terms of autonomy, only 6.4% of participants in this study had full autonomy. Meanwhile, 47.5% of the participants had a grade III of dependency, 24.8% had a grade II of dependency, and 21.3% had a grade I of dependency. In this case participants were recognized the dependence degree mainly due to physical limitations, and had difficulties in getting up from a seat, with personal hygiene and had serious cognitive impairment. A pretest-posttest quasi-experimental design was employed for the implementation of the project, and the sample was divided into two groups: a control group formed by 68 people and an experimental group with 73 participants. Subjects assigned to the control group continued to participate in the general program provided by the nursing home, that is, geriatric exercise and cognitive stimulation through the use of worksheets and debates. The experimental group participated in the comprehensive active aging program during the development thereof. Instruments Psychological well-being. The Spanish adaptation of Ryff’s (1989) Psychological Well-Being Scales carried out by Díaz et al. (2006) was used. This instrument comprises 29 items grouped into six factors: self-acceptance (e.g., “In general, I feel confident and positive about myself”), positive relations (e.g., “I know that I can trust my friends, and they know they can trust me”), autonomy (e.g., “I am not afraid to voice my opinions, even when they are in opposition to the opinions of most people”), environmental mastery (e.g., “In general, I feel I am in charge of the situation in which I live”), personal growth (e.g., “I have the sense that I have developed a lot as a person over time”), and purpose in life (e.g., “I enjoy making plans for the future and working to make them come true”). Participants had to rate how strongly they agreed or disagreed with the items, using a Likert-type scale with six answer options (from 1 = completely disagree to 6 = completely agree). Internal consistency in the validation study to Spanish showed adequate Cronbach’s alpha values ranging between .70 and .84 (Díaz et al., 2006). In this study Cronbach’s alpha values were between .72 and .98. Likewise, its use with older people has been ratified in previous studies (Tomás, Meléndez, & Navarro, 2008). Life satisfaction. The Spanish adaptation of Diener’s Satisfaction with Life Scale (SWLS; Diener, Emmons, Larsen, & Griffin, 1985; adapted by Atienza, Pons, Balaguer, & García-Merita, 2000) was used. This questionnaire includes a total of five items (e.g., “In most ways my life is close to my ideal”) with five answer options (1 = totally agree to 5 = totally disagree). It has an extensive use because of its briefness, and the fact that it prevents possible fatigue and random answers in the older people surveyed. The psychometric properties of the Spanish version are adequate, with a Cronbach’s alpha value of .84 (Atienza et al., 2000). Reliability in this study was .98. Procedure After contacting the nursing home and obtaining their authorization, direct contact was made with the older people at the facility. For data collection, the ethical standards of the American Psychological Association (APA) were employed. Firstly, the objective and confidentiality of the study and the estimated duration of the interview were explained. Participants were then informed of its voluntary nature and of their right to finalize the interview or their participation. Upon concluding this initial agreement, participants signed their informed consent and face to face interviews were individually conducted. The interviewer read each question aloud and marked into the answer sheet participants’ answer; participants had “showcards” with the answer options for each scale. Following the initial collection of data, the program of activities was applied based on the cornerstones of active aging. To that end, the sample was subdivided into an experimental group (n = 73) that took part in the activities of this new comprehensive active aging program and a control group (n = 68) that continued to carry out the activities provided by the facility that could be considered a more limited active aging intervention program. Assignment to the control or experimental group was carried out voluntarily by the participants. The experimental group participated in the active aging program during a three-month period, with four-hour sessions each day dived into morning and afternoon activities from Monday to Friday and specific activities during the weekends. Over these months, ten activities that were related with the different active aging pillars (health, social participation, lifelong learning, and security throughout empowerment) were implemented and, in this way, psychological well-being and life satisfaction of those older people taking part in the activities were promoted. Due to the high number of participants, some of the activities were carried out individually, some were carried out in small groups that included between 15 to 20 participants, and some others were performed with all the participants. In the following section these activities are described and the number of participants that took part in each one is specified. In order to implement the intervention program, the researchers, together with 10 trained volunteers and the nursing home staff (psychologist, nurse, and 4 auxiliary nurses), cooperated to help the participants to move about if they needed it. The ten activities with their workshops are listed below.
During the three months when the program was conducted, the control group carried out the facility’s regular activities, a limited active aging program consisting of physical exercise and group-based cognitive stimulation through activities and exercises focused on memory, calculation, and concentration, among others. Such activities were carried out during group sessions with a board and written sheets and with the same daily duration as the activities of the experimental group. In order to determine whether there had been changes in participants’ psychological well-being and life satisfaction, once the intervention activities finished the instruments used in the initial evaluation were applied once again. Subsequently, twelve months after the program completion, the instruments were once again applied to evaluate whether the results obtained in the experimental group had been maintained over time. Data Analysis The SPSS 20 software was used for data analyses. For the general description of psychological well-being and life satisfaction levels in this sample, descriptive analyses were carried out. In order to ascertain that there were no differences between control and experimental groups and that the samples were homogeneous in terms of socio-demographic variables, the independent samples t-test and chi-square test were employed. To determine whether the intervention was effective, analyses of variance for repeated measures with Bonferroni correction were conducted. The main effects both on the pretest, on the posttest, and on the follow-up were evaluated, and the interaction was analyzed (group x time). To determine the effect size, the eta-squared statistic was employed and was interpreted in accordance with Cohen’s (1988) recommendations, whereby a value of .20 is considered a low effect size, .50 moderate effect, and .80 large effect. First, differences in socio-demographic variables between the control and experimental groups were analyzed (Table 1). No significant differences were found between the control and the experimental groups in terms of gender, X2(1) = 2.360, p = .124; age, t(139) = -.025, p = .980; educational level, X2(4) = 3.954, p = .412; or marital status X2(3) = 1.535, p = .674. Furthermore, no significant differences were found between control and experimental groups in the pretest scores of any of the study variables. Table 1 Pretreatment Differences in Sociodemographic and Studied Variables by Group 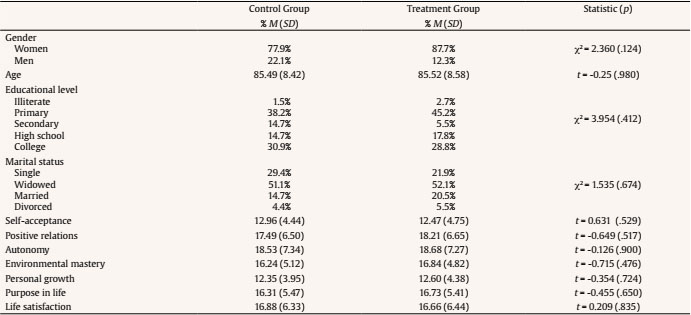 The main effects of the interaction were then analyzed, along with the simple effects on each of the periods of time, namely, pretest, posttest, and follow-up. The results of the main effects of the interaction are shown in Table 2. As it can be seen, significant differences were found in terms of group interaction and the period of time of the evaluation in all of the psychological well-being scales and also in participants’ life satisfaction. In all cases the effect size was moderate, ranging between .335 and .501. Table 2 Effects of Interaction and Group means for Analyzed Variables  Note. T1 = pretreatment scores; T2 = post treatment scores; T3 = follow-up scores. ***p < .001. As it can be seen in Table 3, the analysis of the simple effects showed that there were no significant differences between the scores of the control and the experimental groups before the implementation of the treatment. Table 3 Simple Effects between Groups in Every Evaluation Moment  ***p < .001. After applying the intervention program, differences were found in all the psychological scales scores and in life satisfaction, as Figure 1 conveys. In all the study variables, the experimental group obtained higher scores than the control group and the effect size was between low and moderate, with eta-squared values ranging between .238 and .364. Twelve months after finalizing the intervention, during the follow-up evaluation, the differences between the control group and the experimental group remained, and the scores continued to be higher in the experimental group. In this case, the effect size was slightly higher compared to the previous case, with eta-squared values ranging between .275 and .408. As it can be seen in Table 2 and Figure 1, the scores of the control group decreased progressively in the three periods of the time analyzed, with scores only recovering slightly in the purpose in life scale. Figure 1 Psychological Well-being and Life Satisfaction Scores by Group and Evaluation Moment. 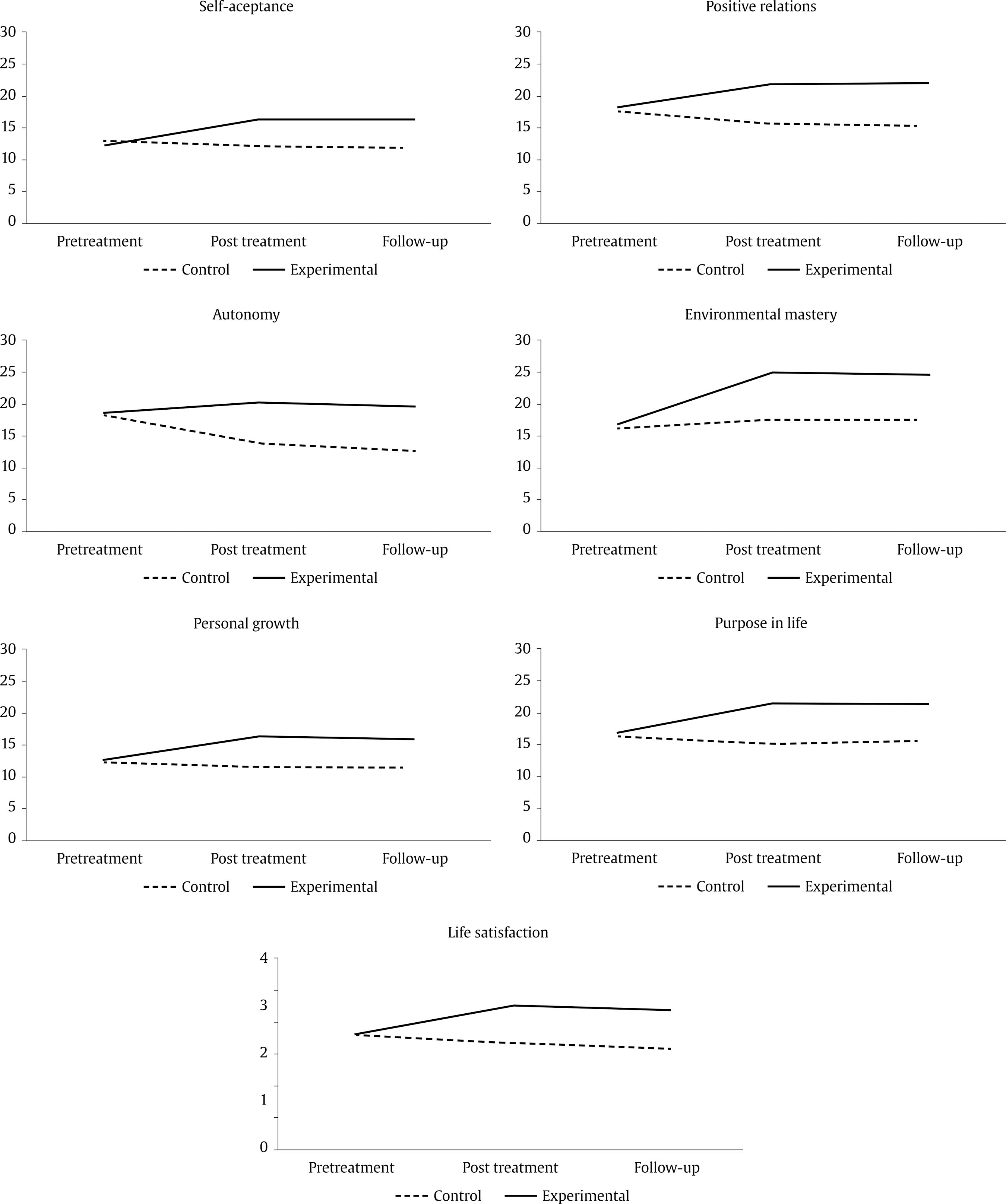 By contrast, after participating in the active aging program, the scores of the experimental group increased in all of the psychological well-being scales and also in the life satisfaction scale (see Figure 1). Subsequently, even after twelve months without receiving this intervention and once again taking part in the normal activities of the care-home facility, the scores of the experimental group in the study variables remained high, with a slight, though non statistically significant, decrease. Active aging plays an important role in older people’s perception of well-being and life satisfaction. It is a concept that has developed simultaneously and in relation with other concepts such as well-being, life satisfaction, and quality of life, having acquired a positive and proactive view of aging (Fernández-Ballesteros, 2009). Active aging acts as a determinant of perceived well-being, and, at the same time, it is decisive for reducing the prevalence of disability and the risk of morbidity in older people (Mendoza-Ruvalcaba & Arias-Merino, 2015; Woo et al., 2016). Among the range of strategies derived from the theoretical framework of active aging, social participation could be considered as one of the cornerstones to sustain older people’s quality of life and to maintain their psychological well-being and life satisfaction (Ho, 2017; Minagawa & Saito, 2015; Zhang & Zhang, 2015). To our knowledge, the literature on active aging programs implemented in care homes for older people is sparse. The majority of initiatives to promote active aging have been carried out with older people who live within the community (Fernández-Ballesteros et al., 2005; Foy et al., 2013; Hooker et al., 2005; Mendoza-Ruvalcaba & Arias-Merino, 2015). Likewise, the programs that have been implemented within care-homes do not usually include the social participation and participation within society of institutionalized older people (Van Malderen et al., 2013) and can be considered limited active aging activities that are mainly focused on improving physical or cognitive functioning. Furthermore, these programs do not monitor the effectiveness of these interventions. For this reason, in this study a comprehensive active aging program has been applied. This program included activities focused on cognitive stimulation and physical exercise to maintain the health of the participating older people, along with other activities to promote their leisure, contact with the environment, and their participation in workshops related to leisure, voluntary work activities, nature therapy and the press and media workshops. The results have been compared with a traditional and limited intervention based on physical and cognitive exercise. As a result of the application of the comprehensive active aging program, the experimental group displayed higher scores in life satisfaction and in all dimensions of psychological well-being. Such dimensions are self-acceptance, positive relations, autonomy, environmental mastery, personal growth, and purpose in life. By contrast, in the control group, or traditional intervention, the scores had decreased in all variables except for environmental mastery, which remained stable. The traditional activities offered in the care facility are geriatric exercise and cognitive stimulation, an intervention similar to that offered in most nursing homes in Spain. Although the aim of both activities is to maintain autonomy and health, they do not promote social relations between residents nor lifelong learning, and they do not encourage people to develop new goals in life after admission into the facility. Furthermore, they do not focus on the individual interests of residents, but rather limit their capacity to decide on the activities to be carried out (Ors & Maciá, 2013). Results of previous studies carried out with community-dwelling older adults show that social participation and lifelong learning are linked with life satisfaction, psychological well-being, quality of life, and a lower risk of mortality (Jenkins, & Mostafa, 2015; Marsillas et al., 2017; Minagawa & Saito, 2015; Zhang & Zhang, 2015). This would explain why participants in the control group, who took part in a limited active aging intervention program that does not promote social participation and lifelong learning, did not increase or maintain their levels of psychological well-being and life satisfaction. By contrast, activities proposed for the experimental group enable older people to participate in society. The participants of this study could decide themselves on activities to be carried out in the leisure workshop. Taking part in creative and leisure activities as well as physical activity is an important component of active aging and is associated with higher life satisfaction (Marsillas et al., 2017; Zhang, Feng, Lacanienta, & Zhen, 2017). Likewise, participants in the experimental group created useful products that could be sold for charity reasons or given as gifts. Previous research shows that voluntary work, such as the ones included in this comprehensive active aging program, promote a strong sense of meaning and personal growth, thus they have a positive influence on older adults’ psychological well-being and life satisfaction (Hansen, Aartsen, Slagsvold, & Deindl, 2018; Ho, 2017; Pilkington, Windsor, & Crisp, 2012). On the other hand, some of the activities included in the intervention program had an educational dimension, another of the active aging pillar, that is associated with higher levels of psychological well-being and life satisfaction (Hammond, 2004; Jenkins & Mostafa, 2015; Marsillas et al., 2017; Yamashita, López, Stevens, & Keene, 2017). Finally, the activities carried out also increased social contact between the participants and actively promoted the importance of social support to cope with changes and losses, which ultimately encouraged them to participate and seek social support. Social participation was found to be linked to life satisfaction (Pilkington et al., 2012). This effect is mediated by social support (Li, Jiang, Li, & Zhang, 2018); higher social participation promotes higher social support, which in turn results in higher life satisfaction (Li et al., 2018). Taking all this into consideration, it was expected for the scores in psychological well-being scales and life satisfaction to increase within the experimental group after participating in this type of activities. Subsequently, twelve months after applying the active aging program, follow-up was conducted to evaluate the maintenance of the improvements observed in the experimental group in terms of psychological well-being and life satisfaction. In the experimental group, it was found that all of the variables analyzed maintained their scores, with very small and non-significant declines. However, in the control group the scores continued to decrease with respect to the pretest and posttest scores. Therefore, the activities carried out during the active aging program were successful in bringing about a marked change in participants’ well-being, a change that remained one year after having finalized the program. It is possible that the relationships of support formed between the participants were sustained and that the skills acquired in the new technologies workshop continued to facilitate their social participation for some time after, which in turn resulted in the maintenance of the improvements we found. Although this study has proved to be effective in increasing institutionalized older adults’ psychological well-being and life satisfaction, it does have certain limitations. One such limitation is related to the sampling technique used to select the sample. An intentional and non-random sampling was used, which leads to the risk that people with a more participative and positive profiles have been included in the active aging program. Furthermore, other positive factors such as initiative, social openness, optimism, and physical circumstances could have influenced the results obtained after applying the program, and these factors have not been taken into account. In future studies these variables should be evaluated and their effect removed upon analyzing the effectiveness of the program. Also, the sample of the present study was very heterogenous in terms of participants’ age range, generational experience, and physical autonomy/disability, thus it is difficult to ascertain how this program might influence different groups of older people. Future studies should test the effect of this intervention program with specific groups of older adults such as 80 year-old and older people and compare the results of this program when applied with people with ages ranging from 65 to 79 years old. Likewise, it would be interesting to apply the intervention program with people with a high level of disability and to compare them with people with a low and medium level of disability. Another limitation of this study is the fact that participants of this study only belonged to a single care home. Residents from other nursing homes might have a different profile. Due to it, the results of this study might not apply to the general Spanish population of institutionalized older adults. However, given that the profile of older people living in care facilities is usually of greater dependence than people living at home, it was impossible to find another facility in which a sample of similar characteristics and with a significant number of participants could take part. Therefore, for future studies it is necessary to expand the sample to analyze the effect at other facilities and even with different profiles of dependence. It would also be important to analyze the influence of the number of sessions on the effectiveness of the program following application and in the long run. In this study, the program was applied for three months with daily sessions. Thus, it would be important to determine whether an increased number of sessions would improve the results or whether there is a maximum number after which an increased effect cannot be observed. Despite these limitations, this is one of the first active aging comprehensive, systematized, and global program to be carried out with institutionalized older people in the Spanish context. Likewise, it is important to point out that it reported improvements in participants’ psychological well-being and life satisfaction and, particularly, that the results were subject to follow-up. This study also highlights the importance of including systematized active aging activities when caring institutionalized older people, comparing its effectiveness with the traditional active aging programs currently applied in nursing homes and limited to cognitive stimulation and physical exercise. This study shows that the implementation of a comprehensive active aging program based of the four pillars of active aging has beneficial effects on psychological well-being and life satisfaction, and this effect remain stable one year later, in spite of participants’ return to the traditional activities of the nursing home. Thus, traditional active aging activities currently implemented in nursing homes must also address participation and contact with society through activities based on openness to the community, empowerment, social participation, and development of positive social relations. This global vision in active aging intervention could be the key element to improving the situation of institutionalized older people, promoting their empowerment and life satisfaction, and strengthening their self-esteem and psychological well-being. Conflict of Interest The authors of this article declare no conflict of interest. Cite this article as: Buedo-Guirado, C., Rubio, L., Dumitrache, C. G., & Romero-Coronado, J. (2020). Active aging program in nursing homes: Effects on psychological well-being andlife satisfaction. Psychosocial Intervention, 29, 49-57. https://doi.org/10.5093/pi2019a18 |
Cite this article as: Buedo-Guirado, C., Rubio, L., Dumitrache, C. G., & Romero-Coronado, J. (2020). Active Aging Program in Nursing Homes: Effects on Psychological Well-being and Life Satisfaction. Psychosocial Intervention, 29(1), 49 - 57. https://doi.org/10.5093/pi2019a18
lrrubio@ugr.es Correspondence: lrrubio@ugr.es (L. Rubio).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
Send






