


ACT-based Stress Management Training Aimed at Improving WorkersŌĆÖ Mental Health in an Intensive Care Unit: A Mixed Methods Study1
[Entrenamiento en el manejo del estr├®s laboral basado en TAC dirigido a la mejora de la salud mental de trabajadores de una UCI m├®dica: un estudio con m├®todo mixto]
Luis M. Blanco-Donoso1, Carlos Garcia-Rubio1, Juan A. Gallardo2, Gladis Pereira1, María L. Rodríguez de la Pinta3, Juan J. Rubio3, and Eva Garrosa1
1Autonomous University of Madrid, Spain; 2National Autonomous University of Mexico, Mexico; 3Puerta de Hierro Hospital, Madrid, Spain
https://doi.org/10.5093/clysa2021a12
Received 22 November 2020, Accepted 15 March 2021
Abstract
This study aimed to explore whether an acceptance and commitment (ACT) approach to stress management training improved the levels of depression, anxiety, and stress among a group of twenty-two health professionals from an intensive care unit. Questionnaires were administered before and after training, and follow-up was carried out one month after training, including semi-structured interviews with nine participants. The results reflected that the quasi-experimental group reduced their depression and stress levels significantly and showed improvements in stress in the follow-up. A qualitative thematic analysis of interviews showed that nurses were seeking a tool that would help them to cope more effectively with stressful situations and increase their knowledge of stress management. The themes in the professionals’ comments claimed specific improvements in their health, well-being, relationships, and psychological processes. In conclusion, ACT-based trainings offer a possible framework for mental health promotion in health care organizations.
Resumen
Este estudio tiene como objetivo explorar si un enfoque de aceptación y compromiso (TAC) para el entrenamiento en el manejo del estrés mejora los niveles de depresión, ansiedad y estrés en un grupo de 22 profesionales de la salud de una unidad de cuidados intensivos. Los cuestionarios se administraron antes y después del entrenamiento y el seguimiento se llevó a cabo un mes después del mismo, incluyendo entrevistas semiestructuradas con 9 de los participantes. Los resultados reflejaron que el grupo cuasiexperimental redujo sus niveles de depresión y estrés significativamente y mejoró el estrés durante el seguimiento. Un análisis temático cualitativo de las entrevistas mostró que los profesionales de enfermería buscaban una herramienta que les ayudara a hacer frente más eficazmente a las situaciones de estrés aumentando el conocimiento en su manejo. Los comentarios de los profesionales reflejaban mejoras específicas en su salud, bienestar, relaciones y procesos psicológicos. En conclusión, los entrenamientos basados en TAC ofrecen un posible marco para mejorar la salud mental en las organizaciones de atención médica.
Palabras clave
Entrenamientos en terapias de aceptaci├│n y compromiso, Depresi├│n, Estr├®s, Dise├▒o de m├®todos mixtos, Trabajadores de la saludKeywords
Acceptance and commitment training, Depression, Stress, Mixed methods design, Health-care workersCite this article as: Blanco-Donoso, L. M., Garcia-Rubio, C., Gallardo, J. A., Pereira, G., Pinta, M. L. R. D. L., Rubio, J. J., and Garrosa, E. (2021). ACT-based Stress Management Training Aimed at Improving WorkersŌĆÖ Mental Health in an Intensive Care Unit: A Mixed Methods Study1. Cl├Łnica y Salud, 32(3), 111 - 117. https://doi.org/10.5093/clysa2021a12
luismanuel.blanco@uam.es. Correspondence: luismanuel.blanco@uam.es. (L. M. Blanco-Donoso).Intensive care units (ICUs) are stressful environments in which pain and human suffering are often experienced alongside great pressure and temporary urgency to perform work (van Mol et al., 2015). In these cases, health professionals are subject to extreme stress and work overload, and are often exposed during their work to occupational risk factors that have the potential to affect their mental health and psychological well-being over time (Gómez-Martínez et al., 2015). In fact, the literature has shown that, within ICUs, professionals may experience psychological problems such as burnout, stress, anxiety, and depression (Gómez-Martínez et al., 2015; van Mol et al., 2015). Nevertheless, many health professionals do not benefit from interventions introduced by psychology professionals in their organizations to improve their levels of mental health and psychological well-being, which could have serious consequences for workers, patients, and organizations (Bond et al., 2010; Waters et al., 2018). Psychosocial interventions to reduce stress and increase workers’ well-being can take two main forms (Van der Klink et al., 2001): interventions which redesign the job or task to reduce the workload and pressure faced by workers, or providing them with greater autonomy and support at work, and interventions which provide workers with the necessary skills and resources to cope with stress. These two complementary types of interventions should not be mutually exclusive. Sources of stress in certain occupations are, to some extent, inherent and unavoidable (e.g., contact with pain and death within the health care professions); hence, training professionals to develop emotional coping strategies can be important in such a professional context (Bond et al., 2010; García et al., 2018). Regarding the second type of intervention, stress management training (SMT) is the most well-known approach (Van der Klink et al., 2001); it is based mainly on cognitive-behavioral techniques and its effectiveness has been widely demonstrated by various meta-analyses (for example Tetrick & Winslow, 2015). SMT provides workers with tools for identifying dysfunctional thoughts (and replacing them with more adaptive ones), improving their social and communication skills, engaging in problem solving and developing techniques that help them to relax when facing stress. Within this context, one type of SMT that is attracting increasing interest among researchers and clinicians is training based on acceptance and commitment therapy (ACT; Flaxman et al., 2013). ACT is part of a larger group of cognitive-behavioral therapies, called third generation or contextual therapies (Hayes et al., 2012), and is based on a functional contextual perspective derived from behavioral principles and extended through relational framework theory. ACT argues that people’s emotional and psychological distress can be explained not so much by the negative content or frequency of their internal psychological experiences, but by how they relate to difficult experiences when they arise (e.g., unpleasant thoughts, emotions, sensations, or memories; Bond et al., 2010). Mental health problems, such as depression or anxiety, may be caused by psychological processes such as attentional rigidity (i.e., not being able to direct one’s attention to what is happening in the present since attention is focused on remembering past events or anticipating future events); avoidance of negative psychological experiences (i.e., devoting energy to controlling or eliminating negative emotions, feelings, or thoughts, due to avoidance); or lack of action by the person based on his or her personal values (i.e., behavior being governed and regulated by adverse mental content, rather than by contingencies of the present situation and an individual’s personal values and goals; Hayes et al., 2012). The ultimate aim of ACT training is therefore to teach people to pay attention to, and engage with, experiences in the present moment, relate to their negative internal events with greater acceptance, and commit to actions that are directed toward their personal values and goals. ACT aims to generate greater psychological flexibility in individuals (Hayes et al., 2012; Waters et al., 2018). Psychological flexibility can be understood as the ability to focus on the situation one is experiencing in the present and, depending on the opportunities offered to the person by that situation with reference to his or her personal values and goals, to take action toward them, even in the presence of negative internal events (Lloyd et al., 2013). Interest in this therapy has been growing over the past two decades and it is already considered to be “possibly efficacious” for the management of depression, anxiety, and stress at work (Öst, 2014). In fact, in the field of occupational psychology, different empirical studies have shown the ability of these ACT interventions to improve workers’ mental health (Macias et al., 2019), their resistance to burnout and their psychological well-being (Frögeli et al., 2016), and/or their personal psychological flexibility and mindfulness (Frögeli et al., 2016; Waters et al., 2018). In occupational fields such as health care jobs, these interventions can help workers to cope with others’ human suffering and prevent the development of certain psychosocial risks, such as burnout or secondary traumatic stress and its consequences (Frögeli et al., 2016; Ortega et al., 2008). ACT training sessions for managing job stress are commonly short (workshop format), group-based, and skill-building to fit workers’ organizational and task requirements (Bond et al., 2010; Waters et al., 2018). In fact, the best-known format involves three face-to-face sessions of approximately three hours (Flaxman et al., 2013). The brief nature of this type of intervention is particularly valuable in health care professions, and even more so in services such as intensive care, since these require professionals to adapt to dynamic working conditions (e.g., high staff turnover, sudden shift changes, and long working days; García et al., 2018; Waters et al., 2018). This study aims to contribute to the literature exploring the effect of ACT-based training on mental health in an organizational environment, and specifically within work contexts characterized by high work demands, such as a ICUs. Despite the fact that international studies have shown the value of such a training, few studies in Spain have explored its effects (Blanco-Donoso et al., 2017; Ortega et al., 2008); therefore, this study proposed to explore the impact of ACT training on ICU workers. Specifically, the study hypothesized that short ACT training sessions would lead to improved levels of depression, anxiety, and perceived stress among workers in an ICU in a Spanish tertiary hospital. In addition, it hypothesized that this improvement would be attributable to an increase in workers’ levels of psychological flexibility—one of the core abilities emerging from ACT, which has been shown to mediate changes in this type of intervention (Waters et al., 2018). Design This research had a mixed methods design, using both quantitative and qualitative methods. The quantitative component involved a quasi-experimental pre- and post-intervention study with two groups (quasi-experimental and waiting-list control group). The participants in the waiting-list control group received the intervention immediately after the quasi-experimental group had completed it. Therefore, the quasi-experimental group was evaluated on three occasions: before (baseline), after, and one month after the intervention. However, the waiting-list control group was assessed on four occasions: the first, concurrent with the first assessment (baseline) of the quasi-experimental group; the second, at the time of the second assessment of the quasi-experimental group (to ensure the control condition); the third, when this group also completed the intervention; and the fourth, one month later, coinciding with the follow-up measurement of the quasi-experimental group. Participants were not randomly assigned to groups due to service restrictions. Specifically, the groups were formed according to professionals’ work shifts, so that the quasi-experimental group was made up of workers who had morning shifts, while the waiting-list control group was made up of workers on afternoon shifts. Sample Twenty-two medical and nursing professionals participated in the training, most of whom were female nurses from the ICU of a large public hospital (tertiary level) in Madrid Region, Spain. The sample was therefore a non-probabilistic, convenience sample. The only inclusion criterion was that practitioners gave their consent to voluntarily participate in the study and be evaluated at various points in time. There were no exclusion criteria. Table 1 shows socio-professional characteristics of the participating sample. As can be seen in Table 1, there were no significant differences in any socio-professional variables between members of one group and the other at the beginning of training. Initially, the quasi-experimental group consisted of 14 participants and 13 completed the pre- and post-measurement. The waiting-list control group was made up of 8 workers, all completing the pre and post measure while on the waiting list status. However, when the waiting-list control group conducted and completed the workshop, only 3 completed the post measure. A total of 16 workers participated in the follow-up. Finally, 9 nurses agreed to attend the semi-structured interviews at this phase of the study. Table 1 Socio-professional Characteristics of Participants 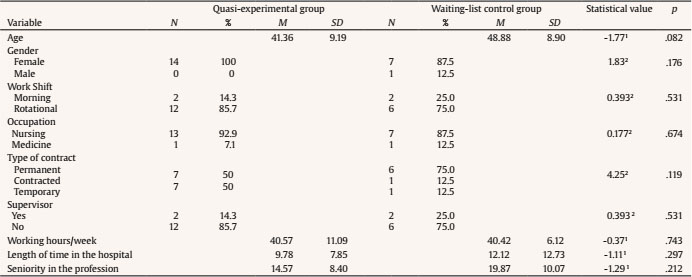 Note. 1Mann-Whitney U; 2chi-square test. N = 22. *p < .05. Procedure First, the approval of the University’s Ethics Committee was obtained [masked for review]. Thereafter, we contacted the hospital’s Occupational Risk Prevention Service, which liaised with the Intensive Care Medicine Service to offer training to its workers. Unit supervisors informed their teams about the study, which they advertised as training to help them manage stress in the work environment. A week before the intervention, enrolled participants from both groups were invited to a joint briefing about the study and the intervention. This session was also used for participants to complete baseline measurements. With regard to post-intervention measurement (at the end of the workshop) and follow-up (after one month), evaluation was carried out electronically, with participants accessing an online questionnaire by means of a personal code. When the intervention was completed, psychologists who conducted it invited participants to attend face-to-face interviews (one month after the intervention), during which they would be asked questions about their experiences of the implemented program. Intervention The training used a group workshop format, with three sessions of three hours duration each during a single working week (on alternate days), but outside working hours. Intervention and interviews were carried out by the first two authors of this paper, who are health psychologists trained in ACT and have experience applying such interventions in work environments. Training sessions followed the format of standard ACT work manuals (e.g., Flaxman et al., 2013). The first session identified workers’ stress responses, along with their main causes, and identified emotional barriers that prevented workers from achieving full and satisfying lives. Ineffectiveness and long-term consequences of experiential avoidance were also analyzed and psychological acceptance was offered as an alternative strategy. During this session therapists investigated, dialogued with, and confronted participants on these issues and used metaphors, paradoxes, and experiential exercises according to standard ACT practices. In addition, in this session mindfulness was introduced as a way of achieving an attitude of acceptance toward negative internal experiences in the present, and attention in breathing and body scanning were practiced. During the second session, therapists worked with professionals on notions of context and cognitive defusion, again supported by experiential exercises. They also worked on the clarification workers’ personal objectives, goals, and values through dialogue, group discussion, and relevant exercises. This session continued the mindfulness practice to promote contact with the present moment, and workers conducted meditation on their thoughts to facilitate cognitive defusion. Finally, in the third session, therapists again used metaphors and experiential exercises to reinforce the material. Regarding the practice of mindfulness, during the session, participants meditated on their emotions, using self-compassion meditation that aimed to promote an attitude of acceptance and self-care in the face of emotionally difficult experiences. During the three sessions, care was taken that all the examples and discussions could be applied to both workers’ work and personal environments. In addition, participants were encouraged from the first day to carry out exercises at home during the week. On the same day that participants attended the session, they received an email containing all the material covered during the session, together with an audio recording to help them to go deeper into practice. Finally, throughout the week and during the follow-up period, participants received messages on their mobile phones to remind them and motivate them to practice activities at home. Study Variables Depression, anxiety, and stress. These factors were evaluated using the Spanish version of the DASS-21 Scale (Daza et al., 2002), which consists of 21 items to assess symptoms of depression (7 items; e.g., “In the last week, I felt sad and depressed”), anxiety (7 items; e.g., “In the last week, I was afraid for no reason”), and stress (7 items; e.g., “In the last week, I felt very nervous”). The Likert-type response scale ranged from 0 = never to 3 = most of the time. Cronbach’s alpha values for this study were .85, .70, and .91 for depression, anxiety, and stress, respectively. Table 2 Means, Standard Deviations, Mann-Whitney U, and ANCOVA Results for the Variables 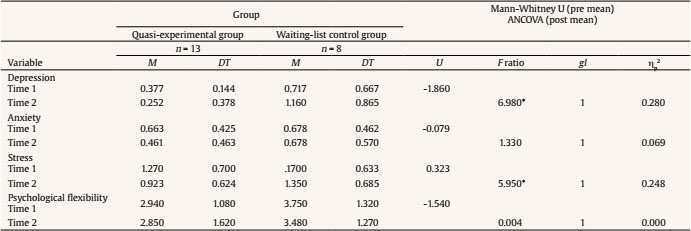 Note. ηp2 = partial eta squared. The Mann-Whitney U test assessed whether the means in both groups at T1 (pre-intervention) for the different variables were statistically different. The ANCOVA assessed whether the means of both groups at T2 (post-intervention) for the different variables were statistically different, controlling for means at T1 (pre-intervention); *p < .05, **p < .01. Psychological flexibility. Psychological flexibility was evaluated using the Spanish version of the AAQ-II questionnaire (Ruiz et al., 2013). This questionnaire consists of 7 items (e.g., “My painful memories prevent me from leading a full life”) and uses a Likert-type response format ranging from 1 = never true to 7 = always true. Cronbach’s alpha values for this study was .90. Semi-structured post-intervention interview. Three questions were asked of each of the nine professionals who agreed to be interviewed after the intervention: (1) “What was your motivation for enrolling in the workshop?”, (2) “Has the workshop helped you in any way?”, and (3) “Have you noticed any changes, since the work-shop, in the way you relate to stress, to your negative emotions, feelings, or thoughts, or to others in your work or personal life?” Data Analysis First, Mann-Whitney U and chi-square tests were performed to determine whether there were differences between socio-professional and dependent variables before starting the intervention. To analyze the effect of the group on the change of dependent variables, a covariance analysis (ANCOVA) was performed, using partial eta squared statistic (ηp2) as an indicator of effect size. For this indicator, values of .01, .06, and .14 indicated small, moderate, and large effects, respectively (Olejnik & Algina, 2000). A non-parametric test of Wilcoxon’s sign ranges was carried out to observe changes before and after the intervention in each of the groups, and to evaluate changes one month after the end of training in the total set of participants attending follow-up. In this case, r values of. 10, .30, and .50 were used to reflect small, medium, and large changes, respectively (Cohen, 1988). To analyze the indirect effect of the “psychological flexibility” variable as an element by which change in dependent variables could be produced, a simple mediation model was tested using a bootstrapping procedure and the PROCESS macro for IBM® SPSS Statistics 24 (model 4; Preacher & Hayes, 2008). Semi-structured interviews were analyzed using a qualitative methodology based on thematic analysis (Braun & Clarke, 2006). This was carried out following the six-step procedure proposed by Braun and Clarke (2006). Specifically, interviews were first transcribed by one of the authors of this paper. At this point, interview transcripts were read and re-read, noting main ideas. In the second phase, carried out by two of the other authors of this paper independently, interesting characteristics of data were coded for the whole data set. Codes were then collected for potential themes, which were identified, defined, compared, discussed, and refined by researchers. Finally, vivid and clear extracts were selected and analyzed in relation to research questions. Quantitative Analysis Mann-Whitney U test (Table 2) revealed that both groups showed no significant differences in dependent variables before the training began. Regarding the results of inter-group comparison, as also shown in Table 2, results of the ANCOVA test revealed that training produced significant changes of large magnitude in depression (F = 6.98, p < .05, ηp2 = .280) and perceived stress (F = 5.95, p < .05, ηp2 = .248) variables, with decreased means for the quasi-experimental group after training; however, there were no changes in either anxiety or psychological flexibility of professionals. In fact, the latter variable did not explain changes found in the depression and stress variables as hypothesized, according to confidence intervals of the mediation test (estimator = -0.0141, SE = 0.08 [0.239, 0.070] and estimator = -0.0158, SE = 0.08 [-0.263, 0.100], respectively). In terms of changes within both groups, the Wilcoxon test (see Table 3) revealed that the quasi-experimental group significantly decreased their levels of perceived stress after training (z = -2.24, p < .05, r = .43)—a change of medium magnitude. The waiting-list control group, while remaining in the waiting list condition, increased their mean for depression (z = -2.55, p < .01, r = -.63), with a large effect size. Later, when this group moved into training, no significant changes were observed within the group. Table 3 Comparison of pre-post Means (Wilcoxon test) within Each Group and at Follow-up  Note. z = non-parametric Wilcoxon test statistics; r = indicates the size of the effect of the z statistics. * p < .05, ** p < .01. One month after the training, participants in both groups who completed the follow-up measure showed significant changes in the perceived stress variable (z = -2.13, p < .05, r = .43), with a moderate effect size. Finally, participants showed a high level of satisfaction with their participation in this workshop. On a scale of 1 (very negative) to 10 (very positive), participants (n = 16) indicated a notable degree of learning (M = 7.6), and found training extremely useful for their daily work (M = 8.5). In addition, workers indicated that the content of the workshop aroused their interest (M = 8.8), and their overall satisfaction was high (M = 8.5). Qualitative Analysis Theme 1: Motivations for participating in the workshop. Most participants reported that their interest in registering for the workshop was mainly linked to “finding tools to deal with the stress” (sub-theme 1.1) that they were experiencing at that time in their lives, both inside and outside work. One of the nurses expressed this view: I thought it might help me to improve my anxiety and stress levels, especially, and my attitude toward my children, my family... I thought it could help me in that sense (E.9). Another, smaller, group of professionals claimed that their main motivation was “the drive to increase their knowledge” (sub-theme 1.2) about SMT. One nurse referred to it as follows: It’s something I had heard about and didn’t have much knowledge about ... and I like it, so I’m interested... It’s something I wanted to know more about really (E.6). Theme 2: Perceived health, wellness, and interpersonal relationship benefits. Brief ACT-based SMT produced changes in nurses’ perceptions of their physical health, energy, and interpersonal relationships, both on and off the job. Below is one of the professionals’ comment that reflected “improvements in physical symptoms” (sub-theme 2.1): Attention on breathing relaxes me and that helps me a lot. Now I don’t have so much tension. I found that, previously, I had back pains... also in the shoulders, but now the area is more relaxed (E.7). On some occasions, an “improvement in energy and vitality levels” was also identified (sub-theme 2.2), as stated by this professional: At work I am more attentive to what I do, which makes me face things with more equanimity, and with fewer expectations, you know? Surprisingly I feel more energy. Anyway, I am open to what comes; bring it on! … It was not so before (E.7). In addition, interviews revealed a generalized sense that, following the workshop, professionals experienced an “improvement in their ways of relating to others, both inside and outside of work” (sub-theme 2.3): As for my colleagues, I had a very bad introduction to them; not with the work itself, but with my colleagues... Taking the course has served me well, because in the end I have realized that we are all as we are, and we all do the same work: I no longer get angry as I did before. Now I focus on me and try to help them [my colleagues] when I can to generate a good climate (E.3). Theme 3: Changes in psychological processes. ACT-based training has always been concerned with knowing what psychological processes are mobilized during training that can account for changes in variables such as workers’ health, well-being, or performance. In this sense, the results of the thematic analysis showed that many nurses felt that the workshop had contributed, among other aspects, to “increasing awareness of the present moment” (sub-theme 3.1). One extract regarding these experiences are given below: The workshop has helped me to be aware of what I am doing; to not focus so much on things from past or things that are going to happen in the future... because you cannot control them, so focus more on the concrete (E.4). In addition, the nurses mentioned that they perceived an “improvement in attention” (subtheme 3.2), which was one of the aspects on which most of them agreed; for example, one nurse expressed it as follows: It’s been good for me. It’s taught me to often stop, think, and be more attentive. I was never able to breathe properly and try to relax, and I was very nervous. I felt exhausted because I could not stop thinking (E.1). In addition, several professionals expressed the experience of having learned “to let go of negative thoughts and emotions” (sub-theme 3.3)—an aspect practiced during the workshop sessions, which related to other aspects, such as observation of the flow of thought: I have learned to breathe, to listen to myself, even if I sometimes don’t succeed... It has helped me with my thoughts. Now I let them go easily (E.8). Quite a few participants also alluded in their comments to an “increase in their personal acceptance levels” (sub-theme 3.4). This was exemplified by the following excerpt from the comment: I am very demanding with myself, and it has helped me to be more tolerant than I used to be (E.4). The narratives also showed that the attitude of acceptance went beyond the limits of the self and an “attitude of acceptance in complicated situations” became widespread (sub-theme 3.5), as shown by this example: There are times when I think and ruminate too much... for example, the other day my son fell and broke his tooth, and I started thinking about the future and the consequences of having a broken tooth and my responsibility for not having been there to watch him... but then I remembered to tell myself that it had already happened and that I couldn’t control it anymore; to accept that it had already happened and to think about what to do (E.1). After the training, quite a few nurses claimed that they had improved “their ability to manage stressful situations” (subtheme 3.6): We move in very stressful situations, very in the moment, you know? I think this course is very good, because now I can control myself and stop to take a breath in critical situations. I think that it is very good not to burn ourselves out (E.8). Finally, participation in the workshop allowed the nurses to “discover and become aware of new aspects of themselves” (sub-theme 3.7). The following comment exemplify this: I value my surroundings a little more, and other people too... What are you doing in this life? You are getting overwhelmed, spending time on the wrong things, wasting your years... you don’t enjoy life and the moment... and I say: “Let’s see! What am I doing? Slow down a bit... I’m going to relax a bit and enjoy life (E.5). The aim of this study was to test whether an ACT approach in SMT was able to improve the levels of depression, anxiety, and stress among a group of health professionals in an ICU. A mixed quantitative and qualitative methodology was used for this purpose, employing questionnaires and semi-structured interviews. The results of this study reflected that ACT training produced improvements in workers’ levels of “depression” and “perceived stress” while maintaining the quasi-experimental condition. In addition, improvements in stress were observed at intra-group level in those who received the training, while levels of depression increased in the waiting-list control group. After one month, the follow-up showed a significant decrease in stress levels across the entire group. The study therefore concluded that stress was the variable on which ACT-based training had the greatest impact, taking into account its change in the different stages of the study. The results achieved in this research were congruent with those of other studies showing the capacity of short ACT-based training to improve aspects of workers’ mental health (Frögeli et al., 2016; Waters et al., 2018), especially their stress levels (Öst, 2014). Regarding the explanatory mechanism for the improvement of stress levels, the quantitative analysis did not reflect changes in the “psychological flexibility” variable. Although this variable usually mediates changes in mental health for this type of training (Lloyd et al., 2013), this is not always the case (Frögeli et al., 2016). This result could have been due to the use of the AAQ-II questionnaire to measure changes in psychological flexibility: according to some authors, the instrument may be insensitive to changes occurring after this type of brief training (McConachie et al., 2014). The thematic analysis of the interviews conducted with a voluntary subsample of participants revealed that the main reason why nurses signed up for the workshop was their search for a tool that would enable them to cope with their stress levels and the stressful situations they experienced in their daily lives—a finding that coincided with the results of other similar studies (Kinser et al., 2016). In fact, the discourses revealed that the levels of stress in this subsample were high, coinciding with the literature that has explored this phenomenon among ICU professionals (Gómez-Martínez et al., 2015; van Mol et al., 2015). The interviews showed that, in line with the quantitative results of the study, training particularly helped nurses to manage their perceived stress levels and to have a greater sense of control when faced with stressful situations, both on and off the job. This observation was also in line with work that revealed that this type of training is especially beneficial for alleviating work stress (Öst, 2014), significantly for those professionals who experience extreme stress (Waters et al., 2018). In addition, according to the nurses’ experiences, training promoted other improvements in their health and well-being that were consistent with previous literature regarding the effects of this type of intervention; for example, it helped participants to improve their energy and vitality levels (Blanco-Donoso et al., 2017), reduce their strain levels (Lloyd et al., 2013), and improve their interpersonal relationships, both on and off the job (Resnicoff & Julliard, 2018). Nurses’ comments also identified improvements in psychological processes relating to elements that are properly addressed by ACT training; for example, improvements in present moment awareness, mindfulness, acceptance, and observation of flow of thought (associated with the acquisition of a perspective of the self as context and cognitive defusion). These four elements more closely related to “processes of acceptance and mindfulness” proposed by the ACT Hexaflex model, than to “commitment and behavior change processes” (Flaxman et al., 2013), and they seemed to be the ones most impacted by training (Rise et al., 2015). In fact, other qualitative studies have reported that developing mindfulness skills is an interesting means of gaining perspective, learning to focus attention, and increasing levels of non-reactive awareness (Kinser et al., 2016; Resnicoff & Julliard, 2018). In addition, nurses reported a change in attitude emphasizing acceptance and self-care, which may have related to the introduction of self-compassion practices in this training, as previously reported by other studies (García et al., 2018). The results of this research should be interpreted taking into account its limitations. First, in relation to the sample, the number of participants was small, their participation was voluntary, and they could not be randomized to different experimental and control groups; therefore, the internal validity of the study was jeopardized. The impossibility of randomizing participants was due to working conditions and needs that are inevitable within an ICU. The study nevertheless had the value of being developed in a real environment, with professionals who are difficult to access and highly specialized, which may have contributed to increasing the external validity of the study. In addition, participants in both groups showed no differences in pre-training measures, nor in their socio-professional variables or variables relating to their health and well-being. Future research should include a larger number of participants, randomized to different experimental conditions. Second, also in relation to the sample, the flow of participants revealed a significant attrition, especially in the follow-up. Although the problem of participant drop-out is frequent in organizational interventions (Flaxman & Bond, 2010), and may even be more pronounced in work environments such as ICUs, because of their work overload and dynamic nature (Blanco-Donoso et al., 2017), it is important to bear this in mind when generalizing the results. It is possible that e-mail follow-up could have boosted this attraction. Third, the quasi-experimental design included only one waiting-list control group and, in order to increase its internal validity, future research should include other groups with different psychological treatments to form active control groups and facilitate comparison with the experimental one. Fourth, the majority of participants in this study were women; hence, future research should check whether this type of training has gender-differentiated effects. Predominance of women in this type of intervention is, however, common, as is their more frequent presence in the health care professions. Finally, this study reported only statistically significant changes, but not at clinical level. Participating sample was not a clinical sample and values for initial mental health variables were relatively low. It would be desirable for future studies to test the effects of such training with clinical samples of workers and analyze clinically significant changes. Despite these limitations, this study gained value by providing empirical evidence of the effectiveness of short ACT-based training for improving Spanish workers’ mental health and psychological well-being using a mixed quantitative and qualitative methodology. Studies designed with a mixed methodology are especially important when the questionnaires used in a research do not fully reflect the direct experience of people (Grossman & Van Dam, 2011), as was the case in this research. We hope that studies such as this one will encourage other researchers in Spain to continue developing and evaluating this type of program with different methodologies within different organizations. We believe that an ACT approach can be highly relevant to addressing emotional issues generated by the COVID-19 crisis among health professionals working in ICUs. Its approach to working with emotional suffering and negative internal events (e.g., traumatic memories or feelings of guilt), its emphasis on behavioral activation, its orientation toward personal values, and its recent incorporation of aspects such as self-compassion, make it an ideal intervention for use in the present crisis. Nevertheless, we insist on the need to implement, together with this type of worker-centered intervention, actions aimed at redesigning the workplace and improving organizational conditions, in order to carry out more holistic interventions that can generate greater impact. Conflict of Interest The authors of this article declare no conflict of interest. Acknowledgements The authors would like to thank the Occupational Risk Prevention Service and the Intensive Care Medicine Service of the Puerta de Hierro Hospital for making this research possible. Note 1 This research has received the Rafael Burgaleta Award, XXVII edition, granted by the Colegio Oficial de la Psicología de Madrid. Cite this article as: Blanco-Donoso, L. M., Garcia-Rubio, C., Gallardo, J. A., Pereira, G., Rodríguez de la Pinta, M. L., Rubio, J. J., and Garrosa, E. (2021). ACT-based stress management training aimed at improving workers’mental health in an intensive care unit: A mixed methods study. Clínica y Salud, 32(3),111-117. https://doi.org/10.5093/clysa2021a12 Funding: This work was supported by I+D+I National Project of the Ministerio de Ciencia e Innovación (PID2019-106368GB-I00) AEI/10.13039/501100011033. Primer Premio de la XVII edición del Premio de Psicología Aplicada “Rafael Burgaleta” 2020 References |
Cite this article as: Blanco-Donoso, L. M., Garcia-Rubio, C., Gallardo, J. A., Pereira, G., Pinta, M. L. R. D. L., Rubio, J. J., and Garrosa, E. (2021). ACT-based Stress Management Training Aimed at Improving WorkersŌĆÖ Mental Health in an Intensive Care Unit: A Mixed Methods Study1. Cl├Łnica y Salud, 32(3), 111 - 117. https://doi.org/10.5093/clysa2021a12
luismanuel.blanco@uam.es. Correspondence: luismanuel.blanco@uam.es. (L. M. Blanco-Donoso).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
Clinical and Health is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License








