


Resilience Moderates the Associations between Bipolar Disorder Mood Episodes and Mental Health
[La resiliencia modera la asociaciĂłn entre los episodios anĂmicos del trastorno bipolar y la salud mental]
Ainara Echezarraga, Esther Calvete, Izaskun Orue, and Carlota Las Hayas
University of Deusto, Spain
https://doi.org/10.5093/clysa2022a8
Received 4 March 2021, Accepted 4 January 2022
Abstract
Resilience could moderate the impact of bipolar disorder (BD) on patients’ quality of life (QoL) and psychosocial functioning. This study aimed to (1) explore the relationships between bipolar disorder mood episodes (depression, [hypo]mania, and euthymia) and mental health outcomes of QoL, personal recovery, impaired work, and psychosocial functioning in individuals with BD; and (2) determine whether resilience domains were moderators of these associations. A clinical adult sample of 97 individuals diagnosed with BD (63.90% female, mean age = 45.02 years) completed a battery of BD-specific measures of resilience and mental health-related variables. Multiple regression showed that self-management of BD resilience domain moderated the negative relationship between (hypo)manic episode and personal recovery. Furthermore, self-confidence moderated the positive relationships between (hypo)manic and depressive episodes and impaired functioning. We suggest that BD patients experiencing (hypo)manic or depressive episodes may improve their mental health and wellbeing through interventions that promote disorder-specific resilience factors.
Resumen
La resiliencia podría moderar el impacto del trastorno bipolar (TB) en la calidad de vida (CV) y funcionamiento psicosocial de los pacientes. Los objetivos del presente estudio fueron: (1) explorar la asociación entre los episodios anímicos bipolares (depresión, [hipo]manía y eutimia) y los resultados de la CV en cuanto a salud mental, la recuperación personal y el deterioro del funcionamiento laboral y psicosocial de personas con TB y (2) determinar si los dominios de resiliencia moderaban esta asociación. Una muestra clínica de 97 personas adultas diagnosticadas de TB (63.90% mujeres, edad media = 45.02) cumplimentaron una batería de medidas específicas de TB sobre resiliencia y variables relacionadas con la salud mental. La regresión múltiple mostró que el dominio de la resiliencia de autogestión del TB moderó la relación negativa entre el episodio (hipo)maníaco y la recuperación personal. Además, la confianza en uno mismo moderó la asociación positiva entre los episodios (hipo)maníacos y depresivos y el deterioro del funcionamiento. Se sugiere que la salud mental y bienestar de los pacientes con TB en episodios (hipo)maníacos o depresivos podrían mejorar mediante intervenciones que desarrollen aspectos de resiliencia específicos de este trastorno mental.
Palabras clave
Trastorno bipolar, Episodios anĂmicos, Resiliencia, Calidad de vida, RecuperaciĂłn personal, Funcionamiento laboral y psicosocialKeywords
Bipolar disorder, Mood episodes, Resilience, Quality of life, Personal recovery, Work and psychosocial functioningCite this article as: Echezarraga, A., Calvete, E., Orue, I., & Hayas, C. L. (2022). Resilience Moderates the Associations between Bipolar Disorder Mood Episodes and Mental Health. ClĂnica y Salud, 33(2), 83 - 90. https://doi.org/10.5093/clysa2022a8
a.echezarraga@deusto.es Correspondence: a.echezarraga@deusto.es (A. Echezarraga).Bipolar disorders (BD) are a group of debilitating chronic mood disorders characterized by repeated recurrence of (hypo)manic and depressive episodes alternating with euthymic periods during which mood disturbances are significantly subsided (American Psychiatric Association [APA, 2013]). Hypomanic and manic episodes are characterized by abnormal and persistent elevated mood. However, for a diagnosis of a manic episode, the duration of elevated mood must be prolonged in time, of greater severity, and usually requires hospitalization. During manic episodes, psychotic features may co-occur together with severe functional impairment. Depressive episodes are characterized by low mood and related symptoms such as profound sadness, feeling worthless and guilty, loss of interest, pleasure, and motivation for daily activity, and impaired functioning (Kendall et al., 2014), with or without psychotic symptoms (APA, 2013). Patients’ evolution is not only measured through clinical symptomatic outcomes but also by the assessment of quality of life (QoL), occupational and psychosocial functioning, and personal recovery. Previous studies coincide reporting that the QoL (Michalak et al., 2005) and psychosocial functioning (Rosa et al., 2010; Strejilevich et al., 2013) of individuals with BD is low, even during euthymic episodes (Haro et al., 2011). Resilience may be a key factor to improve health outcomes for people with BD. Resilience refers to a dynamic process in which a spiral of interactions between interrelated resilience resources emerges to respond adaptively to adversity, promoting mental health from the vulnerability that may be involved in suffering a psychiatric disorder (Hofer et al., 2017; Wathen et al., 2012). Resilience resources may be inherent to individuals’ traits or capacities and may include contextual resources, which may all be learned and acquired. Thus, research on resilience has focused on identifying the protective factors that might moderate the negative effects of adverse conditions (Luthar et al., 2006). Previous studies have evidenced that individuals with BD and high levels of resilience reported better outcomes in recovery, QoL (Echezarraga et al., 2018; Lee et al., 2017), and psychosocial functioning (Bozikas et al., 2018; Echezarraga et al., 2018) compared to individuals with high BD and low levels of resilience. Specific resilience factors, such as self-care, self-confidence, and interpersonal support, have been reported by individuals who no longer present symptoms of BD as essential ingredients for their recovery (Echezarraga, Las Hayas et al., 2019). Furthermore, previous findings have suggested the existence of important differences between bipolar mood episodes in QoL, occupational and psychosocial functioning, and personal recovery. Both manic and depressive episodes are more related to significantly poorer QoL (Votja et al., 2001) and psychosocial functioning (Rosa et al., 2010) than euthymic episodes. Furthermore, the greater the depressive symptomatology after episode remission, the lower the QoL (Michalak et al., 2005) and personal recovery (Dodd et al., 2017) in BD. These previous studies, although scarce, have considered the disorder-specific particularities of QoL, functioning, and personal recovery (see, for a review Michalak & Murray, 2010; Michalak et al., 2007). Nonetheless, concerning previous health-related outcomes (e.g., QoL, functioning), research on BD has mainly focused on euthymic or clinically stable individuals (e.g., Özer et al., 2002) or, when including those in manic, hypomanic, or depressed episodes, clinician-reported assessments have been employed and/or has focused on bipolar episodes as predictors of clinical recovery outcomes such as the polarity of relapse (e.g., Calabrese et al., 2004) but not on self-report measures or other mental health outcomes, such as personal recovery, QoL, or psychosocial functioning. Resilience has been proven a potential moderator of health-related outcomes, such as social functioning, in patients with BD (Bozikas et al., 2018). Nevertheless, to date, there has been no research focusing on the mechanisms or processes through which resilience might modify the damaging effects of bipolar mood episodes. Our present study aims to tackle this issue, by exploring the possible moderating role of resilience factors between bipolar mood episodes and health outcomes in BD. Thus, further studies are needed that delve into the relationship between resilience, BD mood episodes, and positive health outcomes. More research is needed to better understand the complex clinical course of BD and why some individuals with the same diagnosis report different health outcomes, which may be explained by the possible protective role of resilience factors. Shedding more light on the specific ways in which resilience might interact with bipolar mood episodes to improve individuals’ mental health outcomes could aid in the prevention of the negative effects of bipolar episodes. Therefore, this study aimed to explore whether health outcomes (i.e., QoL, personal recovery, work and psychosocial functioning) differ as a function of a person’s bipolar mood episode. In addition to that, we also analyzed whether resilience factors predicted better health outcomes depending on bipolar mood episodes. First, we expected that individuals experiencing bipolar mood episodes of (hypo)mania and depression would present worse QoL, personal recovery, and functioning in contrast with those experiencing euthymic phases. Second, we hypothesized that specific resilience domains would have different moderating effects concerning each bipolar episode and associated health outcomes. Participants The participants were recruited from nine public mental health services in the Basque Country (Spain) and non-governmental national BD associations. Inclusion criteria were having a diagnosis of BD confirmed by their therapist according to criteria of the Diagnostic and Statistical Manual of Mental Disorders (APA, 2000), being aged between 18 and 65 years, and being sufficiently fluent in Spanish. Exclusion criteria were having a clinically serious multi-organic disorder, acute psychosis, or cerebral organic deterioration that would prevent them from understanding the measures. Clinicians referred patients who met the previous study criteria to the researchers so that they could be requested to participate in the study. According to DSM-5 criteria, the mixed episode category is no longer considered to have diagnostic purposes (APA, 2013). Therefore, participants experiencing a mixed episode, according to the Spanish version of the Internal States Scale (ISS; Ruggero et al., 2004), were removed from the sample. The distinction between BD-I and BD-II was only made available by the therapist for a minority of the participating patients, leading to excluding these data from the analyses. Initially, 113 individuals diagnosed with BD were included in the study, but 16 participants were removed for meeting the exclusion criteria of being in a mixed bipolar state. Thus, a total of 97 individuals (63.90% female, mean age = 45.02 years, SD = 10.66, range 19-65) took part in the study. All participants self-completed sociodemographic and clinical data (see Table 1). There were no significant differences in any of the sociodemographic variables of age, F(2, 94) = 1.60, p = .21; gender distribution, χ2(2) = 0.22, p = .89; marital status, χ2(8) = 11.90, p = .16; educational level, χ2(10) = 10.08, p = .43; or employment status, χ2(4) = 4.08, p = .28, between the groups of individuals with depression, (hypo)mania and euthymia. Sociodemographic and clinical data are presented in Table 1. Table 1 Sociodemographic and Clinical Data 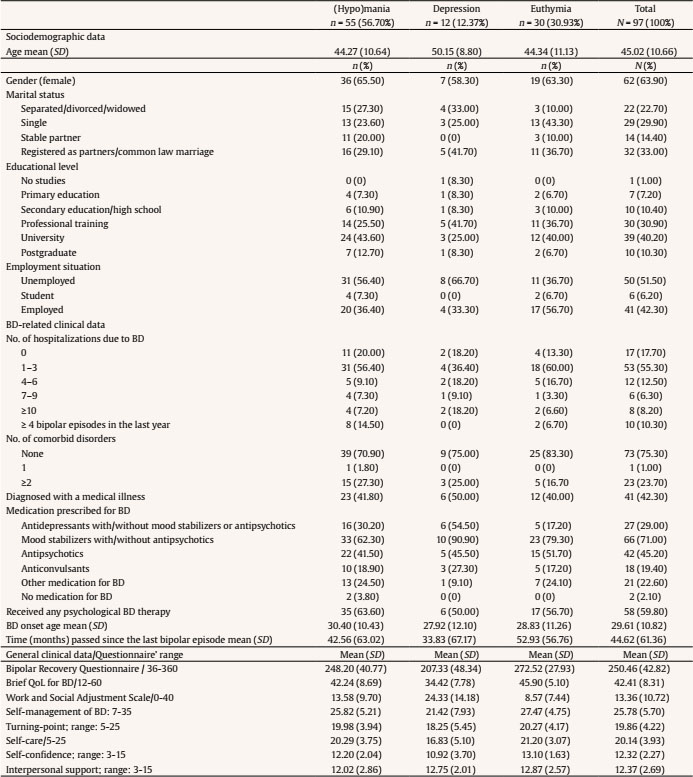 Measures Internal States Scale (ISS). The ISS (Bauer et al., 2000) includes 15 self-report items that are designed to discriminate co-occurring manic and depressive symptoms among people diagnosed with BD. It is composed of four indexes: Activation, Depression, Wellbeing, and Perceived Conflict. We adjusted the time framework of the Spanish version (Ruggero et al., 2004) to the last two weeks and adapted the original Visual Analogue Scale (VAS) to a 10-point Likert-type scale that ranges from 1 (not at all/rarely) to 10 (very much so/much of the time) for simplicity. The scores from the first two indexes (Activation and Depression) were used to indicate whether participants were currently experiencing a euthymic (n = 30), (hypo)manic (n = 55), or depressed (n = 12) mood state, as indicated by the authors (Bauer et al., 2000). In the present study, Cronbach’s alphas were appropriate (αactivation = .86, αdepression = .71). Resilience Questionnaire for Bipolar Disorder (RBD). This questionnaire was developed to measure resilience in BD (Echezarraga et al., 2017), based on a previous qualitative study (Echezarraga, Las Hayas et al., 2019). The RBD consists of five domains of resilience that are specific to BD: (1) Self-Management of BD, which refers to a sense of personal agency in the strategies used to manage the disorder; (2) Turning-Point, consisting of a moment of feeling committed to moving out of their current adversities; (3) Self-Care, which deals with taking care of one’s mental health through a balanced lifestyle; (4) Self-Confidence, consisting of maintaining attitudes of self-reliance and self-respect; and (5) Interpersonal Support, described as feeling cared for and loved by significant others. Each of these BD-specific resilience factors has shown unique direct and indirect effects in the explanation of recovery from BD (Echezarraga et al., 2018), indicating that different dimensions of resilience are worth considering separately when analyzing their indirect roles. The questionnaire consists of 23 items that are rated on a five-point Likert-type scale ranging from 1 (strongly disagree) to 5 (strongly agree). In the present study, Cronbach’s alpha coefficients for the RBD subscales were .89 for Self-Management of BD, .81 for Turning-Point, .84 for Self-Care, .78 for Self-Confidence, and .74 for Interpersonal Support. Brief Quality of Life in Bipolar Disorder (Brief-QoL.BD). We used the Spanish version (Morgado et al., 2015) of the Brief-QoL.BD (Michalak & Murray, 2010). It is a BD-specific self-report of QoL with 12 items and one total score. The items are rated on a five-point Likert-type scale ranging from 1 (strongly disagree) to 5 (strongly agree). The Cronbach’s alpha in the present study was .86. Bipolar Recovery Questionnaire (BRQ). It is a 36-item BD-specific self-report questionnaire that assesses personal recovery (Jones et al., 2013). Echezarraga et al. (2017) translated the BRQ from English to Spanish, also adapting the original VAS to a 10-point Likert-type scale that ranges from 1 (strongly disagree) to 10 (strongly agree). In the present study, Cronbach’s alpha was .90. Work and Social Adjustment Scale (WSAS). It is a self-report measure of the experiential impairment caused by an identified problem in several areas of daily-life functioning (e.g., ability to work, social leisure, and close relationships). It is composed of five items that are rated on a nine-point scale ranging from 0 (not at all) to 8 (very severely), where higher scores indicate higher impairment in work and psychosocial adjustment attributable to an identified problem (Mundt et al., 2002). We used the Spanish validation that adapted the WSAS to BD (Echezarraga, Calvete et al., 2019). In the current study, Cronbach’s alpha was .86. Procedure The study received approval from the Clinical Research of Basque Country’s Ethics Committee (Spain) (Internal code: [masked for review]). Participants completed the questionnaires in their mental health center, at their homes, or online. All participants signed an informed consent form before completing the assessment. Statistical Analyses Statistical analyses were performed on IBM SPSS Statistics for Windows (Version 26). Normality was tested by means of Kolmogorov-Smirnov test. Accordingly, non-parametric correlations were analyzed. Multiple regression analyses were performed to evaluate the predictive role of each resilience domain and bipolar mood type for three separate mental health outcome variables: QoL, personal recovery, and work and psychosocial functioning impairment. Separate multiple regression analyses were performed for each mental health outcome variable and each resilience domain. The bipolar episode was indicated with dummy coding for (hypo)mania and depression, and with euthymia set as the reference category. Thus, to build the model, firstly, resilience domains and bipolar episodes were included (Step 1). Then, to analyze the moderating role of each resilience domain in the relationship between bipolar mood episodes and mental health outcomes, the interaction terms (“Hypo)mania x Resilience” and “Depression x Resilience” were entered (Step 2). Spearman’s bivariate correlations are reported in Table 2. The higher effect sizes for BD-related clinical variables were found for the number of comorbid disorders and time passed (in months) since the last bipolar episode with resilience factors and with health-related outcomes (i.e., QoL, personal recovery, and impairment in work and psychosocial functioning). Nevertheless, as these effect sizes were small to medium (Rs = .19-.40), we did not include them as covariates in the first stage of regression analyses. Table 2 Bivariate Correlation Coefficients between Study Variables 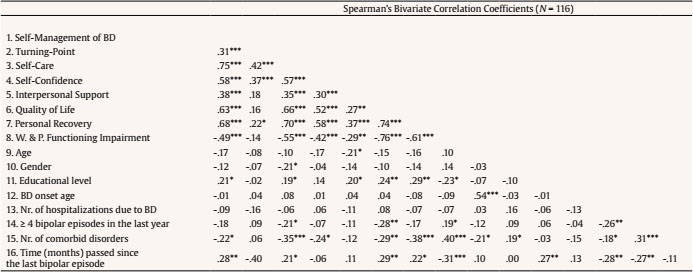 Note. Abbreviation W. & P. functioning impairment = work and psychosocial functioning impairment. *p ≤ .05, **p ≤ .01, ***p ≤ .001. As shown in Table 3, (hypo)manic and depressive mood episodes, in contrast to the euthymic phase, were negatively associated with QoL and personal recovery, and positively associated with work and psychosocial functioning impairment. The resilience domains of self-management of BD and self-care were positively associated with personal recovery but had no significant relationship with the other mental health outcomes. Table 3 Multiple Regression Analyses Evaluating the Moderating Role of Resilience in the Relationships between (Hypo)manic and Depressive Mood States and Quality of Life, Personal Recovery and Work and Psychosocial Functioning Impairment 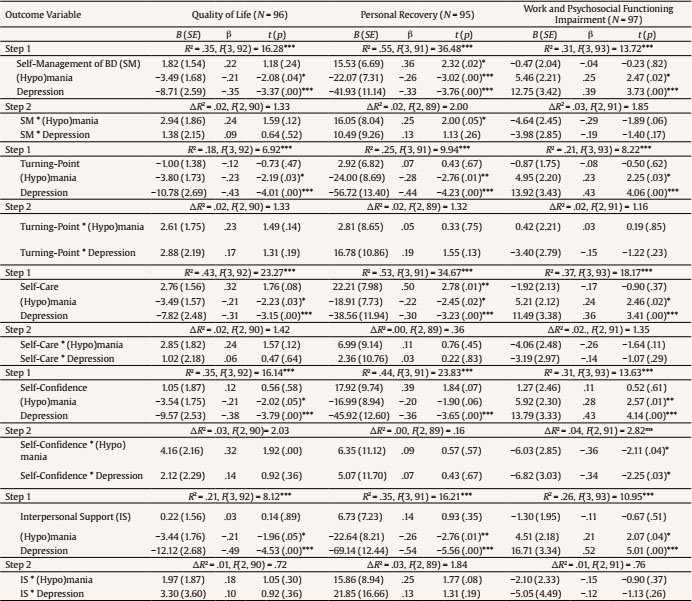 *p ≤ .05. **p ≤ .01. ***p ≤ .001. The interaction between being in a (hypo)manic episode and self-management of BD significantly predicted better personal recovery (see Table 3). Figure 1a presents the moderating role of self-management of BD in the relationship between (hypo)manic mood (compared to euthymic phase) and personal recovery. Figure 1a shows that the negative association between a (hypo)manic episode and personal recovery is weakest when levels of self-management of BD are higher. Besides, the interactions between (hypo)mania/depression and self-confidence significantly predicted work and psychosocial functioning impairment (see Table 3). As shown in Figures 1b and 1c, the positive association between (hypo)mania/depression and work and psychosocial functioning impairment are weakest when self-confidence is higher. There was also a marginally significant (p = .06) interaction term between self-confidence and (hypo)mania in the model predicting QoL (see Table 3). The present study shows that being in a (hypo)manic or depressive mood episode, compared to a euthymic phase, was associated with lower QoL and personal recovery, and higher work and psychosocial functioning impairment. This is consistent with previous studies finding that bipolar episodes—both (hypo)manic and depressive—have adverse effects on QoL (Votja et al., 2001), and functioning (Rosa et al., 2010), and that depressive episodes predict worse personal recovery (Dodd et al., 2017). The results of the present study also indicate that certain aspects of BD-specific resilience can moderate the negative effects of BD mood episodes on wellbeing. The self-confidence dimension of resilience was the most prominent moderator in the relationship both between hypo(mania) and depression and work and psychosocial functioning impairment. The positive associations between depression and hypo(mania) and functional impairment were weakest when participants reported high scores on self-confidence. In a previous qualitative study, bipolar individuals who were functioning outstandingly well also indicated that self-efficacy strategies moderated the disorder’s damaging effect on their functioning (Michalak et al., 2007). Especially, to improve work and psychosocial functioning, it was key to keep self-confidence high while in (hypo)manic episodes and to increase it while in depressive episodes. Therefore, self-confidence would be an aspect to try to keep track of, especially in the previous phases of (hypo)mania or during it. A similar effect, although marginally significant, was observed for the negative association from the interaction between self-confidence and hypo(mania) to QoL. Moreover, the BD-self-management domain of resilience moderated the negative association between (hypo)mania and personal recovery. Individuals in a (hypo)manic episode who scored high in self-management of BD obtained higher personal recovery scores compared to those who scored low in self-management. However, this resilience domain was not associated with personal recovery for participants in a euthymic phase. According to previous literature, self-management and self-care (i.e., sleep, rest, exercise, and diet) are wellbeing strategies that help people with BD to self-manage their symptoms (Miklowitz, 2008; Russell & Browne, 2005; Suto et al., 2010). Therefore, self-management strategies focusing on the core areas impaired by the (hypo)manic episode could be of great relevance to enhance personal recovery. In the current study, the resilience domain of BD-self-management predicted better personal recovery for those in a (hypo)manic episode, in contrast with those in a euthymic phase. This might be surprising at first, as self-management has been positively associated with wellbeing in people diagnosed with BD. However, resilience involves many processes that are deployed when the adversity is strong enough to imply a significant threat to healthy functioning (Riley & Masten, 2005). Thus, this resilience domain works better when the symptomatology is highly pronounced in contrast to when there are no symptoms or they are less threatening to health. Figure 1 Moderating Roles of Self-management of BD and Self-confidence between (Hypo)manic and/or Depressive State and Personal Recovery or Functional Impairment. 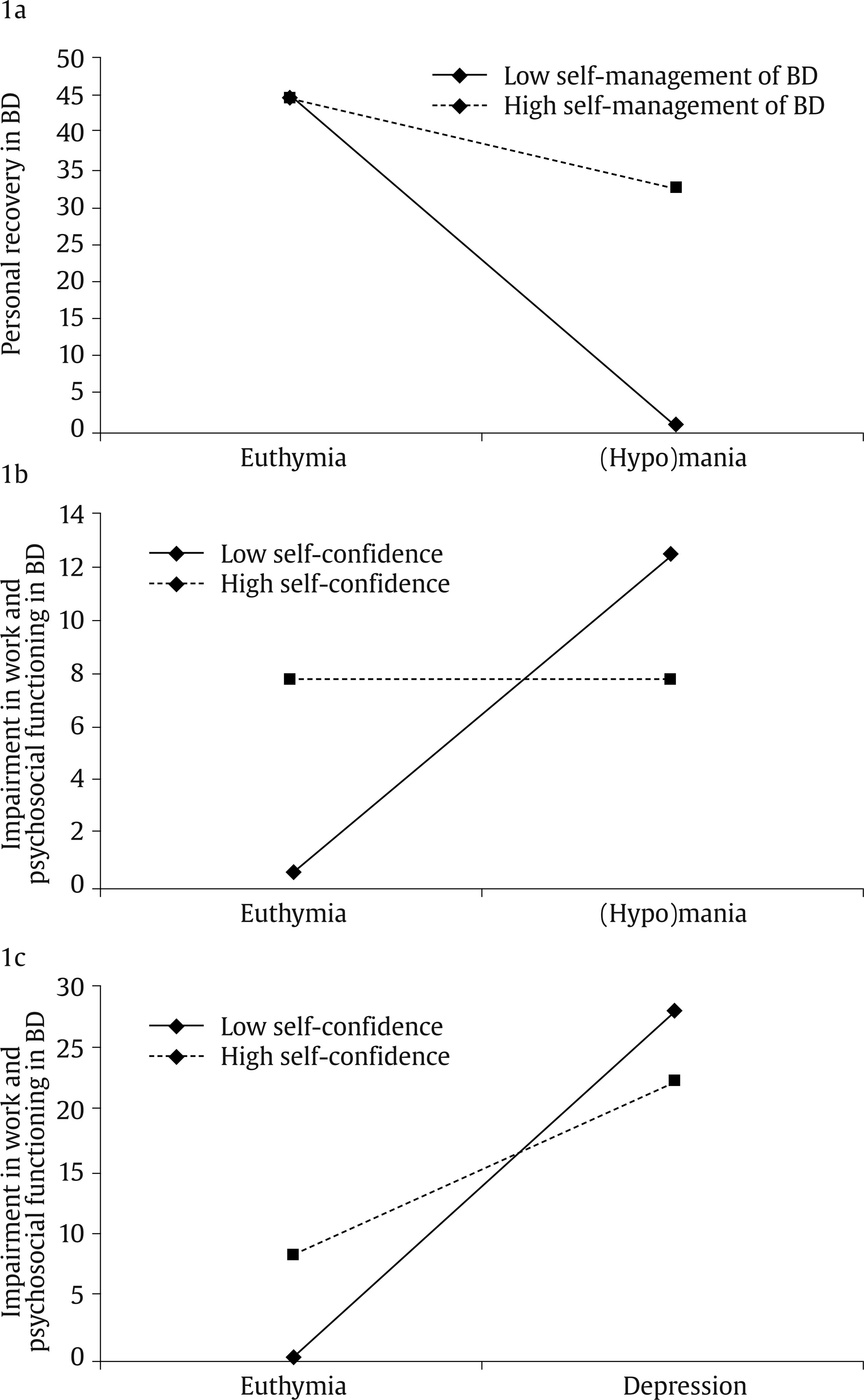 Subjects with BD may overestimate their self-confidence and self-management during (hypo)manic episodes and may underestimate them during depressive episodes. For example, subjects in a (hypo)manic episode mistakenly perceive that they have greater BD self-management capacity, and feel that they are more capable and self-sufficient to cope successfully with the difficulties associated with BD (Echezarraga, Las Hayas et al., 2019). However, the reality may not be a real increase in their self-management capacity, but an exaggerated perception of their capacity as a consequence of their (hypo)manic episode. Alternatively, resilience, specifically self-confidence and self-management of BD, may have been generated in individuals who, due to the experienced course of their disorder, could pay more attention to the energy drain, the risks, and impairments from hypomanic episodes—such as their possible escalation into mania—, which could lead them to feelings of shame and guilt (Fletcher et al., 2013). We propose that the knowledge—based on their previous experience—of the detrimental effects that bipolar episodes may imply for their mental health and lives may prevent attenuating the forthcoming (hypo)manic episodes in patients with high self-management of BD. Notwithstanding, bidirectional associations between the perception of self-confidence and self-management of BD and bipolar episodes should be especially considered in long-term functional impairment and QoL outcomes. Finally, both BD-self-management and self-care were associated with higher scores on personal recovery. This finding is congruent with previous studies demonstrating that resilience is related to personal recovery (Echezarraga et al., 2018). Similarly, people with BD have indicated that illness management strategies are a crucial factor for smooth functioning despite their disorder (Michalak et al., 2007). Resilience was not directly associated with QoL or with work and psychosocial functioning impairment, in contrast to previous findings (Bozikas et al., 2018; Hofer et al., 2017). It should be noted that the present study used a BD-specific resilience measure that allowed us to analyze the differential effects of separate resilience components in syndromic patients, thereby advancing knowledge of protective factors during bipolar episodes, unlike previous research analyzing generic resilience in subsyndromal bipolar patients (Bozikas et al., 2018; Hofer et al., 2017). The study is not exempt from limitations. We did not ensure the diagnosis of patients coming from non-governmental national BD associations with a clinical interview, and we did not distinguish between participants’ bipolar diagnosis type (i.e., BD-I or BD-II). Bipolar mood episodes were determined based on self-rated internal symptomatic state, which may have been influenced by patients’ current mood bias (Judd et al., 2005), and thus not following the same clinician-assessed criteria for categorization within a certain bipolar episode. For example, individuals experiencing (hypo)mania may have underestimated their vulnerabilities and overestimated their mental health status and resilience levels (Fletcher et al., 2013). Also, this study did not assess the type of BD treatment participants were receiving or whether they had comorbid psychiatric diagnoses. Despite of the fact that the study relies exclusively on self-reported measures, in the absence of enough physician-administered assessments of symptomatic state, previous studies have provided similar findings for clinician-versus patient-reports of patients’ health-related outcomes (Votja et al., 2001). In fact, there appears to be a correspondence between patients’ self-estimation of their internal symptomatologic state and their clinical recovery in terms of symptom severity and functioning impairment (e.g., Jones et al., 2006). Patients’ subjective perspective is also of interest. Another limitation was the high number of analyses carried out, given the small size of the sample. Forthcoming research should replicate the study with larger samples. Future studies should include BD-related variables, such as the number of episodes, comorbidity, and illness duration, as possible covariates to explore the associations between BD mood episodes and QoL, personal recovery, and impairment in work and psychosocial functioning. Forthcoming studies should obtain more homogeneous groups for each bipolar mood state category, which might increase the statistical power. In addition, in the current study, living with BD was considered a stressful experience per se, as it impacts all life areas, such as work and psychosocial functioning. Nonetheless, for a more precise evaluation, future studies might also include a measure of stress perception to control for its effect. Finally, note that the cross-sectional methodology prevents us from inferring causal and predictive relationships. The findings of the present study support the controversial fact that (hypo)manic episodes are not synonymous with increased wellbeing. In fact, both (hypo)manic and depressive mood states predicted worse QoL, personal recovery, and psychosocial functioning. Furthermore, by providing evidence of protective factors that may contribute to the improvement of the illness course (i.e., salutogenic approach), we complement the pathogenic focus of previous studies that have investigated factors precipitating bipolar episodes (e.g., Proudfoot et al., 2011). Our results showed that resilience, especially self-management of BD, plays a protective role. Individuals may show better treatment adherence if they feel they have more control over the management of their disorder. For example, individuals may be encouraged to increase self-management and self-confidence when considering risky behaviors and the severe impact of manic episodes. Moreover, considering the protective role of resilience together with the fact that the risk of relapse and hospitalizations increase with each episode (Goldberg et al., 2005), therapeutic interventions for BD could be more effective if they focus on resilience. Conflict of Interest The authors of this article declare no conflict of interest. Acknowledgements We appreciate the assistance from Ana Maria González-Pinto in sample recruitment. We are indebted to the people that gave their time to participate in this study. Cite this article as: Echezarraga, A., Calvete, E., Orue, I., & Las Hayas, C. (2022). Resilience moderates the associations between bipolar disorder mood episodes and mental health. Clínica y Salud, 33(2), 83-90. https://doi.org/10.5093/clysa2022a8 References |
Cite this article as: Echezarraga, A., Calvete, E., Orue, I., & Hayas, C. L. (2022). Resilience Moderates the Associations between Bipolar Disorder Mood Episodes and Mental Health. ClĂnica y Salud, 33(2), 83 - 90. https://doi.org/10.5093/clysa2022a8
a.echezarraga@deusto.es Correspondence: a.echezarraga@deusto.es (A. Echezarraga).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
Clinical and Health is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License








