


Efficacy of Early Intervention Programmes: Systematic Review and Meta-analysis
[Eficacia de los programas de atención temprana: revisión sistemática y metaanálisis]
Ramón Gómez-Cotilla, María de los Ángeles López-de-Uralde-Selva, and Luis Valero-Aguayo
Facultad de Psicolog├şa y Logopedia, Universidad de M├ílaga, Spain
https://doi.org/10.5093/psed2024a1
Received 26 February 2022, Accepted 18 January 2023
Abstract
Background: Early childhood intervention is a form of intervention aimed at children to overcome difficulties in different areas of their development after birth. There are multiple early intervention programmes, but only a few studies assess their efficacy using data. Objective: A systematic review and meta-analysis of early intervention programmes was carried out. Method: Inclusion criteria were considered to be empirical studies, with outcome data on children between 0 and 6 years of age with various developmental problems. The review was conducted in nine databases. Results: Of the total number of studies from 2000 to 2021 in English and Spanish, 40 studies were included that looked at the efficacy of the programmes. Of these, 19 used comparisons with a control group, and 13 used single-subject designs, as well as other designs. The programmes were very diverse, mostly based on behavioural procedures, and aimed at promoting the development of specific areas. The quality of the studies is medium-high. The meta-analysis included 18 studies with a mean effect size d = 0.45 (CI = 0.18, 0.67), with high sample heterogeneity and low study selection bias. Conclusions: Early childhood interventions have a medium and positive efficacy on the skills and abilities of children with developmental problems. The limitations of the reviewed studies are discussed, as well as the need for well-defined programmes, long-term measurements, and comparisons of different types of programmes among them.
Resumen
Antecedentes: La atención temprana es una forma de intervención dirigida a niños y niñas para intentar superar las dificultades en distintas áreas de su desarrollo tras el nacimiento. Existen múltiples programas, pero pocos estudios comparando con datos su eficacia. Objetivo: Se ha realizado una revisión sistemática y un metaanálisis de los programas de atención temprana. Método: Como criterios de inclusión se consideró que fuesen estudios empíricos con resultados sobre niños con diversos problemas de desarrollo entre 0 y 6 años. La revisión se realizó con nueve bases de datos. Resultados: Del total de estudios desde 2000 a 2021 en español e inglés se incluyeron 40 estudios que permitían ver la eficacia de los programas. De ellos 19 utilizaron comparaciones frente a un grupo control y 13 con diseños de caso único, además de otros diseños. Los programas de atención temprana fueron muy diversos, en su mayoría basados en procedimientos conductuales y dirigidos a impulsar el desarrollo de áreas específicas. La calidad de los estudios es media-alta. En el metaanálisis se incluyeron 18 estudios con un tamaño del efecto medio, d = 0.45 (CI = 0.18, 0.67), con gran heterogeneidad de las muestras y poco sesgo en la selección de estudios. Conclusiones: Los programas de atención temprana presentan una eficacia media y positiva con respecto a las habilidades y capacidades de los niños y niñas con problemas de desarrollo. Se comentan las limitaciones de los estudios revisados y la necesidad utilizar programas bien definidos, mediciones a largo plazo y comparaciones de diversos tipos de programas entre sí.
Palabras clave
Atenci├│n temprana, Revisi├│n sistem├ítica, Metaan├ílisis, Retraso, Discapacidad intelectual, Autismo, S├şndrome de DownKeywords
Early intervention, Systematic review, Meta-analysis, Developmental delay, Intellectual disability, Autism, Down syndromeCite this article as: Gómez-Cotilla, R., López-de-Uralde-Selva, M. D. L. Á., & Valero-Aguayo, L. (2024). Efficacy of Early Intervention Programmes: Systematic Review and Meta-analysis. Psicolog├şa Educativa, 30(1), 1 - 10. https://doi.org/10.5093/psed2024a1
Correspondencia: lvalero@uma.es (L. Valero Aguayo).
Early intervention (EI) is a way of dealing with the multiple developmental problems in some children with special characteristics, or children at risk of suffering from them. EI is a form of intervention that involves comprehensive care that is provided to the children and their family during the first years of life (Belda et al., 2000; Perera, 2011). Initially, it was Dunst (1985) who defined EI as a composition of multiple interventions in different areas consolidated in different resources for families. The European Agency for Development in Special Needs Education (Meijer, 2003) produced a document to reflect the different trends in European countries and the contributions of different disciplines (psychology, neurology, paediatrics, physiotherapy, pedagogy, and speech therapy). This document was key for the development of the concept of EI and its application. Thus, currently, the concept of EI covers contributions from the sphere of health, education, and social sciences. The intervention becomes exclusively child-centred, from a perspective that includes the child, the family, and the community where they live (Belda et al., 2000; Guralnick, 2001; Perera, 2011). In Spain there are two forms of EI: (1) the health system with its network of hospitals and (2) the social services system, with IMSERSO as the most important service for those problems. In the 1990s, EI services were shared among the different institutions (health, educational, and social services), with no division of competences between them, and also with great disparity of actions, varying according to the regional community where they were offered. Subsequently, the Early Intervention Group (GAT, 2005) was created and transformed into a manual (Early Intervention White Paper) that describes EI as “the set of interventions aimed at the child population aged 0-6 years, the family, and the environment, whose objective is to provide, as soon as possible, the transitory or permanent needs of children with development disorders or who are at risk of suffering them” (p. 12). Despite the advances, EI programmes are very diverse, depending on the policies and each regional community, hence, the results and publications of their efficacy can be very diversified. In Spain, this work is mainly carried out in the Early Childhood Development and Care Centres (CDIAT), where individualised interventions are provided to children and families who need them. Those centres could show data on the efficacy of these programmes, taking into account the potential areas and difficulties of each child in his/her development, the contexts in which he/she is placed, and the resources of his/her family and school settings (Millá-Romero, 2020). Nowadays, EI programmes are based on theoretical foundations that highlight the importance of the context/environment and their relationship with the child (Tollan et al., 2023). Basically, six approaches can be identified: (1) the biopsychosocial model, developed by the World Health Organization (WHO, 2001), which seeks to integrate the child into his/her context as well as his/her autonomy; (2) the ecological-systemic model, which also seeks to normalise a child’s situation and his/her continuing integration into his/her family and social context (Burger, 2014); (3) the transactional model, which also emphasises the interdependence of the child with his/her social context (Sameroff & Fiese, 2000); (4) Feuerstein’s theory of structural cognitive modifiability (SCM) (Feuerstein & Jensen, 1980), focusing on a child’s capacity for learning and maturation always within the mechanism of cultural transmission; (5) the activity-based approach (Bricker & Cripe, 1992), which proposes a global learning theory of the authors about developmental psychology and functional activities for a child’s life; and (6) intervention programmes with a behavioural approach (Howlin et al., 2009), which are usually part of many of the elements of the previous programmes, but which have demonstrated their efficacy in a specific way, such as Applied Behaviour Analysis (ABA), Early Intensive Behaviour Intervention (EIBI), Treatment and Education of Children with Autism and Associated Communication Problems (TEACCH), the DENVER model (Fuller et al., 2020), which involves intensive communication training, cognitive-behavioural therapy, and parent training, or the LOVAAS programme, which proposes a comprehensive and highly-structured training of functional and life-relevant behaviours for the child. On the basis that EI practices should be evidence-based and ethical, the Division of Early Childhood (2014) has aimed at organising these finding into different topics. This association recommends a series of EI practices in order to advise families and professionals on the most effective ways to enhance learning and promote the development of children under five years of age. The Workgroup on Principles and Practices in Natural Environments (WPPNE, 2008) also outlines some principles that EI should have in a child’s natural context. These associations usually describe the forms of intervention that are available and recommend some of them, but mostly without providing quantitative data on their effectiveness. Research on the efficacy of EI is essential in order to increase knowledge about the different aspects of this topic, to develop more effective intervention programmes, to determine which intervention practices give better results, or which characteristics of these interventions influence their success, and also to address the challenge of homogenising the intervention methods in EI professional services. Some systematic reviews and meta-analyses of EI, with specific programmes or populations, have been published, although most of them focus only on autism problems (Daniolou et al., 2022; French & Kennedy, 2018; Fuller & Kaiser, 2020; Sandbank et al., 2020; Virués, 2010), or a specific population such as the study by Taubner et al. (2015), which focussed on German children, or the study by Ribeiro et al., (2022), with only Brazilian people in the study sample. Other studies analyse the effect of EI on later cognitive and social development (Camilli et al., 2010), its impact on overcoming the deficiencies of unstructured and poor environments (Barnett, 2011), or the intervention with parents where the positive influence on the outcomes seems to be demonstrated (Rojas-Torres et al., 2020). On the other hand, the accessibility to these services for families is also a major influence (Sapiets et al., 2021). In turn, other meta-analysis studies have focused only on one aspect, such as language and communication (Seager et al., 2022). However, much of the literature on the topic is theoretical or consisting of compilations or qualitative literature reviews (Kingsley & Mailloux, 2013; NSW, 2005; OECD, 2020; Romsky et al., 2015). For these reasons, the present study carries out a systematic review of effective treatments or programmes in the field of EI, with children aged 0 to 6 years, who present different types of disorders (motor, cognitive, sensory, generalised, emotional, somatic, etc.), during the period of 2000 to 2021. From this review, a general quantitative conclusion is sought on the efficacy of these programmes; hence, a meta-analysis of those selected studies that present comparative data on which to carry out this analysis is also carried out. A search was carried out for empirical studies on EI, involving some type of intervention or treatment that is aimed at children aged 0 to 6 years who have or may have developmental problems of different types and diagnoses. Specifically, the search was carried out on those treatments that were aimed at the most common disorders: autism spectrum disorder (ASD), developmental disorder (DD), Down syndrome (DS), prematurity, and Fragile X syndrome (FXS). Document Selection The search was conducted through format sources including nine data bases: PubMed, ScienceDirect, PsycInfo, Scopus, Dialnet, Psicodoc, Isoc-Psicología, Redalyc, and the dissertation platform (TESEO). The following were considered as inclusion criteria:
Figure 1 PRISMA Scheme of the Study Selection Process. 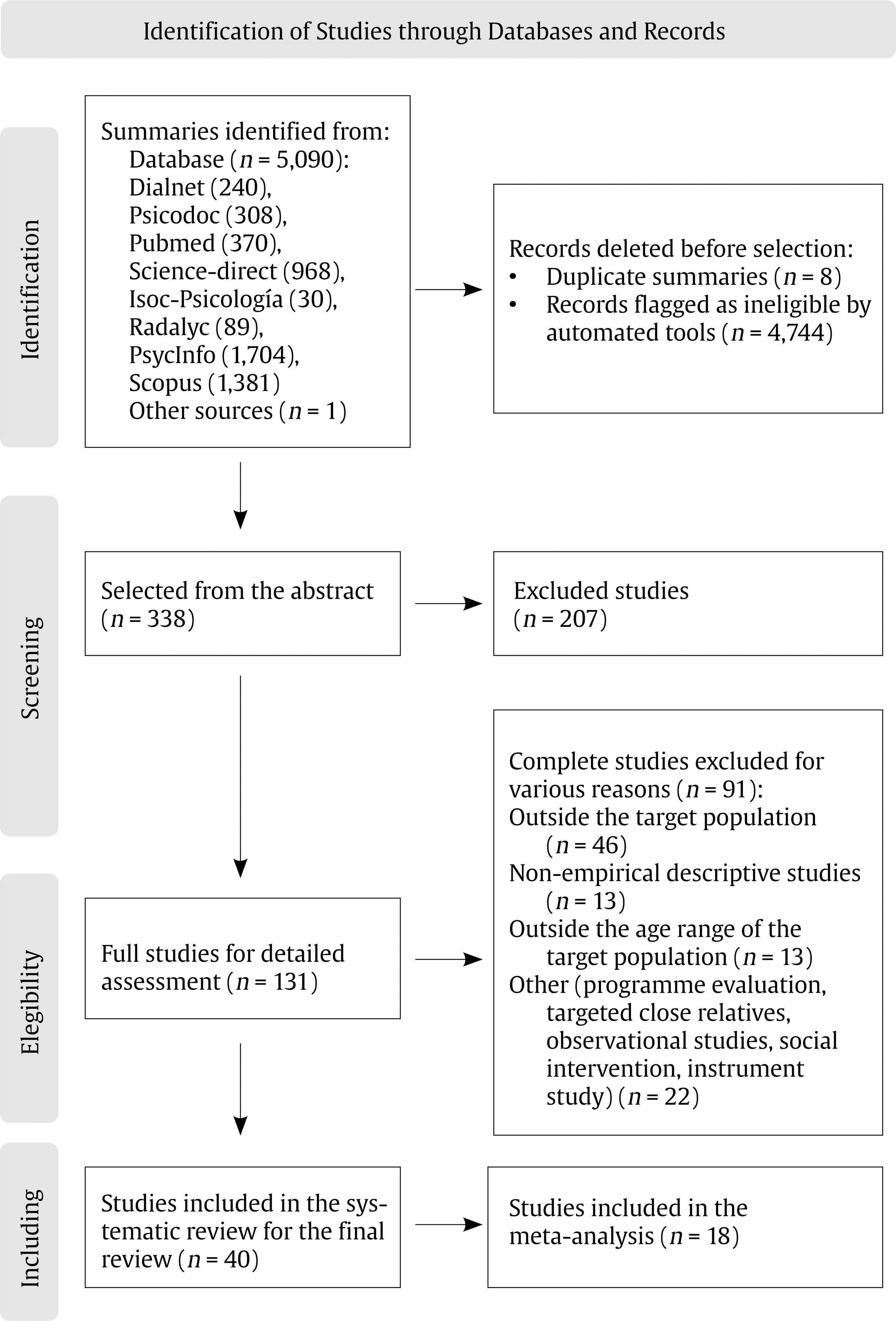 The following were used as exclusion criteria:
The search terms used were: (“Early chilhood” OR “Child*”) AND (“Intervention” OR “Treatment” OR “Programme”), and similarly in the Spanish database (“Infancia” OR “Niñ*”) AND (“Intervención” OR “Tratamiento” OR “Programa” OR “Tempran*”). These terms were adapted according to the database used, including filters determined as inclusion and exclusion criteria. Searches were conducted in both English and Spanish languages. The data range of the studies was from 2000 to 2021. Selection and Coding Process The first identification phase included a total of 5,090 studies, of which those that did not meet the inclusion criteria and were duplicated were eliminated from the titles, both automatically by search tools and by direct review by the authors. In the screening phase, from the abstract, another 207 additional studies that did not meet the inclusion criteria were excluded. Of these, a total of 131 studies were selected to read the full texts, of which 91 were excluded for different reasons, with respect to the inclusion or exclusion criteria. Finally, 40 studies that met these criteria were included in the systematic review. In turn, for the meta-analysis, a total of 18 studies were included from all of those that included specific data on the results and on the sample, in order to compare their effect size. An Excel file was used for coding the different studies, in which the characteristics of these studies were included as categories: authors, date, country, type of disorder, type of design, assessment tests, type of participants, sex, range and mean age, duration of the treatment, general results, N, M, and SD data in control and experimental groups, and also in intra-groups with a design that includes the pre- and post- N, M, and SD data, and also drop-out participants. The review was carried out by one of the authors, and supervised by another author, and finally the selected texts were read and classified in consensus by all of the three authors. Figure 1 shows the PRISMA scheme of the selection process. Quality of the Studies Each of the 40 selected studies underwent methodological quality assessment following a summary scale (García-Llana et al., 2014), based on the criteria of Berra et al. (2008). This 12-item scale assesses yes/no compliance with each criterion:
According to this scale, each study would have a score between 0 and 12, where it is rated as low (1-4), medium (5-8) and high (9-12) quality. Data Analysis A meta-analysis was performed on the basis of these selected studies. In this case, as inclusion criteria for the meta-analysis, studies had to provide the quantitative data that are necessary to calculate their effect size (means, standard deviation, and tests of statistical significance for the compared groups); and single case studies were excluded, even if they included efficacy data. We also excluded studies that lacked data in any of the groups, that did not use standardised tests (some used only observational data) that would allow comparison between studies, or that were aimed at change in family relationships or parent training, rather than changes and improvements in children. Thus, a total of 18 studies were selected for meta-analysis, some of which involved multiple comparisons because they had several groups. Of these, 15 used between-group designs and 3 used within-group designs. The data from each study were included in the statistical programme RevMan 5.3 (http://tech.cochrane.org), where the meta-analysis was carried out in two sections: (1) studies with between-group designs and (2) studies with within-group designs. As specific comparison data for each study we used data that involved standardised tests on intellectual, social, verbal, motor, and other skills that were the more common among the various studies compared (e.g., ADOS-G, CUMANIN, Portage, IQ, SISS, EHPAP, Mullen-ELC). Since some studies included several measures, many of them aimed at parents, we selected the instrument that was more general and common to all studies on the topics and that assessed the set of behavioural areas and (motor, language, autonomy, relational, social) skills. In the case of studies with between-group designs, M and SD of the experimental and control groups in the post-measures were taken, in addition to the corresponding number of participants. In the case of intra-group designs, M and SD at pre- and post-treatment were taken. A random effect analysis model was used. In some of the studies two comparisons were included because the design was not only with the control group, but also with two different intervention groups or normative groups. A funnel plot was performed to look at possible publication bias and analysis of which study contributed most to the overall effect size. A forest plot was performed, with the studies ordered by their possible weight in the sample with respect to the overall analysis in order to observe their influence on the final result. Further, to analyse the possible sensitivity of each study, a re-analysis was performed by eliminating each study, one by one, as a process with which to estimate the sensitivity effect on the overall impact by including or excluding the effects. Among the 40 studies that met the inclusion criteria, half of them (20) focused on treatments of children with autism (ASD), 9 evaluated treatments for children with developmental disorder (DD), 5 focussed treatments on children with Down syndrome (DS), 4 focussed on therapies or programmes for premature children, and 2 provided treatment for infants with Fragile X syndrome (FXS). The studies reviewed included a total of 1,884 participants (22.5% girls and 77.5% boys), which is in line with the usual data for a higher prevalence of developmental problems in girls and boys. Most of the studies provide information on the sex of the participants, but 5 of them do not provide such data. Two studies included only girls, and 8 studies included only boys. The study with the smallest number of participants was a single-case design (Robles-Bello, 2011) and the study with the largest number had 519 participants (Smith et al., 2019). The age range of the participants was between 7.5 and 78 months. Only one of the studies did not report the age of the participants. Data on the duration of treatment also show a wide range of duration from 2 months to 4 years of intervention. In 7 of these studies, the duration of the treatment used was not indicated. The validated and standardised instruments used in these studies varied widely. As children are in the early childhood intervention age range, they are usually assessed with many instruments at the same time in order to make an overall evaluation of their development and to see if the treatment proposed really has the desired effect. This is why we have found a wide variety of instruments in the different studies, all of which assess different types of skills and abilities (physical, motor, intellectual, emotional, social, developmental, comprehensive and productive communication, etc.). Among them, we can highlight, from the most to the least used, the following: Autism Diagnostic Observation Scale (ADOS), 10 studies; Mullen Scales of Early Learning (MSEL), 6 studies; Vineland Adaptive Behavior Scales (VABS), 6 studies; Brunet-Lezine Early Childhood Development Scale (B-L), 4 studies; Autism Diagnostic Interview-Revised (ADI-R), 3 studies; Childhood Autism Rating Scale (CARS), 2 studies; and others that are used in specific studies or added to the above instruments. The research teams and their publications were mostly from the USA (16 studies), Spain (10 studies), and to a lesser extent from other countries such as Australia (3), Brazil (3), and Canada (2), and the remainder were from other countries with only one study. In terms of design, most of the studies analysed used a between-group experimental design (19 studies), comparing a control versus an experimental group with the EI programme, and also single-case designs (13 studies), with various measures in each case and replications with several participants with different characteristics; to a lesser extent there are single group pre-post studies (3 studies) and 4 studies with longitudinal designs following participants with multiple measures over several months and also one correlational study with respect to treatment. Regarding the ways of intervention, practically all the studies used some type of treatment or programme that was based on behavioural procedures (modelling, routine training, ABA, reinforcement programme, stimulation prompts, etc.). Different areas of child development were addressed: intelligence, joint attention, verbal and non-verbal language, adaptive function, communication, social skills, emotions, cognitive skills, personal autonomy, socialisation, visual and verbal memory, and global development. Other studies focussed on concrete learning, such as the use of objects, word-object association, regulation of emotional states, signs learning, and generalisation of behaviour in a natural context, at other times and in other situations. Table 1. Methodological Quality of the 40 Studies Reviewed, according to the Criteria of Berra et al. (2008) and García-Llana et al. (2014) 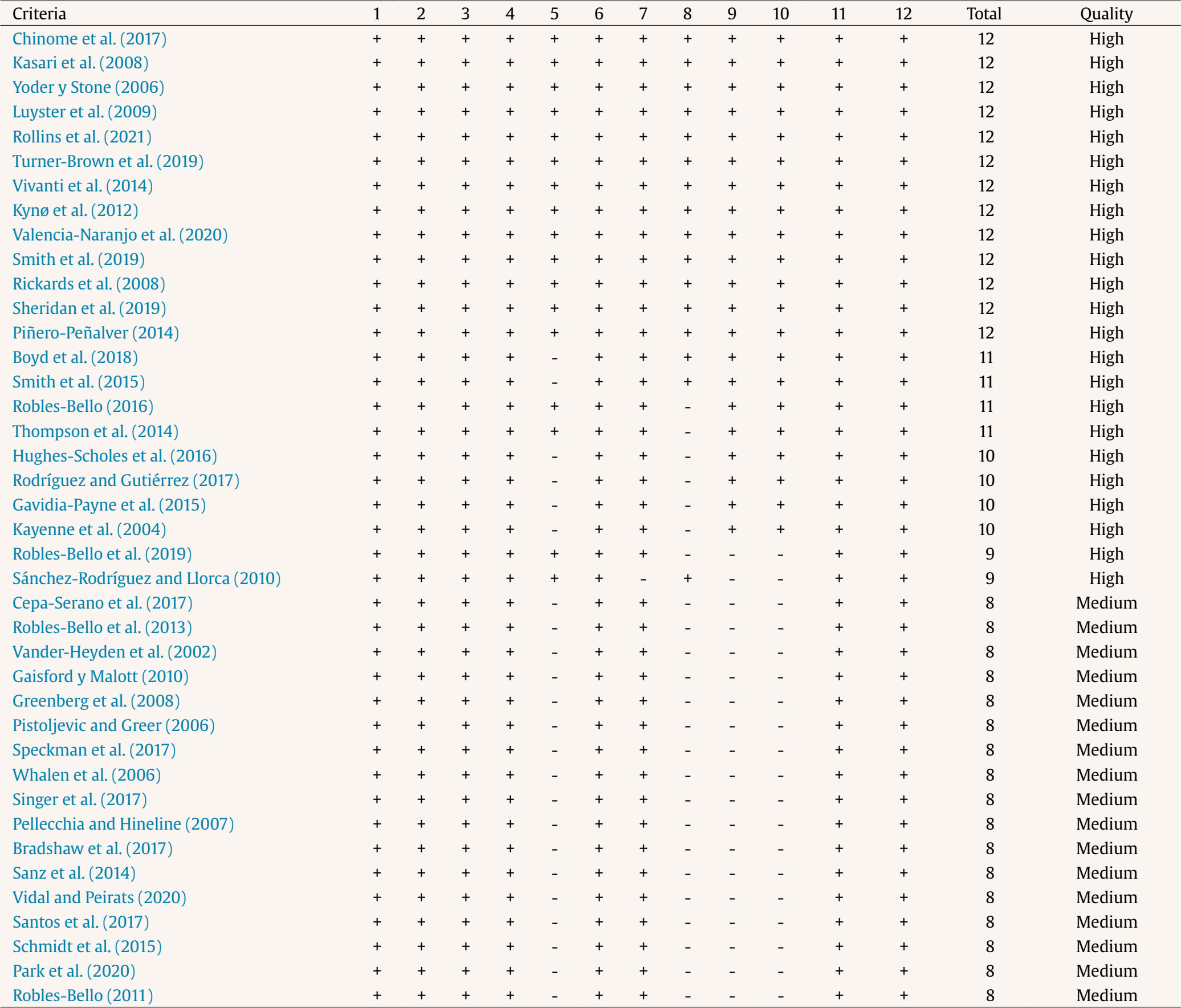 Regarding the quality assessment of these studies, following the scale of the criteria adapted from Berra et al. (2008) and García-Llana et al. (2014), as described above, most of the studies were of medium-high quality, with a range of scores between 8 and 12. There were no studies classified as low quality (1-4 points), 16 were classified as medium quality (5-8 points), and 24 were classified as high quality (9-12 points). The results of this methodological quality assessment are shown in Table 1. In several articles, it is specified at what point there was a drop-out of participants, and/or data for the correct treatment of these in the statistical analysis. In all studies, practical implications of the results for future research appear in the discussion. Results according to the Type of Disorder Autism (ASD) From the studies analysed in the review, 20 of them evaluated programmes which included children with autism. We found that most of them improved some area of children’s development, and a small percentage had no effect in some areas. In general, the programmes produced improvements in the areas of expressive language, joint attention, joint participation, social skills, communication, social interaction, adaptive functioning, cognition, decrease of disruptive behaviour, and daily routines. They also improved practice in object use, word-object association, and object matching. In one study, communication with adults improved, but did not generalise with respect to siblings and peers (Pellecchia & Hineline, 2007); in another study, social communication and play did not improve, but participation did (Boyd et al., 2018); finally, in one study, there was no effect on global measures, although there was an effect on social and communication skills (Turner-Brown et al., 2019). Figure 2 Meta-analysis Data from Studies with between-group and Pre-post Designs, comparing Early Intervention Programmes with Control Groups. 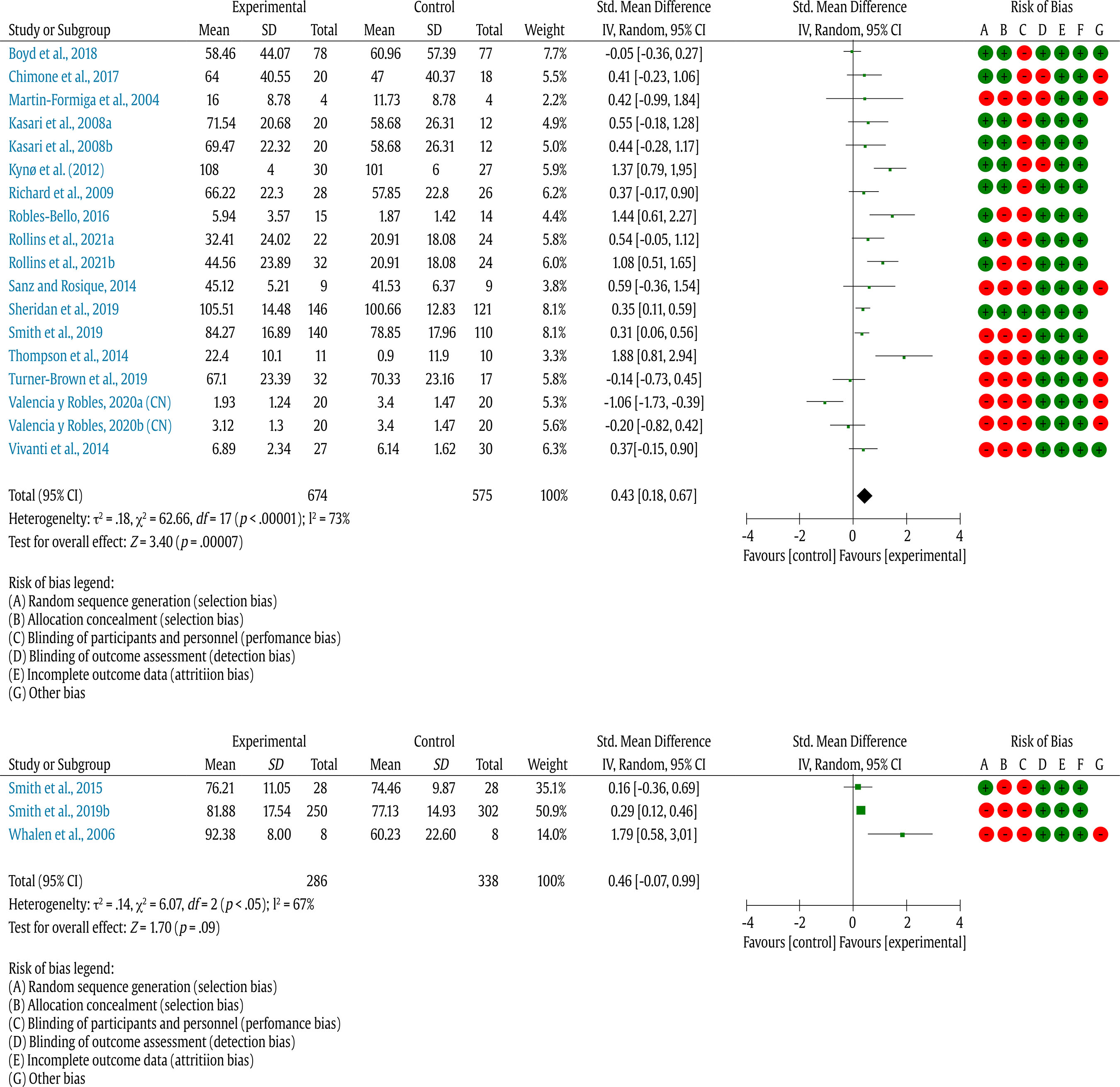 Developmental Disorder (DD) Nine of the studies reviewed proposed programmes aimed at children with developmental disorders. They highlighted improvements in the following areas: development of emotional competences, social interaction, communication, expressive language, autonomy, and social skills. On the other hand, progress was observed in routines at home and in the community, generalisation of object matching, word-object association, and learning signs. Down Syndrome (DS) Five of the studies in the review address the treatment of children with this problem, where object handling improves after social reinforcement, socialisation, autonomy, language, perception, and cognition. In one of the studies, the results support a differentiated intervention for children with Down syndrome and mosaic trisomy 22 despite the similarity of the disorders (Robles-Bello, 2016). Finally, in another study a girl showed improvement in interaction with adults, but not in object handling, a fact that does not occur in the boy participant in the same study, who improves in interaction with objects and with the adults (Vander-Heyden et al., 2002). Premature In the 4 studies that evaluated the efficacy of EI in preterm infants, we found the following: improvement in typical developmental behaviours, improvements in state regulation and social interaction. In addition, one study highlights that intervention of these children, carried out in the hospital setting and in the EI centre, had immediate and medium-term positive effects for the preterm baby (Piñero-Peñalver, 2014). In another study, no significant effects were found in the development of different areas (Kynø et al., 2012). Fragile X Syndrome (FXS) The 2 studies included in the review on this disorder indicate the need to work on the area of autonomy for these children, and in one of them the motor area was also added (Robles-Bello, 2011). However, in both studies there is an improvement in the children in the different areas of development after the EI programme. Meta-analysis Finally, 15 studies with between-group designs were included in the meta-analysis, after discarding those studies that did not offer direct data for comparison, only showed post data or only showed final statistical data. In several studies there are three groups, because of the effect of two with experimental treatment versus the untreated control group, or normative control groups, with a total of 18, by comparison. Given the heterogeneity of studies, a random effects analysis model was performed. Figure 2 shows the forest plot with the mean effects and confidence interval for each of these comparisons. The mean effect size is 0.43 (CI = 0.18, 0.67), which implies a significant effect (Z = 3.40, p = .0007). That is, overall, there is a significant effect on the increase in scores of tests of skills and normative development of children who have participated in these EI programmes, and it is a medium value for the effect size following Cohen’s (1988) criteria. The greatest effects are found in the study by Kynø et al., (2012), with d = 1.37 in which, although they do not show significant differences in individual skills, they do appear on the global development scale, and that of Robles-Bello (2016), with d = 1.44, which shows improvements in the different areas of activities in children with Down syndrome, and that of Thompson et al. (2014), with d = 1.88, focused on the family, where parent-child interactions and communications improved, although not so much regarding language. The study by Valencia-Naranjo and Robles-Bello (2020), with d = -1.06, is the only study that shows a negative effect on the learning potential programme, but this is due to the comparison of the children with Down syndrome with the normative groups, and the other group with intellectual disabilities also with the normative control group; hence, both groups advanced and improved in their skills, but not enough to match the normative children. On the other hand, there are only 3 studies that make a pre-post comparison with the EI programme. In this case, although there is a similar effect size (d = 0.46), it is not significant (Z = 1.760, p = .09), and the small number of studies means that these results are not considered. In the set of studies, a total of 674 participants in the experimental groups applying EI were compared to 575 in the controls. No study can be considered to have more weight than the others in the average result (the weights range from 2.2% to 8.1%). When the studies are removed one by one from the overall result, the result is only 0.10-point variation in the mean effect; therefore it can be said that the results are systematic and there is no study that particularly biases the data. The heterogeneity of the selected studies is high (I2 = 73%, τ2 = .18, χ2 = 62.66, p < .00001), hence a random effects analysis has been selected. This is probably due to the variety of problem types addressed, as well as the variety of assessment instruments. Although they are all comprehensive and standardised, there is no single instrument that covers all the repertoires that are involved in a normative development process. As aforementioned, in the various studies there was progress in some areas, but not in others, and improvements were not uniform in all of them. For this reason, the variety was such that it was not possible to include an analysis of variance for possible moderating variables of this efficacy. The analysis of the tunnel plot also shows a normal triangle distribution which allows us to state that there is no publication bias (see Figure 3). Regarding possible bias in research quality, we included an assessment of each study for possible biases in randomisation, allocation of participants, double blinding of treatment and assessment, incomplete results, or selection to support conclusions. In this case, most of the potential biases are found in the form of randomisation and allocation of participants, as many of the studies do not randomise completely or are assigned to groups according to their prior characteristics. Figure 3 Tunnel Plot Showing the Distribution of Possible Publication Biases. 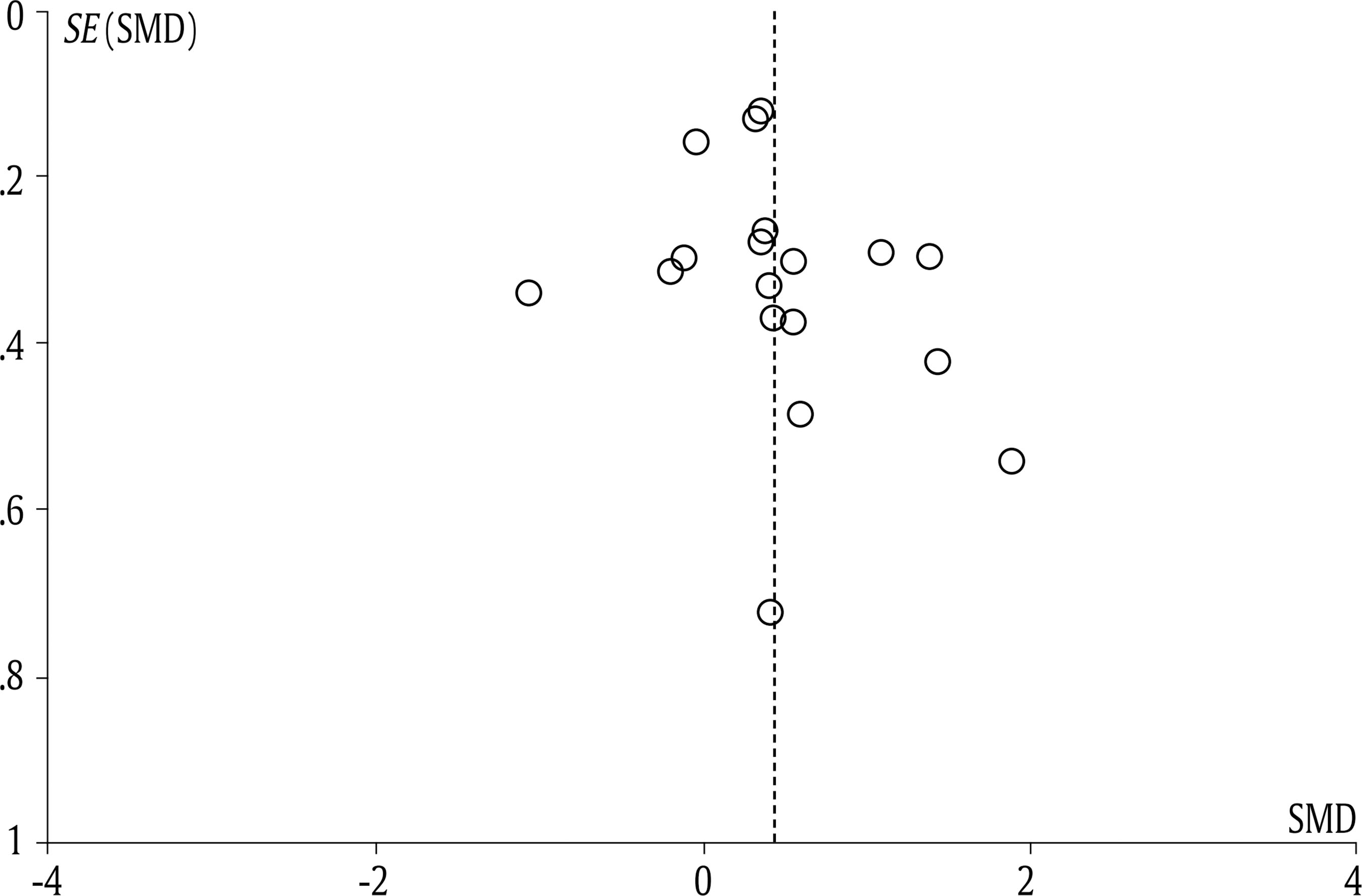 In general terms, the studies analysed present treatment or programmes implemented in children who show the different types of disorders related to intellectual disability (due to ASD, TD, Down, FXS, etc.), apart from other difficulties in communication, and social and emotional relationships. In this way, the interventions were aimed at children with ASD, which usually affects the development of the areas of social skills and social interactions, being the most marked deficit in these disorders. In this line, it was found that the EI suggested by the different studies improved motor skills and daily life especially (Daniolou et al., 2022); also, social skills, communication (verbal and non-verbal language), social interaction through the learning of relationships with adults, objects, peers, and also procured the development of adaptive functions, autonomy and adaptive behaviour. Other meta-analyses have also found these benefits (French & Kennedy, 2018; Virués, 2010), although other analyses show no differences between different types of treatment approaches (Sandbank et al., 2020). The EI programmes aimed at children with DD focus on working in all areas (language, cognition, motor, autonomy, perception), obtaining outstanding results in the improvement of all these areas for the child’s quality of life, in the form of learning daily routines at home and in the community, greater autonomy, and adaptation to the surrounding context. With regard to the EI programmes that were found in the studies for children with Down syndrome, we find that most of them are also aimed at the development of different areas, with improvements in the use of object, socialisation, and cognitive performance. One of the studies reviewed here (Robles-Bello, 2016) should be highlighted regarding the differentiation in the EI programme with respect to variants of the syndrome (mosaic trisomy 22 vs. Down syndrome). In the studies of EI programmes that were implemented for preterm infants, the intervention targeted the overall development of the child, finding improvement in all areas, but with more evidence in social interaction and regulation of emotional states. One of the studies failed to find any significant effect on development after the intervention. However, reviews on EI have always found a positive effect in programmes that intervene at home and with parents (Puthussery et al., 2018; Tollan et al., 2023). Studies related to EI programmes for children with FXS highlight the work on the development of all areas of the child, and suggest to focus on the area of autonomy and the constant evaluation of the deficit in a specific area, and to work in accordance with this individual basis. Although the studies evaluated in the review are by and large of good methodological quality, most of which use randomised designs and between-groups comparisons, many of these studies do not provide an adequate description of the treatment or programme carried out, thus raising doubts about their implementation. Further, they tend to provide very general descriptions. On the other hand, in almost half of the studies (19 out of 40), there is no statistical evidence to assess the effect of the EI programme, because they are single-case designs or with few participants. In 24 of the studies, the samples evaluated do not exceed 30 participants, which may be a problem for the generalisability of the results to the broad population at which the EI is aimed. In some of them, the loss of participants is not properly addressed, which may bias the final effect of the intervention. However, only 4 of the 40 studies show no results or negative results (when compared to normative groups), implying an overall positive effect of all of these EI programmes. Taking these characteristics into account, a meta-analysis was also performed with studies that included direct data in order to compare a mean effect size of EI programmes. In this case, 18 studies were selected, 15 of them with between-groups designs comparing EI with control groups, most of them also randomised. The results show a significant mean effect, d = 0.43, with high reliability, low selection bias, but high variability in the studies. This denotes the efficacy of EI programmes in increasing the different capacities and skills of participant children, always with developmental problems. This effect is larger that the one found in the meta-analysis of Daniolou et al. (2022), which ranged in several areas between 0.28 and 0.40; or that of Fuller & Kaiser (2020), with a mean effect size of 0.35, although their study was focused only on language outcomes. Thus, it can be concluded that EI programmes are effective in overcoming the possible initial deficit that these children have from birth. Although almost all programmes are “packages” of treatment, including multiple procedures and techniques at the same time, they mostly involve behavioural techniques and training of specific skills (gross and fine motor behaviour, comprehensive and productive verbal behaviour, emotional behaviour, daily living, autonomy, social relationships, etc.). In fact, this is a common finding in other reviews on autism, where programmes based on ABA and its application in the child’s natural context obtain better results (Franz et al., 2022; Virués, 2010). With this meta-analysis, we cannot conclude on the greater efficacy of one type of EI programme over another, but we can conclude in general about the efficacy of EI over control groups, or over “treatment as usual”, which is usually merely psychoeducational or informational. Many of these programmes always include components of parent training, emotional and family relationships, etc., which, as Puthussery et al.’s (2018) meta-review shows, are essential for the generalisation and maintenance of these benefits in the daily lives of these children. These results, together with those of other foreseen reviews, would allow advising professionals who are dedicated to EI to focus on specific behaviours and skills to be promoted in children, especially those that are functionally useful for daily life, autonomy, and social relationships. However, it would also be essential to include behavioural techniques and procedures in these EI programmes, which have already been tested and proven to be effective, which are sometimes included as part of other programmes, and other times are present even though professionals are unaware of their using them, so that their education potential is not fully exploited. Further, it would also be important to always include training or teaching of parents as the main instructors or applicators of the programmes, since the intervention in an EI centre is limited in time. But, at home and in a natural context they can promote all of these skills for a large amount of time and with variety, thus promoting the generalisation and maintenance of the gains that can be achieved up to schooling ages. However, we have also noted some shortcomings of these studies. On the one hand, the selection of participants who, logically, due to the practical characteristics of the population, are not all randomised, or they involve a “compulsory” allocation, given that children attending prevention and EI centres are eligible. This is also noted in the meta-analysis by French and Kennedy (2018). Added to this, is the use of very small samples in most of the studies, where only two studies have more than 100 participants. An added difficulty in comparing studies is the diversity of instruments for the assessment of the children’s skills. Although many screening tests, intelligence assessment tests, or developmental scales are used, there is a wide diversity of instruments. Moreover, these scales and questionnaires are usually answered by parents, i.e., few studies use direct observational tests that can give a direct indication of children’s behaviours. On the other hand, there is a wide diversity in the form and duration of EI programmes, ranging from short programmes like a couple of months to long-term programmes for two years. None of the studies include long-term follow-ups, at most after two or three months, so that there are no data on the preventive effectiveness of these EI on children’s later development when they are older. Similarly, some EI programmes are implemented directly by professionals or education systems, while in others the parents are involved, and home-based activities are also included. These facts make it even more difficult to make comparisons among different EI programmes. In conclusion, it is necessary to advocate for future studies that: (1) have a clear definition and description of the programmes, activities, and specific skills they develop; (2) use standardised instruments for the evaluation of efficacy that would also include direct observation; (3) make comparisons not only with control groups, but also with other EI programmes to study comparative effectiveness; and (4) carry out long-term evaluations to know exactly the effect of EI programmes after the age of six years, when children develop their most autonomous life, and at the schooling stage. Early intervention needs programmes that show their efficacy and, if possible, with an effect size greater than the one shown here, and also in the longer term. More homogeneous programmes need to be developed, with a better-defined form of intervention, with more rigorous procedures and techniques applied. We believe that the review and meta-analysis provided here contributes to a better understanding of the efficacy of EI, but with improvements in research and outcome studies, as described in this paper, future benefits may be even bigger. Conflict of Interest The authors of this article declare no conflict of interest. Cite this article as: Gómez Cotilla, R., López de Uralde Selva, M. A., & Valero Aguayo, L. (2024). Efficacy of early intervention programmes: Systematic review and meta-analysis. Psicología Educativa, 30(1), 1-10. https://doi.org/10.5093/psed2024a1 References References marked with an asterisk indicate studies included in the meta-analysis. |
Cite this article as: Gómez-Cotilla, R., López-de-Uralde-Selva, M. D. L. Á., & Valero-Aguayo, L. (2024). Efficacy of Early Intervention Programmes: Systematic Review and Meta-analysis. Psicolog├şa Educativa, 30(1), 1 - 10. https://doi.org/10.5093/psed2024a1
Correspondencia: lvalero@uma.es (L. Valero Aguayo).
Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Imprimir
Imprimir Enviar
Enviar
ALERTA POR E-MAIL
La Revista de Psicología Educativa está distribuida bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObra Derivada 4.0 Internacional.com








