


Home-visiting Parenting Programs to Improve Mother-Infant Interactions at Early Ages: A Systematic Review
Claudia R. L. Alves1, Bruna L. Seibel2, Cláudia M. Gaspardo3, Elisa R. P. Altafim3, and Maria B. M. Linhares3
1Federal University of Minas Gerais, Brazil; 2Federal University of Rio Grande, Brazil; 3University of SĂŁo Paulo, Brazil
https://doi.org/10.5093/pi2024a7
Received 18 July 2023, Accepted 2 February 2024
Abstract
Objective: To systematically review studies examining the effects of home-visiting preventive parenting programs (HV-PPs) on improving the quality of mother-child interactions in early childhood. Method: Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses protocol, we identified 3,586 studies published between 2018 and 2022 by searching the following databases: PubMed, Web of Science, BVS/LILACS, SciELO, and PsycNET/PsycINFO. After applying the eligibility criteria, 17 articles were selected for review. Results: Most studies were conducted in high-income countries (53%) and the remainder were conducted in upper-middle-income countries, predominantly using a randomized controlled trial design and with strong methodological quality. The 17 studies applied 13 different HV-PPs, predominantly using video feedback, based on various dosages and schedules. Most studies (77%) showed significant positive effects on mother-child interactions by improving mainly positive maternal behaviors (e.g., sensitivity and responsiveness). Positive effects occurred independent of the study design, sample characteristics, measures, and constructs assessed. However, the findings suggest that the combination of fewer than six sessions, durations shorter than three months, and a very early start did not impact mother-child interactions, as expected. Few studies have explored negative maternal behaviors, children’s behaviors, and dyadic interactions such as mutuality and synchrony. Conclusions: HV-PPs positively impacted mother-child interactions in early childhood despite the large heterogeneity across program designs, outcome measures, and overlapping constructs. Based on the results, we discuss the practical and economic implications of using parenting programs as a preventive approach.
Keywords
Mother-child interactions, Parenting programs, Preventive interventions, Home-visiting programsCite this article as: Alves, C. R. L., Seibel, B. L., Gaspardo, C. M., Altafim, E. R. P., & Linhares, M. B. M. (2024). Home-visiting Parenting Programs to Improve Mother-Infant Interactions at Early Ages: A Systematic Review. Psychosocial Intervention, 33(2), 117 - 132. https://doi.org/10.5093/pi2024a7
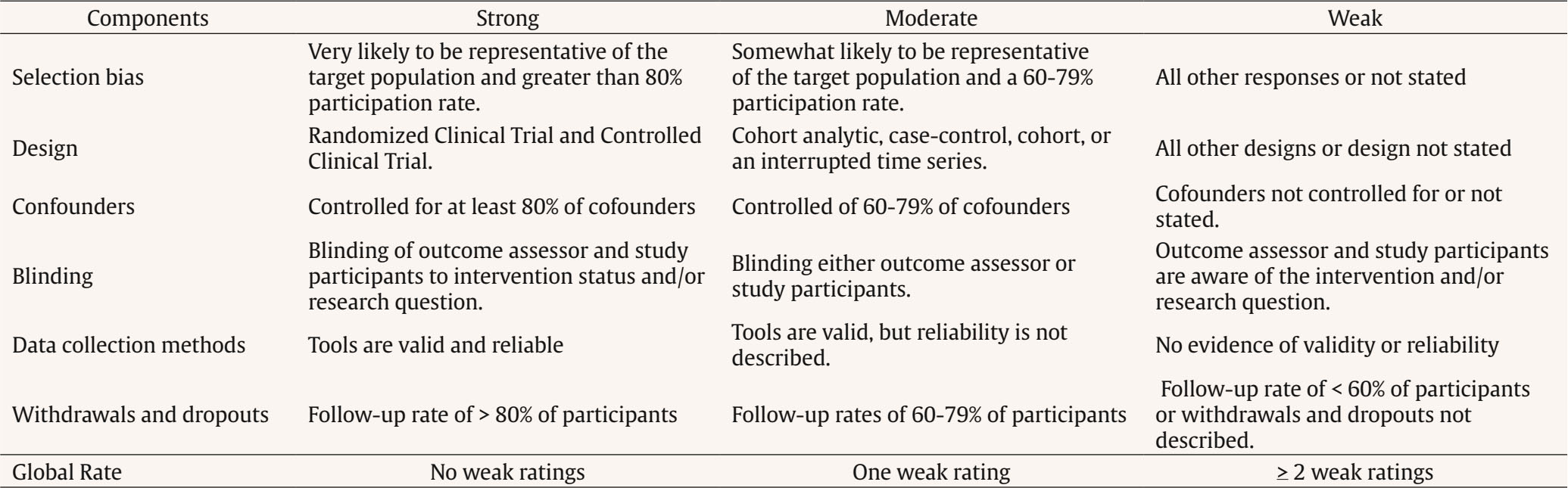
Correspondence: lindgrenalves@gmail.com; lindgren@ufmg.br (Claudia R. L. Alves)The slogan “If we change the beginning of the story, we change the whole story” (World Health Organization et al., 2018) highlights the priority and urgency of investing in early childhood development. Investments in early childhood positively impact children’s lives and enhance human capital, supporting society’s development and bringing lifelong benefits (Britto et al., 2017; Daelmans et al., 2015). The Nurturing Care Framework is a roadmap that supports countries in developing and implementing evidence-based actions to ensure opportunities for young children’s development and well-being (World Health Organization et al., 2018). In this sense, a stable familial environment sensitive to children’s needs that provides protection, opportunities for learning, and responsive interactions should be at the core of interventions targeting child development and health outcomes (Bornstein et al., 2022; Britto et al., 2017; Jeong et al., 2022). Globally, several interventions have been proposed to improve early childhood development (Bornstein et al., 2022; Britto et al., 2017; Britto et al., 2015; Jeong et al., 2021). Beyond cognitive stimulation, intergenerational approaches supporting caregivers’ parenting skills, such as parent-child responsive interaction and positive parenting, are powerful, longstanding, and cost-benefit strategies for promoting child development (Britto et al., 2017; Fisher et al., 2016; Jeong et al., 2021; Shonkoff & Fisher, 2013; Tereno et al., 2019). In early childhood, mother-child interactions are particularly important for establishing secure attachment, preventing behavioral and mental disorders, and developing resilience in the face of adverse situations throughout life (Bernier et al., 2016; Goldblatt et al., 2014; Vu et al., 2015). Mother-child interactions can be positively affected by parenting interventions aimed at improving and supporting positive parenting behaviors, knowledge, beliefs, attitudes, and practices, consequently promoting children’s socio-emotional, cognitive, and language development and self-regulation (Bornstein et al., 2022; Britto et al., 2017; Britto et al., 2015; Fisher et al., 2016; Jeong et al., 2021; Obradovic´ et al., 2016). Moreover, the quality of mother-child interactions can positively and negatively affect cognitive, language, and social outcomes during the first year of life (Rocha et al., 2020). Despite the considerable heterogeneity across models, contents, and measures, a convergent result of previous reviews is that preventive interventions improve parenting outcomes such as parenting knowledge and practices (Britto et al., 2015; Jeong et al., 2021; Jeong et al., 2018; Morrison et al., 2014), psychosocial outcomes (Barlow et al., 2011; Britto et al., 2017; Britto et al., 2015), and positive parent-child interactions (Jeong et al., 2021; Jeong et al., 2018; Letourneau et al., 2015; Shah et al., 2016). Among preventive interventions, home-visiting programs are considered the oldest and most widely used to promote positive parenting (Bakermans-Kranenburg et al., 2003; Britto et al., 2015; Duffee et al., 2017; Finello et al., 2016; Jeong et al., 2021; Jeong et al., 2018; Morrison et al., 2014; Mountain et al., 2017). Home visits provide support and information that enable families and caregivers to provide nurturing care for children (World Health Organization et al., 2018; World Health Organization & UNICEF, 2022). On this topic, in their meta-analysis, Jeong et al. (2021) found that from 102 randomized controlled trials (RCTs) published before 2020, 75% of the programs were delivered at home or in a combination of other settings (e.g., community settings, health clinics). According to previous studies, the impact of interventions relies on program characteristics (e.g., duration, intensity, tools, provider) as well as on sample characteristics (e.g., multiple risks, children’s and mothers’ age), and these aspects interact, modeling the effect size of the interventions (Bakermans-Kranenburg et al., 2003; Britto et al., 2015; Bower et al., 2020). However, Jeong et al. (2021) did not find evidence that child age, intervention duration, delivery, setting, or risk of bias in the studies modified the effect of the interventions but noted that the context in which the programs were implemented and their content did. The authors showed that programs implemented in low- and middle-income countries (LMICs) have greater effects than those implemented in high-income countries. Additionally, programs focused on responsive caregiving were nearly four times more effective in improving parenting outcomes than those that used other approaches, such as programs that provided information on child development, parental stimulation, and/or learning materials (Jeong et al., 2021). Historically, home visiting programs were thought to be a universal approach across many health-focused services (Dufee et al., 2017; Finello et al., 2016) and nowadays, are one of the main strategies to support families and children at risk, such as low-income families and adolescent parents, or with additional needs (World Health Organization & UNICEF, 2022). In this sense, many programs, despite being designed to be universal, address mothers or children with clinical conditions, such as maternal depression, autism spectrum disorders, or infants at biological risk for developmental disorders (Bornstein et al., 2022; Ferreira et al., 2020; Mountain et al., 2017; Puthussery et al., 2018). Nevertheless, there is still a need to understand how well the home-visiting parenting programs work and fit the population without clinical conditions. Furthermore, most studies have focused on child development and behavior, and few have explored the crucial role of mother-child interaction in child development, as highlighted by Jeong et al. (2021) and Jeong et al. (2022). Previous reviews (Bakermans-Kranenburg et al., 2003; Britto et al., 2017; Mountain et al., 2017; Shah et al., 2016) have demonstrated robust evidence of the positive effects of home-visiting parenting programs (HV-PPs) on early childhood development and parenting outcomes. Recently, a systematic review by Jeong et al. (2021) analyzed 102 unique RCTs designed to assess the effectiveness of parenting interventions on early child development and parenting outcomes. This review included studies published up to November 2020 and found that 69% used responsive caregiving components to improve parent-child interactions (n = 70). However, only 24 studies specifically analyzed the impact of home visiting programs on parent-child interactions, and most of them (n = 19) were published before 2018 (Jeong et al., 2021). Considering previous reviews were very heterogeneous regarding the intervention design and parenting outcomes, there is a need to focus exclusively on HV-PPs addressing the mother-child interaction outcomes in early childhood. Furthermore, most studies analyzed in previous reviews were published before the Nurturing Care Framework was announced in 2018 (Britto et al., 2017; World Health Organization et al., 2018). This framework is a benchmark for studying responsive caregiving in early childhood. Therefore, there is still a need to examine the evidence on this topic after this timeframe. The present study aimed to systematically review empirical studies published in the scientific literature that examined the effects of home-visiting parenting programs delivered to improve the quality of mother-child interactions in early childhood. The following questions guided this review: (i) What are the main characteristics of HV-PPs? (ii) What constructs and measures were used to assess the quality of mother-child interactions (main outcome)? (iii) What were the main effects of HV-PPs on mother-infant interactions? (iv) What was the methodological care of the studies reviewed? The systematic review protocol was registered on the PROSPERO platform on 09/13/2019 (CRD42020151122). This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statements (Page et al., 2021). We performed a formal narrative synthesis based on the Synthesis Without Meta-analysis (SWiM) guidelines (Campbell et al., 2018). Eligibility Criteria The inclusion criteria were as follows: (i) studies on universal preventive HV-PPs aiming to improve the quality of the interactions between mothers (or other female caregivers with parental roles) and their infants up to two years old; (ii) mother-infant interactions as primary outcomes; and (iii) experimental design (RCT, with at least two arms), quasi-experimental design (non-randomized or nonequivalent control group), or pre-experimental trials (one single group with pre- and post-intervention). With this criterion, we aimed to include a broader set of studies assessing parent-child interactions in preventive programs, considering that Jeong et al.’s (2021) meta-analysis was limited to an RCT design. The exclusion criteria were as follows: (i) letters, editorials, commentaries, book chapters, qualitative studies, psychometric studies, observational research, reviews, meta-analysis, case reports, protocols, and pilot studies; (ii) interventions targeting exclusively fathers, pregnant women, or other caregivers (e.g., foster care caregivers); (iii) studies involving clinical populations (e.g., mothers or children diagnosed with mental health disorders, clinical conditions, or victims of current violence); (iv) therapeutic interventions using psychological and psychiatric techniques, rehabilitation, or pharmacological management; (v) interventions not delivered in the home-visiting format (e.g., group-based interventions, remote programs); (vi) interventions delivered exclusively during pregnancy or neonatal hospitalization; (vii) studies that measured exclusively other outcomes different from mother-child interactions (e.g., maternal attributes, competencies, behavior or mental health, child or family outcomes); and (viii) studies that analyzed mother-child interaction as a mediator variable or a moderator variable and not as a primary outcome. Information Sources The present review searched for recent articles published between 01/01/2018 and 12/31/2022 written in English, Spanish, or Portuguese (the authors are fluent in these languages). Studies were identified by searching the following electronic databases: PubMed, Web of Science, BVS/LILACS, SciELO, and PsycNET/PsycINFO. The search strategy used the following keywords in all databases: (((((Mother-Child OR maternal-child OR mother-infant OR maternal-infant OR Dyad OR dyadic) AND (Interaction OR Relation*) AND (intervention OR program))))) AND ((infant OR infancy)). The electronic search was performed on 01/05/2023. Selection Process The references were downloaded directly from the databases and imported to the Rayyan software (Ouzzani et al., 2016), where the duplicates were identified and the remaining articles screened. We used the Rayyan software to organize the references, manually apply the inclusion and exclusion criteria based on titles and abstracts, and categorize the reasons for excluding articles. Subsequently, a second screening was performed by reading the full texts to verify the inclusion and exclusion criteria for eligibility. The first author screened the articles, and the second and last authors participated in the final decision regarding the inclusion and exclusion criteria. Data Collection Data were extracted from the articles using an Excel sheet to record organized columns with the following information: reference; country in which the study was performed; study aims; study design; sample characteristics; characteristics of the intervention program (name, dosage, delivery setting, strategy, profile of providers, eligible population for the specific program, and children’s age when the intervention was applied with mothers); mother-child interaction domains (primary outcomes) and the instruments used to measure them; age of children at assessments; and main findings of the studies. The first author performed the initial screening of the papers and the second and last authors double-checked the entire process till the final decision. A summary of the studies was reviewed independently by the last author to ensure data extraction accuracy. Discrepancies were resolved by consensus among the three researchers. Effect Measures Considering that the primary interest of the present review was the effects of intervention programs on the quality of mother-infant interactions, the efficacy/effectiveness of interventions was analyzed, considering a significance level of 5% for between-group comparisons for the main outcome in each study. Methodological Quality of the Studies The Effective Public Health Practice Project (EPHPP) Quality Assessment Tool for Quantitative Studies (Thomas et al., 2004) was used to assess the methodological quality of the studies included in this review. The third author, who is an expert in this analysis, performed the methodological assessment. The EPHPP protocol considers the following six items: selection bias, design, confounders, blinding, data collection methods, and dropouts. The item’s classification could be strong, moderate, or weak, and then the EPHPP global rate is based on the classifications of all the items. A table detailing how items were classified considering each EPHPP component and the global rate can be found in the Appendix. Study Selection Figure 1 presents the flowchart with details on the processes of identification, screening, eligibility, and inclusion of articles according to the PRISMA guidelines (Page et al., 2021). Figure 1 Flowchart of the Identification, Screening, Eligibility, and Inclusion of Studies Process, according to PRISMA Guidelines (Page et al., 2021). 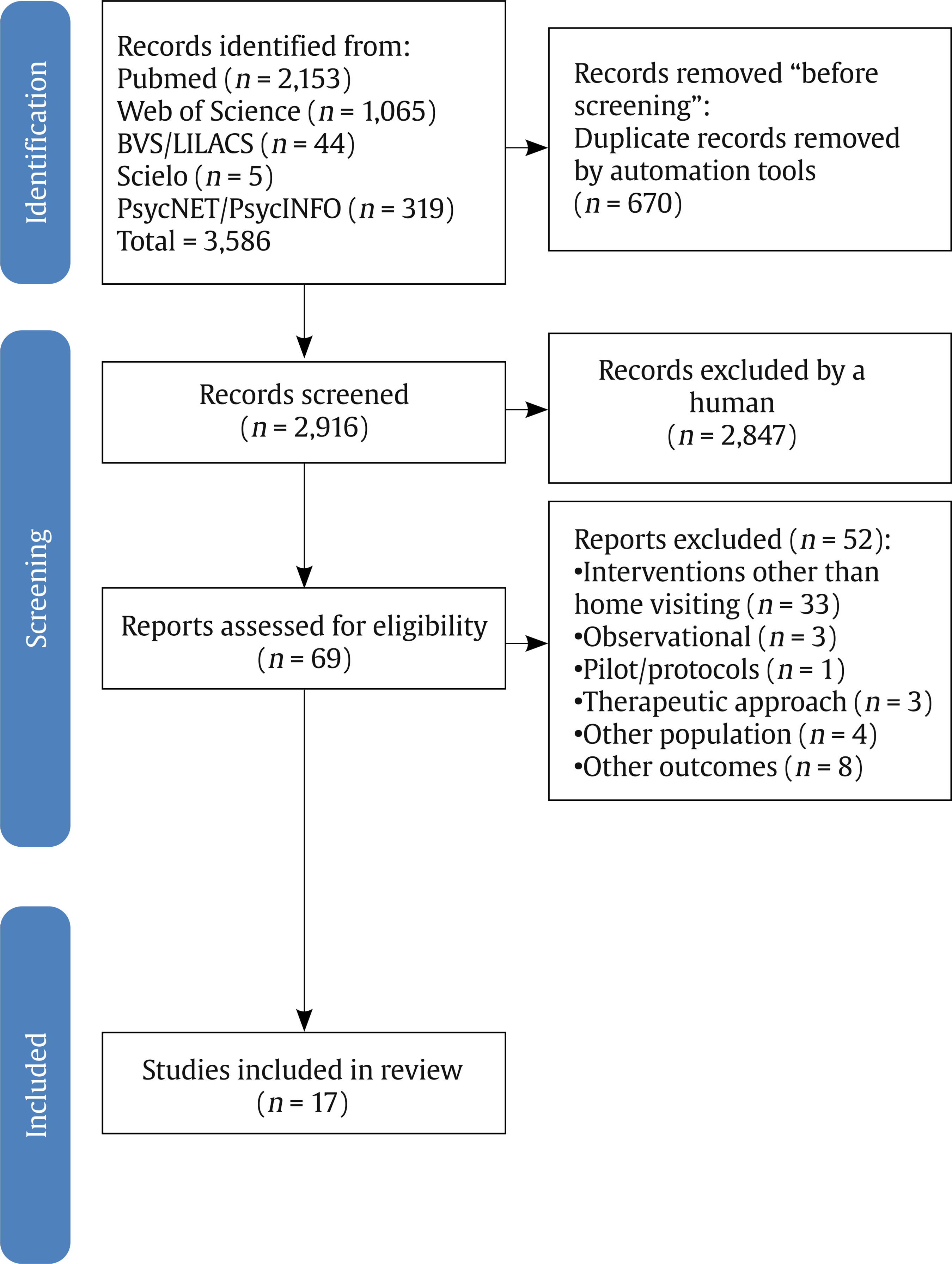 A total of 3,586 records were identified in the database search (Figure 1). First, 670 duplicate articles were excluded and 2,916 titles and abstracts were screened. Second, 2,847 papers were excluded based on the inclusion and exclusion criteria. The main reasons for the exclusion of articles were as follows: other issues different from the main objective of the present review (n = 2,172), observational studies without intervention (n = 328), reviews and meta-analysis (n = 54), qualitative studies (n = 50), psychometric studies (n = 52), pilot studies and protocols (n = 53), the primary outcome was not mother-child interaction (n = 76), samples of mothers with children over two years old, clinical samples, caregivers who were not the mothers (n = 44), interventions with therapeutic or clinical approaches (n = 16), and case reports (n = 2). Thus, 69 eligible articles were retained for full-text reading. Third, after reading the texts, 52 articles were also excluded based on the following reasons: studies in which interventions did not involve home visits or were restricted to pregnancy or neonatal hospitalization phases (n = 33), the primary outcome was not mother-child interaction (n = 8), samples comprising mothers with children over two years old or involving clinical populations or caregivers who were not the mothers (n = 4), observational studies without intervention (n = 3), interventions with therapeutic or clinical approaches (n = 3), and protocol studies (n = 1). Finally, 17 studies were included in this review. Overview of the Study Characteristics Regarding the countries in which the studies were conducted, 29% were made in North America (USA, n = 5); 29% in Latin America (Brazil, n = 3 and Colombia, n = 2)); 24% in Europe (Denmark, n = 1, Germany, n = 2, and Norway n = 1); 12% in Africa (South Africa, n = 2); and 6% in Asia (China/Taiwan, n = 1). Then, based on the World Bank (2023) classification, 53% of the studies were conducted in high-income countries (n = 9), and the remaining 47% were conducted in upper-middle-income countries (n = 8). Regarding study design, most studies (n = 15, 88%) were RCTs with two arms, with two studies adopting a cluster-randomized design. Only two studies (12%) were two-arm non-randomized trials, of which one used a single-blind multiple-time series method and the other used a cluster design. In addition, the usual-care control group was adopted in 59% of the studies (n = 10), and the remaining seven studies (41%) had comparisons between groups using another structured intervention or dummy intervention, similar to a “placebo” intervention (see Table 1). Table 1 Overview of the Studies: Designs and Characteristics of the Interventions (n = 17) 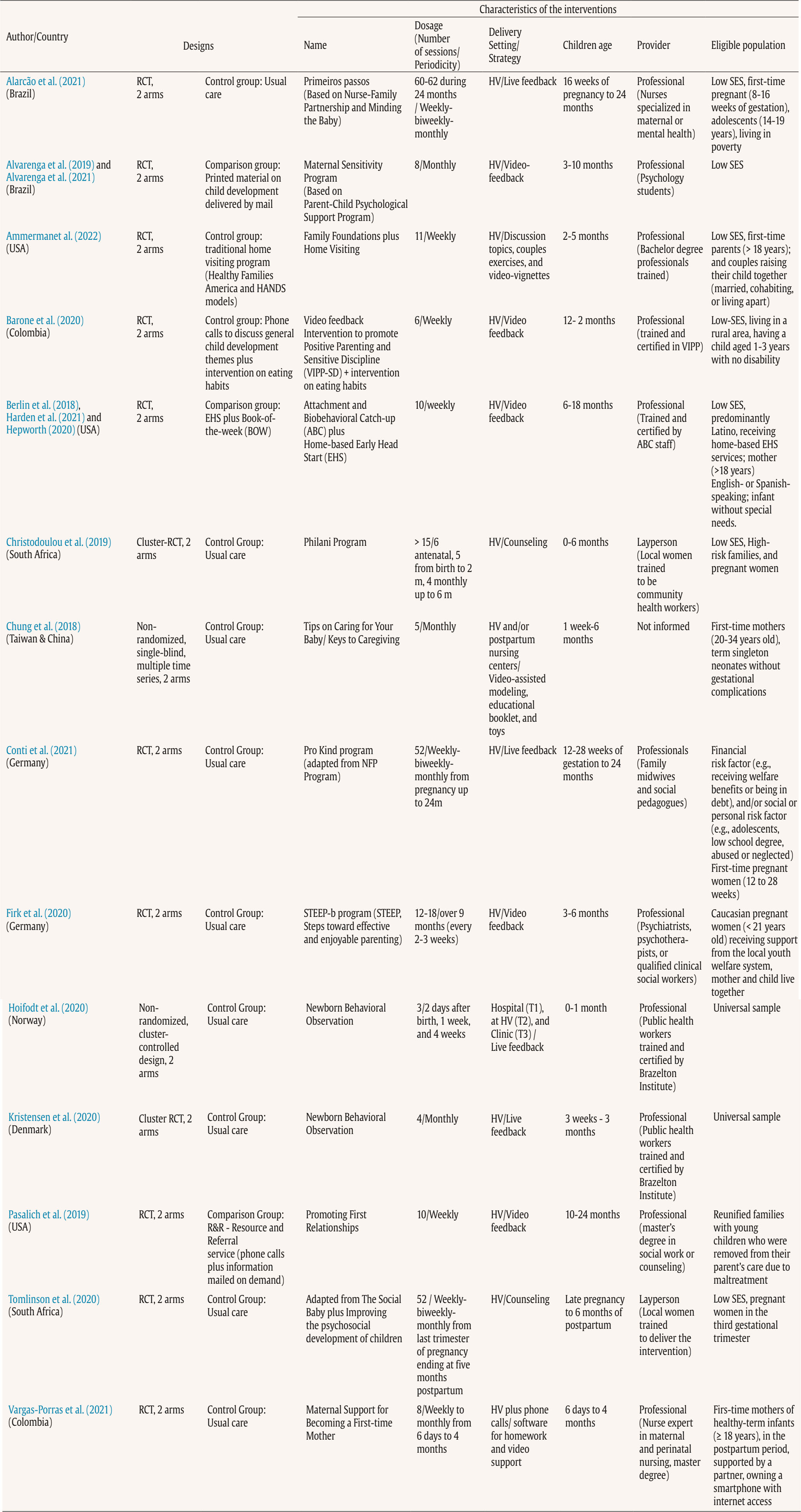 Note. Categories based on the coding system proposed by Bakermans-Kranenburg et al. (2003). HV = home visiting; RCT = randomized controlled Trial; SES = socioeconomic status; T = timepoint; USA = United States of America; UK = United Kingdom. Characteristics of the Preventive Parenting Programs Table 1 presents the main characteristics of the preventive parenting programs examined in the 17 studies. As seen in Table 1, the 17 studies examined the effects of 13 preventive parenting programs using home-visiting strategies to improve mother-child interactions. Only three interventions (Maternal Sensitivity Program, Attachment and Biobehavioral Catch-up plus Home-based Early Head Start, and Newborn Behavioral Observation [NBO]) were used in two studies at least. In these studies, the original programs were adapted to meet the specific aims of the research, with some flexibility from the original version. It is important to note that all the programs adopted an individual approach for mothers. Only two programs involved both mothers and fathers (Ammerman et al., 2022; Tomlinson et al., 2020). The dosage of the 13 programs presented great diversity in the number of sessions and periodicity schedules. The number of program sessions ranged from three to 62. The periodicity of interventions was weekly in six studies (Ammerman et al., 2022; Barone et al., 2020; Berlin et al., 2018; Harden et al., 2021; Hepworth et al., 2020; Pasalich et al., 2019) and monthly in four studies (Alvarenga et al., 2019; Alvarenga et al., 2021; Chung et al., 2018; Kristensen et al., 2020). The remaining studies had a variable periodicity during the program, such as weekly-biweekly-monthly during 24 months of the infants’ age (Alarcão et al., 2021; Conti et al., 2021); weekly-biweekly-monthly from pregnancy to six months of postpartum (Christodoulou et al., 2019; Tomlinson et al., 2020); weekly-monthly from six days to four months (Vargas-Porras et al., 2021); every two-to-three weeks during nine months (Firk et al., 2020); and one session two days after birth, one session one week after birth, and another session four weeks later (Høifødt et al., 2020). Regarding delivery characteristics, as expected, all the studies used home-visiting strategies; however, three of them also used complementary strategies, including phone calls (Vargas-Porras et al., 2021), sessions in the hospital and the clinic setting (Høifødt et al., 2020), and sessions in the postpartum nursing centers (Chung et al., 2018). Most programs used video support to deliver the intervention (n = 8/13, 62%), mainly video feedback (n = 5/13, 39%). Other strategies using video resources included video-assisted modeling associated with educational booklets and toys (Chung et al., 2018), couple exercises using video vignettes (Ammerman et al., 2022), and software for homework and video sharing (Vargas-Porras et al., 2021). A few studies used live feedback (n = 3/13, 23%) and counseling strategies (n = 2/13, 15%) during home visits. The programs were delivered by health, education, or social work professionals in 14 studies (82%). Trained laypersons delivered the intervention in two programs (12%), and one program did not provide this information (6%). The eligible population for these programs was predominantly families from low socioeconomic backgrounds and/or families with psychosocial vulnerabilities, such as adolescents, single or first-time mothers, and reunified families after maltreatment experiences. Main Findings of the Studies Regarding the main findings, it is important to highlight that 77% (n = 13) of the studies demonstrated significant effects of the interventions on mother-child interaction outcomes. Table 2 summarizes the main findings of the 17 studies based on their samples, mother-child interaction outcomes, and assessment procedures. Table 2 Main Findings of the Studies (n = 17) 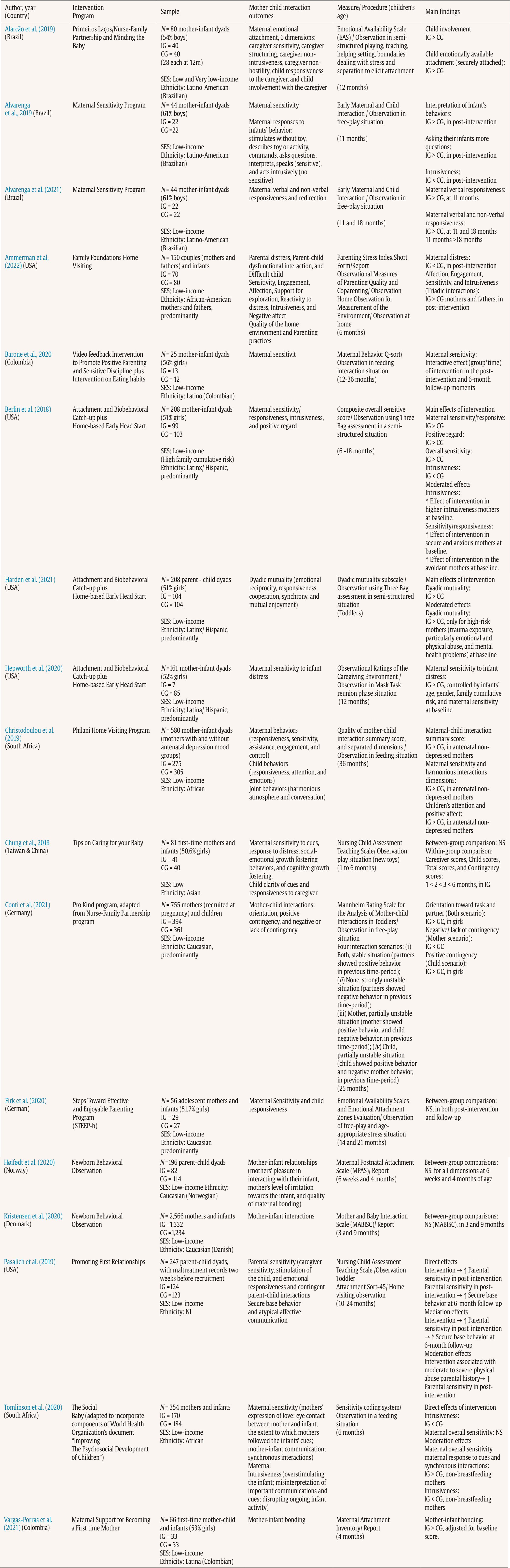 Note. N = number of participants; IG = intervention Group; CG = control group/comparison group; SES = socio-economic status; NS = not significant; NI = not informed; MABISC = Mother and Baby Interaction Scale; MPAS = Maternal Postnatal Attachment Scale; STEEP-b = Steps Toward Effective and Enjoyable Parenting Program. Most studies assessed samples of adult mothers of infants up to two years of age. Although most studies were conducted in high-income countries, they all had predominantly vulnerable samples, including families from low socioeconomic levels and/or with psychosocial risks such as pregnancy during adolescence, first-time mothers, and ethnic minorities (mainly Latina/Latinx/Hispanic and African ethnicities). The sample size varied greatly among the studies, ranging from 25 to 2,566 mother-child dyads (mean = 342 dyads). Most studies used exclusively observational methods to assess mother-child interactions (Alarcão et al., 2021; Alvarenga et al., 2019; Alvarenga et al., 2021; Barone et al., 2020; Berlin et al., 2018; Christodoulou et al., 2019; Chung et al., 2018; Conti et al., 2021; Firk et al., 2020; Harden et al., 2021; Hepworth et al., 2020; Pasalich et al., 2019; Tomlinson et al., 2020) or used mixed methods (observation plus maternal report) (Ammerman et al., 2022), and three studies assessed the mother-child interactions exclusively based on mothers’ reports (Høifødt et al., 2020; Kristensen et al., 2020; Vargas-Porras et al., 2021). Most observational procedures were performed during free-play situations. The instruments applied to analyze the observed mother-child interactions were diverse, as follows: Emotional Availability Scale (EAS), Early Maternal and Child Interaction, Observational Measures of Parenting Quality and Coparenting, Home Observation for Measurement of the Environment, Maternal Behavior Q-sort, Composite overall sensitive score and Dyadic Mutuality Subscale of the Three Bags Assessment, Caregiving Environment ratings of Mask Task reunion phase situation, Quality of mother-child interaction summary score, Nursing Child Assessment Teaching Scale, Mannheim Rating Scale for the Analysis of Mother-child Interactions in Toddlers, Emotional Attachment Zones Evaluation, Toddler Attachment Sort-45, and Sensitivity Coding System. Strategies using video resources were predominant in home-visiting programs. Concerning the “video-feedback strategy”, three RCT studies applied the Attachment and Biobehavioral Catch-up (ABC) associated with Home-based Early Head Start (EHS) in predominantly Latinx/Hispanic samples of mothers from families with high-cumulative risks living in the USA. In the first ABC-EHS study, mothers in the intervention group showed more overall sensitivity, sensitivity/responsiveness, and positive regard, as well as less intrusiveness in mother-child interactions, observed during a semi-structured situation (Three Bag Assessment) at 6-18 months of the children’s age (Berlin et al., 2018). In addition, baseline maternal intrusiveness significantly moderated the intervention effect, which was stronger in mothers with high intrusiveness at baseline. The intervention effects on sensitivity and responsiveness were stronger for mothers with secure or anxious attachment at baseline. However, the intervention effect was significantly negative for avoidant mothers. In the second ABC-EHS study, the intervention group showed a main effect on dyadic mutuality and a moderated effect on mutual mother-child interactions only in high-risk mothers (e.g., trauma exposure and mental health problems) identified at baseline (Harden et al., 2021). In the third ABC-EHS study, the intervention group demonstrated higher maternal sensitivity to infant distress in the reunion phase of an observational procedure (Mask Task) than the control group, controlling for infants’ age and gender, family cumulative risks, and maternal sensitivity at baseline (Hepworth et al., 2020). In a randomized controlled study, the Maternal Sensitivity Program using video feedback showed that mothers in the intervention group performed better in the interpretation of infants’ behaviors, asked their infants more questions, and displayed reduced intrusiveness in an observational mother-infant interaction assessment during a free-play situation in the post-intervention, compared to the control group (Alvarenga et al., 2019). Subsequently, in a secondary analysis of this RCT, the intervention group presented more maternal verbal responsiveness at 11 and 18 months of the children’s age and maternal nonverbal responsiveness at 18 months of the children’s age; maternal responsiveness toward children aged 11 months was higher than that toward children aged 18 months (Alvarenga et al., 2021). The Promoting First Relationships program improved toddlers’ attachment security by strengthening caregivers’ sensitivity in low-income parent-child dyads with maltreatment records two weeks before the recruitment phase (Pasalich et al., 2019). The findings showed a direct effect of the intervention on parental sensitivity in the post-intervention period, which, in turn, mediated the increase of the security-based behavior at the six-month follow-up, assessed at 10-24 months of the children’s age during the home visit. Interestingly, the moderation analysis showed that the intervention effect on parental sensitivity was higher for parents with a history of moderate to severe physical abuse. The Promote Positive Parenting and Sensitive Discipline Program associated with interventions on eating habits using a video-feedback strategy presented an interactive effect of group and time. Compared with the control group, the intervention group increased maternal sensitivity in low-income Colombian mother-infant dyads post-intervention and at the six-month follow-up (Barone et al., 2020). As complementary results of this study, the positive food habits of the intervention group improved in the post-test, and there was a significant interaction between group and time variables. Finally, despite the mothers’ satisfaction with the Step Toward Effective and Enjoyable Parenting Program using a video-feedback strategy with a sample of adolescent mothers and their infants aged 14-21 months, there was no effect of the intervention on maternal sensitivity and child responsiveness in comparison to the usual care control group, both post-intervention and at the follow-up (Firk et al., 2020). Focusing on the “video support” strategy used in the Family Foundations Home Visiting program, mothers who participated in the intervention group showed greater affection, engagement, and sensitivity than those who participated in the traditional home visit program. Unexpectedly, during observational triadic interactions, it was noted that there was more intrusiveness between children aged six months, mothers, and fathers in the post-intervention assessment compared to the baseline (Ammerman et al., 2022). The Maternal Support for Becoming a First-Time Mother Program, delivered using a video-assisted strategy to low-income Colombian mothers, increased bonding, functional social support, and perceived maternal self-efficacy in the post-intervention evaluation compared with the control group when infants were four months old (Vargas-Porras et al., 2021). Meanwhile, the Tips on Caring for Your Baby program using a “video-assisted modeling strategy” did not show significant effects on mother-child interactions (maternal sensitivity cues and response to distress and child clarity of cues and responsiveness to caregiver) when children were 1-week to 6 months old, in low-income Asian first-time mothers (Chung et al., 2018). Otherwise, in this study, the within-group comparison analysis showed continuous growth of caregiver, child, total, and contingency scores through time in the intervention group. Regarding the “live-feedback strategy”, the First Bonding intervention showed that infants at 12 months of age in low- and very-low-income families in the intervention group showed higher involvement and emotionally available attachment during observed mother-child interactions (assessed by the EAS) than those in the usual care control group (Alarcão et al., 2021). As a complementary finding, the Nc, an event-related potential that reflects attentional and memory processes of six-month-old children, was directly associated with child involvement at 12 months of age. In the Pro-Kind Program study, the intervention group presented more orientation toward the task and partner than the usual care control group (in the interaction scenario of both mothers and children showing positive behavior in the previous time period) and positive contingency (in the interaction scenario of the children showing positive behavior and mothers showing negative behavior in the previous time period), specifically in girls in a sample of low-income mothers and 25-month-old toddlers (Conti et al., 2021). Additionally, compared with the control group, the intervention group had less negative/lack of contingency in the interaction scenario of the mother showing positive behavior and the child showing negative behavior in the previous time period. It was noted that two studies that used NBO interventions with live feedback did not present significant effects in a universal sample of mothers. In the Danish cluster randomized controlled trial, mothers receiving the NBO intervention from three weeks to three months postpartum did not show better mother-infant interactions (assessed by the Mother and Baby Interaction Scale-Report) than the control group at three and nine months of the children’s age (Kristensen et al., 2020). Further, in the Norwegian non-randomized cluster-controlled trial, no significant effects of the NBO intervention on mother-infant relationships were observed at six weeks and four months of the children’s age assessments in a low-income sample (Høifødt et al., 2020). In this study, the intervention group presented higher scores in the mother’s knowledge of caring for infants compared to the control group, but not in the mother-child interaction outcome. Regarding the “counseling” strategy, in the Philani Home Visiting program delivered to African mothers in an RCT longitudinal study from the antenatal period to six months of the children’s age (Christodoulou et al., 2019) the intervention group showed higher maternal-child interaction summary scores, maternal sensitivity, and harmonious interactions, and children showed more attention and positive affect than the control group, in antenatal non-depressed mothers. The Social Baby Program, delivered to low-socioeconomic pregnant African mothers using counseling strategies, demonstrated that the intervention group had significantly decreased maternal intrusiveness in observed feeding situations in six-month-old children (Tomlinson et al., 2020). In addition, there were moderate effects, showing that overall maternal sensitivity, maternal response to cues, and synchronous interactions were higher and intrusiveness was lower in the intervention group than in the control group, specifically in non-breastfeeding mothers. As complementary findings, this study examined mothers’ mental health and showed that children’s positive emotional affect and talking to their mothers were higher for non-depressed mothers in the intervention group. Additionally, children’s responsiveness and attention were higher in depressed mothers in the control group. Methodological Quality of the Studies Table 3 shows that, regarding the methodological care of the 17 studies assessed by the EPHPP tool, 82% and 18% of the studies presented strong and moderate results in the overall ratings of methodological assessment, respectively. Specifically, the studies showed strong design (except one study classified as moderate), data collection methods, and control of confounders (except one study also classified as moderate). Regarding selection bias, 70% of studies were classified as strong and 30% as moderate. Concerning withdrawal, 59% were strong, 29% were moderate, and 11% were weak. Finally, the blinding component was moderate in 82% of the studies, strong in 12%, and weak in 6%. Only one study was classified as strong in all components of the methodological assessment (Vargas-Porras et al., 2021). Table 3 Methodological Quality of the Studies, Assessed by EPHPP 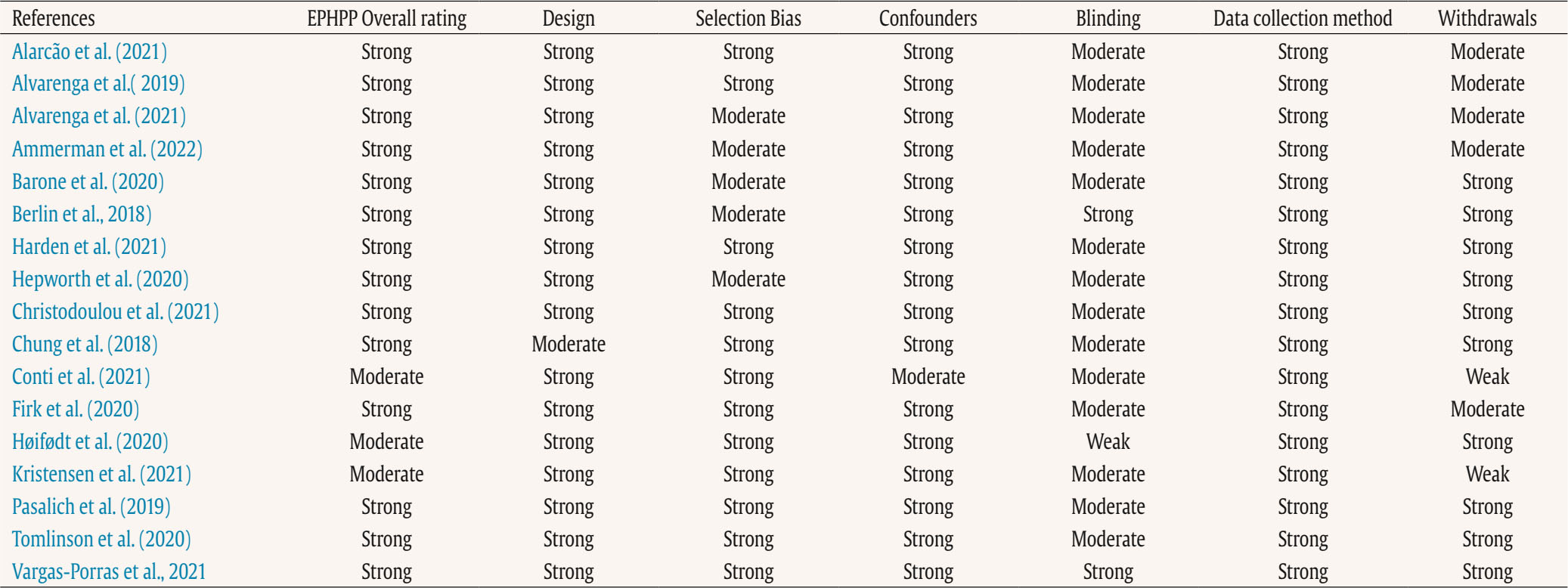 Note. EPHPP = Effective Public Health Practice Project Quality Assessment Tool for Quantitative Studies. The findings of the present review provided evidence that home-visiting preventive parenting programs improved mother-child interactions. In 76% of the studies reviewed, positive effects were observed despite the diversity in their study design, sample characteristics, measures, and constructs assessed. Even though four studies did not demonstrate effects on the main outcome, they demonstrated other benefits of home-visiting programs, such as improved mothers’ knowledge of caring for infants (Høifødt et al., 2020) and reduced parental stress (Firk et al., 2020). The present systematic review adds to the current literature with its in-depth exploration of preventive home-visiting programs specifically designed to improve mother-infant interactions, an essential component of nurturing care to promote child development. First, it is important to highlight that the studies reviewed presented good methodological care, with more than 80% classified as strong and 18% classified as moderate in the overall rating of the EPHPP tool (Thomas et al., 2004). Notably, almost 90% of the studies analyzed were RCTs, which is the recommended study design for examining the efficacy of intervention programs. Then, the methodological aspects of these studies guarantee the reliability of their findings. With regard to the “main characteristics” of HV-PPs, 13 different programs on mother-child interactions were analyzed. Most studies, except those by Chung et al. (2018) and Vargas-Porras et al. (2021), were based on other known programs in which positive effects have been previously demonstrated (e.g., Berlin et al., 2018; Conti et al., 2021; Harden et al., 2021; Hepworth et al., 2020). Most programs made adaptations to address a specific population (e.g., Firk et al., 2020), providers (e.g., Christodoulou et al., 2019), setting characteristics (e.g., Ammerman et al., 2022); others used mixed programs (e.g., Alarcão et al., 2021) or components of another program (e.g., Alvarenga et al., 2019; Alvarenga et al., 2021). In addition to home visits, some programs used additional strategies, such as sessions at postpartum nursing centers (Chung et al., 2018), hospital visits before mothers’ delivery (Høifødt et al., 2020), and phone calls (Vargas-Porras et al., 2021). Mixing strategies to deliver programs is an effective option as it enhances participants’ exposure to the program’s main messages (Britto et al., 2015). In general, adaptations and fidelity assessments were carefully described, as recommended by Bakermans-Kranenburg et al. (2003) and Mountain et al. (2017), ensuring methodological consistency in program implementation. Moreover, cultural adaptations were also described, mainly for studies conducted in middle-income countries (e.g., Barone et al., 2020), ensuring the program’s core components but also allowing some flexibility to the local culture and population, as recommended by Lansford et al. (2022). The heterogeneity of the programs in terms of the number of sessions (dosage), intensity, and start time was noteworthy. The mean number of sessions was 19, ranging from three to 62, delivered according to various schedules. A mixed schedule, starting weekly with a subsequent monthly schedule, has been used for the longest programs (Alarcão et al., 2021; Conti et al., 2021; Tomlinson et al., 2020). The three studies that presented the lowest number of sessions (three to five sessions) did not report positive effects of the programs compared to the control group (Chung et al., 2018; Høifødt et al., 2020; Kristensen et al., 2020). Regarding the reviewed studies, the minimum dosage of the programs that verified effects on mother-child interactions was six sessions (Barone et al., 2020). In 76% of the studies reviewed, the effects of home-visiting programs on mother-child interactions were independent of the dosage and intensity schedule. Despite the vast literature on this topic, the best dosage and intensity of parenting programs remain unknown (Bakermans-Kranenburg et al., 2003; Britto et al., 2015; Morrison et al., 2014; Mountain et al., 2017). In this sense, our findings are consistent with those of Jeong et al. (2021) and Britto et al. (2017), who showed that the program’s effectiveness was not modified by intervention duration, delivery, or setting. However, our review indicated that fewer than six sessions were insufficient to promote positive effects in interactions between mothers and children. Nevertheless, implementing home-visiting programs may have significant economic implications; thus, it would be relevant to establish the optimal number of home visits necessary to achieve the best effects on parenting and child development outcomes (Tazza et al., 2023). In studies examined in the current review, most programs started their activities when the children were six months old or younger, and few offered sessions from the gestational period through the months following childbirth. Notably, from 15 programs that started their activities from pregnancy up to the third postpartum month, only four studies did not report a positive impact on mother-child interactions when intervention and control groups were compared (Chung et al., 2018; Firk et al., 2020; Høifødt et al., 2020; Kristensen et al., 2020). Although the meta-analysis by Bakermans-Kranenburg et al. (2003) reported that interventions starting when children were older than six months of age achieved better results than those starting prenatally or before six months of the children’s age, these findings were not confirmed by Jeong et al.’s (2021) meta-analysis. Interestingly, Britto et al. (2015) highlighted that the duration of programs may be more relevant than dosage and intensity depending on the intended outcomes. For instance, programs aimed at enhancing parenting knowledge could be shorter than those aimed at impacting children’s outcomes, such as cognitive development (Britto et al., 2015). Thus, the combination of short duration, very early start, and a small number of sessions could explain the absence of effects compared to the control group observed in the present review of the NBO (Høifødt et al., 2020; Kristensen et al., 2020) and “Tips on Caring for Your Baby” (Chung et al., 2018) programs on mother-child interactions. Provider profiles have technical and economic implications. In the present review, most programs (88%) were delivered by trained health and education professionals. Unlike previous reviews (Bakermans-Kranenburg et al., 2003; Britto et al., 2015; Jeong et al., 2018), only two programs, both from South Africa, have been delivered by laypersons (Christodoulou et al., 2019; Tomlinson et al., 2020). The authors showed that the program delivered by trained community workers and mentor mothers improved maternal responsiveness and sensitivity compared to the usual care group, encouraging this sustainable service in low-resource settings. Programs delivered by nonprofessionals seem to be more cost-effective and culturally adapted (Munns et al., 2016) and are as effective as those delivered by professionals (Bakermans-Kranenburg et al., 2003; Britto et al., 2015; Jeong et al., 2018; Mountain et al., 2017). However, as pointed out by Peacock et al. (2013), although home-visiting programs delivered by trained nonprofessionals improved child development and health outcomes, they frequently did not significantly impact high-risk children from disadvantaged families with complex problems. Then, assuring adequate training and support for paraprofessionals (Munns et al., 2016; Peacock et al., 2013; Vu et al., 2015), beyond addressing issues concerning program design and implementation processes, would help improve the quality and effectiveness of parenting programs (Aboud & Prado, 2018; Lansford et al., 2022). Our findings showed that video support was the main strategy used to deliver the interventions, mostly as video feedback during home visits but also as non-in-person strategies, such as video-assisted programs and vignettes (Ammerman et al., 2022; Chung et al., 2018; Vargas-Porras et al., 2021). Programs also used live feedback (e.g., Alarcão et al., 2021; Conti et al., 2021) and counseling strategies (Christodoulou et al., 2019; Tomlinson et al., 2020). Video feedback is a common strategy that is used for various purposes. Specifically, it is extremely useful to improve parent-child relationships as it provides opportunities for parents to reflect on their own behaviors and register their progress along with the intervention (Balldin et al., 2018; Juffer et al., 2017). Nevertheless, video feedback interventions are frequently time-consuming and more expensive than other strategies, which may limit their scalability with fidelity in real-world community settings (Balldin et al., 2018). Interestingly, in the current review, most programs using video feedback were developed in high-income countries (e.g., the USA and Germany) and included smaller sample sizes (mean = 124 participants). In contrast, other strategies were used in more diverse cultural contexts (e.g., South Africa, China, and Colombia) with larger samples (mean = 536 participants), suggesting constraints on using video feedback in low-resource settings. However, with technological advances, the development of apps may facilitate the implementation of large-scale video-supported programs (Vale et al., 2022). The studies analyzed in the current systematic review included diverse tools and measures to assess many aspects of mother-child interaction. We observed that mother-child interactions are typically evaluated using observational methods. Conversely, Brito et al.’s (2015) systematic review of studies developed exclusively in LMICs reported the extensive use of self-report tools to assess the impact of programs on parenting outcomes. Most studies in the present review were conducted in high-income countries; thus, these differences may be related to the settings in which the studies were conducted. Nevertheless, a prior review of group-based parenting programs demonstrated that studies using observational and self-reported measures showed consistent results, indicating the effectiveness of both methods in assessing changes in parenting practices following the programs (Branco et al., 2022). Of note, among the four studies that did not show significant effects of the intervention, two used observational and validated scales (NCATS and EAS) and assessed mothers’ and children’s behaviors and dyadic interactions (Chung et al., 2018; Firk et al., 2020). The other two studies used self-report scales (MPAS and MABISC) and assessed only maternal behaviors (Høifødt et al., 2020; Kristensen et al., 2020). In the present review, eight different tools were used in 14 studies based on observational measures. Observational measures are considered the “gold standard” when assessing parent-child interactions in particular, as they can capture positive and negative details of the early dyadic relationship in real-time, in naturalistic or experimental scenarios, using structured- or free-play tasks (Gridley et al., 2019; Nascimento et al., 2023; Roggman et al., 2013). However, recent systematic reviews (Gridley et al., 2019; Jeong et al., 2022) showed that the psychometric properties of these tools have not been sufficiently explored, which may compromise their use for research and clinical purposes. Most studies analyzed in the current review reported inter-rater reliability; however, cultural adaptations and other psychometric measures, such as validity assessments, were poorly described, which is in agreement with previous reviews (Gridley et al., 2019; Jeong et al., 2022). Of note, a few tools have been created by the authors themselves and tested in previous studies, but their measurement properties have not been reported (e.g., Christodoulou et al., 2019; Tomlinson et al., 2020). Despite the increasing interest in promoting responsive caregiving in the last few decades, Jeong et al. (2022) highlighted the need for more research and guidance regarding valid and reliable measures of parent-child interactions and responsive caregiving. Maternal behaviors, such as sensitivity, responsiveness, warmth, and intrusiveness, were the main constructs assessed in the 14 studies in the current review. Child behaviors were assessed separately in six studies, and the mother-child dyadic interaction assessment was used in seven studies. Only four studies used a holistic approach to explore mothers’ and children’s behaviors and dyadic interactions (Alarcão et al., 2021; Christodoulou et al., 2019; Chung et al., 2018; Firk et al., 2020). The constructs were highly determined by the tools used in the studies, but we noted some concept overlap, making it difficult to quantify which aspects of the mother-child interactions were more commonly assessed and impacted by the programs. For instance, the Parental Stress Index, a tool frequently used to assess parent-child interaction, has three subscales, but only parent-child dysfunctional interaction directly measures dyadic relationships. Furthermore, this subscale is focused on stressful situations involving parental caregiving; thus, it may not capture “healthy” interactions satisfactorily. This issue was also highlighted in a prior systematic review by Jeong et al. (2022), which revealed that among 47 studies examining responsive caregiving, only one used a tool developed specifically to measure responsiveness; the other studies assessed correlated and broader aspects of the parent-child interaction. We observed a predominance of interest in positive maternal behaviors, such as sensitivity, responsiveness, and warmth, during interactions with their children, compared with negative behaviors, such as intrusiveness and hostility. Only five studies have measured negative maternal behaviors (Ammerman et al., 2022; Berlin et al., 2018; Conti et al., 2021; Hepworth et al., 2020; Tomlinson et al., 2020). Certainly, the main objective of all parenting programs is to improve positive behaviors; however, this does not ensure a decrease in negative behaviors (Roggman et al., 2013). Thus, balancing these complementary aspects of mother-child relationships would help us better understand the effects of parenting programs. Another unexpected finding from our review was the small number of studies (12%) that assessed mothers’ and children’s behaviors as well as dyadic interactions, such as synchrony, contingency, and mutuality, using observational tools (Alarcão et al., 2021; Chung et al., 2018; Christodoulou et al., 2019; Firk et al., 2020). Mother-child interactions are complex and multifaceted relationships that require a broad and holistic approach (Knerr et al., 2013; Leclère et al., 2014). Children are active elements of the mother-child relationship, so their behaviors, temperaments, and preferences may modulate their interactions, as well as the characteristics of their mothers do. Thus, assessing mothers’ and children’s behaviors separately is insufficient to understand the quality of their interactions (Knerr et al., 2013; Leclère et al., 2014). Since most programs improve positive behaviors (e.g., sensitivity, responsiveness, and contingency) and reduce negative behaviors (e.g., intrusiveness and hostility) during mother-child interactions, attention should be paid to interventions without expected effects. Chung et al. (2018) observed an increase in the quality of mother-infant interactions within the intervention group, but the differences between the groups were not significant. Despite the methodological strengths, the authors argue that cultural aspects, for example, the “Do the months” ritual, staying at nursing care centers after childbirth, and modesty and humility values in Taiwanese society, might have compromised the program’s results (Chung et al., 2018). Furthermore, the Taiwanese was based on the American evidenced-based program “Keys to Caregiving” program (Spietz et al., 1990), with the materials (CD and manuals) translated into Chinese; however, a cultural adaptation was not described, possibly affecting the implementation process (Lansford et al., 2022). In addition to cultural issues, delivery strategies based on educational materials may explain this study’s results. According to Jeong et al.’s (2021) meta-analysis, programs that did not include responsive caregiving components in their delivery strategies were less effective than those based on these contents. Surprisingly, two other studies (Høifødt et al., 2020; Kristensen et al., 2020) using Brazelton’s concepts and framework (Brazelton et al., 1974; Nugent et al., 2007) did not attain the expected positive effects of their programs on mother-child interactions. Moreover, these three programs share some program design characteristics, such as low dosage, low intensity, and a very early start time, suggesting that these strategies could not improve the mother-child interactions as expected. Differing from the study by Chung et al. (2018), Høifødt et al. (2020), and Kristensen et al. (2020) examined programs based on the NBO, another American program with promising positive effects on mother-child relationships, inclusive in previous studies in Nordish cultures (Yago et al., 2023). Nevertheless, another review did not find a consistent impact of home-visiting programs based on Brazelton’s approach on the sensitivity and emotionality of the mother-infant relationship, although positive effects on other parenting outcomes, such as knowledge, have been reported (Tazza et al., 2023). The assumption that increased parental knowledge would be associated with increased parental sensitivity and confidence in their caregiving skills was not confirmed by Høifødt et al. (2020) and Kristensen et al. (2020). According to Tazza et al. (2023), the heterogeneity of the samples in terms of exposure to risk factors and vulnerability explains the inconsistency of findings across studies, with programs involving clinical conditions performing better than universal preventive interventions. Notably, the samples included in studies by Høifødt et al. (2020) and Kristensen et al. (2020) constituted predominantly well-functioning families, and the “ceiling effect” on questionnaires used to assess mother-child bonding and maternal confidence may explain the absence of significant differences between groups. Firk et al. (2020) highlighted the need to customize programs according to sample characteristics because of the differential effects of interventions across populations. Their study included a small sample of German adolescent mothers and used an adaptation of a well-known program (STEEPTM); (Erickson & Egeland, 2004). Nevertheless, despite participants’ satisfaction with the program (Firk et al., 2020) and the positive impact of the German version of the program on a high-risk sample (Suess et al., 2016), no effects on mother-child interactions were observed. Although the STEEP program has been proven effective, Firk et al. (2020) argued that longer and more intense programs may be necessary to achieve goals for specific groups, such as adolescent mothers. They also pointed out that problematic interaction patterns could emerge very soon in high-risk groups; therefore, interventions starting after the third month of a child’s age could be too late. These findings highlight the need to understand “what works for whom” and are supported by the differential susceptibility theory of parents in the context of preventive programs (Chhangur & Belsky, 2023). Moreover, this shows that an ideal program design is far from being defined. In conclusion, the present review confirms the effectiveness of different home-visiting preventive parenting programs on mother-child interactions in early childhood. However, the findings do not allow us to recognize a pattern of program design that is more effective than others; further, it seems that the combination of fewer than six sessions, a duration shorter than three months, and a very early start time did not positively impact the mother-child interactions, as expected. Notably, most interventions with significant outcomes used a video feedback approach and were assessed using observational methods. Despite these distinct results, our findings revealed that there is still a predominant interest in positive maternal behaviors, both in the program content and the outcomes measured. Gaps remain in our understanding of the effectiveness of programs in reducing negative maternal behaviors such as intrusiveness. Few studies have used a comprehensive approach to mother-child interactions, including child behaviors and assessing aspects of dyadic relationships, such as synchrony and contingency. These findings indicate the need to widen the gaze at the parent-child relationships to capture the real impact of home-visiting programs on families’ lives. We noted significant heterogeneity in the program design, analyzed constructs, and tools used to measure their effects. The most evident concern is how authors use and interpret measures and define constructs, sometimes causing discrepant findings between studies that use the same tool. These distortions obscure the understanding of the results since the mother-child interaction is marked by overlapping constructs. We have provided a careful and updated synthesis of studies analyzing the effectiveness of home-visiting preventive programs on mother-child interaction, following recognized protocols. Notably, none of the reviewed studies included clinical samples (e.g., participants with maternal depression and child behavioral disorders), reinforcing the preventive focus of the programs and making the results more generalizable. Nevertheless, the present review has some limitations. We did not perform a two-author independent screening of the papers, although the other authors double-checked the entire review process. Furthermore, the authors have extensive expertise in the topic and producing systematic reviews, which has contributed to improving the accuracy of the current review. We included only studies assessing interactions between mothers and their children under two years old, preventing us from analyzing the long-term effects of the interventions. Further, we did not evaluate programs involving other caregivers, such as fathers, which would have provided a broader picture of the environment in which early interactions occur. This review has several practical implications. Most of the studies were classified as having strong methodological quality, but it was not yet possible to establish the “ideal” format for home-visiting preventive parenting programs due to the huge heterogeneity of intervention models. However, our findings suggest that more individualized strategies, such as video feedback and live feedback, could have benefits since they strengthen maternal self-awareness and provide space for mothers to reflect on their own parenting behavior. The choice of the best strategy relies on the objectives and resources of each program as well as the context in which the intervention will be implemented. The “unsuccessful” studies also brought reflections that should be considered when designing interventions to improve mother-child interactions from a preventive perspective. First, the cultural adaptation of programs and measurement tools should be strongly considered, not only for LMICs but also across different cultures. Second, the characteristics and functioning of the addressed population may require special program adjustments, such as the number of sessions, program intensity, and starting point. Third, the core messages and materials of the program and how to deliver them should be carefully considered by choosing content and approaches that best fit the cultural and sociodemographic characteristics of families eligible for the programs, as well as their previous parental knowledge, skills, and experiences in responsive caregiving and child development. At least, more studies on the sustainability of these programs and how to implement them feasibly in different contexts, especially in LMICs, are required. Conflict of Interest The authors of this article declare no conflict of interest. Authors’ Contribution All authors worked together in the conception and design, analysis, and interpretation of the findings, discussion of results, writing, and review of the final version of the paper. All the authors agree to submit the final version of the paper for publication. Cite this article as: Alves, C. R. L., Seibel, B. L., Gaspardo, C. M., Altafim, E. R. P., & Linhares, M. B. M. (2024). Home-visiting parenting programs to improve mother-infant interactions at early ages: A systematic review. Psychosocial Intervention, 33(2), 117-132. https://doi.org/10.5093/pi2024a7 Funding: This study was funded by the National Council for Scientific and Technological Development (CNPq – Grant 103801/2019-7; Pos Doc Senior and Grant 305462/2022-9; Scientific Investigator) for CRL Alves and (CNPq - Grant 310726/2021-2, Senior Scientific Investigator) for MBM Linhares. |
Cite this article as: Alves, C. R. L., Seibel, B. L., Gaspardo, C. M., Altafim, E. R. P., & Linhares, M. B. M. (2024). Home-visiting Parenting Programs to Improve Mother-Infant Interactions at Early Ages: A Systematic Review. Psychosocial Intervention, 33(2), 117 - 132. https://doi.org/10.5093/pi2024a7
Correspondence: lindgrenalves@gmail.com; lindgren@ufmg.br (Claudia R. L. Alves)Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
Send






