


Impact of Fragile X Syndrome on Their Families
[Impacto del SĂndrome de X frágil en sus familias]
Concha Iriarte-Redín1, Manuel Soriano-Ferrer2, and Beatriz Hidalgo-Alés2
1Universidad de Navarra, España; 2Universidad de Valencia, España
https://doi.org/10.5093/psed2020a12
Received 11 October 2019, Accepted 4 February 2020
Abstract
The aim of the present study is to describe the behavioral and emotional disturbances in the Fragile X Syndrome (FXS) and to analize the impact of having a member with FXS on different aspects of family functioning. A sample of 79 parents with a member with FXS and 80 parents with a member with typical development participated in the study. Results showed that between 17% and 66% of children and adolescents with FXS displayed significant behavioral and emotional disturbances and fewer prosocial behaviors. In addition, after controlling for behavioral and emotional difficulties, our results showed that families affected by FXS experienced a more negative impact on feelings about parenting, finances, siblings, and the degree of difficulty of living with a child or adolescent with FXS, and greater family adaptability and cohesion than the comparison group. In conclusion, our results highlight that it is important to consider these differences in clinical practice when supporting and counselling families affected by FXS.
Resumen
El objetivo del presente estudio es describir las alteraciones conductuales y emocionales en el síndrome de X frágil (SXF) y analizar las reperecusiones de tener un miembro con SXF en diferentes aspectos del funcionamiento familiar. Participaron 79 padres con un miembro con SXF y 80 padres con un miembro con desarrollo típico. Los resultados mostraron que entre el 17% y el 66% de los niños y adolescentes con SXF mostraron trastornos conductuales y emocionales significativos y menos comportamientos prosociales. Además, después de controlar las dificultades emocionales y de comportamiento, nuestros resultados mostraron que las familias afectadas por SXF experimentaron un impacto más negativo en los sentimientos relativos a la crianza de los hijos, las finanzas, los hermanos y el grado de dificultad de vivir con un niño o adolescente con SXF y más capacidad de adaptación familiar y cohesión que el grupo de comparación. Como conclusión, nuestros resultados destacan que en la práctica clínica es importante tener en cuenta estas diferencias al apoyar y asesorar a las familias afectadas por SXF.
Palabras clave
SĂndrome de X frágil, Familia, ImpactoKeywords
Fragile X Syndrome, Family, ImpactCite this article as: Iriarte-Redín, C., Soriano-Ferrer, M., & Hidalgo-Alés, B. (2020). Impact of Fragile X Syndrome on Their Families. PsicologĂa Educativa, 27(1), 93 - 99. https://doi.org/10.5093/psed2020a12
manuel.soriano@uv.es Correspondence: manuel.soriano@uv.es (M. Soriano Ferrer).Fragile X Syndrome (FXS) is the main hereditary cause of intellectual disability (ID) and the most common, known monogenic disability (Kerr et al., 2015; Klusek et al., 2014). It is caused by a mutation in the FMR1 gene, located on the X chromosome. The prevalence rates provided by the literature vary considerably, with an incidence in men ranging from 1 in 2,500 to 1 in 7,000, and in women from 1 in 4,000 to 1 in 11,000. In Europe, the overall prevalence of the disease is estimated at 20 out of every 100,000 inhabitants (Chevreul et al., 2016; Hunter et al., 2014). Children and adolescents with FXS typically have moderate to severe intellectual disability < 55 (Raspa et al., 2017). In addition to cognitive delay, research has reported that children and adolescents with FXS have an increased risk of behavioral and emotional disorders compared to peers with typical development (TD). Neuropsychiatric phenotypes include a high risk of autism spectrum disorders (Chevreul et al., 2015; Chromik et al., 2019; Hare et al., 2016; Klusek et al. 2014; Moskowitz & Jones, 2015; Thurman et al., 2014), as well as other behavioral symptoms (Raspa et al., 2017): a) between 36% and 93% of individuals with FXS have associated hyperactivity and attention deficit (Angriman et al., 2015; Hare et al., 2016; Hartley et al., 2012; Thurman et al., 2014; Wheeler et al., 2008); b) around 70% of individuals with FXS have emotional problems, such as anxiety and depression (Bailey et al., 2012; Cordeiro et al., 2011; Roberts et al., 2014; Wheeler et al., 2014), and often show characteristics of social anxiety, including gaze avoidance, delay in initiating social interactions, and difficulty forming meaningful peer relationships (Holsen et al., 2008); and c) other distinctive features of FXS are behavior problems, including tactile defensiveness, hand flapping, poor eye contact, tantrums, perseveration, hyperarousal to sensory stimuli, and impulsivity (Muller et al., 2018; Symons et al., 2010). More than 30% of children and adolescents with FXS have committed acts of aggression, with their parents or caregivers even requiring medical attention in some cases (Bailey et al., 2012). Self-injury (e.g., hand and finger biting) is also common in about 79% of individuals with FXS (Symons et al., 2010). For example, Wheeler et al. (2016) pointed out in their study that 83% of females and 92% of males between 3 and 67 years old with FXS had participated in at least one aggressive act. More than a third of the males (38%) and 18% of the females had participated in an aggression serious enough to be diagnosed or treated for this reason (30% had caused injuries to their caregivers, and 22% had caused injuries to their peers or friends). The most common form of physical aggression was hitting, pushing, or kicking (54% of males and 31% of females). Less common was bullying (8% of males and 10% of females) or threats to others (19% of males and 7% of females). Behaviors such as tantrums, defiance, and arguments affect approximately 50% of all the age and sex groups. These difficulties may continue into adulthood (Chromik et al., 2019; Frolli et al., 2015). This phenotype has a clear impact on families because it increases parenting demands and stress, influences family functioning, and requires families to reorganize and adapt their routines (Burke & Heller, 2016; Gardiner et al., 2018; Schlebusch et al., 2016; Summers et al., 2005; Wheeler et al., 2008). Although the link between FXS and lower parental wellbeing has been well established, including more stress, higher levels of depression, and health problems (Hayes & Watson, 2013; Miodrag et al., 2015), the degree to which FXS might affect broader aspects of family functioning has been less investigated. In this regard, in the study by Lewis et al. (2006), mothers of children with FXS claimed to have less privacy than mothers of children with other types of disabilities. In addition, Hartley et al. (2012) found that 15.9% of parents with FXS children reported depressive symptoms that required clinical intervention, compared to 30.4% of parents of children with ASD and 6.8% of parents of children with DS. Thus, parents of children with FXS had higher wellbeing than parents of children with ASD and lower than parents of children with DS. Behavior problems are considered a strong predictor of parental stress. According to Cantwell et al. (2015), a child who exhibits challenging behavior in a public place can be very problematic and distressing for parents because of feelings of perceived stigma (feeling judged), hostile encounters with the general public, feelings of isolation, and a sense of impotence. A prospective study conducted in Germany between 2013 and 2016 observed 75 people with FXS from two to 82 years old in their social environment, showing the considerable burden experienced by the parents and the person with FXS. The main caregivers were either the parents or one parent in the case of 62 patients (82.7%). The fact that in 17 cases (22.7%) there were siblings with FXS means that these families had an additional burden (Haessler et al., 2016). In addition, families of individuals with FXS require significant resources of a non-medical nature that have a considerable economic cost, especially in the case of children (Bailey et al., 2012; Ouyang et al., 2014). In France, the estimated annual direct cost per patient per year is €25,800 (Chevreul et al., 2015). In turn, a family environment with high stress levels affects a child’s self-regulatory development and social competence. That is, the impact is bidirectional and affects the quality of life of the entire family system (Summers et al., 2005). In general, therefore, higher stress levels, lower general wellbeing, a greater prevalence of health problems (depression and anxiety), poorer social relationships, negative parenting feelings, less marital satisfaction, and greater economic and care demands have been found (Cantwell et al., 2015; Chan et al., 2017; Hall et al., 2016; Hartley et al., 2012; Minnes et al., 2015; Patton et al., 2018; Wheeler et al., 2016; Wheeler et al., 2008; Woodman et al., 2015). However, research is not conclusive because some positive effects also appear (Berglund et al., 2015): better parent-child interaction, more family cohesion, and a greater sense of purpose in life and of priorities (Grein & Glidden, 2015; Wheeler et al., 2008). Resilience, coping strategies, family routines, financial resources, and social support seem to be “protective” factors against the negative effects mentioned, and they contribute to wellbeing by improving the quality of life, not only of the disabled child, but also of the whole family (Grein & Glidden, 2015; Jess et al., 2018; Migerode et al., 2012; Minnes et al., 2015; Norling & Broberg, 2013; Schlebusch et al., 2016; Usher et al., 2018), including the siblings (Iriarte et al., 2015; McHale et al., 2016; Rossetti & Hall, 2015). Objectives Our first objective was to describe levels of emotional and behavioral difficulties in a Spanish sample of children and adolescents with fragile X syndrome (FXS), as well as the percentage of children with abnormal scores on each subscale. Our second objective was to analyze the impact of FXS on different aspects of the family: a) to analyze the perceptions of parents of children with FXS about family environment – parents’ feelings and attitudes, social life, family finances, marital relationships, relations among siblings, as well as general questions related to the degree of difficulty of living with a child with FXS and the influence this has on the family; b) to determine the effect of FXS on family adaptability and family cohesion. Given the difficulties involved in raising and educating children with FXS, compared to children without FXS, we expected to find significant differences between the two groups. Participants In order to carry out this study, the participation of two groups of families was required: one group composed of families of children or adolescents with FXS and the other group composed of comparison families with a child or adolescent with typical development. Thus, participants in the present study were 159 families with children and adolescents, corresponding to these two groups. All the children were boys. The FXS group was composed of 79 families with a child or adolescent with FXS between 6 and 17 years old, with a mean age of 12.3 (SD = 3.9). Parents reported the intellectual disability severity levels: 34.2% mild (n = 27), 54.4% moderate (n = 43), and 11.4% severe (n = 9). Children and adolescents were diagnosed with FXS in the first year of life (10.1%), between 2-3 years old (35.4%), between 4-6 years old (48.1%), and after the age of 6 (6.3%). The majority of the FXS sample were taking some kind of medication (n = 59, 74.6%). The comparison group was composed of 80 families with a child or adolescent without disability between 6 and 17 years old, with a mean age of 13.2 (SD = 3.6). No statistically significant differences were found between the groups in chronological age, F(1, 158) = 2.330, p < .129, η2 = .015. Table 1 includes family demographic information for the FXS and comparison groups. In both groups, questionnaire respondents were mothers (77.2% for FXS and 67.5% for the comparison group), and the majority of the parents were married or living together (82.2% for FXS and 95% for the comparison group). There were no statistically significant differences between the two groups of families on fathers’ age (range: 34-56), F(1, 158) = .329, p < .567, η2 = .002, or mothers’ age (range: 33-54), F(1, 158) = 4.781 p < .130, η2 = .003. Moreover, 77.2% of the children and adolescents with FXS had siblings with no disability, and 17.7% had more than two siblings with intellectual disabilities (range 2-4), whereas only 7.5% of the comparison children and adolescents had a sibling with a disability (see Table 1). Finally, with regard to occupations, most of the fathers had a paid job in both groups, whereas around 20% of mothers in both groups did not have a paid job. Occupations of fathers and mothers were distributed in four skill levels (see Table 1), in accordance with the international standard classification of occupations (International Labour Organization [ILO, 2012]). Table 1 Demographic Characteristics of Families with FXS and Comparison Group 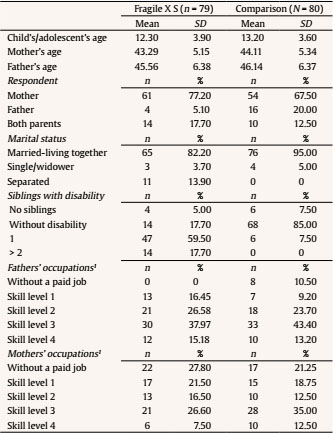 Note. 1Based on International Standard Classification of Occupations (2012). Instruments Demographic information. Respondents gave information about their age and that of other family members, gender, parents’ occupation, intellectual disability severity level, siblings with disabilities, age of FXS diagnosis, and marital status. Strengths and Difficulties Questionnaire (SDQ; Goodman, 2001). The SDQ consists of 25 questions designed to gather information about emotional and behavioral difficulties experienced by children from 3 to 17 years old, as well as information about impairments in daily functioning (available for viewing and downloading at www.sdqinfo.com). For scoring purposes, the SDQ categorizes strengths and difficulties into five scales: emotional problems (e.g., often unhappy, down-hearted); conduct problems (e.g., often has temper tantrums or hot temper); hyperactivity (e.g., restless, overactive, cannot stay still for long); peer problems (e.g., rather solitary, tends to play alone); and prosocial behavior (e.g., considerate of other people’s feelings). Each item receives a score between 0 (strongly disagree) and 2 (strongly agree). The test has been shown to have criterion validity and good test-retest reliability after four and six months (mean .62). Furthermore, the internal consistency is satisfactory, with a Cronbach’s alpha ranging from .57 to .88 (Goodman, 2001). The confirmatory factor analysis carried out by Ortuño-Sierra et al. (2017) in a large Spanish sample confirmed a five-factor model as the more appropriated and showed an internal consistency for Total Difficulties score of .84, ranging from .75 to .78 for SDQ subscales. Moreover, the SDQ has been found to be a useful instrument to assess difficulties experienced by children and adolescents with intellectual disabilities (Emerson, 2005). Family Impact Questionnaire (FIQ; Donenberg & Baker, 1993). This questionnaire had been translated by one author following the International Test Commission Guidelines for Translating and Adapting Tests (International Test Commission, 2017). The FIQ has 50 items that assess parents’ perceptions of their child’s impact on their families, compared to the impact that “most children his/her age have on their parents/family” (e.g., “I am more embarrassed by his/her behavior in public”). Forty-eight items are rated a 4-point Likert scale, and the last two items (49 and 50) are rated on a 7-point Likert scale. The questionnaire consists of six scales: a) impact on social life (10 items), b) negative feelings toward the child (9 items), c) positive feelings toward the child (6 items), d) impact on finances (7 items), e) impact on the marriage (7 items), and f) impact on siblings (9 items). The last two items refer to general questions related to the degree of difficulty of living with their child and its influence on the family. In the current sample, scale reliabilities ranged from r =.81 to .92. Family Adaptability and Cohesion Evaluation Scales (FACES-III; Olson et al., 1985). The abbreviated Spanish version was used (Martínez-Pampliega et al., 2006), consisting of 20 items, 10 of which were from the adaptability dimension and the other 10 from the cohesion dimension. Cohesion is the emotional attachment system that family members have with each other, and adaptability is understood as the ability of that system to change (assertiveness, leadership, negotiation). The internal consistency analysis of the items in the cohesion dimension presents a Cronbach’s alpha coefficient of .82, and .79 in the case of the adaptability dimension. The instrument has good construct validity, demonstrated by the goodness of fit indices obtained by the models tested. Procedure Parents with a child or adolescent with FXS were recruited by the Spanish FXS Federation [Federación Española de FXS]. To reach a national audience, we recruited a wide array of national organizations to post announcements on their websites. Associations sent e-mails to all members asking them to complete and return the questionnaires to us. All participants were given detailed information about the study, and complete anonymity of the collected data was guaranteed. No patient identification was required. The families included were those who declared that they had a family member between 6 and 17 years old suffering from FXS and completed the questionnaire. Because the questionnaires were anonymous, making follow-up impossible, no verification of the diagnosis was undertaken by a physician. The study was conducted with the understanding and consent of the participants, and it was approved by the Research Ethics Committee of the University of Valencia, which is regulated by Ethical Principles for Medical Research Involving Human Subjects according to the Declaration of Helsinki in 1964 (World Medical Association, 2013). Emotional and Behavioral Difficulties in Children and Adolescents with Fragile X Syndrome Multivariate analysis of variance (MANOVA) was computed, based on dependent variables, with the group of origin as the grouping factor. Next, a between-groups analysis of variance (ANOVA) was conducted for each measure. The level of significance was established after applying the Bonferroni correction (.008). Furthermore, the effect size was calculated through eta-squared (η2). Additionally, we computed the percentage of cases where parents reached (or surpassed) the cut-off point established for each scale on the SDQ. Table 2 Comparison of Families with FXS and Comparison Group on Emotional and Behavioral Difficulties  Note. 1Level of significance with Bonferroni correction (.008); 2values between .01 and .10 were considered small effect sizes, values between .10 and .30 were considered medium, and values above .30 were considered large. The MANOVA showed significant main effects by group (Wilks’ lambda (Λ) = .461, F(5, 145) = 33.895, p < .000, ηP2 = .53), with a large effect size. Results of between-group ANOVAs showed significant differences. The FXS group scored significantly higher than the comparison group on emotional symptoms (rated using the SDQ scale), conduct problems, hyperactivity, peer problems, and total difficulties, with medium to large effect sizes in all cases. Moreover, the FXS group had lower prosocial behaviors, with a medium effect size (see Table 2). As Table 2 shows, the percentage of cases with abnormal scores was higher in the FXS group than in the comparison group. Thus, in the FXS group, the percentage of cases with abnormal scores ranged from 16.9% for prosocial behaviors to more than 60% for hyperactivity, peer problems, and total difficulties, whereas in the comparison group the percentage of cases with abnormal scores was below 7.6% on all scales (see Table 2). Family Impact of Fragile X Syndrome To carry out our second objective, due to the high incidence of emotional and behavioral difficulties of children and adolescents with FXS, we performed a multivariate analysis of covariance (MANCOVA) with SDQ total difficulties as covariate, based on the dependent variables, with the group of origin (FXS vs. comparison) as the grouping factor. Next, a between-groups analysis of covariance (ANCOVA) was performed for each measure. The level of significance was established after applying Bonferroni correction (.005). Additionally, we reported effect sizes using the partial eta squared statistic (ηP2), which estimates the proportion of total variance accounted for by the independent variables. The MANCOVA, with SDQ total difficulties as covariate, showed significant main group effects (Wilks’ Lambda (Λ) = .439, F(9, 100) = 14.191, p < .000, ηP2 = .56), with a large effect size. Results of between-group ANCOVAs showed significant differences. The FXS group scored significantly higher than the comparison group on negative feelings about parenting, impact on finances, and siblings, and the degree of difficulty of living with a child with FXS, with large effect sizes in all cases (see Table 3). However, there were no significant differences between groups on social life, positive feelings about parenting, marriage, or the impact of the child on the family. Table 3 Means and Standard Deviations of Families with FXS and Comparison Group on Family Impact Measures 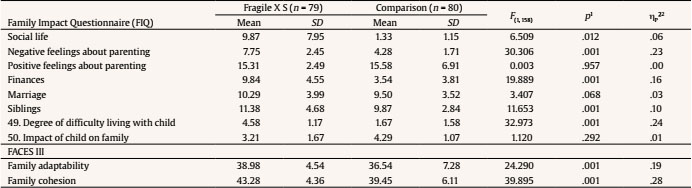 Note. 1Level of significance with Bonferroni correction (.005); 2for this statistic, values between .01and .05 are considered a small effect size, values between .06 and .12 a medium effect size, and values above .13 a large effect size (Richardson, 2011). In relation to family adaptability and family cohesion, the ANCOVAs reported significant differences between groups. Thus, the FXS group scored higher than the comparison group on family adaptability, and family cohesion, with large effect sizes. The aims of this study were to describe levels of emotional and behavioral difficulties in a Spanish sample of children and adolescents with FXS and analyze the impact of having a child with FXS on different aspects of family functioning. The results of the study contribute to the knowledge about the behavioral phenotype of children and adolescents with FXS and, specifically, the impact of FXS on family functioning. Overall, our results found that between 17% and 66% of children and adolescents with FXS displayed significant behavioral and emotional disturbances. In this regard, children and adolescents with FXS displayed more conduct problems, hyperactivity, peer problems, and emotional problems, as well as fewer prosocial behaviors. Our results are consistent with previous literature (Bailey, 2012; Cordeiro et al., 2011; Haessler, 2016; Newman et al., 2015; Roberts et al., 2014). In general, a defined pattern of problem behaviors, including hyperactivity, inattention, autistic features, and aggression, along with comorbid anxiety, has emerged for this population, and this pattern is estimated to occur in up to 86% of males with FXS (Low Kapalu & Garstein, 2016). These behavioral and emotional difficulties can negatively impact the health and safety of the individual involved and others (Hall et al., 2016; Minnes et al., 2015; Ouyang et al., 2014; Suzumura, 2015; Wheeler et al., 2016; Woodman et al., 2015) because they can produce negative feelings in parents and siblings and affect family economy and coexistence with a child with FXS. In fact, once behavioral and emotional problems were covaried, our results showed that families with FXS experienced a greater negative impact on feelings about parenting, finances, siblings, and the degree of difficulty of living with a child or adolescent with FXS. In general, our results are similar to those of other studies (Haessler et al., 2016; Johnston et al., 2003; Lewis et al., 2006; Raspa et al. 2016). First, parents of children with FXS in our study showed more negative feelings about parenting than parents in the control group. Haessler et al. (2016) found that in a group of 64 patients with FXS, 39.1% of parents reported low/normal stress, 34.4% high, and 78.1% very high. In the study by Johnston et al. (2003), 25% of mothers of children with FXS felt stress due to isolation and lack of parental competence. Problems and concerns about parenting and family relationships are affected by the diagnostic status of the child, and are greater in the case of parents of children with FXS (Lewis et al., 2006; Raspa et al., 2016). Second, parents also point out the impact that caring for a child with FXS has on their finances. Emerson et al. (2006), in a British national study (Department for Work and Pensions: Families & Children Study - FACS), found that mothers (n = 6,954) with at least one dependent child had a higher risk of low wellbeing (less happiness, self-esteem, and self-efficacy) due to greater economic difficulties. These additional burdens are also predictors of family distress (Minnes et al., 2015). Ouyang et al. (2014) compared family’s financial and employment impact of having a child with FXS, autism spectrum disorder (ASD), or intellectual disabilities (ID), and found that higher percentages of caregivers of children with FXS reported a negative family financial (60%) and employment (40%) impact. Bailey et al. (2012), in their study with 350 caregivers, found that most families reported that FXS had at least some financial impact on the family, and caregivers had to take an average of 19.4 hours off work each month to care for their child’s needs. Regarding economic costs, the studies by Chevreul et al. (2015) and Chevreul et al. (2016) include all types of costs associated with FXS, including the least visible ones, such as informal costs and loss of job productivity. In addition, it is the first study to estimate both the cost incurred by FXS and the impact on HRQOL (health-related quality of life) for FXS patients and caregivers. It highlights the high cost of the disease from a social perspective, despite its low prevalence, and that its life expectancy is similar to that of the rest of the population. Some of the data collected indicate that lifetime costs of FXS patients range from €1,113,000 for males to €620,000 for females, and the annual cost per patient ranges from €8,208 to €25,800. Third, our results also indicate that having a child with FXS has a negative influence on siblings. They often have to help more with housework, they are ashamed of their sibling’s behavior, or they invite their friends to their home less often. O’Neill and Murray (2016) found that siblings observed incoherent and negative parenting styles in their parents. Fourth, in our study, parents point out that it is very difficult to live with a child with FXS. According to Rodas et al. (2016), there are differences between parenting practices of parents of children with and without ID. Children with disabilities have an increased risk of developing other (internalizing) psychiatric disorders and of receiving negative parental education associated with these problems, which can create a vicious cycle. Fifth, in our study, however, there were no significant differences between groups in their social life. Some studies (Muller et al., 2018; Mulroy et al., 2008) reported restrictions on family activities due to a child’s disability. However, although no significant differences were found between groups in social life, group means are quite different: 9.87 for FXS and 1.33 for the comparison group. The reason for this may be that the standard deviation is quite large in the FXS group (SD = 7.95). Sixth, in our study, there are no significant differences related to positive feelings (see Table 3), and this result may be due to high self-esteem in the group of parents with children with FXS. As Cantwell et al. (2015) noted, the higher the parents’ self-esteem, the greater their resilience and psychological health, because self-esteem buffers the impact of stress on psychological wellbeing. These results are also supported by Wheeler et al. (2008), who found that perceived quality of life of mothers of children with FXS was not different from that of the general population. Instead of being overwhelmed by their child’s disability, they felt full of energy and support. The hope factor appears in this study as a predictor of quality of life. Parents’ hope factor, associated with adaptive coping strategies, is related to a warmer parenting style and a more cohesive and active family environment. Finally, families with FXS displayed more family adaptability (mean = 38.98) and cohesion (mean = 43.28) than those in the comparison group. In this regard, Baker et al. (2012) also reported higher levels of cohesion in families of adolescents and adults with FXS than what had been previously reported for families of individuals with developmental disabilities. Johnston et al. (2003) indicated that greater family cohesion and support are related to less stress and and feelings of isolation in the study mothers, as well as greater confidence in their parenting skills. It is important to note the limitations of our study. First, the majority of respondents were mothers (77.2% in the FXS group and 67.5% in the comparison group). Although this is common in research (Allison & Campbell, 2015; Ly & Goldberg, 2014; Ouyang et al., 2014; Usher et al., 2018), not all family members experience similar effects as a result of being a relative of a child with a disability (Hastings et al., 2005). Problems experienced by mothers may not reflect those of other family members. Second, our study is cross-sectional in nature, and so it would be useful to examine longitudinal data in FXS because previous studies suggest the possibility of a decline in the reported positive impact over time (see Blancher et al., 2013; Raspa et al., 2017). Third, respondents were members of FXS family associations, and samples drawn from these associations may not be representative of the total population affected by FXS. Finally, findings may not be generalizable outside Spain. In summary, our conclusions are: Behavioral and emotional difficulties shown by children and adolescents with FXS in our study have a negative impact on parents and siblings, generating negative feelings and affecting family’s economy and coexistence with the child with FXS. Knowing the impact of having a child with FXS on the family allows us to identify factors susceptible to intervention that can contribute to improving the welfare of the person with FXS and his/her family. This information can help to design appropriate management strategies and services that meet the needs of affected families, thus reducing vulnerability and increasing resilience in the long term. It is important that this intervention be carried out as early as possible in order to improve the adaptive behavior of these children regarding issues specific to the syndrome, such as emotional regulation, social anxiety, or behavior problems. In fact, the literature emphasizes that behavior management is one of the aspects that most affects mental health, depression, stress, and anxiety in the parents of these children. In this regard, we know that parental support programs focusing on behavior management are the key to moderating the psychological impact. These programs not only improve skills of children affected by FXS – a definite asset for independence in adulthood – but also the adaptability and mental health of their parents, who are no longer isolated thanks to these support groups. Likewise, it is essential to promote family group cohesion because this is another variable that has a buffering effect on the negative psychological impact. Thus, it is necessary to ensure that fathers cease to be only “a shadow” of mothers. Encouraging fathers’ participation can lead to greater family competence, reduced parental stress, and less physical and emotional burden for mothers, as well as greater adaptive skills for children. Support for families of children with FXS should adopt a family-centered approach that recognizes that parents are affected by the nature of their child’s disability and that the psychological wellbeing of one of the parents is linked to the psychological well-being of the child. Therefore, the best intervention recognizes the importance of interconnections among family members in promoting positive wellbeing within the family and fostering a strong family system. Another variable to consider is family’s socioeconomic position because this factor can moderate the relationship between the child’s disability and stress. It is advisable to identify family subgroups that are most likely to experience stress for this reason. Finally, supporting parents in the process of regulating their emotions is crucial because the more effective they are in focusing on positive aspects of their experiences with their children, the more successful they can be in defending them and experiencing better family quality of life. Intervention programs must promote parents’ self-esteem in order to improve their psychological health and resilience, thus buffering the impact of stress, in addition to increasing hope and positive expectations, which, in turn, foster a warmer and more protective parenting style that is cohesive and active in the family group. Conflict of Interest The authors of this article declare no conflict of interest. Acknowledgments The authors are especially thankful to all the family members who participated in this study, and to Feli Peralta, a tireless researcher in the field of disabilities, for her great generosity. Cite this article as: Iriarte-Redín, C., Soriano-Ferrer, M., & Hidalgo-Alés, B. (2020). Impact of Fragile X Syndrome on their families. Psicología Educativa. 27(1), 93-99. https://doi.org/10.5093/psed2020a12 References |
Cite this article as: Iriarte-Redín, C., Soriano-Ferrer, M., & Hidalgo-Alés, B. (2020). Impact of Fragile X Syndrome on Their Families. PsicologĂa Educativa, 27(1), 93 - 99. https://doi.org/10.5093/psed2020a12
manuel.soriano@uv.es Correspondence: manuel.soriano@uv.es (M. Soriano Ferrer).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Imprimir
Imprimir Enviar
Enviar
ALERTA POR E-MAIL
La Revista de Psicología Educativa está distribuida bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObra Derivada 4.0 Internacional.com








