


Integrated Motivational Strategies for Intimate Partner Violence Perpetrators with Substance Use: A Randomized Controlled Trial
Cristina Expósito-Álvarez1, Manuel Roldán-Pardo1, Gail Gilchrist2, and Marisol Lila1
1Department of Social Psychology, Faculty of Psychology and Speech Therapy, University of Valencia, Spain; 2National Addiction Centre, Institute of Psychiatry, Psychology & Neuroscience, King’s College London, UK
https://doi.org/10.5093/pi2024a13
Received 29 April 2024, Accepted 3 July 2024
Abstract
Objective: Intimate partner violence (IPV) perpetrators with alcohol and/or other drug use problems (ADUPs) have been identified as one of the main high-risk and highly resistant groups of perpetrators requiring special attention in intervention programs for IPV perpetrators. This randomized controlled trial (RCT) aimed to evaluate whether an individualized motivational plan adjusted to ADUPs (IMP-ADUPs) was superior to standard motivational strategies (IMP) in reducing ADUPs, and IPV and increasing treatment adherence in IPV perpetrators. Method: Data from a full sample of IPV perpetrators (n = 140) and a subsample of participants with ADUPs (n = 55) were collected at pre- and post-intervention and 12-month follow-up. Final outcomes included alcohol, cocaine, and cannabis use, self-reported IPV, risk of recidivism assessed by facilitators, and official IPV recidivism. Proximal outcomes included treatment adherence (stage of change, intervention dose, active participation, and dropout). Results: Both intent-to-treat (ITT) and per-protocol (PP) analyses were conducted. The IMP-ADUPs condition was superior to the IMP in reducing alcohol use at post-intervention in both the full sample and ADUPs subsample. The full sample of participants in the IMP-ADUPs condition were in a more advanced stage of change post-intervention and showed increased active participation during the intervention process than IMP participants. All participants were in a more advanced stage of change at post-intervention and reduced their alcohol use and their risk of recidivism at post-intervention and 12-month follow-up. Conclusions: These results underscore the need to develop individualized treatment approaches to address participants’ risks and needs and promote their motivation to change.
Keywords
Intimate partner violence, Motivational strategies, Perpetrator intervention programs, Randomized controlled trial, Substance useCite this article as: Expósito-Álvarez, C., Roldán-Pardo, M., Gilchrist, G., & Lila, M. (2024). Integrated Motivational Strategies for Intimate Partner Violence Perpetrators with Substance Use: A Randomized Controlled Trial. Psychosocial Intervention, 33(3), 187 - 200. https://doi.org/10.5093/pi2024a13
Correspondence: Marisol.Lila@uv.es (M. Lila).Intimate partner violence (IPV) perpetrated by men is one of the most common forms of violence against women (World Health Organization [WHO, 2021, 2022]). International efforts, including intervention policies focused on perpetrators have been made in response to this human rights concern, increasingly recognized as a public health problem (Babcock et al., 2016; Gracia et al., 2023; Lilley-Walker et al., 2018; Mackay et al., 2015). Since intervention programs for IPV perpetrators emerged in the late 70s, a need to evaluate their effectiveness has been raised (Cheng et al., 2021; Karakurt et al., 2019; Lila & Gilchrist, 2023). As indicated by previous systematic reviews, there is still room for improvement in enhancing the effectiveness of intervention programs for IPV perpetrators (Arce et al., 2020; Eckhardt et al., 2013; Nesset et al., 2019) by providing targeted programs tailored to meet their criminogenic needs (Bonta & Andrews, 2017; Crane & Easton, 2017; Travers et al., 2021). This is particularly relevant considering that participants court-mandated to attend intervention programs for IPV perpetrators often exhibit high levels of resistance to intervention (e.g., low active participation), poor treatment engagement (e.g., high dropout rates and low intervention dose), and limited motivation to change, factors that have been associated with an increased risk of IPV recidivism and that require special attention (Lila et al., 2019; Olver et al., 2011; Tutty et al., 2020). Participants with alcohol and/or other drug use problems (ADUPs) have been identified as one of the main high-risk and highly resistant groups of IPV perpetrators, exhibiting higher frequency rates of IPV recidivism and the potential for perpetrating more severe violence (Cafferky et al., 2018; Jewell & Wormith, 2010; Leonard & Quigley, 2017). In addition, participants with ADUPs often present poorer treatment outcomes (Expósito-Álvarez et al., 2023; Moore & Stuart, 2004; Timko et al., 2012). Specifically, IPV perpetrators with ADUPs attending IPV interventions have consistently shown higher dropout rates and lower treatment engagement than participants who did not use substances (Lila et al., 2020; Olver et al., 2011). In addition, when compared to participants without ADUPs, participants with ADUPs also presented other potential risk factors for IPV: risk factors at an individual level, such as those associated with personality disorders and psychological adjustment, namely higher anger and impulsivity levels (Expósito-Álvarez et al., 2021, 2023; Oberleitner et al., 2013), social-relational risk factors including higher exposure to childhood trauma (Alexander, 2014; Semiatin et al., 2017; Travers et al., 2022), and risk factors related to attitudes towards women, such as higher responsibility attributed to the offenders’ personal context (Expósito-Álvarez et al., 2021, 2023; Satyanarayana et al., 2015). These participants represent approximately 50% of all IPV perpetrators attending court-mandated intervention programs (Kraanen et al., 2010). The association between IPV perpetration and ADUPs has been well documented within the literature (Gilchrist et al., 2022), which contributes to the importance of providing interventions tailored to meet the needs of perpetrators with these co-occurring problems together (Easton & Crane, 2016; Murphy & Ting, 2010; Tarzia et al., 2020). Recent advancements in intervention strategies have been achieved through the integration of innovative approaches, such as motivational strategies (Santirso, Gilchrist, et al., 2020; Soleymani et al., 2018). Motivational strategies (Miller & Rollnick, 2002), effective in reducing substance use (e.g., DiClemente et al., 2017; Lundahl et al., 2010), have also shown promising results in a range of other behaviors, including IPV (Pinto e Silva et al., 2023; Santirso, Gilchrist, et al., 2020; Soleymani et al., 2018; Wilson et al., 2021), and co-occurring IPV and ADUPs (Expósito-Álvarez et al., 2024; Murphy et al., 2018; Stephens-Lewis et al., 2021). This person-centered, non-confrontational approach fosters a strong therapeutic alliance and focuses on exploring and overcoming ambivalence about change (DiClemente et al., 2017). When implemented in intervention programs for IPV perpetrators, motivational strategies can yield better outcomes, including increased motivation to change, greater assumption of personal responsibility for their violent behaviors, increased engagement with the intervention, and decreased resistance to the intervention (Babcock et al., 2016; Karakurt et al., 2019; Santirso, Lila, et al., 2020; Soleymani et al., 2022). For example, a recently updated systematic review by Wilson et al. (2021) that evaluated court-mandated intervention programs for IPV perpetrators found that programs that have recently incorporated motivational interviewing have resulted in improved treatment outcomes such as better completion rates and treatment engagement. The results of this body of research could be particularly relevant for high-risk and highly resistant perpetrators, such as those who are court-mandated and have ADUPs (Scott et al., 2011; Stephens-Lewis et al., 2021). According to the most up-to-date research, one key strategy for improving the effectiveness of intervention programs for IPV perpetrators is tailoring them to the specific risks and needs of participants (Massa et al., 2020; Travers et al., 2021; Turner et al., 2023). However, in many court-mandated intervention programs, although ADUPs are considered a risk factor, they are not a primary intervention target (Graña et al., 2008). Despite the implementation of motivational strategies in certain perpetrator programs, which have demonstrated more evidence in fostering adherence to the intervention (Crane & Eckhardt, 2013), there remains a lack of targeted strategies to address ADUPs in such programs (Santirso, Gilchrist, et al., 2020). Integrated interventions, which combine evidence-based strategies for reducing IPV and ADUPs within a program, are the prevailing standard of care for effectively addressing both IPV and ADUPs (Yule & Kelly, 2019). This integrated approach may help prevent any of the co-occurring problems from being neglected (Crane & Easton, 2017; Gilchrist & Hegarty, 2017; Stephens-Lewis et al., 2021). Systematic reviews on the effectiveness of interventions for IPV perpetrators suggest promising results for integrated approaches (Karakurt et al., 2019; Tarzia et al., 2020; Turner et al., 2023). Prior randomized controlled trials (RCTs) have demonstrated promise in decreasing both alcohol use and IPV through the implementation of brief integrated interventions compared to control conditions (Easton et al., 2018; Murphy et al., 2018). For instance, Stuart et al. (2013) examined the effectiveness of a standard intervention for IPV perpetrators plus a 90-minute alcohol intervention in contrast to a control, standard IPV intervention and demonstrated short-term improvements in both alcohol use and IPV in hazardous drinking participants in the experimental condition. More recently, Mbilinyi et al. (2023) compared a 2-session telephone-based motivational enhancement therapy (MET) intervention with a mailed educational booklet on IPV and substance use (control) and found greater short-term reductions of IPV and cannabis use in the MET participants. This body of research highlights the potential advantages of brief integrated approaches for IPV and ADUPs over standard, stand-alone interventions. Motivational integrated interventions that concurrently address IPV and ADUPs, not only implemented as a brief adjunct to a standard program but throughout the whole intervention, could effectively reduce the typically high dropout rates, promote behavior change over time, and reduce both, substance use and IPV in this population (Gilchrist et al., 2021; Kraanen et al., 2013; Santirso, Lila, et al., 2020). However, there is a notable lack of evidence-based treatments that address both issues simultaneously (Mootz et al., 2022). As a result, there is an urgent need to develop integrated interventions that implement evidence-based strategies to enhance the likelihood of the intervention’s effectiveness within this high-risk and highly resistant population (Fernández-Montalvo et al., 2019; McMurran, 2017; Romero-Martínez, Lila, & Moya, 2019). In this vein, studies with more robust designs, such as RCTs, are strongly required to evaluate the effectiveness of integrated, motivational-based interventions for IPV perpetrators and to examine the distinct impact of these interventions on groups of IPV perpetrators and specifically on participants with ADUPs (Mootz et al., 2022). The Present Study This study aimed to evaluate the effectiveness of a new motivational strategy tool to address ADUPs and their associated risk factors for men court-mandated to attend a standard intervention program for IPV perpetrators. To this aim, we conducted an RCT to determine whether an individualized motivational plan adjusted to the specific risks and needs of participants with ADUPs (IMP-ADUPs) was superior to the standard individualized motivational plan (IMP; for more information, see Lila et al., 2018) in reducing ADUPs (alcohol, cocaine, and cannabis use) and IPV (officially reported at 12-month follow-up, self-reported, and risk of IPV recidivism assessed by facilitators) in a full sample of IPV perpetrators and a subsample of participants with ADUPs. Additionally, we evaluated whether the IMP-ADUPs would be superior to the standard IMP in increasing treatment adherence (i.e., dropout, intervention dose, active participation, and stage of change). It is important to note that IPV perpetrators were assigned to heterogeneous groups by the judicial system, rather than by their ADUPs status. Therefore, while only some participants may have presented ADUPs, all participants were expected to benefit from the inclusion of IMP-ADUPs components in the group sessions. We hypothesized that groups randomly assigned to IMP-ADUPs would exhibit better final and proximal outcomes compared to groups in the standard IMP condition. However, differences with small to moderate effect sizes were expected, given that the control condition is a standard evidence-based IMP, which has demonstrated its effectiveness in this population (Lila et al., 2018). The study was approved by the University of Valencia Ethics Committee (No H1537520365110) and registered in the ClinicalTrials.gov Protocol Registration and Results System (NCT03885349). Participants Participants in our study were 140 men who participated in a community-based intervention program for IPV perpetrators developed at the University of Valencia (Programa Contexto; Lila et al., 2018). Participants had been sentenced to less than two years in prison for committing IPV against women and had no previous criminal record, so their sentences were suspended on the condition that they participated in an intervention program for IPV perpetrators. Eligibility criteria were screened by program staff and included men who: a) were over 18 years of age, b) had been convicted of IPV, c) had no current severe mental disorders, d) had no severe cognitive impairments, and e) signed a written consent delivered by facilitators to participate in our study. The mean age was 40.7 (SD = 11.2, 20-79). Regarding marital status, 23.6% of the participants were married or in a relationship (n = 33), and the rest were single, divorced, or widowed (76.4%, n = 107). As for educational level, 10.7% of the sample had no schooling (n = 15), 44.3% completed elementary studies (n = 62), 37.9% high school (n = 53), and 7.1% college degrees (n = 10). Most of the participants were Spanish (77.2%, n = 108), 9.2% Latin American (n = 13), 7.1% European (other than Spanish, n = 10), 5.7% African (n = 8), and 0.8% Asian (n = 1). At the time of the initial assessment, approximately one-third of the participants were unemployed (35%, n = 49). Median family household annual income was between €6,000 and €12,000 (M = 4.41, SD = 2.37, 1-12). Treatment Conditions Individualized Motivational Plan (IMP) The control condition consisted of an intervention program for IPV perpetrators which includes a standard IMP. The intervention program for IPV perpetrators consisted of 35 weekly group sessions, each lasting 2 hours, totaling 70 hours over approximately 12 months. The program employed a cognitive-behavioral intervention using a feminist approach and based on the ecological model (Bronfenbrenner, 1979). It consisted of five modules in which several evidence-based intervention strategies were applied (for more information, see Lila et al., 2018 and Santirso, Lila, et al., 2020). The standard IMP relies on evidence-based approaches such as motivational interviewing (Miller & Rollnick, 2002), the therapeutic alliance (Bordin, 1979), the stages of change approach (Prochaska & DiClemente, 1982), and the Good Lives Model (Langlands et al., 2009; Ward, 2002). The main intervention strategies of the standard IMP include: (1) five individual motivational interviews, three of which are conducted at intake to identify IPV-related personal goals, one in the middle of the intervention to monitor their progress, and one at the end to follow up goal achievement; (2) three group sessions throughout the program in which participants are encouraged to share their personal goals, reflect on their progress with the group, and receive feedback, advice and support from facilitators and other group members; (3) facilitators’ monitoring and emphasis on participants’ personal goals at each weekly group session; and (4) retention techniques, including phone calls when participants do not attend a group session. It also involves facilitators adopting an empathetic, collaborative, and non-confrontational attitude to reduce participants’ resistance to treatment and increase their motivation to change. The standard IMP has previously demonstrated its effectiveness in intervention programs for IPV perpetrators (Lila et al., 2018; Romero-Martínez, Lila, Gracia, et al., 2019; Santirso, Lila, et al., 2020). Individualized Motivational Plan-Alcohol and/or other Drug Use Problems (IMP-ADUPs) The experimental condition consisted of the standard intervention program for IPV perpetrators plus the implementation of the IMP adjusted to ADUPs (IMP-ADUPs). This new motivational tool consists of the implementation of an adjusted IMP (Lila et al., 2018) to reduce ADUPs and their associated risk factors (IMP-ADUPs), which has been recognized as a crucial factor in the reduction of IPV recidivism (Stuart et al., 2009). The experimental condition protocol incorporated the standards, objectives, and structure of the standard IMP. Therefore, the same number of hours of clinical contact was provided to participants in both the control and experimental conditions (e.g., a total of 35 group sessions, including three that were motivational-based; plus five individual motivational sessions). However, the IMP-ADUPs protocol included a particular focus on addressing ADUPs. Specifically, during the three individual motivational interviews at intake participants with ADUPs were identified and supported in setting the reduction of ADUPs as their primary goal. In addition, individual motivational sessions held at the middle and end of the program focused on monitoring participants’ progress and achievements in reducing ADUPs. During the IMP group sessions, participants with ADUPs had the opportunity to share their goals, update their group on their progress, and receive support and guidance from the group regarding their ADUPs and associated problems. Additionally, the IMP-ADUPs protocol included content adaptation of the group-based sessions including the incorporation of tailored strategies and activities addressing ADUPs and the recommendation to seek substance use treatment services for men in need of treatment. Although this protocol was implemented specifically in participants with ADUPs, IMP-ADUPs implied both individual and group activities (e.g., ADUPs-related goals were shared and discussed in the group). These adaptations of the group-based sessions could have the potential to impact all participants within the group. Facilitators Training and Treatment Adherence Facilitators were psychologists, both male and female at masters’ or doctorate level, with at least one year of practical experience in IPV intervention group management. The facilitators underwent approximately 25hr of training in their respective treatment condition protocols. Facilitators in the IMP-ADUPs condition received an additional 15hr of training on the implementation of the IMP-ADUPs protocol. A double-blind approach to condition assignment was employed, ensuring that participants and facilitators remained unaware of their respective group conditions. Specifically, participants were not informed about the existence of different conditions. Facilitators in the IMP condition were not informed about the content or condition of the IMP-ADUPs groups, and facilitators of the IMP-ADUPs were also unaware of the presence of a different condition and its respective content. Each condition consisted of six groups led by separate pairs of facilitators. To guarantee the content and adherence to the protocol, written intervention manuals for each condition were employed. Additionally, the facilitators’ treatment fidelity was monitored by two supervisors through four sessions (i.e., two at the beginning, one in the middle, and one at the end of the intervention) using a one-way mirror. Randomization A total of 167 men were assessed for eligibility. After screening, the percentage of the sample that participated in the study was 83.8% (n = 140). A computer random generator was used to randomly assign groups of 14 participants by blocks, in a 1:1 allocation ratio, to receive the standard IMP or IMP-ADUPs condition prior to the initial evaluation. Participants were assigned to the intervention groups by the probation system. The program staff implemented the groups’ random assignment to conditions. Procedure Court-mandated men were randomly assigned to the IMP or IMP-ADUPs condition. They were clearly told that declining to participate in the study would not affect their legal situation. Participants were informed by facilitators that the only circumstance in which the confidentiality rule would be broken would be in the event of an immediate risk of harm to themselves or others. There were no incentives offered to the participants to complete the assessments or participate in the study. At intake, all participants completed a self-report assessment battery of questionnaires including socio-demographic data and self-report data (e.g., substance use and IPV data) administered by the program staff at the facilities of the Faculty of Psychology and Speech Therapy (University of Valencia). The pre-intervention assessment took two 2-hour sessions and was conducted prior to the intervention program. Then, participants received three individual motivational interviews. Facilitators and supervisors assessed participants’ risk of recidivism and stage of change according to the information collected from the self-report measures, the individual motivational interviews, and the judicial sentence. Participants’ self-reported data were also assessed at post-intervention, within a 2-hour session at the faculty facilities immediately following the conclusion of the group sessions at the end of the program. Risk of recidivism, participants’ stage of change, dropout, intervention dose, and active participation were also assessed by facilitators at post-intervention. Self-reported substance use data, risk of recidivism assessed by facilitators, and official recidivism data were also collected at the 12-month follow-up after the post-intervention assessment. Official recidivism, intervention dose, dropout, and active participation data were obtained for all participants (n = 140). To evaluate the impact of the IMP-ADUPs on those participants with high problematic substance use (i.e., ADUPs), a subsample of participants was classified as ADUPs if they scored above the cut-off point in the AUDIT (≥ 8; Babor & Grant, 1989) or SDSCan or SDSCo (≥ 3; Kaye & Darke, 2002) or alcohol or drug dependence subscale of the Millon Clinical Multiaxial Inventory-III (MCMI-III; ≥ 75; Millon, 2007; Spanish version by Cardenal & Sánchez, 2007). This procedure has been used previously in this population (see Expósito-Álvarez et al., 2021, 2024). Measures Final Outcomes Alcohol Use. The AUDIT (Babor & Grant, 1989; Spanish version by Contel et al., 1999), a well-validated 10-item Likert-type scale, was used to screen and evaluate the level and frequency of current and past 12-month drinking and alcohol-related consequences. Responses were on a 3-point or 5-point scale, with items including, for example, 0 = never, 1 = less than once in a month, 2 = once a month, 3 = once a week, and 4 = daily or almost daily. A greater total score indicates a higher risk of hazardous drinking. Scores equal to or above 8 suggest problematic drinking. Cronbach α in this study was .81 at pre-intervention and .65 at post-intervention. The AUDIT has demonstrated construct and discriminant validity and sensitivity and specificity (Allen et al., 1997), and its Spanish version has been used with samples of IPV perpetrators (e.g., Romero-Martínez et al., 2023). Cocaine and Cannabis. Cocaine and cannabis dependence in the past 12 months were measured using the SDS (Gossop et al., 1995; Spanish version by Vélez-Moreno et al., 2013), a 5-item self-report scale with responses given on a 4-point scale, including 0 = never, 1 = sometimes, 2 = often, and 3 = always. Scores of 3 or higher indicate dependence. Cronbach’s αcannabis and αcocaine were .89 and .84 at pre-intervention, and .84 and .95 at post-intervention, respectively. The SDS has shown criterion validity (Gossop et al., 1995) and its Spanish version has been previously used in IPV perpetrator populations (Sarrate-Costa et al., 2022). Self-reported IPV. Self-reported physical and psychological violence subscales from The Revised Conflict Tactics Scale (CTS-2; Straus et al., 1996; Spanish version by Loinaz et al., 2012) were used to assess the extent to which individuals employ violent behaviors against their partner in the past 12 months. Responses were on a 7-point Likert-type scale including 0 = this has never happened, 1 = once in the past year, 2 = twice in the past year, 3 = 3 to 5 times in the past year, 4 = 6 to 10 times in the past year, 5 = 11 to 20 times in the past year, and 6 = more than 20 times in the past year. The frequency-based scoring method of Straus et al. (1996) was followed. Responses ranging from 3 to 6 were computed as an average within the specified frequency ranges (e.g., 3 = 3 to 5 times, average = 4). To reduce asymmetric and skewed distributions, extreme outliers were truncated. This method was described by Smamash (1981) and used in previous similar studies (Kan & Feinberg, 2010; Lee et al., 2022; Marshall et al., 2021). In this study, Cronbach’s αphysical violence and αpsychological violence were .60 and .84 at pre-intervention, and .71 and .95 at post-intervention, respectively. The CTS-2 has proven to have construct and discriminant validity (Straus et al., 1996), and its Spanish version has been widely administered in samples of IPV perpetrators (Lila et al., 2018). Risk of Recidivism Assessed by Facilitators. The risk of recidivism was assessed by facilitators using the Spousal Assault Risk Assessment Guide (SARA; Kropp et al., 1999; Spanish version by Andrés-Pueyo et al., 2008), a 20-item protocol with a clinical checklist format which includes the key risk factors for IPV to determine the risk of recidivism. Responses were given on a 3-point scale (0 = absent, 1 = possibly present, 2 = present). An overall score was used as the indicator of total risk of recidivism. A greater total score represents a higher risk of recidivism. SARA has demonstrated predictive validity (Messing & Thaller, 2013), and its Spanish version has been applied to samples of IPV perpetrators (e.g., Lila et al., 2018). Official IPV Recidivism (at 12-month follow-up). Recidivism data were obtained from the Ministry of Home Affairs’ monitoring system for IPV, VioGén (López-Ossorio et al., 2016). This official database includes data on acts of violence committed by individuals convicted of IPV or any breach of the mandatory restraining order and reported by the victim support services. Recidivism was coded as 0 = no recidivism when any further incident appeared in the system and as 1 = presence of recidivism when it appeared and occurred in the 12 months after completing the program. Proximal Outcomes Stage of Change. Facilitators assessed participants’ stage of change following the transtheoretical model of change of Prochaska & DiClemente (1982). It was coded as 1 = precontemplation, 2 = contemplation, 3 = preparation, 4 = action, and 5 = maintenance. Cohen’s kappa (k) was calculated to measure inter-rater agreement for this categorical item, accounting for agreement occurring by chance. The level of agreement among facilitators in this study was substantial (k = .70), consistent with Landis and Koch’s (1977) classification of strengths of agreement. Intervention Dose. The ratio of attended sessions to the total number of sessions provided. Active Participation. The ratio of homework activities completed by the participant to the total number of homework activities requested. Dropout. IPV perpetrators were coded as 0 = completers and 1 = dropout if they stopped attending the intervention. Data Analysis First, we examined the comparability of male participants in both conditions during the adjudication period. To compare categorical and continuous variables between conditions, we conducted chi-square and independent t-tests, respectively. The Mann-Whitney U test was used for continuous variables that did not follow a normal distribution. Sociodemographic variables, risk of recidivism, stage of change, and substance use variables (AUDIT, SDS cannabis, and cocaine) were included. Second, this procedure was also employed for conducting the attrition analysis, wherein potential dissimilarities in sample characteristics for the full sample were examined between completers and non-completers during adjudication. Third, to assess the effect of the treatment condition on the outcomes, different analyses were conducted. For variables with a single measurement, chi-square tests were used to compare categorical variables (e.g., official recidivism), whereas independent t-tests were used to compare continuous variables (e.g., intervention dose). For variables with pre- and post-test measurements (e.g., alcohol use), two-way repeated measures ANOVAs were conducted. The sphericity assumption was assessed using Mauchly’s test of sphericity. When sphericity was not assumed, corrected tests were applied. The Greenhouse-Geisser corrected test was used when the epsilon was lower than .75, and the Huynh-Feldt corrected test was used when the epsilon was greater than .75 (Armstrong, 2017). In addition, to quantify the magnitude of the results, effect size statistics were calculated. For continuous variables, Cohen’s d statistic was used for variables with one single measurement, and eta partial squared (η²p) for those with multiple measures. Cramér's V was used for categorical variables. When extreme outliers were identified, data were removed from the analysis. Results were analyzed using per-protocol (PP) and intention-to-treat (ITT) approaches. PP analyses were conducted for participants who completed the intervention. ITT analyses were conducted using the multiple imputation method (MI) for missing data and were performed for the dropouts’ post-intervention data of all variables except for intervention dose, active participation, dropout, and official recidivism. Despite the fact that any imputation method used to handle missing data is open to criticism (Tan et al., 2021), MI by fully conditional specification is considered a valid method for missing data in categorical and continuous variables (Y. Liu & De, 2015). ITT analyses are a valuable approach for estimating the effectiveness of an intervention, as it includes all randomized participants, regardless of their adherence to the treatment protocol (Gupta, 2011). This ensures that the results are representative of real-world conditions and maintain prognostic balance (Gupta, 2011; McCoy, 2017). Finally, two-way repeated measures ANOVAs were performed to assess the durability of the results at the 12-month follow-up. The sphericity assumption was assessed using Mauchly’s test of sphericity and its corrected tests (Armstrong, 2017). Additionally, the eta partial squared (η²p) was calculated. The same procedure was applied to evaluate the effect of the treatment condition on the outcomes at pre-, post- and follow-up on the ADUPs subsample. This study was adequately powered to detect small (d = 0.25, n = 34), medium (d = 0.50, n = 12) and large effects (d = 0.80, n = 6) with 80% power (α = .05) both in the per-protocol and follow-up analysis (n = 28, 10, and 6, respectively). All statistical analyses were conducted using SPSS 28.0.1.1. Transparency and Openness In this study, the methodologies employed for ascertaining the sample size, data exclusion, and measuring variables are elucidated. The guidelines outlined in the Journal Article Reporting Standards (JARS; Applebaum et al., 2018) were adhered to. Data and research materials are not available because the participants are under court order and their confidentiality must be always maintained. SPSS 28.0.1.1. syntax is available upon request from the first author. Group Assignment and Allocation Figure 1 provides the description of participant flow from recruitment to study completion and 12-month follow-up. Men assessed for eligibility were convicted of IPV and referred by the probation system (n = 167). Twenty-seven men were excluded from the study, mainly because they did not attend the initial meeting (n = 19). Two declined to participate in the study. Four did not meet the inclusion criteria: they had severe physical conditions and/or mental health problems (i.e., major depression, psychotic symptomatology, hernia surgery, and anxiety disorder). The diagnosis of severe physical and mental health problems was conducted by psychiatrists and other relevant specialists from the National Health System. The other two men were excluded for other reasons. Specifically, they were unable to attend due to living a significant distance away from the program. Groups were randomly assigned to IMP or IMP-ADUPs condition. Twelve groups were formed (69 and 71 participants in IMP and IMP-ADUPs condition, respectively). Groups had an average of 11 men. The allocated intervention was received by 51 participants in the standard IMP condition and by 56 in the IMP-ADUPs condition. The main reason why participants discontinued the intervention was non-compliance with program rules (n = 8 in each condition; see Figure 1). With regards to the 12-month follow-up, 41 participants were assessed, including 22 participants in the standard IMP condition and 19 in the IMP-ADUPs condition. The main cause for not completing the 12-month follow-up was that participants could not be contacted (19 and 21 participants in IMP and IMP-ADUPs condition, respectively). Figure 1 Flow Diagram 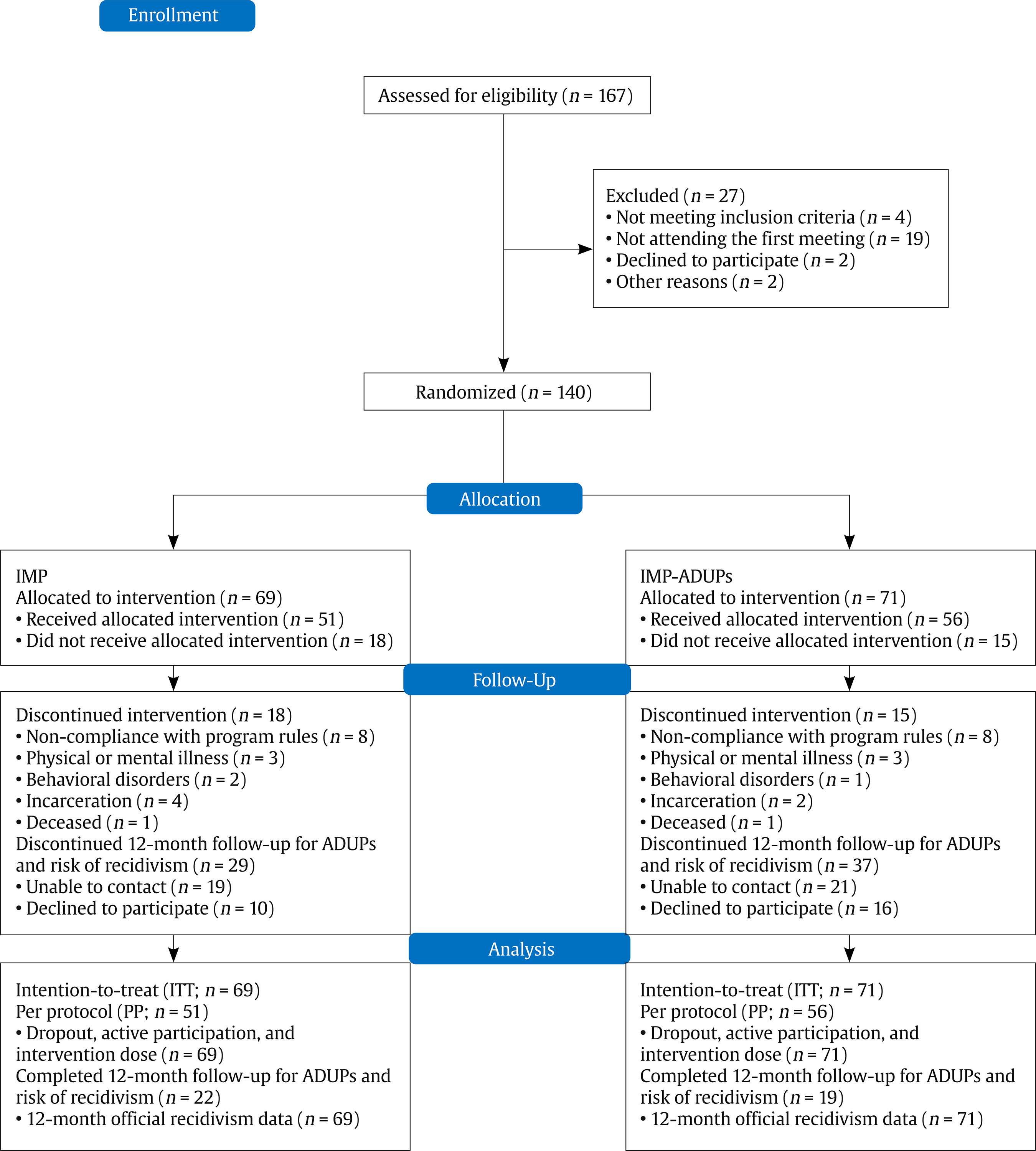 Baseline Characteristics Table 1 displays a comparison of the baseline characteristics of participants in each treatment condition and across the full sample and ADUPs subsample. The results obtained showed that the randomization process was successful. Eleven variables were compared between control and experimental groups, none of which reached significance (p ≤ .05). Consequently, the groups were statistically equivalent on baseline characteristics in each condition in both the full sample and the ADUPs subsample. Table 1 Comparison of Baseline Characteristics in Each Treatment Condition 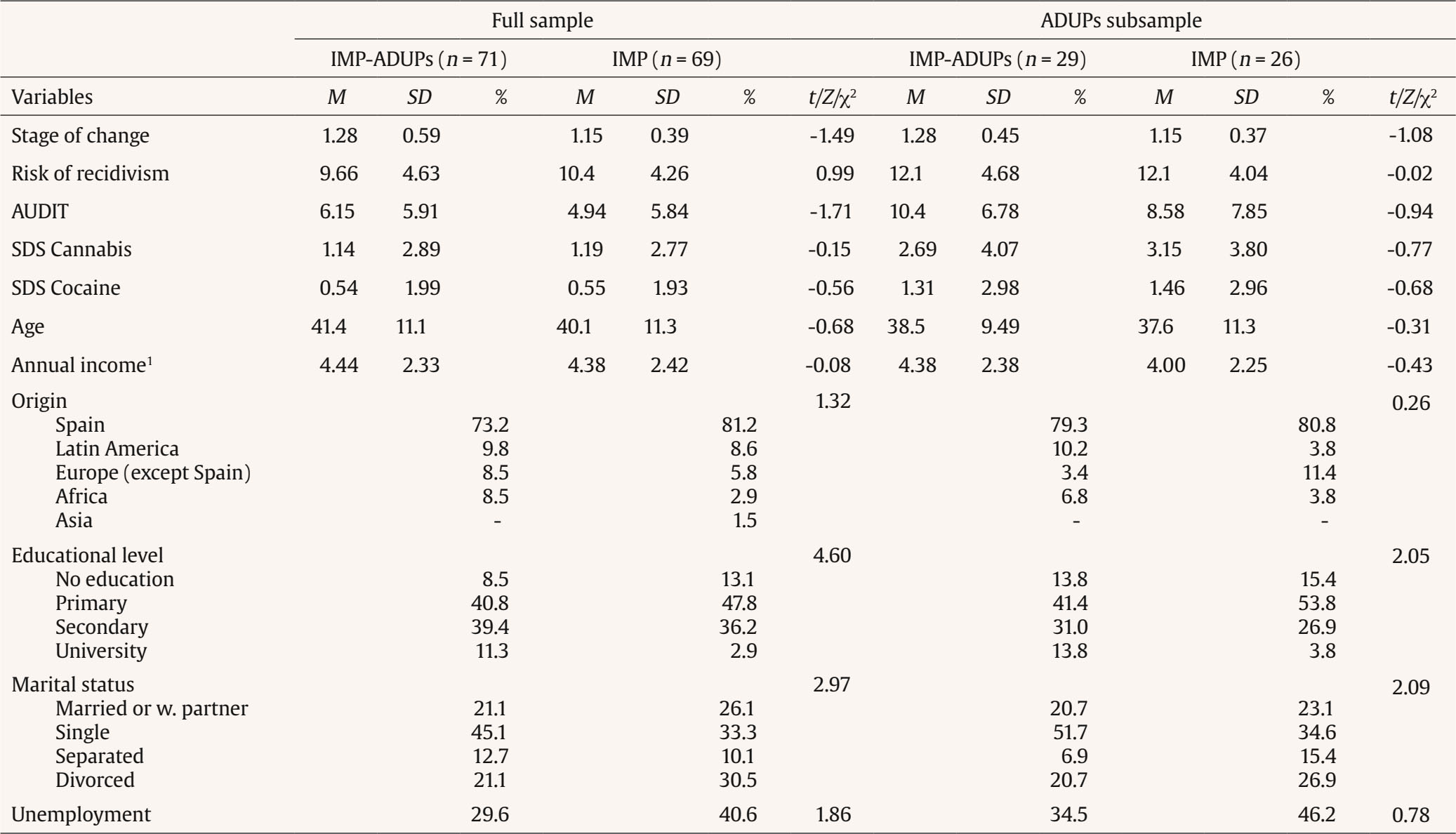 Note. ADUPs = Alcohol and/or other Drug Use Problems; IMP-ADUPs = Individualized Motivational Plan adjusted to Alcohol and/or other Drug Use Problems; IMP = Individualized Motivational Plan; M = Mean; SD = Standard Deviation; t = independent t test; Z = Mann-Whitney U test; χ2 = chi-square test; AUDIT = Alcohol Use Disorders Identification Test; SDS = Severity of Dependence Scale. 1 Annual income: 1 ≤ €1,800, 2 = €1,800-€3,600, 3 = €3,600-€6,000, 4 = €6,000-€12,000, 5 = €12,000-€18,000, 6 = €18,000-€24,000, 7 = €24,000-€30,000, 8 = €30,000-€36,000, 9 = €36,000-€60,000, 10 = €60,000-€90,000, 11 = €90,000-€120,000, and 12 ≥ €120,000. All comparisons were not significant at the .05 level. Attrition Analysis Several analyses were conducted to assess if there were disparities between participants who finished the intervention program and those who did not at the time of adjudication. Overall, 23.6% (n = 33) of the participants dropped out of the intervention. Specifically, completion rates did not differ between IMP and IMP-ADUPs conditions, χ2(1) = 0.48, p = .489, with 73.9% (n = 51) of participants in the IMP condition completing the intervention, and 78.9% (n = 56) in the IMP-ADUPs. For non-completers, the number of sessions attended ranged from 1 to 21, with a mean of 3.33 (SD = 5.44) for IMP non-completers and 4.07 (SD = 6.78) for IMP-ADUPs non-completers. Analyses of baseline characteristics of completers and non-completers revealed differences in income and unemployment. Specifically, completers reported higher annual income levels (Z = -3.34, p < .001) and lower rates of unemployment (χ2 = 5.18, p = .023). Final Outcomes Full Sample Table 2 presents the descriptive statistics for the final outcome variables in the PP and ITT samples. All participants in the PP sample reported lower levels of alcohol use after the intervention, F(1, 104) = 4.48, p = .037, η2p = .04. This result was also consistent in the ITT sample, F(1, 138) = 4.95, p = .028, η2p = .04. Further, there was a significant effect for condition-by-time interaction, as participants in the IMP-ADUPs condition showed a significant reduction in alcohol use post-intervention, while those in the IMP condition maintained their alcohol use, F(1, 104) = 5.76, p = .018, η2p = .05, in the PP sample. This finding was not replicated in the ITT sample. Finally, all participants in the PP and ITT samples reduced their risk of recidivism as assessed by facilitators at the end of the intervention, F(1, 105) = 46.4, p < .001, η2p = .31; F(1, 138) = 76.9, p < .001, η2p = .36, respectively, although there were non-significant effects on condition-by-time interaction. Non-significant time or condition-by-time interaction effects were also found for cocaine and cannabis dependence and self-reported psychological and physical IPV (p > .05). Table 2 Comparison on Final and Proximal Outcomes over Time by Condition in the Full Sample 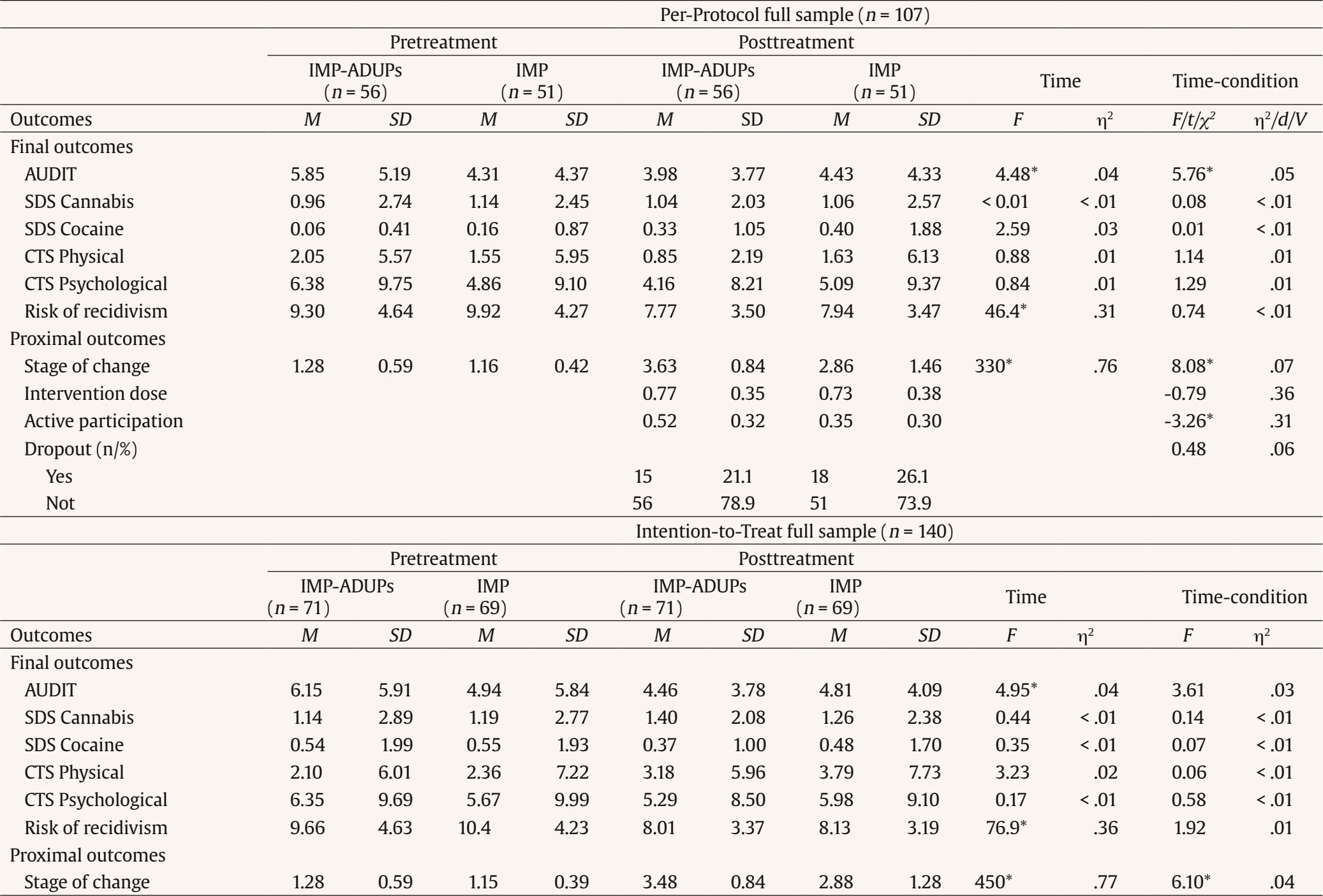 Note. ADUPs = Alcohol and/or other Drug Use Problems; IMP = Individual Motivational Plan; IMP-ADUPs = Individualized Motivational Plan Adjusted to Alcohol and/or other Drug Use Problems; M = Mean; SD = Standard Deviation; AUDIT = Alcohol Use Disorders Identification Test; SDS = Severity of Dependence Scale; CTS = Conflict Tactics Scale. * p ≤ .05. ADUPs Subsampl Table 3 displays the descriptive statistics of the final outcome variables for the PP and ITT samples. Participants reported lower levels of alcohol use post-intervention both in the PP, F(1, 37) = 7.62, p = .009, η2p = .17, and ITT sample, F(1, 53) = 14.5, p < .001, η2p = .22. Furthermore, there was a significant effect for condition-by-time interaction in the PP sample, as participants in the IMP-ADUPs condition reported a greater reduction in alcohol use, while participants in the IMP condition maintained their level of alcohol use, F(1, 37) = 6.25, p = .017, η2p = .15. This effect was not found in the ITT sample. Finally, although there were non-significant effects on the interaction between condition and time on the risk of recidivism assessed by facilitators, all participants in the PP and ITT samples reduced their risk of recidivism after the intervention, F(1, 37) = 19.6, p < .001, η2p = .35; F(1, 53) = 40.7, p < .001, η2p = .44; respectively. Non-significant time or condition-by-time interaction effects were found for cocaine and cannabis dependence and self-reported psychological and physical IPV (p > .05). Table 3 Comparison on Final and Proximal Outcomes over Time by Condition in the ADUPs Subsample 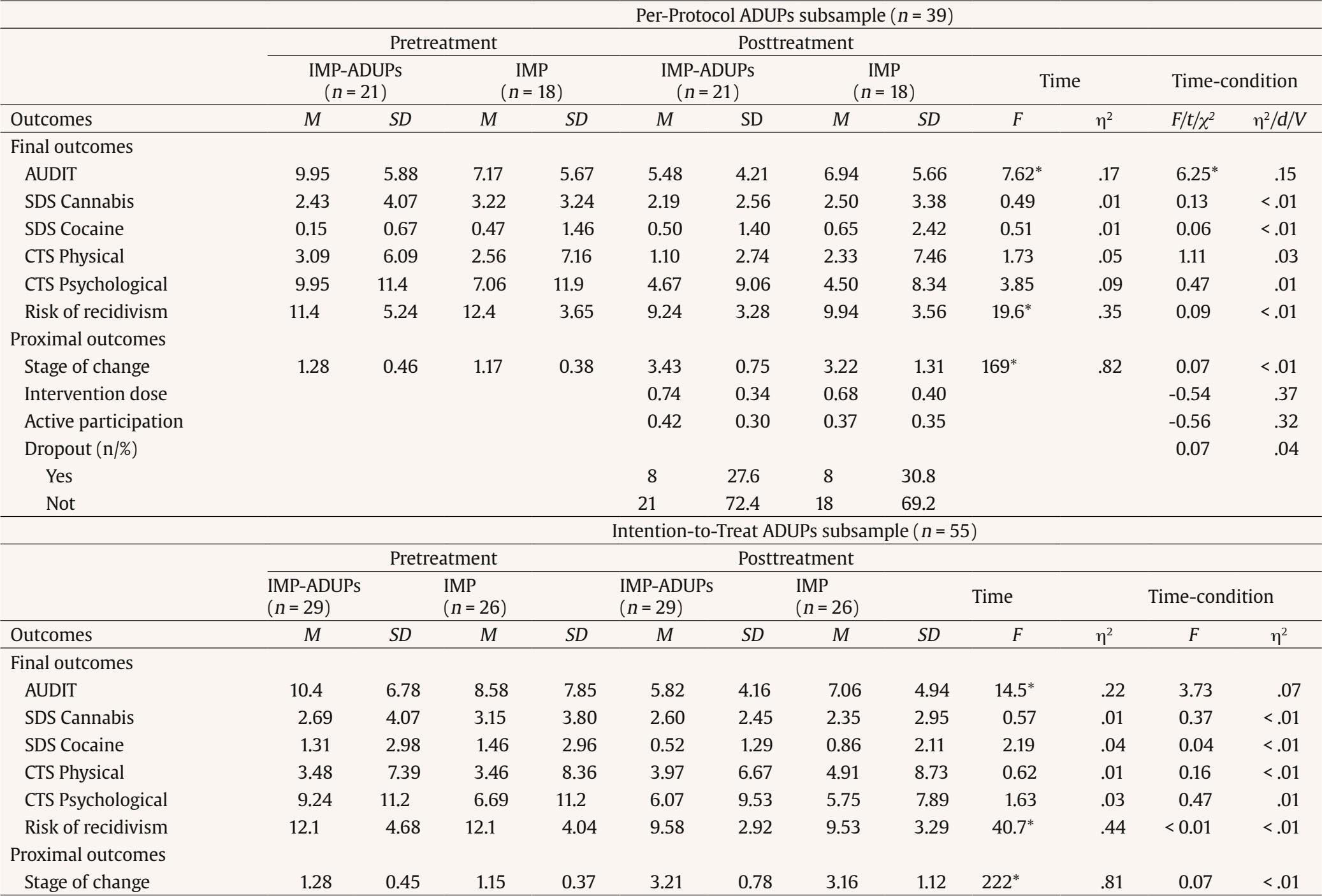 Note. ADUPs = Alcohol and/or other Drug Use Problems; IMP = Individualized Motivational Plan; IMP-ADUPs = Individualized Motivational Plan Adjusted to Alcohol and/or other Drug Use Problems; M = Mean; SD = Standard Deviation; AUDIT = Alcohol Use Disorders Identification Test; SDS = Severity of Dependence Scale;CTS = Conflict Tactics Scale. * p ≤ .05. Proximal Outcomes Full Sample Descriptive statistics for the proximal outcome variables in the PP and ITT samples are presented in Table 2. Participants in the IMP-ADUPs condition showed more active participation during the intervention than participants in the IMP condition, t(138) = -3.26, p < .001, d = 0.31. In relation to the stage of change in the PP sample, a generalized significant positive progression was observed for all participants, F(1, 105) = 330, p < .001, η2p = .76. Further, participants in the IMP-ADUPs condition showed greater progress than participants in the IMP condition, F(1, 105) = 8.08, p = .005, η2p = .07. Both time and condition-by-time interaction effects in the stage of change were also found in the ITT sample, F(1, 138) = 450, p < .001, η2p = .77; F(1, 138) = 6.1, p = .015, η2p = .04; respectively. Non-significant differences between conditions were found for intervention dose and dropout (p > .05). ADUPs Subsample Descriptive statistics for the proximal outcome variables in the PP and ITT samples are presented in Table 3. All participants in the PP and ITT samples demonstrated a generalized significant positive progression in their stage of change at the end of the intervention, F(1, 37) = 169, p < .001, η2p = .82; F(1, 53) = 222, p < .001, η2p = .81, respectively), although non-significant effects were found on the interaction between condition and time. These interaction effects were also non-significant for intervention dose, active participation, and dropout (p > .05). 12-Month Follow-up Finally, differences in final outcomes were assessed after 12 months of follow-up. Table 4 shows the descriptive statistics in the full and ADUPs subsample. Participants reported significant reductions in alcohol use, F(2, 78) = 9.91, p < .001, η2p = .2, and risk of recidivism, F(2, 78) = 21.9, p < .001, η2p = .36, after follow-up, although non-significant effects were found for condition-by-time interaction. These results were also found in the ADUPs subsample. ADUPs participants had significantly lower rates of alcohol use, F(2, 28) = 7.91, p = .002, η2p = .36, and risk of recidivism, F(2, 28) = 10.4, p < .001, η2p = .43, at the end of the intervention, while non-significant effects were found for the interaction between condition and time. Non-significant time or condition-by-time interaction effects were also found for official recidivism and cocaine and cannabis dependence (p > .05). Table 4 Comparison on Final Outcomes over Time by Condition after 12-month Follow-up 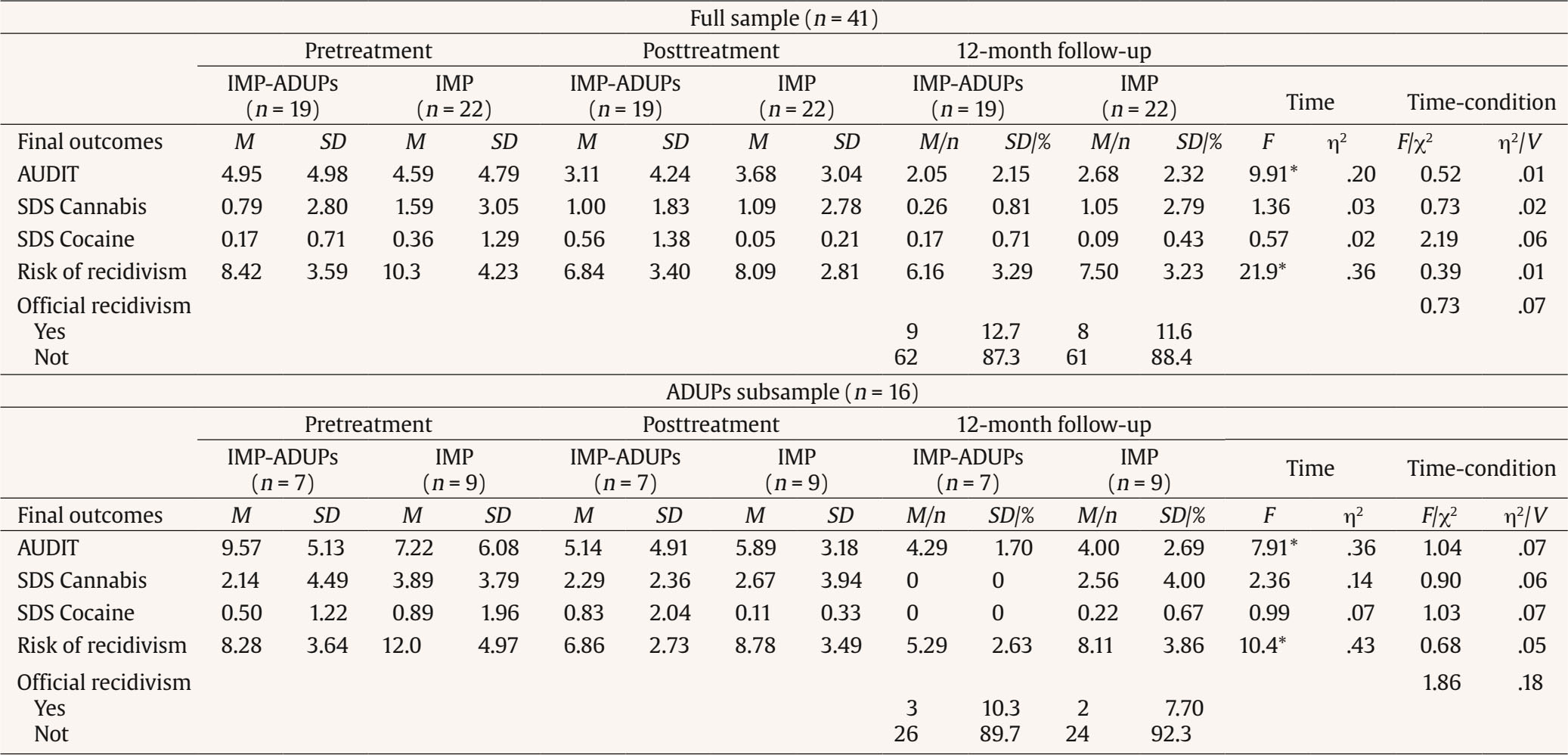 Note. ADUPs = Alcohol and/or other Drug Use Problems; IMP-ADUPs = Individualized Motivational Plan Adjusted to Alcohol and/or other Drug Use Problems; IMP = Individualized Motivational Plan; M = Mean; SD = Standard Deviation; AUDIT = Alcohol Use Disorders Identification Test; SDS = Severity of Dependence Scale. * p ≤ .05. Previous reviews have suggested the potential benefits of addressing ADUPs in intervention programs for IPV perpetrators by including integrated, motivational strategies to promote change in men (Karakurt et al., 2019; Murphy & Ting, 2010; Pinto e Silva et al., 2023). As a result, new intervention approaches have been recently developed which aim to move beyond a “one-size-fits-all” model approach to tailoring interventions to the risks and needs of high-risk IPV perpetrators, such as those with ADUPs, as a way to increase programs’ effectiveness (Leonard & Quigley, 2017; Radatz & Wright, 2016; Richards et al., 2022). The aim of this RCT was to evaluate whether an IMP adjusted to ADUPs (i.e., IMP-ADUPs) was superior to standard individual motivational strategies (i.e., IMP) in improving proximal and final outcomes in men court-mandated to attend an intervention program for IPV perpetrators and specifically in those with ADUPs. Results revealed that incorporating IMP-ADUPs was more effective in reducing alcohol use among the full sample of IPV perpetrators, compared to the standard IMP. Reducing alcohol has been acknowledged as a key strategy to reduce further IPV (Easton & Crane, 2016; Gilchrist et al., 2021; Leonard & Quigley, 2017) since it has been recognized as a criminogenic factor that increases the likelihood of participants to perpetrate more severe violence and reoffend (Cafferky et al., 2018; Hilton & Radatz, 2021; Olver et al., 2011). The IMP-ADUPs condition was also superior to the IMP condition in increasing participants’ active participation and promoting progress in the stage of change among the full sample of IPV perpetrators. These findings hold significant importance since improving treatment adherence and motivation to change are two of the main challenges to improving the effectiveness of court-mandated intervention programs for IPV perpetrators (Cunha et al., 2024; Richards et al., 2022; Travers et al., 2021). Thus, tailoring motivational strategies to address ADUPs (i.e., IMP-ADUPs) may have additional potential benefits over the standard IMP for all participants, which is an important finding considering the documented efficacy of the IMP among court-mandated IPV perpetrators (Lila et al., 2018; Romero-Martínez, Lila, Gracia, et al., 2019; Santirso, Lila, et al., 2020). Our results also indicated that the significantly greater reduction in alcohol use in the IMP-ADUPs condition relative to the IMP condition did not persist when considering the ITT analysis. This discrepancy may be attributed to the inclusion of imputed post-intervention data from the initial assessments of participants who dropped out, who tend to have higher rates of alcohol and drug use, thus attenuating the observed reduction in alcohol use within the PP sample (Jewell & Wormith, 2010; Lila et al., 2020). This finding underscores the importance of enhancing retention strategies to minimize participant dropout rates and strengthen their commitment to reducing alcohol use throughout the intervention program (Crane et al., 2015; Expósito-Álvarez et al., 2024; Taft & Murphy, 2007). When evaluating the effectiveness of this new motivational tool in the subsample of IPV perpetrators with ADUPs, it was also observed a significantly greater reduction in alcohol use after the intervention in the IMP-ADUPs condition compared to the standard IMP within the PP sample. This finding supports the inclusion of IMP-ADUPs in such programs to reduce alcohol use in both whole groups of IPV perpetrators and specifically in participants with ADUPs. Our results also showed that participants with ADUPs in the IMP-ADUPs condition did not display significant improvements compared to those in the IMP condition across the remaining analyzed outcomes. It is noteworthy that participants with ADUPs have been identified as a high-risk group of IPV perpetrators, so improving their outcomes can be especially challenging (Expósito-Álvarez et al., 2021, 2023; Lila & Gilchrist, 2023; Mootz et al., 2022). Providing intervention programs with more robust, integrated strategies specifically targeting ADUPs may further reduce both IPV and ADUPs, fostering improved treatment outcomes in IPV perpetrators with ADUPs (Easton et al., 2018; Kraanen et al., 2013). This RCT also showed that participants exhibited significant improvements at the end of the intervention in several variables regardless of the condition they were randomly assigned to, and their ADUPs status. For instance, both participants in the IMP-ADUPs or IMP conditions reduced their risk of recidivism at the end of the intervention, suggesting the overall efficacy of motivational interventions for the full sample of IPV perpetrators and for those with ADUPs. In addition, participants with ADUPs made significant progress in their stage of change at the end of the intervention in both the IMP and IMP-ADUPs conditions. This is consistent with prior research showing greater participants’ motivation to change after implementing motivational strategies in intervention programs for IPV perpetrators (Murphy et al., 2020; Santirso, Lila, et al., 2020; Soleymani et al., 2022). Moreover, this study found non-significant effects on time or condition-by-time interaction for self-reported cocaine and cannabis use and self-reported psychological and physical IPV. More efforts should be made in this direction to improve such outcomes. For instance, developing a coordinated response with victim-support services that assist in obtaining victim-related IPV reports or data assessed by professionals could help perpetrator programs collect more accurate and reliable information regarding participants’ disclosures of IPV (Graham et al., 2021). In addition, self-reported measures might introduce potential biases, such as social desirability at intake or increased disclosure of substance use and IPV at the end of the intervention due to increased self-awareness (Tutty et al., 2020). Future studies should employ specific measures to control these effects. However, one strength of this study is that it included IPV recidivism data assessed by facilitators, which showed significant improvements at the end of the intervention across samples and conditions. Dropout rates did not differ significantly between conditions. Specifically, the dropout rate was 21.1% in the IMP-ADUPs condition and 26.1% in the IMP condition. Notably, a recent systematic review found an average dropout rate of 35.44% in intervention programs for IPV perpetrators (Cunha et al., 2024). This may suggest that the absence of significant differences between conditions could be attributed to the below-average dropout rate observed in both groups, rendering it challenging for substantial differences to manifest. Adding to this, a study conducted by Expósito-Álvarez et al. (2024) showed that goal setting, which is a core strategy in the IMP of both conditions, predicted lower dropout rates both in a full sample of IPV perpetrators and in those with ADUPs. This may indicate that the IMP could help reduce dropout rates and increase intervention dose irrespective of whether participants’ goals addressed ADUPs or other relevant issues (Waller, 2016). Following the research recommendation proposed by Stuart et al. (2013), we conducted a 12-month follow-up analysis aimed to evaluate substance use, official recidivism, and risk of IPV recidivism in the IMP-ADUPs group relative to the standard IMP group. Results indicated a significant time effect for alcohol use and risk of recidivism both in the full sample of IPV perpetrators and among those with ADUPs. Specifically, participants significantly reduced their alcohol use and their risk of IPV recidivism both in the IMP and IMP-ADUPs condition at 12-month follow-up, which underscored the enduring positive effects of the motivational strategies. Official recidivism rates, though not statistically different between conditions, were low and similar to those reported in previous research (Lila et al., 2018). Given the limited sample size at the 12-month follow-up in the current trial, there is an increased risk of Type II error, potentially resulting in false negatives. To address this concern, future research should use larger sample sizes or employ appropriate statistical procedures to mitigate this risk (Freiman et al., 2019). Moreover, developing and implementing specific evidence-based strategies designed to address additional risk factors associated with ADUPs among IPV perpetrators, such as impulsivity and anger management techniques or trauma-informed components, hold promise for enhancing participants’ outcomes and reducing IPV recidivism (Karakurt et al., 2019; McKenna & Holtfreter, 2021; Travers et al., 2022). Overall, the IMP-ADUPs intervention was superior to the IMP in reducing alcohol use at post-intervention among the full sample of IPV perpetrators and the subsample of perpetrators with ADUPs. In addition, the IMP-ADUPs showed greater improvements relative to the IMP intervention in promoting active participation and fostering a more advanced stage of change among the full sample of IPV perpetrators at the end of the intervention. This could be explained by the fact that many participants, although not meeting the criteria for ADUPs, may engage in culturally normalized substance use behaviors and benefit from the knowledge of the negative consequences of ADUPs on their intimate relationship (Satyanarayana et al., 2015; Stephens-Lewis et al., 2021). Further, group dynamics within the intervention program may facilitate shared reflection and support, promoting active participation and amplifying the impact of these strategies on increasing participants’ self-awareness of their need to change (Murphy et al., 2020; Roldán-Pardo et al., 2024). Our results have important treatment implications since they help inform program facilitation and design about the potential effectiveness of addressing ADUPs in the IPV perpetrators’ groups. Further intervention efforts should be made to adjust the interventions to high-risk IPV perpetrators’ specific risks and needs (Babcock et al., 2024; Butters et al., 2021; Massa et al., 2020; Travers et al., 2021). This study has certain limitations. First, this study relied on self-reported measures to identify participants with ADUPs, potentially limiting the accuracy in correctly identifying this subgroup of participants. Second, due to Spanish legislation restrictions, intervention programs for IPV perpetrators are restricted from obtaining information that could identify victims and contact them, hence hampering the ability of this study to use victim-related data (Lila et al., 2018) or provide support to participant’s current or ex-partners. However, a strength of this study is that it uses data from three different sources (e.g., self-reported by participants, assessed by facilitators, and official IPV data). Third, our ability to detect statistically significant effects, particularly at the 12-month follow-up, would have been enhanced with a larger sample size, which would have increased the power of the study. Fourth, with regards to the double-blind process, and due to the nature of the interventions and their extended duration (i.e., approximately one year), there is a possibility that some facilitators may have inferred the existence of different conditions over time. Future studies should implement a verification procedure to ensure the integrity of the blinding process and evaluate how successful it was for both participants and facilitators (Bang et al., 2010). In addition, although two supervisors monitored treatment fidelity through a one-way mirror, future studies could quantitatively evaluate facilitators’ adherence to the intervention protocols. Another potential limitation could be related to the additional 15 hours of training on ADUPs that facilitators in the IMP-ADUPs condition received. While it is unlikely that these limited additional hours had a significant impact due to their small proportion of the total training, their potential impact on the facilitators’ therapeutic skills should be acknowledged. Finally, this study’s participants’ sample characteristics could limit the generalizability of results to other populations, such as imprisoned men, or other partnerships that may involve IPV, such as the LGBTIQ+ population (Gilchrist et al., 2023; M. Liu et al., 2021). Notwithstanding these limitations, this study has some strengths. RCTs evaluating the effectiveness of integrated motivational strategies addressing ADUPs and IPV are still scarce (Mbilinyi et al., 2023; Murphy et al., 2018; Stuart et al., 2013). To our knowledge, this is the first RCT conducted in a Spanish-speaking country which compares the efficacy of integrated motivational strategies to standard motivational strategies among both a full sample of IPV perpetrators and a full sample of participants with ADUPs. Our results underscore the need to develop individualized approaches which aim to reduce the risk of IPV recidivism, foster participants’ willingness to change, and promote healthier and safer intimate relationships. Conflict of Interest The authors of this article declare no conflict of interest. Funding: This study was supported by PROMETEO 2022: Projects for Research Excellence Groups (CIPROM/2021/46), Generalitat Valenciana, and the National Drugs Plan of the Spanish Ministry of Health, Consumption and Social Services (PND2018/021). Cristina Expósito-Álvarez was supported by the FPU program and the complementary grant for international mobility of the Spanish Ministry of Universities (FPU19/05278; EST22/00468). Manuel Roldán-Pardo was supported by the ACIF Program of the Generalitat Valenciana (ACIF/2021/362). Cite this article as: Expósito-Álvarez, C., Roldán-Pardo, M., Gilchrist, G., & Lila, M. (2024). Integrated motivational strategies for intimate partner violence perpetrators with substance use: A randomized controlled trial. Psychosocial Intervention, 33(3), 187-200. https://doi.org/10.5093/pi2024a13 |
Cite this article as: Expósito-Álvarez, C., Roldán-Pardo, M., Gilchrist, G., & Lila, M. (2024). Integrated Motivational Strategies for Intimate Partner Violence Perpetrators with Substance Use: A Randomized Controlled Trial. Psychosocial Intervention, 33(3), 187 - 200. https://doi.org/10.5093/pi2024a13
Correspondence: Marisol.Lila@uv.es (M. Lila).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
Send






