


Cognitive Assessment of Very Preterm School-age Children by Chronological vs. Corrected Age
[La evaluación cognitiva de los niños muy prematuros en edad escolar según su edad cronológica en comparación con su edad corregida]
Yolanda Sánchez-Sandoval1, 2, Agustina Lambrisca1, 2, Isabel Benavente-Fernández1, 2, 3, Laura Lacalle1, 2, Melissa L. Martínez-Shaw1, and 2
1University of Cádiz, Spain; 2Biomedical Research and Innovation Institute of Cádiz (INiBICA), Spain; 3Puerta del Mar University Hospital, Cádiz, Spain
https://doi.org/10.5093/psed2025a4
Received 30 March 2024, Accepted 16 September 2024
Abstract
Children born preterm (≤ 37 weeks) are at higher risk of developing cognitive problems and score lower on cognitive developmental assessments than full-term children. The objective of the paper is to analyse the impact of correction for prematurity on IQ scores amongst preterm born children at school age. A sample of 153 Spanish school-age children were assessed using the WISC-V (Full Scale IQ and all indexes). Assessments were re-scored based on corrected age. Pairwise t-tests were used to analyse the difference in mean IQ scores between corrected age and uncorrected (chronological) age. WISC-V IQ scores <70, <85 and <90 were used to define the cognitive impairment level. Age-corrected scores were significantly higher than chronological age scores, except for processing speed. The percentage of children whose scores could be classified as cognitively impaired was not affected by the correction. When evaluating the cognitive skills in preterm children it should always be indicated whether or not prematurity correction was used, even at older ages, in order to avoid possible biases in the interpretation of the results.
Resumen
Los niños nacidos prematuramente (≤ 37 semanas) tienen un mayor riesgo de desarrollar problemas cognitivos y obtienen puntuaciones más bajas en la evaluación cognitiva que los nacidos a término. El objetivo del estudio ha sido analizar el efecto de la corrección por prematuridad en las puntuaciones de CI en niños nacidos prematuramente en edad escolar. Se evaluó a 153 niños españoles en edad escolar utilizando el WISC-V (CI a escala completa y todos los índices). La evaluación se volvió a puntuar en función de la edad corregida. Se utilizaron pruebas t para muestras relacionadas para analizar la diferencia en las puntuaciones medias de CI entre la edad corregida y la edad no corregida (cronológica). Se utilizaron puntuaciones del CI del WISC-V <70, <85 y <90 para definir el nivel de deterioro cognitivo. Las puntuaciones con edad corregida fueron significativamente mayores que las puntuaciones con edad cronológica, excepto para la velocidad de procesamiento. El porcentaje de niños cuyas puntuaciones podían clasificarse como extremadamente bajas no se vio afectado por la corrección. Es aconsejable, por tanto, cuando se evalúan las capacidades cognitivas, que se indique siempre si se ha utilizado o no la corrección por prematuridad, incluso a mayor edad, para evitar posibles sesgos en la interpretación de los resultados.
Palabras clave
Nacimiento prematuro, Prematuridad, EvaluaciĂłn cognitiva, Cociente Intelectual, CI, Edad corregida, Edad escolar, WISC-VKeywords
Preterm birth, Prematurity, Cognitive assessment, Intelligence quotient, IQ, Age correction, School age, WISC-VCite this article as: Sánchez-Sandoval, Y., Lambrisca, A., Benavente-Fernández, I., Lacalle, L., & Martínez-Shaw, M. L. (2025). Cognitive Assessment of Very Preterm School-age Children by Chronological vs. Corrected Age. PsicologĂa Educativa, 31(1), 29 - 36. https://doi.org/10.5093/psed2025a4
Correspondence: yolanda.sanchez@uca.es (Y. Sánchez-Sandoval).Preterm (PT) birth, i.e., that which occurs before 37 weeks of gestation, continues to be the main cause of mortality among children under 5 years of age (Perin et al., 2022), and represents approximately 10% of births worldwide (World Health Organization [WHO, 2022]). Despite the improvement of neonatal care in Neonatal Intensive Care Units (NICU), PT birth still poses an increased risk for adverse neurodevelopmental outcomes to these children, especially to children born very preterm (VPT; born < 32 weeks) (Marlow et al., 2021; Twilhaar et al., 2018). VPT children have been reported to have a higher rate of developmental difficulties (Palomo-Osuna et al., 2022). Children born preterm are more likely to suffer from developmental difficulties and disorders, mostly in the presence of added risk factors, such as brain lesions, neonatal sepsis, retinopathy, small for gestational age, multiple pregnancies, and mothers younger than 25 years with low income (García-Martínez et al., 2018; McKinnon & Huertas-Ceballos, 2019). Early school-age disorders (e.g., mild cognitive impairments and behavioural problems) can be developed even by low-risk preterm children (Fan et al., 2013). For the study of cognitive difficulties, researchers usually employ general intellectual functioning as a measure, specifically the Intelligent Quotient (IQ), since it provides a broad measurement of cognitive functioning. Regarding cognitive development, recent systematic reviews and meta-analyses continue to show that PT children get lower cognitive scores than full-term children (≥ 38 weeks) (Lacalle et al., 2023; Sentenac et al., 2020). In the meta-analysis of Brydges et al. (2018), VPT children scored 0.82 SDs lower on intelligence tests, 0.51 SDs lower on measures of executive functioning, and 0.49 SDs lower on processing speed than term-born controls. These deficiencies could be due to an incomplete prenatal neural development, which causes generalised alterations in the frontoparietal network. The integrity of this network is linked to optimal executive function, processing speed, and intelligence (Aylward, 2014; Si et al., 2021). Other studies corroborate these brain vulnerabilities in PT children, specifically in the subgroup of VPT children (Thompson, 2019). In some cases, the mean differences are not big, and some studies report that PT children obtained scores predominantly in the normative range (García-Martínez et al., 2018; Nagy et al., 2019; Nobre et al., 2020). The normative range is generally considered to be a score between 85 and 115 points in IQ, which is no more than 1 SD above or below the normative mean (100). A severe cognitive impairment is defined by the World Health Organization as having an IQ below 70, a mild cognitive impairment is defined as having a score below 85 and requiring special assistance, and an IQ higher than 90 is not considered to be a previous requirement for further follow-up, support, or intervention (Wechsler, 2014). In any case, these studies do not usually consider the impact of age correction on the evaluations conducted. From the 1930s, researchers started to correct the age for prematurity in the first years of life (Mohr & Bartelme, 1930), and it continues to be recommended nowadays in the clinical guidelines (Kallioinen et al., 2017). To calculate the corrected age, the number of weeks and days that the child was born prematurely is subtracted from the chronological age, understanding that full-term pregnancy is 40 weeks of gestation (Committee on Fetus and Newborn, 2004). While the American Academy of Pediatrics (AAP) recommends that corrected age is usually used in assessments up to the first two or three years of life, in practice there is no clear consensus as to when and under what circumstances correction should cease (Bernbaum et al., 2008; Engle, 2006; Wilson & Cradock, 2004). Van Veen et al. (2016) suggest that studies should always report whether or not age correction for prematurity was used, since they may lead to different results and/or conclusions. A longitudinal study (Harel-Gadassi et al., 2018) showed that corrected age scores were significantly higher than chronological scores on measures of developmental functioning at all ages during the first 3 years of life. According to the analyses of Wilson-Ching et al., (2014), after 3 years of age, the differences between the corrected and chronological scores may still be important from the clinical perspective. Furthermore, it is highlighted that age correction can eliminate an important bias for premature children in research approach. Research on the use of corrected-age or chronological-age cognitive scores shows that children up to 36 months of age have significantly higher corrected-age scores than chronological-age scores, using the Bayley scales (Morsan et al., 2018; Parekh et al., 2016; Wilson-Ching et al., 2014). Corrected IQ points were also significantly higher than chronological IQ points in studies with PT children assessed at 5 years (Van Veen et al., 2016), as well as in school-age children using a version of WISC (Roberts et al., 2013; Wilson-Ching et al., 2014). The variables associated with these differences, as well as their magnitude, have not been thoroughly analysed by previous studies beyond pointing out their relationship with gestational age. While some authors have found that the difference is greater at younger gestational ages and lower weights (Van Veen et al., 2016), others have reported no differences in this sense (Harel et al., 2018). Exceptionally, a longitudinal study indicates that the differences found during the first two years of life persisted at the age of 7 years, although the magnitude of the differences was small in the second evaluation (Gould, et al. 2021). Doyle and Anderson (2016) stated that at the clinical level,a greater difference between corrected age and chronological age would put the child at greater disadvantage during the first years of life; at the age of 12 years, they still observed differences of up to a third of a standard deviation in IQ when the age was corrected for children born 4 months before term. Additionally, the scores in IQ have been used to determine the existence of low functioning or cognitive impairment. Several studies have noted that school-age PT children have a significantly higher proportion of impaired FSIQ scores than full-term infants (Kim et al., 2021; Rozé et al., 2021). At school age, studies with PT children do not tend to carry out corrections for prematurity, thus it is not entirely possible to know whether these differences would persist after such correction. On the other hand, it is worth highlighting the work of Roberts et al. (2013), who showed that when children’s age was corrected there were no significant differences in the proportion of children whose FSIQ scores fell within the category of cognitive impairment. Consequently, the objective of this study is to analyse the impact of age correction on IQ scores in school-age children. As a novelty, this study explored not only the FSIQ scores, but also the different dimensions analysed with WISC-V. We expected to observe differences between these two scores, with those standardised with corrected age being higher. We also hypothesised that this difference is greater at younger gestational ages; for instance, the differences in the scores were expected to be greater in the children born before 28 weeks than those born after 28 weeks. The secondary aim of the current study is to compare the proportions of children identified with lower cognitive functioning or impairment from the scores of WISC-V with chronological and corrected age. It was expected that fewer children would be identified with cognitive impairment after correcting their age. Participants This cohort was selected from the prospective PRETERM study conducted at Puerta del Mar University Hospital for the follow-up of PT children’s development. The inclusion criteria were: to be born between January 2011 and December 2014; to be born at 32 weeks and/or fewer or with a birth weight equal to or lower than 1500 grams; and being admitted to the NICU in Puerta del Mar Hospital (Cadiz, Spain). The present study involved 153 school-age PT children. The data were collected between July 2020 and March 2023 at approximately eight years of the participating children’s chronological age (all children were between 6 years and 2 months old and 11 years and 1 month old at the time of the assessment; M = 8.65, SD = 0.95). The exclusion criteria were no genetic disease or major congenital anomaly. Moreover, children were excluded from the study if their clinical profile precluded valid performance in the administration of the test (e.g., due to severe cognitive, visual or hearing impairment). Figure 1 presents the flowchart of the participant selection. Figure 1 Flowchart of the Participant Selection. 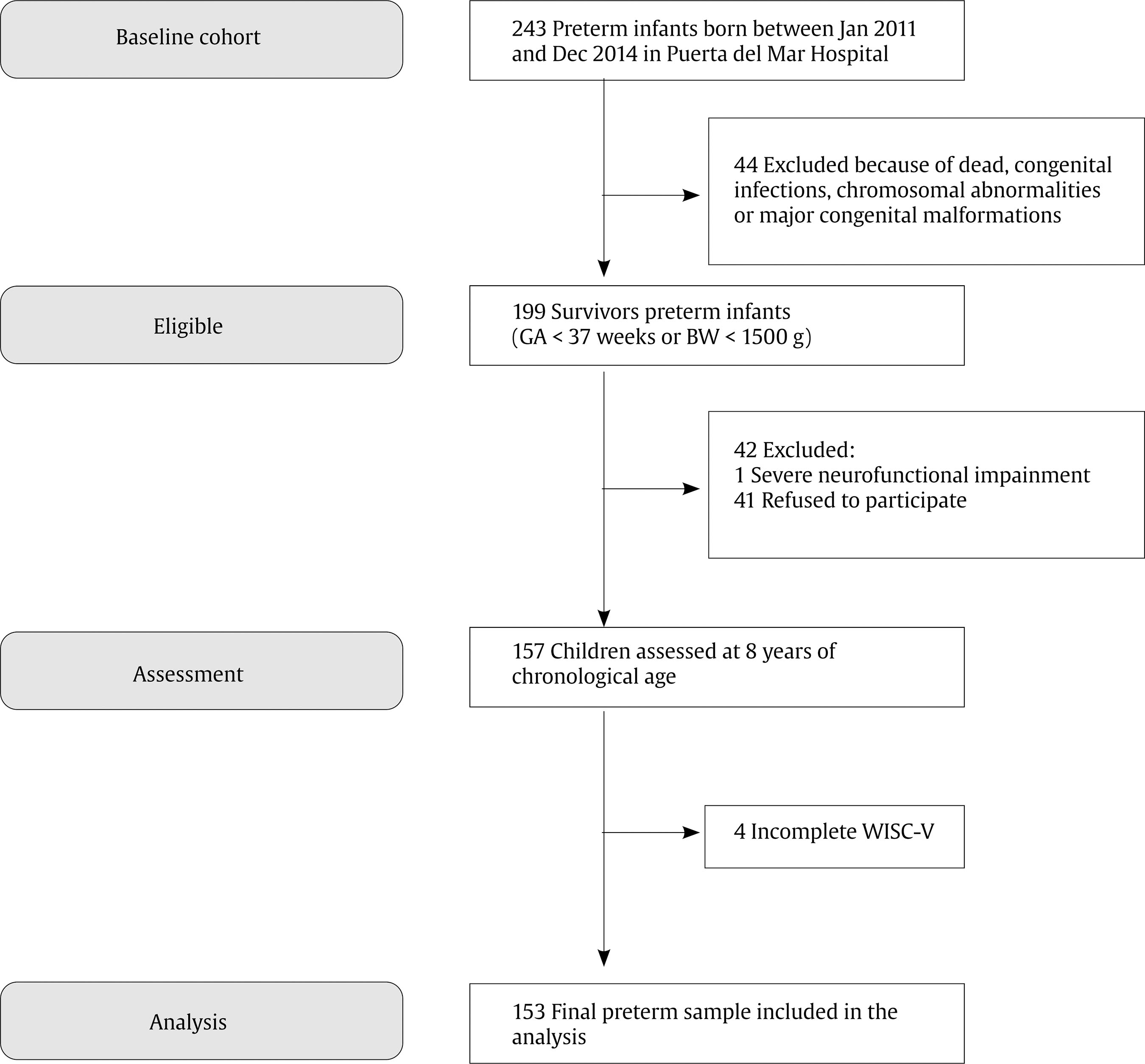 After comparing the characteristics of the included and excluded participants, the PT children who participated in the study had a significantly lower gestational age and weight than those who did not agree to participate: gestational age, t(97.3) = 2.58, p < .01, d = 0.19; birth weight, t(197) = 2.07, p < .05, d = 0.17. No significant differences were observed between the sex ratios of participants and non-participants. The characteristics of the participants are summarised in Table 1. Table 1 Neonatal and Demographic Characteristics of the Sample 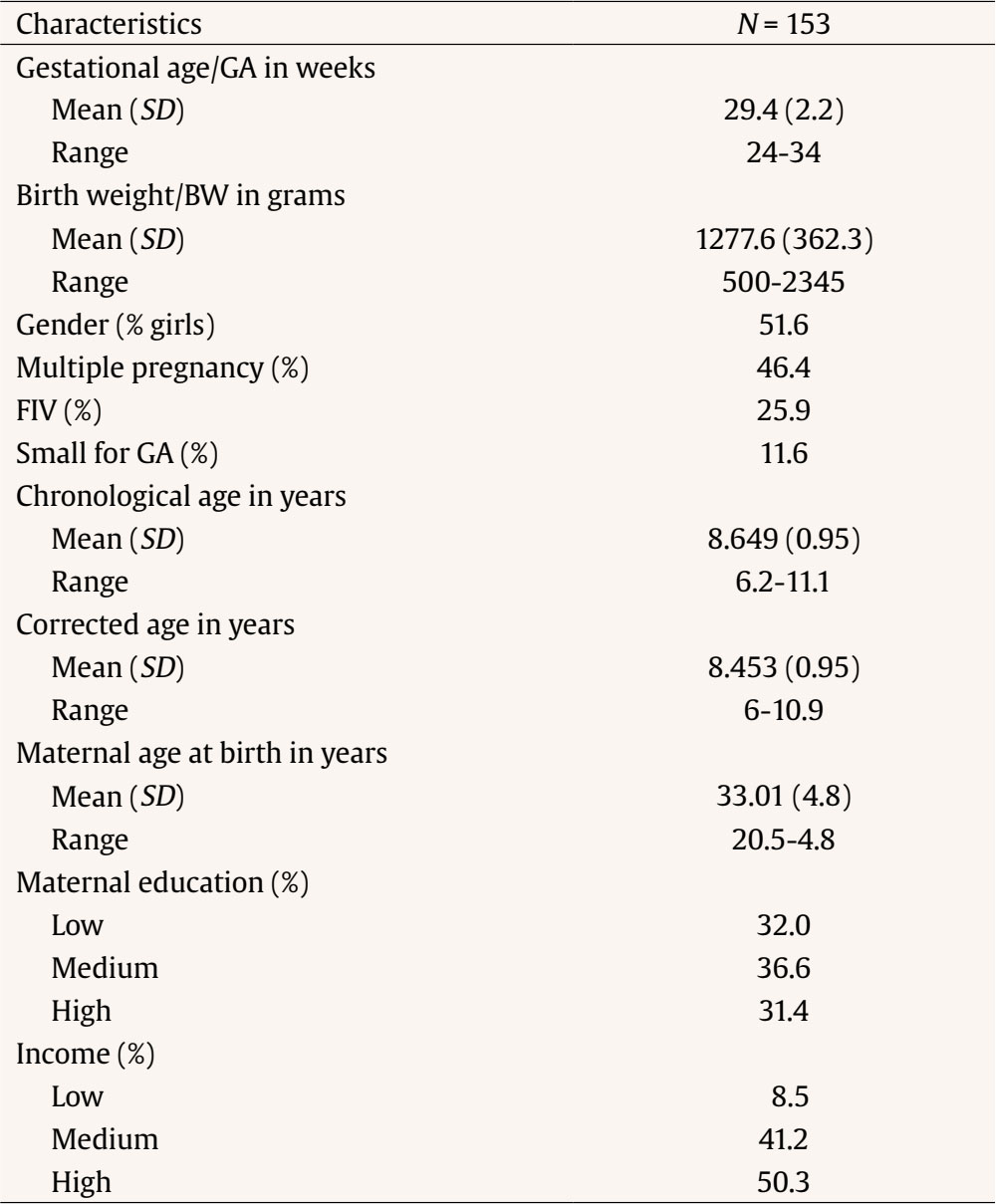 Measures Gestational and perinatal data were derived from the hospital’s medical records, and demographic characteristics (such as family income and maternal education) were obtained through an ad hoc interview with the parents. Intellectual functioning was measured using Weschler’s Scale of Intelligence for Children-Fifth Edition (WISC-V) (Wechsler, 2014). The Spanish version of WISC-V is a reliable and valid test to evaluate intellectual performance in Spanish children between 6 and 16 years of age (Fenollar-Cortés & Watkins, 2019). Through the individual administration of ten core subtests, it provides the Full-Scale Intelligence Quotient (FSIQ) and five indexes: Verbal Comprehension Index (VCI), Spatial Visual Index (SVI), Perceptual Reasoning Index (PRI), Working Memory Index (WMI), and Processing Speed Index (PSI). Scores are also obtained on secondary indexes that reflect cognitive skills in different groupings, which address clinical needs such as Nonverbal Index (NVI), General Ability Index (GAI), and Cognitive Competence Index (CCI). WISC-V has age-standardised scores (mean of 100, SD of 15). Procedure The study was approved by the regional Research and Bioethics Committee. Written informed consent was signed by the parents or legal guardians of each participant, and they were interviewed. Assessments were conducted by trained psychologist examiners. PT children’s raw scores were age-standardised by chronological age, according to the children’s chronological age at the time of the assessment. Subsequently, raw scores were re-standardised for prematurity (number of weeks that the child was preterm subtracted from the chronological age). Children who were born more than 3 months and 30 days early fall into different age groups rationally based on their chronological and corrected ages. Chronological and corrected ages of children born less than 3 months prematurely would only fall into the same age group if the corrected and chronological age-at-assessment are close to the start point and end point of that age group, respectively. WISC-V scores differences were calculated for each child by subtracting the score based on the chronological age from the score based on the corrected age. The proportions of children with a score < 70, < 85, and < 90 were calculated, based on corrected and chronological scores. Subsequently, to analyse whether differences differ across the age assessment, the sample was divided into 3 chronological age groups (< 8, 8, and > 8 years). Statistical Analyses Data analysis was performed using IBM SPSS Statistics (version 24). Prior to performing each statistical test, the necessary assumptions were checked in each case. Independent two-sample t-tests were performed to assess sex differences in some variables, including gestational age, age-at-assessment, birth weight, and FSIQ. Pairwise t-tests were used to contrast the theoretical WISC-V scores (both Full Scale IQ and indexes) with chronological age scores. Then, pairwise t-tests were used to compare chronological and corrected scores for WISC-V (Full Scale IQ and indexes). Bonferroni corrections were used. Cohen’s d values were used to assess the effect sizes (Cohen, 1988), considering it negligible if < 0.10, small between > 0.10 and < 0.30, medium between > 0.30 and < 0.50, and large if > 0.50. Also provided is the Cohen coefficient U3, or non-overlap measure, which compares the percentage of a population that exceeds the upper half of the cases, with a contrast (comparator) group. The value ranges from .50 or 50 % to 1.0 or 100 %. The effect is important if it is greater than .70 or 70 % and is much better if it is greater than 90% (Ventura-León, 2018). Simple correlations (Pearson or Spearman correlations as appropriate) were conducted to examine the associations between gestational age, birth weight, age-at-assessment and all WISC-V indexes, as well as their differences. Additionally, using independent t-tests, children born before and after 28 weeks of gestation were compared. Subsequently, McNemar tests were performed to compare the number of children with developmental delays when corrected age and chronological age, according to the previously mentioned WISC-V classification (IQ < 70, IQ < 85, and IQ < 90). The profile of each subject according to the dimensions of the WISC-V was analysed. We calculated a variable that measures stability, and a McNemar test (with Yates correction) was used to determine whether such stability differed between chronological age and corrected age. Lastly, after the sample was divided into 3 age groups, pairwise t-tests were conducted to analyse differences of chronological and corrected IQ scores between age groups. The differences were also tested using ANOVA. Statistical significance was set at p < .05 (2-tailed). According to a power analysis, our sample size (N = 153) had more than 80% power to identify associations and group differences with small-to-moderate effect sizes at a significance level of α = .05 (Cohen, 1992). As is indicated in Table 2, there were no significant sex differences in gestational age, age-at-assessment, chronological age IQ and corrected age IQ. There were differences only in birth weight, with girls having the lowest birth weight, with a small effect size (d = 0.25; 59.9% of the boys had a birth weight above the mean weight of the girls). There were no significant differences between the three groups in age-at-assesment, gestational age, sex, chronological age IQ, and corrected age IQ, but a significant difference was observed in birth weight, F(2, 150) = 5.063, p < .01, with the group of 8 years obtaining the greatest weight. Figure 2 Comparisons Chronological and Corrected WISC Scores. 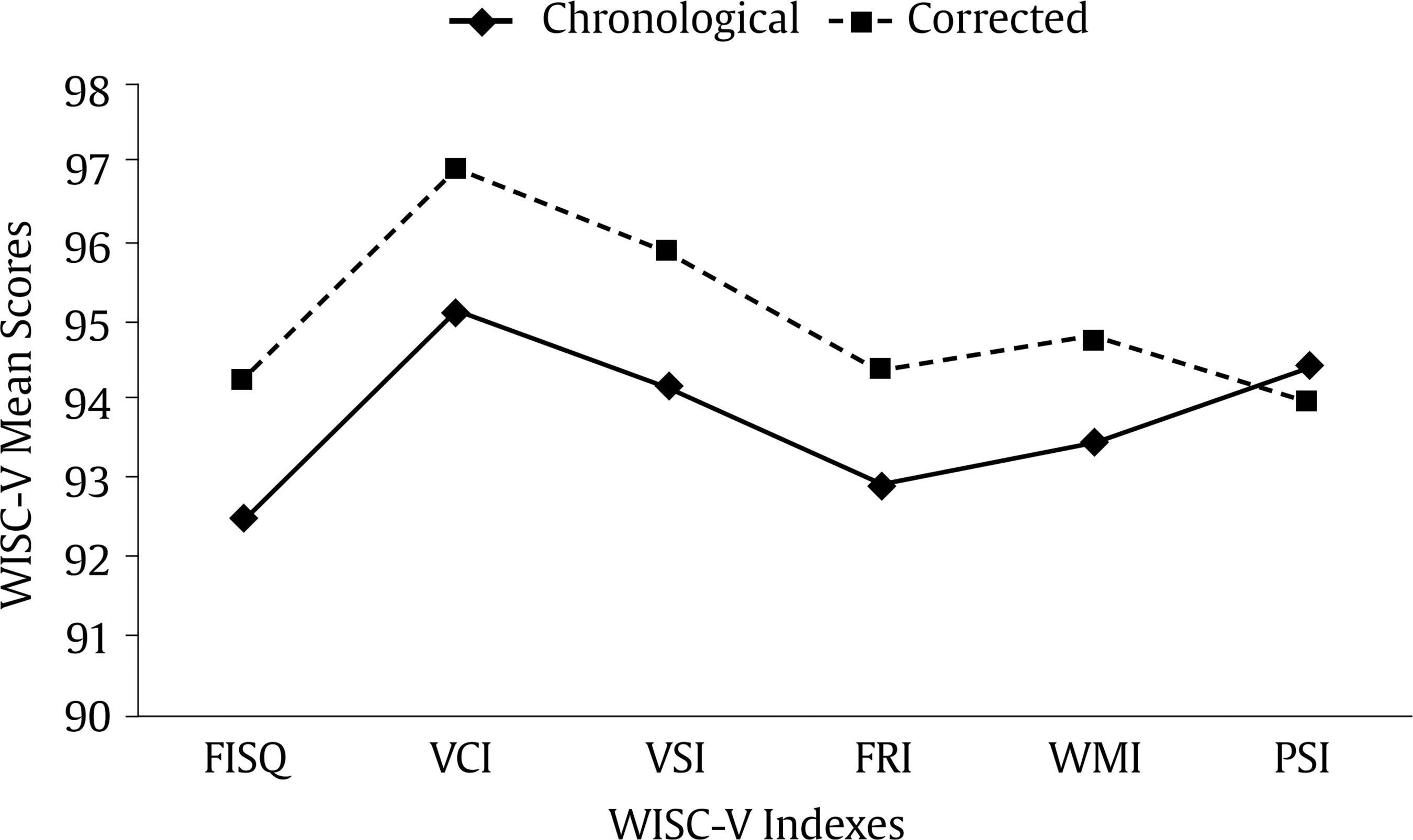 Note. Full Scale IQ (FSIQ), Verbal Comprehension Index (VCI), Visual Spatial Index (VSI), Fluid Reasoning Index (FRI), Working Memory Index (WMI), and the Processing Speed Index (PSI). Table 2 Means (and Standard Deviations) for Differences by Sex  *p < .05. After comparing the uncorrected mean FSIQ scores with the theoretical mean of 100, the scores of the PTs were significantly lower, as well as all dimensions, with a small effect size (Table 3). In the case of the corrected scores, the comparison with the theoretical mean of 100 also indicates that the scores of the PT group were lower, with a small effect size (d < 0.20). As shown, the U3 of the comparisons range between 50.4% and 59.9%, showing a high overlap of the curves of the variables compared, and thus a small effect size. In the comparison of WISC-V scores obtained using chronological age versus using corrected age, all corrected age-based scores were higher than those based on chronological age, and the differences were statistically significant, with a small effect size (Table 3, illustrated in Figure 2). However, in the case of PSI, non-significant differences were found between chronological-age and corrected-age score. Table 3 Comparison of WISC-V Scores with Chronological Age and Corrected Age 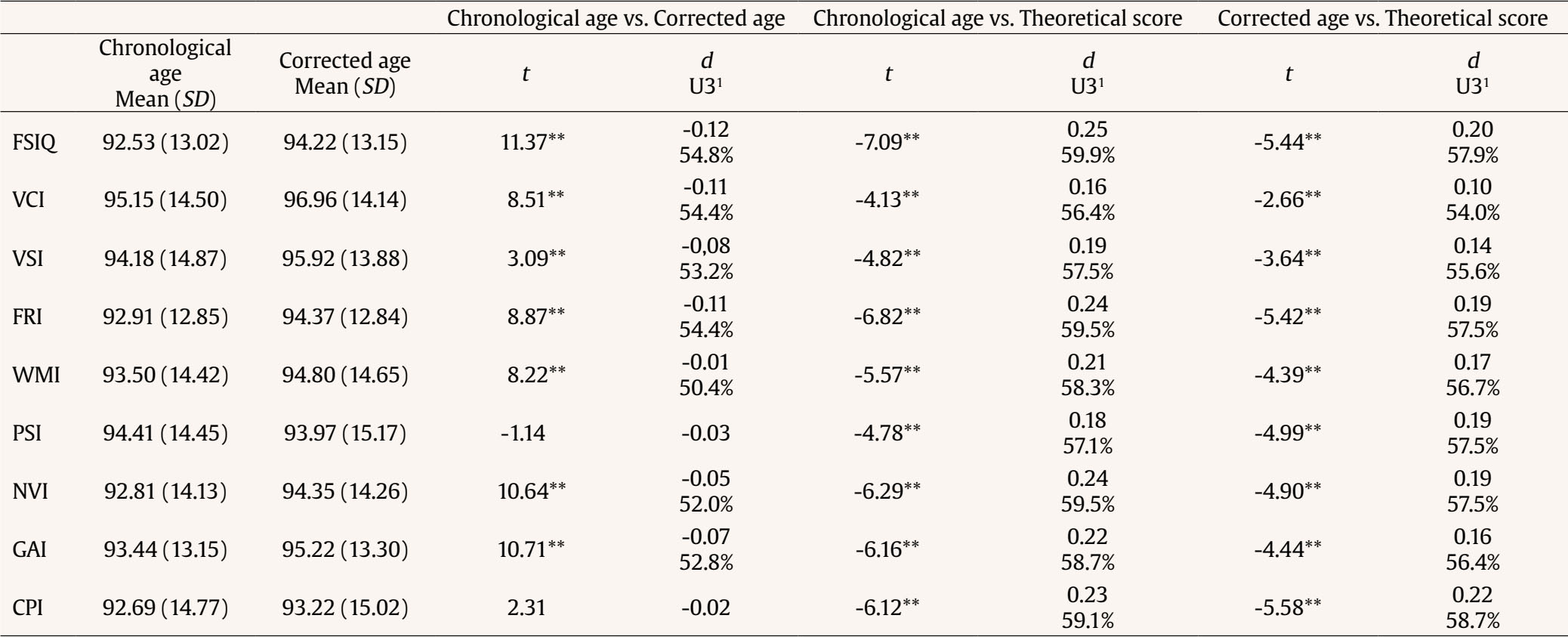 Note. Bonferroni corrections; 1U3: percentage of the group’s scores that are above the mean of the other group’s scores; Full Scale IQ (FSIQ), Verbal Comprehension Index (VCI), Visual Spatial Index (VSI), Fluid Reasoning Index (FRI), Working Memory Index (WMI), Processing Speed Index (PSI), Nonverbal Index (NVI), General Ability Index (GAI), and Cognitive Proficiency Index (CPI). **p < .01. As is shown in Table 4, there were no significant correlations between gestational age and chronological FIS or any of the WISC-V chronological indexes. Greater differences between corrected-age and chronological-age scores were significantly correlated with lower gestational age. Children in the lowest gestational age group (< 28 weeks) had a greater difference between chronological and corrected FSIQ scores in comparison to children in the oldest gestational age group (> 28 weeks), and this discrepancy was statistically significant, t(151) = 5.03, p = .015. Regarding differences in the WISC-V indices, negative correlations with gestational age were found for VCI, VSI, FRI, NVI, and GAI. The correlations with the rest of the indexes were not significant. Furthermore, there was a significant correlation between BW and FSIQ, showing that the greater the birth weight, the higher the FISQ score, while the correlation between birth weight and all WISC-V indexes was also significant, except for FRI and WMI. Furthermore, birth weight was significantly correlated with differences between chronological and corrected scores in FRI, NVI and GAI. Table 4 Correlations between Neonatal Characteristics, WISC-V Chronological Scores and WISC-V Differences Scores 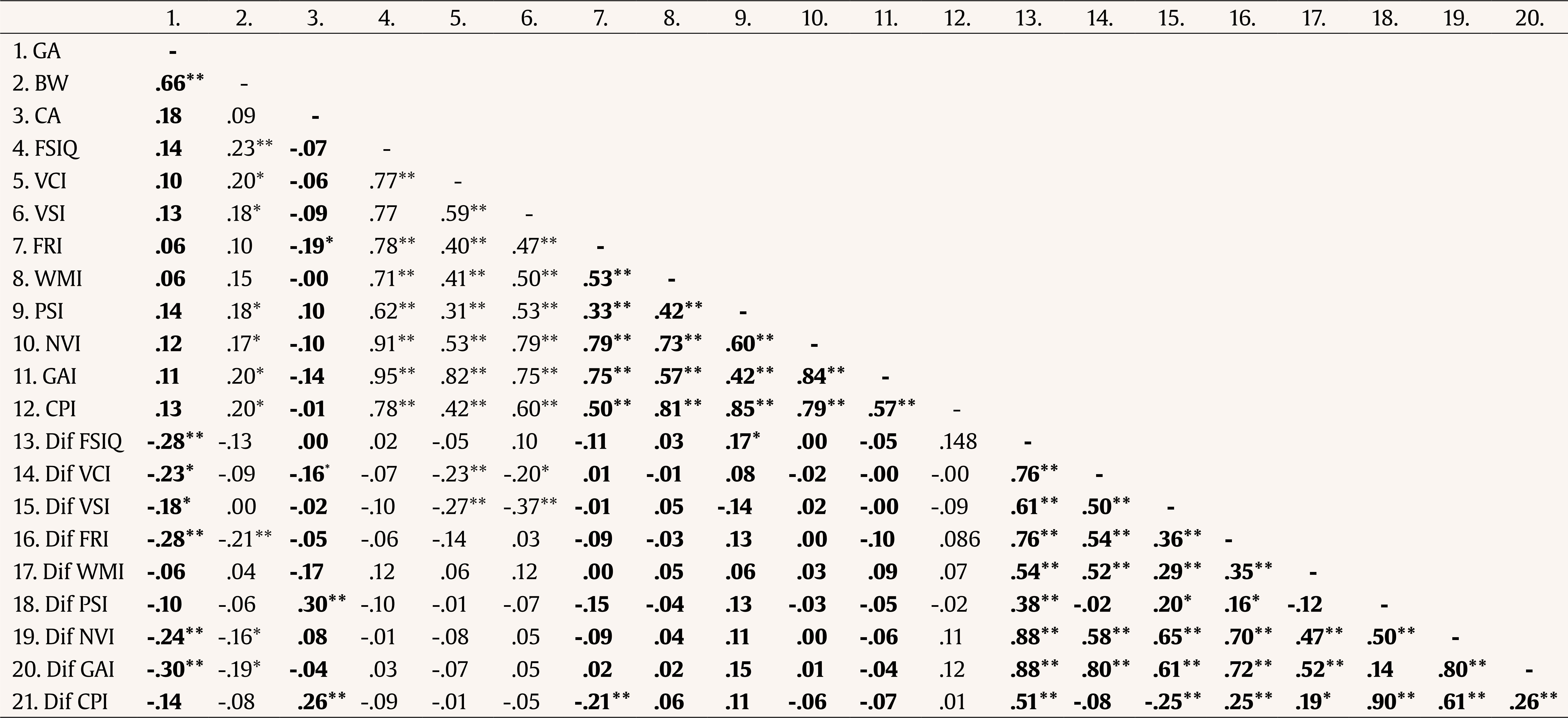 Note. Spearman p in italic type, Pearson r in normal type. Gestational Age (GA), Birth Weight (BW), Chronological Age (CA), Full Scale IQ (FSIQ), Verbal Comprehension Index (VCI), Visual Spatial Index (VSI), Fluid Reasoning Index (FRI), Working Memory Index (WMI), and the Processing Speed Index (PSI), Nonverbal Index (NVI); General Ability Index (GAI); and the Cognitive Proficiency Index (CPI). Dif = Differences between WISC-V chronological scores and WISC-V differences scores. *p < .05, **p < .01. Using chronological scoring, a total of 3.3% of FISQ scores fell within the range of severe cognitive impairment (2 SD below average, IQ < 70), as opposed to 2.6% when corrected scores were used. This proportional difference was not, however, statistically significant, according to the McNemar test. Similarly, higher proportions of children with moderate cognitive impairment (1 SD below average, IQ < 85) were found with chronological scores than with corrected scores (28.9% vs. 25.7%, respectively), although the differences in proportions were not statistically significant (p = .063). When FISQ scores were uncorrected, 42.1% of the children were below the average range of intelligence (IQ < 90), whereas this proportion was statistically significantly reduced to 34.2% (p < .001) when the scores were corrected. When analysing the profile of each child according to the different primary dimensions of the WISC-V, it is possible to identify the strengths and weaknesses of each child or whether he/she has a stable profile. A total of 21.1% of our sample presented a stable profile in chronological age, with no strong or weak points in any of the dimensions. When corrected for age, this stability occurred in 19.6% of the sample, although this difference was not statistically significant (p = .648). Kruskal Wallis test showed no significant differences between the age groups regarding the difference in the chronological and corrected FSIQ scores, χ²(2, 150) = 1.478, p = .478. When compared in each of the three groups based on age-at-assessment, the pairwise t-test showed that the corrected FISQ scores were significantly higher than the chronological FSIQ scores: less than 8 years, t(29) = -3.607, p < .001, at 8 years, t(67) = -8.137, p < .001, and more than 8 years, t(54) = -7.959, p < .001. In addition, with regard to the correlations, the differences between corrected and chronological FSIQ scores at all age groups increases with decreasing gestational age (r = -.41, r = -.26, r = -.36, respectively; all p values < .05). Greater birth weight was associated with higher FISQ scores, for both chronological and corrected age, at 8 years (r = .29, N = 68, p < .05), but not at less or more than 8 years (p > .05). The aim of this study was to provide empirical evidence of the effect of correction for prematurity in IQ assessments in premature children. As in previous studies on cognitive function using correction of age-standardised scores (Roberts et al., 2013; Wilson-Ching et al., 2014), our sample showed significant differences between the scores in chronological and corrected WISC-V in premature school-age children. IQ calculated with age corrected for prematurity was significantly higher than that calculated with chronological age. The difference was 1.69 points between the mean score of chronological age and the mean score of corrected age (92.53 vs. 94.22, respectively). Specifically, in the study by Gould et al. (2021) it was reported that at 7 years of age the difference in scores was 1.9 points between the mean chronological and corrected age scores (97.2 vs. 99.1, respectively). The significant differences were obtained not only from the comparisons of FSIQ, but also in all the comparisons performed in the rest of the indexes. In PSI, in contrast with the rest of the indexes, a higher mean score was obtained with chronological age than with corrected age. This could be due to the fact that specifically in this dimensions in some of the age groups the scales of the Spanish version of WISC show higher scores at younger ages (Wechsler, 2015). In turn, the results of the current study corroborate that PT children show significantly lower scores compared to the theoretical average of WISC at school age, which is in line with the results of Arreguín-González et al. (2017). Moreover, this score below the normative average remained lower when the age was corrected for prematurity. To date, no studies have conducted similar analyses; however, studies with comparison groups also show that PT children usually present a lower IQ than full-term children when the age is corrected (Morsan et al., 2018). With regard to the children who fell within the range of cognitive impairment (IQ < 70), our results are in agreement with those of Roberts et al. (2013), that is, at age 8 years the dissimilarity in the proportions of children with intellectual difficulties using corrected and chronological measures was not statistically significant. Nevertheless, when the cut-off point was set in more average scores (Roberts et al., 2013), it is worth mentioning that when scores were corrected the proportion of children below the average range of intelligence (IQ < 90) was statistically significantly lower. Gould et al. (2021) report similar results. With chronological age 31% of the PT children were classified as susceptible to presenting learning difficulties, and after age correction 22.1% no longer presented such risk, with a significant difference evaluated with Weschler’s Abbreviated Scale of Intelligence 2nd-Edition. Therefore, our results suggest that age correction in not required to define severe cognitive impairment and for indicating the need for special education at a clinical level, although it does better adjust the actual score within normal ranges. There are mixed recommendations on the age at which age correction should be discontinued in school-age and older children. On the one hand, it is usually advised to conduct a complete correction of age, at least in the first years of life due to the rapid development, in order to prevent an overdiagnosis of developmental delay (Kallioinen et al., 2017). On the other hand, age correction is advised against based on the fact that development quotients may be inadequately high, that is, they could be corrected in excess; thus, possible developmental delays could be ignored, thereby losing the right to receiving funding and services that respond to the real needs. In the clinical practice, when correcting the age of the children, it is important to consider the risk of misinterpreting the skills in this sense. In turn, in research, correcting the age of the children may remove an important bias regarding the skills of PT children, especially when the sample is constituted by both PT and full-term children. Based on the results of the current study, although the average differences in the WISC-V scores are significant, they have a small effect size, which indicates that these are discrete differences, suggesting that the correction was not excessive. In fact, Cohen’s tests of effect size indicate that the distribution of scores calculated with chronological age and those calculated with corrected age overlap in more than 95% of the cases. Furthermore, in the present study, the score could only be corrected in 56.21% of the sample. The main difficulty for the correction for prematurity that we encountered was the magnitude of the age groups for the correction of WISC-V, i.e., 4 months (e.g., the same scale to correct the scores ranged from 8 years and 0 days to 8 years, 3 months and 30 days). In our case, the other 43.79% of the children, once their age was corrected, remained in the same age group. Therefore, only the children whose adjusted age was 4 months lower than the chronological age would surely be in a lower group, or those whose chronological age (e.g., 8 years and 15 days) were near the beginning of the age group. Age-grouping in child neurodevelopmental assessment has previously been subject to a thorough analysis and discussion (Veldhuizen et al., 2015). Thus, our findings would support the hypothesis which states that the greatest differences in the correction occur in lower gestational ages, since the temporal distance to a gestational age of 40 weeks is greater and also due to the problem of the width of the age groups in calculating norm scores. This difficulty would be overcome if, as suggested by (Van Veen et al., 2016), we had scales that, using the ongoing norm procedure, calculate day-by-day norm scores online. We support this demand for current cognitive test publishers to incorporate this possibility, or at least narrower age groups (e.g., 15 days or 1 month, instead of 3 or 4 months), which would allow performing more rigorous corrections. As was observed, although chronological FISQ was correlated with birth weight, this was not a strong relationship. The discrepancy between the chronological and corrected IQ scores was not related to birth weight. This result was expected, because the birth weight did not have an effect on the amount of correction that established the differences between scores. These results are in agreement with those of Roberts et al. (2013), who found no association between differences in IQ scores and birth weight in the WISC-IV sample. Regarding the association with gestational age, the relationship between differences in IQ scores and gestational age was weaker. Moreover, we found differences between the children born before and after 28 weeks, showing that the more preterm a child is, the more imperative it is to take prematurity into account, due to the larger difference between chronological and corrected scores, which is in line with the findings of Wehrle et al. (2021). With respect to the association between the effects of correction and age-at-assessment, no relationship was found between age-at-assessment and the differences in corrected and chronological IQ scores. Similarly, there were no statistically significant differences between the age groups as a function of the discrepancy in IQ scores; specifically, corrected FISQ scores were significantly higher than the chronological FISQ scores for the three age groups. On the contrary, in Wilson-Ching et al. (2014) the effects of age correction were stronger at younger ages on age-at-assessment, with a considerable fluctuation in the different ages of the school stage. In children older than 10 years these authors found the lowest difference between chronological and corrected scores. Our findings suggest that, although the differences between chronological and corrected IQ scores were statistically significant, they were low at school age. This finding may be understood as supportive of the ‘catch up theory’, as showed in the study of Ment et al. (2003), who concluded that the cognitive skills of PT children improve progressively with age, and thus correction is not as necessary. This could be partly due to the fact that cortical growth and maturation are also favoured by the increase of the demand for higher-order cognitive skills during this stage of life (Wilson-Ching et al., 2014). In fact, Marlow (2004) stated that age adjustments after 3 years old do not affect scores notably, and thus using corrected scores at these ages is not relevant. This study has some limitations that should be pointed out. Firstly, some children who were included had a range of perinatal disorders, such as attention deficit disorder, sepsis, intraventricular hemorrhage, and bronchopulmonary dysplasia. It is unclear whether the demonstrated lower cognitive performance could be linked to preterm birth or comorbidities, so these circumstances may have affected the results. It would be interesting for future studies to analyse the results considering the possible medical risk in the neonatal stage, and even the possible psychosocial risk as has already been done in other recent research (Jiménez-Luque et al., 2023; Sánchez-Joya et al., 2017; Sánchez-Sandoval & Verdugo, 2021; Yaari et al., 2019). Recognising these limitations, we think that this study can help to highlight the effect of age correction on cognitive scores in school-age children. It is also worth emphasizing the importance of the decision of whether or not to correct the age for prematurity, depending on the purpose of the cognitive evaluation of the PT child. Moreover, the mean scores for the preterm group may be biased, since meta-analysis indicate on average a 12 point IQ-difference to full term born but in this study is only 7.5 points. This may be due to the bias introduced by not having a full term control group. Previous research has shown that norms for IQ-tests outdate quickly due to the Flynn effect (younger generations improve in General IQ usually) and thus over-estimate the IQ of very preterm born (Trahan et al., 2014). Although the present study was not designed to this end, a longitudinal approach would be essential to monitor the results of neurodevelopment after a very premature birth. The broad inclusion criteria to be included in this study enable the generalisation of the results to other countries with similar healthcare systems. To conclude, although the literature insists on the importance of using corrected scores especially in the first years of life, as well as at very early gestational ages, our paper shows that, even at school age, it provides a slightly more realistic and positive view of the cognitive capabilities of these children. However, the correction would not affect the diagnosis of severe impairments. In any case, as in the study by Bogievi et al. (2019), it is suggested that research that evaluates cognitive function should always indicate whether or not they used correction for prematurity, even if they did so at older ages, in order to prevent possible biases in the interpretation of the results. Conflict of Interest The authors of this article declare no conflict of interest. Cite this article as: Sánchez-Sandoval, Y., Benavente-Fernández, A. I., Lacalle, L., Martínez-Shaw, M. L. (2025). Cognitive assessment of very preterm school-age children by chronological vs. corrected age. Psicología Educativa, 31(1), 29-36. https://doi.org/10.5093/psed2025a4 Funding This study was supported the Department of Economic Transformation, Industry, Knowledge, and Universities. Andalusian Regional Government. Project co-funded by 80% by the European Union, within the framework of the ERDF Andalusia 2014-2020 Operational Program; grant number P20-00915, and by the Department of Health and Families, Andalusian Regional Government, 2020; grant number PI-0016-2020. The data that support the findings of this study are available on request from the corresponding author. References |
Cite this article as: Sánchez-Sandoval, Y., Lambrisca, A., Benavente-Fernández, I., Lacalle, L., & Martínez-Shaw, M. L. (2025). Cognitive Assessment of Very Preterm School-age Children by Chronological vs. Corrected Age. PsicologĂa Educativa, 31(1), 29 - 36. https://doi.org/10.5093/psed2025a4
Correspondence: yolanda.sanchez@uca.es (Y. Sánchez-Sandoval).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Imprimir
Imprimir Enviar
Enviar
ALERTA POR E-MAIL
La Revista de Psicología Educativa está distribuida bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObra Derivada 4.0 Internacional.com








