


Special Issue: Treatment Resistant Perpetrators of Intimate Partner Violence: Research Advances
Neuropsychological Performance, Substance Misuse, and Recidivism in Intimate Partner Violence Perpetrators
[Rendimiento neuropsicol├│gico, abuso de sustancias y reincidencia en hombres penados por violencia contra la mujer en las relaciones de pareja]
Ángel Romero-Martínez1, Marisol Lila2, Carolina Sarrate-Costa1, Javier Comes-Fayos1, and Luis Moya-Albiol1
1Department of Psychobiology, University of Valencia; 2Department of Social Psychology, University of Valencia
https://doi.org/10.5093/pi2022a7
Received 1 November 2021, Accepted 8 February 2022
Abstract
Previous research has pointed out the importance of neuropsychological impairments in intimate partner violence (IPV) perpetrators for reoffending/recidivism once treatment ends. However, less is known about whether substance misuse is associated with impairments or deficits, which facilitate recidivism. In this study, we first aimed to assess whether IPV perpetrators with (n = 104) and without (n = 120) substance misuse showed differences in specific neuropsychological variables in comparison with non-violent men (n = 82). Second, we examined whether there were differences in IPV perpetrators’ recidivism and whether these differences were explained by neuropsychological performance. Our results revealed that IPV perpetrators with substance misuse showed worse cognitive performance than controls. Furthermore, we also found differences between IPV perpetrators without substance misuse and controls, but only in terms of executive functioning. There were no differences in neuropsychological performance between the two groups of IPV perpetrators, although those with substance misuse presented higher recidivism rates than those without substance misuse. Finally, cognitive flexibility, verbal fluency, and worse attention functioning were related to high recidivism in both groups of IPV perpetrators. This study underlies the importance of performing neuropsychological assessments during the initial stages of intervention programs for IPV perpetrators in order to design coadjutant neuropsychological/cognitive training to address not only the psychological needs (including substance misuse) of IPV perpetrators, but also their neuropsychological needs.
Resumen
La investigación previa ha puesto de manifiesto la importancia de los déficits neuropsicológicos para la reincidencia en los hombres penados por violencia contra la mujer en las relaciones de pareja (o maltratadores) una vez que han finalizado el tratamiento. Sin embargo, disponemos de un menor conocimiento sobre si el abuso de sustancias se relacionaría con los déficits neuropsicológicos, lo que, a su vez, facilitaría la reincidencia por parte de los maltratadores. Por lo tanto, el primer objetivo de este estudio fue el de analizar si existían diferencias entre un grupo de maltratadores con abuso de sustancias (n = 104) y otro sin consumo de sustancias (n = 120) en comparación con un grupo de hombres no violentos (n = 82). En segundo lugar, examinamos si existían diferencias en la reincidencia entre los grupos de maltratadores y si estas diferencias se explicaban por su funcionamiento neuropsicológico. Nuestros resultados pusieron de manifiesto que los maltratadores con abuso de sustancias mostraron un peor rendimiento cognitivo que los controles. Además, también encontramos diferencias entre el grupo de maltratadores sin abuso de sustancias y los controles, pero solo en las funciones ejecutivas. Del mismo modo, no hubo diferencias en el rendimiento neuropsicológico entre los dos grupos de maltratadores, aunque aquellos con abuso de sustancias presentaron tasas de reincidencia más altas que aquellos sin consumo de sustancias. Finalmente, la flexibilidad cognitiva, la fluidez verbal y el peor funcionamiento de la atención se relacionaron con una alta reincidencia en ambos grupos de maltratadores. Este estudio subraya la importancia de realizar evaluaciones neuropsicológicas durante las etapas iniciales de los programas de intervención para los maltratadores con el fin de diseñar programas neuropsicológicos o de entrenamiento cognitivo para abordar no solo las necesidades psicológicas (incluido el abuso de sustancias) de los maltratadores, sino también sus necesidades neuropsicológicas.
Keywords
Attention, Emotion decoding, Executive functioning, Intimate partner violence perpetrators, Recidivism, Substance misusePalabras clave
Atenci├│n, Decodificaci├│n de emociones, Funcionamiento ejecutivo, Maltratadores, Reincidencias, Abuso de sustanciasCite this article as: Romero-Martínez, Á., Lila, M., Sarrate-Costa, C., Comes-Fayos, J., & Moya-Albiol, L. (2023). Neuropsychological Performance, Substance Misuse, and Recidivism in Intimate Partner Violence Perpetrators. Psychosocial Intervention, 32(2), 69 - 77. https://doi.org/10.5093/pi2022a7
Correspondence: Angel.Romero@uv.es (├ü. Romero Mart├şnez).Studying underlying factors of intimate partner violence (IPV) perpetration might be crucial for developing better strategies to reduce and prevent it (World Health Organization, 2021). Research has paid attention to the effectiveness of intervention programs for IPV perpetrators (Arce et al., 2020; Santirso et al., 2020; Wilson et al., 2021) and characteristics of male IPV perpetrators. Specifically, important efforts have been made to analyze their profiles from social and/or clinical perspectives (Capaldi et al., 2012; Carbajosa et al., 2017; Catalá-Miñana et al., 2013; Catalá-Miñana et al., 2017; Expósito-Álvarez et al., 2021; Holtzworth-Munroe & Stuart, 1994; Lila et al., 2012; Wilson et al., 2014). Nevertheless, less is known regarding cognitive functioning of IPV perpetrators. Neuropsychology is a scientific discipline that seeks to link central nervous system functioning to cognition and behavior. A set of cognitive tests has been developed to assess the functioning of individuals, classifying them as statistically normative or not. The establishment of a normative distribution of neuropsychological abilities might make it possible to develop cognitive training programs designed to enhance the performance of individuals who score below average (Goldberg, 2019). Three reviews indicated that IPV perpetrators tend to present significant cognitive alterations, especially executive function impairments (Horne et al., 2020; Humenik et al., 2020; Romero-Martínez & Moya-Albiol, 2013). According to Lezak (1995), these cognitive processes could be defined as the essential mental capacities that are needed to carry out effective and creative behaviors which are socially accepted. Although there has been an extensive debate regarding which cognitive abilities are included in executive functioning, the main processes are adaptable or flexible thinking (e.g., switching ability and low perseverations after receiving negative feedback regarding performance, rule detection), planning abilities (e.g., sequencing, monitoring, strategy allocation), inhibitory control (e.g., for verbal and non-verbal stimulus), and decision making (Chan et al., 2008). These cognitive processes directly affect self-regulation or goal-directed behavior and social competence given that they are related to inhibiting irrelevant information, constantly adapting to environmental demands, top-down control of attention, suppression of rumination processes, and decision making based on contemplating future consequences (Goldstein & Naglieri, 2014; Hofman et al., 2012). To understand the correct interpretation of social signals and to act consequently with social adaptive behaviors, it is important to understand the interrelationships between executive functioning and other relevant processes such as decoding emotional facial expressions (e.g., measured with the eyes test). The existence of a link between both processes has been suggested, given that patients with neurodegenerative diseases and neurological conditions tend to present concurrent impairments in both, while preserving other cognitive processes (Aboulafia-Brakha et al., 2011; Wade et al., 2018). However, less is clear about which specific executive functioning subdomain maintains an association with the process of decoding emotional facial expressions (Wade et al., 2018). Regarding executive functioning in IPV perpetrators, research has pointed out that they tend to present reduced cognitive flexibility or score slightly below non-violent men (Horne et al., 2020; Humenik et al., 2020; Pinto et al., 2010; Romero-Martínez et al., 2013). Several studies, which employed different neuropsychological tests for measuring cognitive flexibility, concluded that IPV perpetrators’ performance was slightly below a comparison group (non-violent men) (Becerra-García, 2015; Easton et al., 2008; Romero-Martínez et al., 2013; Stanford et al., 2007; Walling et al., 2012). Low cognitive flexibility (or high mental rigidity) might underlie the maintenance of sexist roles and other cognitive schemas related to women (Romero-Martínez et al., 2013; Vitoria-Estruch et al., 2017). Furthermore, low cognitive flexibility also seems to be relevant in explaining, at least in part, the risk of IPV perpetrators’ recidivism (Romero-Martínez et al., 2016; Romero-Martínez, Lila, Gracia, et al., 2021). In addition to cognitive flexibility seemingly being altered in IPV perpetrators, certain dysfunctions have also been found in verbal fluency, planning abilities, and/or decision-making processes (Easton et al., 2008; Romero-Martínez et al., 2019; Romero-Martínez, Lila, Moya-Albiol, et al., 2021; Vitoria-Estruch et al., 2018). This poor functioning in high level cognitive processes might be at least partly explained by low inhibitory control, slow processing speed, working memory impairments, or even emotion decoding abilities (Romero-Martínez, Lila, Victoria-Estruch, et al., 2021). Thus, there might be a reduced capacity to process surrounding clues that affect the evaluation of future consequences of current decisions. Dysfunctions in these basic cognitive processes also affect the expression of thoughts, the verbalization of ideas, and/or the processing of emotions (Cohen et al., 1999; Romero-Martínez et al., 2019; Romero-Martínez, Lila, Moya-Albiol, et al., 2021). For example, an overload in attention and working memory substantially interferes with the ability to correctly process and identify emotional facial expressions (Phillips et al., 2008). Therefore, it is possible to conclude that some IPV perpetrators in a context of ambiguity tend to misinterpret environmental and inner stimuli, which ultimately reduces their threshold for reacting violently when they also have hostile schemas regarding partner intentions (e.g., domestic dispute, dealing with daily stressors) (Babcock et al., 2008; Medina et al., 2004). After exploring the main causes for these neuropsychological impairments or deficits, scientific research has revealed that alcohol misuse presents a strong link with those impairments, given its neurotoxic effects on central nervous system morphology and functioning when individuals present a heavy and sustained consumption of this substance (Houston et al., 2014; Oscar-Berman & Marinkovi, 2007; Stavro et al., 2013). Alcohol misuse has also shown a strong link with current perpetration and long-term maintenance of IPV (Stuart et al., 2009). For this reason, therapists have focused on reducing alcohol misuse in IPV perpetrators which, in turn, reduces the risk of IPV recidivism (Capaldi et al., 2012; Wilson et al., 2014). In this line, two studies divided a sample of IPV perpetrators according to their daily alcohol use or alcohol misuse. Both studies concluded that IPV perpetrators with higher daily alcohol use presented worse neuropsychological performance (e.g., executive functioning, attention, memory, and emotion decoding abilities), compared to non-IPV perpetrators or controls (Easton et al., 2008; Vitoria-Estruch et al., 2018). They were able to conclude the existence of differences between IPV perpetrators without alcohol misuse and controls, although less pronounced than in the IPV perpetrators’ group with alcohol misuse. However, Easton et al. (2008) did not find differences among groups of IPV perpetrators in terms of neuropsychological performance. Vitoria-Estruch et al. (2018) pointed out that IPV perpetrators with drug misuse presented higher attention shifting problems than those without drug misuse. Drastic reductions in alcohol consumption also correspond to improvements in neuropsychological performance that are also related to a decrease in IPV recidivism (Romero-Martínez et al., 2016). Therefore, even though we cannot establish a causal association between the above-mentioned variables (alcohol misuse, neuropsychological performance, and recidivism; Dowden & Brown, 2002), cognitive or neuropsychological functioning maintained a significant association with alcohol misuse and risk of recidivism (Meijers et al., 2017; Romero-Martínez, Lila, Gracia, et al., 2021). Simultaneous and concurrent alcohol, cannabis, and cocaine misuse exponentially increases the risk of perpetrating IPV more than alcohol or other drugs alone (Kraanen et al., 2014; Smith et al., 2012). A review showed that high proneness to violence might be explained by a concurrent use of alcohol and cocaine, which produces worse cognitive performance than each of them alone, especially regarding alterations in speed processing, working memory, and cognitive flexibility (Romero-Martínez & Moya-Albiol, 2016). More specifically, the amount of alcohol, cannabis, and/or cocaine consumed per week by IPV perpetrators correlated negatively with neuropsychological functioning (i.e., the higher the consumption, the worse the cognitive performance; Easton et al., 2008). The diminished or low cognitive functioning of IPV perpetrators might explain why certain individuals under the influence of drugs or during an abstinence period show a restricted ability to process environmental or inner signals, which in combination with hostile cognitive schemas or high levels of hostility might lead to IPV perpetration or recidivism. Additionally, cognitive impairments are also of considerable value for predicting IPV perpetrators’ dropout, which increases the risk of future recidivism (Lila et al., 2019; Romero-Martínez, Lila, Gracia, et al., 2021). To our knowledge, no studies have considered whether the neuropsychological functioning of IPV perpetrators with alcohol, cannabis, and/or cocaine misuse differs from the functioning of those IPV perpetrators without substance misuse, and from male non-IPV perpetrators without substance misuse (control group). Furthermore, it would be important to know whether neuropsychological impairments are related to IPV recidivism. The main objective of this study was twofold. First, to analyze whether IPV perpetrators (with and without substance misuse) and controls showed differences in specific neuropsychological variables, such as verbal and non-verbal abilities, working memory, processing speed, attention, verbal fluency, cognitive flexibility, planning abilities, and emotion decoding processes. We first hypothesized that, in line with previous research (Horne et al., 2020; Humenik et al., 2020; Romero-Martínez et al., 2013; Romero-Martínez et al., 2019; Vitoria-Estruch et al., 2018; Vitoria-Estruch et al., 2017), IPV perpetrators with substance misuse (i.e., alcohol, marijuana, and cocaine) would present worse neuropsychological performance than IPV perpetrators without substance misuse and controls. Second, we also aimed to assess whether there were differences between the IPV perpetrator groups regarding risk of recidivism (based on intervention facilitators’ assessment) and official recidivism, and whether the neuropsychological performance of the IPV perpetrator groups predicted recidivism. Hence, based on previous results in this field, we expected worse neuropsychological functioning to be associated with the highest recidivism rate (Romero-Martínez, Lila, Gracia, et al., 2021). Participants To conduct this study, considering an effect size of 0.5, a margin of error of 5% (α = .05, 1-β = .95), and a statistical power of .95, a minimum of 210 participants would be necessary (AICBT Ltd, 2021). To increase the soundness of our study, we recruited a total of 320 healthy men who initially agreed to participate, but after verifying whether they met the inclusion criterion, only 307 were finally included. Participants were recruited from 2020 to 2021. To be included in this research, participants had to meet the following criteria: to be older than 18 years of age, have adequate Spanish reading and writing skills, and an IQ equal to or above 80. Furthermore, participants were excluded if they presented physical or mental/cognitive disorders, such as schizophrenia, severe traumatic brain injury, and strokes with severe brain damage. Regarding IPV perpetrators, they had been sentenced to less than two years in prison and had no previous criminal record. As an alternative to going to prison, they could have been attending an intervention program designed specifically for this kind of violent population. They had received a court mandated psycho-educational and community-based treatment program. This intervention is a cognitive behavioral treatment that also includes motivational strategies to increase treatment compliance and promote change (Lila et al., 2018, 2020). The intervention program lasted approximately 35 weeks (2 hours per session). With regard to controls, we posted advertisements for male volunteers in the city of Valencia. After potential participants contacted us, we initially screened them to ensure that they met the inclusion criteria. Specifically, only men with no physical or mental disorders, no criminal record (asking for official records issued by a public institution), and a score below 1 on the Conflict Tactics Scale-2 (e.g., physical assault and psychological misuse) were part of the study. Finally, they had to present similar sociodemographic characteristics to those of the IPV perpetrator group. All participants voluntarily gave their written informed consent, as proposed in the Declaration of Helsinki. This project was also approved by the University of Valencia Ethics Committee (assigned codes: H1515749368278 and H1537520365110). Procedure Before agreeing to participate, the IPV group was informed that refusing to participate in the study would not affect their legal status. They were completely free to participate in the study, and they were all informed that the study measurements would be confidential. Sociodemographic data, substance misuse, and neuropsychological measurements were collected at the start of the IPV intervention program. During the first evaluation session, participants were interviewed to exclude any individual with physical or mental illnesses that could seriously disrupt the functioning of the intervention, and sociodemographic data and substance misuse patterns were collected. Participants were classified as engaging in substance misuse if they scored above 8 on the Alcohol Use Disorders Identification Test (AUDIT; Contell-Guillamón et al., 1999; Saunders et al., 1993) and/or 3 on the Severity Dependence Scale (SDS) for cannabis and/or cocaine (Kaye & Darke, 2002; Miele et al., 2000; Vélez-Moreno et al., 2013). Participants who scored below the cutoff scores on the previously mentioned scales were classified as non-substance misusers. Conversely, those who scored above the cutoff score for AUDIT and/or SDS for cocaine and/or marijuana were classified as substance misusers. The second evaluation session took place the following weekday between 10 a.m. and 2 p.m. to minimize possible effects of daily fatigue. After arriving at the laboratory, participants were taken to a room where the neuropsychological tests were administered for approximately 90 minutes. The Spousal Assault Risk Assessment Guide (SARA; Andrés-Pueyo et al., 2008; Kropp et al., 1995) to assess recidivism after the intervention ended was completed during the last stage of the intervention program by program facilitators. Additionally, official recidivism, which was provided by the Spanish Ministry of the Interior, was recorded a year after intervention ended. Instruments To measure verbal and non-verbal abilities, the Kaufman Brief Intelligence Test was employed (K-BIT; Kaufman & Kaufman, 1997). This test contains two subtests: vocabulary and matrices. Specifically, the vocabulary subtest measures expressive vocabulary and definitions, whereas matrices consist of a series of abstract figures in which participants have to discover the logic underlying the sequence of figures. To assess working memory, we employed the digits subscale of the Wechsler Intelligence Scale-III (WAIS-III; Wechsler, 1999). For this study we only considered the total score (direct + indirect order). For processing speed and attention, Conners’ Continuous Performance Test-III (CPT-III; Conners, 2015) was employed to assess inattention, impulsivity, sustained attention, and vigilance. For approximately 14 minutes, participants had to press the space bar on the computer when any letter except “X” appeared on the screen. For this study, we considered total reaction time (milliseconds, ms), number of omissions, commissions, and perseverations. While omissions and commissions might be employed as markers of inattentiveness, total reaction time and perseverations might be related to impulsivity. For verbal fluency, F-A-S verbal phonemic fluency was used. During this test, participants have to verbalize as many words as possible starting with F, S, and A for 60 seconds for each letter. A total score is obtained by adding one point for each correct response. Furthermore, for verbal semantic fluency, participants must provide as many animal names as they can for 60 seconds. In both cases, a higher total score indicates better verbal fluency (Del Ser Quijano et al., 2004). To measure cognitive flexibility, we employed the Wisconsin Card Sorting Test (WCST; Heaton et al., 1993). This test consists of 4 stimulus cards and 128 response cards containing various colors (red, blue, yellow, or green), shapes (circle, cross, star, or triangle), and numbers (one, two, three, or four) of figures. For this study, we considered the number of trials, non-perseverative and perseverative errors, number of categories completed, and failure to maintain the set. A low number of trials and errors and a high number of categories indicated better performance (good abilities for rule detection after switching following test logic). To measure planning abilities, the Key test was employed, which is part of the Behavioural Assessment of Dysexecutive Syndrome (Wilson et al., 1996). Participants have to draw an itinerary to discover how to find a lost key. For this test, we included the total score and the time spent planning and executing the task. To measure “emotion decoding abilities”, we included the Eyes Test (Baron-Cohen et al., 2001). Participants have to correctly identify the emotion that best represents the expression in the eyes in 36 photographs that show the eye region of different men and women. The total score, which ranges from 0 to 36 points, is obtained by adding up the number of correct answers, with a higher score indicating better emotion decoding abilities. Internal consistency for this study was α = .61, which is in line with previous studies employing this test (Oakley et al., 2016). We employed the Spanish version of Alcohol Use Disorders Identification Test (AUDIT; Contell-Guillamón et al., 1999; Saunders et al., 1993) to measure “alcohol misuse”. This test consists of 10 self-report items rated from 0 (never) to 4 (daily or almost daily), with a minimum score of 0 and a maximum of 40. As recommended by García-Carretero et al. (2016), we established a cutoff score of 8. Men scoring below 8 were considered individuals without alcohol misuse. Individuals scoring 8 or above were considered in the alcohol misuse group (i.e., with heavy and sustained alcohol consumption). Cronbach’s alpha for this study was .83. To assess cannabis and cocaine misuse, we adapted the Spanish version of Severity Dependence Scale (Miele et al., 2000; Vélez-Moreno et al., 2013). This test consisted of five items, with a scale ranging from 0 (never) to 3 (always). Following Kaye and Darke’s (2002) recommendations, we considered a cutoff score of 3 for this study. Those who scored below this number were considered in the no substance misuse group. Men who scored 3 or above were considered in the substance misuse group. Cronbach’s alpha for cannabis scale was .89 and for cocaine scale .87. Additionally, we registered the number of joints and grams per week, respectively. We employed the Spanish version of the Revised Conflict Tactics Scale (CTS2; Muñoz-Rivas et al., 2007; Straus et al., 1996), to assess how individuals respond to and resolve conflicts in their relationships. This test contains 78 items, rated on a scale ranging from 0 (this has never happened) to 6 (more than 20 times in the past year). Additionally, 7 represents not in the past year, but it has happened before. Cronbach’s alphas for this study were .73 and .82 for physical assault and psychological misuse, respectively. We employed the Spanish version of the Spousal Assault Risk Assessment Guide (SARA; Andrés-Pueyo et al., 2008; Kropp et al., 1995), to measure the risk of recidivism. This measure consists of 20 items, rated on a scale ranging from 0 (absence) to 2 (presence). This checklist was administered by trained program facilitators specialized in this field to assess participants’ risk of recidivism. The measurement was based on information provided by judicial and probation system professionals and by the participant. A higher total score indicates a higher risk of recidivism, with a maximum score of 40. Cronbach’s alpha for this study was .70. Regarding official recidivism, it was assessed one year after the treatment ended, using the monitoring system of the Spanish Ministry of the Interior (responsible for the penitentiary system), specifically from the VioGén database. This system was developed for monitoring the legal measures applied to IPV perpetrators and to prevent additional criminal activities which might lead to IPV. It was coded as 0 (if the participant did not recidivate) and 1 (if the participant recidivated). Data Analysis Plan Initially, one-way ANOVAs were conducted to check for significant differences between the three groups in age and number of children. Furthermore, a chi-square analysis was used to assess group differences in sociodemographic characteristics (e.g., educational level, nationality, and working status). To address the first objective of the study, after checking for normal distribution of the data, a one-way ANOVA was used to check for significant differences between the groups on digit span WAIS-III and risk of recidivism. MANOVA were performed for the rest of the neuropsychological measures with more than one subscale, using the Greenhouse-Geisser adjustment for degrees of freedom. A chi-square analysis was conducted to assess group differences in official recidivism. With regard to the second objective of the current study (i.e., neuropsychological performance as predictor of official and risk of recidivism), to assess whether the neuropsychological performance of IPV perpetrators (both groups together) predicted official recidivism (dichotomous variable) and risk of recidivism (continuous variable), logistic and linear regression models were conducted, respectively. In both cases, ‘group’ was included as a covariate to control its potential effect. Data analyses were carried out using IBM SPSS Statistics for Windows, version 26.0 (Armonk, NY, USA); p values < .05 were considered statistically significant for initial analysis or the main effects. Due to the elevated number of comparisons for post hoc analysis (three comparisons per variable for neuropsychological variables) and to reduce the risk of obtaining false positives (Armstrong, 2014; Lee & Lee, 2018), we applied Bonferroni correction for multiple comparisons, setting the significance level at .001 Initially, we checked for differences in demographic variables between groups. As Table 1 shows, there were no differences in any of the variables considered, that is, age, number of children, educational level, nationality, and/or working status. As expected, the groups differ in alcohol, F(2, 306) = 42.11, p < .001, ηp2 = .233; cannabis, F(2, 306) = 125.43, p < .001, ηp2 = .669; and cocaine consumption, F(2, 306) = 169.13, p < .001, ηp2 = .740. In all cases, IPV perpetrators with substance misuse consumed more alcohol (t = 5.97, p < .001 and t = 5.40, p < .001, respectively), cannabis (t = 5.95, p < .001 and t = 5.95, p < .001, respectively), and cocaine (t = 6.60, p < .001 and t = 6.60, p < .001, respectively) than non-substance misuse IPV perpetrators and controls. Additionally, we specified the number of joints as well as the grams of cocaine per week. Table 1 Means (Standard Deviations) of Anthropometric and Demographic Variables of Participants 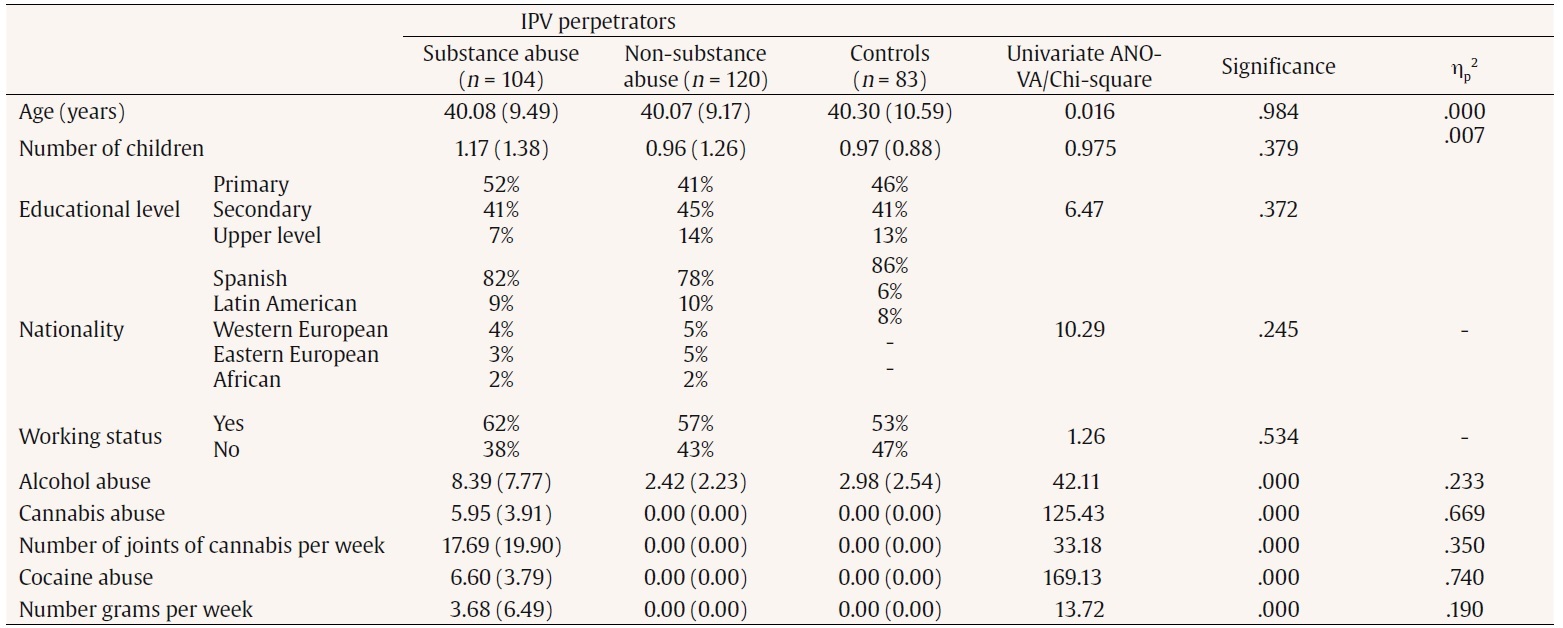 Note. IPV = intimate partner violence; SDS = Severity Dependence Scale. Statistical significance for post hoc tests. ***p < .001. Groups’ Neuropsychological Performance With regard to the first objective, we checked for differences in the neuropsychological performance of the IPV perpetrators groups (with and without substance misuse) and controls. Several significant differences were observed in verbal and non-verbal abilities, F(2, 306) = 5.19, p = .006, ηp2 = .046, and working memory, F(2, 306) = 4.57, p = .001, ηp2 = .029. A post-hoc analysis revealed that IPV perpetrators with substance misuse presented worse working memory than controls (t = -2.12, p = .001). Group differences were found in attention (omissions), F(2, 306) = 6.42, p = .002, ηp2 = .046; commissions or false alarms, F(2, 306) = 9.19, p < .001, ηp2 = .065; and perseverations, F(2, 306) = 12.52, p < .001, ηp2 = .087. A post-hoc analysis revealed that IPV perpetrators with substance misuse performed worse than controls on omissions (t = 3.27, p = .001, d = 0.64), commissions (t = 12.89, p < .001, d = 0.63), and perseverations (t = 0.47, p < .001, d = 0.74). Regarding executive functioning, a significant effect was found for verbal fluency (phonemic), F(2, 306) = 44.58, p < .001, ηp2 = .237, and semantic, F(2, 306) = 116.00, p < .001, ηp2 = .447. Thus, both groups of IPV perpetrators (with and without substance misuse) presented worse performance than controls on phonemic (t =15.67, p < .001, d = 1.19, and t =15.43, p < .001, d = 1.17, respectively) and semantic (t = 19.88, p < .001, d = 2.12, and t = 17.03, p < .001, d = 1.63, respectively). The groups also differed on the cognitive flexibility measure, specifically the number of trials, F(2, 306) = 35.08, p < .001, ηp2 = .194; non-perseverative errors, F(2, 306) = 21.14, p < .001, ηp2 = .126; perseverative errors, F(2, 306) = 11.46, p < .001 ηp2= .073; number of completed categories, F(2, 306) = 23.29, p < .001, ηp2 = .138; and failure to maintain the set, F(2, 306) = 7.46, p = .001, ηp2 = .031. Post hoc analysis revealed that IPV perpetrators with and without substance misuse had a greater number of trials (t = 21.91, p < .001, d = 1.07, and t = 21.76, p < .001, d = 1.04, respectively), more non-perseverative (t = 12.69, p < .001, d = 0.98, and t = 12.73, p < .001, d = 0.87, respectively) and perseverative errors (t = 9.89, p < .001, d = 0.65 and t = 10.90, p < .001, d = 0.72, respectively), and fewer completed categories than controls (t = 1.75, p < .001, d = 0.95, and t = 1.73, p < .001, d = 0.94, respectively). Additionally, IPV perpetrators with substance misuse had more failures to maintain the set than controls (t = 0.77, p < .001, d = 0.55). The assessment of planning abilities revealed that the groups differed on time planning, F(2, 306) = 3.58, p = .029, ηp2 = .024, and the total score on the key test, F(2, 306) = 15.32, p < .001, ηp2 = .096. However, a post-hoc analysis only revealed differences on the total key test, on which IPV perpetrators with and without substance misuse scored below controls (t = -2.80, p < .001, d = 0.74, and t = -2.71, p < .001, d = 0.71, respectively). Regarding emotion decoding, a significant group effect was found, F(2, 306) = 19.89, p < .001, ηp2 = .123, with IPV perpetrators with and without substance misuse detecting fewer correct responses than controls (t = -3.23, p < .001, d = 0.74, and t = -3.95, p < .001, d = 0.88, respectively). Group Differences in Risk and Official Recidivism For risk of recidivism and official recidivism, significant group effects were found (t = -2.66, p = .008, d = 0.376, and c2(1) = 5.27, p = .022). IPV perpetrators with substance misuse presented higher risk and official recidivism than IPV perpetrators without substance misuse (see Table 2). Table 2 Means (Standard Deviations) for Neuropsychological Variables, Risk of Recidivism, and Official Recidivism for all Groups 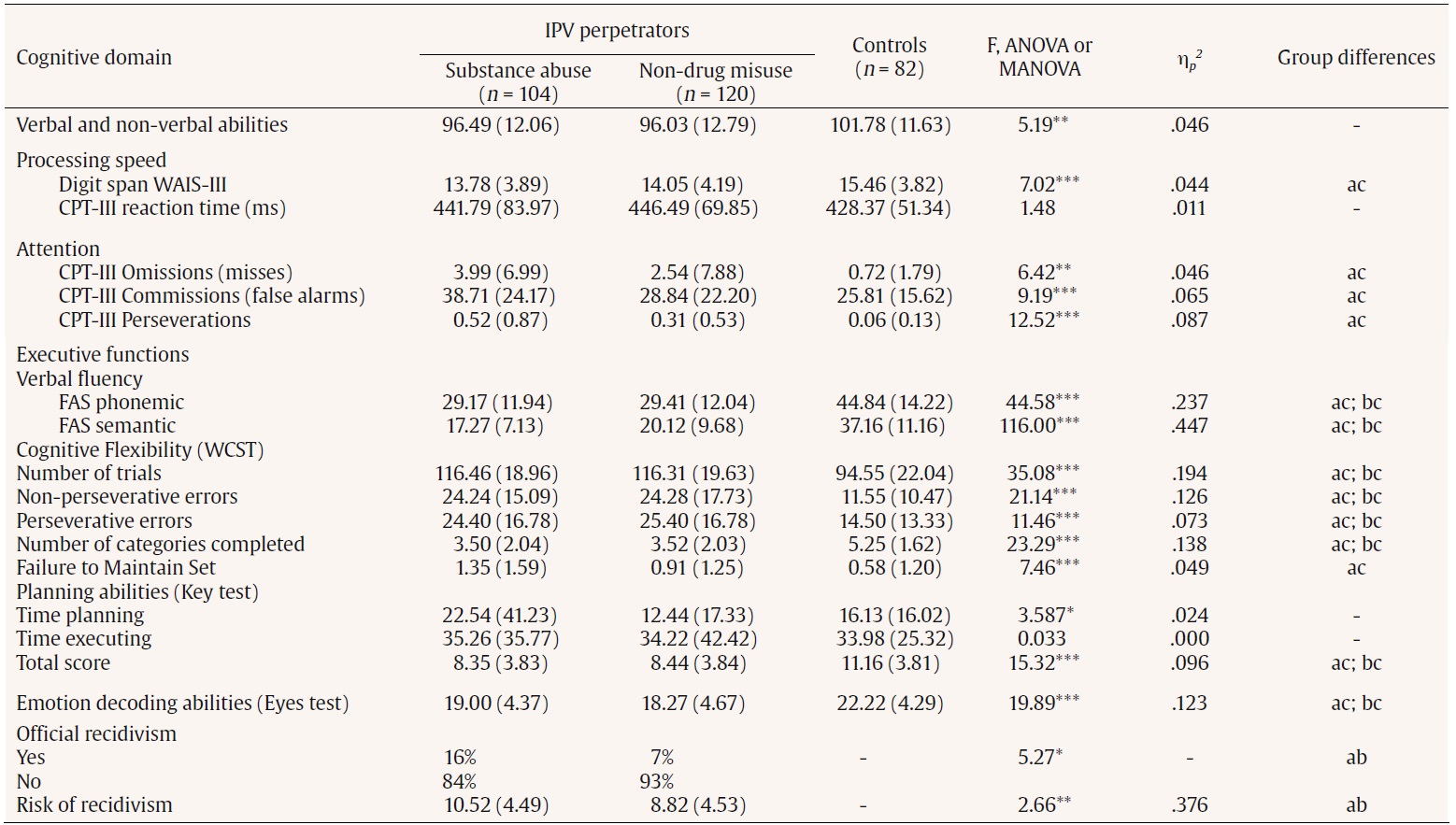 Note. IPV = intimate partner violence. Group differences: a: IPV perpetrators drug misuse; b: IPV perpetrators non-drug misuse; c: controls. *p < .05, **p < .01, ***p < .001. Neuropsychological Measures as Predictors of Risk and Official Recidivism A linear regression model was conducted to assess the main effects of IPV perpetrators’ neuropsychological functioning on the risk of recidivism. A significant main effect of attention (commissions or false alarms) and verbal fluency (semantic) was found on risk of recidivism, R2 = .134, F(1, 223) = 11.43, p < .001; β = .315, t = 3.93, p < .001; and β = -.214, t = -2.68, p = .008, respectively (see Table 3). After including ‘group’ as covariate, attention (commissions) and FAS semantic still predicted the dependent variable, (β = .299, t = 3.61, p < .001, and β = -.211, t = -2.62, p = .010). A logistic regression was conducted to assess the main effects of IPV perpetrators’ neuropsychological functioning on official recidivism. We found significant main effects of cognitive flexibility (perseverative errors) and attention (perseverations) on official recidivism, Wald(1) = 7.47, SE = 0.01, p = .006, Exp(β) = 1.04, 95% CI [1.01, 1.07], and Wald(1) = 4.48, SE = 0.29, p = .032, Exp(β) = 1.83, 95% CI [1.01, 1.07] (see Table 3). After including ‘group’ as covariate, both variables still predicted official recidivism, Wald(1) = 7.66, SE = 0.01, p = .006, Exp(β) = 1.04, 95% CI [1.01, 1.07], and Wald(1) = 3.58, SE = 0.29, p = .05, Exp(β) = 1.73, 95% CI [.098, 3.05]. Table 3 Neuropsychological Functioning as Predictor of Risk and Official Recidivism for the Complete Sample of Intimate Partner Violence Perpetrators  Note. CI = confidence interval. *p < .05; ** p < .01; ***p < .001. The main aim of our study was twofold: 1) to find out whether or not there are neuropsychological differences between two groups of IPV perpetrators (with and without substance misuse) and controls and, more importantly, 2) whether there are differences in recidivism among IPV perpetrators (with and without substance misuse) and whether these differences are explained by neuropsychological performance. Our results reveal that IPV perpetrators with substance misuse showed worse cognitive performance than controls, specifically in terms of working memory, attention, executive functioning, and emotion decoding abilities. Differences were also found between IPV perpetrators without substance misuse and controls only in terms of executive functioning (i.e., verbal fluency, cognitive flexibility, and planning abilities). It is worth highlighting that Cohen’s d value ranged from 0.2 (small effect sizes) to 0.5 or close to it (medium effect sizes). The highest value corresponded to semantic fluency followed by phonemic and several WCST subscales. Finally, there were no differences in neuropsychological performance between the two groups of IPV perpetrators, but those with substance misuse presented higher recidivism than IPV perpetrators without substance misuse. Furthermore, whereas verbal fluency and attention impairments were related to a high risk of recidivism, cognitive flexibility and attention impairments explained official recidivism, and these patterns of associations were the same for both groups of IPV perpetrators. Regarding the first aim of our manuscript, our results are congruent with several studies in this field of research (Becerra-García, 2015; Easton et al., 2008; Romero-Martínez et al., 2019; Stanford et al., 2007; Vitoria-Estruch et al., 2018; Walling et al., 2012). In this sense, IPV perpetrators with substance misuse presented worse neuropsychological performance than controls. Additionally, this group of IPV perpetrators also presented the highest rate of recidivism. The main novelty of the current research was that we included polysubstance misusers – not only alcohol as in previous studies — in a relatively large sample size. Our data support the idea that substance misuse tends to interfere more in specific cognitive domains such as attention and working memory. Nonetheless, both groups of IPV perpetrators presented slightly worse performance on executive functioning and emotion decoding compared to controls. This is congruent with the model that theorizes that low cognitive functioning, especially executive functioning impairments, might explain antisocial behaviors such as violence, particularly under the influence of certain toxic substances such as alcohol and/or other drugs (Fishbein & Tarter, 2009; Hoaken et al., 1998). However, the performance of both groups of IPV perpetrators could not be qualified in this study as “deficit” or “mild cognitive impairment”, given that they did not score 1.5-2 standard deviations below age-matched control group performance (Dunne et al., 2021). Contrary to our expectations, we did not find significant differences in neuropsychological performance among IPV perpetrators groups. This was congruent with the results of Easton et al. (2008) but contradict the conclusions of Vitoria-Estruch et al. (2018). Vitoria-Estruch et al. highlighted the existence of differences in attention shifting between IPV perpetrators with different levels of alcohol consumption. Specifically, those with high daily alcohol levels presented serious difficulties in shifting their attention in comparison with men who consumed less alcohol. It is not possible to explain differences across studies because previous research did not apply, for example, statistical control of post-hoc analysis, as we did in the current study. In fact, we only interpreted significant between-group differences as those with a p value equal to or less than .001. In addition, different computerized tasks were employed in different studies to assess attention, with the CPT-III being widely employed to measure attention disorders (Berger et al., 2017). We consider it particularly important to include other variables inherent to substance misuse in future studies to understand these kinds of differences. Variables such as the number of years consuming, polysubstance misuse, time of abstinence, among others, would offer valuable information about the effects of substance misuse beyond cognition. Rather than considering subgroups of IPV perpetrators according to their drug consumption levels, it might be suitable to assess how other variables, such as personality traits, interact with substance misuse to explain neuropsychological functioning differences. A previous study assessing the Holtzworth-Munroe and Stuart’s (1994), typologies of IPV perpetrators found significant differences in executive functioning, specifically cognitive flexibility, between these typologies (Romero-Martínez, Lila, Gracia, et al., 2021). The authors concluded that generally antisocial IPV perpetrators, who presented the highest substance misuse levels, showed the lowest levels of cognitive flexibility. Therefore, it is necessary to be cautious when interpreting the current data, without considering simplistic models of IPV perpetration. Due to the different tests employed for assessing a specific cognitive domain (e.g., Trail Making Test, WCST, CPT-III, etc.) in the scientific literature of this field, it would be important to standardize a reliable set of neuropsychological tests for screening the cognitive needs of IPV perpetrators during the initial stages of interventions designed for these men. Regarding the second aim of this study, our data showed that IPV perpetrators with substance misuse presented the highest levels of risk of recidivism and official recidivism. Previous research indicated that substance misuse showed a strong association with recidivism rates after being released from prison, even after controlling for participant characteristics such as mental disorders and type and severity of crime (Håkansson & Berglund, 2012; Taxman and Mun, 2018). Although these authors did not explore whether cognitive domains were associated with substance misuse and recidivism, in our study we have tried to respond to this question. In this regard, our study offers some background about which cognitive functioning processes are important for recidivism. The analysis of the patterns of associations between the variables allowed us to conclude that the worse the cognitive flexibility, verbal fluency, and attention abilities, the higher the recidivism rate, the same thing being true for both groups of IPV perpetrators. Taking our results into account (i.e., absence of differences among IPV perpetrators with and without substance misuse and the same pattern of association between variables in both groups of IPV perpetrators), we cannot conclude that neuropsychological variables act as mediating variables between substance misuse and recidivism. As explained above, it should be important to control for other potential variables, such as personality traits or other sociodemographic characteristics, that interact with neuropsychological impairments to mediate the association between substance misuse and recidivism. Alterations in cognitive functioning of IPV perpetrators underline the need to implement cognitive training focused on these neuropsychological impairments. These kinds of programs should be considered complementary to IPV interventions, along with others focused on reducing substance misuse. A pioneering randomized controlled trial assessed the effects of implementing cognitive training combined with a standard intervention program (SIP), and the authors concluded that IPV perpetrators who received the reinforcement focusing on their cognitive needs experienced greater cognitive improvements (e.g., cognitive flexibility, speed processing, etc.) and a lower risk of recidivism, in comparison with those who received the SIP alone (Romero-Martínez, Santirso, et al., 2021d). Hence, the combination of different programs according to patients’ needs would benefit their adherence to treatment, which in turn would reduce the future risk of recidivism (Expósito-Álvarez et al., 2021; Lila et al., 2020). Despite the promising significance of these results, several limitations of this study should be taken into account. The first is the absence of an additional control group of non-IPV perpetrators (controls) with substance misuse. Furthermore, as Table 1 shows, the groups characterized as “non-substance misuse” and “controls” did not present an absence of alcohol consumption. They actually could be described as “low alcohol use” or “normative alcohol use”. Further research should consider this given that it would help better characterize the neuropsychological profile of different subsamples of men, as well as their proneness to violence. Thus, it would be necessary to replicate the results in future studies in a larger sample size. Second, it is also necessary to include a complete set of neuropsychological tests to assess the reliability of our results. For example, planning abilities were measured in this study with a subtest of the Behavioural Assessment of the Dysexecutive Syndrome, but other tests are more complex and accurate for assessing planning, such as the Tower of London. It would also be interesting to employ the short version of the WCST, which considerably reduces the assessment time. This, in turn, underlines the need to standardize a set of tests for this sample. Third, due to the quasi-experimental, cross-sectional, and nonrandomized nature of our study, it might be difficult to conclude whether our results were stable over time or changed with the changes in drug use patterns. We cannot establish whether IPV perpetrators’ neuropsychological performance preceded substance misuse or, conversely, this last variable or other non-contemplated sociodemographic variables were the main cause of their performance. Hence, it is extremely difficult to establish a hierarchy order or causal associations between the above-mentioned variables. Fourth, one of the neuropsychological tests included in this study (eyes test) presented poor internal consistency (Cronbach’s alpha below .70). However, our data are congruent with the internal consistency presented in a systematic review (Oakley et al., 2016). Although the value of this test for differentiating IPV perpetrators from controls has been demonstrated, more robust tools should be developed to measure emotion decoding abilities. Moreover, the new versions of some tests such as WAIS-IV and K-BIT 2 validated into Spanish should be incorporated into future studies. The current data emphasize the need to incorporate neuropsychological tests to screen the therapeutic needs of IPV perpetrators. This initial assessment might make it possible to develop cognitive training coadjutant to IPV perpetrator intervention programs, which would reduce the future risk of recidivism. Even though neuropsychological tests do not present the same biases as self-reports (e.g., social desirability, low reliability, honesty of respondent), malingering responses should be detected by including specific tests that assess them. These results should be combined with other objective measurements such as brain measurements, hormonal markers, correlates of central nervous system functioning, and other qualitative data from interviews. In summary, our study offers information about the complexity of the association between cognitive domains, substance misuse, and IPV recidivism. In this regard, not only it is necessary to control substance misuse in IPV perpetrators, but coadjutant cognitive training programs should also be developed for these dysfunctions, parallel to IPV perpetrator intervention programs. To do so, it would be necessary to establish a reliable set of neuropsychological tests administered during the initial stages of SIP, in order to develop cognitive training based on IPV perpetrators’ cognitive needs. In addition, we also recommend incorporating or exploring other alternative treatments to the current ones (e.g., pharmacological treatments, non-invasive brain techniques, among others). Conflict of Interest The authors of this article declare no conflict of interest. Cite this article as: Romero-Martínez, A., Lila, M., Sarrate-Costa, C., Comes-Fayos, J., & Moya-Albiol, L. (2022). Neuropsychological performance, substance misuse, and recidivism in intimate partner violence perpetrators. Psychosocial Intervention, 32(2), 69-77. https://doi.org/10.5093/pi2022a7 |
Cite this article as: Romero-Martínez, Á., Lila, M., Sarrate-Costa, C., Comes-Fayos, J., & Moya-Albiol, L. (2023). Neuropsychological Performance, Substance Misuse, and Recidivism in Intimate Partner Violence Perpetrators. Psychosocial Intervention, 32(2), 69 - 77. https://doi.org/10.5093/pi2022a7
Correspondence: Angel.Romero@uv.es (├ü. Romero Mart├şnez).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
Send






