


Gender Differences in Patients with Substance Use Disorder and Physical/Sexual Abuse: A Preliminary Study
[Las diferencias de gĂ©nero en pacientes con trastorno por consumo de sustancias y abuso fĂsico/sexual: un estudio preliminar]
Begoña Haro1, 2, Javier Fernández-Montalvo1, 2, Alfonso Arteaga1, 2, José J. López-Goñi1, and 2
1Universidad PĂşblica de Navarra, Spain; 2IdiSNA, Instituto de InvestigaciĂłn Sanitaria de Navarra, Spain
https://doi.org/10.5093/clysa2023a12
Received 3 January 2023, Accepted 3 May 2023
Abstract
Aim: To explore the differential characteristics in sociodemographic variables, severity of consumption, psychopathological symptomatology, life maladjustment, trauma characteristics, and post-traumatic stress symptomatology between women and men who seek treatment for substance use disorder (SUD) and have experienced lifetime physical and/or sexual abuse. Method: The sample consisted of 26 women and 31 men who had experienced physical/sexual abuse and sought treatment for SUD. Results: Women had been victims of sexual abuse in a significantly higher percentage than men. Women presented a significantly higher frequency of revictimization to another traumatic event and a significantly higher presence of avoidance symptoms than men. Conclusions: This study supports the existence of a more severe profile in women than in men with SUD who have experienced lifetime physical and/or sexual abuse. Consequently, gender-related trauma-informed practice in SUD treatment programmes should be promoted. More research in this field is needed, as this is a preliminary study.
Resumen
Objetivo: Explorar las diferencias de género en distintas variables (sociodemográficas, gravedad del consumo, sintomatología psicopatológica, inadaptación a la vida cotidiana, características del trauma y sintomatología de estrés postraumático) en pacientes que acuden a tratamiento por trastorno por consumo de sustancias (TCS) y han sufrido abuso físico y/o sexual. Método: La muestra estuvo compuesta por 26 mujeres y 31 hombres que habían sufrido abuso físico y/o sexual y buscaban tratamiento para TCS. Resultados: Las mujeres habían sido víctimas de abuso sexual en un porcentaje significativamente mayor que los hombres. Además presentaban una frecuencia significativamente mayor de revictimización a otro evento traumático y una presencia significativamente mayor de síntomas de evitación que los hombres. Conclusiones: El estudio confirma la existencia de un perfil más grave en las mujeres que en los hombres con TCS que han sufrido abuso físico y/o sexual a lo largo de la vida. En consecuencia, se debe promover la atención informada sobre el trauma con perspectiva de género en los programas de tratamiento del TCS. Dada la naturaleza preliminar de este estudio, se necesita más investigación en este campo.
Palabras clave
Trastorno por consumo de sustancias, Abuso fĂsico y/o sexual, PsicopatologĂa, Diferencias de gĂ©nero, EvaluaciĂłnKeywords
Substance use disorder, Lifetime abuse, Psychopathology, Gender differences, AssessmentCite this article as: Haro, B., Fernández-Montalvo, J., Arteaga, A., & López-Goñi, J. J. (2023). Gender Differences in Patients with Substance Use Disorder and Physical/Sexual Abuse: A Preliminary Study. ClĂnica y Salud, 34(3), 123 - 130. https://doi.org/10.5093/clysa2023a12
Correspondence: begona.haro@unavarra.es (B. Haro).
The development of post-traumatic symptomatology is one of the main consequences of suffering physical and/or sexual abuse (Campbell et al., 2016; Olaya et al., 2015). Gender differences in suffering different types of potentially traumatic events and in the derived consequences have been well established (Armstrong et al., 2018; Christiansen & Hansen, 2015; Mitra et al., 2021; Tolin & Foa, 2006). Overall, men suffer a higher number of lifetime traumatic events than women. Moreover, the types of traumatic events experienced by men vary. Specifically, men present a higher proportion of accidents, robberies, and war consequences than women, whereas women are victims of sexual abuse and childhood abuse in a higher proportion than men (Tolin & Foa, 2006). On the other hand, women present greater psychopathological consequences than men, such as depression, anxiety or post-traumatic stress disorder (PTSD; Armstrong et al., 2018). There is evidence for a link between having experienced any type of abuse and the development of problematic substance use (Afifi et al., 2012; Bailey et al., 2020; Haller & Chassin, 2014; Mesa-Gresa & Moya-Albiol, 2011; Proctor et al., 2017). This relationship has been traditionally explained by self-medication theory, which proposes the use of substances as a coping strategy to deal with the consequences of traumatic experiences (Khantzian, 1997). Furthermore, 18% to 53.7% of patients who seek treatment for substance use disorder (SUD) present a history of physical abuse, and 9.2% to 22.7% have experienced lifetime sexual abuse (Daigre et al., 2015; Fernández-Montalvo et al., 2015; Grundmann et al., 2018; Potthast et al., 2014). Patients in SUD treatment programmes who have experienced histories of physical and/or sexual abuse present a more severe psychopathological profile (Daigre et al., 2015; Fernández-Montalvo et al., 2015; Haro et al., 2021; Lotzin, et al., 2016; Zaorska & Jakubczyk, 2019) and higher rates of treatment dropout (Brems et al., 2004; Daigre et al., 2015; Fernández-Montalvo et al., 2017) than those without histories of abuse. In addition, post-traumatic stress symptomatology seems to play an important role in SUD development and severity (Kok et al., 2015; Müller et al., 2015). This relationship has been widely studied in women (Bailey et al., 2019; Min et al., 2007; Smith et al., 2014; Sullivan et al., 2009; Ullman et al., 2005; Ullman et al., 2009; Ullman et al., 2013; Ullman & Sigurvinsdottir, 2015; Vaszari et al., 2011). However, gender differences in patients with SUD and lifetime physical and/or sexual abuse remain little explored given the scarcity of comparative studies with male samples (Danielson et al., 2009). Gender differences in the link between having suffered a potentially traumatic event and substance use have been found in the general population. For example, cumulative exposure to a potentially traumatic event has been associated with cannabis use and illicit drug use in women but not in men (Cunradi et al., 2020). Regarding patients in SUD treatment programmes, this differential profile has been studied in veterans (Livingston et al., 2021) and in persons with severe mental illness (Lipschitz et al., 2000; Sharif et al., 2020). Although little is known about gender differences in patients in treatment for SUD who have experienced physical and/or sexual abuse, Ouimette et al. (2000) recommended gender-related trauma-informed practice in SUD-treatments. Nevertheless, this research presented some specific limitations. For example, measure of physical and sexual abuse was based on one-item measures. The present study tries to improve this aspect, using more accurate measures. Thus, the main objective of this study was to explore the differential characteristics between women and men who seek treatment for SUD and have experienced physical and/or sexual abuse. The variables studied were sociodemographic aspects, substance motivating treatment, severity of consumption, number of previous SUD treatments, psychopathological symptomatology, everyday life maladjustment, type of abuse, trauma characteristics and consequences, post-traumatic stress symptomatology, and diagnosis. In comparison to the study of Ouimette et al. (2000), the trauma-related variables were explored using a more in-depth interview. Based on the few previous studies, the primary hypothesis of this study is that women will present a more severe profile in most of the variables studied and a higher prevalence of sexual abuse than men. Participants The initial sample consisted of 496 patients seeking treatment for SUD in the “Proyecto Hombre Navarra and ANTOX” addiction programmes in Navarra, Spain between February 2017 and June 2019. These programs have a cognitive behavioural basis and are geared towards abstinence. Study inclusion criteria were as follows: a) meeting the diagnostic criteria for SUD based on the DSM-5 (American Psychiatric Association, 2013); b) having experienced physical and/or sexual abuse; c) being older than 18 years old; d) receiving SUD treatment; and e) giving consent to participate in the study. The exclusion criteria were a) presenting serious mental illness that made it inadvisable to participate in the study (e.g., psychotic disorders); and b) not having knowledge of the Spanish language. Based on these criteria, 57 patients were selected for the study (11.5% of the initial sample). Of these subjects, 54.4% (n = 31) were men, and 45.6% (n = 26) were women. The average age of the final sample was 41.5 years (SD = 11.8). About half of the participants were single (47.4%, n = 27), had secondary studies (50.9%, n = 29), and were unemployed (56.1%, n = 32). The main substance that motivated treatment was alcohol in 45.1% (n = 25) of the final sample, followed by cocaine (22.8%, n = 13), poly consumption (21.1%, n = 12), and other substances (12.3%, n = 7) as heroin, cannabis, etc. The remaining patients were excluded for not having experienced lifetime abuse (n = 439). Two previous studies were done with part of this sample (Haro et al., 2021; López-Goñi et al., 2021). Measures and Variables The EuropASI (Kokkevi & Hartgers, 1995; Spanish version by Bobes et al., 1996) is the European version of the Addiction Severity Index (ASI; McLellan et al., 1980). This tool assesses the need for treatment in patients with SUD in seven different areas: (a) general medical condition, (b) employment and financial situation, (c) alcohol consumption, (d) use of other drugs, (e) legal problems, (f) family and social relationships, and (g) psychological state; scores ranging from 0 (no problem) to 9 (extreme problems). Interviewer Severity Rates (ISRs), which are directly related to the severity of consumption (López-Goñi et al., 2012), were used. Moreover, some items of the EuropASI were used to obtain specific information about the presence of psychopathological problems (psychiatric scale: items 3, 4, 6, 7, 8, 9, 10, and 10A). Thus, the variables derived from the interview considered in this study were: substance motivating treatment, the seven areas of the EuropASI, number of previous SUD treatments, depressive problems, anxiety problems, hallucinations, violence problems, suicidal ideation and attempts, and previous psychopharmacological treatments. For the assessment of lifetime physical and/or sexual abuse, two specific items from the family/social area of the EuropASI were used: 18B (“Has anyone ever physically abused you?”) and 18C (“Has anyone ever sexually abused you?”). The short-term test-retest reliabilities of the ASI severity ratings have been reported to be greater than or equal to .92 for all domains in McLellan et al. (1985). The Symptom Checklist (SCL-90-R) (Derogatis, 1992) is a self-report tool that assesses psychopathological symptoms in the last two weeks. It is composed of 90 items that are answered on a five-point Likert scale, from 0 (never) to 4 (more than seven days). This tool aims to assess the symptoms of psychological distress. It consists of nine primary symptom dimensions: somatization (e.g., headaches), obsession-compulsion (e.g., unwanted thoughts, words, or ideas that won’t leave your mind), interpersonal sensitivity (e.g., seeing people in a negative way), depression (e.g., feeling low in energy or slowed down), anxiety (e.g., suddenly scared for no reason), hostility (e.g., feeling easily annoyed or irritated), phobic anxiety (e.g., feeling afraid to go out of your house alone), paranoid ideation (e.g., feeling uneasy when people are watching or talking about you), and psychoticism (e.g., the idea that someone else can control your thoughts); and three global indices of severity: the Global Severity Index (GSI), which reflects overall symptom severity; the Positive Symptom Distress Index (PSDI), which indicates symptom intensity; and the Positive Symptom Total (PST), which includes the number of items answered with a score different from 0. In this sample the internal consistency ranges from .70 to .90. The Maladjustment Scale (Echeburúa et al., 2000) reveals how each patient is currently affected in six different areas of everyday life: labour, social, leisure, partner, family and general (e.g., “because of my current problems, my usual social life has been affected...”). This scale evaluates maladjustment in each area and it ranges from 0 (nothing) to 5 (extremely) on a six-point Likert scale. The total scale range is 0-30. Higher scores indicate higher levels of maladjustment. In this sample the internal consistency is .94. The Severity Posttraumatic Stress Disorder Scale - Revised (EGS-R; Echeburúa et al., 2016) is a Spanish semi structured interview that evaluates the presence of PTSD and the severity of the symptoms. It is based on the diagnostic criteria of the DSM-5. It is composed of two parts: a) exposure to a traumatic event and b) severity and frequency of PTSD symptoms. It consists of 21 items scored from 0 (nothing/never) to 3 (extremely/5 or more times a week) on a four-point Likert scale. The variables evaluated were type of abuse, frequency of the traumatic event, previous treatments, exposure during childhood/adolescence, revictimization, physical sequalae, PTSD symptoms severity, and PTSD diagnosis. In addition, six items valorise the interference of trauma in different daily life areas. In this sample the internal consistency is .91. Procedure The ethics committees of the Universidad Pública de Navarra (code: PI-006/16), Proyecto Hombre Navarra (code: PHN2016-01), and ANTOX (code: A2017-01) approved the protocol for this study. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. All participants signed informed consent forms. Informed consent was obtained from all patients for being included in the study. All patients were interviewed by clinical psychologists specialized in the assessment and treatment of addictions and trauma. The assessment of the sample was carried out in two sessions at the beginning of the addiction treatment. Self-reports were completed in the presence and with the support of the interviewers. During the first session, sociodemographic data and physical and/or sexual abuse variables were screened as well as the EuropASI (Kokkevi & Hartgers, 1995; Spanish version by Bobes et al., 1996). The procedure to determine the EuropASI scores was the two-step methodology suggested by Bobes et al. (2008). In the first step, the scores of each area were calculated based on the interviewer’s judgement considering the patient’s answers. In the second step, once the interview with the patient had finished, the interviewer’s scores were reviewed by the intervention team, blind to the participant’s identity. If a discrepancy was observed, the intervention team discussed it until an agreement was reached. In the second session, the psychopathological and maladjustment consequences were assessed. An in-depth interview was carried out with patients who reported a history of physical and/or sexual abuse to confirm the traumatic event and evaluate the corresponding variables with the EGS-R (Echeburúa et al., 2016). The same researcher was in charge of these in-depth interviews. For individuals experiencing more than one traumatic event, the event with the most severe consequences on the patient was considered the principal type of abuse. The clinical judgment about the PTSD diagnosis was made considering the scores of the EGS-R (Echeburúa et al., 2016). When a doubt appeared, the researcher team discussed the symptomatology of the patient until reaching an agreement. Data Analysis Descriptive analyses were conducted for all variables. Bivariate analyses were performed using χ2 tests or Student’s t-tests for independent samples, depending on the nature of the variables analysed. The variance homogeneity was assessed in the case of the Student’s t-tests. Depending on the result of Levene’s test, the corresponding correction was used (Glass & Stanley, 1970). The t-test was used because data presented a random distribution (assessed by Runs test for randomness), and the size of the sample was higher than 40. The statistical analyses were two-sided. Effect sizes (Cohen’s d or Cramer’s V) for the analyses were provided. The interpretation of Cohen’s d was made following the next considerations: d < 0.20 (no effect size), 0.2 ≤ d < 0.5 (small effect size), 0.5 ≤ d < 0.80 (medium effect size) and d ≥ 0.80 (large effect size; Cohen, 1998). The interpretation of Cramer’s V was made according to Rea and Parker’s (1992) conventions: V ≤ .20 (small effect), .20 < V ≤ .60 (medium effect), and V > .60 (large effect). Statistical power post-hoc was calculated as a function of α = .05, the population effect size, and N. Scores above .80 are considered adequate for accepting the statistically significant (p < .05) differences. Regarding multivariate analyses, a logistic regression analysis (forward stepwise entry method) was conducted to determine which specific factors were the most important to differentiate between men and women. In this analysis, all the variables were included. Due the preliminary character of the study, the variable entry criterion was set to 0.05, and the variable retention criterion was set to 0.10. The proportion of the variance explained was calculated as Nagelkerke’s R2. Moreover, the Hosmer-Lemeshow test was used to assess the goodness of fit of this model (Hosmer & Lemeshow, 2013). A difference of p < .05 was considered significant. Statistical analysis were performed with the SPSS program (25.0) and G*Power 3 software (Faul et al., 2007). Comparisons of Sociodemographic, Severity of Consumption, and Psychopathological Variables by Gender There were no gender differences in sociodemographic characteristics (Table 1). Comparisons between men and women in severity of consumption and psychopathological characteristics are presented in Table 2. Statistically significant differences in the substance that motivated treatment were observed (χ2 = 6.0, p = .014), with a low effect size. Alcohol was the substance that motivated treatment in 43.9% (n = 25) of patients: 61.5% (n = 16) of women and 29% (n = 9) of men. Regarding addiction severity assessed by the EuropASI, men showed higher scores in drug use (t = 2.2, p < .033) and legal problem area (t = 2.6, p < .012) than women, with moderate effect sizes. Moreover, women presented a higher prevalence of previous psychopharmacological treatments than men (χ2 = 6.4, p = .014), with a low effect size. Regarding psychopathological variables assessed by the SCL-90-R, men obtained significantly higher scores on the hostility dimension (t = 3.3, p = .0002), with a large effect size. Table 1 Comparisons of Sociodemographic Characteristics by Gender 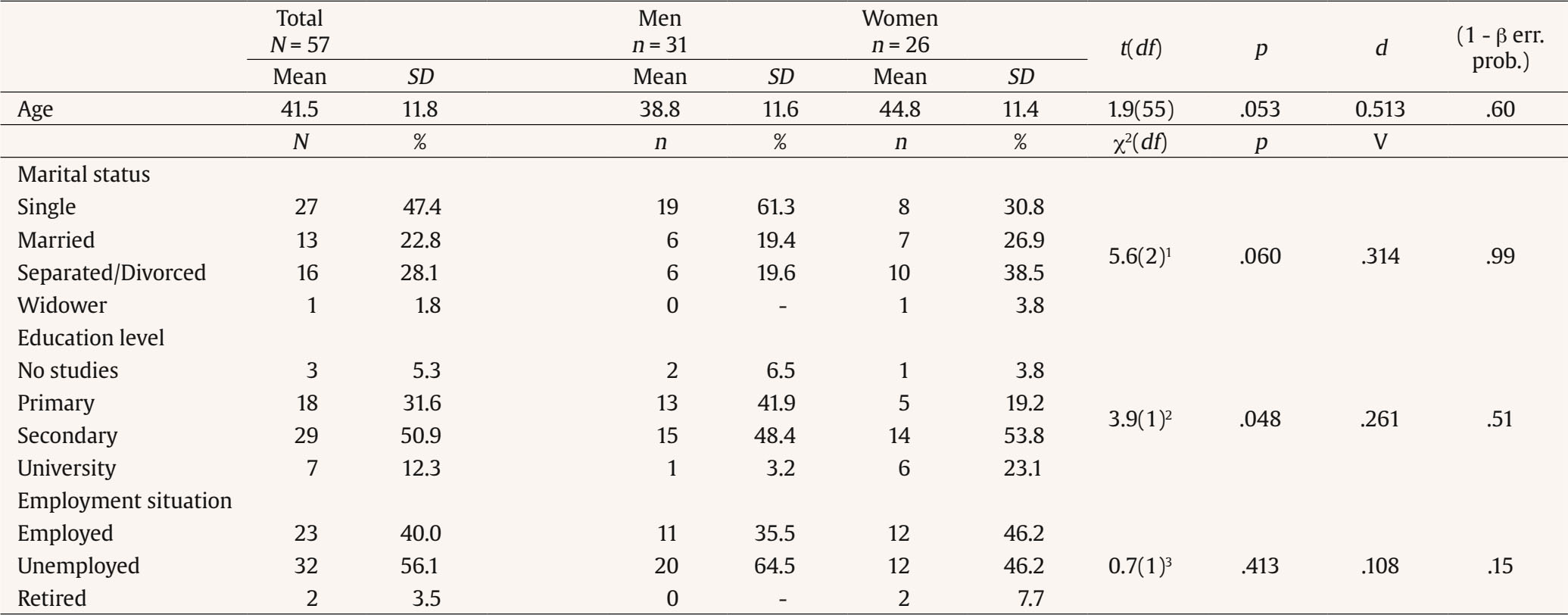 Note. 1In the χ2 analysis of marital status, the categories “separated/divorced” and “widower” have been joined. 2In the χ2 analysis of education level, the categories “no studies” and “primary”, as well as “secondary” and “university”, have been joined. 3In the χ2 analysis of employment situation, the categories “unemployed” and “retired” have been joined. Table 2 Comparisons of the Severity of Consumption and Psychopathological Characteristics by Gender 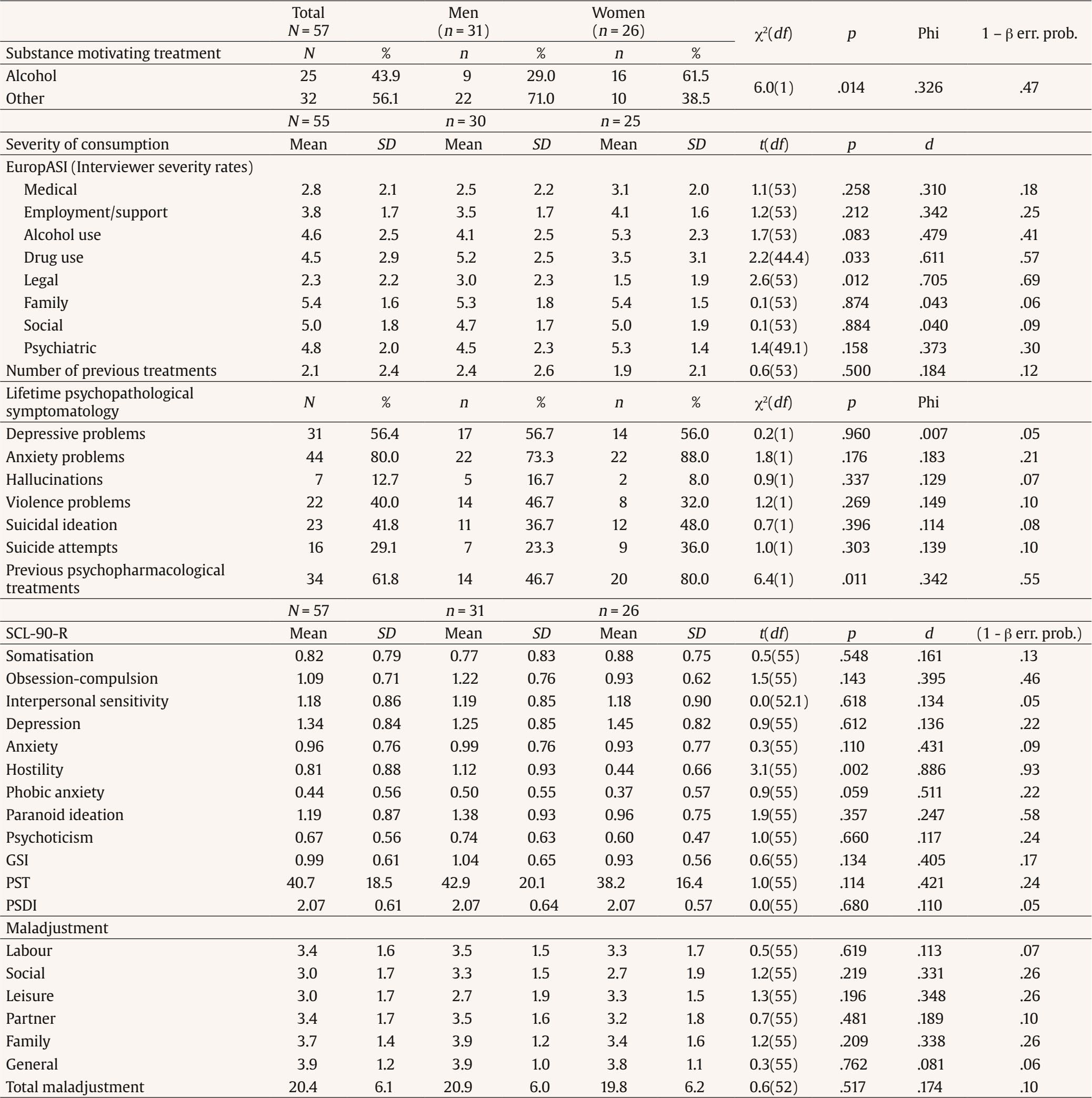 Note. SCL-90-R = Symptom Checklist; ISR = Interviewer Severity Rate; GSI = Global Severity Index; PSDI = Positive Symptom Distress Index; PST = Positive Symptom Distress. Comparisons of Trauma-related Variables by Gender Most patients had been victims of more than one traumatic event (n = 47, 82.5%) and had experienced the traumatic event during childhood or adolescence (n = 43, 75.4%), without gender differences. Moreover, 26.3% (n = 15) of the sample presented a diagnosis of PTSD. The results showed a differential profile in trauma-related variables between men and women (Table 3). Regarding the type of abuse, more women (n = 20, 76.9%) than men (n = 5, 16.1%) had experienced at least one event of sexual abuse, with a significant gender difference (χ2 = 21.2, p < .001) and a moderate effect size. Most of men had been victims of physical abuse (n = 26, 83.9%). On the other hand, women presented a higher frequency of revictimization to another traumatic event than men (χ2 = 15.0, p < .001), with a moderate effect size, and a higher presence of avoidance symptoms as a consequence of having experienced the traumatic event (t = 2.1, p < .037), with a moderate effect size. Regarding violence perpetration against people, men (80.6%, n = 25) presented a higher percentage than women (38.5%, n = 10), which was significantly different (χ2 = 10.6, p = .001) with a low effect size. Table 3 Comparisons of the Characteristics and Consequences of Traumatic Events by Gender 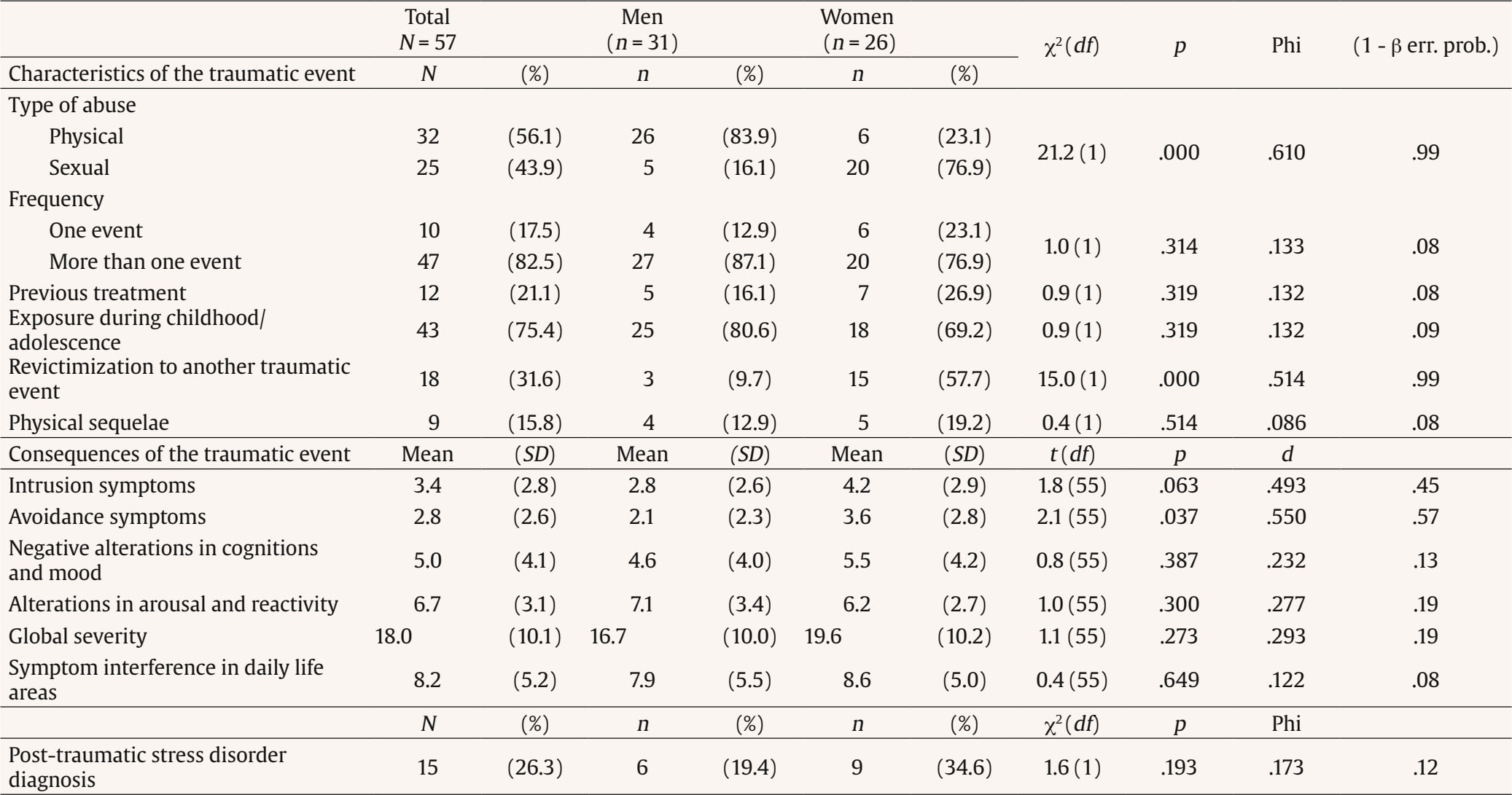 Variables Related to Gender The logistic regression analysis showed that the three variables that best differentiated women from men were having experienced sexual abuse, alcohol as the substance that motivated treatment, higher scores in depression and lower paranoid ideation scores (SCL-90-R). These three variables explained 79.6% of the variance and correctly classified 87.3% of the patients (Table 4). Table 4 Variables Related to Gender  Note. SCL-90-R = Symptom Checklist. This study supports the existence of a differential profile between women and men in treatment for SUD who have experienced lifetime physical and/or sexual abuse, similar to previous findings (Lipschitz et al., 2000; Livingston et al., 2021; Sharif et al., 2020). Specifically, as hypothesized, women presented a more severe profile than men regarding trauma characteristics and consequences. This more severe profile in women who have experienced trauma has also been reported in the general population (Cunradi et al., 2020), in people who use drugs (Mitra et al., 2021) and in patients with co-occurring SUD, such as veterans or patients with severe mental illness (Lipschitz et al., 2000; Sharif et al., 2020). The main contribution of this study is that these gender differences have been found in patients who seek treatment for SUD and who have suffered lifetime physical and/or sexual abuse. With regard to the severity of consumption and psychopathological characteristics, women presented alcohol as the substance that motivated treatment more frequently and more previous psychopharmacological treatments than men. Therefore, women with SUD and lifetime physical and/or sexual abuse seem to seek help for their psychopathological problems more frequently than men (Estancial et al., 2018; Simoni-Wastila, 2000), opposite to what usually happens in the addiction centres, where women face barriers in access to treatment (Taylor, 2010). However, they presented lower drug consumption and legal problems than men. These results obtained in patients with histories of abuse are in line with those found in general patients in SUD treatment (Fernández-Montalvo et al., 2014; Santos-de-Pascual et al., 2020). Regarding the characteristics and consequences of the traumatic event, women presented a greater presence of sexual abuse and a higher probability of revictimization to another traumatic event than men. In this sense, previous studies have shown that women who present lifetime sexual abuse and substance abuse have a higher probability of revictimization due to the effect of consumption (Filipas & Ullman, 2006; Klanecky et al., 2008; Ullman et al., 2009). Similar results were found in this study. One of the greatest predictors of chronification of psychopathological traumatic consequences is the use of avoidance coping strategies (Min et al., 2007), such as substance abuse (Shuai et al., 2022) and misuse of psychopharmacological treatments. This relationship has been traditionally explained by self-medication theory. It is one of the main explanations for the relationship between suffering a potentially traumatic event and the development of problematic substance use (Khantzian, 1997). In this study, women showed more severe avoidance symptoms and a higher rate of previous psychopharmacological treatments than men. Substance use could be a maladaptive coping skill related to the traumatic event. These specific characteristics could jeopardize SUD treatment progress in women. In this sense, other adaptative coping strategies should be provided to prevent dropout from SUD treatment (López-Goñi et al., 2021). From a multivariate perspective, women showed higher presence of lifetime sexual abuse, alcohol as the principal substance that motivated treatment compared with other drugs, higher scores in depression and lower paranoid ideation scores. Thus, the gender perspective is relevant in patients in SUD treatment who have experienced physical and/or sexual abuse. This study had some limitations. First, the size of the sample was limited. Future studies should replicate this research with larger samples. A larger sample would enable a deeper exploration of gender differences in trauma characteristics and consequences in patients receiving SUD treatment and a greater generalizability of the results. This is especially important in those variables in which a statistical power under .80 has been obtained (drug use and legal problems, symptom avoidance, psychopharmacological treatments). Second, this study included patients from only two treatment centres in Navarra, Spain, which might have introduced a bias that prevents us from generalizing the findings of the study to other contexts. Third, as this investigation was a cross-sectional study, a causal relationship cannot be established between having experienced physical and/or sexual abuse and the development of a substance use disorder. One strength of this study is that the participants presented two very specific conditions: SUD and lifetime abuse. These specific patients are difficult to find and recruit, especially women. This research fills a gap in scientific knowledge and provides a first step for future research. In summary, the gender perspective in patients in SUD treatment with lifetime abuse remains a neglected aspect that needs in-depth research. The results of this study provide valuable information to the field. Patients could benefit from integrated treatments that consider both problematic areas (Ouimette et al., 2000; Roberts et al., 2015; Simpson et al., 2017). As the results of this study suggest, this is very relevant for women due to their more severe profile compared to men. Trauma-informed practice in SUD treatment programmes should be promoted (Ouimette et al., 2000). This implies a paradigm shift in the culture of SUD treatment centres. First, it is necessary to recognize the differential profile of this population and its prevalence among SUD patients. And second, to apply specific interventions to address these differences and reduce the risk of revictimization (Substance Abuse and Mental Health Services Administration, 2014). In conclusion, the inclusion of a gender perspective practice in SUD treatments would benefit women who have suffered lifetime abuse. Conflict of Interest The authors of this article declare no conflict of interest. Acknowledgements The authors thank the staff of the “Proyecto Hombre Navarra” and “ANTOX” programmes for their help with assessing the clinical sample. Cite this article as: Haro, B., Fernández-Montalvo, J., Arteaga, A., & López-Goñi, J. J. (2023). Gender differences in patients with substance use disorder and physical/sexual abuse: A preliminary study. Clínica y Salud, 34(3), 123-130. https://doi.org/10.5093/clysa2023a12 Funding: This study was supported by a grant (code PSI2016-76511-R) from the Agencia Estatal de Investigación (AEI) of the Spanish Government and the Fondo Europeo de Desarrollo Regional of the European Union (FEDER, EU). C References |
Cite this article as: Haro, B., Fernández-Montalvo, J., Arteaga, A., & López-Goñi, J. J. (2023). Gender Differences in Patients with Substance Use Disorder and Physical/Sexual Abuse: A Preliminary Study. ClĂnica y Salud, 34(3), 123 - 130. https://doi.org/10.5093/clysa2023a12
Correspondence: begona.haro@unavarra.es (B. Haro).
Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
Clinical and Health is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License








