


Dependency, detachment and psychopathology in a nonclinical sample: General relations and gender differences. Is there a new line of inquiry on paranoid pathology?
[Dependencia, desapego y psicopatología en una muestra no clínica: relacionesgenerales y diferencias de género. ¿Hay una nueva línea de investigación de lapatología paranoide?]
Manuel R. Abuín1 , Luis de Rivera2
1Univ. Complutense de Madrid, Fac. Psychology, Dep. Personality, Assessment and Clinical Psychology, Spain ,2Univ. Autónoma de Madrid, Spain
https://doi.org/10.1016/j.clysa.2015.06.003
Abstract
In this study, both Bornstein's Relationship Profile Test (RPT) and Derogatis' Symptom Ckeck List (SCL-90-R)were administered to a nonclinical sample of 119 subjects from Madrid (Spain). Healthy dependency, dysfunctional detachment and destructive overdependence (RPT subscales) were evaluated and correlated with SCL-90-R symptom dimensions. Destructive overdependence correlated positively with every SCL-90-Rpsychopathology dimension. On the contrary, healthy dependency correlated negatively with all these SCL-90-R dimensions. Gender differences were significant with regard to the correlation between dysfunctional detachment and paranoid ideation. In women dysfunctional detachment correlated positively with paranoidideation, whereas in men the resultant correlation was negative and not significant. This gender difference in the relationship between dysfunctional detachment and paranoid ideation may suggest a new line of inquiry on paranoid pathology. Besides, the study explores the SCL-90-R psychopathology scores of several clusters of individuals with different profiles of dependency-detachment obtained from the RPT subscale scores.
Resumen
En este estudio, se administraron tanto el Test del Perfil de la Relación de Bornstein (RPT) como el cuestionario de 90 síntomas de Derogatis (SCl-90-R) a una muestra no clínica de 119 sujetos de Madrid. La dependencia saludable, el desapego disfuncional y la sobre dependencia destructiva (subescalas del RPT)fueron evaluadas y correlacionadas con las dimensiones de psicopatología del SCL-90- R. La sobredependencia destructiva correlacionó positivamente con todas las dimensiones de psicopatología. Por el contrario, la dependencia saludable correlacionó negativamente con todas estas dimensiones de psicopatología. Se han encontrado diferencias de género con respecto a la correlación entre el desapego disfuncional y la ideación paranoide. En las mujeres, el desapego disfuncional correlacionó positivamente con la ideación paranoide, mientras que en los hombres esta correlación fue negativa y no significativa. Estas diferencias de género en la relación entre el desapego disfuncional y la ideación paranoide sugieren una nueva línea de investigación sobre la patología paranoide. Se exploran además las puntuaciones de psicopatología del SCL-90-R en diferentes grupos de individuos con diferentes perfiles de dependencia desapego, a partir de las puntuaciones del Test del Perfil de Relación.
In the last thirty five years there has been an increasing interest in the measurement of dependency factors and their relationship with psychopathology. Since the study conducted by Hirshfeld et al. (1977) with the Interpersonal Dependency Inventory (IDI), different researchers have linked dependency factors with psychopathological clinical disorders such as dependent personality disorder ( Bornstein, 1993 ), affective and anxiety disorders (Akiskal et al., 2008; Darcy, Davila & Beck, 2005; Shulte, Mongrain & Flora, 2008 ), substance abuse disorders ( Bornstein, Gottdiener, & Winarick, 2010; McMain & Ellery, 2008 ), and eating disorders (Bornstein, 2001). Bornstein and Johnson (1990) studied the relationship between dependency and psychopathology in a nonclinical sample. The authors used the Dependency subscale of the Personality Diagnostic Questionnaire-Revised PDQ-R ( Hyler et al., 1988 ) and Derogatis’ Symptom Check List SCL-90-R ( Derogatis, 1983; Derogatis, Lipman, & Covi. 1973 ). They found significant positive correlations between dependency and several psychopathology dimensions. In contrast to other studies ( AbuĂn & Rivera, 2014; Bornstein et al., 2004; González de Rivera et al., 1991 ), they did not find gender differences on psychopathology and dependency scores.
As the concept of dependency evolved through different theoretical models, dependency has been assessed in different ways. The dynamic model linked dependency traditionally – in its classic metaphor – to fixation on oral satisfaction needs and on the vicissitudes of object relations. New approaches from cognitive and interactionist models have tried to integrate cognition, motivation, affect, behavior, and context related behavior with the object relations theory ( Bornstein, 1996 ). Recently, from a psychometric point of view, McClintock, McCarrick, and Anderson (2014) have found a significant relationship between interpersonal dependency and excessive reassurance-seeking (ERS). From the behavioral and social learning theory point of view, dependency is based on the individual's reinforcement history. Dependent behaviors are displayed because they are rewarded by others or, as Bornstein has pointed out, because the individual perceives them as likely to elicit rewards ( Bornstein, 2005 ). These patterns may be learned by own experience or by vicarious identifications.
Dependency and its seemingly opposite, detachment, are not unidimensional constructs. Several researchers ( Bornstein, 2005; Bornstein et al., 2004; Cross, Bacon, & Morris, 2000; Cross & Madson, 1997 ) consider different types of dependency and detachment. Bornstein et al. (2004) distinguish three dimensions: destructive overdependence, healthy dependency, and dysfunctional detachment. Destructive overdependence (DO) is characterized by maladaptive and inflexible dependency. It includes a) the perception of the self as weak and helpless, the extreme need to establish and maintain close ties to caregivers or authority figures, c) the fear of negative evaluations and abandonment by others, and d) clinginess. Healthy dependency (HD) is characterized by flexible and adaptive dependency and is associated with appropriate seeking of help and support. It includes a) the perception of the self as competent, b) a healthy need of close ties, c) well-being in intimate situations, d) appropriate confidence in oneself, and e) autonomous functioning. Dysfunctional detachment (DD) is characterized by a) a perception of others as hurtful or untrustworthy, b) an extreme autonomous self-presentation, c) a marked need to maintain distance from others, and d) fear of being hurt or overwhelmed by closeness.
To measure these dependency-detachment dimensions, Bornstein created the Relationship Profile Test RPT ( Bornstein & Languirand, 2004 ). Construct validity of the RPT has been supported by several studies ( Bornstein, Geiselman, Eisenhart, & Languirand, 2002; Bornstein et al., 2004; Bornstein & Huprich, 2006 ).
Dependency is a significant source of gender differences. A plethora of studies have consistently supported the fact that women obtain higher scores than do men on self-report measures of dependency, although this pattern of results is not so consistent with projective dependency scores ( Bornstein, 1995 ). Previously, Bornstein, Manning, Krukonis, Rossner, & Mastrosimone (1993) had found that women obtained higher dependency scores than men when a self-report measure was used (in this case, Hirshfeld's interpersonal dependency inventory), but there were no significant differences when a projective dependency measure vas used (in this case the ROD scale; Masling, Rabie, & Blondheim, 1967 ). Gender differences in detachment were especially studied by Bornstein et al. (2004) , who did not find any differences between men and women using the RPT. Similar findings with regard to dysfunctional detachment and gender differences were obtained by Haggerty, Blake, and Siefert (2010) . Healthy dependency, a concept closely related to interdependence, is a source of gender differences according to Bornstein et al. (2004) , who found that women obtained higher scores than men on healthy dependency subscales, a result that is congruent with Cross and Madson's (1997) model of self-construal. However, other studies have not found these gender differences related to interdependence ( Gabriel & Gardner, 1999; Haggerty et al., 2010 ). As Baumeister and Sommer (1997) and Gabriel and Gardner (1999) suggest, there can be two types of interdependence, depending on taking in consideration either men or women. Men's type of interdependence seems to be related to a feeling of group belongingness, whereas women's type seems to be related to intimate and close relationships rather than to group belongingness.
The purposes of this paper are, on the one hand, to study the intercorrelations among RPT dimensions and the relationships between the dependency and detachment measures of the RPT with the SCL-90-R psychopathology dimensions in a nonclinical sample; and, on the other hand, to explore the scores on SCL-90-R dimensions and indices of clusters of subjects with different profiles of dependency-detachment and to investigate the effects of gender on the different relationships between dependency-detachment and psychopathology. According to the studies developed with the English version of the RPT in USA samples ( Bornstein & Huprich, 2006; Bornstein & Johnson, 1990; Bornstein et al., 2004 ), the following predictions were tested with the Spanish version of the RPT in a nonclinical sample in Spain: (1) destructive overdependence, dysfunctional detachment, and healthy dependency should be correlated with each other; destructive overdependence and/ or dysfunctional detachment should correlate negatively with healthy dependency; (2) destructive overdependence and dysfunctional detachment should be positively correlated with psychopathology dimensions measured by a self-report instrument (SCL-90-R); (3) healthy dependency should be negatively correlated with dimensions of psychopathology measured by the SCL-90-R; (4) the links between dependency variables and psychopathology should tend to be generalized, rather than limited to specific dimensions; and(5)gender should affect specific correlations rather than global correlations.
Method ParticipantsParticipants were 119 subjects (38 males and 81 females). They participated in a psychoeducational project on “how to manage stress and anxiety”, offered by a private psychiatric and psychological clinic of Madrid. All of them had been previously assessed through a clinical interview. Subjects with either history of psychiatric disorder or current clinical psychopathology were not included in the study. The mean age was 25.67 years ( SD = 6.48), with a range from 18 to 66 years.
MeasuresVariables of dependency and detachment were assessed by the Spanish version of Bornstein's Relationship Profile Test ( AbuĂn, MesĂa, & Rivera, 2007 ). The RPT consists of 30 items that define three dimensions related to dependency or to detachment: a) destructive overdependence (DO), b) dysfunctional detachment (DD), and c) healthy dependency (HD). Items are assessed on a scale with a range from 0 to 5.
Psychopathology was assessed by the Spanish version of Derogatis’ Symptom Check List-90 Revised ( Rivera, De las Cuevas, RodrĂguez-AbuĂn, & RodrĂguez-Pulido, 2002 ). The SCL-90-R yields subscale scores for nine dimensions of psychopathology (somatization, obsessive-compulsive, interpersonal sensitivity, depression, anxiety, phobic anxiety, hostility, paranoid ideation, and psychoticism) and three global psychopathology scores (Positive Symptom Total PST, General Symptom Index GSI, and Positive Symptoms Distress Index PSDI). Reliability and validity properties of the Spanish version are described by the authors ( González de Rivera, De Las Cuevas, RodrĂguez-AbuĂn, & RodrĂguez-Pulido, 2002 ).
ProcedureSubjects completed three questionnaires in the following order: a socio-cultural questionnaire, the RPT, and the SCL-90-R.
ResultsThe results of this study are summarized in tables 1 through 9. RPT subscale scores adjusted to normal distribution except healthy dependency scores (HD), according to the results of the Kolmogorov-Smirnov Test (HD; Z = .09, p < .05). Healthy dependency, however, has both skewness and kurtosis values and respective standard errors that seem to fit with normal distribution (healthy dependency: skewness/ SE skewness = .77; kurtosis/SE kurtosis = .26; expected values between ± 2 for a normal distribution). On the contrary, SCL-90-R dimension scores did not adjust to normal distribution as it is reported in the same Table 1 (p < .05 for all the dimensions) and, thus, non parametric analyses were conducted to test the different hypotheses that involved psychopathology dimensions. When comparing distributions of RPT subscale scores in men and women, it can be noted through the KolmogorovSmirnov Test ( Table 2 ) that there are different distributions for destructive overdependence ( Z = 1.46, p < .05) and somatization (Z = 1.55, p < .05), depending on gender.
Goodness of Fit Analysis. Skewness, Kurtosis and Kolmogorov-Smirnov Test for Dependency-Detachment and Psychopathology Variables.
| Mean | SD | Skew | Skew SE | K | K SE | Z a | |
|---|---|---|---|---|---|---|---|
| DO | 27.45 | 6.04 | -0.11 | .22 | -0.14 | .44 | .06 |
| DD | 29.53 | 4.92 | 0.03 | .22 | -0.30 | .44 | .05 |
| HD | 33.81 | 5.01 | -0.17 | .22 | -0.12 | .44 | .09* |
| SOM | 0.72 | 0.65 | 0.93 | .22 | 0.14 | .44 | .15*** |
| O-C | 1.03 | 0.72 | 0.86 | .22 | 1.18 | .44 | .12** |
| I-S | 0.84 | 0.74 | 1.50 | .22 | 2.91 | .44 | .13*** |
| DEP | 0.87 | 0.74 | 0.98 | .22 | 0.39 | .44 | .12*** |
| ANX | 0.70 | 0.67 | 1.11 | .22 | 0.59 | .44 | .17*** |
| HOS | 0.71 | 0.69 | 1.50 | .22 | 3.56 | .44 | .15*** |
| PHOB | 0.30 | 0.48 | 2.16 | .22 | 5.32 | .44 | .26*** |
| PAR I. | 0.88 | 0.76 | 1.24 | .22 | 1.76 | .44 | .15*** |
| PSY | 0.52 | 0.59 | 1.72 | .22 | 3.02 | .44 | .19*** |
| GSI | 0.75 | 0.59 | 1.24 | .22 | 1.57 | .44 | .12*** |
| PST | 37.29 | 21.89 | 0.31 | .22 | 0.44 | .44 | .08 |
| PSDI | 1.68 | 0.50 | 1.68 | .22 | 4.43 | .44 | .13*** |
Note. RPT subscales: DO = destructive overdependence, DD = dysfunctional detachment, HD = healthy dependency. SCL 90 R dimensions and indices: SOM = somatization, O-C = obsessive-compulsive, I-S = interpersonal sensitivity, DEP = depression, ANX = anxiety, HOS = hostility, PHOB = phobic anxiety, PAR I. = paranoid ideation, PSY = psychoticism, GSI = global severity index, PST = positive symptom total, PSDI = positive symptom distress index.
Skew = skewness, K = kurtosis, SE = standard error, Z = Kolmogorov-Smirnov statistic.
a Results of Kolmogorov-Smirnov test with Lilliefors correction.
* p < . 05, ** p < .01, *** p < .001
Z Kolmogorov-Smirnov Test for Two Samples.
| Diff | Z | |
|---|---|---|
| DO | .28 | 1.46* |
| DD | .23 | 1.18 |
| HD | .11 | 0.56 |
| SOM | .30 | 1.55* |
| O-C | .14 | 0.73 |
| I-S | .18 | 0.91 |
| DEP | .19 | 0.98 |
| ANX | .24 | 1.23 |
| HOS | .09 | 0.50 |
| PHOB | .15 | 0.76 |
| PAR I. | .13 | 0.67 |
| PSY | .13 | 0.65 |
| GSI | .23 | 1.16 |
| PST | .20 | 1.00 |
| PSDI | .22 | 1.11 |
Note. RPT subscales: DO = destructive overdependence, DD = dysfunctional detachment, HD = healthy dependency. SCL 90 R dimensions and indices: SOM = somatization, O-C = obsessive-compulsive, I-S = interpersonal sensitivity, DEP = depression, ANX = anxiety, HOS = hostility, PHOB = phobic anxiety, PAR I. = paranoid ideation, PSY = psychoticism, GSI = global severity index, PST = positive symptom total, PSDI = positive symptom distress index.
Diff = most absolute extreme differences between cumulative distributions of men and women.
*p < .05, **p < .01, ***p < .001
Gender differences were found in both RPT and SCL-90-R scores and are reported in Table 3 and Table 4 . Women obtained higher scores than men on destructive overdependence (DO) subscale ( t = -2.47, p < .05; d = -0.48), whereas men obtained higher scores than their female counterparts on dysfunctional detachment (DD) subscale ( t = 2.32, p < .05; d = 0.46). When considering SCL-90-R dimensions, women obtained higher scores than men in the following subscales: somatization ( z = -2.84, p < .01), depression (z = -2.30, p < .05), and anxiety (z = -2.46, p < .05).
Gender Differences in Dependency Variables (Student- t ) and Effect Size Measure (Cohen's d).
| Men | Women | t | d | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| DO | 25.53 | 5.94 | 28.39 | 5.91 | -2.47* | -0.48 |
| DD | 31.00 | 4.49 | 28.81 | 4.98 | 2.32* | 0.46 |
| HD | 33.77 | 4.43 | 33.82 | 5.30 | -0.06 | 0.00 |
Note. DO = destructive overdependence, DD = dysfunctional detachment, HD = healthy dependency.
*p < .05, **p < .01, ***p < .001
Gender Differences in SCL-90-R Variables (based on Mann-Whitney U test).
| Men | Women | Z | |||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| SOM | 0.47 | 0.48 | 0.83 | 0.69 | -2.84** |
| O-C | 0.94 | 0.57 | 1.06 | 0.79 | -0.49 |
| I-S | 0.64 | 0.54 | 0.93 | 0.81 | -1.78 |
| DEP | 0.62 | 0.52 | 0.99 | 0.79 | -2.30* |
| ANX | 0.46 | 0.46 | 0.81 | 0.72 | -2.46* |
| HOS | 0.63 | 0.52 | 0.76 | 0.76 | -0.48 |
| PHOB | 0.20 | 0.34 | 0.35 | 0.52 | -1.51 |
| PAR I. | 0.77 | 0.60 | 0.93 | 0.83 | -0.63 |
| PSY | 0.43 | 0.39 | 0.57 | 0.66 | -0.39 |
| GSI | 0.58 | 0.40 | 0.83 | 0.65 | -1.07 |
| PST | 303.21 | 20.71 | 39.20 | 22.29 | -1.35 |
| PSDI | 1.54 | 0.29 | 1.73 | 0.57 | -1.47 |
Note . SCL-90-R dimensions and indices: SOM = somatization, O-C = obsessive-compulsive, I-S = interpersonal sensitivity, DEP = depression, ANX = anxiety, HOS = hostility, PHOB = phobic anxiety, PAR I. = paranoid ideation, PSY = psychoticism, GSI = global severity index, PST = positive symptom total, PSDI = positive symptom distress index.
*p < .05, **p < .01, ***p < .001
As Table 5 shows, dysfunctional detachment was negatively correlated with healthy dependency (-.185, p < .05). As Table 6 shows, there is a gender difference in this correlation; in men the correlation was positive but not significant (.14), whereas in women it was negative and statistically significant (-.31, p < .01). Using a statistical analysis to test differences of correlations ( Preacher, 2002 ), this difference was significant ( z = 2.27, p = .02).
Intercorrelations of RPT Subscale Scores.
| RPT subscales | DO | DD | HD |
|---|---|---|---|
| DO | .017 | -.116 | |
| DD | -.185* |
Note. N = 119 (81 women and 38 men)
Relation Profile subscales: DO = destructive overdependence, DD = dysfunctional detachment, HD = healthy dependency.
*p < .05, **p < .01, ***p < .001
Gender Differences in Intercorrelations of Relation Profile Test Subscales Scores.
| RPT subscales | DO | DD | HD |
|---|---|---|---|
| DO | - | .069 | -.139 |
| DD | .065 | - | .140 a |
| HD | -.113 | -.307** a | - |
Note. N = 119 (81 women and 38 men)
Relation Profile subscales: DO = destructive overdependence, DD = dysfunctional detachment, HD = healthy dependency.
Subscale intercorrelations for men are above the diagonal; women are below the diagonal.
a Significant difference between men and women: z = 2.27, p = .002
*p < .05, **p < .01, ***p < .001
Table 7 shows that unhealthy dependency-detachment scores of the RPT (destructive overdependence and dysfunctional detachment) were positively correlated with SCL90-R global scores and dimensions in the whole sample. The RPT measure of unhealthy dependency, destructive overdependence, was positively correlated with all the SCL-90-R global scores and dimensions: significant correlations ranged from .18 (hostility) to .45 (interpersonal sensitivity). Dysfunctional detachment was positively correlated with all the global scores of SCL-90-R and with some dimension scores: obsessive-compulsive (.23, p < .05), interpersonal sensitivity (.22, p < .05) depression (.21, p < .05), hostility (.27, p < .01), and psychoticism (.27, p < .01). On the contrary, the RPT measure of healthy dependency (HD) was negatively correlated with all the SCL-90-R dimensions scores. Correlations ranged from -.24 (somatization) to -.41 (depression). HD scores also correlated negatively with all SCL-90-R global scores.
Dependency-Psychopathology Correlations in the Whole Sample.
| SCL-90-R scores | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RPT variables | SOM | O-C | I-S | DEP | ANX | HOS | PHOB | PAR I. | PSY | GSI | PST | PSDI |
| Destructive overdependence | .24** | .29** | .46*** | .29** | .37*** | .18* | .21* | .34** | .30** | .34*** | .34*** | .19* |
| Dysfunctional detachment | .08 | .23* | .22* | .21* | .15 | .27** | .10 | .17 | .28** | .22* | .18* | .24** |
| Healthy dependency | -.22* | -.30** | -.39*** | -.36*** | -.25** | -.30** | -.22* | -.37*** | -.23* | -.34*** | -.34*** | -.21* |
Note. N = 119 (81 women and 38 men)
SCL-90-R dimensions and indices: SOM = somatization, O-C = obsessive-compulsive, I-S = interpersonal sensitivity, DEP = depression, ANX = anxiety, HOS = hostility, PHOB = phobic anxiety, PAR I. = paranoid ideation, PSY = psychoticism, GSI = global severity index, PST = positive symptom total, PSDI = positive symptom distress index.
*p < .05, **p < .01, ***p < .001
Attending to gender differences (Table 8 ), there is a particular disparity between men and women with regard to the correlation between dysfunctional detachment and paranoid ideation. In women, dysfunctional detachment was positively correlated with paranoid ideation (.32, p < .01), whereas in men this correlation was negative but not significant (-.17); this difference of correlation is significant ( z = -2.47, p < .05). It can also be noted that most of the correlations of dysfunctional detachment with SCL-90-R dimensions tended to be significant in women (exceptions: correlations of dysfunctional detachment with somatization and with phobic anxiety), whereas in men all the correlations were not significant. This differential pattern of correlations between men and women was not found with regard to healthy dependency and destructive overdependence. In men, destructive overdependence was positively correlated with somatization (.40, p < .05), interpersonal sensitivity (.49, p < .01), depression (.36, p < .05), anxiety (.54, p < .01), and paranoid ideation (.43, p < .01); in women, some of the significant correlations were different (obsessive-compulsive, .28, p < .05; interpersonal sensitivity, .42, p < .001; anxiety, .27, p < .05; paranoid ideation, .30, p < .01; psychoticism, .30, p < .01). With regard to healthy dependency, it can be noted that in women its correlations with SCL-90-R dimensions are negative and significant in all cases. On the contrary, in men healthy dependency is only significantly correlated with interpersonal sensitivity (-.34, p < .05), depression (-.34, p < .05), and paranoid ideation (-.47, p < .01).
Gender Differences in Dependency-Psychopathology Correlations.
| SCL-90-R var.? | RPT vars.? | Destructive overdependence | Dysfunctional detachment | Healthy dependency |
|---|---|---|---|---|
| SOM | Men | .40* | .04 | -.15 |
| Women | .10 | .18 | -.26* | |
| Z | 1.59 | -0.70 | 0.56 | |
| O-C | Men | .32 | .10 | -.19 |
| Women | .28* | .28* | -.35** | |
| Z | 0.22 | -0.92 | 0.85 | |
| I-S | Men | .49** | .22 | -.34* |
| Women | .42*** | .29* | -.42*** | |
| Z | 0.66 | -0.36 | 0.46 | |
| DEP | Men | .36* | .23 | -.34* |
| Women | .21 | .28* | -.38** | |
| Z | 0.80 | -0.26 | 0.23 | |
| ANX | Men | .54** | .11 | -.27 |
| Women | .27* | .25* | -.28* | |
| Z | 1.60 | -0.71 | 0.05 | |
| HOS | Men | .18 | .03 | -.21 |
| Women | .16 | .38** | -.35** | |
| Z | 0.10 | -1.82 | 0.75 | |
| PHOB | Men | .13 | .14 | -.12 |
| Women | .19 | .12 | -.27* | |
| Z | -0.30 | 0.10 | 0.77 | |
| PAR I. | Men | .43** | -.17 | -.47** |
| Women | .30** | .32** | -.33** | |
| Z | .53 | -2.47* | -.82 | |
| PSY | Men | .21 | .19 | -.20 |
| Women | .33** | .32** | -.26* | |
| Z | -0.64 | -0.68 | 0.31 | |
| GSI | Men | .39* | .12 | -.33* |
| Women | .29* | .30** | -.34** | |
| Z | 0.56 | -0.93 | 0.05 | |
| PST | Men | .46** | .09 | -.32* |
| Women | .25* | .26* | -.36** | |
| Z | 1.18 | -0.86 | 0.22 | |
| Men | -.11 | .27 | -.27 | |
| PSDI | Women | .26* | .31** | -.20 |
| Z | -1.85 | -0.21 | -0.36 |
Note . SCL-90-R dimensions and indices: SOM = somatization, O-C = obsessive-compulsive, I-S = interpersonal sensitivity, DEP = depression, ANX = anxiety, HOS = hostility, PHOB = phobic anxiety, PAR I. = paranoid ideation, PSY = psychoticism, GSI = global severity index, PST = positive symptom total, PSDI = positive symptom distress index.
Table 9 shows clusters of subjects from dependency-detachment variables of the RPT resulting from a K-means cluster analysis and contingency analysis between gender and resultant clusters. As it can be noted in this table, there are three different clusters that define a set of subjects with a different profile of dependency and detachment scores on the RPT subscales. Cluster 1 was defined by the highest scores on DO (Mean = 32.00, SD = 3.87) and on HD (Mean = 37.75, SD = 4.34), whereas the lowest scores were on DD (Mean = 24.33, SD = 31.07). Cluster 2 was defined by intermediate scores on DD (Mean = 29.65, SD = 4.22) and HD (Mean = 34.96, SD = 3.96) subscales, whereas the lowest scores were on DO subscale (Mean = 21.84, SD = 4.34). Cluster 3 was defined by the highest scores on DD subscale (Mean = 32.11, SD = 4.18), high scores on DO subscale (Mean = 31.07, SD = 3.82) and the lowest scores on HD subscale (Mean = 30.52, SD = 4.33). As it is noted below the table, cluster membership is related to gender (contingency coefficient, .249, p = .02). As it is presented below, in Figure 1 , a very low percentage of men belongs to cluster 1 (7.7%) and more than 50% belong to cluster 2, whereas women are more balancedly distributed among the three clusters. These three clusters that define styles of interpersonal relationship were a significant source of individual differences in SCL-90-R psychopathology dimensions and indices, as it is summarized in Table 10 . Means and standard deviations among all SCL-90-R variables are reported by cluster membership. Z values were obtained through a non parametrical Kruskal-Wallis one-way analysis of variance. Results of comparisons of SCL-90-R variables among these three groups through the U Mann-Whitney test are reported in the same table. Table 10 reveals significant differences of the average ranks between cluster 1 and 3, and between clusters 2 and 3.
Mean and Standard Deviation of Dependency-Detachment Clusters and Contingency Analysis between Gender and Cluster Membership.
| RPT Subscale | CL1 | CL2 | CL3 | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| Destructive overdependence | 32.00 | 3.88 | 21.84 | 3.72 | 31.07 | 3.83 |
| Dysfunctional detachment | 24.33 | 3.34 | 29.65 | 4.22 | 32.11 | 4.19 |
| Healthy dependency | 37.75 | 4.34 | 34.96 | 3.96 | 30.52 | 4.33 |
Note . Contingency coefficient: .249 ( p = .02) CL1 (n = 24; 3 men, 21 women)
CL2 (n = 49; 22 men; 27 women)
CL3 (n = 46; 14 men, 32 women)
Cluster membership is a source of significant differences on all the three RPT subscale scores ( p < .001).
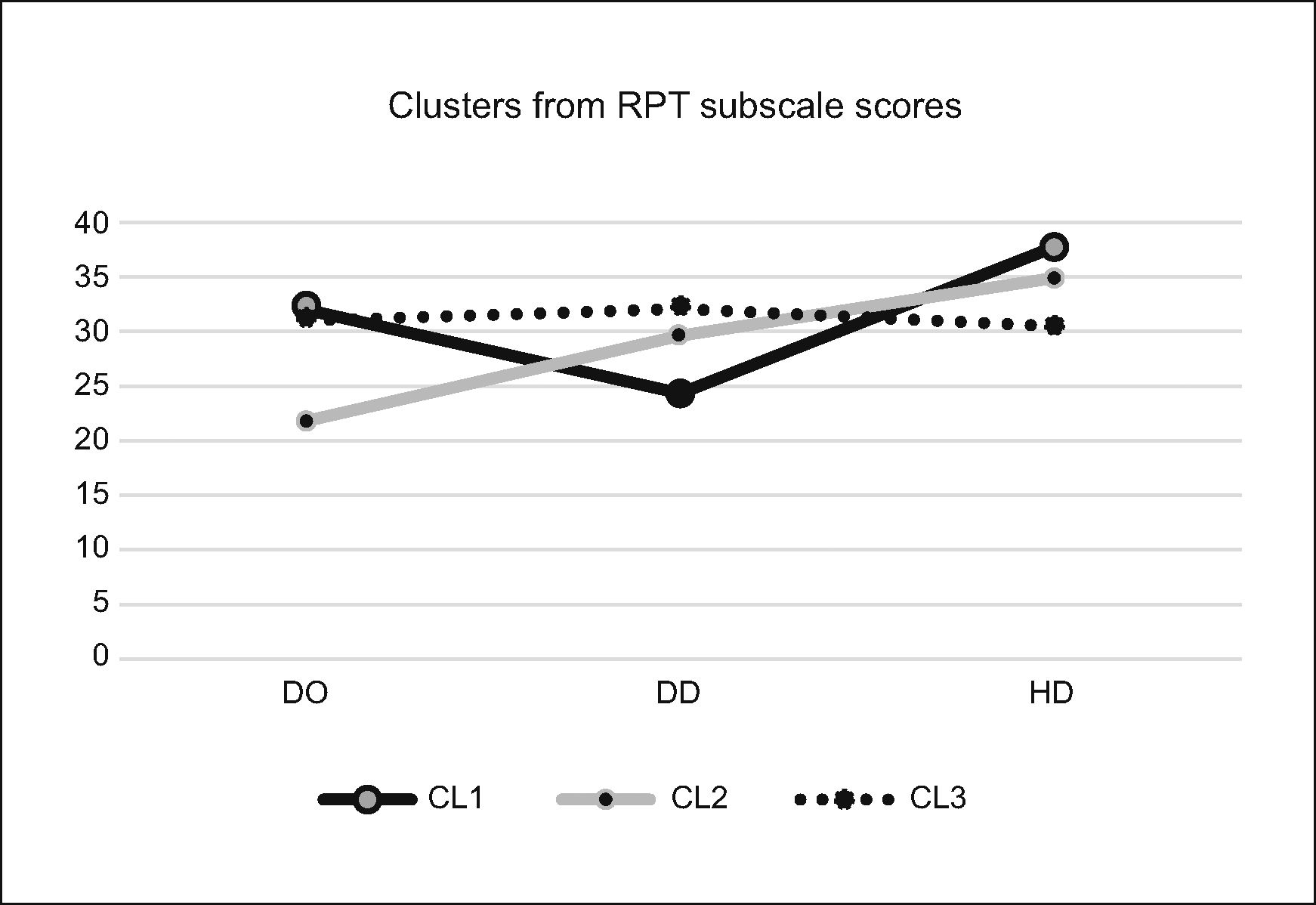
Clusters from RPT Subscale Scores
Note . Cluster 1: 7.7% men, 26% women; cluster 2: 56.4% men, 33.8% women; cluster 3: 35.9% men, 32.8% women.
% of the total of men and women, respectively DO: destructive overdependence
DD: dysfunctional detachment HD: healthy dependency.
| CL1 | CL2 | CL3 | Kr-W | U 1-2 | U 1-3 | U 2-3 | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Chi2 | Z | Z | Z | |
| SOM | 0.65 | 0.65 | 0.51 | 0.57 | 0.99 | 0.65 | 16.53*** | -0.85 | -2.38* | -4.00*** |
| O-C | 0.82 | 0.65 | 0.75 | 0.56 | 1.45 | 0.74 | 24.53*** | -0.24 | -3.36** | -4.73*** |
| I-S | 0.76 | 0.71 | 0.53 | 0.52 | 1.23 | 0.81 | 26.50*** | -1.24 | -2.71** | -5.16*** |
| DEP | 0.68 | 0.75 | 0.65 | 0.61 | 1.22 | 0.75 | 18.51*** | -0.19 | -3.14** | -3.99*** |
| ANX | 0.56 | 0.59 | 0.47 | 0.55 | 1.03 | 0.70 | 20.31** | -0.77 | -2.85** | -4.36*** |
| HOS | 0.45 | 0.50 | 0.53 | 0.56 | 1.07 | 0.78 | 19.79** | -0.83 | -3.58** | -3.85*** |
| PHOB | 0.26 | 0.38 | 0.20 | 0.45 | 0.44 | 0.53 | 7.39* | -0.43 | -1.53 | -2.69*** |
| PAR I. | 0.72 | 0.66 | 0.61 | 0.65 | 1.28 | 0.78 | 24.52*** | -0.80 | -3.06** | -4.83*** |
| PSY | 0.45 | 0.57 | 0.35 | 0.48 | 0.75 | 0.66 | 15.53*** | -0.62 | -2.22* | -3.94*** |
| GSI | 0.61 | 0.53 | 0.54 | 0.47 | 1.07 | 0.61 | 25.29*** | -0.37 | -3.22** | -4.90*** |
| PST | 31.96 | 21.85 | 28.78 | 19.33 | 49.78 | 19.11 | 24.67*** | -0.50 | -3.20** | -4.82*** |
| PSDI | 1.60 | 0.63 | 1.56 | 0.35 | 1.85 | 0.54 | 11.26** | -0.68 | -2.52** | -3.03*** |
Note . SCL-90-R dimensions and indices: SOM = somatization, O-C = obsessive-compulsive, I-S = interpersonal sensitivity, DEP = depression, ANX = anxiety, HOS = hostility, PHOB = phobic anxiety, PAR I. = paranoid ideation, PSY = psychoticism, GSI = global severity index, PST = positive symptom total, PSDI = positive symptom distress index.
Kr-W: Kruskal-Wallis one-way analysis of variance by ranks
U: Mann-Whitney U
N = 119 (81 women and 38 men)
*p < .05, **p < .01, ***p < .001
These results confirm the findings of other studies on the dependency-psychopathology link ( Bornstein et al., 2004; Bornstein & Johnson, 1990 ) and add some not previously reported findings about gender differences. The results also suggest that it is useful to distinguish healthy dependency-detachment from unhealthy dependency-detachment. As it has been pointed out by Bornstein et al. (2004) , dependency and detachment are complex constructs. In this study, dysfunctional detachment (DD) correlated negatively with healthy dependency (HD) in women, supporting some Bornstein's previous reports with samples of college students ( Bornstein et al., 2004; Bornstein et al., 2003 ). However, the fact that this correlation is significant in women but not in men is a particular new finding that needs further investigation. Dysfunctional detachment in men is not incongruent with the presence of healthy dependency. According to the different types of interdependence depending on gender referred and argued by Baumeister and Sommer (1997) or by Gabriel and Gardner (1999) , men's type of interdependence is related to a feeling of group belongingness, whereas women's type is related to intimate and close relationships rather than to belongingness. This difference of correlation when distinguishing men from women can make sense, considering that this interdependence of men may be related to group belongingness and not to emotional closeness, as it seems to be usual among women. Besides, there is no link between destructive overdependence (DO) and HD and between DO and DD, contradicting, respectively, some other studies ( Bornstein et al., 2003; Bornstein, Porcerelli, Huprich, & Markova, 2009 ). Relationships between these three components of dependency-detachment attending to gender differences do not seem very clear, and they seem to vary depending on the characteristics of the sample. For example, in a sample of low income urban women seeking medical services, Bornstein et al. (2009) found that DD scores were positively correlated to DO scores, though DD scores were not correlated to HD scores. AbuĂn, Becerril, and Vilariño (2015) , with a new instrument for measuring interpersonal bonding, found that scores on an unhealthy dependency subscale were positively correlated to scores on an emotional distancing subscale, in both clinical and non clinical samples. These various and apparently contradictory results seem to point out, on the one hand, that dysfunctional detachment may appear simultaneously with destructive overdependence, suggesting that both of them can be components of intercorrelated insecure modes of attachment. On the other hand, contradictory results of correlations that involve healthy dependency may show that there could be different types of interdependence, depending on gender and on the characteristics of the sample. Further research has to be conducted in order to distinguish and conceptualize both dysfunctional detachment and destructive overdependence, and how they can be integrated into different types of interpersonal bonding. Besides, it is necessary to pay attention to the type of samples studied by researchers, especially when the sample consists of a group of college psychology students. Results can be different if samples from the general population are used.
Besides, the results of this study go much further than the confirmation of findings previously reported by Bornstein and Johnson (1990) and Bornstein et al. (2004) . On the one hand, it is noticeable that high scores on healthy dependency scales are associated to low scores on the psychopathology dimensions, whereas high scores on the destructive overdependence subscale are associated to high scores on the psychopathology SCL-90-R dimensions. Therefore, healthy dependency seems to promote and preserve psychological health. Adequate help-seeking, self-reliance, desire for closeness, and intimacy and autonomous functioning are components of healthy dependency which are linked to low levels of psychopathology in the nonclinical population. As Bornstein (1993, 1998) has pointed out, healthy interdependent persons delay seeking treatment after physical or psychological symptoms appear less long than nondependent persons; or it seems easier for them to ask for help than for non dependent persons, which may also result in higher academic performance ( Bornstein & Kennedy, 1994 ). On the other hand, there are particular and meaningful gender differences in RPT subscales intercorrelations. As reported in Table 4 , there is no significant correlation between DD scores and HD scores (positive but not significant) in men, whereas this correlation is significantly negative in women. As for current social roles, this difference suggests that for men, trying to maintain emotional distance from others is “acceptable” and does not imply a lack of healthy dependency; on the contrary, this same pattern is not acceptable for women, for whom dysfunctional detachment is not compatible with healthy dependency. Men are supposed to be “stronger” and more “independent” than women, which is supported by the significant differences on DD subscale scores ( Table 3).
With regard to dysfunctional detachment, it maintains fewer links with psychopathology than the rest of the RPT subscale scores. Besides, there is a meaningful gender difference that involves the link of dysfunctional detachment with psychopathology. With regard to gender differences, dysfunctional detachment was positively correlated with paranoid ideation in women, whereas in men this correlation was negative and not significant. This seems to mean that maintaining too much distance from others is less “acceptable” for women than for men. The image of social avoidance or emotional distancing is related to paranoid symptoms in women, whereas in men it looks more acceptable and is not related either to paranoid ideation or to any other suffering of psychopathology. It is also remarkable that, in men, dysfunctional detachment did not correlate significantly with any psychopathology dimension of SCL-90-R. On the contrary, in women dysfunctional detachment correlated positively with several dimensions of psychopathology (obsessive-compulsive dimension, interpersonal sensitivity, depression, anxiety, hostility, paranoid ideation, and psychoticism). However, the contrast of correlations showed gender differences that only involved the dysfunctional detachment-paranoid ideation pair. There was another correlation between dysfunctional detachment and hostility, with the same tendency and quite close to statistical significance ( Z = -1.82, p = .068). It would be interesting to replicate the study with a larger sample. The fact that emotional distancing in women may be correlated with paranoid symptoms and even with hostility makes sense and could be consistent with social roles and the types of self-construal depending on gender pointed out by Cross and Madson (1997) and completed and put into context by other researchers, such as Baudmeister and Sommer (1997) or Gabriel and Gardner (1999) . On the contrary, in men emotional distancing can be considered as a normal and social characteristic expected by others and not linked with psychopathology. This gender difference can be explained in two compatible principal ways:
- a.
It can be explained as an effect of gender differences in the “explicit social image”. Men are supposed to show more autonomy and an independent self-image, whereas women are expected to show more closeness and intimacy in their interpersonal relationships. Self-report measures seem to be sensitive to this effect ( Bornstein, Manning, Krukonis, Rossner, & Mastrosimone, 1993 )
- b.
It can also be explained as an effect of gender differences in emotional reactivity. Gender differences in biological reactivity and hormonal patterns (e.g., Taylor et al., 2000 ) could explain the need for more emotional proximity in women than in men and its implications in the suffering of psychopathology.
The psychopathology-dependency links, in general, tend to be non-specific or generalized to a wide variety of psychopathological dimensions. Healthy dependency and destructive overdependence are correlated with a wide range of dimensions of psychopathology.
Dysfunctional detachment has fewer links with psychopathology and could be considered as a defensive mode of self-presentation that is linked with gender-related psychopathological symptoms; in men, dysfunctional detachment is not associated with psychopathology, whereas in women it is associated with paranoid symptoms.
It is remarkable that although there was this particular gender difference in the DD-paranoid ideation correlation, there were no significant gender differences in paranoid ideation scores, as well as in quite a few other SCL-90-R subscale scores (there were significant gender differences only in somatization, anxiety, and depression). It may be due to some particular characteristics of the sample that do not seem to fit exactly with a sample from general population. Both men and women seem to obtain higher mean scores on the SCL-90-R dimensions than their Spanish counterparts ( González de Rivera et al., 2002 ). Besides, in the general Spanish population women obtain higher scores than men on SCL-90-R subscales, even with other psychopathology screening measures (AbuĂn y Rivera, 2014). It is noticeable that this sample consists of people who are volunteer to participate in a psychoeducational project on learning how to manage stress and anxiety. This condition can skew a bit the participants of the resultant sample, although people with clinical disorders were excluded from the participants.
The different scores on psychopathology SCL-90-R subscales and global indices among the three clusters obtained from dependency-detachment subscales of the Relationship profile test give room for debate on the relationships of attachment-bonding styles and psychopathology. In line with most research ( Ainsworth, Blehar, Waters, & Wall, 1978; Roissman et al., 2007 ) attachment styles are supposed to be categorical and non-continuous, a premise that is very arguable. In the present research, considering dependency-detachment in a continuous way, it is interesting to find different profiles of dependency-detachment and their relations with SCL-90-R psychopatology dimensions. In this particular sample, it is interesting to remark that the highest mean scores on SCL-90-R dimensions were obtained by the cluster that had subjects with the highest scores on DD subscale, quite high scores on DO subscale, and the lowest scores on HD subscale. This finding, along with the fact that there were no differences on SCL-90_R between cluster 1 and cluster 2, seems to point out that healthy dependency is likely to be a relevant variable to prevent the suffering of psychopathological distress, and that when both dysfunctional detachment and destructive overdependence present high scores, the risk of suffering psychopathological stress maybe higher. It is also interesting to consider in these clusters from dependency-detachment variables that very few men belong to cluster 1. This cluster is characterized by the lowest scores on DD subscale and the highest scores on HD and OD subscales. Men are expected to be more emotionally distant and, perhaps, less overdependent than women. Their adaptive style of interpersonal bonding seems to fit better to cluster 2 (lowest scores on OD subscale and intermediate scores on DD and HD subscales) than to cluster 1.
Findings described in this paper are useful and congruent with both clinical practice and investigation that is well structured and summarized by Bornstein (2005) . It is well known and supported by research that there are some relevant links between dependency factors and psychopathology (e.g., Akiskal et al., 2008; Bornstein, 1993, 2001; Darcy et al., 2005; Shulte et al., 2008 ). In clinical practice, it has often been found that unhealthy dependency needs are correlated with somatic and psychological pathology, a relationship existing between duration of hospitalization of patients with persistent somatization ( Mallouh, Abbey, & Gillies, 1995 ). Besides, there is a relationship between the history of loss and clinical syndromes whose pathoplasty and recovery depends on several factors as comorbidity with dependent personality disorder ( Mallouh et al., 1995) and perhaps on the gender ( Huprich, Stepp, Graham, & Johnson, 2004 ). Paranoid syndromes are not related to help-seeking from others and their treatment is not easy. In women, these paranoid responses related to a difficult management of dependency and attachment links may suggest a borderline personality disorder. Therefore, in the psychological assessment of paranoid disorders, it is useful to explore the attachment aspects of personality. There could be some different patterns of paranoid disorders related or not to emotional distancing, attending to gender differences. In contrast with men, paranoid symptoms seem to be associated with dysfunctional detachment in women. It is necessary to find out the determinants of the genesis and development of emotional distancing and its implications. Three general hypothesis can be suggested: a) stressful affective experiencing could result in either paranoid symptoms or paranoid disorders (e.g., paranoid reactions); b) there could be a rejection of emotional proximity related to a personality dysfunction (e.g., paranoid personality disorder); and c) there could be both stressful affective experiences and a personality dysfunction (e.g., borderline personality disorder and its stress related paranoid symptoms). Treatment methods that foster a healthy dependency and a flexible autonomy are appropriate to enhance people's well-being. These methods are useful in both preventive interventions and psychotherapy.
From these results, future studies should aim at exploring three challenges:
- a.
Gender differential relationship between dysfunctional detachment and paranoid ideation. There are some questions not yet answered: (1) is the gender difference found in this study with regard to dysfunctional detachment-paranoid ideation specific for this sample or can it be extended to other samples? (2) Can this gender difference be extended to other correlations, as it may be suggested with the differences found in the correlation between dysfunctional detachment and hostility? (3) How can social roles and cultural differences affect the relationship between dysfunctional detachment and paranoid ideation?
- b.
The impact of dependency-detachment factors and gender differences on the triggering and development of psychological and somatic health disorders. Particularly, it would be interesting to explore the gender-based relationship among dysfunctional detachment, paranoid disorder and borderline personality disorder.
- c.
How we can promote well-being and health from the development of healthy dependency-detachment links . Particularly, it would also be interesting to study how dysfunctional detachment, destructive overdependence, and healthy dependency in childhood predict health and well-being in adulthood; and, in accordance with this, how health and wellbeing can be promoted from the development of an appropriate dependency and attachment.
Lastly, there are some limitations to the results obtained in this study. Firstly, gender related differences in the relationship of dysfunctional detachment with paranoid symptoms have been studied in a specific or particular non clinical sample; these differences support a new line of inquiry on paranoid pathology and it would be interesting to replicate this study in other samples. Secondly, gender-related differences in the relationship of dysfunctional detachment with paranoid symptoms might be specific to culture. It would be interesting to replicate this study in other cultures.
Conflict of InterestThe authors of this article declare no conflict of interest.
Copyright © 2024. Colegio Oficial de la Psicología de Madrid






 PDF
PDF CrossRef
CrossRef Print
Print Send
SendEMAIL ALERT
Clinical and Health is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License







