


Exploratory Study on the Prevalence of Speech Sound Disorders in a Group of Valencian School Students Belonging to 3rd Grade of Infant School and 1st Grade of Primary School
[Estudio exploratorio sobre la prevalencia de trastornos fonol├│gicos en un grupo de escolares valencianos de tercer grado de educaci├│n infantil y primero de primaria]
Omaya Amr Rey, Purificación Sánchez-Delgado, Mª Rosario Salvador Palmer, Mª Cibrian Ortiz De Anda, and Vanessa Paredes Gallardo
Universitat de Val├Ęncia
https://doi.org/10.5093/psed2022a1
Received 15 January 2021, Accepted 2 August 2022
Abstract
Dyslalia or sound speech disorder is the most common speech production difficulty among school children. This epidemiological study aims to know the prevalence of SSD in school children and to analyze the relationship between articulatory disorders and bad oral habits, age, gender and socioeconomic situation. Two hundred and ninety children between 4 and 7 years old were evaluated by means of the Marc Monfort Test, a myofunctional test, and a questionnaire was applied to families. The results show that 51.4% of the schoolchildren present SSD. The most frequent type of error is distortion followed by substitution. Multiple dyslalia is more frequent than simple dyslalia. The relation of dependence between phonetic alterations and masculine gender is observed, as well as a decrease of articulation disorders as age increases and a significant relation between bad oral habits and the presence of dyslalia.
Resumen
La dislalia o trastorno fonológico es la dificultad en la producción del habla más frecuente entre escolares. Este estudio epidemiológico pretende conocer la prevalencia de TF en escolares y analizar la relación de las alteraciones articulatorias y los malos hábitos orales, la edad, el género y la situación socioeconómica. Se evalúan 290 niños y niñas entre 4 y 7 años mediante el Test de Marc Monfort, un examen miofuncional y la aplicación de un cuestionario a las familias. Los resultados muestran que el 51.4% de los escolares presentan TF. El tipo de error más frecuente es el de distorsión, seguido del de sustitución. Es más frecuente la dislalia múltiple que la simple. Se observa la relación de dependencia entre las alteraciones fonéticas y el género masculino, así como una disminución de trastornos de articulación a medida que aumenta la edad y una relación significativa entre los malos hábitos orales y la presencia de dislalias.
Palabras clave
Prevalencia de trastorno fonol├│gico, Diagn├│stico de trastorno fonol├│gico, Trastorno fonol├│gico, Dislalia, Trastorno de articulaci├│nKeywords
Prevalence of sound speech disorder, Diagnosis of sound speech disorder, Sound speech disorder, Dyslalia, Articulation disorderCite this article as: Rey, O. A., Sánchez-Delgado, P., Palmer, M. R. S., Anda, M. C. O. D., & Gallardo, V. P. (2022). Exploratory Study on the Prevalence of Speech Sound Disorders in a Group of Valencian School Students Belonging to 3rd Grade of Infant School and 1st Grade of Primary School. Psicolog├şa Educativa, 28(2), 195 - 207. https://doi.org/10.5093/psed2022a1
purificaci├│n.sanchez@uv.es Correspondencia: purificaci├│n.sanchez@uv.es (P. S├ínchez Delgado).Dyslalia or speech sound disorder (SSD) is the most frequent speech disorder among schoolchildren, which manifests itself in the difficulty of being able to articulate one or more phonemes (Ahmadi et al., 2019; Salvago et al., 2019). The prevalence of SSD depends on the type of study, childhood age, type of sample or methodology used. This prevalence varies from 7.4% to 50.72 % (Gallego Ortega, 2019; Tresoldi et al., 2015; Vázquez-Reyes et al., 2014; Wren et al., 2016). According to the ASHA (American Speech-Language-Hearing Association, 2020) speech sound disorders refers to the combination of difficulties in perception, motor production or phonological representation of speech sounds that affect intelligibility. Speech sounds disorders can be classified according to the type of error produced in the phoneme or phonemes, such as distortion, substitution, addition, and omission (Van Riper, 1963). The process of acquiring phonemes implies the anatomical and functional integrity of the speech organs (Georgievska-Jancheska, 2019). In a literature review study on the acquisition of phonemes at school age, 27 different languages were analysed and it was concluded that at 5 years of age boys and girls pronounce at least 93% of consonants correctly. Plosives, nasal, and nonpulmonic consonants were acquired earlier than trills, flaps, fricatives, and affricates. (McLeod & Crowe, 2018). In English the first phonemes to be acquired are /m/, /n/, /p/, /b/, / d/, /w/ and the last /r/ and /s/ (Chung et al., 2019; Dodd et al., 2003). North American English rhotic /╔╣/ may not reach mastery level in the population until over eight years of age (McAllister Byun & Tiede, 2017; Preston et al., 2019). In other languages, such as Serbian, they observed that the phonemes with the greatest difficulty were affricates and fricatives, and the most common articulation disorder was distortion. (Mihajlovi et al., 2015). In a study of the Italian language of 602 children aged 3 to 10 years, it was observed that the nasal and labiodental fricatives were acquired first, followed by the affricates and fricatives. The greatest difficulties occurred in the phonemes /r:/, /spr/, /tst/, /zm/, /rd/, /ks/, and /fg/ (Tresoldi et al., 2015). In the Spanish language there are few studies on the acquisition of phonemes in childhood. The study carried out by Bosch (1984) concluded that at 3 years old the acquired phonemes are /m/, /n/, /ñ/, /p/, /t/, /k/, /b/, /x/, /l/, and ascending vowel diphthongs. By 4 years old the phonemes /d/, /g/, /f/, /ch/, /r/ have been acquired. Then, at 6-7 years /s/, /z/, /rr/, and descending diphthongs. Vivar and León (2009) conclude that the least difficulties occur in nasal and occlusive sounds, with alveolar and velar vibrating sounds and fricatives presenting greater difficulty. The substitution phenomenon is the most frequent. According to Heras Mínguez (2015), nasal phonemes are the first to be acquired, then the stops and fricatives and, finally, the multiple and lateral vibrations. This author also considers that the consonant clusters formed by liquids appear later than the rest of the consonant groups. The phoneme /r/ would have be acquired between 5.6 and 5.11 years (Rojas Contreras et al., 2019). Different studies point to a universal theory in the development of speech acquisition. Maphalala et al. (2014) studied the isiXhosa language and concluded that there is a universal theory in the acquisition of speech but that this South African language has its own sounds, such as the consonant click, that have different acquisition times. In addition to the fact that the language is characterized by open syllables, many words contain 5 or 6 syllables and the tonality with which a word is emitted can vary the meaning. The exact nature of phonological processes will vary according to the structure of the language. Therefore, although there is a universal theory of speech acquisition, it is necessary to carry out studies into different languages since each language has certain phonemes that imply specific places and manners of articulation. Likewise, the process of acquiring the different phonemes varies depending on the language being learned. The difference is sometimes minimal, but it is necessary to have clear understanding in each case since it implies a specific articulation and rhythm. The application to different languages is problematic since each language has different rules for consonant and vowel phonemes according to their position in a word as well as the complexity of the formation of words and also in prosody (Maphalala et al., 2014; Tresoldi et al., 2018). Relating phonology with learning, it can be said that between 0 and 6 years of age is enough time for the phonological system of any language to be adequately developed (McLeod & Crowe, 2018; Priester et al., 2011; Wren et al., 2016). Bad oral habits, such as thumb sucking, nail biting, lip sucking, bruxism, or the type of diet can be the cause of a dental malocclusion and an articulatory disorder (Barbosa et al. 2009, Ferriolli 2010). There is also atypical swallowing, defined by many authors as persistence of infantile swallowing (Tulley, 1969); however, there is insufficient evidence to support this claim. Besides, the forward position of the tongue against or between the anterior teeth favours the appearance of articulatory disorders (Proffit & Mason, 1975). The tongue in the resting position places the tip and dorsal portion on the alveolar ridge, or the palatine rugae. The tongue should not touch the incisors or be placed on the soft palate (Kotsiomiti et al., 2005; Lebrun 1985). The high position of the tongue at rest is a decisive factor for the rhythmic activity of swallowing and an orientation for the entire orofacial musculature (Huang et al., 2015). Many studies have linked poor oral habits to difficulty articulating phonemes. Different studies corroborate the distortion of phonemes in individuals with atypical swallowing, both in the Persian language (Eslamian & Leilazpour, 2006) and in Japanese (Suzuki et al. 1981), with the distortion of the phonemes /s/, /f/, /dz/, in the Flemish language the distortion of the alveolar phonemes (Van Lierde et al. 2015), and in Portuguese with deviation in the phonemes /t/, /d/, /n/, /l/ (Pizolato et al. 2011). In contrast, the study by Khinda and Grewal (1999) did not find a direct relationship between atypical swallowing and alterations in the evaluated phonemes, but did find a direct relationship between anterior open bite and SSDs, and between anterior open bite and atypical swallowing. Other studies indicate that sucking habits such as pacifier use, finger sucking, or prolonged feeding with a bottle are associated with speech impairment in children aged 3 to 5 years (Barbosa et al. 2009). In the study, conducted in Portuguese, it was concluded that children with prolonged use of a pacifier and bottle had greater problems and alterations in the linguadental and dento-alveolar phonemes (Ferriolli 2010). In the study of children between 6 and 10 years old, in the Italian language, almost half of those with SSDs had bad oral habits such as nail biting or finger sucking (Farronato et al. 2012). Other etiological factors of articulatory disorder are gender, age, and socio-economic status. Regarding gender, SSD has always been associated more frequently with boys than with girls (Georgievska-Jancheska, 2019; Salvago et al., 2019). In the English language study, it was found that girls were more proficient in interdental fricatives and had fewer articulation problems (Dodd et al., 2003). There are studies where no significant relationship was found between gender and SSDs where the prevalence is higher in boys, although without a significant value (Ahmadi et al., 2019). Most studies conclude that the articulatory disorders decrease with age (Ahmadi et al., 2019; Stahl et al., 2007). However, other studies found no significant relationship between SSDs and different age groups (Farias et al., 2006; Lubit, 1967). Socio-economic situation could well be important in the articulatory disorders present in schoolchildren (Eadie et al., 2015; Wren et al., 2016). According to Dodd et al. (2003), the availability of normative data is essential for the clinical evaluation of children to detect SSD in time, this being necessary to carry out epidemiological studies that provide an explanation of phonetic development in school-age children. Epidemiological studies provide explanations about the difficulties of language acquisition in school age and provide knowledge about the etiology of diseases. They are not associated with norms, but they help professionals to identify the causes or the explanation for a specific phenomenon. Given the scarcity of epidemiological studies of children’s language in the Spanish language, as well as the lack of studies that relate the influence of bad oral habits on speech or how tooth replacement affects articulation difficulty, this study, in which schoolchildren aged 4 to 7 years participate, was carried out in the province of Valencia with the aim of ascertaining the prevalence of SSD in schoolchildren and analysing the relationship of alterations in articulation with bad oral habits, age, gender, and socio-economic situation. Design This is an observational, descriptive, and cross-sectional epidemiological study aimed at analysing the characteristics of speech disorders and their relationship with other variables. Although there are other studies that analyse the presence of articulatory disorders and poor oral habits with age, sex and socio-economic level, in our context, the Valencian Autonomous Region, it is a pioneering study. A study of the literature reveals a great diversity of research in the types of habits studied (Benavides et al., 2017; Bravo Rivera et al, 2019; Cab et al, 2012; Chamorro et al., 2016; Vázquez-Reyes et al., 2014). In some, only the influence of the pacifier is investigated, while others prioritize finger and lip suction rather than nail biting or bruxism. In the Discussion section, this problem is considered within the studies of oral habits. Habits is a variable that depends on time and type, so that it can have a greater or lesser effect at the level of speech articulation. Furthermore, no study on swallowing in children has been able to develop a more enlightening classification regarding this variable. The study of atypical swallowing in children has not been investigated at the epidemiological level in such detail. No classification of swallowing has been found specifying that swallowing in children in the absence of anterior teeth is classified as adaptive and separate from atypical swallowing, which is clearly pathological. Because the infant is in the process of tooth replacement or has the typical diastemas of infant dentition, which forces the child to place the tongue in an advanced position, this would be adaptive swallowing. Knowledge of the area of dentistry helps to clarify whether the position of the tongue at the time of swallowing and the articulation is correct since dental malocclusion may be present in orofacial dysfunction. Spanish language studies are lacking in bilingual communities with populations of children where the rate of migrants is high and who tend to speak two or three languages at home. There are also no recent studies on the prevalence of SSDs in schoolchildren that specify the number of phonemes that are usually most affected, nor the most frequent types of errors. Neither has any study of the Spanish language been found that investigates the prevalence of infantile lisp – both substitution of /z/ with /s/ and of /s/ with /z/ is very common in substitution errors This study was approved by the Ethics Committee for Research in Humans of the University of Valencia with the file number H1355744230207 and by the Department of Education in the Resolution of December 16, 2014 according to Decree 190/2012 of December 21. Permission was requested from the management teams of the schools to carry out the study. Family members were informed in writing, asking them to sign the informed consent. The questionnaire was given to the students’ relatives/guardians/parents and the clinical examination was carried out in a school room. Research Hypothesis There is a high prevalence of phonological disorders in school age children. The infant during the language acquisition process can make mistakes in the production of phonemes such as substitution, distortion, omission, and addition of phonemes. Sex and socio-economic status influence on phonological disorders. The high prevalence of bad oral habits in schoolchildren conditions an orofacial dysfunction that can affect the articulation of phonemes. The multifactorial origin of phonological disorders makes it necessary to study bad habits in greater depth. In various studies (Benavides et al., 2017; Bravo Rivera et al., 2019; Cab et al, 2012; Chamorro et al., 2016; Vázquez-Reyes et al., 2014) it was found that the presence of abnormal habits in early childhood, such as finger sucking, lip sucking, the introduction of objects in the mouth and atypical swallowing, causes imbalances. These imbalances can produce alterations in the other functions involved in the stomatognathic apparatus, such as breathing, phonation, swallowing, and chewing. There may also be abnormalities in facial development. SSD is a phonetic alteration that manifests itself in the difficulty of being able to articulate one or more phonemes correctly. Its etiology is due to different causes such as psychological factors, auditory discrimination, or fine motor skills, among others, affecting the speech process at any level. Among the causes of SSD are dental dysglossia, which is the difficulty in articulating phonemes due to dental malocclusion. Dental malocclusions can be caused by the persistence of bad oral habits so frequent in childhood. The language acquisition process is a complex process in which the functionality of all the organs involved in phonation is important. The orofacial musculature intervenes in speech since this is a complex motor behaviour. For this reason, we observe that the orofacial muscles, the tongue, and habits determine the morphological development of the jaws. Oral habits will condition orofacial morphology, and as a result functions involved in the stomatognathic apparatus, such as phonation, may be compromised. In consideration of the above, an evaluation was carried out with a high degree of precision of occlusion, musculature, mucous membranes, or the articulation of speech, and to what extent the imbalance of any of these affects the functionality of the others. Objectives The present epidemiological study aims to reveal some of the causes of the high prevalence of phonological disorders in school age children. Most professionals focus the evaluation protocol and rehabilitation of SSD on auditory discrimination. This work involves a myofunctional examination to investigate the orofacial dysfunction that students with phonological disorders present.
Participants The study group consisted of schoolchildren in Infant Education and first grade of Primary School, aged between 4 and 7 years old, belonging to six public state schools in Valencia. The selection and recruitment of cases was made by availability. For this, the schools were contacted and access was requested, facilitating the collection of information by school years. In this way, work was carried out in 3rd grade of infant education and 1st grade of primary school, which explains the fact that there are some cases of children with 4 years of age. It should be taken into account that these children would be close to turning 5 years old (these are children born between October and December). The global mean age is 5.7 years. There are 5 children of 4-year-olds (1.7%), 103 children of 5-year-olds (35.3%), 147 children of 6-year-olds (50.3%), and 37 children of 7-year-olds (12.7%). By gender, 152 girls (52.1%) and 140 boys (47.9%) with no statistically significant difference (p = .520). The inclusion criteria were the schoolchildren belonging to the schools in which permission of the management team was available and whose informed consent is signed by the responsible parents or guardians. The exclusion criteria were schoolchildren with disabilities in order to maintain normotypical subjects. After applying the above criteria, a final sample of 290 schoolchildren was obtained. They were also grouped according to the socio-economic status (geographic location of the school). Group 1 corresponds to a medium-low socio-economic situation (Sagunto schools) and group 2 to medium-high (Valencia schools). The distribution by grade shows that there are 155 (53.3%) schoolchildren in 3rd grade and 136 (46.7%) in 1st grade, with no statistically significant difference (p =.226). It is observed that of the 290 schoolchildren in the sample 105 still have not begun tooth replacement (36.1%) and 186 (63.9%) present mixed dentition, with a statistically significant difference (p =.000002). Instruments Firstly, for the evaluation of the articulation of phonemes, the evaluation test of Marc Monfort (Monfort, 1989), called Induced Phonological Record (RFI), was used. It contains a list of words with all the phonemes in Spanish to record the characteristics of the speech of children between three and six and a half years of age, to quantitatively compare a child’s oral production with that of others in his/her age group. Auditory discrimination was also evaluated (see Appendix, Table S2 and S3). In addition, a questionnaire aimed at families was applied with the aim of differentiating aspects of the child that would allow us to identify the etiology of the articulation difficulty. The languages spoken by the schoolchildren at home were taken into account, due to the multicultural nature of some classes and because the study was carried out in a bilingual community. Furthermore, if the child presented oral habits, the type and duration of these was evaluated – see Appendix, Table S1. Finally, the swallowing function was assessed by subjective myofunctional examination. The exercise to assess swallowing consisted of swallowing saliva or swallowing water (American Speech-Language-Hearing Association, 2020; Stahl et al., 2007). The placement of the tongue while performing swallowing was observed and was classified as normal, when the tip of the tongue was situated on the palatine rugae and there was no involvement of orofacial musculature. Adaptive atypical swallowing was considered when there was a growth at the upper bone level and the teeth appeared with more marked diastemas than those of the dental replacement. This group was made up of children with absence of teeth due to replacement, with anterior open bite due to eruption and with interincisal diastemas due to buccal braces. Additionally, atypical swallowing was considered when there was an inappropriate movement of the tongue and/or other structures involved in the act of swallowing during the oral phase of swallowing. An evaluation was also made to see if there were any further signs, such as force in the chin at the perioral level, corners, parted lips, or sucking the lower lip. It was observed whether the tongue in the atypical swallowing acquired an anterior, lateral unilateral or bilateral position. The tongue was also observed at rest, evaluating whether the tongue was located in a low position, intermediate against the palatal face of the anterior teeth, or in a high position. Finally, the type of dentition presented by each of the subjects was evaluated (see Appendix, Table S3). Process Permission was requested from the school. The questionnaire was distributed to the students for their parents or guardians to fill out. The teachers reported which children received specialized care at the school and in the family questionnaire they reported whether they received outside speech therapy. All records were made by a single examiner and can be consulted in the Appendix. Mirrors, latex gloves, masks, and protective glasses were used as examination material. Cards, candles, balloons and, on occasions, a recording device were used to assess articulatory disorders in order to establish a better diagnosis. For the evaluation of swallowing and the position of the tongue at rest, the student was asked to drink water or chew a sandwich. First, an infant’s spontaneous language was observed by asking a series of questions. Subsequently, the Induced Phonological Record test (see Appendix) was carried out individually in a room belonging to the school. This lasted about 10 minutes and consisted of 57 words with the phonemes of the language. The corresponding images were presented to the subject to see the spontaneous expression of the word and then the evaluator asked them to repeat the poorly articulated phoneme. A word incorrectly pronounced on the first attempt and corrected on repetition was judged as wrong when applying the general barometer. A series of words for auditory discrimination were also applied. The ability to differentiate the phonemes that make up the words was observed, identifying the change in meaning from the discrimination of contrasting pairs of phonologically similar words. The student was then asked to drink water to observe swallowing and the position of the tongue at rest in relation to the soft tissues and teeth. With all the information collected, an individualized diagnosis of all the children included in the study was carried out. Analysis of Data All the variables analysed were recorded in an EXCEL spreadsheet and the results were subsequently analysed with the statistical package SPSS v21. The analyses carried out were adjusted to the metric characteristics of the variables and their distributions, respecting the necessary assumptions for the application of each indicator used, for which an exploratory data analysis (EDA) was carried out (Tukey, 1977). The analysis of the size of the effect in hypothesis contrasts (to adequately assess the level of significance – p), although frequently recommended by many authors (Frías-Navarro, 2011; Frías-Navarro et al., 2000) was not considered necessary to be included in this case, as the significance of the difference is so broad. To study the dependence of factors in the categorical variables, contingency tables were used with Pearson’s chi-square test statistic and to determine the dependent group or groups, the residuals between the observed and expected frequencies were analysed. Comparison of proportions was carried out using binomial tests. In all cases the test was considered significant for p < .05. The results are presented in tables indicating the specific significations for each test performed. In the cases where a p-value equal to .000 appears, p < .001 should be understood. The results, attending to the first objective, show that the prevalence of schoolchildren with SSD is 51.4%. Taking into account the frequency of distorted phonemes, four groups can be formed: the highly distorted phonemes (/s/, /z/, /r/, /rr/), which make up 68% of the cases; medium distorted phonemes (/f/, /ch/) with 21% incidence; phonemes with low degree of distortion (/l/, /ll/, /t/, /d/) 7.7%; and phonemes with very low distortion (/p/, /b/, /k/, /g/, /j/, /m/, /n/, /ñ/) only make up 3.3% of our cases. Thus, the descriptive analysis of articulatory disorders shows a frequency of deviation in the different phonemes according to percentages, as can be seen in Table 1, with 141 subjects showing no deviation in any phoneme (48.6%) and 51.4%, as previously been indicated, with articulatory errors. The phonemes that require more difficulty in articulation are /s/ and /z/, followed by /r/, /rr/. The most frequent type of error is distortion, followed by substitution and, to a lesser extent, omission and addition, as can be seen in Table 2. As the phonemes /s/ and /z/ are most altered, it is interesting to analyse the frequency of interdental sigmatism (lisp), the substitution of the phoneme /s/ by /z/ which represents 16.2% and the presence of substitution of the phoneme /z/ for /s/ (8.7%) – see Appendix, Table 4S. Table 1 Distribution of the Study Group according to the Most Altered Phonemes as Dyslalias Increase 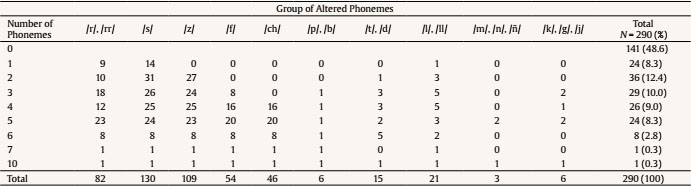 Table 2 Descriptive Analysis. Distribution of the Study Group according to the Articulation or not of Phonemes and according to the Type of Error. Valid Percentage Representation 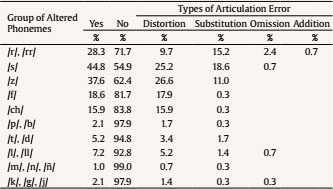 The results show the significant relationship between age and SSD (p = .019), the age of 5-6 years showing the highest incidence, with a statistically significant difference at 5 years and between gender and SSD (p = .032), showing that there is a slightly higher incidence in children (standard residual = 1.1). When performing the chi square test between the type of dentition and the phonetic alterations, it was found that there was no association; neither was there any between phonetic alterations and socio-economic groups, with p = .764 and p = .411, respectively. Regarding the results obtained from the second objective (Table 3), it was observed that more than a quarter of the study group had one or more bad oral habits. The percentage of schoolchildren is also indicated according to the types of habits: pacifier, introduction of objects in the mouth, finger sucking or lip sucking. The introduction of objects in the mouth has the highest percentage with a statistically significant difference. When observing swallowing patterns, atypical swallowing was present in 30.7% of children and adapted swallowing in 38.3%. Atypical swallowing is classified according to whether the lingual interposition is anterior or lateral. The anterior position of the tongue was observed in 23.7% of the cases with a statistically significant difference (p < .001). Orofacial muscle contraction was evaluated and classified as perioral contraction, chin contraction, or lower lip suction. The contraction of the chin with a statistically significant difference (p < .001) was the most frequent, followed by the perioral and, then, by suction of the lower lip. The altered position of the tongue at rest occurred in 30.9% of cases, more frequently in a situation of anterior rest. Finally, taking into account objective 3 proposed in this study (Table 4), the results do not show a dependency relationship of bad oral habits in SSD. To study the dependence of factors in the categorical variables, contingency tables were used with the Pearson’s chi-square test statistic. This showed us if among the variables any of them was statistically significant with respect to the others. For example, if in atypical swallowing the muscle contraction at the chin level was more significant with respect to the perioral, finger suction or lower lip suction. The descriptive statistics presented reveal one of the causes within the complexity of etiological factors that SSD can present. This group would include habits such as the use of pacifiers, lip sucking, finger, and the introduction of objects. If the different groups of phonemes with bad oral habits are analysed, a dependency relationship is observed with the altered group of phonemes, such as /p/, /b/ and /k/, /g/, (p = .029) (Table S5). Atypical swallowing shows a dependency relationship in children with phonological disorders (p < .001). Table 5 shows that there is no association between bad oral habits (lip sucking, finger sucking, pacifier, and introduction of objects) and the type of teething, with a p value of .458. When performing the chi-square test for the type of dentition according to whether or not atypical swallowing was present or not, it was observed that there was no association (p = .911). The presence of bad oral habits does not depend on the age of the study group. This is because as you get older some habits are discarded and others are acquired. Table 3 Distribution of the Study Group Depending on the Presence or Absence of Bad Oral Habits. Valid numbers and Percentages  *p < .05, *** p < .001. Table 4 Presence or not of Phonological Disorders according to Different Ages, Sex, Socio-economic Situation and Bad Oral Habits. Valid Frequencies and Percentages 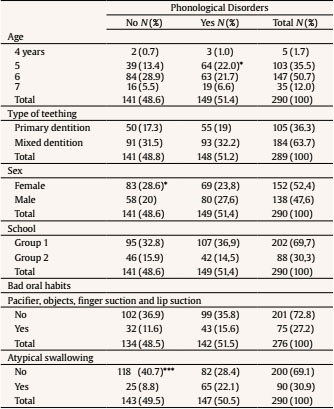 *p < .05, *** p < .001. Table 5 Distribution of the Study Group according to the Presence of Bad Oral Habits according to the Type of Teething 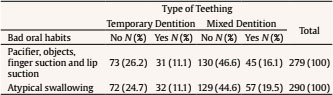 This study investigates the phonemes that present the greatest difficulty in the acquisition of speech and at what ages, together with the most frequent types of speech error and the factors affecting phonetic articulation, such as gender, socio-economic situation, tooth replacement, and bad oral habits. The results show that phonetic alterations are present in 51.4%, which indicates a 95% CI (51,0%, 51,7%) with respect to the population studied. The frequency of SSD in schoolchildren varies greatly between some studies and others. Several factors influence this, such as age and number in the sample. We find similar percentages in the study of Italian and Spanish languages (Farronato et al., 2012; Vázquez-Reyes et al., 2014). In the Portuguese language study, the speech of children aged 4 to 6 years was evaluated and it was observed that 25% had no speech alterations (Farias et al., 2006). Regarding the type of error, the most frequent is the distortion of phonemes, followed by substitution and, to a lesser extent, the addition and omission of phonemes. This result coincides with the study of the Serbian language where it was observed that the most frequent type of error was distortion, followed by substitution and the absence of omission of phonemes (Mihajlovi et al., 2015), as with the study of the Italian language, in which distortion is the most frequent type of error between 3 and 6 years of age (Tresoldi et al., 2015). This study, like Tresoldi et al.’s (2015) of Italian and Dodd et al.’s (2003) of English, concludes that the first phonemes that are acquired are occlusives, nasals, and labiodental fricatives, affricates and, finally, fricatives /r/, /rr/. It also coincides with the study in Spanish carried out on 200 patients aged 5 and 14 years, in which the most frequent errors were rotacism, sigmatism, deltacism, and problems with the pronunciation of the phoneme /f/ (Nelcys et al., 2000) and with the study by Vivar and León (2009), where the later acquired phonemes are the fricatives like /x/ and /s/ and, in a greater proportion, /r/. Here too the first acquired were nasals and occlusives. In this study, the phonemes with the fewest errors are nasals and occlusives, and those with the greatest difficulty /s/, /r/ and /rr/. Early distortion errors can turn into persistent speech errors in some children, the importance of detecting and treating them early is noted (Preston et al., 2013). Based on the results obtained, it can be affirmed that this research supports the hypothesis of the universal tendency to acquire speech. The presence of infantile lisp, both substitution of /z/ with /s/ and of /s/ with /z/, is very common in substitution errors. It is a developmental disorder that does not require speech therapy in most cases, as it is resolved with age. In our study, the high presence of substitution of /z/ with /s/, 16.2%, 95% CI (12%, 20%) and of /s/ with /z/, 8.7%, 95% CI (5,5%, 12%) is observed. When the child substitutes a phoneme, he/she usually does it with another one that is similar. This is the case with the lisp where /s/ (alveolar fricative) is replaced by /z/ (dental fricative). One of the hypotheses that is evaluated in this study is that a high percentage of schoolchildren have this type of sigmatism, due to the mechanisms used by the child in the language acquisition process. This could be due to the lower position of the tongue caused by tooth replacement and to this being a more comfortable position for the tongue as a result. Anterior open bites due to tooth replacement will facilitate the escape of air and, therefore, a distortion of the phonemes with anterior place of articulation, as the position of the tongue varies, placing it in a lower position. In the literature review, no other study was found that investigated the prevalence of lisps in a sample of schoolchildren, like this study. Groups of altered phonemes are often observed in schoolchildren. It has been shown that there are few schoolchildren with just a single altered phoneme, the most frequent single SSDs being those involving /r/ and /s/. There is a significant relationship between phonetic alterations and age, these being significant in 5-year-old children, who still have their primary dentition. The SSDs observed in children decrease as age increases. The etiology of SSD may be due both to a lack of motor skills in the speech organs and to a deficit in auditory discrimination. This coincides with other studies carried out (Ahmadi et al., 2019; Stahl et al., 2007) in that the number of phonetic alterations decreases with mixed dentition. There is a significant relationship between male gender and SSD. This coincides with most of the studies, in which it is associated to a higher degree with SSD (Georgievska-Jancheska, 2019; Riekman & el Badrawy, 1985; Salvago et al., 2019). In other studies there is no significant association, but the percentage of boys is higher than that of girls (Ahmadi et al., 2019; Farias et al., 2006). There is no significant relationship between SSD in children and lower-middle socio-economic status. Economic situation does not appear to have an influence on dyslalia found in the children in this study. This is in contrast to various studies where it appears to be a predictive factor for the appearance of speech alterations (Eadie et al., 2015). The results obtained show that the most frequent habit is the introduction of objects in the mouth, followed by finger and lip suction and the use of a pacifier. Both in the literature review and in this study, it can be observed that the percentage of the presence of oral habits in the population of schoolchildren depends on the variables that have been studied, as well as the age at which the study was carried out. In the study by Laganà et al. (2013) it was observed that the prevalence of habits was similar to that of this research. Children from 7 to 15 years old who did not present habits represented 80.6% of the population, 10% of the total with digital suction and 4% with lip suction. This differs from our study in terms of age and percentage of habits. Farsi and Salama (1997) observed that 48.36% of children had oral habits. This coincides with both studies where finger suction is approximately 10% of the sample. In the case of Farsi and Salama (1997), pacifier sucking is linked to samples at earlier ages. The introduction of objects in the mouth also appears in younger children and is related to the transition from breastfeeding to bottle feeding. This is one of the reasons why children satisfy their anxiety by putting objects in their mouth. As the child grows, this habit is suppressed, but other later habits such as nail biting may appear. Regarding atypical swallowing and the resting position of the tongue, similar results are found in studies carried out by Grabowski et al. (2007), both in atypical swallowing (62%, 63.5%) and by altered position of the tongue at rest (36.6%, 42.6%). Other studies present lower percentages than this one regarding the presence of atypical swallowing, these being 23% (Farronato et al., 2012) and 16.2% (Laganà et al., 2013) and with the low resting position of the tongue representing 9.6% of the population in the case of Laganà (2013). These very low percentages, compared to this study, are basically due to the fact that they were obtained from older children and in many cases tooth replacement had already been completed. Hanson et al. (1969) observed that of the 1,615 children from 6 to 18 years of age studied, 41% had atypical swallowing. Several studies agree that the altered resting position of the tongue has a lower percentage than that of atypical swallowing. Cases of atypical swallowing may occur, but when the tongue is at rest it acquires a normal position, that is, a high position in the palatine ridges. In this study we highlight the significant relationship between bad oral habits and SSD. In this case, the groups of altered phonemes have been calculated separately, specifically with the groups /p/, /b/ and /k/, /g/, /j/. The results agree with different studies, although they differ in the age of the sample and in that the same habits are not always evaluated (Barbosa et al., 2009; Farronato et al., 2012; Ferriolli, 2010). There is a highly significant relationship between the presence of SSDs and atypical swallowing, coinciding with different studies (Eslamian & Leilazpour, 2006; Lebrun, 1985; Suzuki et al., 1981; Van Lierde et al., 2015) and in contrast to other authors (Khinda & Grewal, 1999) who did not find a direct relationship between atypical swallowing and alterations in the phonemes evaluated, but did find a direct relationship between malocclusion and SSDs and between malocclusion and atypical swallowing. Likewise, the Malandris and Mahoney’s (2004) study established a relationship between crossbites and difficulty in articulating the phonemes /s/, /r/, and /l/ and concluded that good oral motor function is essential for proper speech development. This dependence between atypical swallowing and SSDs is due to the fact that the inadequate position of the tongue in the oral cavity leads to a disorder of the orofacial muscles and a possible dental malocclusion. Inadequate oral motor function influences a child’s phonetic articulation. This is important to the language acquisition process. In this study, the dependency relationship of dyslalias and oral habits is not strong, although it does appear in certain phonemes. As limitations of this study, it should be mentioned that the socio-economic level is studied in more depth in other studies looking at the income of each family, while we take as a reference the location of the schools and the geographical areas. It has been carried out in this way to facilitate the study, since the request for information as sensitive as income would have limited the number of participants. In addition, we are aware that as the study was carried out in the Valencian Community with a group of schoolchildren who, although all speak Spanish, in many cases may have Valencian as their mother tongue and/or schooling language, this represents another limitation in terms of its generalizability. Rhotic phonemes, which are the most difficult to articulate and the last in phoneme acquisition, could also have been studied in more depth. It would be important to evaluate the phoneme at the beginning of the word, in the middle, and at the end, as well in consonant clusters, as has already been done in English language studies (Chung et al., 2019). It has not been possible to investigate this topic further because, as mentioned in the introduction, the acquisition of these phonemes extends to 8 years of age and our study was carried out in children aged 4 to 7 years. As a strength and key finding of the study carried out, in addition to identifying the prevalence of error in fricative phonemes /s/ and /z/, since many studies identify the difficulty of their articulation, we have studied the frequency with which one phoneme is substituted by another. In addition, this study identifies the number of altered phonemes that commonly occur in schoolchildren. It is more common to find two, three or four altered phonemes in the school than just one. There are few studies in the Spanish language that investigate in depth the process of acquisition of phonemes in the infant and those etiological causes in the difficulty of articulation of the phonemes such as the type of dentition, the position of the tongue, gender, age, and the socio-economic situation. SSDs in school-age children are highly relevant due to the repercussions they can have on personal and academic development. The acquisition and development of language at the oral level must follow a certain process that, if interrupted by any factor, can lead to difficulties in educational performance, in development of social skills, and even at the psycho-affective level. This study helps us to quantify the prevalence of phonetic alterations in schoolchildren, the most frequently altered phonemes, and the type of error. Both the evaluation and rehabilitation of phonological disorders often overlook the type of swallowing. This study shows that there is an important significant relationship between these alterations that would fall within the orofacial dysfunctions of the infant. Epidemiological studies are essential, since they highlight the importance of carrying out early evaluations in order to detect the existence of articulatory difficulties as soon as possible and carry out early intervention programs. The different professionals who work with children with speech difficulties (teachers, speech therapists, counsellors, educational psychologists, etc.) play a key role, being fundamental for the stimulation of communicative linguistic competences, thus avoiding the development and consolidation of SSD. In short, this research gives importance to multidisciplinary work, be it paediatric dentists, paediatricians, psychologists, or speech therapists who can complement the diagnosis and identify SSD. Conflict of Interest The authors of this article declare no conflict of interest. Cite this article as: Amr Rey, O., Sánchez-Delgado, P., Salvador Palmer, M. R., Cibrian Ortiz De Anda, R. M., & Paredes Gallardo, V. (2022). Exploratory study on the prevalence of speech sound disorders in a group of Valencian school students belonging to 3rd grade of infant school and 1st grade of primary school. Psicología Educativa, 28(2), 195-207. https://doi.org/10.5093/psed2022a1 References Appendix Supplementary material Table S1 Questionnaire for Parents  Table S2 Induced Phonological Register  Table S3 Auditory Discrimination 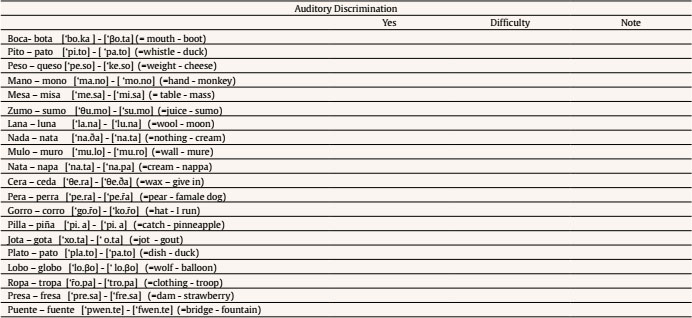 Table S4 Orofacial Myofunctional Clinical Examination 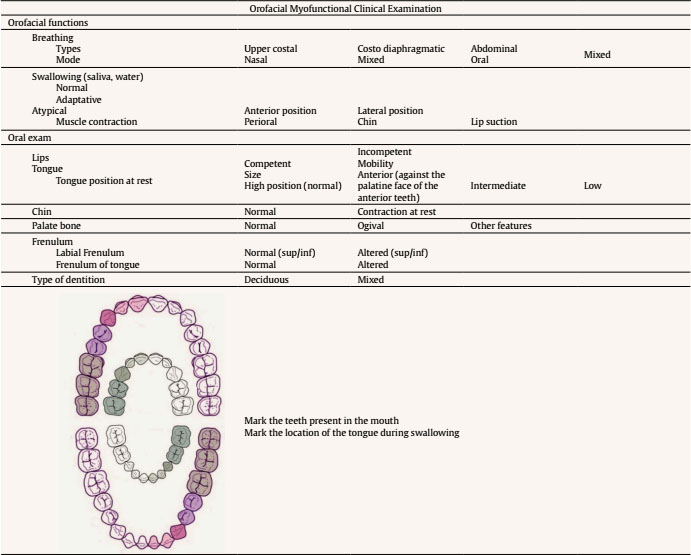 Table S4 Distribution of the Study Group according to whether or not There is Presence of Interdental Sigmatism  Table S5 p-value of the Chi-square Test corresponding to the Relationship between the Alteration of the Phoneme and Poor Oral Habits  Note. Bold values indicate statistical significance equals p < .05. |
Cite this article as: Rey, O. A., Sánchez-Delgado, P., Palmer, M. R. S., Anda, M. C. O. D., & Gallardo, V. P. (2022). Exploratory Study on the Prevalence of Speech Sound Disorders in a Group of Valencian School Students Belonging to 3rd Grade of Infant School and 1st Grade of Primary School. Psicolog├şa Educativa, 28(2), 195 - 207. https://doi.org/10.5093/psed2022a1
purificaci├│n.sanchez@uv.es Correspondencia: purificaci├│n.sanchez@uv.es (P. S├ínchez Delgado).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Imprimir
Imprimir Enviar
Enviar
ALERTA POR E-MAIL
La Revista de Psicología Educativa está distribuida bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObra Derivada 4.0 Internacional.com








