


Special Issue: Treatment Resistant Perpetrators of Intimate Partner Violence: Research Advances
Systematic Investigation of Meta-Analysis Data on Treatment Effectiveness for Physical, Psychological, and Sexual Intimate Partner Violence Perpetration
[Investigaci├│n sistem├ítica de los datos de meta-an├ílisis sobre la eficacia del tratamiento de la agresi├│n de pareja f├şsica, psicol├│gica y sexual]
Çerağ Oğuztüzün, Mehmet Koyutürk, and Günnur Karakurt
Case Western Reserve University, Cleveland, Ohio, USA
https://doi.org/10.5093/pi2023a6
Received 30 August 2022, Accepted 18 February 2023
Abstract
Intimate partner violence can lead to physical, economical, mental, and sexual well-being issues, and even death, and it is most commonly experienced by women. There exist a number of treatment models for the prevention and treatment of intimate partner violence (IPV). In this study, we provided a comprehensive meta-regression analysis of the effectiveness of batterer treatment programs, with a view to characterizing the interplay between different forms of IPV (physical, psychological, and sexual). Using meta-regression, we explore the effect sizes and whether IPV treatment methods have distinct impacts on the outcomes. We use the difference normalized by pretreatment mean and variance foldchange to uncover the relationship between different violence subtypes and how they drive each other. Specifically, our study found that studies with more pre-treatment psychological and/or sexual violence, lead to less favorable outcomes while the studies that start with more physical violence are able to demonstrate their effects more effectively. Results of this study can be used to help the clinician effectively select the treatment for the perpetrator based on the violence type and severity of violence in order to more effectively treat the needs for each specific relationship.
Resumen
La violencia de pareja puede llegar a afectar al bienestar físico, económico, mental y sexual e incluso llevar a la muerte, siendo experimentada con más frecuencia por las mujeres. Hay diversos modelos de prevención y tratamiento de la violencia de pareja (VP). En este estudio se lleva a cabo un análisis global de meta-regresión de la eficacia de los programas de tratamiento para maltratadores centrado en caracterizar la interacción entre diferentes formas de VP (física, psicológica y sexual). Mediante meta-regresión se explora el tamaño del efecto y si los distintos métodos de tratamiento de la VP influyen de modo distinto en los resultados. Se utiliza la diferencia normalizada por la media y la reducción de la heterogeneidad (varianza) del pretratamiento para analizar la relación entre los distintos tipos de violencia y cómo se influyen mutuamente. En concreto en este trabajo encontramos que los estudios con más violencia psicológica y/o sexual en el pretratamiento tienen resultados menos favorables, mientras que los que comienzan con más violencia física pueden demostrar sus efectos de un modo más eficaz. Los resultados de este estudio pueden ser de ayuda para que el profesional seleccione de modo más eficaz el tratamiento para el agresor teniendo en cuenta el tipo de violencia y su gravedad, con el fin de tratar de forma más adecuada las necesidades de cada relación específica.
Keywords
Intimate partner violence, Meta-analysis, Meta-regression, Psychological abuse, Emotional abuse, Physical abuse, Sexual abusePalabras clave
Violencia de pareja, Meta-an├ílisis, Meta-regresi├│n, Abuso psicol├│gico, Abuso emocional, Abuso f├şsico, Abuso sexualCite this article as: Oğuztüzün, Ç., Koyutürk, M., & Karakurt, G. (2023). Systematic Investigation of Meta-Analysis Data on Treatment Effectiveness for Physical, Psychological, and Sexual Intimate Partner Violence Perpetration. Psychosocial Intervention, 32(2), 59 - 68. https://doi.org/10.5093/pi2023a6
Violence against women in relationships is a pervasive problem globally. It is an endemic public health crisis that has devastating effects on individuals, families, and their communities (Jewkes et al., 2017; Sorenson et al., 2021; United Nations, n.d.). Intimate partner violence (IPV) can be defined as any form of physical, sexual, emotional, and economic abuse perpetrated by a current or previous intimate partner (Breding et al., 2015). It also includes stalking behaviors (Breiding et al., 2015). According to World Health Organization (WHO), at least one out of every three women around the world has been beaten, coerced into sex, or otherwise abused in her lifetime (Gibbs et al., 2020; Sardinha et al., 2022; WHO, 2013, 2021). According to Center for Disease Control (CDC) data, women are more likely than men to experience severe violence by an intimate partner (24 percent) in their lifetime and the rates are lower, but still significant, with approximately one in seven men reporting severe violence by an intimate partner (14 percent) (Basile et al., 2011). IPV can affect a victim’s mental (Dillon et al., 2013; Trevillion et al., 2012), physical (Dillon et al., 2013), and sexual health (Dillon et al., 2013) and it can also lead to death due to homicide and suicide (Oram et al., 2022; Potter et al., 2021). Acute, chronic, and long-term consequences of IPV are commonly observed (Karakurt et al., 2017; Whiting et al., 2017). In addition, traumatic brain injury is frequently observed since physical violence often involves an attack on the face and neck of the victims (Karakurt et al., 2021). Numerous treatment programs are developed to prevent further violence and improve safety in relationships since the recognition of IPV as a detrimental social problem in the late 60s (Eckhardt et al., 2013; Gondolf, 2002). IPV is traditionally treated with Duluth model approaches utilizing the feminist sociocultural perspectives (Pence et al., 1993). Duluth model interventions emphasize re-education of batterers with the goal of guiding the perpetrators toward a more egalitarian relationship with women (Gondolf, 2002). Treatments through justice systems, including probation and case management, were also used frequently (Dunford, 2000; Peterson, 2008). Furthermore, various therapeutic approaches such as (i) psychodynamic approaches through narrative processing of traumatic memories of perpetrators (Lawson et al., 2012; Saunders, 1996), (ii) supportive group therapy for IPV perpetrators (Morrel et al., 2003), (iii) cognitive-behavioral approaches focusing on changing hostile cognitive biases (Murphy et al., 2020; Wexler, 2020), (iv) standardized treatments addressing skill deficiencies in problem-solving and communication skills (Webermann et al., 2022), and (v) action-based approaches replacing avoidance and denial with acceptance and commitment to change were implemented within all-male perpetrators (Zarling & Russell, 2022). However, the effectiveness of some of these approaches, particularly widespread Duluth-based approaches, has been yielding mixed findings (Babcock et al., 2004; Feder & Wilson, 2005; Karakurt et al., 2019; Miller et al., 2013). In order to improve the treatment outcomes, researchers started shifting from one-size-fits-all approaches to more personalized treatments based on the needs of the perpetrators in recent years (Labarre et al., 2019; Travers et al., 2021). Specifically, factors affecting treatment disparities, preparedness to change violent behaviors, and co-occurring mental health concerns have been gaining attention in identifying the treatment needs of the perpetrators (Butters et al., 2021). In recent years, combining multiple treatments was also started gaining attraction to address co-occurring issues among perpetrators (Butters et al., 2021). More specifically, such efforts concentrate on substance abuse and trauma issues to augment IPV treatments (Meyer et al., 2020). Furthermore, motivational enhancement techniques are also utilized as a preclude approach to improving preparedness to change, and to lessening resistance and high dropout rates during the treatment process (Lila et al., 2018; Santirso et al., 2020). Understanding the effectiveness of IPV treatment strategies is important for reducing its effects. Through subgroup analysis, it is possible to identify treatment groups that assist perpetrators in responding well to different violence subtypes. In this project, we evaluated the effects of treatment on physical, psychological, and sexual subtypes of violence. Our aim is to characterize the effectiveness of different treatment models by investigating the physical, emotional, and sexual dimensions of relationship violence. Intimate partner violence (IPV) is analyzed using meta-regression to examine the relationship between treatment outcome and treatment. In addition to the environmental nature of these associations, meta-regression also presents a number of other challenges: 1) not every study measures every treatment in its group and 2) variable distributions and ranges differ drastically between studies, making comparisons difficult. In the following subsections, we describe our meta-analysis dataset and how we address these challenges. Description of Data A set of studies listed in Table 1 were used previously as part of our meta-analysis on the treatment of IPV perpetrators (Karakurt et al., 2019). The 16 studies were screened between 1997 and 2018 according to inclusion and exclusion criteria. Among these criteria were the use of a treatment, the reporting of pre- and post-test outcomes, and the use of the Conflict Tactics Scale (CTS) (Straus et al., 1996). Karakurt et al. present detailed study criteria in their 2019 article (Karakurt et al., 2019). Table 1 List of Studies on the Treatment Variables of IPV Perpetrators Used in our Analyses. 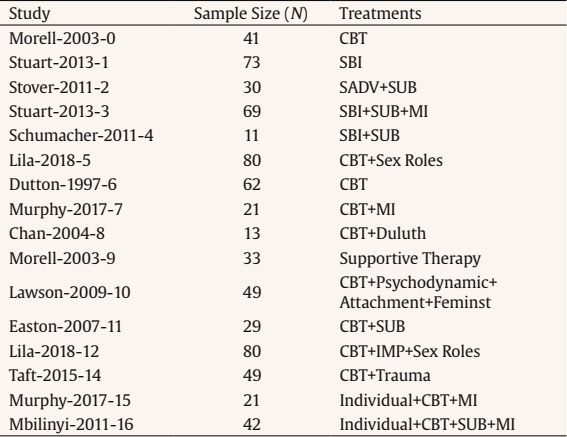 Note. CBT = cognitive behavioral therapy; SBI = standard battered intervention; SADV = standardized violence treatment; SUB = substance abuse treatment; MI = motivational treatment; IMP = Individualized Motivational Plan. Five hundred ninety eight studies published from 2018 to 2022 in PubMed (n = 255) (PubMed, n.d.) , PsycINFO (n = 413) (PsycINFO, n.d.), and Cochrane (n = 18) (Cochrane Library, n.d.) were identified and evaluated based on the same criteria. Among the 598 citations, 530 were excluded for not being related to the treatment of IPV perpetrators. Among the remaining 38 citations, 25 were excluded since the sample does not include IPV perpetrators. Among the 13 articles that remained reviewed, outcomes were unclear (n = 3), the sample included both males and females (n = 3), did not have usable data (did not report mean and standard deviation, n = 3), studies did not use behavioral assessment (n = 2), and studies which are already using and reporting follow up data (n = 2). Any of the studies published since 2018 did not meet the inclusion criteria. Each study’s treatments are presented in Table 1. Handling Missing Data We use meta-regression for our objective to assess the relationship between treatment effectiveness and the treatments with respect to different violence subtypes in the scope of treatment of IPV, at the study level. Table 1 illustrates that the treatment methods differ drastically among studies. Toward this end, we developed a two-armed approach that aims to combine all data available, while also accounting for the effects of data imputation. The two-armed approach starts by exporting the data from all studies on the treatment of perpetrators of IPV. First, we remove the studies with missing outcome variables which are pre-treatment and post-treatment mean and variance of violence as measured by CTS. Subsequently, using these studies, we use two meta-regression models for treatment and violence subtype variables to compute each of their “effect sizes”. When fitting a “full model”, the missing values are imputed using k-nearest neighborhood imputation with k = 5 (Mucherino et al., 2009). The resulting data is used in meta-regression to fit a full model for the outcome variable. During the analysis of the “individual model”, the studies without the independent variable are removed. Using the data from the remaining studies, for each treatment variable, a separate meta-regression is fitted with only the treatment variable of interest as an independent variable. We yielded two effect sizes for each independent variable, one for the full model and one for the individual model, based on the regression coefficients of the treatment and violence subtype variables. A standard meta-regression framework is used to calculate the associated statistics in addition to the effect sizes. When compared to individual models, full models are more informative since they assess the impact of each independent variable in combination with others. It is necessary to impute missing data in order to use all studies in the full model, but this can introduce noise and bias (Kang, 2013). For individual models, however, missing data imputation can be avoided, since only the studies that report the variable of interest can be used in the fit of the individual model. Hence, the simultaneous analysis of both variables gives us a better understanding of the association between each subtype of violence, treatments, and the outcome variable. Data Normalization and Wrangling for Meaningful Comparisons In Figure 1, we show the mean and standard deviation of violence reported by each study before and after treatment. It is difficult to draw meaningful comparisons between studies because these values vary greatly across studies, as shown in the figure. Figure 1 Computation of Outcome Variables and their Distribution across Studies.  Note. For each of physical, psychological, and sexual violence (from top to bottom), the left panel shows the pre-and post-treatment mean of the respective type of violence in each study (bottom left) and its standard deviation within each study (bottom right), difference normalized by pre-treatment mean (DNPM) for each study (top left) and variance fold change (VF) (top right). The right panel shows the histograms of DNPM (top, purple) and VF (bottom, blue) across studies. We use two outcome variables that capture the average relative improvement in violence and the reduction of violence heterogeneity in the study sample. For study k, we calculate the difference normalized by pre-treatment mean (DNPMk) as follows: The pretreatment meank and posttreatment meank are respectively the means of the pre-treatment and post-treatment violence across all study participants. Therefore, DNPMk reflects the relative average reduction in violence in study k, regardless of the degree of violence observed among participants. Because this measure does not take into account study heterogeneity, we propose an additional measure to determine how variances change between pre- and post-treatment. As a result, for study k we compute variance fold change (VFk) as follows: The standard deviation of violence pre- and post-treatment in the study is represented by PosttreatmentSDk and PretreatmentSDk respectively. In Figure 1, we present the normalized outcome variables difference normalized by pre-treatment mean (DNPM) and variance fold (VF) for each study. The figure illustrates how this transformation maps outcome variables to interpretable ranges so that the results of different studies are comparable. Assessment of The Effect of Treatment Factors To predict the observed effect sizes of studies, meta-regression models are used with study-level predictors. In meta-regression, an estimate of the effect size of studies that have never been analyzed before is derived from variations in predictor variables and observed effects. Meta-regression models included discrete predictors for the usage of treatment variables and continuous predictors of violence subtypes. Weighted least squares (WLS) is used to fit the meta-regression line, which ensures that studies with a smaller standard error are weighed more heavily. In the meta-analysis, the real effect sizes diverge less from an optimal regression line, suggesting that the predictor variable can explain some of the heterogeneity variances. According to the regression weight estimate, the effect size of a study is predicted to increase or decrease proportionately to the independent variable. As a result, we can observe the effects of treatments on outcome sizes, as well as their significance. In fitting the meta-regression models, we take into account the treatment distributions reported by each study. This analysis contains information at the level of averages, we are not looking to identify associations at the level of individuals which would be as: “This type of treatment is more effective for participants that are in the group which has a high average of pre-treatment psychological violence.” Rather than providing treatment-outcome correlations, meta-regression provides environmental information. As an example, “Studies enrolling participants with higher pre-treatment psychological violence have less reduction in violence on average.” In addition to defining the subtypes of violence and treatment variables, this information provides valuable insight into what goes unnoticed by the individual and what becomes more visible to the group. The formulaic description of our two-armed workflow: 1. By focusing on studies in which x(i) is the only “independent variable”, we compute an individual meta-regression model for each independent variable x(i). The independent variable is a continuous variable (the violence variables): where, yk : = the value of the outcome variable (DFNM or VF) in study k x(ki) : = the value of the predictor in study k (the fraction of a specific group in the study) βi(I) : = the regression coefficient for predictor x(i) ∈k and ζk : = the error terms α = the intercept value In the formula for categorical independent variables like treatment usage, the variables can be dummy-coded as: x(ki) is replaced with Tk. The formula (3) for these independent variables are formulated as: 2. Using k-nearest neighbor imputation (Mucherino et al., 2009), we fill in the missing data and calculate a “full meta-regression model” that includes all studies and includes all variables as independent variables: The formula (6) for categorical independent variables are formulated as: Figure 2 Meta-regression of Outcome Variables by Treatment Models.  Note. For each meta-regression, the treatments (dichotomous variable indicating whether the respective treatment was applied in the study) are shown on the left, the outcome variables are shown on the left, the width of the line connecting a treatment to an outcome variable indicates effect size (regression coefficient) and the color indicates its direction and significance (red means more reduction in violence). Individual models are shown on the left, full models are shown on the right. Results for difference normalized by pre-treatment mean (DNPM) are shown in the upper panel, and those for variance fold change (VF) are shown in the lower panel. CBT = cognitive behavioral therapy; SBI = standard battered intervention; SADV = standardized violence treatment; SUB = substance abuse treatment; MI = motivational treatment; IMP = Individualized Motivational Plan. We anticipate highly heterogeneous true effects across studies. Various differences exist between the studies we use, such as different target populations, different treatment lengths, different treatment intensities, etc. In order to account for the fact that individual studies vary not only due to sampling error alone, but also do so because they come from different populations, we used a random-effects model. The outputted effect sizes, in this case, will be based on the distribution of true effect sizes, and modeling will help estimate the mean. (τ2) is the variance of the distribution of true effect sizes. We use the Sidik-Jonkman estimator (Sidik & Jonkman, 2002) to estimate (τ2) because there is a high level of heterogeneity in our sample, and preventing false positives is very important. Outcome Variables In order to facilitate meaningful comparisons between different studies, we computed two normalized quantities that reflect treatment effectiveness: difference normalized by pretreatment mean (DNPM) and variance fold change (VF). Difference normalized by pretreatment mean thus it is a measure of the relative reduction in violence (as measured by the respective subscale of the Conflict Tactics Scale), negative meaning reduction in violence. Variance fold change is a measure of the reduction in the heterogeneity of the study group in terms of violence, negative meaning increase in homogeneity in the study. The relationship between these quantities and pre- and post-treatment mean/standard deviation for each study, as well as the resulting distributions of these quantities, are shown in Figure 1. Figure 3 Effect Sizes of Violence Variables 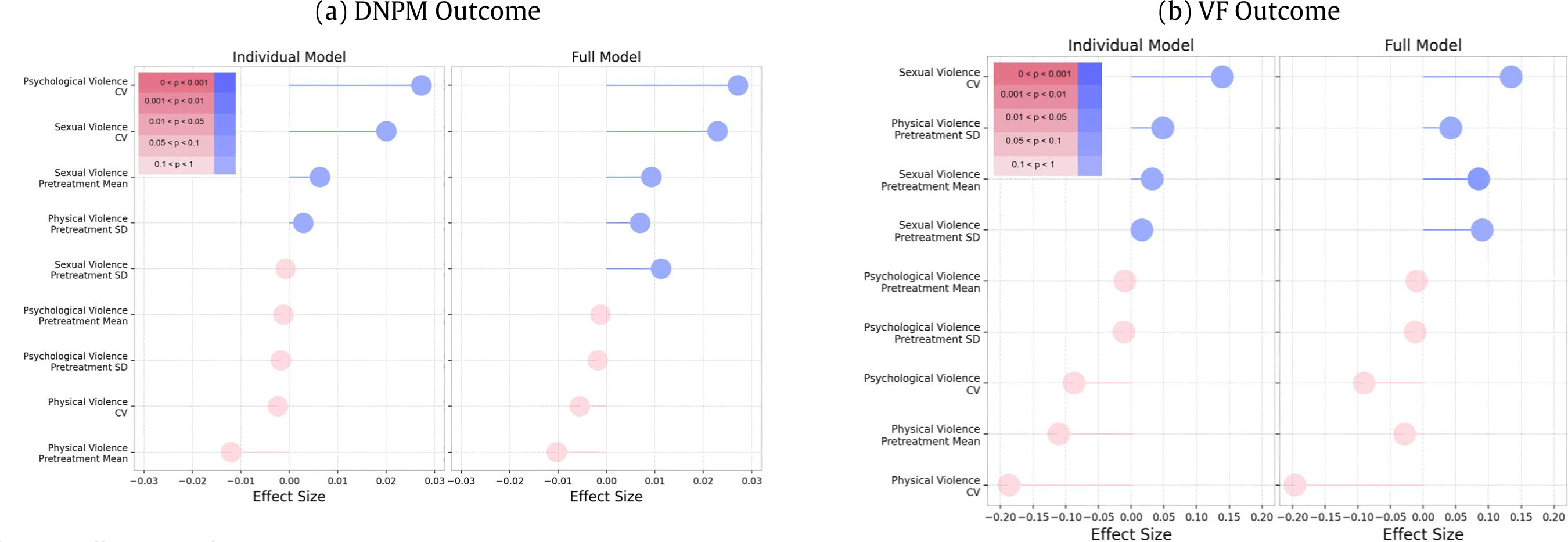 Note. CV = Coefficient of Variation. As seen in Figure 1, the pre-treatment mean and standard deviation for each violence type is quite variable across different studies. This makes it difficult to compare different studies to assess the effect of the treatment(s) applied in the study. The normalized measures of DNPM and VF, on the other hand, render these quantities comparable and capture the dynamic range of differences between studies. As seen in the histogram, the normalized reduction in mean violence seems to be higher (closer to -1.0) for most studies, while the reduction in psychological abuse is relatively modest (centered around -0.4). Relatively fewer studies reported results for sexual violence, thus the distribution for sexual violence is somewhat skewed, but we see that studies that report on sexual violence generally report a considerable reduction in sexual violence (4 out of 5 studies reporting more than 0.6 reductions). The reduction in the variance of physical violence is distributed almost uniformly across studies, suggesting the considerable discrepancy between different studies in terms of the reported reduction in the heterogeneity of the population. The reduction in heterogeneity is particularly low for psychological violence for most of the studies. Relationship between Treatment Models and Outcomes We first performed a meta-regression of outcome variables (separately for each violence type) by the treatment models. For this purpose, we represented each treatment model by a dichotomous variable, whose value was set to 1 if the study utilized the treatment and 0 otherwise. We then ran two meta-regression models: (i) an individual model in which only the corresponding treatment was entered into meta-regression, thereby quantifying the effect of the treatment directly, and (ii) a full model in which all treatment variables were entered into the model, thereby quantifying the effect of each treatment in the presence of others. The results of this analysis are shown in Figure 2. In the figure, the line connecting a treatment to a violence type shows the relationship between the treatment and the corresponding violence type (physical, psychological, and sexual), in terms of the respective outcome variable. The color indicates the significance of the effect size. The darker the color, the greater the significance. There is a positive effect size in blue for DNPM of violence subtypes, which indicates that violence increased, suggesting the variable is indirectly associated with the decline in violence. The violence decrease is indicated by the red color, which is beneficial. The blue color in the VF of violence subtypes indicates that the study has become more heterogeneous as a consequence of the independent variable. The red color, on the other hand, indicates a more homogeneous study. In the supplementary section (Figure A1 to A19), we used histograms to visualize the distribution of outcome variables across violence subtypes for the result of each meta-regression done for each treatment variable. Because our summary measurement is the standardized mean difference, the X axis of the histograms represents a variable’s effect on DNPM on violence subtypes of physical, psychological, and sexual violence across studies. As a result of eliminating studies with missing outcome variables, we eliminated studies where treatments were applied in some cases. Since there is only one subgroup for such treatments, the intercept value of a meta-regression is used as a result. Treatment Variables In Figure 2(a), we can see that IPV treatments such as sex roles, Individualized Motivational Plan (IMP), attachment, feminist, and psychodynamic failed to reduce physical violence. With the largest and most significant negative effect size, SADV is the most effective treatment for psychological violence, along with SUB, individual, and CBT+SUB. Duluth, SADV, and SUB are better treatments for sexual violence than CBT. In the case of negative effect sizes, imputation substantially increases the effect sizes, as shown by the difference between the effect sizes of individual and full models. In indirect proportion to the effect sizes regarding DNPM, IPV treatment results in more homogenous study participants (Figure 2). Violence Variables Figure 3 shows how the pre-treatment mean, pre-treatment standard deviation and CV coefficient Figure 4 Regression Slopes of Violence Variables’ DNPM Outcome according to the Individual Models (continued). 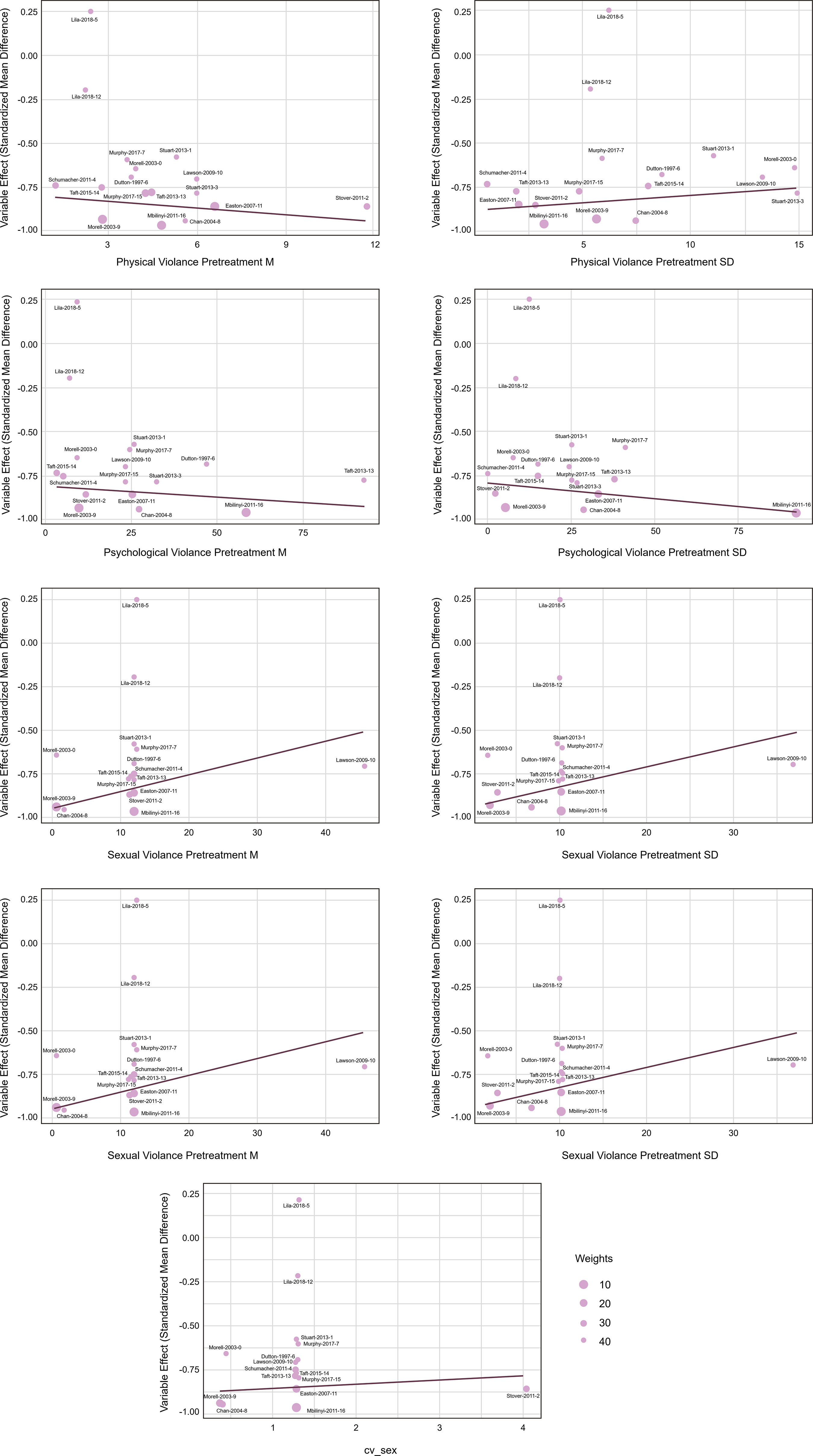 Note. See, Tables A1, A2, A3 (supplementary materials) for assessment of skewness for studies. As psychological violence standard deviation (pre-treatment) increases, the post-treatment homogeneity of the study group increases in Figure 3(b). However, as physical and sexual violence standard deviations (pre-treatment) increase, the study group is reported to get more heterogeneous in the post-treatment (Figure 4). Intimate partner violence (IPV) is a complex problem that intersects issues from the biological level to larger societal issues within couple and family systems. IPV is composed of aggressive and violent, physical, sexual, verbal, and psychological acts by an intimate partner. IPV sustained over time may be associated with lasting physical, behavioral, and cognitive consequences. Using meta-regression, we examined the type of violence that influences the effectiveness of treatments. Different studies work with different groups of participants and apply different combinations of treatment models in terms of the interventions they use, related co-morbidities such as substance use issues and trauma, and psycho-social outcomes. These multiple sources of heterogeneity within and between studies complicate meta-analyses that aim to carefully characterize the effectiveness of treatments. The current study examined the effect sizes and whether IPV treatment methods have distinct impacts on the outcomes. Our results showed that the effect of treatment on the study group can be better understood by taking into account the variance in violence pre-and post-treatment and the presence of type and severity of violence pre-treatment can have a significant effect on the effectiveness of treatment in reducing a different type of violence. Regarding the studies in Table 1, the study characteristics were not included in the meta-analysis due to incomplete partial information. We investigated 16 studies that collected data on physical violence as an outcome. Physical violence, defined as using physical force to harm, inflict injury, and cause death, includes specific behaviors such as pushing, kicking, hitting, and using weapons (Breiding et al., 2015). Our results indicated that for physical violence, supportive therapy, motivational interview (MI), individual cognitive behavioral therapy augmented with substance abuse treatment (CBT-SUB), substance abuse treatment augmented with a motivational interview (SUB-MI), standard battered intervention augmented with substance abuse treatment (SBI-SUB), and cognitive behavioral therapy augmented with motivational interviewing (CBT-MI) have negative regression coefficients meaning slightly higher levels of reduction in violence, but this effect appears to be quite modest. Additionally, some of these treatments contribute to a reduction in heterogeneity particularly, e.g., supportive therapies, cognitive behavioral therapy augmented with substance abuse (CBT-SUB), and substance abuse treatment augmented with a motivational interview (SUB-MI), while others are associated with an increase in heterogeneity motivational interviewing (MI), standard batterer intervention augmented with substance abuse treatment (SBI-SUB), suggesting that motivational interviewing (MI) and standard batterer intervention augmented with substance abuse (SBI-SUB) treatments may have different mechanisms of effectiveness and may be working differently in different groups. On average, the treatments for perpetrators of physical violence that utilized substance abuse, and standardized violence treatment (SADV) were found to be successful in terms of their approach of building skills, changing hostile cognitive distortions, and including substance abuse components in eliminating and diminishing physically aggressive behaviors toward their intimate partners. Similarly, motivational enhancement treatments (MI) also suggest having a differential mechanism for eliminating and reducing violence. Readiness to treatment and starting stage for change and resistance to treatment could be potentially the source of this heterogeneity. Our results also indicate that physical violence variance fold (VF) and physical violence pre-treatment mean have strong negative coefficients for overall treatment outcome (DNPM). This may be because the reduction in physical violence is more detectable, hence studies that start with more physical violence are able to demonstrate their effects more effectively. On another note, sex roles and IMP have strong positive coefficients for both DNPM and VF for physical violence, suggesting that these treatments are less effective on average than typical treatments for physical violence, while also increasing heterogeneity in the population. It is possible that they may be increasing violence in severe cases while reducing violence in less severe cases. Among the 16 studies, 11 of them reported data on psychological violence as an outcome. Psychological violence can be defined as verbal and non-verbal communication perpetrated in order to mentally and emotionally harm the intimate partner (Breiding et al., 2015). Identifying psychological violence can be challenging since it involves abusive situations that need contextualization due to the broad range of behaviors that can be vague (Breiding et al., 2015; Trinh Ha et al., 2022). Explosive anger, coercive control, degradation, isolation, and manipulation are a few of the behaviors considered psychological violence (Follingstad, 2009; Jacobson & Gottman, 1998). Our results indicated that for psychological abuse, SADV and SUB have negative regression coefficients for DNPM, i.e., appear to contribute the most to the reduction in violence, both individually as well as when other treatments are considered. This is regardless of the degree of psychological abuse at the beginning, as DNPM is normalized by the pre-treatment mean. These treatments also appear to contribute to the reduction in heterogeneity in the population, i.e., the perpetrators in the group perpetrate more similar levels of abuse post-treatment as compared to pre-treatment. Many of the treatments have a positive regression coefficient for psychological abuse, i.e., they are less effective than a typical treatment in reducing psychological abuse. These include SBI-SUB, IMP, attachment, sex roles, CBT, feminist, psychodynamic, supportive, and trauma. We observe a similar pattern in reducing heterogeneity, i.e., these treatments do not contribute to the reduction in heterogeneity in the population, hence they may be more effective for less severe psychological abuse cases. Psychological violence has the most positive effect size on overall treatment outcome (DNPM). This suggests that studies with more pre-treatment psychological violence might be linked to less favorable outcomes. There are not many studies – only four studies reported sexual violence as a distinct outcome in their treatment studies. Sexual violence in intimate relationships can be defined as sexual acts perpetrated either committed or attempted without the informed consent of the victim and/or despite their refusal (Breiding et al., 2015). These sexual acts include but are not limited to intentional unwanted sexual touching, pressuring for sex, and forced sex (Breiding et al., 2015; Straus et al., 1996). Our results on the limited number of studies on sexual violence showed that sexual violence CV has the most positive effect size on overall treatment outcome (DNPM). This suggests that studies with more pre-treatment sexual violence lead to less favorable outcomes. IPV can manifest itself in multiple patterns in relationships, including varying degrees of emotional, physical, and sexual violence. Analysis of nationally representative large data from participants across the United States indicated that while emotional and physical violence frequently co-occurs together, sexual violence tends to exhibit less co-occurrence with physical or emotional violence (Hacıaliefendioğlu et al., 2020). Unfortunately, many IPV treatments are designed specifically for eliminating physical violence, and some of these treatments also include some emotional abuse components such as coercive control issues in their treatment model; however, in our meta-analyses we did not come across any study that specifically targets sexual intimate partner violence. In addition, social (dis)advantage and health disparities are critical issues in the prevalence, treatment access, and supportive environment for preventing and treating IPV. The availability, accessibility, and extent of treatment services for offenders based on their needs call for it to be addressed by the larger systems, including judicial, health, and community services. The results of this study can inform clinical policies and programs to improve treatment decisions. Our aim was to investigate heterogeneity within and between studies to develop a more sophisticated understanding of treatment effectiveness for IPV perpetrators. Treatment models can be tailored to reflect the variability of violence in terms of the type of violence as well as the severity of violence in order to improve treatment outcomes. When individuals are able to get appropriate treatment for IPV, violence in their relationships will be reduced more quickly. It is critical to give special attention to distinctive emotional, sexual, and physical violence characteristics of the specific IPV perpetration and designing treatments to reflect this need. Limitations and Future Work The interpretation of our results is environmental as we can quantify effects only at the population level (e.g., average reduction and variance in the study population), thus the effects we observe at the environmental level can be opposite at the individual level. While this is a limitation of the current study, this also demonstrates the value of our results as the patterns we observe suggest effects that should be analyzed at the individual level to correctly characterize the relationship between pre-treatment violence, treatment model, and the type of violence at the individual level. Therefore, our study calls for more detailed data collection and analysis in studies on treatment effectiveness. The study focuses on the limitations of IPV studies including the lack of data and highlights the need for more individual-level data on IPV in the field in order to increase its efficacy. One of the highlights of our study is recognizing the limitations of the field and setting standards for publications of treatment effectiveness. Additionally, we believe judicial, health, and community services must address the availability, accessibility, and extent of treatment services for offenders based on their needs. We aim to conduct impactful research that is relevant to communities. Our research hopes to extend the treatment toolbox available to clinicians and policymakers. In summary, violence between intimate partners is a complex global public health crisis. Advanced and sophisticated methodological understanding is needed to investigate the complexity of IPV cases. Our results indicated that the type (physical, sexual, and psychological violence) and severity of IPV are critical in guiding treatment efforts and clinical decisions. Conflict of Interest The authors of this article declare no conflict of interest. Cite this article as: O uztüzün, Ç., Koyutürk, M., & Karakurt, G. (2023). Systematic investigation of meta-analysis data on treatment effectiveness for physical, psychological, and sexual intimate partner violence perpetration. Psychosocial Intervention, 32(2), 59-68. https://doi.org/10.5093/pi2023a6 Funding: This publication was made possible by US National Health Institutes (NIH) grant R01-LM012518 from the National Library of Medicine. Supplementary Data Supplementary data are available at https://doi.org/10.5093/pi2023a6 |
Cite this article as: Oğuztüzün, Ç., Koyutürk, M., & Karakurt, G. (2023). Systematic Investigation of Meta-Analysis Data on Treatment Effectiveness for Physical, Psychological, and Sexual Intimate Partner Violence Perpetration. Psychosocial Intervention, 32(2), 59 - 68. https://doi.org/10.5093/pi2023a6
Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB Supplementary files
Supplementary files CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
Psychosocial Intervention is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License







