


Trauma, Reparation, and Quality of Life in Victims of Armed Conflict after Peace Agreements
[El trauma, la reparaci├│n y la calidad de vida de las las v├şctimas de conflicto armado tras los acuerdos de paz]
Marlen R. Simancas-Fernández1, José C. Celedón-Rivero1, Wilson M. Salas-Picón1, Diana E. Salgado-Ruiz1, María C. Echeverry-Londoño1, John H. Vásquez-Campos1, Marta Guarch-Rubio2 y Antonio L. Manzanero3
1Universidad Cooperativa de Colombia, Colombia; 2University of Limerick, Ireland; 3Universidad Complutense de Madrid, Spain
https://doi.org/10.5093/apj2021a21
Recibido a 30 de Enero de 2020, Aceptado a 22 de Abril de 2021
Resumen
The present study evaluates the quality of life of 1,139 surviving victims of the Colombian armed conflict benefited from some actions of reparation, through a brief sociodemographic and victimological survey and the WHO quality of life (WHOQOL-BREF) questionnaire, which takes into account perceived physical and mental health, social relations, and environmental factors. The results show that the quality of life of the victims of the armed conflict, once peace agreements had been reached, remained low or medium-low. The number of victimizing events suffered and the time elapsed have little effect on the quality of life, with type of trauma being more relevant. Land-related experiences, such as expropriation, had fundamentally an influence on environmental factors. Kidnappings, sexual assaults, and events where minors were involved affected mental health. Victims of sexual assault were those whose quality of life was most affected and torture victims were those with a lower index of global quality of life. Simple passing of time did not mean quality of life increase with specific interventions being needed to repair damage. To repair the damage caused, special attention should be paid to the sociodemographic characteristics of each victim, the type of aggression suffered, and their needs in the areas of physical and mental health, and economic resources.
Abstract
El presente estudio evalúa la calidad de vida de 1,139 víctimas supervivientes del conflicto armado colombiano beneficiadas con algunas acciones de reparación, mediante una breve encuesta sociodemográfica y victimológica y el cuestionario de calidad de vida de la OMS (WHOQOL-BREF), que toma en cuenta factores de la percepción de salud física y mental, relaciones sociales y ambientales. Los resultados muestran que la calidad de vida de las víctimas del conflicto armado, una vez alcanzados los acuerdos de paz, se mantuvo baja o media-baja. El número de hechos victimizantes sufridos y el tiempo transcurrido tienen poco efecto en la calidad de vida, siendo más relevante el tipo de trauma. Los hechos relacionados con la tierra, tales como la expropiación, tuvieron un efecto fundamentalmente en los factores ambientales. Los secuestros, agresiones sexuales y hechos en los que participaron menores afectaron a la salud mental. Las víctimas de agresión sexual fueron aquellas cuya calidad de vida se vio más afectada y las víctimas de tortura fueron aquellas con un índice más bajo de calidad de vida global. El mero paso del tiempo no implicó una mejora en la calidad de vida, siendo necesarias intervenciones específicas para reparar el daño causado. Se debe prestar especial atención a las características sociodemográficas de cada víctima, el tipo de agresión sufrida y sus necesidades en las áreas de salud física y mental y recursos económicos.
Palabras clave
Trauma, Quality of life, Colombia, Reparation, Peace agreementKeywords
Trauma, Calidad de vida, Colombia, Reparaci├│n, Acuerdo de pazPara citar este art├şculo: Simancas-Fernández, M. R., Celedón-Rivero, J. C., Salas-Picón, W. M., Salgado-Ruiz, D. E., Echeverry-Londoño, M. C., Vásquez-Campos, J. H., Guarch-Rubio, M. y Manzanero, A. L. (2022). Trauma, Reparation, & Quality of Life in Victims of Armed Conflict after Peace Agreements. Anuario de Psicolog├şa Jur├şdica, 32(1), 79 - 86. https://doi.org/10.5093/apj2021a21
antonio.manzanero@psi.ucm.es Correspondence: antonio.manzanero@psi.ucm.es (A. L. Manzanero).Quality of life has a global effect on society as a whole. The pragmatic study of quality of life allows to improve the conditions of mental health in a society, especially in those that are in a process of social, political, technological, and economic transformation (Cáliz et al., 2013). As Castañeda (2017) indicated, quality of life determines the level of mental health of a group through the evaluation of its impact on public policies and the assessment, diagnosis, and individual intervention promoting specific treatments and identifying their level of effectiveness. The Colombian armed conflict is the result of the military political confrontation that has shaken Colombia for more than 50 years (Grupo Memoria Histórica, 2013). Throughout the second half of the twentieth century, the cyclical crises of the Colombian state led to the emergence of guerrillas, the violent counter-response of paramilitary groups and the public force, and the emergence of drug trafficking, turning the Colombian civilian population into direct victims of the armed conflict. Actions of violence and cruelty have left victims throughout the national territory, mainly in rural areas, promoting forced internal displacement. Colombia is the first country in the world with internal victims of forced displacement (7.8 million) and the second, after Syria, with the largest displaced population (8 million) (UNHCR, 2019). In 1998, the United Nations defined the ‘internally displaced’ as “the person or group of people who have been forced to flee and leave their homes or habitual places of residence, in particular, to avoid the consequences of an armed conflict, of widespread violence, of human rights violations, as well as of human or natural disasters and have not crossed a recognized international border” (UNHCR, 1998). However, being a victim of the armed conflict in Colombia does not only imply having suffered forced displacement; in fact, individuals may have suffered damage and not suffered forced displacement. In Colombia, the rate of victims of the armed conflict is recorded in the Single Registry of Victims [Registro Único de Víctimas, RUV], where 9,113,500 are registered as victims of the conflict since 1985. Colombian Law 1448/2011 recognized forced displacements due to the armed conflict and established the obligation to repair the damage caused to the victims through actions of restitution, compensation, rehabilitation, satisfaction, and guarantees of non-repetition in their individual, collective, material, moral, and symbolic dimensions (Castrillón-Guerrero et al., 2018). In this way, the majority of these victims would be beneficiaries of care and reparation actions, with the exception of 1,645,613 people because they have died, are missing, or not properly identified (Red Nacional de Información, 2019). However, the Historical Memory Group (Grupo de Memoria Histórica, 2013) questions the reliability of this registry as does not collect victims before 1985, those killed in military actions and indirect victims, who would increase the official figure. This same group documented selective killings, massacres, death of civilians in military actions, terrorist attacks, attacks on populations and civilian assets. Furthermore, the victims of the Colombian conflict should also include cases of forced disappearances, kidnappings, torture, sexual violence, land mines, illegal recruitment, injuries, and forced displacement. Therefore, it is found that under situations of armed conflict it is difficult to specify the real number of victims and the forms of violence exerted towards them. In addition, functionality of violence has a subjective component that responds to its intentionality and the damage it infringes on the victim. Thus, similarly to the development of psychological trauma, there will be individual variations in coping and, consequently, in the perception of quality of life of Colombian victims. Quality of Life Quality of life is defined as “individuals’ perceptions of their position in life in the context of culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns” (WHO, 1996, p. 5). In general terms, quality of life is determined by subjective and objective aspects, as well as by the assessment of the interrelationship established between these aspects. The interest in the study of quality of life has generated a willingness to define and evaluate the concept scientifically (Ardila, 2003; Cardona & Agudelo, 2005; Urzúa & Caqueo-Urízar, 2012). Quality of life has been studied in different disciplines (social, economic, and health), and is linked to the dichotomous health-disease construct (Urzúa, 2010). Some studies have focused on quality of life and civilian victims in the context of wars, armed conflicts, or violence (Araya et al., 2011; Ghazinour et al., 2004; Giacaman et al., 2007; Hammoudeh et al., 2013; Morina et al., 2013), with the study of mental health being the most frequent study (Ayazi et al., 2014; Bentley et al., 2011; De Fouchier et al., 2012; Eisenman et al., 2003; Gómez-Varas et al., 2016; Guarch-Rubio & Manzanero, 2017; Manzanero et al., 2021; Mollica et al., 2014; Mollica et al., 1992; Sabin et al., 2003; Stanciu & Rogers, 2011; Vinson & Chang, 2012). In general, all these studies show a deterioration in the quality of life and serious effects on mental health in survivors of armed conflicts and wars. Steel et al.’s (2009) meta-analysis of 161 articles (181 surveys) reported rates of 30.6% and 30.8% for posttraumatic stress disorder and depression, respectively. Different factors influence the quality of life of victims of armed conflicts, among which sociodemographic, social, and psychological support stand out (Huijts et al., 2012; Wagner et al., 2012). In a study on the quality of life of residents of the Gaza Strip, Abu-Rmeileh et al. (2012) found that the main predictors were age, educational level, residing in rural settings, destruction of private property, or levels of stress and suffering. In Colombia, Simancas et al. (2019) evaluated the quality of life in victims of the armed conflict, identifying that the environmental domain was the most affected due to disadvantages related to physical, health, and social assistance resources. Campo-Arias et al. (2014) conducted a systematic review of 13 studies that assessed the mental health of victims of armed conflict, finding very wide ranges of prevalence of mental disorders between 1.5 and 32.9%. Abello-Llanos et al. (2009) evaluated the well-being of forcibly displaced people in Colombia due to the armed conflict, finding that the trauma suffered was related to perceived psychological, subjective, and social well-being. As in victims of other conflicts, different studies have also evaluated quality of life of demobilized people, showing the effect that personal networks have on quality of life (Amar et al., 2011; Madariaga & Molinares, 2016). Velasco and Londoño (2011) evaluated perceived quality of life in demobilized Colombian individuals and identified multiple psychosocial factors predictive of an improvement in quality of life, such as perceived health, optimism, educational level, type and time of demobilization, as well as years of permanence in the armed group, among others. The aim of the present study is to analyze the effect of type of victimizing traumatic experiences, perception of aid, and sociodemographic factors on the quality of life of victims of armed conflicts, once peace agreements have been reached and aid has been received. According to the results of previous studies, it can be hypothesized that quality of life is expected to be directly related to the amount and severity of the trauma suffered. Perception of aid should favor a better quality of life. Similarly, older victims, those in rural settings, and victims with family support are expected to have a better quality of life. Participants One thousand one hundred thirty-nine (1,139) survivor victims of the armed conflict in Colombia were selected from a non-probabilistic sample. The inclusion criteria established that participants had to be officially registered in the RUV and had to be recipients of some type of actions according to Colombian Law 1448/2011 about care, assistance, and full reparation to victims of the armed conflict. In total, 431 participants lived in the city of Santa Marta, 318 in Barrancabermeja, 209 in Montería, 100 in Medellín, and 81 in Cali. The group was composed of 29% of men (n = 332) and 71% of women (n = 805). Participants’ mean age was M = 42.51 (SD = 15.39, range = 16-85). Men’s mean age was M = 45.71 (SD = 16.87), and women’s was M = 41.19 (SD = 14.54); 362 participants (31.78%) had non-formal education, 378 participants (33.18%) had primary education, 302 participants (26.51%) had secondary education, and 94 participants (8.25%) had high and technological education. Procedure For data collection, support of directors of Regional Centers of Care, Assistance, and Integral Reparation for Victims of the cities of Santa Marta, Barrancabermeja, Montería, Medellín, and Cali was obtained. In these regional centers, victims of armed conflict receive care, humanitarian aid, and guidance in assistance and reparation services, among others. Individuals were asked for their collaboration when they attended these centers and the investigative nature of the study was explained. Participation was voluntary and after the assent and informed consent of participants, a sociodemographic data survey and the WHOQOL-BREF were applied. The evaluations were carried out over a period of six months, with a duration of 45 minutes per participant. Table 1 WHOQoL-BREF structure 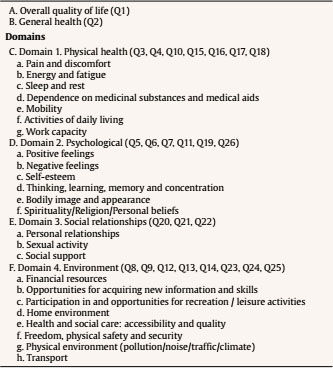 Instruments Sociodemographic and victimological survey. It included questions regarding age, gender, marital status, educational level, employment status, and socioeconomic status of participants, as well as their cohabitation group, place of residence, date, and last victimizing event and year in which they received the first aid typified by Law 1448/2011. Measurement of quality of life was carried out through the application of WHOQOL-BREF. The World Health Organization (WHOQOL Group, 1993) designed the WHOQOL-100 as a multicultural quality of life assessment tool, with the WHOQOL-BREF being its reduced version (WHO, 1996). As can be observed in Table 1, this questionnaire consists of 26 items. The first two items assess quality of life and health in general terms, and the remaining 24 items evaluate the four domains of quality of life: physical health (pain and discomfort, dependence on medication or treatment, energy and fatigue, daily activity, mobility, sleep and rest, and ability to work), psychological health (positive feelings, spirituality, religion and personal beliefs, thinking, learning, memory and concentration, personal image and appearance, self-esteem, and negative feelings), social relations (personal relationships, sexual activity, and social support), and environment (physical security and protection, physical environment, economic resources, opportunities for information/skills acquisition, home, health and social care, and transportation). The WHOQOL-BREF follows a Likert type response format with a scale from 1 to 5, asking about satisfaction of each item in the past two weeks, where 1 is very dissatisfied, 2 is a little dissatisfied, 3 is medium, 4 is quite satisfied, and 5 is very satisfied. Higher scores indicate a higher perceived quality of life, in a range of zero to 100. WHOQOL-BREF psychometric properties in the sample analyzed for the 26 items was Cronbach’s α = .865 and inter-item correlation was r = .201. Table 2 Mean scores (M), standard deviations (SD) and maximum and minimum values for each of the indices evaluated. 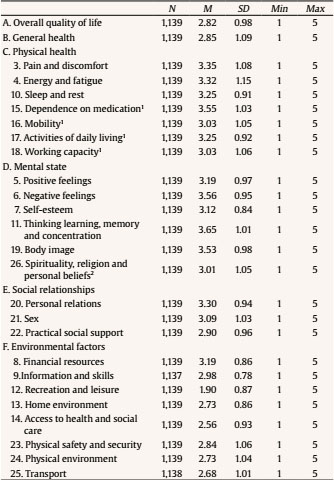 Note. 1Independence domain; 2Spirituality domain in 6-domain model. Data Analysis From data collected, statistical analyses (ANOVAs and correlations as appropriate) were performed in order to study the relationship between the different indices of quality of life and sociodemographic factors, and the support or help received. Answers provided by participants to the 26 questions raised were coded, and then corrected according to the instructions of the WHOQOL-BREF manual (WHO, 1996). Scores of questions 3, 4, and 26 were reversed so that a higher score indicated a better quality of life, similarly to the rest of the questions. According to this, results show that general quality of life and satisfaction with health of people affected by the conflict in Colombia over the last 40 years was between low (2) and medium (3) (see Tables 2 and 3). With respect to the domains, once the data was coded and transformed according to the WHOQOL-BREF manual, scores were distributed across a range of 0-100. Table 3 Mean Scores (M), Standard Deviations (SD), and Maximum and Minimum Values for each of the Evaluated Domains 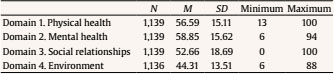 Sociodemographic Factors Quality of life, as can be observed in Table 4, was related to age, r(1139) = -.152, p < .001; marital status, F(1, 1135) = 3.150, p < .05, η2 = .008; level of completed studies, F (3, 1135) = 12.958, p < .001, η2 = .033; and income, F (1, 1131) = 22.079, p < .001, η2 = .019. The elderly, divorced, or widowed victims, with lower education and salaries below minimum wage showed a lower quality of life. Table 4 Mean scores (and standard deviation) according to the Sociodemographic Variables 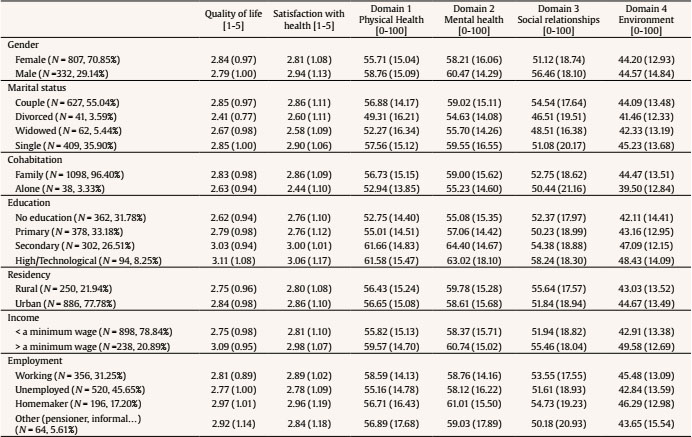 Health satisfaction was related to age, r(1139) = -.139, p < .001; type of coexistence, F(1, 1137) = 5.396, p < .05, η2 = .005; level of completed studies, F(3, 1135) = 4.484, p < .005, η2 = .012; and income, F(1, 1137) = 4.455, p < .05, η2 = .004. The older victims, those who lived alone, had lower education, and received salaries below minimum wage showed less satisfaction with their overall health. Physical health, with respect to the four domains evaluated, was related to age, r(1139) = -.246, p < .001; gender, F(1, 1134) = 9.621, p < .01, η2 = .008; marital status, F(3, 1132) = 5.564, p < .001, η2 = .015; educational level, F(3, 1132) = 25.454, p < .001, η2 = .063; income, F(1, 1134) = 11.696, p < .001, η2 = .010; and employment, F(3, 1132) = 3.659, p < .05, η2 = .010. Physical health was worse in older victims, males, divorced, or widows, with lower education, less income, and those who do not work. Mental health was related to age, r(1139) = -.174, p < .001; gender, F(1, 1134) = 4.947, p < .05, η2 = .004; education level, F(3, 1132) = 24.209, p < .001, η2 = .063; and income, F(1, 1134) = 4.335, p < .05, η2 = .004. Mental health was worse in older victims, women, with lower education and less income. Social relations quality was related to gender, F(1, 1134) = 19.414, p < .001, η2 = .017; marital status, F(3, 1132) = 5.625, p < .001, η2 = .015; place of residence, F(1, 1134) = 8.087, p < .01, η2 = .007; level of education, F(3, 1132) = 5.865, p < .001, η2 = .015; and income, F(1, 1134) = 6.684, p < .01, η2 = .006. Women, widowed or divorced, from urban settings, with lower education and less income showed a worse quality in their social relationships. Table 5 Mean scores (and standard deviation) according to the Type of Received Aids 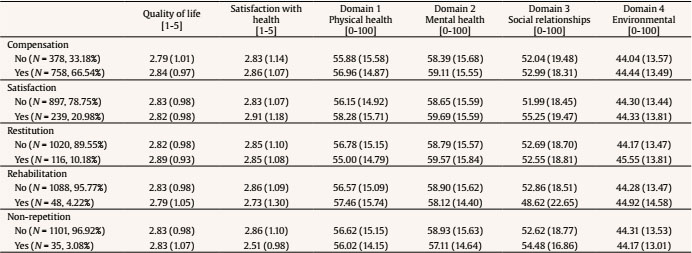 Table 6 Mean Scores (and Standard Deviation) according to the Type of Experienced Traumatic Event 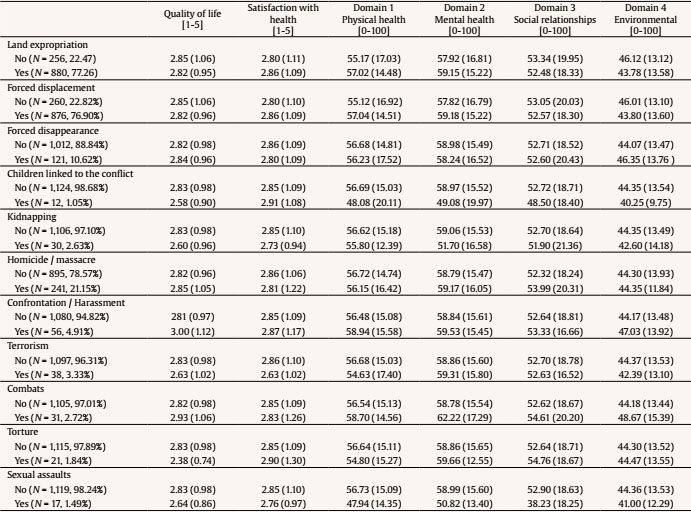 Environmental factors were related to age, r(1139) = -.086, p < .01; cohabitation, F (1, 1134) = 5.001, p < .05, η2 = .004; educational level, F(3, 1132) = 11.616, p < .001, η2 = .030; income, F(1, 1134) = 47.708, p < .001, η2 = .040; and employment, F(3, 1132) = 4.429, p < .01, η2 = .012. Quality of environmental factors was worse in older victims, those who live alone, with lower education, lower income and were unemployed or their income depended on sporadic pensions or informal jobs. Effects of the Aid Received In relation to the aids received (see Table 5), administrative “compensation” implies financial compensation for the victimizing acts suffered; “satisfaction” actions intend to repair pain through dissemination of historical memory, dignification of victims, and reconstruction of truth; the “restitution” measure is understood as actions taken to restore the situation prior to violations contemplated by Law 1448/2011, implying the legal and material restitution of the land of dispossessed and displaced persons; “rehabilitation” is the restoration of physical and psychosocial conditions of victims through plans, strategies, programs, and actions of a legal, psychological, medical, and social nature; finally, guarantees of “non-repetition” involve actions aimed at society with the aim of not repeating violation of victims’ rights, overcoming and eliminating the causes of massive violation of these rights. Regarding the aids received, it was observed that the average aid was M = 1.22 (SD = 0.49, range = 1-5). Many victims of the conflict had received some financial compensation (n = 758). No effects of number of aids received or time since they had been received on quality of life were found. There were no effects of type of aid received on quality of life. Overall quality of life, satisfaction with general health, physical and mental health, and environmental factors were not affected by this variable. Compensation, restitution, medical and psychological rehabilitation, and guarantees of non-repetition had no effects on none of these factors. Only satisfaction increased social relationships, F(1, 1137) = 5.771, p < .05, η2 = .005. Effects of Traumatic Events Average number of traumatic events experienced was M = 2.05 (SD = 0.86, range = 1-10). Average time since the last event was M = 11.15 years (SD = 7.46, range = 0-40). The analysis of the relationship between trauma and quality of life indicated that the number of traumas suffered was no related to quality of life, while time elapsed since the last victimizing event was only related to social relations, r(1139) = .061, p < .05, and environmental factors, r(1139) = .076, p < .01. Table 7 Percentage (and N) of male and female according to type of Experienced Traumatic Event. 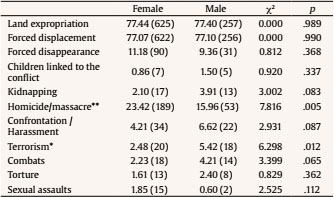 *p < .05, **p < .01. As can be observed in Table 6, the majority of victims suffered expropriation of land (880), forced displacement (876), witnessed homicides or massacres (241), and suffered forced disappearances (121). Less frequently the victims suffered confrontations or harassment (56), terrorism (38), battles (31), kidnapping (30), torture (21), sexual assault (17), linking children with conflict (12), effects of land mines (2), and unexploded ammunition (5). The “overall quality of life” was only affected by having been the victim of torture, F(1, 1137) = 4.434, p < .05, η2 = .004. “Mental health” is the domain most related to traumatic events, being worse in victims of kidnapping, F(1, 1137) = 6.553, p < .01, η2 = .006; sexual assaults, F(1, 1137) = 4.614, p < .05, η2 = .004; and the connection of children with conflict, F(1, 1137) = 4.796, p < .05, η2 = .004. “Satisfaction with health” was not affected by any of the traumatic events suffered. “Physical health”, F(1, 1137) = 5.697, p < .05, η2 = .005, and “social relationships”, F(1, 1137) = 10.373, p < .001, η2 = .009, were related to having suffered sexual assaults. “Environmental factors” were related to events that imply the relocation of the place of residence due to the expropriation of land, F(1, 1134) = 5.976, p < .05, η2 = .005, and forced displacement, F(1, 1134) = 5.404, p < .05, η2 = .005. Suffering from sexual aggressions was the trauma that most affected the dimensions of quality of life, causing worse physical and mental health and deteriorating social relationships. Some facts (forced disappearance, homicides and massacres, harassment and confrontations, terrorism and battles) were not linked to quality of life. As can be seen in Table 7, no differences were found in type of experienced traumatic events according to gender, except for terrorism and witnessed homicides or massacres. The results of the present study indicate that the quality of life of victims of armed conflicts during the past decades, once peace agreements had been reached and aid had been received, was low or medium low, having obtained lower scores than those found in other studies of quality of life in the general population of Colombia (Cardona-Arias et al., 2015). These data could indicate that their quality of life is affected by their condition as victims. As can be observed, values obtained in the first three quality of life domains evaluated were located in 2nd quartile and the last domain, on environmental factors in the 3rd quartile. In comparison with other studies (Cardona-Arias et al., 2015) where the general adult population in Colombia was evaluated, values found in the present study were clearly lower for all domains. Cardona-Arias et al. (2015) obtained averages of 68 for physical health, 70 for mental health, 60 for social relations, and 59 for environmental factors. The fact that the passage of time did not imply an improvement in their quality of life could indicate that it is not enough to let time pass but that specific interventions are necessary to repair the possible damage caused. In this vein, emotional and behavioral dispositions such as reconciliation and forgiveness enhance the recuperation, even though they are thought to be materialized in the mentioned Colombian context of armed conflict (Cortés et al., 2016). Factors that seem to play a greater role in victims’ quality of life are factors related to sociodemographic variables (age, gender, family support, education, work, and income level). Apparently, contrary to expectations, the aid received seemed to have little effect on quality of life indices. However, the objective of this study was not to assess this aspect, as all the victims evaluated received aid; therefore it is not possible to reach conclusions on the usefulness of the aid, only on the effect that type and quantity of aids may have. The direction of the relationship between aid and quality of life could go either way. That is, quality of life might impact whether aid is received (with those with lower quality of life more likely to receive aid) and reception of aid could impact quality of life (with those who receive aid experiencing subsequently improvements in quality of life). As such, it is difficult to interpret findings when both are assessed retrospectively. In this way, we can only affirm that among these victims who receive aid, there are few differences in quality of life depending on these factors. However, data show that they were adequately granted, as the most vulnerable victims (worse health and less social support) were the ones that received the most attention. It would be of interest to compare data in this study with those of victims who have not received any help. This comparison based on previous studies is difficult, due to the variety of instruments used to assess quality of life, thus warranting a new study with a comparable population that does not receive aid. Contrary to what was expected from previous studies (see, for example, Abello-Llanos et al., 2009; Guarch-Rubio et al., 2020), in the present study, the number of victimizing events suffered, and time elapsed since such events had little effect, with the type of trauma being much more relevant. Victims of sexual assault showed a more affected quality of life. The events related to the land were fundamentally influenced by environmental factors, whereas kidnappings, sexual assaults, and the events where minors were involved affected mental health. Victims of torture showed the lowest global quality of life index. Conclusions The results of these studies suggest that quality of life could induce an improvement in the mental health of victims, regarding physical and psychological health, social relations, and environment. However, it is still necessary to move forward in the identification of mechanisms by which such influence would be generated and of factors that can potentiate it, remembering that maintaining such long-term benefits will depend largely on life changes and avoiding the victimological condition. In this way, it is recommended that public policies for the care of victims of armed conflict take into account their sociodemographic characteristics and the specific type of violence suffered. In this context, the reflections of different authors in the context of the Colombian conflict (Melo-Hernández et al., 2006; Rodado & Grijalva, 2001) regarding cultural issues and quality of life are interesting. Some implications that these results may have for the practice of professionals working with these populations victim of armed conflict are, on the one hand, the attention to how these people perceive their own quality of life and how they feel about such a perception as a way to establish comprehensive reparation actions, since dissatisfaction with some domain of quality of life could lead to altered mental health, aggression, and generalized violence, which could become a complication against the actions contemplated to their reparation. Programs that cover the whole society among which are the actions of satisfaction that seek to repair the damage caused to the victims through the dissemination of the historical memory, dignification of the victims and reconstruction of the truth, as well as guarantees of non-repetition involving actions directed at society with the objective of not repeating the violation of the rights of the victims, overcoming and eliminating the causes of the massive violation of rights, are of great importance, although they are not enough. In addition, specific and individualized care programs for victims that include mental and physical health and financial support are necessary. We hope that the results of the present study will contribute to the design of future care programs for victims of armed conflicts and wars based on their characteristics and specific needs. Conflict of Interest The authors of this article declare no conflict of interest. Para citar este artículo: Simancas-Fernández, M. R., Celedón-Rivero, J. C., Salas-Picón, W. M., Salgado-Ruiz, D. E., Echeverry-Londoño, M. C., Vásquez-Campos, J. H., Guarch-Rubio, M., & Manzanero, A. L. (2021). Trauma, reparation, and quality of life in victims of armed conflict after peace agreements. Anuario de Psicología Jurídica, 32, 79-86. https://doi.org/10.5093/apj2021a21 Funding: This work is part of a research project on psychological wellbeing, quality of life and social support in the victims of the armed conflict in Colombia, developed by Neurocognición Research Group (ref. COL0052341), in the framework of the project financed by CONADI- Universidad Cooperativa de Colombia (Cod.1800); and part of a research project on assessment of memories and psychological disorders associated to trauma in refugees and victims of war, developed by UCM Research Group on Eyewitness Testimony (ref. 971672), in the framework of the project financed by Santander-Universidad Complutense de Madrid (PR75/18-21661). References |
Para citar este art├şculo: Simancas-Fernández, M. R., Celedón-Rivero, J. C., Salas-Picón, W. M., Salgado-Ruiz, D. E., Echeverry-Londoño, M. C., Vásquez-Campos, J. H., Guarch-Rubio, M. y Manzanero, A. L. (2022). Trauma, Reparation, & Quality of Life in Victims of Armed Conflict after Peace Agreements. Anuario de Psicolog├şa Jur├şdica, 32(1), 79 - 86. https://doi.org/10.5093/apj2021a21
antonio.manzanero@psi.ucm.es Correspondence: antonio.manzanero@psi.ucm.es (A. L. Manzanero).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






Herramientas:
 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Imprimir
Imprimir Enviar
EnviarALERTA POR E-MAIL
La Revista de Anuario de Psicología Jurídica está distribuida bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObra Derivada 4.0 Internacional.com








