


The Relationship between Healthcare Experience and Perinatal Depression during COVID-19 Pandemic
[La relaci├│n entre la experiencia de la atenci├│n sanitaria y la depresi├│n perinatal durante la pandemia COVID-19]
Katina Kovacheva1, Maria F. Rodríguez-Muñoz1, Diego Gómez Baya2, Sara Domínguez Salas3, and Emma Motrico3
1Universidad Nacional de Educaci├│n a Distancia (UNED), Madrid, Spain; 2Universidad de Huelva, Spain; 3Universidad Loyola Andaluc├şa, Dos Hermanas, Seville, Spain
https://doi.org/10.5093/clysa2022a13
Received 26 January 2022, Accepted 21 June 2022
Abstract
Background: The prevalence of peripartum depression (PPD) has increased substantially since the start of the COVID-19 pandemic. To reduce the probability of contagion, hospitals had to adapt their care protocols, including the care of women in the perinatal period. Method: A cross-sectional study was used in a total sample of 3,356 women, 1,402 in the prenatal period and 1,954 in the postnatal period. They completed the Edinburgh Postnatal Depression Scale to assess depressive symptoms and the Spanish version of the Coronavirus Perinatal Experiences to assess health experience. Results: The results showed that feeling very well supported by a health professional was associated with a lower risk of PPD. On the other hand, believing it very important to have access to a mental health professional and being concerned about changes in infant care due to COVID-19 were associated with a higher risk of PPD. Conclusion: The results showed the relationship between health experience and the risk of depressive symptoms, highlighting the importance of considering the psychological aspects in the development of measures and protocols for perinatal care.
Resumen
Antecedentes: La prevalencia de la depresión perinatal ha aumentado sustancialmente desde el inicio de la pandemia debido al coronavirus (COVID-19). Para reducir la probabilidad de contagio, los hospitales tuvieron que adaptar sus protocolos asistenciales, incluyendo la atención a las mujeres en el periodo perinatal. Método: Se utilizó un estudio transversal en una muestra total de 3,356 mujeres, 1,402 en el período prenatal y 1,954 en el período postnatal. Cumplimentaron la Escala de Depresión Postnatal de Edimburgo para evaluar los síntomas depresivos y la versión española de la Encuesta sobre Experiencias Perinatales durante el Coronavirus para evaluar la experiencia de la atención sanitaria. Resultados. Los resultados mostraron que sentirse muy bien apoyada por un profesional de la salud se asoció con un menor riesgo de desarrollar depresión perinatal. Por otro lado, creer que es muy importante tener acceso a un profesional de la salud mental y estar preocupada por los cambios en el cuidado del bebé debido al COVID-19 se asociaron con un mayor riesgo de depresión perinatal. Conclusión: Los resultados mostraron la relación entre la experiencia sanitaria y el riesgo de síntomas depresivos, destacando la importancia de considerar los aspectos psicológicos en el desarrollo de medidas y protocolos de atención perinatal.
Palabras clave
Depresi├│n, Perinatal, COVID-19, Experiencia sanitariaKeywords
Depression, Peripartum, COVID-19, Healthcare experienceCite this article as: Kovacheva, K., Rodríguez-Muñoz, M. F., Baya, D. G., Salas, S. D., & Motrico, E. (2022). The Relationship between Healthcare Experience and Perinatal Depression during COVID-19 Pandemic. Cl├şnica y Salud, 33(3), 117 - 125. https://doi.org/10.5093/clysa2022a13
katina.ilieva.90@gmail.com Correspondence: katina.ilieva.90@gmail.com (K. Kovacheva).Since the World Health Organization (WHO) declared COVID-19 an international public health emergency, healthcare systems have to adapt continuously. To reduce the risk of contagion, healthcare providers have adopted practices based on the scientific knowledge that has gradually been gathered regarding COVID-19 (López-Rubio, 2020). For vulnerable groups, such as women in the perinatal period, healthcare systems have adapted their resources at national and local levels. This change includes developing specific guidelines on perinatal care focused on assistance in possible or confirmed cases of COVID-19 (López-Rubio, 2020). These guidelines have provided general and illustrative indications, leaving the adaptation of recommendations to health centers. This situation creates great heterogeneity in pregnancy, childbirth, and puerperium (Baena-Antequera et al., 2020). Throughout the pandemic, the fear of the alarming numbers of admissions and deaths led to situations far removed from the concept of “humanization” of pregnancy and childbirth on which medicine is focusing at present (López-Rubio, 2020). Restrictions such as the exclusion of companions and the separation of mothers and babies are changes not evidence-based that can have unintended iatrogenic effects (Lalor et al., 2021), in addition to increasing feelings of anxiety and causing women to feel inadequately supported (Aydin et al., 2022). As an important part of maternity care activities, the WHO recommends supporting pregnant women’s emotional and psychological facets (American Health Organization, 2018). The WHO (2018) declared peripartum depression (PPD) as an issue of global importance. The approximate prevalence of PPD is 15.2% in pregnant women (Marcos-Nájera et al., 2020) and 13% in women in the puerperium period (WHO, 2018). However, during the pandemic, depressive symptoms increased substantially from 22% to 47% overall prevalence (Hessami et al., 2020; Motrico et al., 2022). These data are significantly related to the specific concerns of pregnant regarding COVID-19 (Lebel et al., 2020). The pandemic has been a major stressor for pregnant women (Chen et al., 2020) and a potential predictor of PPD (Lancaster et al., 2010). PPD is a mental disorder characterized by a depressive mood and loss of interest with mild to major severity occurring during pregnancy or in the first year postpartum (Fonseca et al., 2020; ). Other characteristic symptoms are permanent sadness, frequent crying, sleep problems, fatigue, difficulty concentrating, feelings of worthlessness, and guilt toward motherhood or the baby (Pereira et al., 2014). PPD has negative medical and psychological consequences for the mother and the baby (Al-Halabí et al., 2021; Slomian et al., 2019), including thoughts of self-harm that can reach severe levels and suicide attempts (Al-Halabí & Fonseca-Pedrero, 2021). PPD also affects family dynamics (Slomian et al., 2019) and has important consequences for the healthcare system, entailing high economic costs for society (Castelao, Le, et al., 2022; Castelao Rodríguez-Muñoz, et al., 2022, Fonseca-Pedrero et al., 2021). These implications highlight the urgent need to identify specific PPD risks and protective factors during the pandemic. Changes in perinatal healthcare due to the COVID-19 pandemic are likely to contribute to perinatal distress, making access to clear information and communication an important strategy to ensure women’s sense of understanding and control over their situation (Suwalska et al., 2021). Lebel et al. (2020) observed that higher symptoms of depression are associated with greater concern about the threats of COVID-19 to the mother’s and baby’s lives and concern about not receiving needed prenatal care. Another common concern is the fear of becoming infected during hospital visits for prenatal check-ups and delivery (Kahyaoglu & Kucukkaya, 2020). Another important variable is the information received from professionals regarding COVID-19, with the risk of depression being 8.87-fold higher in uninformed women than in informed (Kahyaoglu & Kucukkaya, 2020). Support from midwives and other healthcare professionals is critical to supporting women’s mental health, understanding it as a fundamental need for maternal well-being (Suwalska et al., 2021). The objectives of this study were to 1) identify the variables of healthcare experiences related to PPD during the COVID-19 pandemic, 2) estimate the extent to which healthcare experiences are related to the risk for PPD, and 3) assess differences between the prenatal and postnatal periods in terms of these risk factors for PPD. We expected to find that variables related to women’s perception of perinatal care are associated with depressive symptoms. In addition to it, having differences in perinatal care needs would be observed between the prenatal and postnatal periods. The healthcare professional has had to adapt to information and communication technologies to reduce face-to-face appointments to those essential for screening or diagnostic tests, thereby minimizing the risk of contagion. But the psychological discomfort that may arise must also be addressed to mitigate its short and long-term results. Design A cross-sectional study was used to examine risk and protective factors in perinatal care of women during pregnancy and postpartum. These data are part of an international study on the impact of the COVID-19 pandemic on perinatal mental health (Riseup-PPD-COVID-19), whose study protocol was published and described in detail (Trial registration: ClinicalTrials.gov; Identifier: NCT04595123; Motrico et al., 2021). The STROBE Statement for reporting cross-sectional studies was followed (Elm et al., 2007). Participants The sample included 3,356 subjects, 1,402 pregnant women, and 1,954 postpartum women living in Spain. The inclusion criteria included a) being pregnant or a biological mother of a child aged 6 months or less, b) being 18 years or older, c) living in Spain, and d) consenting to participating in the study. Before performing the statistical analyses, 4,316 respondents were manually verified, and 960 records were eliminated due to an erroneous duration of pregnancy (> 42 weeks) or children being older than six months of age (n = 636). The present study received approval from the Ethics Committee (Ethics Protocol: 1257-N-20). All data were completely anonymized, according to the Helsinki Declaration of Research with Human Beings. Procedure Participants were recruited between June 16 and December 04, 2020 through social networks, organizational networks, policymakers, local organizations, and other stakeholders (using the network provided by The Research Innovation and Sustainable Pan-European Network in Peripartum Depression Disorder (Riseup-PPD). The ethics committee approved the study of the Junta de Andalucía (Department of Health of the Andalusian government, Spain) (Ethics Protocol: 1257-N-20), complying with all national data protection regulations. Participation in the study was voluntary, and we guaranteed the confidentiality of all information provided. Participants completed the questionnaire online through the project website link (https://momsduringcovid.org) using the Qualtrics survey platform. Participants were previously informed about the study’s objectives, the content of the questions, the possible risks and benefits, and the ethical aspects of the study. Instruments The Spanish version of the Coronavirus Perinatal Experiences- Impact Survey (COPE-IS) assessed the healthcare experience during the COVID-19 pandemic. The COPE-IS is a newly developed measure designed to ask about the experiences of new and expectant mothers in the time of the Coronavirus COVID-19 (SARS-CoV-2) pandemic. At present, psychometric properties for the measure have yet to be established and scoring procedures have yet to be determined (Thomason et al., 2020). Specifically in this study, we selected items related to prenatal and postnatal experiences during the COVID-19 pandemic. The items used in the prenatal stage were: (1) “How supported do you feel by the health care professional during pregnancy [very well supported-somewhat well supported-not very well supported]?”; (2) “Has the support you receive in health care visits during pregnancy changed due to COVID-19 (coronavirus) [significantly worsened-somewhat worsened-no change-somewhat improved-significantly improved]?”; (3) “Are you concerned about possible future changes to your medical care during your baby’s birth as a result of the COVID-19 outbreak [1-7 Likert scale, 1 = no concern, 7 = highly concerned]?”; (4) ”Do you have any concerns about your child’s health as a result of the COVID-19 outbreak [yes-no]?”; (5) “How important are the following to help you and your family during the COVID-19 outbreak [not important at all-somewhat important-very important]: (a) more personalized care with the prenatal care provider; (b) information about how to reduce stress; (c) access to a mental health provider; (d) online support groups; (e) interaction with other pregnant people; (f) rapid response to questions and concerns; (g) examples of how other women are planning for potential changes in their pregnancy, birth and postpartum care; (h) information on COVID-19 and infant health?”. Table 1 Main Characteristics of the Participants  The items used in the postnatal stage were: (1) “How would you evaluate the support received from postnatal health care professionals [very well supported-somewhat well supported-not very well supported]?”; (2) “Did the support you received from postnatal care professionals change due to COVID-19 (coronavirus) [significantly worsened-somewhat worsened-no change-somewhat improved-significantly improved]?”; (3) “How concerned are you about possible future changes in the way you will care for your baby [1-7 Likert scale, 1 = no concern, 7 = highly concerned]?”; (4) “How concerned are you about your child’s health as a result of the COVID-19 (coronavirus) outbreak [1-7 Likert scale, 1 = no concern, 7 = highly concerned]?”; (5) “How important are the following to help you and your family during the COVID-19 outbreak [not important at all-somewhat important-very important]: (a) more personalized care with my healthcare professional; (b) information about how to reduce stress; (c) access to a mental health professional; (d) online support groups; (e) interaction with other parents; (f) quick response to questions and concerns; (g) examples of how other mothers are preparing for possible changes in their postpartum and infant care plans; (h) information on COVID-19 and children’s health; (i) more personalized attention with my child’s physician?”. The Edinburgh Postnatal Depression Scale (EPDS; Cox et al., 1987) assessed depressive symptoms. EPDS is the most internationally recommended and used scale (Levis et al., 2020), specifically designed to detect PPD (Cox, 2019). EPDS consists of 10 items with four response options. The total score of the scale ranges from 0 to 30. The Spanish validation of the scale was used (García-Esteve et al., 2003), establishing a cut-off point of 13 or more to identify clinically significant symptoms. We assumed a lower sensitivity but higher specificity (Levis et al., 2020). In the present study, the Cronbach’s α obtained was .89. A sociodemographic questionnaire was included to ascertain the main characteristics of the participants (age, educational level, unemployment status, giving birth for the first time, and cohabiting couple). Statistical Analysis All analyses were performed with the IBM SPSS Statistics package (version 24). The criterion variable (PPD) was measured dichotomously with the EPDS ≥ 13. Records with no missing values were used for all analyses. Differences between the presence or absence of depression were analyzed concerning the categorical variables, contingency tables were performed, and the Pearson’s chi-square statistic was applied. Cramer’s V effect size index accompanied the scores following the interpretation scale: .00-.19, insignificant; .20-.49, small; .50-.79, medium; > .80, high (Cohen, 1988). Binary logistic regression analyses were performed by the intro method to estimate predictors. The confidence level was set at 95%, and the significance levels were at 1% and 5% (p < .01 and p < .05, respectively). Sociodemographic Profile of the Participants The sample participants were 3,356 subjects, 1,402 pregnant women and 1,954 postpartum women. Table 1 shows the socio-demographic characteristics of the sample. The mean age was 33.67 (4.25). The majority lived with a partner (81.4%), had a university level of education (71.7%), and were employed (89.2%). Table 2 Descriptive and Comparative Analysis between Women in Prenatal Period with and without PPD 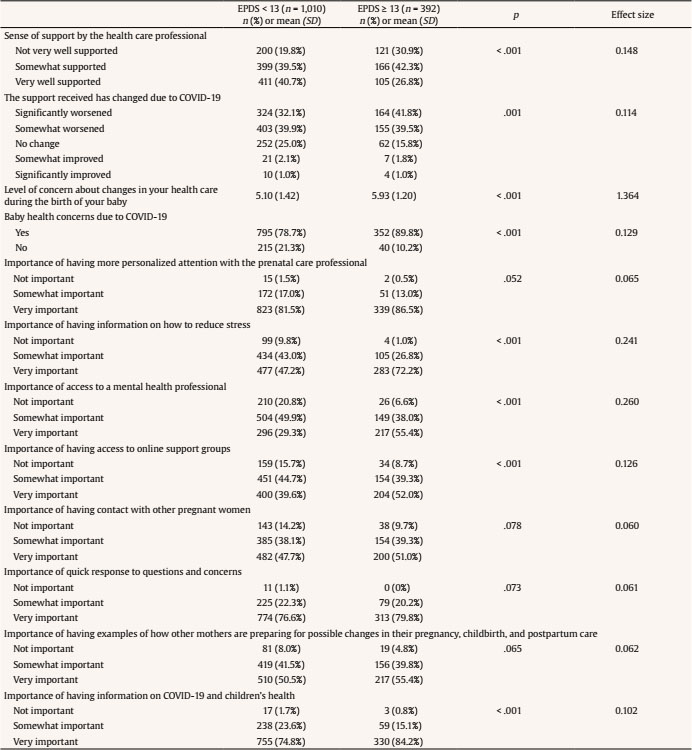 Descriptive and Comparative Analysis Table 2 shows the comparison of healthcare experience and the importance of prenatal care resources during the prenatal period between women who had clinically significant symptoms of depression and those who did not. Regarding healthcare experience, the results showed significant differences in all five items. Specifically, among women with suspected depression, the percentages of those who did not feel supported by a healthcare professional (30.9% vs. 19.8%), considered that the support received significantly worsened due to COVID-19 (41.8% vs. 32.1%), and were concerned about changes in healthcare during birth due to COVID-19 (90.1% vs. 79.6%) were high. The percentage among those concerned about the baby’s health due to COVID-19 was high (89.8% vs. 78.7%), with a high mean level of concern (5.93 vs. 5.10). We compared the importance of prenatal care resources. The results showed significant differences in information about stress reduction, access to a mental health professional, online support groups, and information about COVID-19 and infant health. Specifically, among women with suspected depression, the percentages of those who considered receiving information on how to reduce stress (72.2% vs. 47.2%), had access to a healthcare professional (55.4% vs. 29.3%), had access to online support groups (52% vs. 39.6%), and received information on COVID-19 and infant health (84.2% vs. 74.8%) were high. Table 3 shows the comparison of healthcare experience and the importance of prenatal care resources during the postnatal period between women who had clinically significant symptoms of depression and those who did not. Table 3 Descriptive and Comparative Analysis between Postpartum Women with and without PPD 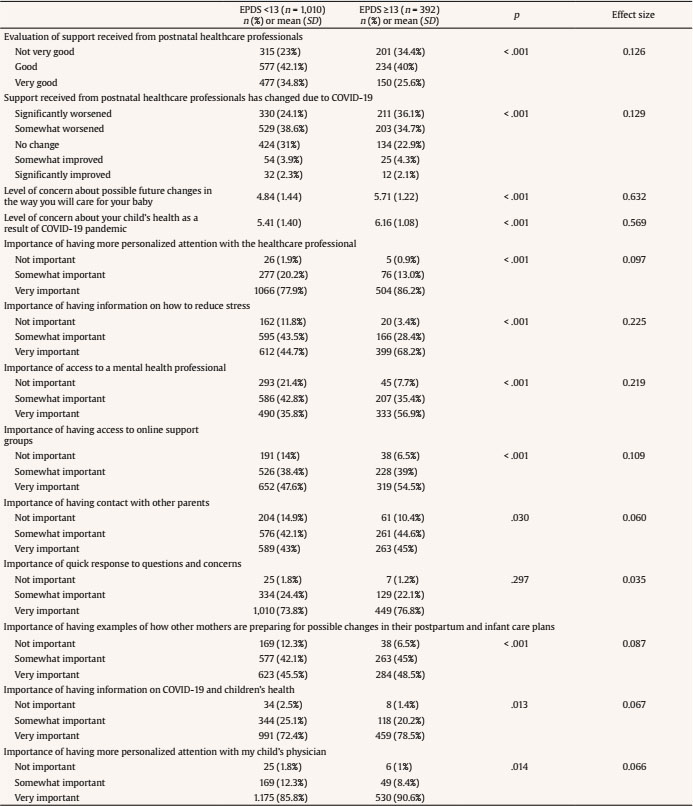 Regarding healthcare experience, the results showed significant differences in all four items. Specifically, the percentage of women with suspected depression is higher among those who did not feel supported by the professional (34.4% vs. 23%), considered that the support received significantly worsened due to COVID-19 (36.1% vs. 24.1%), were more concerned about changes in the care of their baby due to COVID-19 (5.71 vs. 4.84) and the level of concern for the baby’s health due to COVID-19 was higher (6.16 vs. 5.41). Regarding the importance of postpartum care resources, the results showed significant differences concerning having more personalized attention with the healthcare professional, information on stress reduction, access to a mental health professional, online support groups, contact with other parents, having examples of how other mothers cope with changes in their postpartum plans and baby care, information on COVID-19 and infant health, and personalized attention with their child’s physician. Specifically, among women with suspected depression, the percentage was higher among those who considered having a more personalized relationship with the healthcare professional as very important (86.2% vs. 77.9%), receiving information on how to reduce stress (68.2% vs. 44.7%), having access to a healthcare professional (56.9% vs. 35.8%), having access to online support groups (54.5% vs. 47.6%), having contact with other parents (45% vs. 43%), having examples of how other mothers prepare for changes in their postpartum plans and baby care (48.5% vs. 45.5%), receiving information about COVID-19 and infant health (78.5% vs. 72.4%), and having a more personalized relationship with their child’s physician (90.6% vs. 85.8%) are shown in Table 3. In both groups, most of these differences were small or insignificant effect sizes. Regression Analysis Regarding the prenatal period, as shown in Table 4, the results showed that women who feel very well supported by healthcare professionals (OR = 0.62, p = .037) had decreased risk of depression. In contrast, women who considered receiving information about stress reduction as very important (OR = 7.50, p = ≤ .001), those who believed it somewhat important (OR = 4.02, p = .016) or very important to have access to a mental health professional (OR = 3.05, p ≤ .001), those who were concerned about their baby’s health due to COVID-19 (OR = 1.73, p = .025), and who were concerned about changes in care during birth due to COVID-19 (OR = 1.50, p ≤ .001) had an increased risk of depression. Table 4 Predictors of Suspected Depression in Women in the Prenatal Period 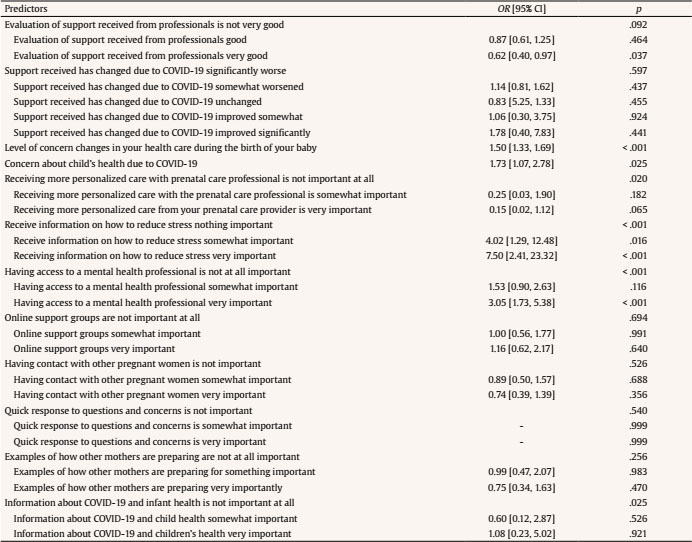 This regression model provided a Nagelkerke’s R2 of .245. Receiving operating characteristics (ROC) curves (Aycaguer, 1994) were analyzed to explore the sensitivity and specificity index, obtaining a value of 70% and 69.97%, respectively. A total of 69.99% of cases were correctly classified by the model. Regarding the postnatal period, as shown in Table 5, the results showed that women who felt very well supported by a healthcare professional (OR = 0.61, p = .035) had a lower risk of depression. Conversely, women who considered having access to a mental health professional as very important (OR = 2.60, p = .002) and were worried about changes in their baby’s care (OR = 1.38, p ≤ .001) and health due to COVID-19 (OR = 1.29, p ≤ .001) had a higher risk of depression. Table 5 Predictors of Suspected Postpartum Pepression in Women  This regression model provided Nagelkerke’s R2 of .217. A ROC curve analysis (Aycaguer, 1994) was performed to explore the sensitivity and specificity index, obtaining 66.26% and 66.29%, respectively. A total of 66.27% of cases were correctly classified by the model. During the perinatal period, women have a higher risk of developing a mental health problem (Hahn-Holbrook et al., 2018). This risk increases even more in extreme stress or conflict situations or during emergencies (WHO, 2020), such as the COVID-19 pandemic. Therefore, the measures adopted to deal with this situation must consider psychological aspects. In this study, we aimed to identify the specific aspects that should be considered. Fear is the normal and central emotional response in an epidemic. The threat of becoming infected, with the consequences that this can have on the fetus, and the lack of information, are stressful for the mother’s mental health (Motrico et al., 2022). This study showed that women who were more worried about their baby’s health due to COVID-19 had a higher risk of depression throughout the perinatal period. One of the most commonly observed concerns in the perinatal period was the fear of becoming infected during hospital visits for check-ups and delivery (Kahyaoglu & Kucukkaya, 2020). Providing inadequate or insufficient information can increase their fear. Hence, people must get information from reliable, accurate, and understandable sources (Brooks et al., 2020). Another predictor variable for PPD was concerned with healthcare changes during birth and infant care due to COVID-19. Women with greater concern had a higher risk of depression, with this risk being slightly higher prenatally than postpartum. Changes in perinatal healthcare, such as hospital restrictions, partner and family visits, and remote consultations, are inevitable (Zhou et al., 2020). Clear communication about preventive measures or any new procedure applied to prenatal care is essential to reduce the discomfort or psychological distress involved in such a change. This practice also promotes commitment and compliance with safety measures (Finset et al., 2020). Hence, the most important outcome throughout the perinatal stage of the study is access to a mental health professional, which is also a predictor variable for depression. This result showed interest in and acceptance of psychological treatment. Women who perceived having access to a healthcare professional as very important had a higher risk of depression, this risk being higher in the prenatal stage. Pandemic stress will affect vulnerable groups more, similarly to the case of pregnant women. It is not unusual for them to request help that is difficult to reach because of the adjustment of mental health services (Chacón-Fuertes et al., 2020). The result showed that another factor pregnant women consider very important in the prenatal stage was the need to receive information on how to reduce stress. Women who considered this variable somewhat important or very important had a higher risk of depression. Thus, providing stress reduction tools can mitigate the negative consequences and lower the levels of distress due to these changes (Zhou et al., 2020). However, given the risk of COVID-19 contagion, non-essential professionals, such as psychologists, are discouraged. Therefore, the task of psychosocial support falls to the medical team attending the person, which is generally the midwife. However, healthcare professionals’ work and emotional overload and the effectiveness of digital interventions (Muñoz et al., 2021) must be taken into account. The feeling of support from a healthcare professional should be highlighted as a protective factor against depression throughout the perinatal stage. Feeling very well supported by a healthcare professional was related to less risk of depression. Multiple studies have been conducted on risk factors for triggering depression; most studies emphasized the strong association between lack of support and prenatal depression (Lancaster et al., 2010). The analysis of the differences between women across the perinatal stage with suspected depression and without depression also showed that the percentage of women who believed that the support received significantly worsened due to COVID-19 was higher among women with PPD. The rate of women with depression was higher among those who considered having online support groups and information about COVID-19 and infant health very important. Another study showed that the variable information received from professionals is influential on depression (Kahyaoglu & Kucukkaya, 2020). In addition to these results, in the descriptive and comparative analysis, we observed a greater need for the availability of care resources in the postnatal stage. This is the stage in which there is a greater relationship with symptoms of depression among women who consider it important to have access to resources related to raising their baby, such as being in contact with other parents, having examples of how other mothers prepare for care, and having a more personalized relationship with their child’s physician. The results are in line with other studies; the need for support resources was greater in the postnatal stage than in the prenatal stage (Xie et al., 2009). All these concerns are normal and natural reactions to the situations in which we find ourselves (WHO, 2020). However, these situations can generate strong emotions (Usher et al., 2020) that must be addressed to avoid becoming a problem. In this situation, clear, brief, consistent, and frequent communication is key to achieving public trust and providing a sense of control, thereby modifying a person’s perception and response (Robles-Sanchez, 2020). The healthcare professional must provide evidence-based information on the effects of COVID. This situation makes mental health professionals more necessary than ever. This study has several limitations. For example, this study was voluntary, and its design was cross-sectional. Therefore, this research had a selection bias, and its design made it difficult to establish causal relationships. However, the sample was large, and the topic of the study was relevant. Population-based measures should no longer be held without the collaboration of expert psychologists or mental health workers (Chacón-Fuertes et al., 2020). Our data agreed with Lebel et al. (2020), who indicated the need to prioritize high-quality perinatal care for women. In particular, when genetic, environmental, and behavioral factors determine the present and future health of the mother and the baby, the pandemic approach determines the health of future generations (Riquelme-Gallego, 2021). However, in addition to the consequences of the pandemic, we must establish improved protocols for future emergencies. The current model of the field of study of emergencies is directed toward a preventive institutional mission. Therefore, the data obtained from this type of research should be taken into account to create action protocols that prioritize risk reduction, attend to emergencies, and advance reconstruction activities (Robles-Sanchez, 2020). Conflict of Interest The authors of this article declare no conflict of interest. Funding: This project is part of the ‘COST Action Research Network in Peripartum Depression’ (Riseup-PPD CA 18138) Cite this article as: Kovacheva, K., Rodríguez-Muñoz, M. F., Gómez Baya, D., Domínguez Salas, S., & Motrico Martínez, E. (2022). The relationship between healthcare experience and perinatal depression during COVID-19 pandemic. Clínica y Salud, 33(3), 117-125. https://doi.org/10.5093/clysa2022a13 References |
Cite this article as: Kovacheva, K., Rodríguez-Muñoz, M. F., Baya, D. G., Salas, S. D., & Motrico, E. (2022). The Relationship between Healthcare Experience and Perinatal Depression during COVID-19 Pandemic. Cl├şnica y Salud, 33(3), 117 - 125. https://doi.org/10.5093/clysa2022a13
katina.ilieva.90@gmail.com Correspondence: katina.ilieva.90@gmail.com (K. Kovacheva).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
Clinical and Health is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License








