


Risk Factors and Treatment Needs of Batterer Intervention Program Participants with Substance Abuse Problems
[Los factores de riesgo y las necesidades de tratamiento de los participantes en los programas de intervenci├│n con maltratadores con problemas de abuso de substancias]
Cristina Expósito-Álvarez1, Marisol Lila1, Enrique Gracia1, and Manuel Martín-Fernández2
1University of Valencia, Spain; 2Autonomous University of Madrid, Spain
https://doi.org/10.5093/ejpalc2021a9
Received 2 May 2021, Accepted 2 June 2021
Abstract
The aim of the present study was to identify the main risk factors and treatment needs of batterer intervention program (BIP) participants with alcohol and drug abuse problems (ADAPs), beyond issues strictly related to their substance abuse, taking into account four sets of variables: sociodemographic (i.e., age, educational level, income, employment, and immigrant status); personality disorders and psychological adjustment (i.e., clinical symptomatology, personality disorders, anger, impulsivity, and self-esteem); social-relational variables (i.e., community support, intimate support, stressful life events, and perceived social rejection); and violence-related variables (i.e., family violence exposure, perceived severity of intimate partner violence against women [IPVAW], ambivalent sexism, risk of future violence, physical and psychological intimate partner violence, motivation to change, and stage of change). The study was based on a sample of 1,039 male IPVAW offenders court-mandated to a community-based BIP. Results from comparisons between BIP participants with and without ADAPs were interpreted in terms of effect sizes to highlight the most salient differences. Differences with moderate effect sizes were found for clinical symptomatology, anger trait, anxiety disorder, depressive disorder, stressful life events, motivation to change and stage of change. Differences with large effect sizes were found for impulsivity, antisocial disorder, borderline disorder, and aggressive disorder. Several intervention strategies are proposed to guide and adjust interventions to risk factors and treatment needs of BIP participants with ADAPs.
Resumen
El objetivo de este estudio fue identificar los principales factores de riesgo y necesidades de tratamiento de los participantes en un programa de intervención con maltratadores (BIP) con problemas de abuso de alcohol y/o drogas (ADAP), más allá de sus problemas de abuso de substancias, teniendo en cuenta cuatro conjuntos de variables: sociodemográficas (i.e., edad, nivel educativo, ingresos, empleo y estatus de inmigrante), trastornos de personalidad y ajuste psicológico (i.e., sintomatología clínica, trastornos de personalidad, ira, impulsividad y autoestima), variables socio-relacionales (i.e., apoyo comunitario, apoyo íntimo, eventos vitales estresantes y rechazo social percibido) y variables relacionadas con la violencia (i.e., exposición a violencia familiar, gravedad percibida de la violencia contra la mujer en las relaciones de pareja, sexismo ambivalente, riesgo de violencia futura, violencia de pareja física y psicológica, motivación al cambio y estadio de cambio). El estudio se basó en una muestra de 1,039 hombres condenados por violencia de género y remitidos a un programa de intervención para maltratadores como medida penal alternativa. Los resultados de las comparaciones entre los participantes con y sin ADAP se interpretaron en función de los tamaños del efecto para destacar las diferencias más salientes. Se encontraron diferencias con tamaños del efecto moderados para sintomatología clínica, rasgo de ira, trastorno de ansiedad, sucesos vitales estresantes, motivación para el cambio y estadio de cambio. Se encontraron diferencias con tamaños del efecto grandes para impulsividad, trastorno antisocial, de personalidad límite y de agresividad. Se proponen diversas estrategias de intervención para guiar y ajustar las intervenciones a los factores de riesgo y necesidades de tratamiento de los participantes de los programas de intervención para maltratadores con ADAP.
Keywords
Intimate partner violence, Batterer intervention programs, Alcohol abuse, Substance abuse, Risk factors, Treatment needs, Partner violence offendersPalabras clave
Violencia de pareja, Programas de intervenci├│n en maltratadores, Abuso de alcohol, Abuso de substancias, Factores de riesgo, Necesidades de tratamiento, MaltratadoresCite this article as: Expósito-Álvarez, C., Lila, M., Gracia, E., & Martín-Fernández, M. (2021). Risk Factors and Treatment Needs of Batterer Intervention Program Participants with Substance Abuse Problems. The European Journal of Psychology Applied to Legal Context, 13(2), 87 - 97. https://doi.org/10.5093/ejpalc2021a9
Marisol.Lila@uv.es Correspondence: Marisol.Lila@uv.es (M. Lila).Intimate partner violence against women (IPVAW) has been acknowledged as a public health, social policy, and human rights concern of epidemic proportions that affects approximately 30% of women at some point in their lives on a worldwide scale (World Health Organization [WHO, 2013]). In Europe, according to the survey conducted by the European Union Agency for Fundamental Rights (FRA), physical and sexual IPVAW had a lifetime prevalence of 22% across the 28 member countries, ranging from 13% in Spain to 32% in Denmark (FRA, 2014; Gracia et al., 2019; Martín-Fernández et al., 2019, 2020). In response to the high prevalence of IPVAW, intervention programs for IPVAW offenders–often referred to as batterer intervention programs (BIPs)–have been widely implemented. Typically, BIPs aim to reduce recidivism by promoting alternative behaviors to violence, raising responsibility awareness, and changing attitudes. Meta-analysis and systematic reviews on BIP effectiveness often show positive but modest effects on reducing IPVAW recidivism, particularly when they incorporate motivational strategies (Arce et al., 2020; Babcock et al., 2016, 2004; Cheng et al., 2019; Eckhardt et al., 2013; Feder & Wilson, 2005; Santirso, Gilchrist, et al. 2020). However, the literature finds that major challenges continue to hamper BIP effectiveness, most notably high dropout rates, low motivation to change, high levels of denial, minimization of responsibility and victim blaming, and dealing with high-risk and highly resistant participants (Carbajosa, Catalá-Miñana, Lila, & Gracia, 2017; Eckhardt et al., 2008; Henning & Holdford, 2006; Holtzworth-Munroe et al., 2000; Jewell & Wormith, 2010; Lila et al., 2019; Lila et al., 2014; Olver et al., 2011). BIP participants with alcohol and/or drug abuse problems (ADAPs) are among the most high-risk and highly resistant groups of IPVAW offenders (Bennett, 2008; Crane et al., 2015; Lila et al., 2020; Romero-Martínez et al., 2019a). ADAPs are one of the strongest correlates of IPVAW (Foran & O’Leary, 2008; Langenderfer, 2013; Leonard & Quigley, 2017; Moore & Stuart, 2004; WHO, 2010), and around 50% of BIP participants have some type of substance abuse problem (Crane et al., 2015; Kraanen et al., 2010; Stuart et al., 2003; Stuart et al., 2009). Research has also shown that ADAPs in BIP participants are strong predictors of low treatment adherence, dropout, recidivism, and severe violence (Easton et al., 2018; Jewell & Wormith, 2010; Moore & Stuart, 2004; Olver et al., 2011). In addition, IPVAW offenders with ADAPs tend to present a history of trauma (Alexander, 2014; Thomas et al., 2013), trait jealousy (Brem et al., 2018; Burch & Gallup, 2020), anger management problems (Eckhardt et al., 2008), emotion dysregulation (Grigorian et al., 2020), diminished empathetic and cognitive abilities (Romero-Martínez et al., 2019b; Romero-Martínez et al., 2016; Vitoria-Estruch et al., 2017), and poorer mental health (Moore & Stuart, 2004; Stuart et al., 2003; Thomas et al., 2013). Given the above characteristics, BIP participants with ADAPs can be defined as offenders who have specific risk factors and treatment needs beyond their substance abuse problems. Identifying and addressing the main risk factors and treatment needs among these BIP participants may contribute to the improvement of BIP effectiveness by targeting the intervention not only to reduce ADAPs but also to address these other related problems. However, available research does not provide a comprehensive view of the main risk factors and treatment needs that differentiate BIP participants with ADAPs from those without ADAPs. Research examining differences between BIPs participants with and without ADAPs typically focus on a single set of variables (e.g., personality, cognitive abilities, treatment related variables) and rely on modest sample sizes that limit the generalization of the results (Giancola et al., 2003; Romero-Martínez et al., 2016; Stuart et al., 2003). The present study addresses the limitations of past research using a large sample of IPVAW offenders attending a BIP to compare participants with and without ADAPs on variables tapping a wide range of risk factors and treatment needs. The aim is to identify the main risk factors and treatment needs of BIP participants with ADAPs that may help to inform and maximize the effectiveness of new intervention approaches with this group of offenders. To examine differences in risk factors and treatment needs between the two groups (offenders with and without ADAPs), we consider four sets of variables: (1) sociodemographic (i.e., age, educational level, income, employment, and immigrant status); (2) personality disorders and psychological adjustment (i.e., clinical symptomatology, personality disorders, anger, impulsivity, and self-esteem); (3) social/relational variables (i.e., community support, intimate support, stressful life events and perceived social rejection); and (4) violence-related variables (i.e., family violence exposure, perceived severity of IPVAW, ambivalent sexism, risk of future violence, intimate partner violence, motivation to change, and stage of change). Participants and Procedure The study is based on a sample of 1,039 male IPVAW offenders sentenced to less than two years in prison, without previous criminal records, and court-mandated to a community-based cognitive-behavioral BIP in Valencia, Spain. Eligible participants were male offenders over 18 years of age without severe substance abuse problems, severe cognitive impairments (i.e., brain damage, degenerative disorders), and/or psychopathologies (i.e., schizophrenia, psychosis) that could interfere with the functioning of the intervention group. Data were gathered as part of regular intake (pre-treatment) data collection for participants entering the BIP. The number of participants assessed varied across measures. Participants were properly informed about the research protocol and signed a written consent form in which confidentiality was guaranteed. This study was approved by the Experimental Research Ethics Committee of the University of Valencia (Ref. H1537520365110). Measures Alcohol and Drug Abuse Problems. These problems were measured with the alcohol dependence and drug dependence clinical syndrome scales included in the Millon Clinical Multiaxial Inventory-III (see the inventory description below). Scores above 75 suggest a significant alcohol and/or drug problem, while scores 85 or higher indicate a persistent, significant clinical concern or personality disorder related to alcohol and/or drug problems. Sociodemographic variables. Information was collected for age (in years), educational level (0 = no schooling, 1 = primary, 2 = secondary, 3 = college), immigrant status (0 = no, 1 = yes), employment status (0 = unemployed, 1 = employed) and income (from 0 = less than 1,800 €/year to 10 = more than 60,000 €/year). Personality disorders and psychological adjustment variables Symptom-Checklist-90-Revised (SCL-90-R; Derogatis, 1977; Spanish version by De las Cuevas et al., 1991). The SCL-90-R is a 90-item self-report inventory to assess psychological symptoms and psychological distress, rated on a 5-point Likert-type scale (0 = none, 4 = very much). In this study, a global index was used (the positive symptom total subscale), indicating the total number of symptoms reported. The original version validation reported Cronbach’s alpha reliability coefficients between .81 and .90. The SCL-90-R has been widely used with samples of Spanish BIP participants (Carbajosa, Catalá-Miñana, Lila, Gracia, et al., 2017; Catalá-Miñana et al., 2013; Fernández-Montalvo et al., 2020). Millon Clinical Multiaxial Inventory-III (MCMI-III; Millon, 2007; Spanish version by Cardenal & Sanchez, 2007). The MCMI-III was used to measure personality disorders and clinical syndromes. It is a self-report inventory composed of 175 true or false questions. The following subscales were used in this study: five clinical personality pattern scales (depressive, dependent, narcissistic, antisocial, and aggressive), two severe personality scales (borderline and paranoid), and three clinical syndrome scales (anxiety, alcohol dependence, and drug dependence). Scores above 75 suggest a significant personality trait or mental health concern, while scores 85 or higher indicate a persistent, significant clinical concern or personality disorder. The Spanish version reported Cronbach’s alpha reliability coefficients between .65 and .92. This version has demonstrated validity to identify specific risk personality traits for IPVAW perpetration and has been widely used in Spanish BIPs (Carbajosa, Catalá-Miñana, Lila, & Gracia, 2017; Catalá-Miñana et al., 2014; Romero-Martínez et al., 2021). State-Trait Anger Expression Inventory (STAXI-2; Spielberger, 1999; Spanish version by Miguel-Tobal et al., 2001). The STAXI-2 is a 44-item inventory which evaluates state anger, as a situational response, and trait anger, as a predispositional quality. Responses are on a 4-point Likert-type scale (1 = not at all, 4 = very much). The Spanish version reported Cronbach’s alpha reliability coefficients between .67 and .89. This inventory has traditionally been used with BIP participants (Fernández-Montalvo et al., 2020; Romero-Martínez et al., 2015; Siria et al., 2021). Plutchik’s Impulsivity Scale (Plutchik & van Praag, 1989; Spanish version by Páez et al., 1996). This is a 15-item self-report scale that assesses impulsivity, an immediate response that occurs when behavioral consequences are not taken into consideration, on a 4-point Likert-type scale (1 = never, 4 = almost always). For this study, Cronbach’s α was .74. The Spanish version of this scale has been widely used with samples of BIP participants (Lila et al., 2019; Romero-Martínez et al., 2013; Sahagún-Flores & Salgado-Pascual, 2013). Rosenberg Self-esteem Scale (RSES; Rosenberg, 1965; Spanish version by Martín-Albo et al., 2007). RSES is a 10-item scale to measure participants’ feelings of global self-worth. Responses are on a 4-point Likert-type scale (1 = totally disagree, 4 = totally agree). For this study, Cronbach’s α was .77. This scale has been used with Spanish samples of IPVAW offenders (Catalá-Miñana et al., 2013; Guerrero-Molina et al., 2020; Lila, Gracia & Murgui, 2013). Social/relational variables Perceived Community Support Questionnaire (PCSQ; Gracia & Herrero, 2006). This is an 18-item scale that assesses three dimensions of community social support: community integration (α = .69), community participation (α = .76), and support from community organizations (α = .72). Responses are on a 5-point Likert-type scale (1 = totally disagree, 5 = totally agree). This scale has been used with samples of IPVAW offenders (Catalá-Miñana et al., 2013; Vargas et al., 2017). Intimate Social Support Questionnaire (Lin et al., 1986; Spanish adaptation by Herrero et al., 2011). This is a 3-item unidimensional scale which measures participants’ perception of intimate support from close relatives and friends (i.e., intimate partner, family, and friends). Responses are on a 5-point Likert-type scale (1 = most of the time, 5 = never), Cronbach’s α was .62. This scale has been used previously with samples of Spanish BIP participants (Catalá-Miñana et al., 2017; Lila, Gracia, & Murgui, 2013; Lila et al., 2019). Stressful Life Events Questionnaire (Gracia & Herrero, 2004). This questionnaire was used to measure the accumulation of stressful situations. From a list of 33 stressful life events, participants identify those they have experienced during the last six months. High scores indicate an accumulation of stressful life events. Cronbach’s α was .74. It has been previously used in the field of Spanish BIPs (Catalá-Miñana et al., 2013; Lila, Gracia, & Murgui, 2013; Lila et al., 2019). Perceived Social Rejection Index (PSRI; Catalá-Miñana et al., 2013). This is a unidimensional 13-item scale which measures participants’ perceived social rejection as a consequence of their conviction of IPVAW. Responses are on a 5-point Likert-type scale (1 = strongly disagree, 5 = strongly agree). A higher score implies greater perceived social rejection. Cronbach’s α was .82. The PSRI has been used with Spanish BIP participants (Catalá-Miñana et al., 2013; Catalá-Miñana et al., 2017). Violence-related variables Family violence exposure. In this study, the participants’ exposure as a victim or witness to family violence during adolescence and/or childhood was assessed by trained program staff using the sixth item of the Spousal Assault Risk Assessment (see the SARA protocol description below). Exposure was rated as 0 = no exposure, 1 = infrequent exposure, 2 = frequent exposure. Perceived severity of IPVAW Scale (PS-IPVAW; Gracia et al., 2008). This scale presents eight IPVAW scenarios that participants had to rate in terms of severity on a 10-point Likert-type scale (0 = not severe at all, 10 = extremely severe). Cronbach’s α was .81. This scale has been used in the law enforcement context, and with Spanish samples of IPVAW offenders (Catalá-Miñana et al., 2013; Gracia et al., 2009, 2014; Lila, Gracia, & García, 2013; Lila et al., 2016; Vargas et al., 2015; Vargas et al., 2017). Ambivalent Sexism Inventory (ASI; Glick & Fiske, 1997; Spanish version by Expósito et al., 1998). This 22-item inventory was used to assess hostile and benevolent sexist attitudes. The hostile sexism scale includes explicit negative attitudes toward women, while the benevolent sexist attitudes scale represents paternalistic attitudes, in both cases based on the assumption of women’s inferiority. Responses are on a 5-point Likert-type scale (1 = strongly disagree, 5 = strongly agree). Cronbach’s α was .89 for hostile sexism and .84 for benevolent sexism. This inventory has customarily been used with BIP participants (Juarros-Basterretxea et al., 2018; Juarros-Basterretxea et al., 2019; Vargas et al., 2015; Vitoria-Estruch et al., 2018). Spousal Assault Risk Assessment Guide (SARA; Kropp et al., 1999; Spanish version by Andrés-Pueyo et al., 2008). This is a 20-item protocol used to assess risk of recidivism toward former or present partners and non-partners. It was completed by trained psychologists who rated risk factors as 0 = low, 1 = moderate, and 2 = high risk. Cronbach’s α was .70. The Spanish version of this risk assessment guide has been widely used with samples of IPVAW offenders (Gallardo & Salgado, 2017; Lila et al., 2018; Romero-Martínez et al., 2021; Vargas et al., 2020). Revised Conflict Tactics Scale (CTS-2; Straus et al., 1996; Spanish version by Loinaz et al., 2012). CTS-2 is a 78-item self-report scale that assesses how individuals choose to resolve relationship conflicts, thus evaluating the presence of violence. Participants report on their behaviors over the previous 12 months (0 = this has never happened, 6 = more than 20 times in the past year, 7 = not in the past year, but it happened before). Cronbach’s α was .83 for physical violence and .79 for psychological violence. The CTS-2 has been used previously with Spanish BIP participants (Juarros-Basterretxea et al., 2018; Lila et al., 2018; Vargas et al., 2017). Motivation to change (Vargas et al., 2020). Facilitators rated participants’ motivation to change at the program intake using one item on a 5-point Likert-type scale, from 1 = not at all to 5 = very much. Stage of change (Carbajosa, Catalá-Miñana, Lila, Gracia, et al., 2017). Facilitators rated participants’ stage of change (1 = precontemplation, 2 = contemplation, 3 = preparation, 4 = action, 5 = maintenance). This measure has been used previously with Spanish samples of IPVAW perpetrators (Lila et al., 2018; Vargas et al., 2020). Analytic Plan The MCMI-III scales measuring alcohol and/or other drug abuse problems (cutoff score ≥ 75) were used to classify BIP participants into two groups, one with ADAPs (n = 204), and one without (n = 835). A series of univariate analyses were conducted to compare BIP participants with and without ADAPs in four sets of variables: 1) sociodemographic, 2) personality disorders and psychological adjustment, 3) social/relational variables, and 4) violence-related variables. For dichotomous variables, χ2-tests were carried out, and for polytomous variables, standardized residuals (Zresid) were computed to assess differences in the various categories (Agresti, 2019). For continuous variables, Welch’s t-tests were conducted, because this procedure is more robust when the homoscedasticity assumption is not met and the sample size is different in the two groups (Delacre et al., 2017; Fagerland & Sandvik, 2009; Howell, 2002; Ruxton, 2006; Wang, 1971). When running multiple univariate tests, the chance of making type I errors (i.e., false positives) increases, as more tests are conducted. For this reason, p-values were adjusted for each set of variables using the false discovery rate, a procedure aimed to control the expected proportion of significant results by penalizing the p-values associated with the null hypothesis (Benjami, 2010; Benjami & Hochberg, 1995). In addition to the adjusted p-values, different effect size measures were computed. Effect size measures reflect the distance between the groups compared and allow researchers to assess the magnitude of the differences found in the data. Hence, the larger the effect size for a given statistical test, the lower the likelihood of finding results biased due to sampling error (Fan, 2001; Kirk, 1996; Maher et al., 2013; Rosenthal, 1984; Sullivan & Feinn, 2012). Cramér’s V was computed to evaluate the effect size for dichotomous and polytomous variables, whereas Cohen’s d and Cohen’s U3 were obtained for continuous variables based on Hedge’s correction, which does not assume equal sample sizes for the groups (Hedges & Olkin, 1985). Cramér’s V ranges between 0 and 1 and indicates the strength of the association between two categorical variables, with values above .10, .30, and .50 indicating small, moderate, and large effect sizes, respectively (Cohen, 1988; Rea & Parker, 1992). Cohen’s d reflects the standardized mean difference between two groups (i.e., participants with and without ADAPs), and d values above 0.20, 0.50, and 0.80 are usually interpreted as small, moderate, and large effect sizes (Cohen, 1988). Cohen’s U3 is an analogous measure of Cohen’s d that expresses the proportion of participants of one group scoring higher than the average of the other group (Hanel & Mehler, 2019). Therefore, in this study we will focus on the effect size measures to interpret the results, in addition to the adjusted p-values, in order to ensure that the differences found between participants with and without ADAPS are substantive. Another advantage of focusing on effect size measures is that the statistical power also tends to be higher as the effect size estimates increase (Chow, 1988; Field, 2013). In our study, the sample size was large enough to ensure adequate statistical power for all tests. Particularly, for small effect sizes (i.e., d = 0.20) power ranged between 0.88 and 0.97 in our sample, meaning that the probability of making type II statistical errors (i.e., false negatives) were low. Power values above 0.80 are usually considered as acceptable for psychological research (Cohen, 1988). All analyses were conducted using the statistical package R (R Core Team. 2020), with psych and car libraries (Fox & Weisberg, 2019; Revelle, 2020). Sociodemographic Variables We first examined the differences between participants with and without ADAPs according to sociodemographic variables (Table 1). Although significant differences were found in employment and immigrant status, with higher unemployment (Zresid = 2.97) and lower proportion of immigrants (Zresid = -2.73) among participants with ADAPs, the effect sizes were negligible (VCramér < .10). Significant differences with a small effect size were found for age, indicating that participants with ADAPs were on average younger than those without ADAPs. No significant differences were found in educational level and income. Table 1 Differences between Participants with and without ADAPs in Sociodemographic Variables 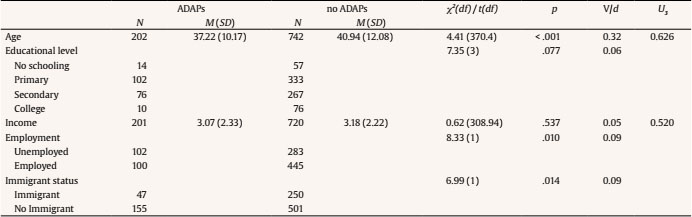 Note. ADAPs = batterer intervention program participants with alcohol and/or other drug abuse problems; no ADAPs = batterer intervention program participants without alcohol and/or other drug abuse problems. Personality Disorders and Psychological Adjustment Variables Regarding differences in personality disorders and psychological adjustment variables, significant differences with small effect sizes were found in narcissist and paranoid disorders, and in anger state. In all these variables, participants with ADAPs presented higher levels (Table 2). Specifically, 68.4% and 61.4% of participants with ADAPs had higher scores than the mean score of participants without ADAPs in narcissist and paranoid disorder subscales of the MCMI-III. For anger state this percentage was 60.3%. Significant differences with a small effect size were also found in self-esteem, with lower levels among participants with ADAPs (64.4% of them scored below the average of participants without ADAPs). Table 2 Differences between Participants with and without ADAPs in Personality Disorders and Psychological Adjustment Variables 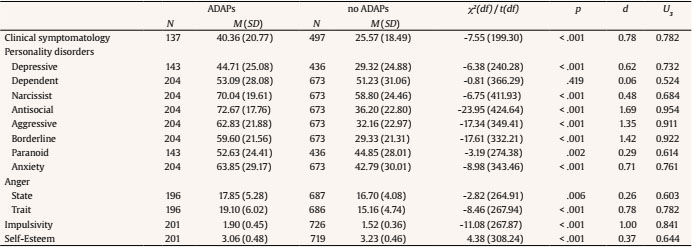 Note. ADAPs = batterer intervention program participants with alcohol and/or other drug abuse problems; no ADAPs = batterer intervention program participants without alcohol and/or other drug abuse problems. Significant differences with moderate effect sizes were found in clinical symptomatology (SCL-90), anger trait, and in anxiety and depressive disorder subscales of the MCMI-III. In all cases, participants with ADAPs showed higher levels than those without ADAPs. Specifically, 78.2% were above the average score of participants without ADAPs in both clinical symptomatology and anger trait. Regarding anxiety and depressive disorders, 76.1% and 73.2%, respectively, showed higher scores than the average of participants without ADAPs. Significant differences with large effect sizes were found in antisocial, borderline, and aggressive disorder subscales of the MCMI-III, indicating that 95.4%, 92.2%, and 91.1% of participants with ADAPs scored above the average of those without ADAPs in these variables, respectively. In addition, significant differences with a large effect size were found in impulsivity, with higher levels among participants with ADAPs (84.1% of them scored higher than the average of participants without ADAPs). Social/Relational Variables Regarding social/relational variables (Table 3), significant differences with small effect sizes were found in perceived social rejection, community, and intimate support. In particular, 64.1% of participants with ADAPs showed higher levels of perceived social rejection than the average of those without ADAPs. Participants with ADAPs also perceived significantly less community social support (i.e., community participation, community integration, and support from community organizations) and intimate support. Specifically, 60.3%, 58.7%, and 58.3%, and 57.9% of participants with ADAPs scored below the average of participants without ADAPs in these variables, respectively. Table 3 Differences between Participants with and without ADAPs in Social/Relational Variables  Note. ADAPs = batterer intervention program participants with alcohol and/or other drug abuse problems; no ADAPs = batterer intervention program participants without alcohol and/or other drug abuse problems. Significant differences with a moderate effect size were found in stressful life events, showing that participants with ADAPs presented a higher number of stressful life events (73.2% of them above the average number of stressful life events of participants without ADAPs). Violence-related Variables Finally, for the violence-related variables (Table 4), significant differences with small effect sizes were found in psychological violence, family violence exposure, and risk of future violence against partners and non-partners. Participants with ADAPs were more psychologically aggressive toward their partners, with 67.0% of them showing higher levels of psychological aggression than the average of participants without ADAPs. Participants with ADAPs were also more exposed to family violence in childhood (Zresid = 5.02), and had higher risk of future violence against partners and non-partners (Zresid = 3.91 and Zresid = 3.56, respectively) than participants without ADAPs. Table 4 Differences between Participants with and without ADAPs in Violence-related Variables 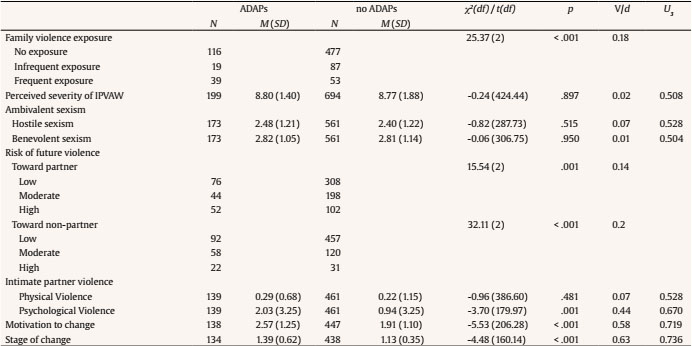 Note. ADAPs = batterer intervention program participants with alcohol and/or other drug abuse problems; no ADAPs = batterer intervention program participants without alcohol and/or other drug abuse problems. Significant differences with moderate effect sizes were found in motivation to change and state of change. Participants with ADAPs presented higher motivation to change and stage of change, with 71.9% and 73.6% of them scoring above the average of participants without ADAPs, respectively. No significant differences were found in perceived severity of IPVAW, hostile and benevolent sexism, and physical violence toward their partners. The aim of the present study was to identify the main risk factors and treatment needs of BIP participants with ADAPs, beyond their substance abuse problems, taking into account four sets of variables: sociodemographic, personality disorders and psychological adjustment, social-relational variables, and violence-related variables. Results from comparisons between BIP participants with and without ADAPs were interpreted in terms of effect sizes to highlight the most salient differences (i.e., moderate and large effect sizes) between these two groups of IPVAW offenders. Regarding the first set of variables, significant differences were found with negligible effect sizes for immigrant and employment status (lower proportion of immigrants and higher rate of unemployment among participants with ADAPs), and with a small effect size for age (participants with ADAPs were younger). However, no significant differences with moderate or large effects were found for sociodemographic variables. For the second set of variables (personality disorders and psychological adjustment variables), significant differences were found for all variables measured except for the dependent personality pattern. Traditional theoretical perspectives on the association between alcohol and IPVAW, such as the spurious model proposed by Leonard and Quigley (1999), suggest that personality and psychological symptomatology influence both drinking behavior and IPVAW. Likewise, alcohol and other drugs may influence psychological functioning because of the psychopharmacological effects they can have on emotional and cognitive processing (Hanson et al., 2011). In this study, however, not all differences in personality disorders and psychological adjustment variables were equally relevant. First, we found that participants with ADAPs showed higher scores in narcissistic disorder, paranoid disorder, and anger state, and lower scores in self-esteem than participants without ADAPs, although these significant differences all had small effect sizes. Second, significant differences with moderate effect sizes were found for clinical symptomatology, anger trait, anxiety disorder, and depressive disorder, with participants with ADAPs scoring higher than participants without ADAPs. Described in terms of Cohen’s U3, the percentages of participants with ADAPs that scored above the average of participants without ADAPs were 78.2% for clinical symptomatology and anger trait, 76.1% for anxiety disorder, and 73.2% for depressive disorder. Our results for clinical symptomatology and depressive disorder are consistent with previous research reporting higher levels of clinical symptomatology among offenders with substance abuse problems attending BIPs (Brown et al., 1999; Catalá-Miñana et al., 2013; Romero-Martínez et al., 2013; Thomas et al., 2013), and higher levels of depressive symptomatology among hazardous drinkers attending BIPs (Stuart et al., 2003). As for anger trait and anxiety disorder, our results are in line with research suggesting that higher alcohol and another substance use among individuals with these characteristics is a coping strategy to alleviate negative feelings (Eftekhari et al., 2004; Hofmann et al., 2009). Third, the most salient risk factors and treatment needs that emerged from our study in this second set of variables were impulsivity, antisocial disorder, borderline disorder, and aggressive disorder. Comparisons between participants with and without ADAPs in these variables yielded significant differences with large effect sizes. Described in terms of Cohen’s U3, the percentages of participants with ADAPs that scored above the average of participants without ADAPs were 84.1% for impulsivity, 95.4% for antisocial disorder, 92.2% for borderline disorder, and 91.1% for aggressive disorder. These results are in line with previous research showing higher levels of impulsivity in IPVAW offenders with ADAPs (Easton et al., 2008). Our results can also be linked to research showing that IPVAW offenders with antisocial, borderline, and aggressive personalities are more likely to have alcohol and drug problems (Fals-Stewart et al., 2005; Holtzworth-Munroe & Stuart, 1994; Klostermann & Fals-Stewart, 2006; Winters, 2005). Significant differences were found in all social-relational variables, the third set examined in this study. Although with small effect sizes, results showed that IPVAW offenders with ADAPs reported higher levels of perceived social rejection, lower levels of community support (participation, integration, and support from community organizations), and intimate support than participants without ADAPs. Stressful life events, with a moderate effect size, emerged as the most salient risk factor in this set of variables (73.2% of participants with ADAPs reported a higher number of stressful life events than the average of participants without ADAPs). Our results are in line with a substantial body of research linking stress and ADAPs (Armeli et al., 2007; Russell et al., 2017; Wills & Hirky, 1996). Violence-related variables was the fourth set of variables examined in this study. Although significant differences between participants with and without ADAPs were found in psychological violence, family violence exposure, and risk of future violence against partners and non-partners, with higher scores among participants with ADAPs, these differences had small effect sizes. Interestingly, the most salient factors found in this set of variables were motivation to change and stage of change, which presented significant differences between groups with moderate effect sizes. In terms of Cohen’s U3, 71.9% of participants with ADAPs showed higher motivation to change and 73.6% scored higher in stage of change than the average of participants without ADAPs. These results are consistent with Alexander and Morris (2008), who suggested that offenders with alcohol-related problems could be more motivated to change because their substance abuse can cause them feelings of distress and guilt, which act as internal motivations to change. Our findings have substantial treatment implications for BIP participants with ADAPs since the most salient risk factors and treatment needs we identified for these participants could be considered important intervention targets that go beyond their substance abuse problems. Clearly, substance abuse problems remain a key intervention target for BIP participants with ADAPs, and a major challenge is how to combine alcohol and drug abuse reduction strategies alongside IPVAW to produce better BIP outcomes. Bennett (2008) described different approaches to combine ADAPs and IPVAW interventions (i.e., consecutive, parallel or integrated interventions). Research seems to favor integrated interventions as they provide a number of advantages over consecutive and parallel approaches, such as needing fewer professionals, saving time, or increasing the probability of participants attending and completing the intervention (Gilchrist & Hegarty, 2017; Leonard & Quigley, 2017; McMurran, 2017). However, these different approaches to combine ADAPs and IPVAW treatments do not usually take into account other risk factors and treatment needs among participants with ADAPs such as those found in the present study. Several theoretical approaches have been proposed to guide and adjust interventions to increase sensitivity to BIP participants’ risk factors and treatment needs. Leonard and Quigley (2017) stressed the need to identify instigatory and inhibitory factors (i.e., risk and protective factors, respectively) underlying alcohol-related IPVAW, and suggested that interventions should address these factors because reducing or eliminating ADAPs alone may not be sufficient to prevent IPVAW occurring. Similarly, a review conducted by Massa et al. (2020) on the instigating-impelling-inhibiting model or “I3 model” (Finkel, 2007), highlighted the importance of developing specific treatment plans in BIPs targeting identified risk factors and treatment needs. Another theoretical approach to adjust interventions to participants risk and needs is the risk-need-responsivity (RNR) framework (Andrews & Bonta, 2010). In a meta-analysis and systematic review, Travers et al. (2021) found that when BIPs adhered to RNR principles results were more promising than the more traditional ‘one-size-fits-all’ intervention approach. Another important challenge for BIPs is how to take into account individual risk factors and treatment needs in a group format intervention. Research suggests that the group format used in the vast majority of BIP interventions (Babcock et al., 2016; Price & Rosenbaum, 2009) has some advantages over individual intervention formats. In this regard, Murphy et al. (2020) found that a group intervention program produced consistently equivalent or greater benefits than an individual intervention. For these authors, “the mutual support and positive social influence available in group intervention may be particularly helpful for IPV perpetrators” (p. 2847). The risk factors and treatment needs of participants beyond their ADAPs, such as the ones identified in our study, could be addressed by adapting and integrating some specific intervention strategies into group format BIPs. For example, BIP participants who present the risk factor of impulsivity could be given specific cognitive rehabilitation activities to do outside the sessions to help reduce it (Romero-Martínez et al., 2021). Intervention strategies could also be integrated in group format BIPs to address specific risk factors and treatment needs of participants with ADAPs, while at the same time benefiting all group participants. For example, strategies based on dialectical behavior therapy (Cavanaugh et al., 2011; Linehan, 1993) could be included in some group sessions to address problems of dependency and emotional instability associated with several personality disorders. Also, BIPs could integrate activities derived from mindfulness-based stress reduction group therapy to counteract stress and enhance psychological adjustment (Nesset et al., 2020). Finally, some general intervention strategies could also be particularly beneficial for BIP participants with ADAPs. For example, retention techniques to increase participants’ compliance with treatment and reduce dropout are particularly relevant for participants with ADAPs, given their high dropout rate from BIPs (Lila et al., 2020; Moore & Stuart, 2004; Olver et al., 2011). Previous research has found that participants with ADAPs who completed the intervention not only showed the same improvements in all intervention outcomes as participants without ADAPs, but also reduced their alcohol consumption (Lila et al., 2020). In turn, motivational strategies can also be particularly relevant for BIP participants with ADAPs. As we found in this study, participants with ADAPs presented higher motivation to change, and more advanced stage of change, suggesting that these participants are more aware of their need to change (Alexander & Morris, 2008). In this regard, a promising strategy to address individual risk factors and treatment needs of participants with ADAPs within a group format BIP is to use motivational strategies (e.g., motivational interviewing at intake) to establish individualized intervention goals, including those related to ADAPs, that can be addressed and monitored both individually and in group sessions (e.g., Lila et al., 2018; Romero-Martínez et al., 2009b; Santirso, Lila, et al. 2020). The present study has certain limitations. Several tests were conducted to assess the differences among participants with and without ADAPs. Although we focused on the interpretation of effect sizes rather than purely statistical significance (i.e., p-values), it is important to note that the effect size estimators used in this study depend on the statistics of their tests and their distributions (Maher et al., 2013). Although the cut-offs Cohen (1988) proposed for the size effect statistics are commonly applied, they are also arbitrary. We therefore urge a cautious interpretation of the variables close to these cut-offs using Cohen’s U3 as a measure of practical significance. Another limitation is the cross-sectional nature of this study, which precludes assessment of how the differences between participants with and without ADAPs might change during and after the intervention. Further, in terms of external validity, more research is needed to generalize these results to other samples, such as women perpetrators, the LGBTIQ+ population, and different ethnic groups. In conclusion, the literature has underscored the need to assess risk factors and treatment needs of participants with ADAPs to properly adjust BIPs to their specific characteristics. We tackled this issue by identifying the most salient risk factors and treatment needs of participants with ADAPs and by informing BIPs about potential intervention targets. Intervention strategies were also suggested to address the risk factors and treatment needs identified among participants with ADAPs. More efforts in this direction are required to improve BIP effectiveness by making interventions more sensitive and responsive to participants’ risk factors and treatment needs. Conflict of Interest The authors of this article declare no conflict of interest. Funding: This research was supported by the Spanish Ministry of Health, Consumption and Social Services, National Drugs Plan (PND2018/021). Cristina Expósito-Álvarez was supported by the FPU program of the Spanish Ministry of Universities (FPU19/05278). Cite this article as: Expósito-Álvarez, C., Lila, M., Gracia, E., & Martín-Fernández, M. (2021). Risk factors and treatment needs of batterer intervention program participants with substance abuse problems. The European Journal of Psychology Applied to Legal Context, 13(2), 87-97. https://doi.org/10.5093/ejpalc2021a9 References |
Cite this article as: Expósito-Álvarez, C., Lila, M., Gracia, E., & Martín-Fernández, M. (2021). Risk Factors and Treatment Needs of Batterer Intervention Program Participants with Substance Abuse Problems. The European Journal of Psychology Applied to Legal Context, 13(2), 87 - 97. https://doi.org/10.5093/ejpalc2021a9
Marisol.Lila@uv.es Correspondence: Marisol.Lila@uv.es (M. Lila).Copyright © 2026. Colegio Oficial de la Psicología de Madrid





 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
The European Journal of Psychology Applied to Legal Context is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License








