


The Spatio-Temporal Distribution of Suicide-related Emergency Calls in a European City: Age and Gender Patterns, and Neighborhood Influences
Miriam Marco1, Antonio López-Quílez2, Francisco Sánchez-Sáez3, Pablo Escobar-Hernández2, María Montagud-Andrés1, Marisol Lila1, and Enrique Gracia1
1Department of Social Psychology, University of Valencia, Spain; 2Department of Statistics and Operational Research, University of Valencia, Spain; 3School of Engineering and Technology (ESIT), Universidad Internacional de La Rioja, Spain
https://doi.org/10.5093/pi2024a8
Received 20 November 2023, Accepted 14 February 2024
Abstract
Objective: The aim of this study was to conduct a comprehensive spatio-temporal analysis of suicide-related emergency calls in the city of Valencia (Spain) over a six-year period. To this end we first examined age and gender patterns and, second, the influence of neighborhood characteristics on general and gender-specific spatio-temporal patterns of suicide-related emergency calls. Method: Geocoded data on suicide-related emergency calls between 2017 and 2022 (N = 10,030) were collected from the 112 emergency service in Valencia. Data were aggregated at the census block group level, used as a proxy for neighborhoods, and trimesters were considered as the temporal unit. Two set of analyses were performed: (1) demographic (age and gender) and temporal descriptive analyses and (2) general and gender-specific Bayesian spatio-temporal autoregressive models. Results: Descriptive analyses revealed a higher incidence of suicide-related emergency calls among females and an increase in calls among the 18-23 age group from 2020 onwards. The general spatio-temporal model showed higher levels of suicide-related emergency calls in neighborhoods characterized by lower education levels and population density, and higher residential mobility, aging population, and immigrant concentration. Relevant gender differences were also observed. A seasonal effect was noted, with a peak in calls during spring for females and summer for males. Conclusions: These findings highlight the need for comprehensive mental health targeted interventions and preventive strategies that account for gender-specific disparities, age-related vulnerabilities, and the specific characteristics of neighborhoods.
Keywords
Suicide-related emergency calls 112 emergency number, Spatio-temporal analysis, Bayesian autoregressive modeling, Gender-specific analysisCite this article as: Marco, M., López-Quílez, A., Sánchez-Sáez, F., Escobar-Hernández, P., Montagud-Andrés, M., Lila, M., & Gracia, E. (2024). The Spatio-Temporal Distribution of Suicide-related Emergency Calls in a European City: Age and Gender Patterns, and Neighborhood Influences. Psychosocial Intervention, 33(2), 103 - 115. https://doi.org/10.5093/pi2024a8
Correspondence: miriam.marco2@uv.es (M. Marco).Suicide is a social and public health problem that is receiving increasing interest around the world. In 2019, approximately 703,000 people died by suicide (WHO, 2021). The latest European data show a rate of 10.5 deaths by suicide per 100,000 inhabitants, which rises to 17.1 in the case of male victims (WHO, 2021). In Spain, where this study took place, suicide is currently the leading cause of external death; in 2022 the number of suicide-related deaths reached a record high of 4,097 (Spanish Statistical Office, 2023), the equivalent of eleven people who died by suicide each day. This represents a rate of 8.5 suicides per 100,000 inhabitants. In response, bodies such as the World Health Organization have added suicide to their list of public health priorities, designing prevention strategies such as the 2013-2020 Mental Health Action Plan, which has been extended to 2030, and the WHO’s 13th General Programme of Work 2019-2023, with the aim of reducing suicide rates by one third and promoting mental health and well-being (WHO, 2013, 2021). Several studies have analyzed the risk factors associated with suicide from an individual perspective. Factors such as a family history of suicide and previous attempts, alcohol abuse, mental illness or job loss have been associated with an increased risk of suicide (Cramer & Kapusta, 2017; Favril et al., 2022; Hawton & van Heeringen, 2009). Furthermore, extensive research has consistently demonstrated significant gender differences in suicide risk and mortality, revealing a substantially higher overall risk and mortality rates among males than females (Skogman et al., 2004; WHO, 2021). Other research has assessed the relationship between community risk factors and suicide risk (Dykxhoorn et al., 2023; Hoffman et al., 2020; Kandula, Martínez-Alés, et al., 2023; Marco et al., 2018; Rehkopf & Buka, 2006; Vandoros & Kawachi, 2021; Xi et al., 2023; Yoshioka et al., 2022). Results suggest that community-level variables related to social deprivation (for example, poverty, educational level, or unemployment), social fragmentation (i.e., high mobility of residents, a high percentage of single people or high rates of divorce), and rurality are associated with higher suicide rates (Congdon, 2011; Dykxhoorn et al., 2023; Hawton et al., 2001; Marco et al., 2018; Näher et al., 2020). In line with these studies, an increasing number of researchers have pointed to spatial patterns of suicide that can go beyond individual elements to explain part of the suicide risk (Baller & Richardson, 2002; Santana et al., 2015; Sung et al., 2021; Tran & Morrison, 2020). Spatial models allow for the study of the spatial distribution of suicide risks, with a focus on high-risk areas and the community-level risk factors related to this elevated risk (Rocha & Nunes, 2020; Orndahl & Wheeler, 2018; Sung et al., 2021). In addition, they can incorporate the temporal dimension so that the spatial distributions of suicide risk can be analyzed over the years. This allows for a detailed analysis of the temporal changes of suicide over time, providing specific-area variations, as well as analyzing the areas that remain chronically at high risk of suicide (Helbich et al., 2017; Liu et al., 2015; Marco et al., 2018). Spatio-temporal approaches, originally developed in the field of medicine and epidemiology, have increasingly been used to shed light on the spatial patterns of a range of social problems. Numerous studies have analyzed the spatio-temporal distribution of phenomena such as crime (Law & Quick, 2013; Sparks, 2011), drug and alcohol consumption and sale (Treno et al., 2007; Zhu et al., 2006), intimate partner violence (Cunradi et al., 2011; Gracia et al., 2015; Gracia et al., 2021), and child maltreatment (Freisthler et al., 2007; Gracia et al., 2017, 2018; Marco et al., 2019; Marco et al., 2020; Morris et al., 2019), among others. Previous research using a spatio-temporal approach has indicated that suicide is not randomly distributed in space and time. Rather, there are certain areas with higher or lower suicide risks, which are closely related to community-level characteristics such as social deprivation, social fragmentation, and rurality, as identified by ecological studies (Helbich et al., 2017; Marco et al., 2018; Yoon et al., 2015; Yoshioka et al., 2022). Additionally, numerous studies have revealed a seasonal pattern, with a peak in suicide rates during the spring and summer months (Marco et al., 2018; Marco et al., 2017; Silveira et al., 2016; Woo et al., 2012). A recent systematic review has analyzed the application of spatial analysis to understanding the association between socio-economic area-level characteristics and suicide outcomes (Qian et al., 2023). The findings revealed a significant increase in the application of spatial statistical approaches, such as Bayesian hierarchical modeling and spatial regression analysis. Bayesian approaches have demonstrated their capacity to address spatial autocorrelation, which can introduce bias and influence the accuracy of findings. The studies these authors reviewed consistently identified an inverse relationship between socio-economic status and suicide risk. The review contributes valuable insights by confirming previous findings that higher deprivation, higher unemployment rates, lower income, and lower education levels are associated with increased suicide rates. It highlights the significant role of socio-economic inequalities as a key social determinant in suicide. The impact of socio-economic factors on suicide, however, varies across areas, indicating that tailored responses are necessary to address specific contributing factors in each region (Qian et al., 2023). This systematic review highlights that most studies have primarily concentrated on analyzing spatial and spatio-temporal patterns of the entire population, overlooking the gender of the individual in crisis. However, evidence from various sources have revealed gender disparities in suicide rates, methods, and risk factors (Boeninger et al., 2010; Oquendo et al., 2001; Skogman et al., 2004; Villanueva et al., 2019). Therefore, to avoid aggregation biases, some ecological studies have also evaluated the spatial patterns of male and female suicide outcomes (Cayuela et al., 2020; Chang et al., 2011; Lin et al., 2019). The Present Study Although previous papers have studied the spatial and temporal determinants of suicide, they have mainly relied on mortality data and suicide-related health records (Amin et al., 2022; Congdon, 2011; Fontanella et al., 2018; Helbich et al., 2017; Jiang et al., 2021; Khademi et al., 2022; Qian et al., 2023). However, other valuable sources, such as emergency calls, have received limited attention in the research (Lersch, 2020b; Marco et al., 2018; Marco et al., 2017). In Qian et al.’s (2023) systematic review, only one of the 58 papers they looked at used suicide-related emergency calls as an indicator of suicide (Marco et al., 2018). Recently, scholars have emphasized the importance of promoting epidemiological research on suicide to design new strategies that provide better insights into suicide and its risk factors (Zalsman et al., 2017). They highlight the significance of including suicide attempts in studies to enhance our understanding of this complex issue. Our research aims to bridge this gap in the literature by examining the spatio-temporal distribution of emergency calls, which encompass a broader spectrum of the issue of suicide. This includes a wide range of suicide-related emergency situations, such as active suicidal thoughts, suicide attempts, or death by suicide. In this study, we examined suicide-related emergency calls made to the 112 service. The emergency telephone number 112 is the equivalent of 911 in the United States, and it operates similarly across European countries. Many suicide events are reported via the 112 service, with either the individual in crisis – someone experiencing distress or facing a suicidal situation – directly seeking assistance, or a bystander – a family member, friend, or anonymous individual at the scene – making the call on their behalf. To the best of our knowledge, there are no published studies that have specifically assessed 112 emergency calls, and only a few studies have used suicide-related emergency call records from other sources such as 092 (local police) or 911 numbers (Lersch, 2020a, 2020b; Marco et al., 2018; Marco et al., 2017). Understanding how 112 suicide-related calls are distributed, and their evolution over the years, can generate further scientific evidence on the specific community characteristics that are related to suicide risk, as well as providing a tool for detecting areas with a higher level of suicide-related emergency calls, where a greater number of resources is needed, and can subsequently guide prevention and intervention efforts. Thus, we conduct a comprehensive spatio-temporal analysis of suicide-related 112 emergency calls in the city of Valencia, Spain, over a six-year period (from 2017 to 2022). We first examine age and gender patterns, and then explore the influence of neighborhood characteristics on the general and gender-specific spatio-temporal patterns of these calls. By doing so, we aim to uncover spatial patterns and temporal trends specific to each gender, thus providing valuable insights into the complex dynamics of suicide-related emergencies within the city. Study Area and Outcome Suicide-related emergency calls in the city of Valencia were collected from the 112 emergency service of the Valencian Community, covering the period from 2017 to 2022. The suicide-related emergency calls include any request from a person in crisis or a bystander reporting suicidal behavior. Each event is only recorded once to prevent duplication. If the same event is reported multiple times (for example, if two different bystanders make two different calls), the system collapses the information to produce a single result and send emergency assistance only once. Every call incorporates geocoded information with the coordinates of the suicide event location, along with the date and time of the call. Demographic information is also recorded, including gender (female or male) and age (in discrete values) of the individual in crisis, along with a brief description of the event as provided by the caller. Over the six-year study period, the 112 service received a total of 10,030 suicide-related emergency calls in the city of Valencia, 4,023 of which involved males in crisis and 6,007, females in crisis. Each call was geolocated on a map of Valencia. R statistical software was used (R Core Team, 2023) to work with this geographic information. “Shapefiles” (where the geometric location and attribute information of geographic features are stored) are uploaded to this software, which displays maps with the geographic coordinates located on them. As unit areas, census block groups were used as proxies for neighborhoods; this is the smallest geographic unit with available information. In total, Valencia is composed of 560 census block groups. The anonymization of the data was guaranteed and only aggregated information was used because of the sensitivity of data. The calls were geolocated using trimestral resolution as the temporal unit, which enabled us to assess the effect of seasonality in the temporal trends. A total of 24 periods (six years with four trimesters) were considered, defined as Trimester 1, January to March, Trimester 2, April to June, Trimester 3, July to September, and Trimester 4, October to December. Three models were constructed: an overall model with all the data on suicide-related emergency calls and two specific models according to the gender of the individual in crisis (male or female). Table 1 shows the distribution of suicide-related emergency calls by gender and year. Tabla 1 Distribution of Suicide-related Emergency Calls by Year according to the Gender of the Individual in Crisis 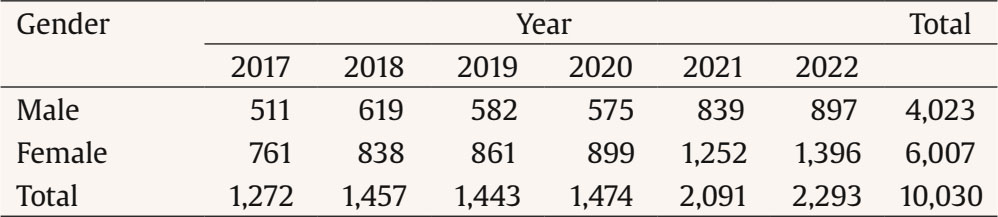 Covariates Several indicators were assessed at the census block group level (see Table 2 for descriptive statistics). Based on previous studies (Congdon, 2011; Marco et al., 2018; Yoshioka et al., 2022), social deprivation, social fragmentation and a proxy for rurality were assessed for their association with the spatio-temporal distribution of suicide-related emergency calls. In addition, following Marco et al. (2018), other neighborhood-level covariates (aging population and immigrant concentration) were collected. Finally, seasonality was also incorporated as a covariate to measure differences by trimester (Marco et al., 2018). The covariates were provided by the Valencia City Hall Statistics Office. Table 2 Variables (Mean, Standard Deviation, Minimum and Maximum Values) at the Census Block Group 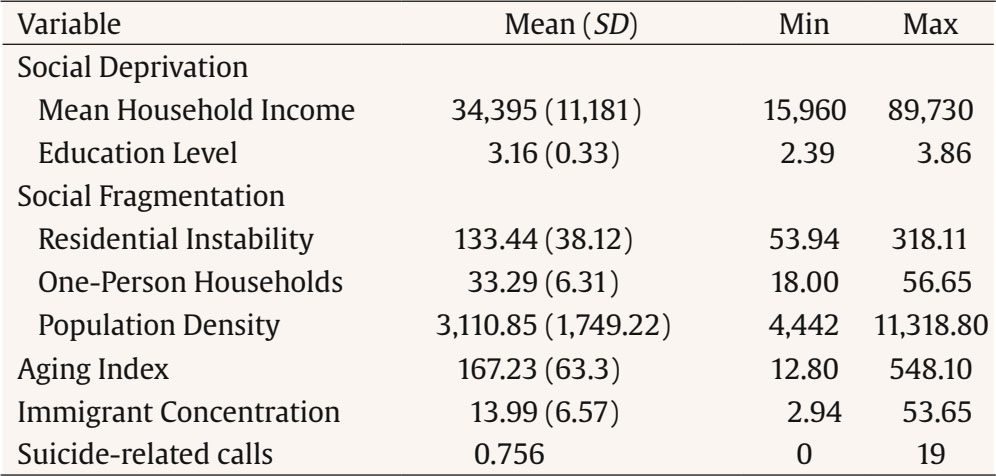 Note. SD = standard deviation; Min = minimum; Max = maximum. Social Deprivation Mean household income was used as an indicator of economic status. In addition, educational level was introduced as the average level of education of each one of the census block groups on a 4-point scale, where 1 = less than primary education, 2 = primary education, 3 = secondary education, 4 = college education. Social Fragmentation We used two indicators to measure social fragmentation. First, residential instability was calculated as the proportion of the population that had moved into or out of each census block group during the previous year (rate per 1,000 inhabitants). Second, one-person households were measured as the number of households with only one person per total number of households. Rurality Since the study area was limited to the census block groups within the city, we were unable to assess rurality directly. However, population density (calculated as square kilometer per 1,000 individuals) was used as a proxy for rurality, as in previous studies (Congdon, 2011; Marco et al., 2018). Other Neighborhood-Level Variables In addition, we introduced two neighborhood-level demographic variables: the aging population index, which is calculated as the ratio of elderly (65 years or older) to youth (15 years or younger) population, and the percentage of immigrant population in each census block group. Seasonality Finally, to explore the effect of seasonality, a dummy variable was introduced, using three binary variables that account for the first three natural trimesters (January-March, April-June, and July-September); the fourth trimester (October-December) was the reference trimester. Data Analysis To comprehensively explore the distribution of suicide-related emergency calls, a detailed demographic descriptive analysis was first conducted. This analysis aimed to provide an understanding of how these calls were distributed among different gender and age groups. Secondly, we applied hierarchical Bayesian models. The Bayesian approach combines the construction of complex models with the inclusion of previously known information on the parameters. In this approach, the prior information can be modeled by decomposing it into different levels or layers, which enables researchers to differentiate between elements of the model structure and elements referring to external information. In addition to incorporating the uncertainty about the parameters through prior distributions, hierarchical models allow random effects to be included in some of their layers, in our case, the spatial and temporal structure. A conditionally independent Poisson distribution was used to model the number of suicide-related emergency calls: where Eit represents the expected number of calls in census block group i during period t in proportion to the population, and ηit is the log relative risk for each area and period. To account for the spatial structure, we introduced a random effect that determines the spatial autocorrelation, which relates the neighboring areas to detect the spatial structure of the data, using a queen contiguity weight matrix to assess vicinity. In addition, a random effect that controls for the overdispersion was introduced to avoid the bias of the existing heterogeneity in the data matrix. Finally, another random variable accounting for the temporal effect was included to detect variations in suicide calls over time. This modeling was specified as a spatio-temporal autoregressive Bayesian model. This approach allows area-specific levels of suicide-related emergency calls to be mapped and differences analyzed over time because it combines the application of autoregressive time series and spatial modeling using a spatio-temporal structure where relative risks are both spatially and temporally dependent (Martínez-Beneito et al., 2008). The log relative risk η for the first period (first trimester of 2017) was defined as: and the relative risks for the following periods were defined as: where μ is the intercept, αt is the mean deviation of the risk in the period t, ρ represents the temporal correlation between the spatial effects of each period, and ϕit and θit refer to structured and unstructured spatial random effects, respectively. Xi is the vector of covariates (social deprivation, social fragmentation, population density, aging index, immigrant population, and seasonality), and β is the vector of regression coefficients. Following the Bayesian approach, we considered a variable as relevant to the model if its posterior probability of being greater or lower than zero (i.e., in either the positive or negative direction) exceeded .95. After a sensitivity analysis, appropriate prior distributions were assigned for the parameters following the structure of Bayesian hierarchical models. Vague Gaussian distributions were used for the fixed effects β; μ was modeled as an improper uniform distribution; the temporal correlation ρ was specified as a uniform U(-1,1); and the structured effect ϕ was specified by a conditional spatial autoregressive (CAR) model (Besag et al., 1991): where ni is the number of neighbors in each census block group i, ϕ-i represents the values of the ϕ vector except the component i, σϕ accounts for the standard deviation parameter, and j~i is the units j neighbors of census block group i. The unstructured spatial effect θ was modeled by means of independent identically distributed Gaussian random variables N(0,σθ2). Finally, uniform distributions were used for the three hyperparameters σα,σϕ,σθ~U(0,1). Monte Carlo simulation techniques using Markov Chain Monte Carlo (MCMC) were applied for statistical inference, implemented by the R software and the R2WinBUGS package. Three chains with 50,000 iterations were generated, with the first 10,000 discarded as burn-in. To ensure the robustness of the results, we checked the convergence of the chains through visual inspection of simulated chains and using the R-hat convergence diagnosis which was close to 1.0 for all parameters. We conducted three different spatio-temporal models. First, we developed an overall spatio-temporal model using the total number of suicide-related emergency calls in order to explore the general patterns and trends. We then performed separate models based on the gender of the individual in crisis (male and female). This approach enabled us to uncover gender-specific spatial patterns and temporal trends. Relative risk mapping was carried out to identify areas where the level of suicide-related emergency calls consistently exceeded the city’s average level in the different models. Mapping was also carried out using R. Descriptive Analysis Figure 1 and Figure 2 show the incidence of suicide-related emergency calls over the study period for the overall and the gender-specific calls, respectively. In the case of overall emergency calls, a clear upward trend can be observed starting from the initial period in 2017. The number of calls rose steadily from initial fluctuations around 350 calls per trimester to over 600 calls in the second trimester of 2022. A notable change in trajectory occurred in 2021 when the rate of increase intensified. Prior to 2021, the highest number of emergency calls was consistently recorded in the third trimester (July to September). However, the second trimester (April to June) of 2022 reflected the highest incidence throughout the entire study period. The upward trend has persisted, continuing to rise towards the end of 2022. Figure 1 Temporal Trends of Suicide-related Emergency Calls for Overall Calls by Trimester. 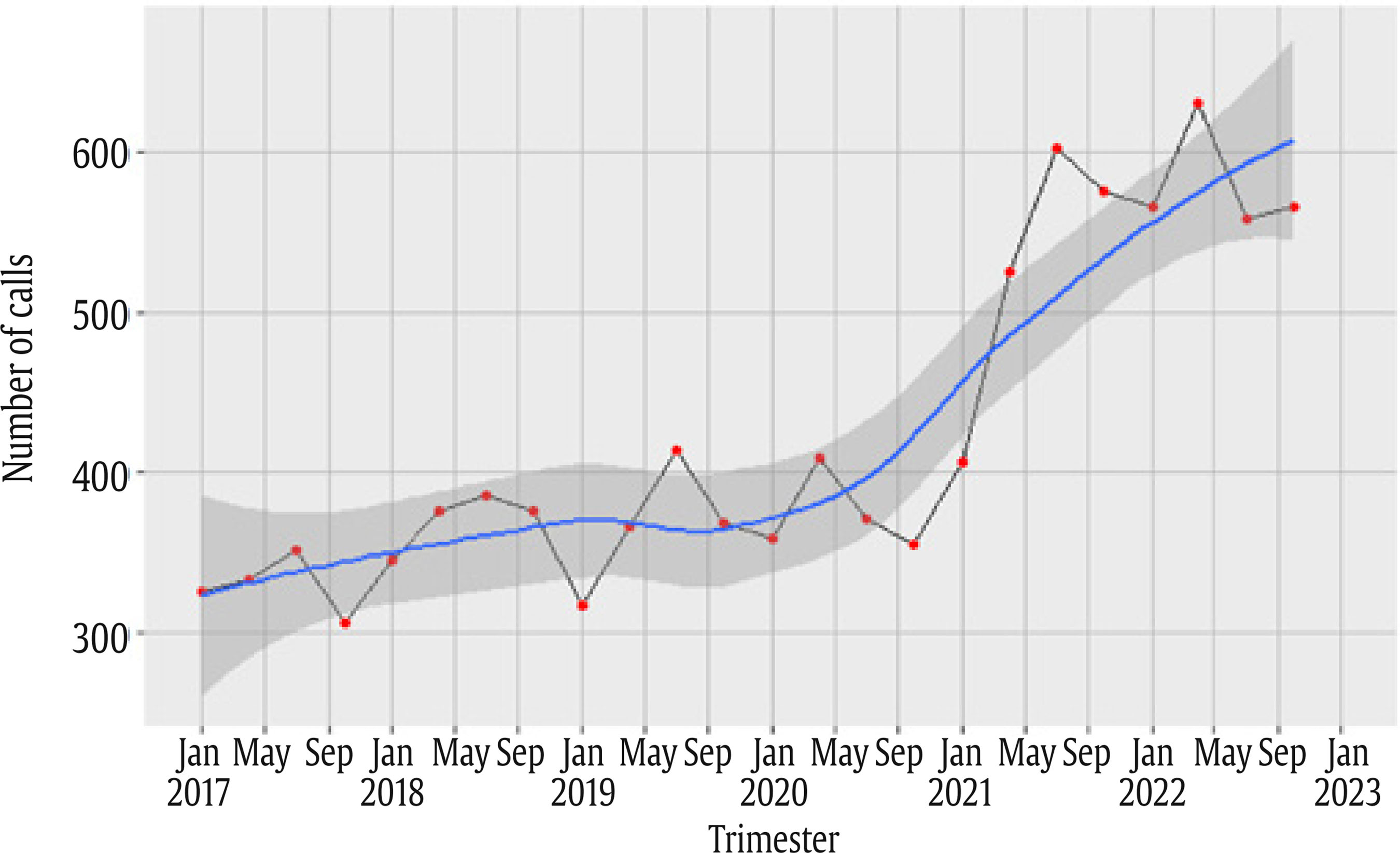 Figure 2 Temporal Trends of Suicide-related Emergency Calls Based on the Gender of the Individual in Crisis by Trimester. 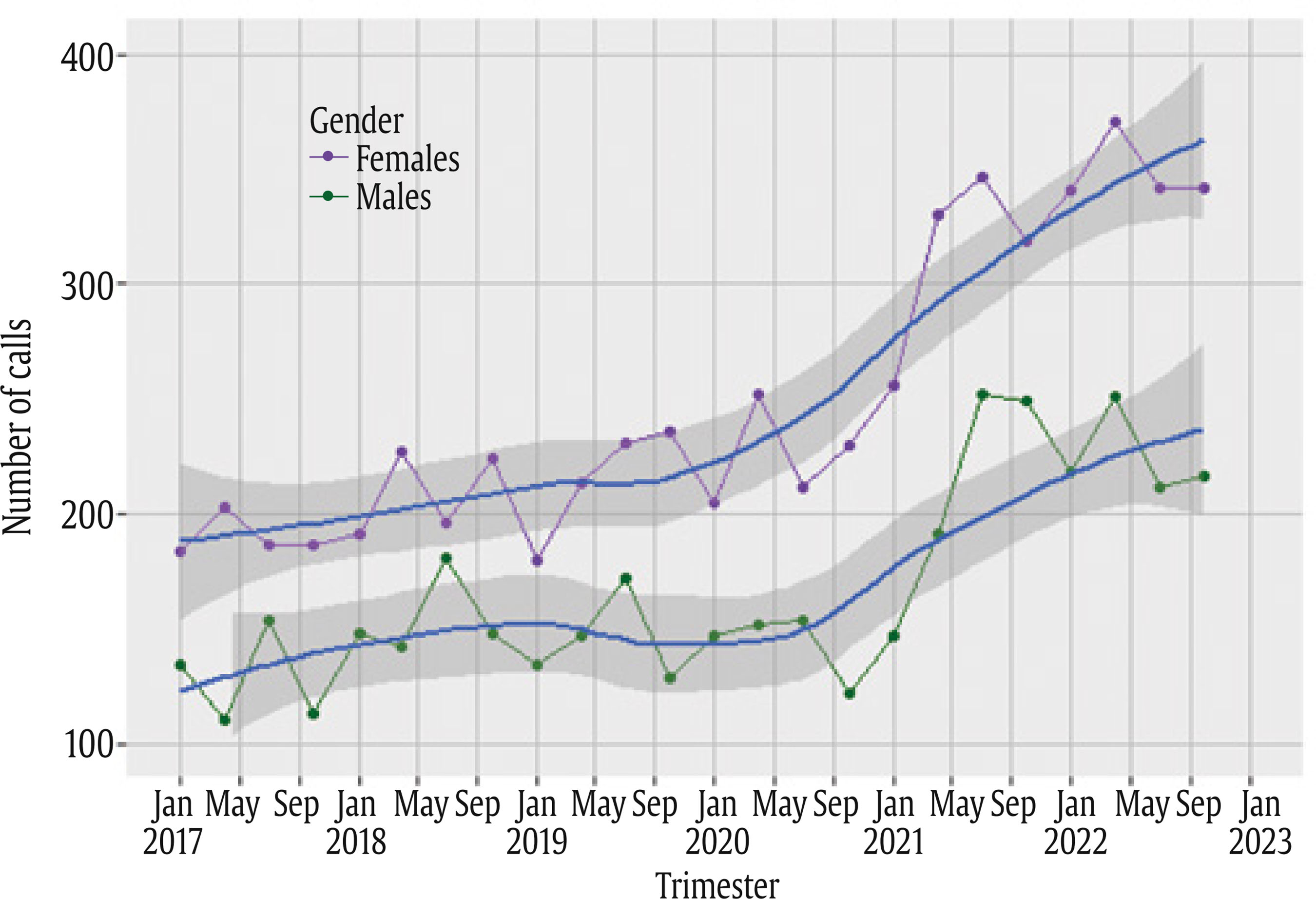 Comparable findings can be observed in the data disaggregated by gender (Figure 2). Specifically, when examining calls involving males in crisis a higher incidence of calls was consistently recorded in the third trimester. Conversely, the second trimester tended to have the highest incidence of calls involving females in crisis. However, 2021 emerges as pivotal in both cases, marking a notable shift in the pattern. Figure 3 Yearly Distribution of Suicide-Related Emergency Calls by Age of the Individual in Crisis. 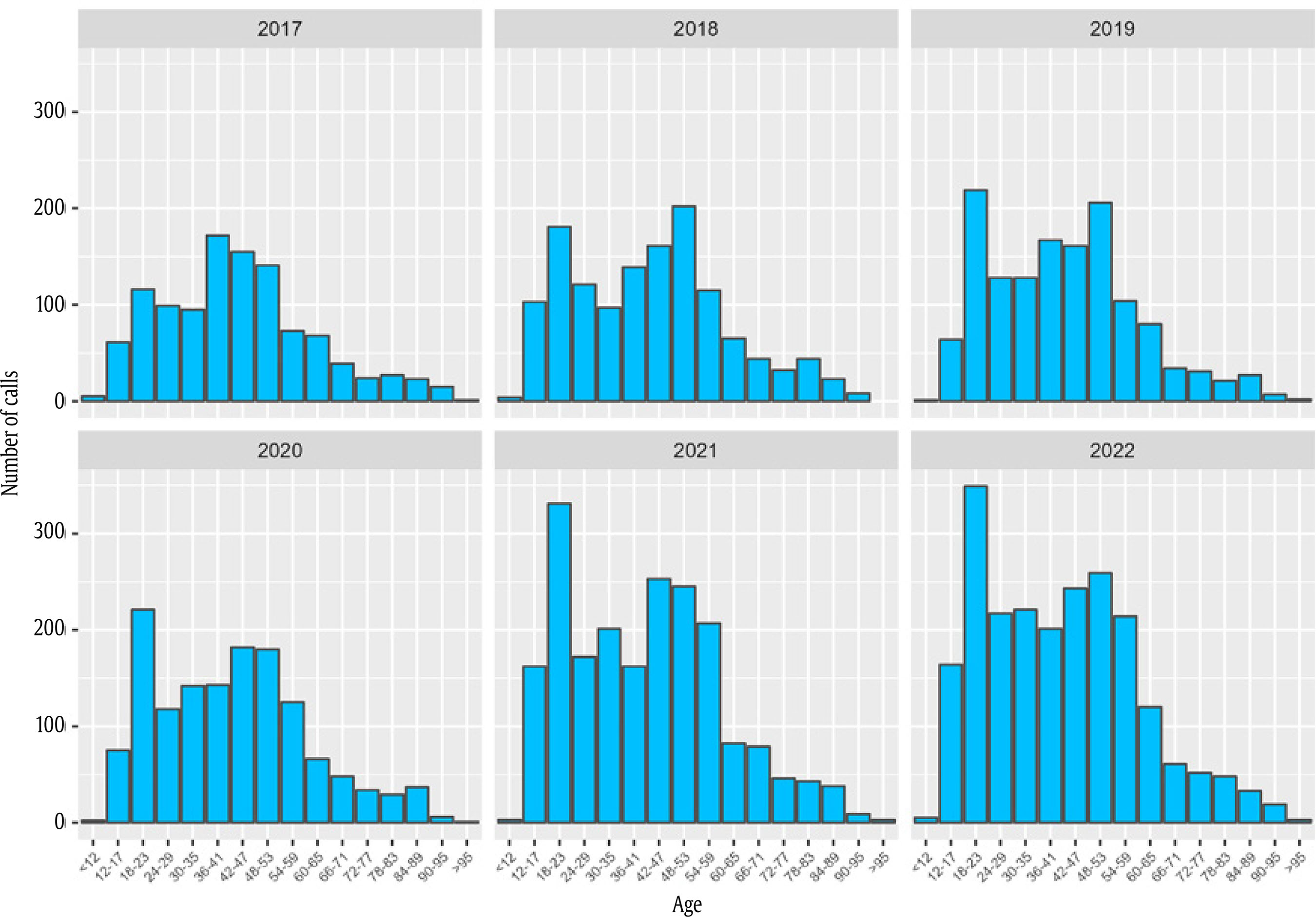 Figure 3 illustrates the yearly distribution of suicide-related emergency calls across different age groups. In the initial two years of the study period, the highest number of calls was related to the middle-aged group. However, from 2019 onward, the number of calls involving individuals in crisis between the ages of 18 and 23 increased substantially, ultimately making it the age group with the highest call volume throughout the entire period. Similarly, we also analyzed the distribution of calls by age groups taking into account the gender of the individual in crisis (Figure 4). The results reveal a distinct pattern based on gender: for females in crisis, an increase in calls is observed in the 18- to 23-year-old age group, which aligns with the findings from the overall calls. However, the same pattern is not observed for males in crisis. While there was an increase in the number of calls in the 18- to 23-year-old age group, the middle-aged group still exhibits a higher number of calls, particularly for those aged between 42 and 53, with the exception of 2020 when the 18- to 23-year-old age group had more. Figure 4 Yearly Distribution of Suicide-related Emergency Calls by Age and Gender of the Individual in Crisis. 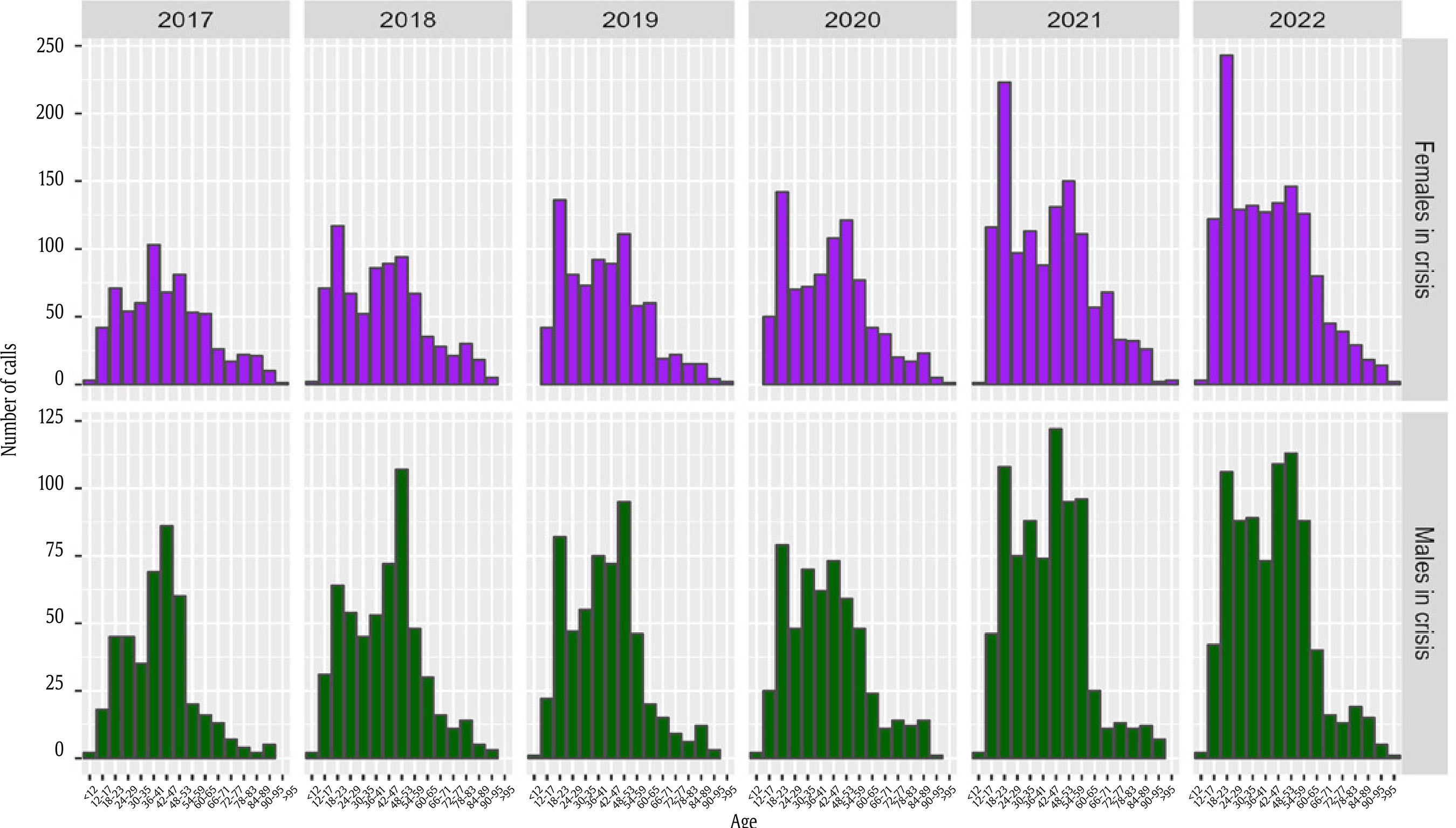 Spatio-Temporal Models Table 3 presents the findings of the spatio-temporal models for suicide-related emergency calls, including the overall model and the gender-specific ones. In the overall model, several factors were found to be associated with higher levels of suicide-related emergency calls. These factors included lower education level, greater residential instability, lower population density, increased aging, and higher immigrant concentration. Mean household income and percentage of one-person households did not show a relevant association with suicide-related emergency calls. Table 3 Results of the Bayesian Autoregressive Model for the Overall Model and the Gender-specific Models 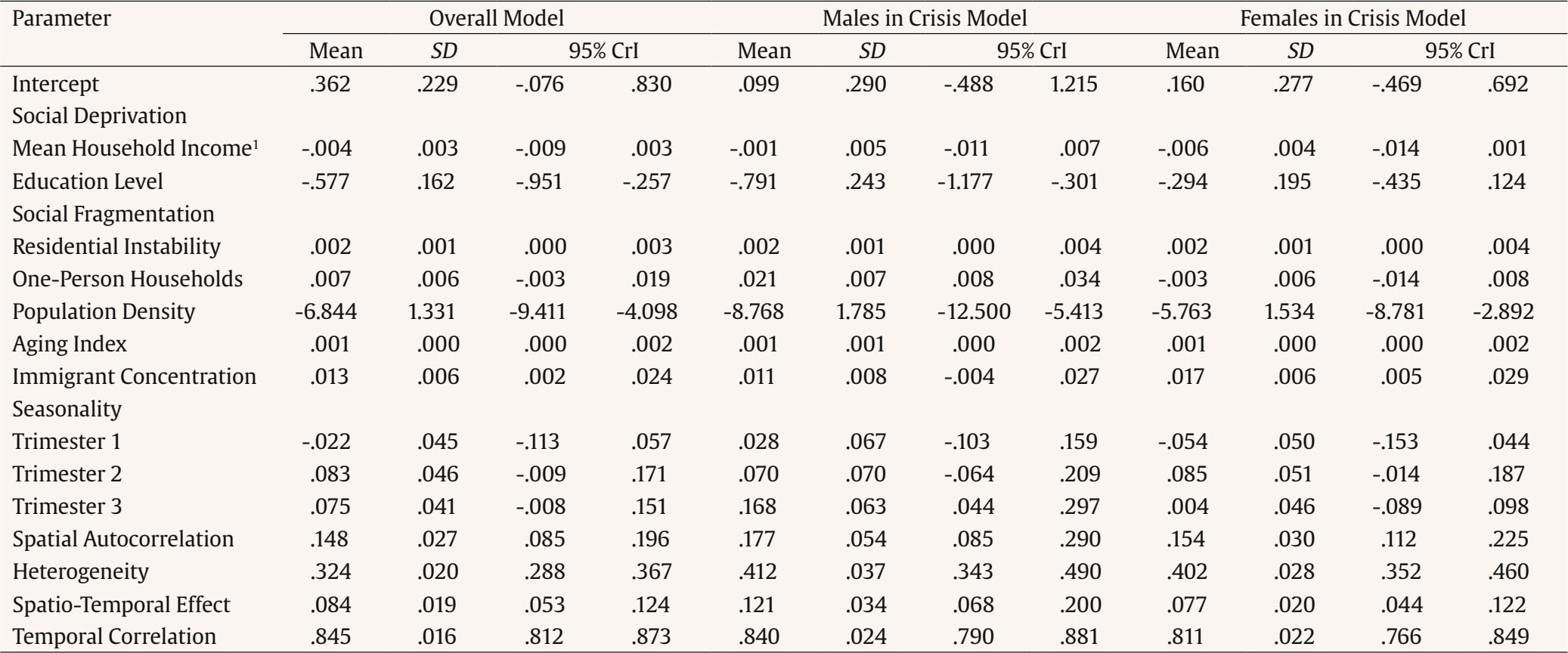 Note. SD = standard deviation; CrI = credible interval 1 Mean household income was divided by 1,000 to solve computation problems. Comparable results emerged for males in crisis, with higher levels of suicide-related emergency calls observed in areas characterized by lower education level, increased residential instability and one-person households, lower population density, and greater aging. Mean household income and immigrant concentration were not relevant in the model for males in crisis. On the other hand, for females in crisis, residential instability, population density, aging, and immigrant concentration showed relevant relationships with suicide-related emergency calls. Education level, mean household income and one-person households were not relevant. Thus, areas with higher levels of suicide-related emergency calls were those characterized by higher residential instability, lower population density, and higher aging and immigrant concentration. Seasonality was also found to be relevant, but it differs depending on the model: in the overall model, the levels of suicide-related emergency calls increased in the second and in the third trimesters; for males in crisis, the increase occurred during the second trimester (from April to June), while for females in crisis, the increase was observed during the third trimester (from July to September). Additionally, a strong temporal correlation was observed across all models, indicating a high degree of similarity between consecutive trimesters for both males and females in crisis. Specifically, the overall model yielded a temporal correlation coefficient of ρ = .845, the males in crisis model had a correlation coefficient of ρ = .840 and the females in crisis model, ρ = .811. This indicates a consistent pattern where each trimester closely resembles the preceding trimester in terms of suicide-related emergency calls for both genders. Relative Risk Maps Figures 5 to 7 depict the relative risks associated with the trimesters of the first and last years in the three models. The maps display census block groups painted in red to indicate a higher risk than the city average (values greater than 1), while blue areas indicate a lower risk than the city average (values lower than 1). White areas (values from 0.9 to 1.1) indicate the average risk. The spatial patterns changed remarkably across the time periods analyzed, revealing a clear and general increase in the levels of suicide-related emergency calls, affecting both males and females. While certain areas such as the north-west part of the city maintained consistently low values of relative risk for suicide-related emergency calls over the years, most census block groups experienced an increase in the levels of such calls. Figure 5 Maps of the Relative Risk of Overall Suicide-related Emergency Calls by Trimesters in the First (2017) and the Last (2022) Years in the City of Valencia, Spain. 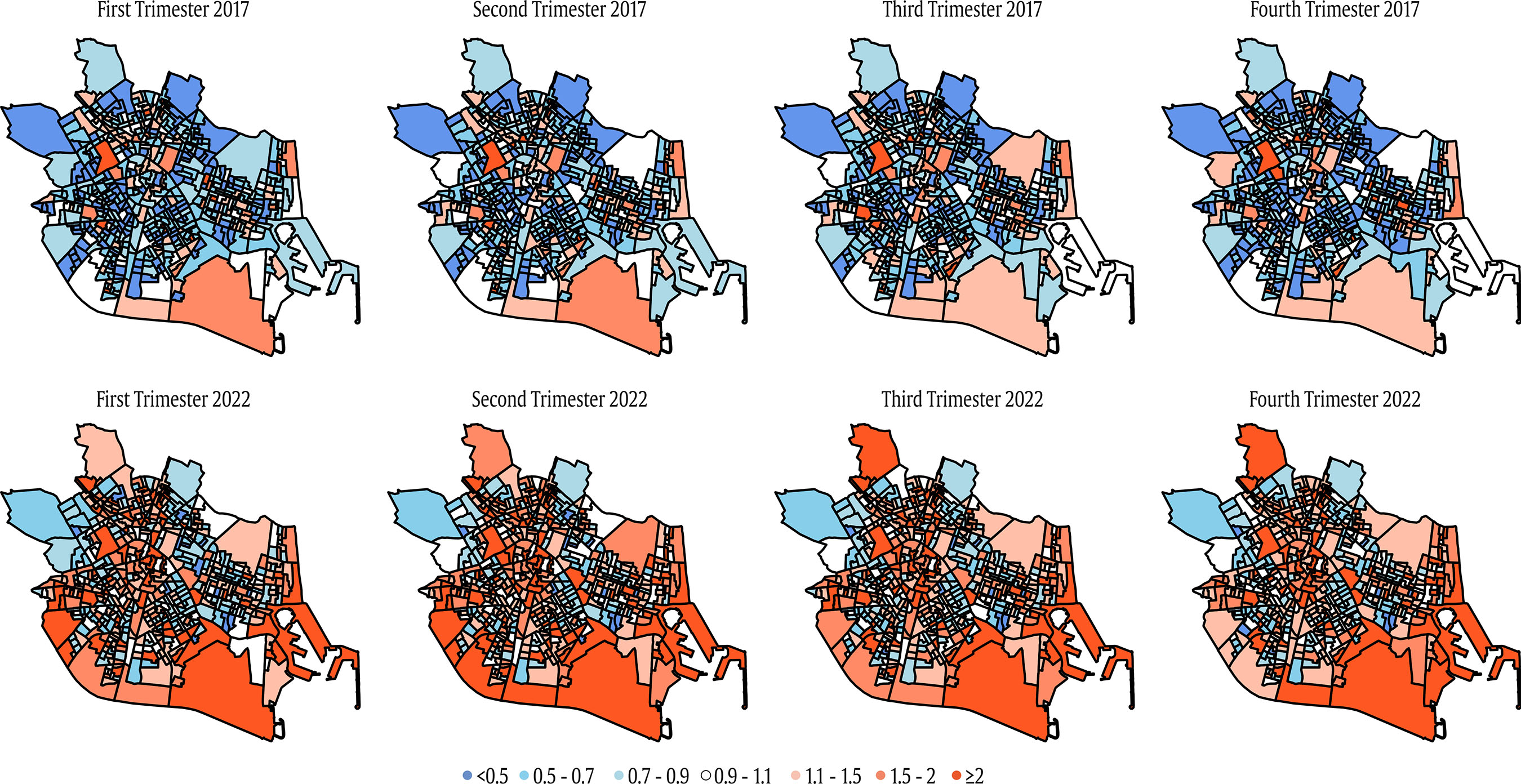 Figure 6 Maps of the Relative Risk of Suicide-related Emergency Calls for Males in Crisis by Trimesters in the First (2017) and the Last (2022) Years in the City of Valencia, Spain. 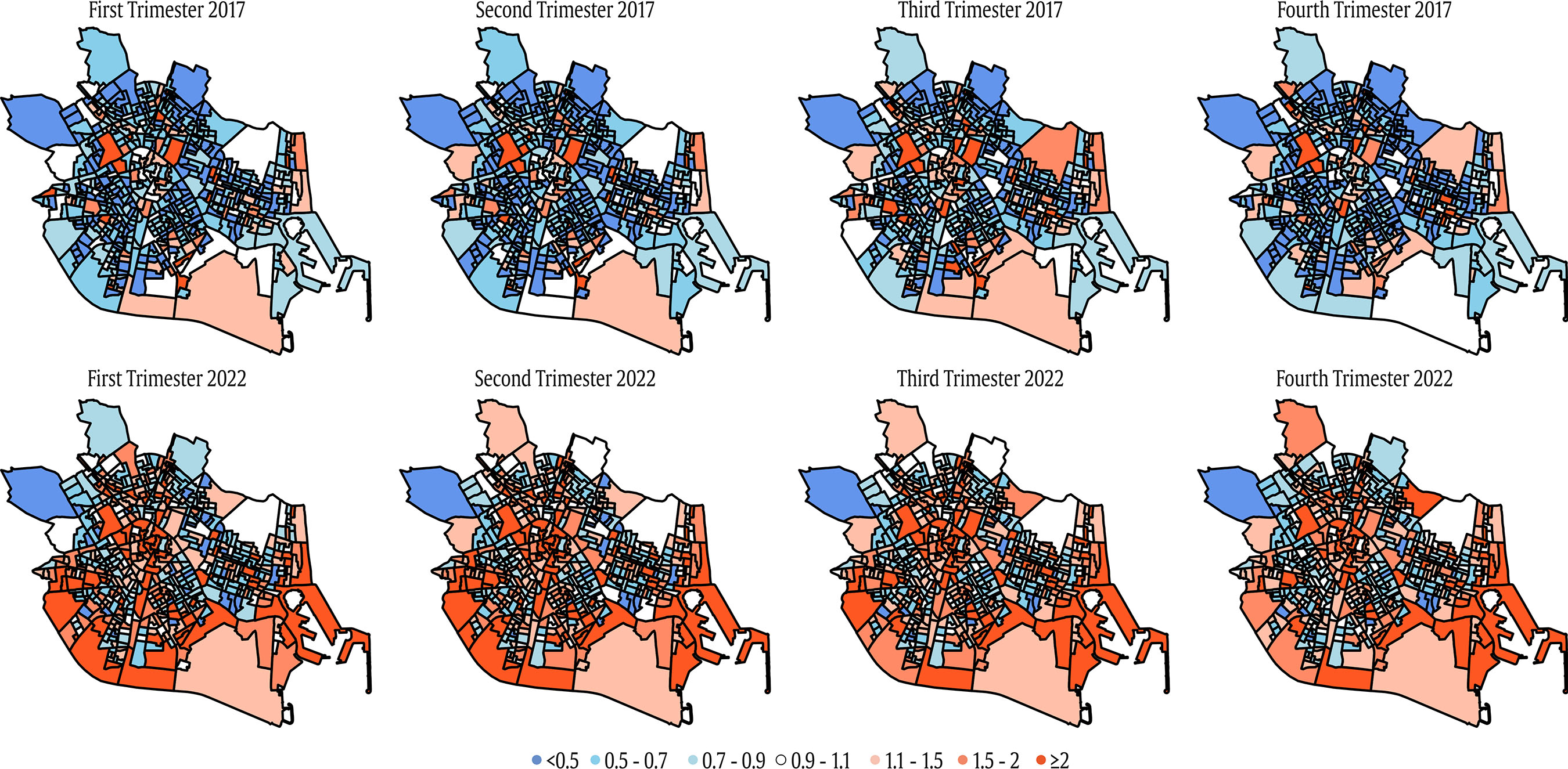 Figure 7 Maps of the Relative Risk of Suicide-related Emergency Calls for Females in Crisis by Trimesters in the First (2017) and the Last (2022) Years in the City of Valencia, Spain. 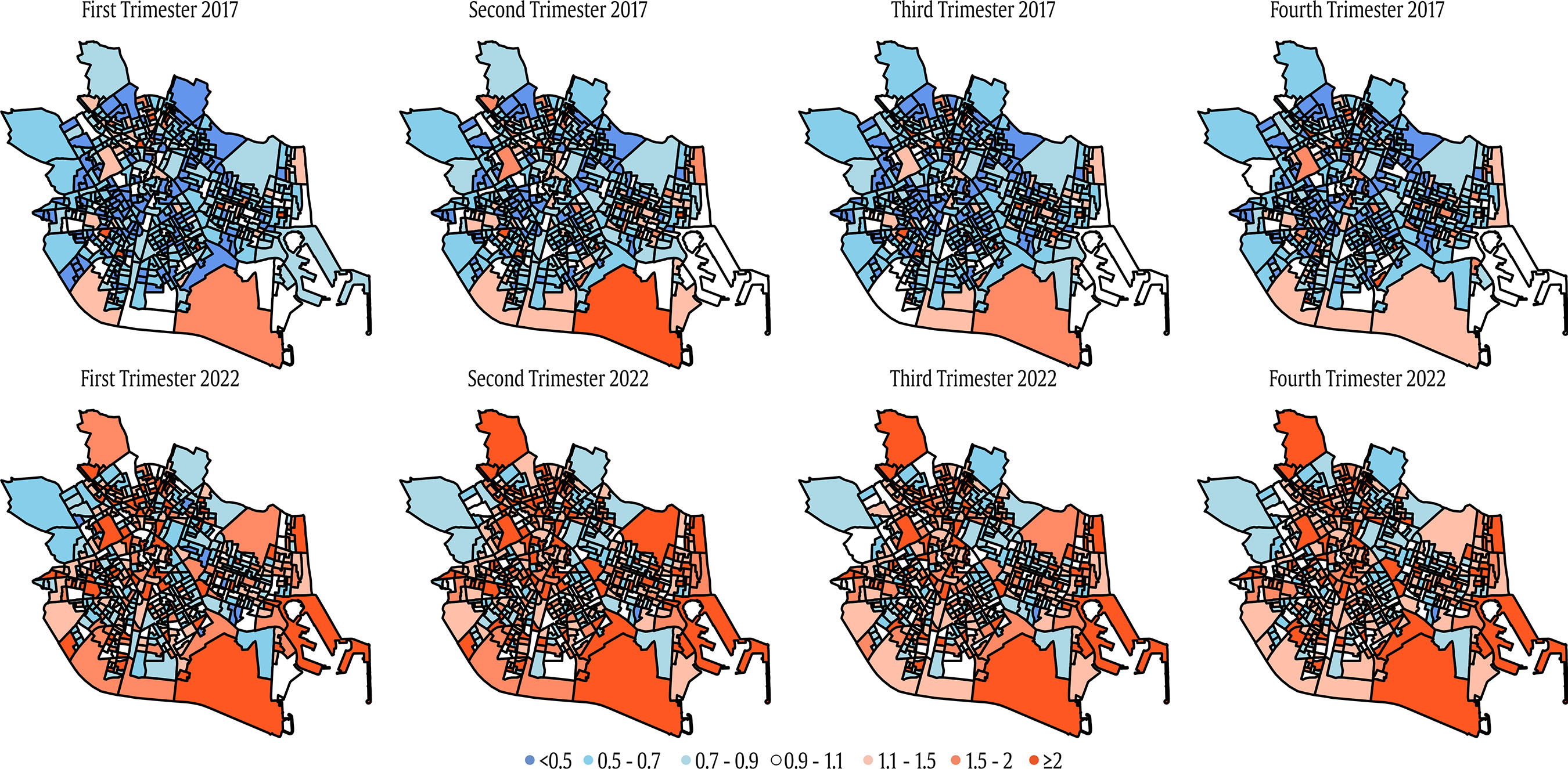 Despite this general increase, the gender-specific models display distinct patterns. For instance, some census block groups located in the city center had high levels of calls for males in crisis from the beginning of the study period. However, for females in crisis, these areas initially had low levels of emergency calls, but were twice the average by 2022. To analyze these differential spatial patterns, we provide a figure with the maps of the relative risk for suicide-related emergency calls for the last period (last trimester of 2022) in the three models (Figure 8). While the patterns across the models are generally similar, local variations can be observed, with certain census block groups indicating higher levels of suicide-related emergency calls for males in crisis, but lower levels for females in crisis. It is important to note that the overall model combines both relative risks and may introduce distortions in the explanations. Figure 8 Comparison Between the Maps of the Relative Risk of Suicide-related Calls according to the Gender of the Individual in Crisis (Last Trimester of 2022) in Valencia, Spain. 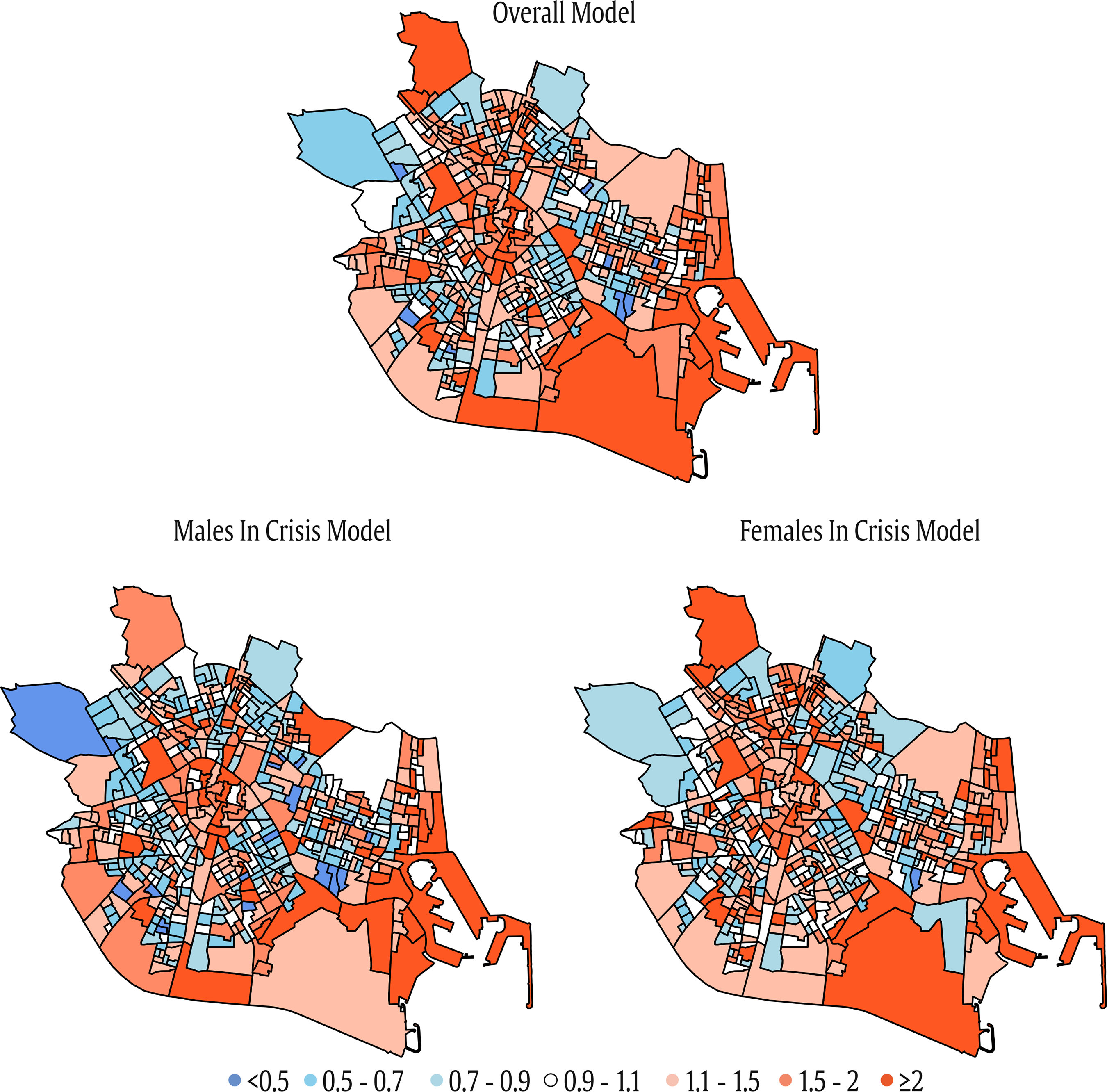 The aim of this study was to analyze the spatio-temporal distribution of suicide-related emergency calls from 2017 to 2022 in Valencia, Spain. We first conducted a descriptive analysis to assess the gender and age patterns of suicide-related emergency calls. We then explored the influence of neighborhood-level characteristics on the general and gender-specific spatio-temporal patterns of suicide-related emergency calls. The descriptive analysis findings consistently depicted a scenario where suicide-related calls concerning females in crisis outnumbered those involving males in crisis. Previous data consistently show a higher incidence of suicide deaths in men (WHO, 2021), while women experience a higher rates of suicide attempts, suicide planning, and suicidal thoughts (Ivey-Stephenson et al., 2022). Our results are consistent with these findings, as many emergency calls involve suicide attempts or ideations prompting requests for emergency assistance rather than actual fatalities, which may explain the higher incidence of female-related suicide calls. This gender difference can be attributed to the fact that women tend to be more inclined to seek help when dealing with suicidal thoughts (Fernández-Montalvo et al., 2021; Villanueva et al., 2019). One explanation lies in traditional gender roles and expectations, which may play a role in the higher suicide rates observed among males. Men are often socialized to embody qualities of self-sufficiency, which can hinder their willingness to seek help for mental health concerns (Addis & Mahalik, 2003). Consequently, this may lead to a greater likelihood of untreated depression and other mental health issues (Smith et al., 2018), thereby increasing the risk of suicide, but may not have a direct impact on the incidence of suicide-related emergency calls. The gender disparities in suicide outcomes are undoubtedly complex and multifaceted. Further research is needed to fully understand the factors that contribute to these differences and to develop effective prevention and intervention strategies that consider the unique needs and experiences of both males and females. On the other hand, the descriptive analysis based on age yielded noteworthy insights. While in the initial year (2017) the age group with the highest frequency of calls was the 36- to 41-year-old group, followed by 42-47 and 48-53, there was a significant increase in the 18- to 23-year-old age group over the study period. Starting from 2020, this age group exhibited a strikingly elevated incidence, clearly surpassing the middle-aged population. One possible explanation for this increase could be the impact of the COVID-19 pandemic. The pandemic has had a profound effect on mental health, leading to increased stress, symptoms of depression and anxiety, and heightened social isolation (Gunnell et al., 2020; Sher, 2020; Vahratian et al., 2021; WHO, 2022), and some studies have suggested that these impacts have been particularly pronounced among young people (Bell et al., 2023), who have endured the consequences of school closures and broader social restrictions (COVID-19 Mental Disorders Collaborators, 2021). Other factors may have also played a role, as the increasing trend in the 18- to 23-year-old age group is noticeable throughout the entire study period. Another possible explanation is that the growing awareness of mental health issues among youth in recent years has encouraged more young people to seek help, and additionally, parents may be more likely to reach out for their children to get help (Foulkes & Andrews, 2023). To examine age-group differences, future studies should analyze specific age-related spatio-temporal patterns. A main goal of this study was to explore the contextual determinants of suicide-related emergency calls at the neighborhood level, drawing on the existing literature (Congdon, 2011; Marco et al., 2018; Yoshioka et al., 2022). Previous research has linked neighborhood characteristics like social deprivation, social fragmentation, and rurality to the spatial distribution of suicide (Congdon, 2011; Rehkopf & Buka, 2006). Thus, we investigated the impact of social deprivation, social fragmentation, and population density as a proxy for rurality. Furthermore, we included additional neighborhood-level variables (i.e., aging and immigrant population), which have previously been explored in the context of spatio-temporal analyses of suicide (Hooghe & Vanhoutte, 2011; Marco et al., 2018). Overall, we found that those neighborhoods with a lower educational level, greater residential mobility, lower population density and higher population aging and immigrant concentration show higher levels of suicide-related emergency calls. These results align with previous research, underscoring the strong correlation between community-level suicide risk and factors such as social deprivation, social fragmentation, rurality, and population aging (Congdon, 1996, 2011; Rehkopf & Buka, 2006; Marco et al., 2018; Sugg et al., 2021; Yoon et al., 2015). The pattern for immigrant concentration in our study differs from earlier research, however. Recent ecological studies have generally either reported no significant association between suicide rates and migration rates or ethnicity (Knipe et al., 2017; Marco et al., 2018; Milner et al., 2012), or have even identified negative associations (Hoogue & Vanhoutte, 2011). The impact of immigrant concentration on suicide rates may vary depending on the specific cultural and community dynamics within the neighborhoods studied. Conducting qualitative research and considering the experiences and perceptions of immigrants and the broader community could provide valuable insights into this relationship. The results of the spatio-temporal modeling reveal notable disparities depending on the gender of the individual in crisis. The analysis indicates that areas characterized by lower education level, increased residential instability and one-person households, lower population density, and greater population aging show higher levels of suicide-related calls for males in crisis. In contrast, the levels of suicide-related emergency calls for females in crisis are higher in areas with higher residential instability, greater population density and aging, and higher immigrant concentration. These findings suggest that the influence of education level on suicide-related emergency calls is gender specific, affecting males but not demonstrating the same association in calls involving females. This is partially consistent with previous studies. Although a recent systematic review showed that, in general, social deprivation was related with both males and females (Cairns et al., 2017), some of the studies analyzed found associations for males only or particularly for males (Congdon, 2013; Huikari & Korhonen, 2015; Hsu et al., 2015; Santana et al., 2015). In addition, Congdon (2013) found that male suicide was primarily influenced by socio-economic deprivation, while female suicide was associated with anomie (i.e., social fragmentation) rather than deprivation. Regarding social fragmentation, residential instability was associated with suicide-related emergency calls in both males and females, but the percentage of one-person households was only related to suicide-related emergency calls in the case of males. Previous studies, however, found a stronger association between social fragmentation and suicide outcomes in females than in males (Congdon, 1996, 2013). The disparities in the findings may be linked to variations in study samples, characterized by demographic distinctions across diverse geographic regions. Additionally, it is noteworthy that previous studies did not specifically examine suicide-related emergency calls but instead focused on other suicide-related outcomes. Cross-cultural studies are needed to comprehensively address this issue. Finally, immigrant concentration was associated with suicide-related emergency calls, but notably, when we examined the gender-specific models, this association was observed only among females. This finding diverges from previous research, which did not identify significant gender differences in this regard (Hooghe & Vanhoutte, 2011; Milner et al., 2012). Immigrant communities often embrace their own cultural norms and social structures. These factors may influence how individuals within these communities perceive and seek help for mental health issues (Kirmayer et al., 2011). A possible explanation of these results, which would need further in-depth analysis, is that within some immigrant communities there are specific challenges or stressors that disproportionately affect women, leading to higher rates of suicide-related emergency calls. We also examined the presence of a seasonal effect to compare our findings with previous studies (Christodoulou et al., 2012; Marco et al., 2018; Salmerón et al., 2013; Silveira et al., 2016). As expected, our results indicate that seasonality has an impact on the model. Specifically, the second and third trimesters, corresponding to spring and summer (i.e., from April to September) showed higher levels of overall suicide-related emergency calls. However, the effect of seasonality varies depending on the gender of the individual in crisis. The highest level of suicide-related emergency calls among males appeared in the third trimester (summer). Conversely, the highest level for females was recorded in the second trimester (spring). These findings align with previous studies that have also identified seasonal disparities in suicide rates between male and females: research has shown that for death by suicide men tend to exhibit a peak in spring, whereas women exhibit two peaks in spring and autumn (Woo et al., 2012). Regarding attempted suicide, evidence suggests that a seasonal peak is predominantly observed among women, whereas no significant seasonal pattern emerges for men (Mergl et al., 2010). However, in relation to suicide-related emergency calls, the available evidence is limited. Currently, there is a lack of studies specifically investigating the seasonality of suicide-related emergency calls based on gender. Previous research has primarily focused on examining the overall seasonality of this outcome (Marco et al., 2018). Our findings suggest that the timing of suicide-related emergency calls varies between males and females, and these differences can likely be attributed to a combination of seasonal factors, social expectations, and gender-specific stressors. For males, the peak in suicide-related emergency calls during the summer months may be connected to the social expectations linked to this season (i.e., vacations, outdoor activities, and social gatherings), which may exacerbate feelings of isolation or depression, leading to an increased need for assistance during this period. In contrast, females exhibited the highest level of suicide-related emergency calls during the second trimester, corresponding to the spring months. This period may coincide with specific life stressors or events that can disproportionately affect females, such as challenges related to family dynamics or work circumstances. Further research and analysis are needed to uncover the specific reasons behind these patterns and to develop targeted interventions to support individuals during these critical periods. Our results highlight the importance of conducting gender-specific analyses when investigating the contextual factors associated with suicide. By considering the specific experiences of both males and females in crisis, our study provides more accurate insights into the reality of suicide, in contrast to many studies that generalize findings across the population (Congdon, 2011; Helbich et al., 2017; Marco et al., 2018). The spatio-temporal approach also provides information on the areas with above-average risk levels, as well as assessing the areas with temporal changes in the spatial patterns. Our findings showed distinct spatial patterns for suicide-related emergency calls, with significantly higher levels of calls from specific areas. The levels of calls increased notably across many areas over the period 2017-2022. Despite the overall upward trend, high levels of calls remained consistent in specific census block groups, including those located in the city center, the eastern area, and the southern area. These high-risk areas have distinct characteristics. The city center is known for being the old town and home to landmarks such as the city hall and the cathedral, attracting a higher level of tourism. This area is also characterized by an aging population. In contrast, the eastern area consists of maritime features and urban beaches, but also includes one of the city’s most deprived neighborhoods. The southern areas of the city have low population density and a significant amount of non-urbanized land, and some of these areas are considered socio-economically vulnerable. Conversely, the north-western area consistently exhibited lower levels of calls over the study period. This area comprises working-class neighborhoods with a medium socioeconomic status and a stable population. In terms of gender-specific differences, the disparities were more pronounced in the initial year (2017), while the map for 2022 showed greater similarity. To further investigate these patterns, future research should conduct targeted studies in specific local areas. This study has valuable strengths. First, previous studies have predominantly examined mortality data and suicide-related health records to understand the spatial distribution of suicide events (Congdon, 2011; Helbich et al., 2017; Qian et al., 2023), and only a few studies have used suicide-related emergency calls (Lersch, 2020a; Marco et al., 2018, 2017). This study addresses a significant gap in the research field by providing novel insights into an indicator of suicide that remains underexplored. Second, we used a Bayesian autoregressive approach to model both spatial and temporal effects. Bayesian methodology has been widely employed as the predominant spatial technique in recent decades, demonstrating its capacity to generate reliable and consistent estimates, even in areas with small population sizes (Ponicki et al., 2018). Using these advanced spatial analytics enhances the probability of obtaining stable estimates of the impact socio-economic factors have (Qian et al., 2023). Furthermore, the autoregressive approach has been increasingly used to assess different social outcomes (Gracia et al., 2017; Gracia et al., 2021; Marco et al., 2018). This methodology also has the advantage that it can be used to design maps identifying areas characterized by persistently higher levels of suicide-related emergency calls over time. This allows for localized analyses of these specific areas, including an exploration of the community factors contributing to these higher levels of suicide-related emergency calls. Furthermore, these maps provide the opportunity to examine areas that have experienced significant increases or decreases in the levels of suicide-related emergency calls, which can be used as a tool for assessing the effectiveness of local prevention strategies (Gracia et al., 2017). This study also has some limitations. Firstly, the analysis is restricted to a single city, and therefore the findings may not be directly generalizable to other locations. However, our methodology has the potential for replication in cities both within Europe and beyond, allowing for broader applicability and comparative analyses across different geographical contexts. The same 112 telephone number is used for emergency calls in European countries, meaning that similar and comparable data can be gathered, thus facilitating further analyses replicating the methodology presented in this paper. Secondly, our dataset comprises emergency calls, which do not include information on mortality or hospitalizations. In emergency calls, some suicidal events may not be classified due to a lack of information, such as a deceased person whose circumstances are unknown. However, the volume of data is sufficient to provide statistical power even if some data is missing, and any possible missing data is likely to be randomly distributed geographically. This distinction should be taken into consideration when comparing our findings with previous studies based on different measures, as they may reflect distinct underlying processes. Previous research has shown that help-seeking behaviors, including crisis calls, are not associated with suicide deaths at the individual level (Kandula, Higgins, et al., 2023). However, there is currently no research available on the correlation between suicide-related calls and suicide deaths from a spatial perspective. Future research could explore the spatial concurrence of suicide mortality data alongside suicide-related emergency calls. Thirdly, it is worth noting that this study spanned a relatively short period of six years. Future research would benefit from analyzing additional time periods, such as months, and extending the study duration to incorporate a longer timeframe, thus enabling a more detailed spatio-temporal analysis of suicide calls within neighborhoods over time. The findings of this study have significant practical implications. This methodology can be useful to closely monitor the specific locations where the levels of suicide-related emergency calls increased to gain a deeper understanding of the factors contributing to such fluctuations. Furthermore, these results underscore the crucial role of the neighborhood as a focal point for the convergence of various social determinants and environmental factors that contribute to social issues such as suicide (Sampson et al., 2002). It goes beyond individual characteristics; each neighborhood also has its distinctive socio-economic, cultural, and structural attributes that significantly impact these issues (Sampson et al., 2002). This emphasizes the need for approaches that focus on the community and the broader social context to design more effective and long-lasting interventions (Gracia et al., 2018). Future research could usefully examine the overlapping spatial patterns of different social problems within the city, which are intricately linked to neighborhood-level characteristics. Using advanced multivariate analysis techniques can help to understand and address the shared community-level explanatory factors affecting community well-being (Gracia et al., 2018; Marco et al., 2021). This comprehensive approach is essential for developing targeted interventions and policies that address the multifaceted challenges faced by communities. In conclusion, this study is the first approach to modeling 112 suicide-related emergency calls in a European city and offers results that may be pivotal in the design of prevention and intervention strategies within the framework of local policies. Our results pave the way for future work that incorporates more evidence on the spatio-temporal distribution of suicide-related emergency calls. Conflict of Interest The authors of this article declare no conflict of interest. Acknowledgements We wish to thank the 112 Valencian Community Emergency Service (Valencia Agency of Security and Response to Emergencies) for providing the dataset. Cite this article as: Marco, M., López-Quílez, A., Sánchez-Sáez, F., Escobar-Hernández, P., Montagud-Andrés, M., Lila, M., & Gracia, E. (2024). The spatio-temporal distribution of suiciderelated emergency calls in a european city: Age and gender patterns, and neighborhood influences. Psychosocial Intervention, 33(2), 103-115. https://doi.org/10.5093/pi2024a8 Funding: This study was funded by the Social Observatory La Caixa Foundation (LCF/PR/SR21/52560010). |
Cite this article as: Marco, M., López-Quílez, A., Sánchez-Sáez, F., Escobar-Hernández, P., Montagud-Andrés, M., Lila, M., & Gracia, E. (2024). The Spatio-Temporal Distribution of Suicide-related Emergency Calls in a European City: Age and Gender Patterns, and Neighborhood Influences. Psychosocial Intervention, 33(2), 103 - 115. https://doi.org/10.5093/pi2024a8
Correspondence: miriam.marco2@uv.es (M. Marco).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Imprimir
Imprimir Enviar
Enviar






