


Mediating Effects of Mindfulness Compassion-based Peer Counseling Program for Breast Cancer Survivors: From Mindfulness, Compassion to Others to Depression Reduction
Fei-Hsiu Hsiao1, 2, Chiao Lo3, Chiun-Sheng Huang3, 4, Wen-Hung Kuo3, 4, Feng-Ying Huang5, Yu-Ting Chen6, & Chia-Chen Hsieh7
1School of Nursing, College of Medicine, National Taiwan University, Taipei, Taiwan; 2Department of Nursing, National Taiwan University Hospital, Taipei, Taiwan; 3Department of Surgery, National Taiwan University Hospital, Taipei, Taiwan; 4Department of Surgery, College of Medicine, National Taiwan University, Taipei, Taiwan; 5Department of Education, College of Education, National Taipei University of Education, Taipei, Taiwan; 6School of Nursing, College of Medicine, Chang Gung University, Taoyuan City, Taiwan; 7School of Nursing, College of Nursing, Taipei Medical University, Taipei, Taiwan
https://doi.org/10.5093/pi2026a6
Received 18 September 2025, Accepted 12 December 2025
Abstract
Objective: The study aimed to test a mindfulness compassion-based intervention for breast cancer survivors serving as peer counselors, exploring whether mindfulness influenced depressive symptoms via a serial pathway of self-compassion, compassion to others, anxiety reduction, and improved quality of life. Method: This 8-month study adopted the randomized controlled trial (RCT) design. Survivors who are diagnosed with breast and complete treatments for at least one year were recruited from outpatient department of the General Hospital Breast Center and non-profit organization. They were randomly assigned into MC-BMS experimental group (the 8 weekly mindfulness compassion-based integrated with body-mind-spirit group therapy), and BMS control group (8 weekly body-mind-spirit group therapy). Results: There was a similarity in increasing general QOL functioning between the BMS and MC-BMS groups. The better improvements in QOL symptoms distress were more favored in MC-BMS than BMS groups. For within-group analyses, significant improvements in the MC-BMS group were depressive symptoms, search for meaning, mindfulness, while the BMS group showed significant improvements in global health, and breast cancer-related functioning. The three serial mediation pathways indicated that increases in mindfulness predicted greater self-compassion, which was associated with increased compassion to others. This, in turn, led to reduced anxiety, enhanced quality of life and breast cancer-related functioning, and ultimately, reduced depression. Conclusions: Enhancing mindfulness and compassionate processes in peer-counselor training serve a central role in improving anxiety and functional quality of life, thereby alleviating depressive symptoms in breast cancer survivors.
Keywords
Anxiety, Body-mind-spirit, Breast cancer, Compassion from others, Compassion to others, Depressive symptoms, Meaning in life, Mindfulness, Peer counseling program, Quality of life, Self-compassionCite this article as: Hsiao, F., Lo, C., Huang, C., Kuo, W., Huang, F., Chen, Y., & Hsieh, C. (2026). Mediating Effects of Mindfulness Compassion-based Peer Counseling Program for Breast Cancer Survivors: From Mindfulness, Compassion to Others to Depression Reduction. Psychosocial Intervention, 35, Article e260814. https://doi.org/10.5093/pi2026a6
Correspondence: cchsieh1116@gmail.com (C.-C. Hsieh).Breast cancer is the most common cancer among women, with approximately 20 million new diagnoses annually (World Health Organization, 2021). Advances in early screening and novel treatments have contributed to high survival rates. As a result, an increasing number of breast cancer survivors are engaging in volunteer work, offering peer support in hospitals or through non-profit organizations. Systematic reviews have demonstrated that peer support programs can significantly improve the psychological adjustment of newly diagnosed breast cancer patients or those undergoing active treatment (Hu et al., 2019). Nevertheless, providing peer support may expose survivors to empathy-based stress—emotional strain resulting from secondary or indirect trauma experienced through empathic engagement with others (Rauvola et al., 2019, p. 299). This exposure, coupled with their own past trauma and fear of cancer recurrence, may negatively impact on their well-being. Cultivating mindfulness self-compassion skills has been shown to alleviate empathy-based stress and improve emotional resilience (Jennings & Min, 2023). The review study by López-Contreras et al. (2024) showed that compassion-based interventions primarily focus on enhancing mindfulness and self-compassion skills among breast cancer patients to reduce emotional distress and improve quality of life. To date, however, these interventions have not been applied for breast cancer survivors learning about coping with the empathy-based stress they might experience when providing peer support to newly diagnosed patients. The impact of compassion training on their perceptions of compassion competency to others is also not well-examined. Therefore, there is an urgent need to develop mindfulness compassion programs specifically tailored for breast cancer survivors who are interested in becoming peer supporters. The peer counselor refers to someone who is trained and supervised in breast cancer survivors, providing information and emotional support and assisting newly dianogsed breast cancer patients to find community resources (Giese-Davis et al., 2006; Giese-Davis et al., 2016). Giese-Davis et al. (2006) and Giese-Davis et al. (2016) developed a peer counselor’s training program via group format, which consisted of a lecture from an oncologist about breast cancer treatments, a nurses’ lecture about side effect managements, a lecture on active listening skills, and a role play in learning how to do active listening. They observed that breast cancer survivors’ emotional suppression increased after they provided peer counseling for patients. Their tendency toward emotional suppression may reflect the insufficient emphasis on self-care and emotional regulation skills in current peer-counselor training programs (Lu et al., 2014; Moon et al., 2017; Schover et al., 2011; Toija et al., 2018). Therefore, peer-counselor training needs to strengthen breast cancer survivors’ self-compassion skills to better support newly diagnosed patients. Self-compassion consists of self-kindness without self-judgment, mindful awareness of painful feelings, and recognition that suffering is a common human experience (Neff, 2023). Breast cancer-related stimuli can intensify patients’ negative interoceptive sensations and dysfunctional cognitive appraisals, such as a negative body image and fear of cancer recurrence (Sebri et al., 2020). Unlike cognitive-behavioral interventions, which focus on modifying irrational or dysfunctional thoughts and identifying the sources of negative or fear-laden internal sensations, self-compassion interventions cultivate mindful and non-judgmental awareness of the self. This approach can foster more positive interoceptive experiences and enhance feelings of bodily reassurance and self-concept (Sebri & Pravettoni, 2023). A review of nine RCTs by López-Contreras et al. (2024) found that compassion-based interventions have positive outcomes for breast cancer patients, including reductions in depression and anxiety, improvements in coping skills (mindfulness and self-compassion), and enhanced quality of life. These interventions mainly include activities such as self-kindness meditation and writing, mindful awareness and savoring of positive events, gratitude practices, and acts of self-kindness. While most compassion-based interventions focus on cultivating self-compassion, few incorporate trainings in compassion to others. For peer counseling programs, both self-compassion and compassion to others are essential for helping breast cancer survivors develop the emotional regulation skills needed to cope with empathy-based stress. According to Gilbert et al.’s (2017) emotional regulation model, compassion operates through three flows: self-compassion, compassion from others, and compassion for others. These flows are moderately correlated, suggesting that increases in self-compassion may strengthen one’s capacity to show compassion toward others. Compassion-Focused Therapy (CFT) aims to cultivate skills in all three flows—being compassionate toward oneself, receiving compassion from others, and extending compassion to others—to enhance feelings of inner warmth, safety, and soothing within the emotional regulation system (Gilbert, 2014, 2017). Evidence shows that CFT can reduce depressive symptoms among breast cancer patients (Dodds et al., 2015; Gilbert & Choden, 2014; Sadeghi et al., 2018). Through CFT, breast cancer patients may respond to bodily changes with greater flexibility and increase compassion toward both themselves and others. Given the observed correlations between self-compassion and compassion to others (Gilbert et al., 2017), it remains unclear whether the mechanisms underlying the effects of compassion-based programs operate through changes in mindfulness, self-compassion, and compassion to others, ultimately influencing breast cancer survivors’ quality of life and depression. The review by López-Contreras et al. (2024) found that compassion-based interventions for breast cancer patients generally do not include the contents of coping with the disease or treatment side effects to improve quality of life. Breidenbach et al. (2022) reported that physical symptoms and impairments are associated with depression and anxiety among breast cancer survivors. Therefore, in this study, our peer-counselor training program integrates both Gilbert’s Compassion-Focused Therapy (CFT) and Body-Mind-Spirit (BMS) group therapy (Hsiao et al., 2012; Hsiao et al., 2022). This combined approach is designed to provide BMS empowerment strategies that help breast cancer patients cope with cancer and treatment side effects, while also strengthening their competencies in both self-compassion and compassion for others. This study examined the effects of mindfulness-compassion therapy integrated with body-mind-spirit (MC-BMS) in peer-counselor training on reducing depressive symptoms for breast cancer survivors. It also investigated the serial mediation effects of mindfulness, self-compassion, and compassion to others on survivors’ quality of life (QoL) and depression. The study hypothesized that MC-BMS enhanced peer-counselor training would lead to reductions in depression among breast cancer survivors. It further hypothesized that mindfulness, self-compassion, and compassion to others would serve as serial mediators of the intervention’s effects on QoL and depression. Trial Design and Setting This study was designed as a randomized controlled trial (RCT) using a parallel-group, superiority framework with an allocation ratio of 1:1. Participants were recruited from the outpatient Breast Center of the hospital and a collaborating non-profit breast cancer organization. All interventions and outcome assessments were delivered in outpatient settings. Eligibility Criteria Eligible participants were breast cancer survivors who had completed active treatment at least one year prior, were between 20 and 65 years of age, and expressed interest in serving as peer counselors. Participants were excluded if they were currently receiving psychotherapy, participating in other mindfulness, meditation, or psychosocial well-being programs, or had initiated such programs within the previous three months. Co-interventions were monitored by asking participants during baseline, post-intervention, and follow-up assessments whether they were receiving any concurrent psychological treatment or had joined any new well-being programs during the study period. Intervention Participants were randomly assigned to one of two training groups: the experimental MC-BMS group (the mindfulness compassion-based integrated with body-mind-spirit group therapy, 120 minutes every week for 2-month) or the active control BMS group (body-mind-spirit group therapy, 120 minutes every week for 2-month). Both the BMS and MC-BMS intervention groups were delivered by the first author (Hsiao), who has formal training in body-mind-spirit (BMS) therapy, mindfulness-based practices, and compassion-focused therapy. She has extensive experience in developing and delivering BMS, mindfulness, and compassion-focused interventions for individuals affected by cancer (Hsiao et al., 2012; 2022). Her training and clinical expertise ensured consistent and competent delivery of the intervention content across both groups. Fidelity was maintained by delivering the intervention using a manualized protocol. After each session, the interventionist completed a standardized fidelity checklist derived from the intervention manual to document adherence to the prescribed content and procedures. The peer-counselor’s training program aims to enhance breast cancer survivors’ body-mind-spirit (BMS) holistic well-being, emotional regulation skills (mindfulness, self-compassion, and compassion to others), spiritual growth (meaning in life), and their ability to provide information and emotional support for breast cancer patients. Therefore, the program consists of BMS holistic empowerment strategies, mindfulness with compassion skills, education for disease and treatment-related knowledge, health-related resources, communication skills, and active listening. Body-mind-spirit (BMS) group therapy was developed in our previous study to enhance breast cancer survivors’ inner strengths and resilience in coping with stress (Hsiao et al., 2012). The empowerment activities in BMS therapy address survivors’ holistic needs, including physical discomfort related to treatment-induced late side effects, emotional distress and fear of recurrence, and spiritual uncertainty regarding the meaning of life. The structured mindfulness integrated BMS group therapy further developed in our previous study effectively reduces lung cancer patients’ depressive symptoms (Hsiao et al., 2022). Mindfulness integrated with BMS holistic empowerment strategies could manage symptom distress and help patients to pay attention to the present moment to disengage them from rumination on past events and fear of death in the future. This study adds the compassion component to train empathy toward self and others and prevent self from empath-based stress. For compassion skills, this study applied the concept of three flows of compassion (self-compassion, compassion from others, compassion to others) and compassion practices from compassion-focused therapy developed by Gilbert and Choden (2014). Compassion-focused practices include mindfulness, soothing breath rhythm, compassionate imagery (creating a safe place, compassionate colors), meditation, and compassionate letter writing. They were encouraged to complete homework practice using audio-supported guided breathing and meditation (body scan, self-compassion, receiving compassion from others, and compassion to others). Group therapy for both the experimental group (MC-BMS) and the control group (BMS) was conducted in small groups of 8-10 survivors, for 120 minutes each week over a 2-month period, and was facilitated by the principal investigator (Hsiao). The primary difference between the two groups was the inclusion of emotional regulation skills training: the MC-BMS program incorporated structured mindfulness, self-compassion, and compassion to others practices, whereas the BMS program included only mindfulness breathing and guided imagery. Both the MC-BMS and BMS programs involved practicing BMS holistic empowerment activities and learning how to provide informational and emotional support to breast cancer patients. Table 1 outlines the content of the MC-BMS program. Each MC-BMS session consisted of 50 minutes of structured mindfulness and compassion training, along with time for participants to share their daily practice experiences. The remaining 70 minutes focused on demonstrating and discussing BMS empowerment activities and providing health-related educational information on self-care and care for newly diagnosed breast cancer patients. In the BMS group, more time (90 minutes) was dedicated to sharing and discussing experiences related to BMS empowerment activities and health-related education, while 30 minutes were allocated to mindfulness breathing and guided imagery. Table 1 The Content Ooutline for the Compassion-based with Body-Mind-Spirit (MC-BMS) Group Therapy 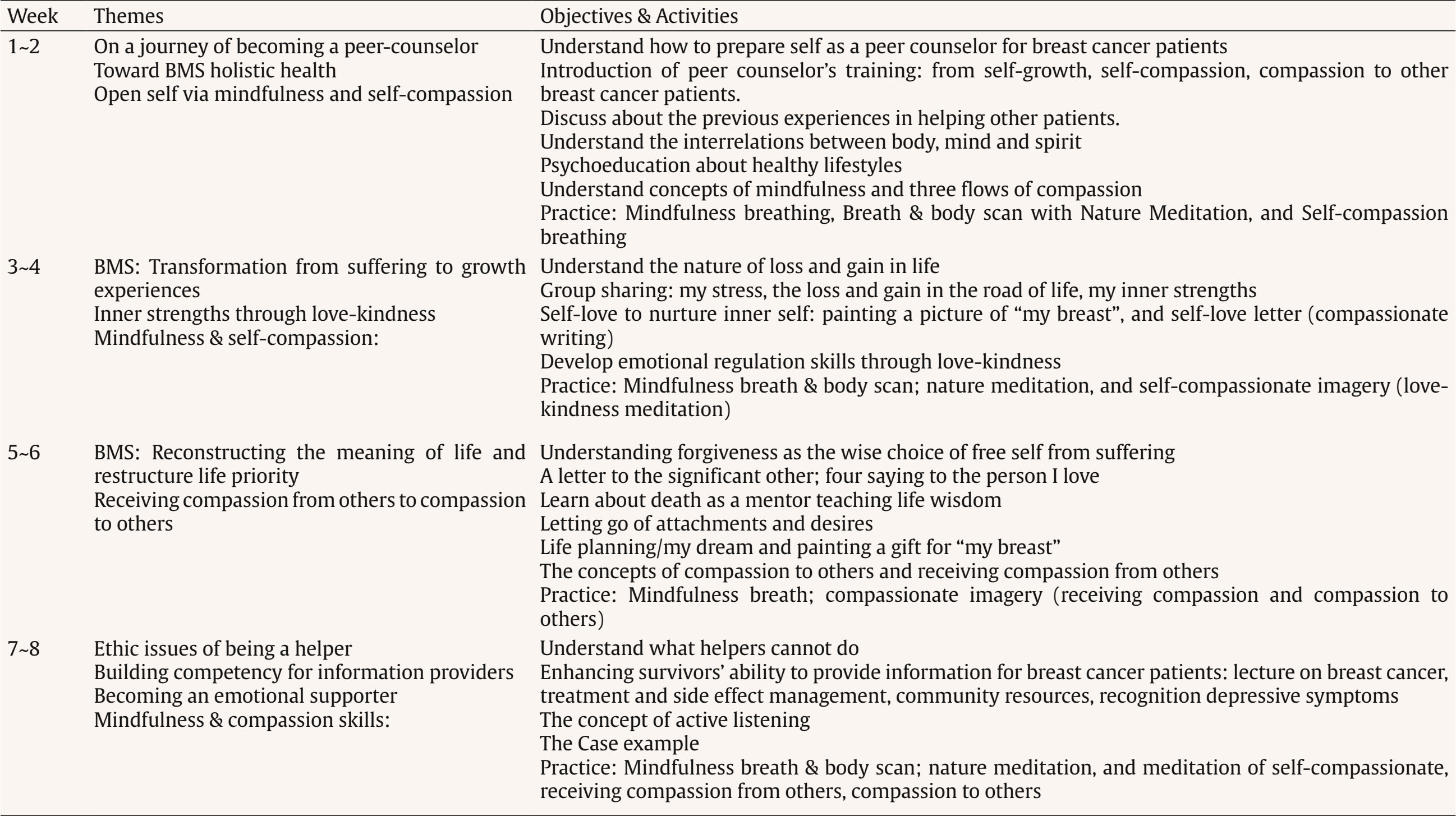 Measurements The primary outcome was depressive symptoms. Secondary outcomes were anxiety, quality of life, mindfulness, self-compassion, compassion to others, and meaning in life. Beck Depression Inventory-II (BDI-II) The BDI-II is a 21-item self-report instrument designed to assess the severity of depressive symptoms (Beck et al., 1996). Scores range from 0 to 63, with higher scores indicating greater levels of depression. In this study, the BDI-II demonstrated good internal consistency (Cronbach’s α = .90). State-Trait Anxiety Inventory (STAI) Developed by Spielberger (1970), the STAI measures state anxiety. The scale consists of 20 items rated on a 4-point scale, with total scores ranging from 20 to 80. Higher scores indicate greater anxiety. In this study, the STAI demonstrated excellent internal consistency (Cronbach’s α = .96). Five Facet Mindfulness Questionnaire (FFMQ-15) The FFMQ-15 is a 15-item self-report scale developed by Baer, Carmody, et al. (2012), will be used to assess mindfulness in this study. The scale measures five dimensions of mindfulness: observing, describing, acting with awareness, nonjudging, and nonreactivity. Items are rated on a 5-point scale from 1 (rarely true) to 5 (always true), with higher scores indicating greater mindfulness. Total and subscale scores are derived from the sum of item scores. In this study, the FFMQ-15 demonstrated acceptable internal consistency (Cronbach’s α = .83). Self-Compassion Scale It is a 13-item scale consisting of an engagement subscale assessing an individual’s ability of being sensitive to their own distress/suffering and engagement with suffering, and an actions subscale assessing an individual’s ability to be motivated to alleviate and prevent distress (Gilbert et al., 2017). Each item is rated on a 10-point Likert scale ranging from 1 (never) to 10 (always). The two subscales can be summed to obtain a total score, with higher scores indicating higher levels of self-compassion. In this study, the scale demonstrated acceptable internal consistency (Cronbach’s α = .74). The Compassion to Others Scale It is a 13-item self-report measure designed to assess the ability to be compassionate to others (Gilbert et al., 2017). It consists of an engagement subscale assessing an individual’s ability of being sensitive to others’ needs, capable of noticing to distress signals, and capable of non-judgmental empathic connection with the suffering of others, and actions subscale assessing an individual’s ability to be motivated to be helpful to people. Each item is rated on a 10-point Likert scale ranging from 1 (never) to 10 (always). The two subscales can be summed up to obtain a total score, with higher scores indicating higher levels of compassion to others. In this study, the scale demonstrated acceptable internal consistency (Cronbach’s α = .80). Meaning in Life Questionnaire (MLQ) The MLQ consists of two subscales: the 5-item MLQ-Presence subscale, measuring the subjective sense that one’s life is meaningful, and the 5-item MLQ-Search subscale, measuring the drive and orientation toward finding meaning in one's life (Steger et al., 2006). Items are rated on a 7-point scale from 1 (absolutely untrue) to 7 (absolutely true), with higher scores reflecting greater meaning in life. Both MLQ subscales showed good reliability, with α = .90 for Presence and α = .87 for Search. Quality of Life Questionnaire Quality of life was assessed using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire–Core 30 (EORTC QLQ-C30), a 30-item instrument comprising five functional scales (physical, role, cognitive, emotional, and social functioning), eight symptom scales (fatigue, nausea/vomiting, pain, dyspnea, insomnia, appetite loss, constipation, and diarrhea), and a global quality-of-life scale (Aaronson et al., 1993). The EORTC QLQ-BR45 (Bjelic-Radisic et al., 2020) is an updated version of breast cancer-specific questionnaire to access the impact and side-effects of current BC therapy on QOL. The QLQ-BR45 assesses body image, sexual functioning, breast satisfaction, systemic therapy side effects, arm and breast symptoms, endocrine therapy symptoms, skin mucosis symptoms, endocrine sexual symptoms, and three single-item to assess sexual enjoyment, future perspective, and being upset by hair loss. All scales range in score from 0 to 100. Higher scores indicate higher levels of functioning and symptom distress. Internal consistency was acceptable in this study (mean Cronbach’s alpha > .70). Harms Harms were defined as any unexpected psychological distress or discomfort during or after the intervention. At each session, participants were asked about adverse effects, and the interventionist noted any observed distress. No harms or adverse events were reported in either group. Given that the intervention was minimal-risk and psychological in nature, no formal stopping rules were required, and participants were free to withdraw from the study at any time. Sample Size To detect small effects in an active-active trial design (BMS vs. MC-BMS), we used a small standardized effect size (d = 0.20), corresponding to a mean difference of 0.20 with an SD of 1. Based on a superiority framework (superiority margin = .05), a two-sided α = .05, 80% power, and a 1:1 allocation ratio, the required sample size was 35 participants per group. The achieved sample sizes (39 and 38 per group) fall within recommended ranges for studies designed to detect small effects. Randomization An independent researcher generated the random allocation sequence using a computer-based randomization program. The allocation sequence was kept by the independent researcher and concealed from the study team until baseline assessments were completed. A research assistant, who was not involved in intervention delivery, informed participants of their assigned group according to the concealed sequence. Blinding Due to the nature of the behavioral group interventions, participants and the interventionist could not be blinded to group assignment. However, outcome assessment and data analysis were blinded. All collected data were de-identified and coded by research staff who were not involved in intervention delivery. The statistician conducting the analyses was blinded to group allocation until all primary analyses were completed. This procedure minimized risk of bias in outcome interpretation. Procedure Ethical approval was obtained from the Institutional Review Board of a university-affiliated hospital (REC No: 202112066RIND). Eligible breast cancer survivors were identified through the Breast Center of the hospital and a collaborating non-profit organization. Potential participants were approached during clinic visits or contacted by telephone or email. A trained research assistant explained the study procedures, and written informed consent was obtained prior to enrollment. Outcome assessments were conducted at baseline, immediately after the 2-month intervention, and at four planned follow-up points. Participants completed mailed questionnaires and returned them using prepaid envelopes. All procedures performed in the studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study protocol was approved by the Institutional Review Board of the National Taiwan University Hospital (REC No: 202112066RIND). Data Analysis All statistical analyses were performed using IBM SPSS Statistics. An intention-to-treat approach was adopted, and missing data were handled using available observed data without any ad hoc imputation. To account for the correlated nature of repeated measures, intervention effects on outcome variables were assessed using Generalized Estimating Equations (GEE) with an autoregressive correlation structure (AR1). Significant group-by-time interactions were interpreted as evidence of differential intervention effects over time between groups. In addition, within-group changes over time were examined to assess the intervention’s impact on each group independently. To examine whether the intervention effects varied according to participants’ demographic characteristics, clinical variables, baseline levels, or adherence to the intervention, moderation analyses were conducted using the PROCESS macro (Model 1) in SPSS (Hayes, 2017). For each significant moderator, simple slope analyses were performed to further probe the interaction effects at ± 1 standard deviation from the mean of the moderator variable. Serial mediation analyses were conducted using PROCESS Models 6 (Hayes, 2017). Because mediators and outcomes were assessed at the same time points, mediation was evaluated using change scores across the intervention period. The hypothesized ordering of mindfulness → self-compassion → compassion to others → psychological functioning (anxiety, meaning in life, quality of life) → depression reflects the theoretical progression of skills emphasized in the intervention program. As both groups were expected to show psychological improvement, mediation analyses were conducted using the full sample. Indirect effects were tested using 5,000 bias-corrected bootstrap resamples, with statistical significance determined by 95% confidence intervals that excluded zero. A total of 406 potential participants were assessed for eligibility. Of these, 23 did not meet the inclusion criteria and 305 declined participations. The main reasons for declining were lack of interest (n = 76) and time constraints due to busy schedules or long distance (n = 229). Ultimately, 78 participants completed baseline assessments. One participant withdrew due to physical health issues, leaving 77 participants who were randomized to either the BMS group (n = 39) or the MC-BMS group (n = 38). At follow-up, 72 participants (94%) completed the T1 assessment, 71 (92%) completed the T2 assessment, and 67 (87%) completed the T3 assessment. Attrition was primarily due to participants declining further follow-up assessments. Details of participant flow are presented in Figure 1. There were no significant differences in attrition between the two groups on most demographic variables and baseline scores (p > .05). However, a chi-square test showed a significant association between marital status and attrition, χ²(1) = 5.12, p = .02. The attrition rates were higher among unmarried participants (24%) compared to married participants (6%). In addition, participants who dropped out of the study scored significantly lower on compassion to others at baseline (mean = 65.70, SD = 6.73) compared to those who remained in the study (mean = 72.46, SD = 11.56), t(75) = 1.80, p = .04. This suggests that lower levels of compassion to others may be associated with increased attrition. Figure 1 Study Flowchart. 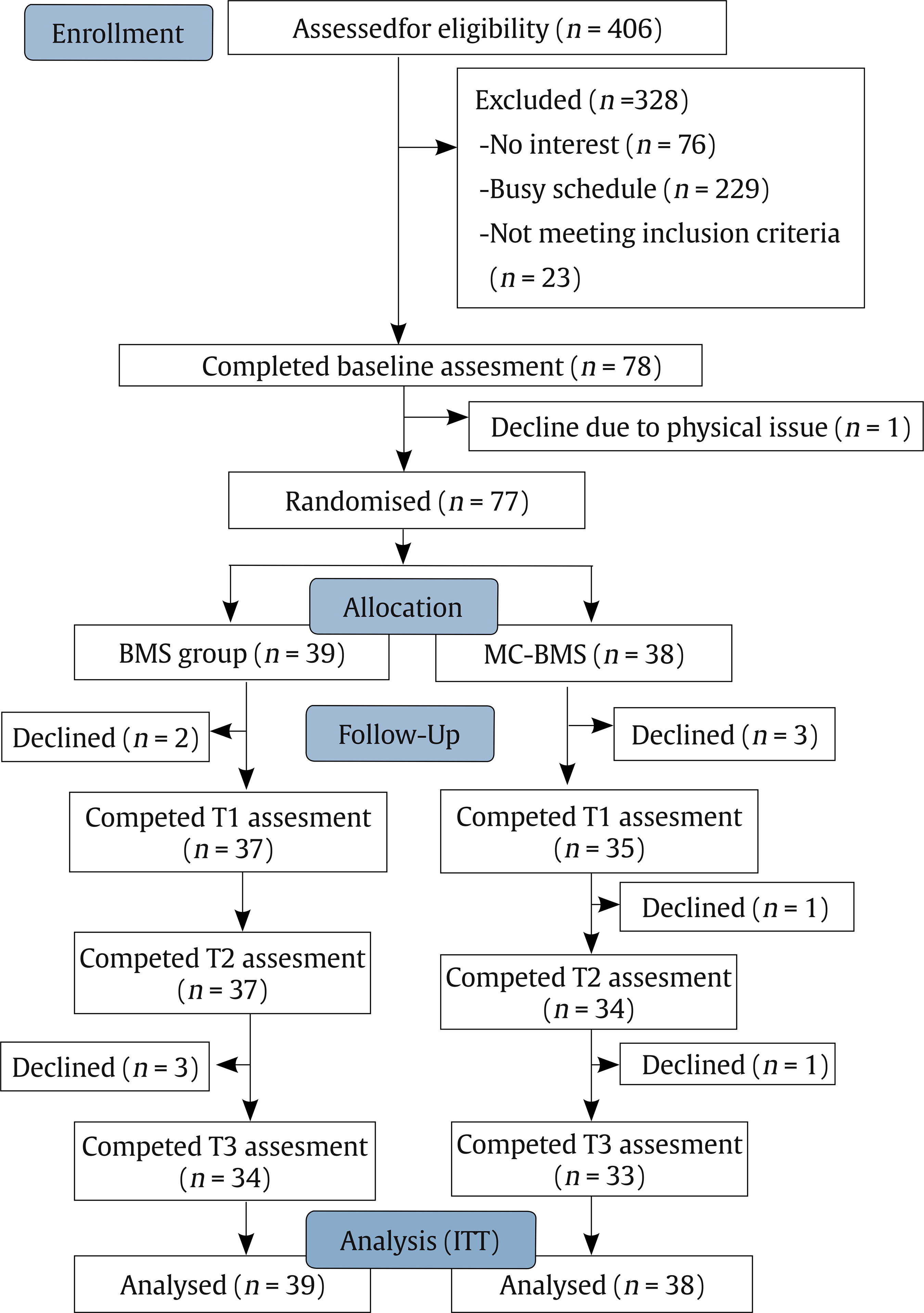 Table 2 presents the baseline demographic and clinical characteristics of participants in the BMS and MC-BMS groups. No significant differences were found between groups across any baseline variables (all p > .05), indicating comparability prior to the intervention. Session attendance was recorded for all participants. The mean (SD) number of sessions attended was 6.62 (2.93) for the BMS group and 6.18 (2.56) for the MC-BMS group (range: 0-12), with no significant difference between groups (p > .05). Table 2 Demographic and Clinical Characteristics at Baseline for Breast Cancer 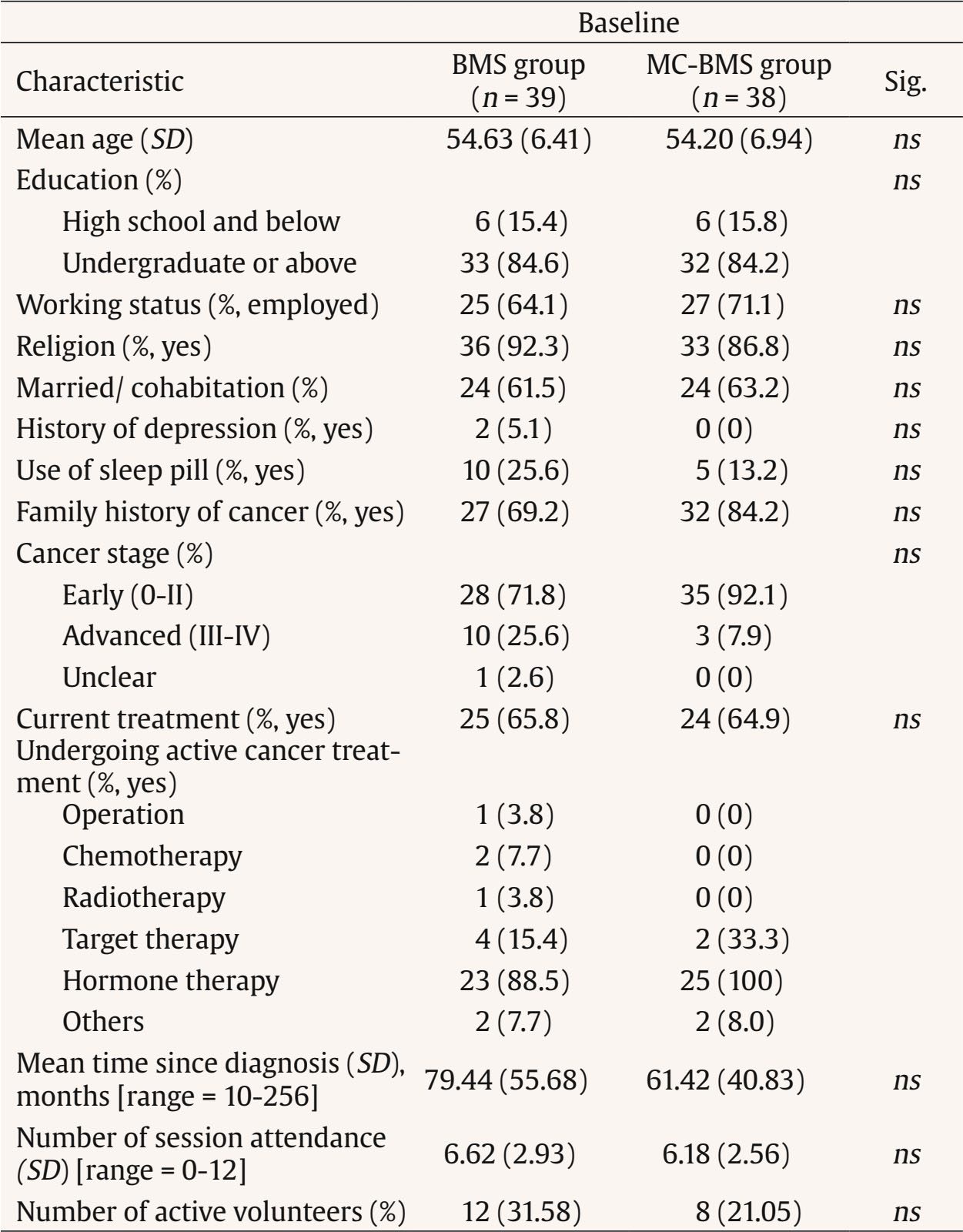 Note. Abbreviation: ns, nonsignificant. Table 3 summarizes the within-group and between-group effects on the outcome measures. Most outcomes did not differ significantly between the BMS and MC-BMS groups (all p > .05), except for QOL symptom distress, which favored the MC-BMS group, Wald χ²(3) = 10.66, p = .014. Within-group analyses indicated significant improvements in overall QOL functioning for both groups, BMS: Wald χ²(3) = 12.12, p = .01; MC-BMS: Wald χ²(3) = 9.45, p = .02. In the MC-BMS group, additional improvements were observed for depressive symptoms, Wald χ²(3) = 11.43, p = .01, search for meaning, Wald χ²(3) = 9.70, p = .02, and mindfulness, Wald χ²(3) = 10.85, p = .01. In contrast, the BMS group showed improvements in global health, Wald χ²(3) = 8.22, p = .04, and breast cancer-related functioning, Wald χ²(3) = 9.49, p = .02. These findings suggest that while both interventions produced beneficial outcomes, BMS was more effective in enhancing breast cancer–specific quality of life, whereas MC-BMS offered additional psychological and existential benefits, particularly in reducing depression, enhancing mindfulness, and fostering meaning in life. Table 3 Intervention Effects for Breast Cancer Survivors Serving as Peer Counselors 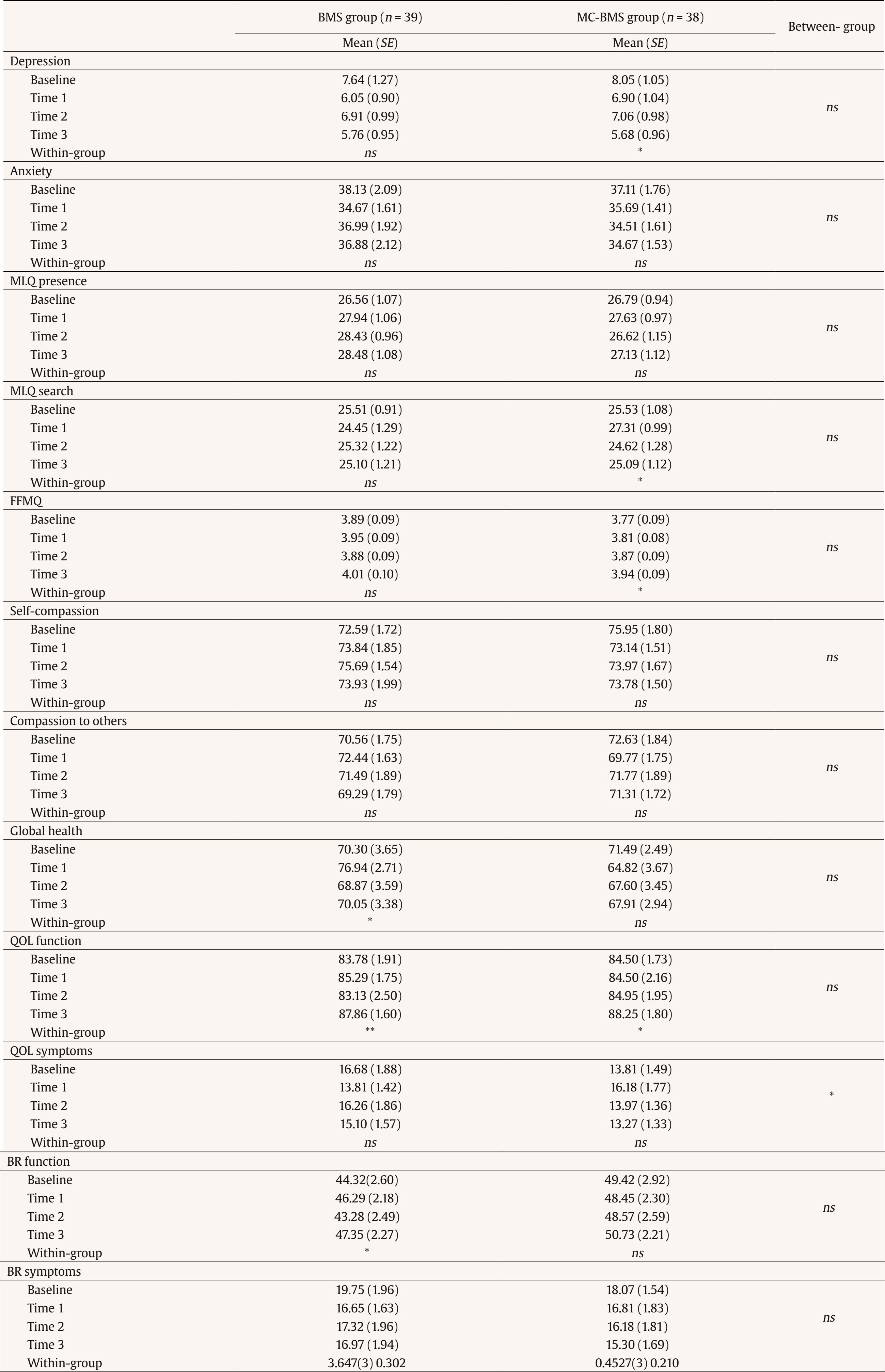 Note. Abbreviation: ns = non significant. *p < .05, **p < .01, ***p < .001. Moderator analyses were further performed to explore which subgroups of participants benefit most from the MC-BMS program. However, none of the tested variables—including demographic characteristics, baseline levels of depression, anxiety, or symptom distress—significantly moderated the intervention effects. The data suggested that the MC-BMS program could be benefited for breast cancer survivors with different background and conditions. Figure 2 illustrates three proposed serial mediation pathways of how mindfulness, self-compassion, and compassion to others influence reductions of depression through their impacts on anxiety and QOL. For the first pathway, increases in mindfulness predicted greater self-compassion, which in turn was associated with increased compassion to others and subsequently reduced anxiety. This reduction in anxiety was associated with lower depressive symptoms (indirect effect = -.229, BootSE = .208, 95% BootCI = [-.803, -.021]). For the second pathway, improvements in mindfulness, self-compassion, and compassion to others led to enhanced QOL functioning, which was also associated with reductions in depression (indirect effect = -.287, BootSE = .180, 95% BootCI = [-.732, -.043]). Thirdly, the pathway also showed the positive changes mindfulness, self-compassion, and compassion to others led to increasing breast cancer–related functioning, which was further associated with reducing depressive symptoms (indirect effect = -0.167, BootSE = .208, 95% BootCI = [-.774, -.001]). These pathways suggest the central role of mindfulness and compassionate processes in improving both anxiety and functional quality of life, which in turn alleviate depressive symptoms in breast cancer patients. Figure 2 Proposed Mediating Pathways Linking Mindfulness to Depression among Breast Cancer Survivors. 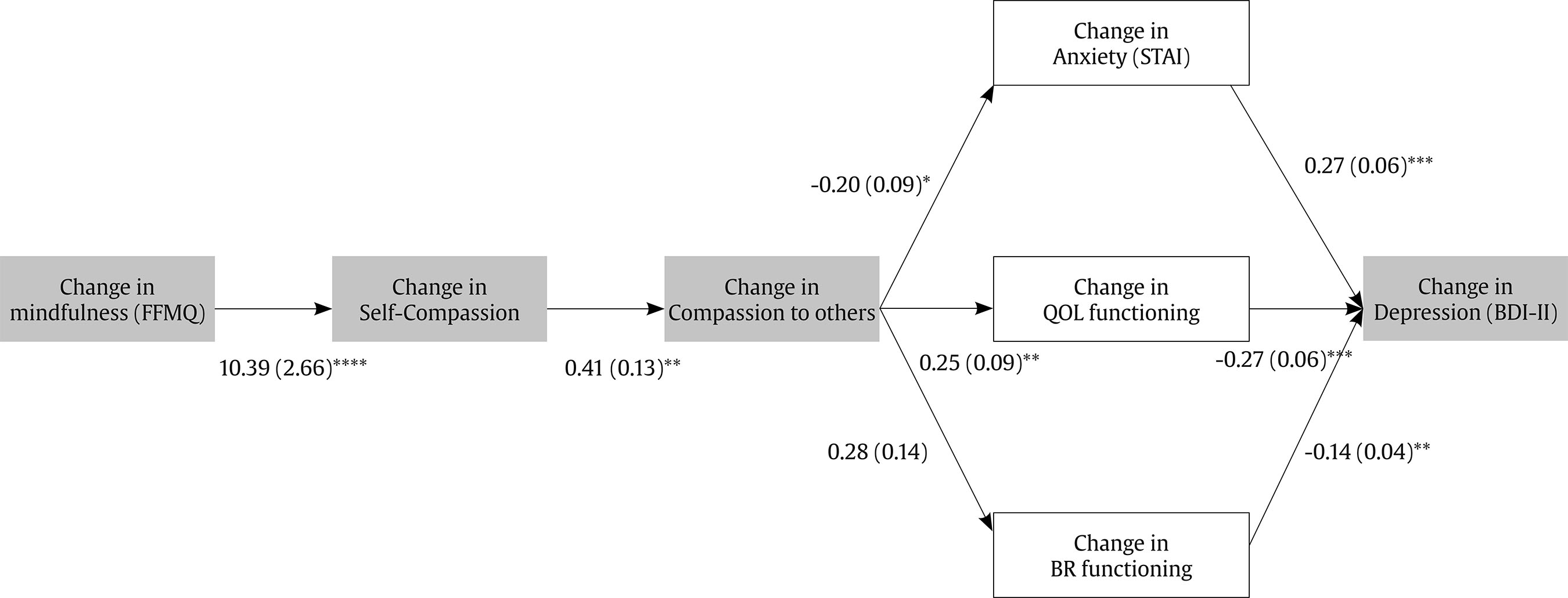 This study found that both BMS and MC-BMS contribute to increasing general QOL for breast cancer survivors while QOL symptom distress reduced more significantly in MC-BMS than BMS groups. For within-group analyses, MC-BMS group showed the more significant improvements in depressive symptoms, search for meaning, and mindfulness, while the BMS group showed significant improvements in global health, and breast cancer-related functioning. The findings suggest that in addition to general QOL, MC-BMS may offer additional benefits for psychological and existential dimensions such as depression, mindfulness, and searching for meaning. Our MC-BMS program combined structured mindfulness and three-flow compassion skill training. Mindfulness and self-compassion both increase physical and mental health (Schutte & Malouff, 2025). The previous study also suggested that included mindfulness and self-compassion skills training could contribute to the beneficial well-being outcomes (Conversano et al., 2020). Based on moderator analyses, none of the factors significantly moderate the intervention effects, which suggested that the MC-BMS program could benefit breast cancer survivors with different backgrounds and conditions. Consistent with the recent review study on compassion-based therapy for breast cancer survivors and patients (López-Contreras et al., 2024), our MC-BMS program also showed the positive outcomes of reducing depression, increasing mindfulness, and quality of life for breast cancer survivors. Moreover, MC-BMS also increased actively searching for positive meanings in their lives, which suggested that cultivating compassion might enhance breast cancer survivors their positive spiritual growth. The review study on general population (Ahmed & Gupta, 2024) found that self-compassion and compassion to others was positively correlated to increasing a sense of meaning in life. Self-compassion process might facilitate breast cancer survivors’ feelings deep within self, which might enter self-discovery journey of spiritual growth and enhance their motivation to find meaning in their lives after a cancer event. Compassion to others process might increase survivors to connect with their surroundings and care for others’ well-being, which might reflect the spiritual growth such as awareness of shared humanity, exploring meaning of life purposes, and transforming toward a state of harmony. MC-BMS consisting of practicing self-kindness and compassionate caring toward others likely increased their emotional regulation skills and subsequently enhanced their spiritual growth. In this study, MC-BMS did not show the direct effect on the changes of self-compassion and compassion to others in MC-BMS or BMS groups. The scores on self-compassion and compassion to others average at 70 above in MC-BMS and BMS groups, which suggests having a ceiling effect to detect the significant changes after intervention. The ceiling effect might be related to our included participants who are interested in becoming a peer counselor, and therefore, they might be more motivated toward self-compassion and compassion to others. Moreover, the attrition was associated with lower levels of compassion to others scores at baseline, which might also influence the observation of changes after intervention. Nevertheless, they played the mediator roles in reducing depression. This study identified three serial mediation pathways that showed increases in mindfulness predicted greater self-compassion, which was associated with increased compassion to others. This mindfulness compassion process led to reduced anxiety, enhanced quality of life and breast cancer-related functioning, and ultimately, reduced depression. This finding demonstrated mediation effect began with mindfulness enhancing self-compassion. The meta-analysis study (Schutte & Malouff, 2025) also identified the positive correlation of mindfulness with self-compassion among a varied population, and mindfulness could facilitate self-compassion. Mindfulness develops the present-moment awareness of self without over-reactivity and non-judgement, which could facilitate nature self-compassion such as the awareness of suffering without over-identification or over-reactivity and taking kindness attitude toward self (Baer, Lykins, et al., 2012; Neff, 2023). In our serial mediation pathway, increased self-compassion further fostered compassion to others. In our study, the design of MC-BMS is building breast cancer survivors’ mindfulness and self-compassion activities first followed by compassion to others meditations. In Gilbert’s emotional regulation model, self-compassion, compassion from others, and compassion to others are moderately correlated to one another (Gilbert et al., 2017). The review study (Ahmed & Gupta, 2024) found that cultivating self-compassion which enhanced self-awareness, self-acceptance, and self-kindness facilitated a flow of compassion toward others. With self-care motivation increasing inner warmth safeness can be directed towards others (Gilbert & Van Gordon, 2023). Neff (2023) also thought that common humanity, the aspect of self-compassion, could enhance connectedness of understanding others’ suffering and life challenges (Neff, 2023). In conclusion, MC-BMS could improve general QOL and psychological and existential aspects of effects such as depression, mindfulness, and searching for meaning. The serial mediation pathways indicated that enhancing mindfulness and compassionate processes in peer-counselor training serve a central role in improving anxiety and functional quality of life, thereby alleviating depressive symptoms in breast cancer survivors. Limitations and Future Research This study has several limitations. First, the relative refusal rate at enrollment may restrict the generalizability of the findings. The main reasons for not participating in this study were time constraints due to busy schedules or long distances (n = 229). The format of in-person training program might be the reason for this limitation. Another reason included lack of interest (n = 76), which suggested that individuals who agreed to participate may have been more motivated toward compassion to others. Second, although overall attrition was low, attrition was significantly associated with unmarried participants and lower levels of compassion to others scores at baseline, suggesting that lower compassion to others may reduce motivation to engage in peer counseling. Third, the study sample was limited to breast cancer survivors with early-stage disease (Stage 0-II). As a result, the effectiveness of MC-BMS for survivors with more advanced disease (Stage III-IV) remains unclear. Fourth, potential biases related to self-reported outcomes need to be addressed. These include a lack of self-awareness regarding one’s psychological status, misinterpretation of questionnaire items, and responding in socially desirable ways. Future studies might consider incorporating physiological measures to correlate with self-reported outcomes. Fifth, the study did not monitor home practice minutes or engagement with audio-guided practices because materials were distributed offline, limiting our ability to assess dose-response outside the structured sessions. Sixth, because mediators and outcomes were measured at the same assessment points, temporal precedence could not be fully established. Therefore, the mediation findings should be interpreted as theory-driven mechanisms rather than definitive causal pathways. Future studies using time-lagged or more frequent assessments are needed to verify temporal ordering. Finally, the numbers of volunteers of hospital or organization at the time of participating in this study are not big enough for testing the different effects of MC-BMS peer counselor training. The future research may explore the moderating effects among volunteers’ background and different cancer stages. Moreover, it can be further examined about the effects of their peer support for breast cancer patients after they receive MC-BMS or BMS training program. Implications of this Study MC-BMS, which consisted of structured mindfulness skills, self-compassion, and compassion to other skills and BMS empowerment strategies could be applied to train breast cancer survivors to be peer counselors. This training can increase breast cancer survivors’ competencies of self-care to prevent self from empathy-based stress while providing information and emotional support for new breast cancer patients. They could build up their mindfulness and self-compassion before compassion to others. This training could increase their quality of life, mental health, and spiritual growth. The moderator analysis found that none of factors significantly moderate the intervention effects, which suggested that the MC-BMS program could benefit breast cancer survivors who are willing to become peer counselors with different backgrounds and conditions. In the future, developing digital-assistance into peer-counseling program for breast cancer survivors might enhance the program to be accessible into a large-scale service. For example, virtual reality is applied to enhance breast cancer patients’ interoceptive awareness of feelings and positive body perceptions (Sebri et al., 2023). The qualitative review study (Senthilmahesh et al., 2024) found artificial intelligence (AI) has been integrated into oncology care through virtual assistants and chatbots to enhance patient care and support. The benefits of using digital assistance include providing real-time information, offering 24 hours emotionally supportive responses, and giving advice on emotional regulation skills to help reduce cancer patients’ stress and emotional distress. However, its limitations include the absence of genuine empathy and insufficient ability to manage complex psychological states. Therefore, hybrid models that combine AI capabilities with human expertise within peer counseling programs may represent the optimal approach. Conflict of Interest The authors of this article declare no conflict of interest. Cite this article as: Hsiao, F. H., Lo, C., Huang, C. S., Kuo, W. H., Huang, F. Y., Chen, Y. T., Hsieh, C. C. (2026). Mediating effects of mindfulness compassion-based peer counseling program for breast cancer survivors: From mindfulness, compassion to others to depression reduction. Psychosocial Intervention, 35, Article e260814. https://doi.org/10.5093/pi2026a6 Funding This study was supported by the Ministry of Science and Technology (MOST), Taiwan, under Grant MOST 111-2314-B-002-077-MY3. Additional support was provided by the 114 World Excellence 100 Support Program (Grant NTU-114L910204). |
Cite this article as: Hsiao, F., Lo, C., Huang, C., Kuo, W., Huang, F., Chen, Y., & Hsieh, C. (2026). Mediating Effects of Mindfulness Compassion-based Peer Counseling Program for Breast Cancer Survivors: From Mindfulness, Compassion to Others to Depression Reduction. Psychosocial Intervention, 35, Article e260814. https://doi.org/10.5093/pi2026a6
Correspondence: cchsieh1116@gmail.com (C.-C. Hsieh).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
Send






