


Anxiety and parent’s beliefs about medication in primary pediatric health care
[La ansiedad y los problemas paternos con la medicación en asistencia pediátricaprimaria]
Antonio Fernández Castillo1 , María J. Vílchez-Lara2
1Univ. de Granada, Fac. Ciencias de la Educación, España ,2Virgen de las Nieves Univ. Hosp. Complex, Granada, España
https://doi.org/10.1016/j.clysa.2014.06.003
Abstract
The goal of the present study is to explore the relation between parents' anxiety and cognitive representations of medication in pediatric treatment of their children, seeking possible differences as a function of gender and age. A total of 1,772 parents of children attended in primary pediatric health care centers of the public health care system of Andalusia, Spain participated in this study. Of the sample, 25.1%were men and 74.9% were women. Negative beliefs about medicines were found to be associated with higher levels of anxiety in parents during primary pediatric health care. Among the variables studied, the beliefs in medication abuse predicted higher levels of anxiety. Intervention initiatives could substantially improve patients and their relatives' well-being during pediatric consultation, adherence to treatment, and lastly general satisfaction. Findings are discussed with reference to other authors, clinical implications, and the need of future research.
Resumen
El objetivo del presente estudio es explorar la relación entre la ansiedad paterna y las representaciones cognitivas sobre la medicación en el tratamiento pediátrico de sus hijos. Para ello, 1.772 padres de niños atendidos en centros de atención pediátrica del sistema público de salud de Andalucía participaron en este estudio. El 25.1% de la muestra eran hombres y el 74.9% mujeres. Se encontró que las creencias negativas acerca de los medicamentos se asociaron con mayores niveles de ansiedad en los padres durante la atención pediátrica. Entre las variables estudiadas, la creencia de abuso de la medicación fue la variable que predijo mayores niveles de ansiedad. Iniciativas adecuadas de intervención podrían mejorar sustancialmente el bienestar de los pacientes y sus familiares durante la consulta pediátrica, la adherencia al tratamiento e incluso la satisfacción general. Se discuten los resultados en relación con otros autores, las implicaciones clínicas y la necesidad de futuras investigaciones.
Beliefs about medication and medical treatments have been a topic of interest for health sciences for many years. Their relevance is associated with important aspects such as following instructions, adherence to treatment, or even the effectiveness of medical interventions (Perpiñá, MartĂnez, Belloch, Lloris, & Pellicer, 2009; Unni & Farris, 2011). In fact, negative beliefs about medication have been associated with 30 to 50% of ceasing to take medication or lack of adherence to treatment in diverse studies (Horne, Parham, Driscoll, & Robinson, 2009; Horne, Weinman, & Hankins, 1999).
A great number of theories from health psychology, such as the Theory of Planned Behavior, the Health Belief Model, or the Common Sense Self-regulatory Model of Illness, have been used to explain variations in adherence to medicines (Horne, & Weinman, 1998). However, neither the responsible variables nor the processes involved are completely known, partly due to the large differences, which may be a function of cultural background (Horne et al., 2004). The adherence promotion interventions are frequent and effective (Cortina, Somers, Rohan, & Drotar, 2013; Wu, et al., 2013). And, of course, noncompliance to drug therapy has been shown to increase mortality, admission to hospital, morbidity, as well as increasing costs, and this problem is very common (Bondesson, Hellström, Eriksson, & Höglund, 2009; Rasmussen, Chong, & Alter, 2007).
Two of the most frequently studied dimensions with regard to beliefs about the use and prescription of medication are the beliefs that patients and doctors abuse medication, and secondly, beliefs about the adverse and potentially harmful side effects of medication (Horne, 1997). It seems clear that people who hold a harmful view of medication will also believe that we overly trust medication, when there may be alternative treatments not based on drugs (Horne, 1997; Horne & Weinman, 1999). It is obvious that if a person believes that drugs are harmful, the probability of taking medicine decreases despite the doctor's indications (Mardby, Akerlind, & Jörgensen, 2007). In this sense, a significant association between belief in medicines and forgetfulness and carelessness about taking medications has also been found (Unni & Farris, 2011).
With regard to age, other authors have found that more advanced ages are associated with a stronger belief in the goodness of alternative medical treatments instead of conventional ones (Van den Bulck & Custers, 2009). And also, general beliefs about medicines remain stable over time, regardless of health status (Porteous, Francis, Bond, & Hannaford, 2010).
Regarding gender, there is a tendency towards no gender differences in beliefs (Horne et al., 2009; Kumar et al., 2008).
Anxiety and other emotional disorders and alterations, both in the family doctor's consulting office, in primary pediatric care, and in other health care contexts, have been studied for many years, in view of their significant presence and the importance of their psychological care (Fernández-Castillo & LĂłpez-Naranjo, 2006a; Mishina & Takayama, 2009; Sakolsky & Birmaher, 2008). With specific reference to pediatric care, emotional alterations have also been studied in other pediatric populations, for example, in children with severe diseases or from different cultural origins (Fernández-Castillo & VĂlchez-Lara, 2009a; Moitra & Armstrong, 2009), in hospitalized children (Fernández-Castillo, Sada-Lázaro, & VĂlchez-Lara, 2008; Fortier, Rosario, Martin, & Kain, 2010; Needle, O'Riordan, & Smith, 2009; Wray, Lee, Dearmun, & Franck, 2011), or in other areas of health care (Fernández-Castillo & VĂlchez-Lara, 2009b; Miklosi, Szabo, Martos, Galambosi, & Forintos, 2013). Emotional alterations in parents of sick children and even contagion and transmission of such alterations among parents and children have been frequently described (Fernández-Castillo & LĂłpez-Naranjo, 2006b; Herren, In-Albon, & Schneider, 2013). In recent years, anxiety has received more attention from investigators, despite the fact that it usually goes unnoticed in primary care (Chavira, Stein, Bailey, & Stein, 2004).
According to Spielberger (1966), state anxiety refers to an empirical process or reaction which is taking place now at a given level of intensity. It is characterized by subjective, consciously perceived feelings of apprehension and tension, accompanied by or associated with activation of the autonomic nervous system. Anxiety is generally due to the perception of a situation as threatening or potentially harmful and health care attention is a situation that can frequently provoke anxious reactions.
Some studies have found higher levels of anxiety in women than in men and in younger people than in older people, in diverse populations and in diverse dimensions of this variable, such as social anxiety or health anxiety (Caballo et al., 2008; Daig, Herschbach, Lehmann, Knoll, & Decker, 2009; MacSwain, et al., 2009). However, other studies focused on pediatric health care have found no differences between fathers and mothers in emotional alterations, such as stress during a child's hospitalization (Fernández-Castillo & López-Naranjo, 2006a).
Although emotional alterations and disorders such as depression and anxiety seem to be associated with noncompliance with medical instructions and treatments, it is not clear whether the belief about the treatment and the prescribed medication may be associated with differential levels of anxiety during consultation. Likewise, there are not many works focused on the study of this relation in pediatric primary care. Although the results in adults indicate that anxiety is not related to non-adherence to treatment (DiMatteo, Lepper, & Croghan, 2000), the study of a possible association between anxiety and negative beliefs about medication is still pending and it remains to be seen whether it is associated with problems of following health instructions and adherence to treatment.
In the present study, we proposed the following goals. Firstly, to determine the presence of anxiety and negative beliefs about medication in the sample of participants. Secondly, to explore the possible relation between negative cognitive representations of medication and anxiety in primary pediatric health care. Thirdly, to determine the existence of possible differences in beliefs about medication and anxiety in primary pediatric care as a function of sex and age. Fourthly, to explore the dimensions of the beliefs about medication studied and whether they predict different levels of anxiety in the sample of our study.
Method
Participants
In this study participants were a total of 1,772 parents of children attended in primary pediatric health care centers of the public health care system of Andalusia (Spain). Participants' age was between 17 and 67 years ( M = 33.58, SD = 6.919). Of the sample, 445 (25.1%) were men and 1,327 (74.9%) were women. All of them were randomly selected from among the parents of patients attended in 28 public primary pediatric health care centers from the provinces of Granada, AlmerĂa, JaĂ©n, and Málaga.
Inclusion criteria were voluntary participation in the study (with signed informed consent) and not having been attended previously on that day by the pediatrician. Exclusion criteria were specific circumstances that dissuaded, impaired, or prevented completing the assessment instruments, such as the presence of difficulties in the child that advised against parents' participation (children with limiting conditions, presence of intense pain, severe discomfort, or other difficulties, etc.), mental disability or inadequate educational level to understand the questionnaires, very poor comprehension of the Spanish language, or the expression of their refusal to participate in the study.
Procedure
An assessment interview was carried out with the parent/parents while they were waiting in the waiting room for consultation sessions.
To collect the data, the investigators contacted the participant primary pediatric health care centers and requested the pertinent authorizations. In all of them, the competent research-ethics committees assessed our study and accepted it in a report.
Then, the investigators visited the waiting rooms of the primary pediatric health care centers, requesting the collaboration of all the families that were waiting for pediatric attention.
The data was collected by means of an interview with the parents, in which the psychological assessment instruments were applied. The inventories were administered individually, with each parent responding separately.
All the families were informed about the research goals, the anonymous nature of their participation, and the confidentiality of their responses. They were also informed about the possibility of dropping out of the process of responding to the questionnaires at any time, and they were requested to sign an informed consent.
Measures
Demographic information . Each participant was asked about his/her age and sex.
Anxiety . All the participants filled out the latest Spanish version of the Spielberger's State-Trait Anxiety Inventory (STAI) (Spielberger, Gorsuch, & Lushene, 2002). The STAI (Spielberger, Gorsuch & Lushene, 1983) was designed to measure both state anxiety and trait anxiety, with two separate questionnaires. The Spanish version of the State Anxiety form of the STAI was administered to participants to measure their anxiety in a particular situation. This form contains 20 items with responses ranging from 0 ( hardly ever) to 3 (almost always).
The internal consistency of the Spanish version of the State Anxiety form in the original study was high: the Kuder-Richardson formula 20 (KR-20) was between .90 and .93, and the split-half reliability was .94 for the state form (Spielberger et al., 2002). Its convergent validity with other measures of anxiety was very satisfactory (Spielberger, Gonzalez, Taylor, Algaze, & Anton, 1978). Internal consistency of the STAI in the present sample was excellent (Cronbach's ? = .89).
Beliefs about medicines . To assess the parents' cognitive representation of medication in pediatric treatment of their children, we used the Spanish version (Beléndez-Vázquez, Hernández-Mijares, Horne, & Weinman, 2007) of the Beliefs about Medicines Questionnaire (BMQ) (Horne et al., 1999).
The BMQ is made up of two separate instruments, the BMQ-General and the BMQ-Specific. In this study we only used the general questionnaire. The BMQ-General was designed to assess cognitive representation of medication and is made up of 8 items rated on a five-point scale, ranging from 1 ( strongly disagree) to 5 (strongly agree ). The questionnaire includes two subscales, abuse and damage beliefs. The abuse scale is made up of items 1, 7, and 8, while the damage beliefs subscale is made up of items 2, 3, 4, 5, and 6. The instrument allows to obtain a general expression of beliefs, which considers the sum of the two subscales.
With regard to its psychometric properties, the study from the original design reached an alpha coefficient of .60 for the abuse scale and .51 for the damage scale (Horne et al., 1999), and the coefficients obtained in validity studies with a Spanish sample of chronic patients reached values of .69 for the abuse scale and .68 for the damage scale (Beléndez-Vázquez et al., 2007). In other language versions and with diverse populations the instrument also showed good internal consistency (Jónsdóttir et al., 2008; Mahler et al., 2009). In our case, Cronbach's alpha coefficient for the general scale was .81. Analysis of internal consistency of the diverse subscales yielded the following results: abuse, .70, and damage, .75.
Data Analysis
To analyze the data, in addition to the pertinent descriptive and frequency analyses, we conducted Pearson's correlational analysis, comparison of means, and multiple linear regression analysis. For all analyses, the level of significance was p < .05. The analyses were performed using the Spanish version of the statistical software SPSS, version 11.5.
Results
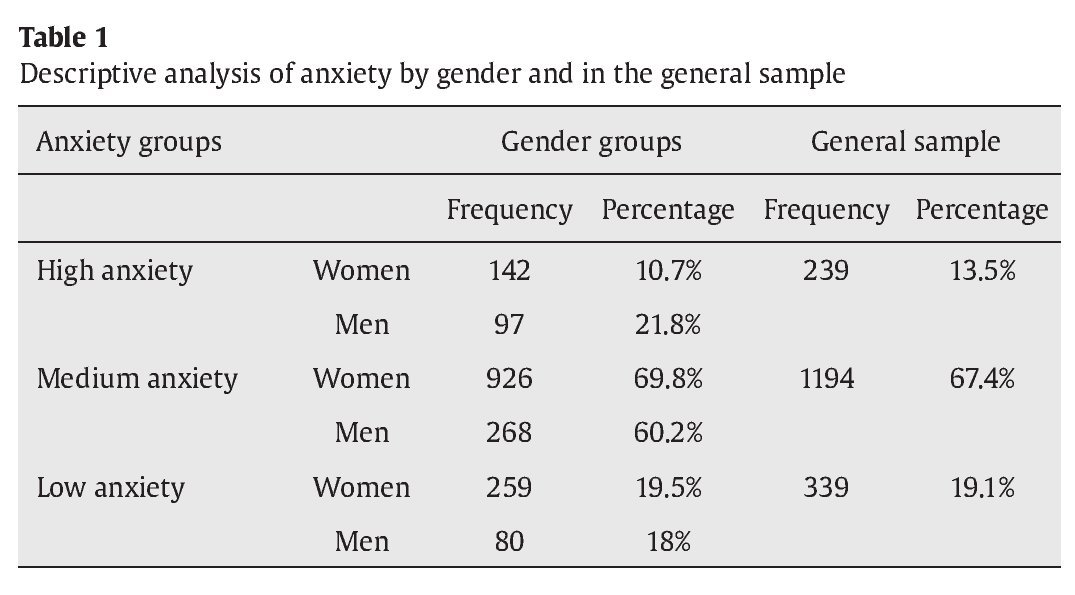
The descriptive analyses showed a level of general anxiety in the entire sample with a mean score of 21.63 ( SD = 8.93). In this sense, the mean by gender was M = 22.51 (SD = 10.22) for men and M = 21.43 (SD =8.43) for women. This difference is significant according to the t-test of difference of means, t (1, 1,770) = 2.40, p = .02.
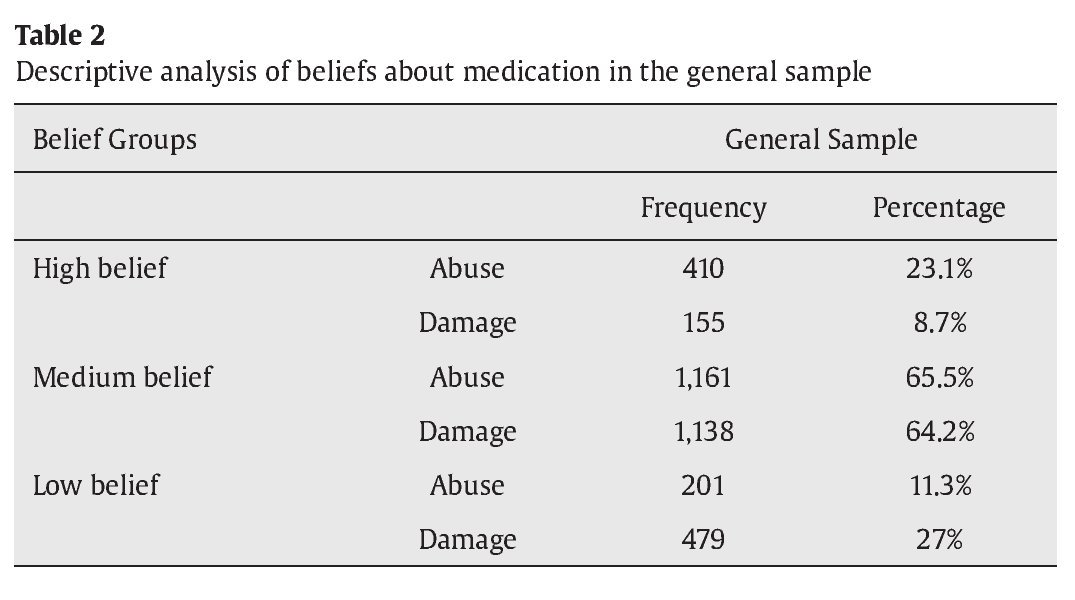
Using the standardization criteria of Spielberger et al.'s instrument (2002), we divided the sample by genders into groups of low, medium, and high anxiety. Table 1 presents the descriptive analysis of the frequency of subjects in each of these categories, as well as their percentages. Table 2 presents descriptive analysis of beliefs about medication in the general sample.
To determine the distribution of the beliefs, we only used the expression of beliefs about abuse and beliefs about damage. The total mean score was 3.18 ( SD = 0.82) for the scale of abuse (range: 1-5) and of 2.74 ( SD = 0.73) for the scale of damage (range: 1-5). For these mean expressions we used the sum of the scores in the items/ number of items according to the criteria of the authors of the Spanish version of the instrument (Beléndez-Vázquez et al., 2007).
Association of Variables
In order to determine the possible association between beliefs about medication and medical treatment and the level of anxiety in primary pediatric health attention, we performed a correlational analysis that not only included the level of general beliefs about medication, but also the two indicators of beliefs considered, as well as the expression of anxiety obtained. The results can be seen in Table 3.

We found a significant relation between the variables. Thus, a higher level of general expression of negative beliefs was associated with higher anxiety when consulting the pediatrician. Along the same lines, we found a significant positive association between higher anxiety and: (a) higher levels of beliefs about the abuse of medication treatments in pediatric attention and (b) higher levels of beliefs about possible damage due to medication treatments.
Differences of Means
In accordance with the goals of our study, we performed various t -tests for independent samples to determine possible discrepancies in beliefs as a function of gender. As shown in Table 4, our results showed higher levels in all indicators of beliefs in men in comparison to women.

In order to determine differences in anxiety as a function of age, we carried out an ANOVA, considering the general score in anxiety as the dependent variable and age as the independent variable. The result indicated significant differences, F (42, 1,729) = 1.61, p = .01. The level of anxiety increases as partcipants' age increases. On the contrary, we found no differences in the general expression of beliefs about medication, F (42, 1,729) = 1.30, p = .09, although the tendency of the data show higher levels of negative beliefs as age is higher.
Likewise, and following the same trend, we found differences in the dimensions of abuse beliefs, F (42, 1,729) = 2.058, p < .00, and, on the contrary, we found no differences in damage beliefs as a function of age, F (42, 1,729) = .99, p = .49. A high level of negative abuse beliefs was found as age increases.
Regression Analysis
With regard to our third goal, we conducted a linear regression analysis, considering the level of anxiety as the dependent variable and the two specific indicators of beliefs on medication as predictor variables. The results are presented in Table 5.
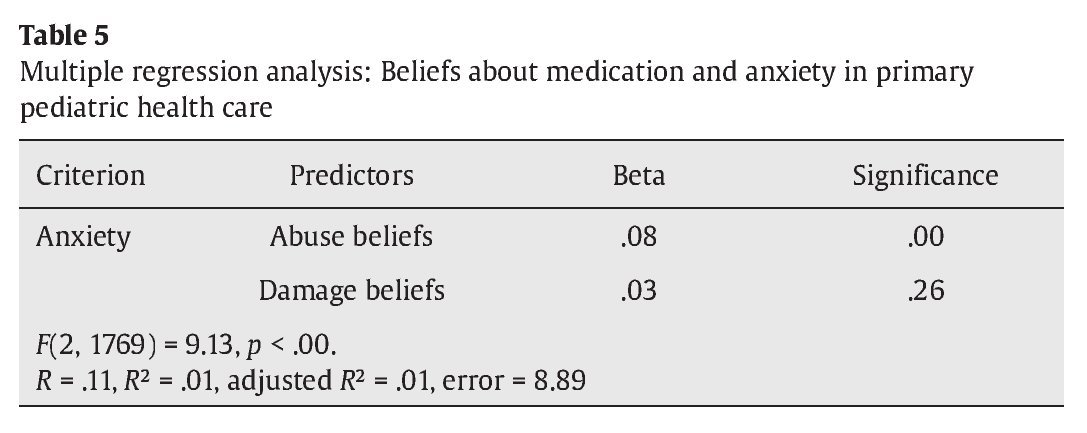
The model explained 1% of the variability of anxiety, according to the adjusted R 2 . Our results indicated that beliefs about abuse were the best predictors of participants' anxiety. The damage beliefs entered in the model were non-significant.
Discussion
In this work, we proposed firstly to study the presence of anxiety and negative representations of medication in primary pediatric attention; secondly, to study the possible association between parents' anxiety and beliefs about medicines in the treatment of their children in primary pediatric health care. We also wished to determine possible differences in anxiety and beliefs about abuse and damage between men and women and as a function of the parents' age. Lastly, we wished to tap the influence of the two specific dimensions of beliefs, abuse, and damage on anxiety.
Our initial results show that the mean levels of anxiety in the sample are fairly similar to those found in the normative studies of the general population (Spielberger et al., 2002). This led to the conclusion that, in general, the situation of pediatric care is not an anxiogenic situation. In fact, 86.5% of the parents who participated showed medium or low levels of anxiety. However, this result is expectable, as primary care does not include many serious situations, because these cases are attended in pediatric emergency units or other health facilities. Nevertheless, 13.5% of the parents showed high or very high levels, a percentage that increased to 21.8% in the sample of male participants.
Our data reflects differences in parents' anxiety in primary pediatric health care as a function of gender. We found higher levels of anxiety in men than in women in the sample. This result does not coincide with the findings from other studies (Caballo et al., 2008; Daig et al., 2009; MacSwain et al., 2009; McLean & Anderson, 2009), which found an inverse result or trend, or with the studies that found no differences between fathers and mothers in emotional alterations during the loss of a child's health (Fernández-Castillo & López-Naranjo, 2006a). Nevertheless, this gender difference deserves more attention in future investigations, especially because there were more women than men in our sample. It is more usual for the mother to accompany her child to the pediatrician, and the father's presence may be due to health consultations that are more serious and less routine, but this hypothesis has not been tested in our study and deserves more attention in the future.
With regard to the beliefs, the general results show that the participants in our study presented general levels similar to those of the normative samples, such as in validation studies. In fact, our results are fairly similar to those obtained in the work of Beléndez-Vázquez et al. (2007), in which the total mean score for the subscales in a group of young university students was 3.42 ( SD = 0.81) for abuse and 2.53 ( SD = 0.65) for damage.
However, it is noteworthy that 23.1% of the participants felt that the prescription of drugs is abusive or that an alternative treatment may also have been adequate. In contrast, only 8.7% of the participants showed high levels of beliefs about the harmful effects of the medication. Therefore, according to these data, the great majority of the participants (91.2%) considered that there is no risk of damage for their child to take the medicines prescribed by the pediatrician.
Secondly, our results reveal the existence of an association between anxiety and general beliefs about medicines. When determining the relations between the diverse specific variables of beliefs about medicines and anxiety, our results showed the same trend. So, higher levels of beliefs about medicine abuse and beliefs about the threat of medicine were associated with higher levels of anxiety. This result is logical if we take into account that one of the frequent causes associated with the onset of anxiety is the perception of a potentially dangerous or threatening situation (Spielberger, 1966). Therefore, the parents' negative perception of a pediatric pharmacological treatment would logically be associated to higher levels of anxiety. And although this implication requires further research, such anxiety could be associated with nonadherence to treatment or, at least, to dissatisfaction with it.
Thirdly, we found significant differences in parents' negative beliefs about medicines in pediatric treatment of their children when taking into account parents' gender. Thus, in the diverse dimensions of beliefs and in the general expression of beliefs about medicines fathers expressed more negative beliefs, more abuse beliefs, and more beliefs about damage of the medicines than mothers. This result disagrees with some studies that have indicated that gender is not a good predictor of differences in beliefs about medicines (Horne et al., 2009; Kumar et al., 2008). This discrepancy should be taken with precaution because it could be due to the particular characteristics of our sample, made up of a high percentage of mothers.
When determining differences as a function of age, our data show a higher level of anxiety as age increases. This result contradicts general studies of anxiety in large samples and in other specific typologies of anxiety (Caballo et al., 2008; Daig et al., 2009; MacSwain et al., 2009), although these authors indicate that as individuals grow older they acquire more skills to cope with anxiety. This may be the case in pediatric care, in view of the tendency observed in the sample of parents studied. According to our data, the situation of a child's illness is associated with higher levels of anxiety in older parents. Again, this result should be studied in view of its contradiction with other relevant studies.
Likewise, in regard to beliefs, only the belief about abuse of medicines presents higher levels as age increases.
Our main results show no differences as a function of age in the general expression of beliefs or in the beliefs about the damage of medicines. Some studies have found similar results, pointing out that beliefs about medicines remain stable over time and finding no differences as a function of age (Porteous et al., 2010). With regard to the result about the abuse of medication, being older may imply having more experience with failure of medication-based interventions, having experienced other alternative interventions, or even trusting alternatives treatments and therapies (Van den Bulck & Custers, 2009).
With regard to our last goal, we wanted to know which variables of those considered - beliefs about abuse and about damage - could better predict the presence of anxiety in primary pediatric health care. The results of the regression analysis were very interesting because not all the variables entered in the model were significant predictors. Thus, damage belief did not predict anxiety in parents.
The variable that reached higher predictive value in the sample was the belief about abuse of medicines. The relevance of this source of anxiety is clear. A possible explanation of this result is that the parents fully trust the pharmacological treatment prescribed by the pediatrician, and do not expect any damage or significant threat due to the medication. However, they do think that there may be some abuse in the use of medication, when alternative measures might also be effective. This issue seems to be a significant predictor of anxiety. Trust in the use of medication is obvious and it is certainly a good precursor of following and adhering to treatment.
In view of the low explanatory power of the model, there are surely important variables associated with anxiety that were not considered in this study. Future research may cast some light on aspects that deserve more attention with regard to parental anxiety during primary pediatric attention.
Given the association between beliefs about medicines and anxiety, it might be helpful for practitioners to assess these types of beliefs in patients for whom they prescribe medication. Such an assessment would provide the opportunity to discuss the patients' beliefs with them and to reduce anxiety in some cases.
The results of this study are indicating, in accordance with other works (Magadza, Radloff, & Srinivas, 2009), that intervention, including psychological and educational initiatives and the improvement of communication between parents and practitioners, will lead to an increase in the parents' levels of knowledge about medical treatment and be a positive influence on their beliefs about medicines.
It would be interesting for future studies to determine whether beliefs about medication may be associated with differential levels of satisfaction with primary pediatric care, as well as whether the anxiety associated with the negative beliefs may explain non-adherence to treatment or other problems with medical treatment.
We highlight that the general level of professional attention and the satisfaction of the patients and their relatives during primary pediatric health care could be improved by reducing anxiety when it occurs (Fernández-Castillo, VĂlchez-Lara, & Sada-Lázaro, 2011; Warner, Reigada, Fisher, Saborsky, & Benkov, 2009) and by increasing health education levels, particularly taking into account the probability of higher levels of anxiety in children of parents with disorders or frequent anxious states (Murray, Creswell, & Cooper, 2009; Rapee, Schniering, & Hudson, 2009).
To conclude, along with the interventions aimed at promoting health education or reducing levels of anxiety in health contexts, there is a need for interventions targeting pediatricians and health professionals to promote skills to detect and cope with anxiety in their patients and their patients' parents.
Conflict of Interest
The authors of this article declare no conflict of interest.
Financial Support
This research was supported by an investigation project promoted by the Health Office of the Andalusian Government. Project Code: 0142/08. (The funder had no role in study design, analysis, interpretation of data, report writing or in the decision to submit the paper for publication. The authors are independent of the funder).
Manuscript received: 21/03/2014
Revision received: 28/04/2014
Accepted: 13/05/2014
Doi: h t t p & # 5 8 ; & # 4 7 ; /dx.doi.org/10.1016/j.clysa.2014.06.003
* Correspondence concerning this article should be addressed to
Prof. Antonio Fernández-Castillo.
Department of Developmental and Educational Psychology.
Facultad de Ciencias de la EducaciĂłn. Universidad de Granada.
Campus de Cartuja s/n. 18071 Granada, Spain. E-mail: afcastil@ugr.es.
Correspondence can also be sent to
Dr. MarĂa J. VĂlchez-Lara. Department of Anesthesiology and Reanimation.
Virgen de las Nieves University Hospital Complex.
Avda. De las Fuerzas Armadas, s/n. 18071 Granada, Spain.
E-mail: mjv1414@yahoo.es
References
Beléndez-Vázquez, M., Hernández-Mijares, A., Horne, R., & Weinman, J. (2007). Evaluación de las creencias sobre el tratamiento: validez y fiabilidad de la versión española del "Beliefs about Medicines Questionnaire" [Assessment of beliefs about treatment: validity and reliability of the Spanish version of the "Beliefs about Medicines Questionnaire"]. International Journal of Clinical and Health Psychology, 7, 767-779.
Bondesson, A., Hellström, L., Eriksson, T., & Höglund, P. (2009). A structured questionnaire to assess patient compliance and beliefs about medicines taking into account the ordered categorical structure of data. Journal of Evaluation in Clinical Practice, 15, 713-723.
Caballo, V. E., Salazar, I. C., Irurtia, M. J., Arias, B., Hofmann, S. G., Bragagnolo, G., ... Barroso, R. (2008). Social anxiety in 18 nations: Sex and age differences. Behavioral Psychology-Psicologia Conductual, 16 , 163-187.
Chavira, D. A., Stein, M. B., Bailey, K., & Stein, M. T. (2004). Child anxiety in primary care: Prevalent but untreated. Depression and Anxiety, 20, 155-164.
Cortina, S., Somers, M., Rohan, J. M., & Drotar, D. (2013). Clinical Effectiveness of Comprehensive Psychological Intervention for Nonadherence to Medical Treatment: A Case Series. Journal of Pediatric Psychology, 38, 649-663.
Daig, I., Herschbach, P., Lehmann, A., Knoll, N., & Decker, O. (2009). Gender and age differences in domain-specific life satisfaction and the impact of depressive and anxiety symptoms: A general population survey from Germany. Quality of Life Research, 18, 669-678.
DiMatteo, M. R., Lepper, H. S., & Croghan, T. W. (2000). Depression is a risk factor for noncompliance with medical treatment: Meta-analysis of the effects of anxiety and depression on patient adherence. Archives of Internal Medicine, 160, 1201-1207.
Fernández-Castillo, A., & López-Naranjo, I. (2006a). Estrés parental en la hospitalización infantil [Parental stress during children's hospitalization]. Ansiedad y Estrés, 12, 1-7.
Fernández-Castillo, A., & López-Naranjo, I. (2006b). Transmisión de emociones, miedo, y estrés infantil por hospitalización [Transmission of children's emotions, fear, and stress due to hospitalization]. International Journal of Clinical and Health Psychology, 6 , 631-645.
Fernández-Castillo, A., Sada-Lázaro, E., & VĂlchez-Lara, M. J. (2008). Anxiety in immigrant parents during hospitalization of their children. International Journal of Psychology, 43 , 492-492.
Fernández-Castillo, A., & VĂlchez-Lara, M. J. (2009a). OpiniĂłn profesional sobre la hospitalizaciĂłn infantil de inmigrantes de origen latinoamericano en AndalucĂa, España [Professional opinion about hospitalization of immigrant children of Latin-American origin in Andalusia, Spain]. Revista de Salud PĂşblica, 11, 336-346.
Fernández-Castillo, A., & VĂlchez-Lara, M. J. (2009b). Necesidades percibidas en la atenciĂłn hospitalaria pediátrica a inmigrantes segĂşn la opiniĂłn profesional: estudio cualitativo [Perceived needs in paediatric hospital care for immigrants according to professional opinion: A qualitative study]. IntervenciĂłn Psicosocial, 18, 153-164.
Fernández-Castillo, A., VĂlchez-Lara, M. J., & Sada-Lázaro, E. (2011). Satisfaction with Hospitalization Scale: Adaptation and psychometric properties. Behavioral Psychology, 20, 383-400.
Fortier, M. A., Rosario, A. M., Martin, S. R., & Kain, Z. N. (2010). Perioperative anxiety in children. Pediatric Anesthesia, 20, 318-322.
Herren, C., In-Albon, T., & Schneider, S. (2013). Beliefs regarding child anxiety and parenting competence in parents of children with separation anxiety disorder. Journal of Behavior Therapy and Experimental Psychiatry, 44, 53-60.
Horne, R. (1997). Representations of medication and treatment: Advances in theory and measurement. In K. Petrie & J. Weinman (Eds.), Perceptions of health and illness. Current research and applications (pp. 155-188). Amsterdam: Harwood Academic Publishers.
Horne, R., Graupner, L., Frost, S., Weinman, J., Wright, S. M., & Hankins, M. (2004). Medicine in a multi-cultural society: The effect of cultural background on beliefs about medications. Social Science & Medicine, 59, 1307-1313.
Horne, R., Parham, R., Driscoll, R., & Robinson, A. (2009). Patients' attitudes to medicines and adherence to maintenance treatment in inflammatory bowel disease. Inflammatory Bowel Disease,15, 837-844.
Horne, R., & Weinman, J. (1998). Predicting treatment adherence: An overview of theoretical models. In L. Myers & K. Midence (Eds.), Adherence to treatment in medical conditions (pp. 25-50). London: Harwood Academic Publishers.
Horne, R., & Weinman, J. (1999). Patients' beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. Journal of Psychosomatic Research, 47 , 555-567.
Horne, R., Weinman, J., & Hankins, M. (1999). The Beliefs about Medicines Questionnaire: The development and evaluation of a new method for assessing the cognitive representation of medication. Psychology & Health, 14, 1-24.
JĂłnsdĂłttir, H., Friis, S., Horne, R., Pettersen, K. I., Reikvam, A., & Andreassen, O. A. (2008). Beliefs about medications: Measurement and relationship to adherence in patients with severe mental disorders. Acta Psychiatrica Scandinavica, 119, 78-84.
Kumar, K., Gordon, C., Toescu, V., Buckley, C. D., Horne, R., Nightingale, P .G., & Raza, K. (2008). Beliefs about medicines in patients with rheumatoid arthritis and systemic lupus erythematosus: A comparison between patients of South Asian and white British origin. Rheumatology, 47, 690-697.
MacSwain, K. L. H., Sherry, S. B., Stewart, S. H., Watt, M. C., Hadjistavropoulos, H. D., & Graham, A. R. (2009). Gender differences in health anxiety: An investigation of the interpersonal model of health anxiety. Personality and Individual Differences, 47 , 938-943.
Magadza, C., Radloff, S. E., & Srinivas, S. C. (2009). The effect of an educational intervention on patients' knowledge about hypertension, beliefs about medicines, and adherence. Research in Social and Administrative Pharmacy, 5 , 363-375.
Mahler, C., Jank, S., Hermann, K. Horne, R. Ludt, S. Haefeli, W. E., & Szecsenyi, J. (2009). Psychometric properties of a German Version of the Satisfaction with Information about Medicines Scale (SIMS-D). Value in Health, 12, 1176-1179.
Mardby, A., Akerlind, I., & Jörgensen, T. (2007). Beliefs about medicines and self-reported adherence among pharmacy clients. Patient Education and Counseling, 69, 158-164.
McLean, C. P., & Anderson, E. R. (2009). Brave men and timid women? A review of the gender differences in fear and anxiety. Clinical Psychology Review, 29, 496-505.
Miklosi, M., Szabo, M., Martos, T., Galambosi, E., & Forintos, D. P. (2013). Cognitive Emotion Regulation Strategies Moderate the Effect of Parenting Self-Efficacy Beliefs on Parents' Anxiety Following Their Child's Surgery. Journal of Pediatric Psychology, 38, 462-471.
Mishina, H., & Takayama, J. I. (2009). Screening for maternal depression in primary care pediatrics. Current Opinion in Pediatrics, 21, 789-793.
Moitra, E., & Armstrong, C. L. (2009). Tumor locus moderates anxiety symptoms in a pediatric neuro-oncologic sample. Child Neuropsychology, 15, 460-470.
Murray, L., Creswell, C., & Cooper, P. J. (2009). The development of anxiety disorders in childhood: An integrative review. Psychological Medicine, 39, 1413-1423.
Needle, J. S., O'Riordan, M., & Smith, P. G. (2009). Parental anxiety and medical comprehension within 24 hrs of a child's admission to the pediatric intensive care unit. Pediatric Critical Care Medicine, 10, 668-674.
Perpiñá, M., MartĂnez, E., Belloch, A., Lloris, A., & Pellicer, C. (2009). Creencias sobre la salud y los medicamentos en la poblaciĂłn asmática española. ValidaciĂłn de dos instrumentos para su medida. [Spanish asthma patients' beliefs about health and medicines: Validation of two questionnaires]. Archivos de BronconeumologĂa, 45, 218-223.
Porteous, T., Francis, J., Bond, C., & Hannaford, P. (2010). Temporal stability of beliefs about medicines. Patient Education and Counseling, 79, 225-230.
Rapee, R. M., Schniering, C.A ., & Hudson, J. L. (2009). Anxiety disorders during childhood and adolescence: Origins and treatment. Annual Review of Clinical Psychology, 5 , 311-41.
Rasmussen, J. N., Chong, A., & Alter, D. A. (2007). Relationship between adherence to evidence-based pharmacotherapy and long-term mortality after acute myocardial infarction. JAMA, 297, 177-186.
Sakolsky, D., & Birmaher, B. (2008). Pediatric anxiety disorders: Management in primary care. Current Opinion in Pediatrics, 20, 538-543.
Spielberger, C. D. (1966). Theory and research on anxiety. In C. D. Spielberger (Ed.), Anxiety and behavior (pp. 3-20). New York: Academic Press.
Spielberger, C. D., Gonzalez, H. P., Taylor, C. J., Algaze, B., & Anton, W. D. (1978). Examination stress and test anxiety. In C. D. Spielberger & I. G. Sarason (Eds.), Stress and anxiety (Vol. 5, pp. 167-191). New York: Wiley.
Spielberger, C. D., Gorsuch, R. L., & Lushene, R. E. (1983). State-Trait Anxiety Inventory . San Francisco, CA: Consulting Psychologists Press.
Spielberger, C. D., Gorsuch, R. L., & Lushene, R. E. (2002). STAI: Cuestionario de Ansiedad Estado-Rasgo [State-Trait Anxiety Inventory]. Madrid: TEA.
Unni, E. J., & Farris, K. B. (2011). Unintentional non-adherence and belief in medicines in older adults. Patient Education and Counseling, 83, 265-268.
Van den Bulck, J., & Custers, K. (2009). Belief in complementary and alternative medicine is related to age and paranormal beliefs in adults. European Journal of Public Health, 20 , 227-230.
Warner, C. M., Reigada, L. C., Fisher, P. H., Saborsky, A. L., & Benkov, K. J. (2009). CBT for anxiety and associated somatic complaints in pediatric medical settings: An open pilot study. Journal of Clinical Psychology in Medical Settings, 16, 169-177.
Wray, J., Lee, K., Dearmun, N., & Franck, L. (2011). Parental anxiety and stress during children's hospitalisation: The StayClose study. Journal of Child Health Care, 15, 163-174.
Wu, Y. P., Rohan, J. M., Martin, S., Hommel, K., Greenley, R. N., Loiselle, K., ... Fredericks, E. M. (2013). Pediatric Psychologist Use of Adherence Assessments and Interventions. Journal of Pediatric Psychology, 38, 595-604.
Copyright © 2024. Colegio Oficial de la Psicología de Madrid






 PDF
PDF CrossRef
CrossRef Print
Print Send
SendEMAIL ALERT
Clinical and Health is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License







