


Long-Term Effectiveness of a Mindfulness Based Intervention (MBI) Program for Stuttering: A Case Study
[La eficacia a largo plazo de un programa de intervenciĂłn basada en la atenciĂłn plena (MBI) para la tartamudez: un estudio de caso]
Jennifer E. Moreno-Jiménez1, Raquel Rodríguez-Carvajal1, Carlos Garcia-Rubio1, Ruth Castillo-Gualda2, and Ignacio Montero1
1Universidad Autónoma de Madrid, Spain; 2Universidad Camilo José Cela, Madrid, Spain
https://doi.org/10.5093/clysa2021a1
Received 19 June 2020, Accepted 14 September 2020
Abstract
A mindfulness-based intervention (MBI) to address emotional factors that may negatively impact the fluency of the subjects was implemented. A MBI consisting of 5 weekly 2-h sessions was designed and applied to two stuttering cases. The goals were to lower stuttering and to reduce anxiety through the acquisition of mindfulness skills. Participants were asked to video-record a speaking task and to fill out anxiety and mindfulness skills self-reports pre and post-intervention. Both participants diminished stuttering error rates from severe (participant 1) and moderate (participant 2) to mild. Participant 2, who showed high pre-treatment anxiety, showed a significant reduction. A year-follow-up revealed that therapeutic gains in anxiety, mindfulness skills, and stuttering were successfully maintained in both participants. This is the first study focused on emotional aspects of stuttering showing long-term improvements through a MBI. MBI programs could serve as a promising complement for stuttering treatments.
Resumen
Se utilizó una intervención basada en mindfulness (MBI) para abordar los factores emocionales que pueden afectar negativamente a la fluidez de los sujetos a través de un estudio de caso. Se diseñó un MBI que constaba de 5 sesiones semanales de 2 horas y se aplicó a dos casos de tartamudez. Los objetivos eran dismunuir la tartamudez y reducir los síntomas de ansiedad mediante la adquisición de habilidades de atención plena. Se pidió a los participantes que grabaran en video una tarea oral y que cumplimentaran los autoinformes de ansiedad y de habilidades de atención plena antes y después de la intervención. En ambos participantes disminuyó el índice de errores de tartamudeo de grave (participante 1) y moderado (participante 2) a leve. El participante 2, que mostró una elevada ansiedad previa al tratamiento, mostró una reducción significativa. Al año de seguimiento los beneficios terapéuticos en ansiedad, habilidades de atención plena y tartamudeo se mantuvieron con éxito en ambos participantes. Se trata del primer estudio centrado en los aspectos emocionales de la tartamudez que muestra mejoras a largo plazo a través de un MBI. Por lo tanto, los programas MBI podrían servir como complemento prometedor a los tratamientos de tartamudez.
Palabras clave
Tartamudez, AtenciĂłn plena, IntervenciĂłn basada en la atenciĂłn plena, Eficacia a largo plazo, Estudio de casoKeywords
Stuttering, Mindfulness, Mindfulness-based intervention, Long-term effectiveness, Case studyCite this article as: Moreno-Jiménez, J. E., Rodríguez-Carvajal, R., Garcia-Rubio, C., Castillo-Gualda, R., and Montero, I. (2021). Long-Term Effectiveness of a Mindfulness Based Intervention (MBI) Program for Stuttering: A Case Study. ClĂnica y Salud, 32(2), 55 - 63. https://doi.org/10.5093/clysa2021a1
raquel.rodrĂguez@uam.es Correspondence: raquel.rodrĂguez@uam.es (R. RodrĂguez-Carvajal).Stuttering is a communication disorder “whose primary symptoms are disfluencies, involuntary disruptions in the normal flow of speech” (Smith & Weber, 2017, p. 2485). People Who Stutter (PWS) exactly know what they would like to say but they encounter difficulties in producing a normal flow of speech (National Institutes of Health, 2020). Findings support that stuttering has a complex and heterogeneous etiology (Smith & Weber, 2017), ranging from genetic predisposition (Frigerio-Domingues & Drayna, 2017) to psychosocial factors (Boyle, 2016). Psychosocial factors are related to the tendency to react anxiously to novel situations or people (Mongia et al., 2019) or with the negative attitude of parents or listeners to speech, who focus especially on involuntary disfluencies or stress (Kefalianos et al., 2012). First symptoms of stuttering usually appear around 2 and 4 years of age (National Institute of Health, 2020), when the child begins to use connected language, longer linguistic forms, and more complex sentences (Wolk & LaSalle, 2015). Generally, in most cases a recovery occurs spontaneously after one year from the first symptoms (Blomgren, 2013). However, if the problem persists, the likelihood for stuttering increases, leading to several difficulties in social, academic, and workplace settings later on (Craig & Tran, 2006). Linked to the stuttering, signs of stress are manifested through facial tension (e.g., eye closing) and/or tension in the speech articulators (e.g., jaw and lips) (Craig & Tran, 2006). Furthermore, a high-level anxiety can cause the appearance of fear of stuttering in public, avoidance behaviors, and a set of negative thoughts related to difficulties in expression (Harasym et al., 2015). Additionally, the stutterer is often able to anticipate the mockery or discrimination that her or she will suffer and may even avoid any situation where his/her stuttering becomes apparent (Kefalianos et al., 2012). This avoidance leads to a lack of social skills and has a profound impact on relationships that could increase negative feelings such as frustration or embarrassment and low self-esteem (Craig et al., 2015). Mindfulness and Stuttering A stuttering disorder is associated with many problems besides speech disruption (Craig & Tran, 2006), highlighting the discussion above about the importance of emotional factors involved in PWS’ daily life. PWS are at risk of meeting criteria for panic disorder, social phobia, and generalized anxiety disorder (Iverach et al., 2009), and their quality of life and social and emotional functioning are decreased (Beilby et al., 2012; Craig et al., 2009). With regard to current treatments for stuttering, research findings suggest that even if therapy improves speech fluency, there is a strong likelihood to suffer from a relapse when the treatment ends (Emge & Pellowski, 2019). Other findings suggest that cognitive and emotional management are related to fewer relapses, in comparison with those who had not been treated with any type of psychological intervention (Hancock & Craig, 2002). Thus there has been an increased interest in adding factors such as cognitive and affective management in cognitive-behavioral therapy (CBT), due to the need for maintaining the expected long-term benefits (Menzies et al., 2009). Menzies et al. (2009) examined the effect of CBT on anxiety and stuttering in PWS. They concluded that in PWS, CBT may improve psychosocial functioning (e.g., decreased avoidance behaviors and anxiety symptoms) but not speech fluency when these treatments are a supplement in speech restructuring treatments; in many cases PWS experience feelings of embarrassment due to the speech control techniques (Emge & Pellowski, 2019). Due to these negative reactions to control techniques, we hypothesize positive benefits of third-generation therapies (Kahl et al., 2012). Therapies within the so-called “third wave” come from Eastern practices and contextual behavioral sciences, and they are mainly focused on awareness, acceptance, and understanding the context of thoughts and emotions rather than controlling them and changing their content (Hayes et al., 2006). The third wave of behavior therapy has been considered as effective in treating different mental health problems, such as anxiety disorders (Gu et al., 2015), which co-occur prevalently in many cases with stuttering disorders (Iverach et al., 2009). These third-wave behavioral approaches may provide valuable dimensions to stuttering therapy beyond or supplemental to those of CBT, such as self-control and self-responsibility interventions (Palasik & Hannan, 2013). Within these therapies, mindfulness interventions might help to achieve these goals (Gu et al., 2015). Mindfulness practice helps the individual to observe and accept the thoughts, feelings, and emotions that arise as phenomena of mind (Baer, 2003). The person becomes aware of his/her private and automatic mind processes, not giving credibility automatically (Segal et al., 2002). Mindfulness-based interventions (MBI) are designed to promote mindfulness skills. Mindfulness is defined as a nonjudgmental awareness developed instant by instant, moment by moment, by a kind of nonreactive attention, open and unprejudiced in the present moment (Baer, 2003). Previous findings in mindfulness interventions for stuttering supported that adding mindfulness exercises (e.g., awareness in daily activities, breath exercises, body scan, change the relationship with thoughts) are useful for an effective speech-treatment, although more research in this line is needed (Medina & Mead, 2020). The application of these mindfulness techniques has shown improvements concerning the stress and anxiety related to the speech situations, linked with a more positive attitude towards these anxious speech scenarios (de Veer et al., 2009). Moreover, previous research strongly pointed out that CBT intervention plus MBI is more effective than CBT alone (Gupta et al., 2016). Therefore, we propose that these MBI techniques can be of great interest for successful management of behavioral and emotional aspects in stuttering cases (Emge & Pellowski, 2019). The Mechanism of Change in Mindfulness that Is Needed in Stuttering Treatments Boyle (2011) proposed a set of techniques drawn from mindfulness-based cognitive therapy consisting of changing a relationship of the person with thoughts, feelings, and body sensations. Behavioral exposure. Behavioral exposure has been used in stuttering treatment to reduce fear and avoidance (Menzies et al., 2009), which is extremely related to successful long-term stuttering management (Plexico et al., 2009). Fear and avoidance have to be diminished to allow a restructuring speech treatment (Menzies et al., 2009). Mindfulness promotes exposure to internal or external events that are usually avoided by observing feared thoughts and emotions nonjudgmentally (Baer, 2003). Baer considered it essential to decrease avoidance and escape behaviors to develop an open, nonreactive, and nonjudgmental attitude toward avoided events, increasing the use of effective coping skills. These goals may be important for PWS and accomplished by MBI. Emotion regulation. Ramel et al. (2004) argued that the accumulation of negative experiences in the past and the anticipation of a failed situation obstruct the behavioral change. In addition, this ruminative pattern favors the maintenance of negative emotions, causing a negative reinterpretation of external events and hindering the use of effective coping strategies (Ramel et al., 2004). In this sense, mindfulness practice leads to emotional self-regulation improvement through the distinction between emotional natural reaction of an event and the process to add extra meaning (Malinowski, 2013), leaving emotions to be experienced naturally but interrupting the reinterpretation cycle (Williams, 2010). Boyle (2011) suggested that “if emotions are effectively regulated, PWS may be more able to focus on the behavioral and emotional targets of their treatment” (p. 124), so mindfulness training may be a valuable way to improve this emotion regulation. Changes in thought perceptions and increased sensory-perceptual processing. Chiesa and Serreti (2011) indicated that training in MBI entails changes in the thought perception through the interruption of one’s literal interpretation considering “just thoughts” and not “absolute truths.” This view of thoughts as passive mental events may reduce the fear response (Teasdale et al., 2002). Furthermore, the practice of mindfulness involves the increased use of the sensory-perceptive process, increasing the attention paid to physical sensations (Hölzel et al., 2011). In addition to this, Boyle (2011) claimed that the increase in the attention paid to the physical sensations in speech movements, combined with a decrease in the literality of thoughts, are essential to long-term stuttering management. Attentional control. This issue appears as a key process in speech therapy (Heitmann et al., 2004), revealing that PWS have difficulty in controlling attention. On the other hand, theoretical models in mindfulness mechanisms posit an attentional regulation process as the basis of mindfulness skills (Malinowski, 2013). Thus, attentional trainings through MBI could be added to speech therapy to improve the effectiveness of the treatment and achieve long-term positive effects and even avoid possible relapses. Moreover, the increase of attention with kindness and a nonjudgmental attitude leads to decreasing the mechanism of denial and avoidance, therefore shortening the cycle of fear, stuttering, and avoidance (Boyle, 2011; Mongia et al., 2019). Acceptance. Acceptance is one of the skills improved by mindfulness practice and is the opposite of avoidance, escape, and suppression of symptoms (Baer, 2003). MBI is associated with lower levels of experiential avoidance (Segal et al., 2002) and with lower levels of anxiety (Levitt et al., 2004). Many authors have emphasized the importance of the acceptance process in the successful management of stuttering (Levitt et al., 2004). In fact, this acceptance component appears to be incompatible with maladaptive reactions, which only exacerbate stuttering (Emge & Pellowski, 2019). More recent studies, such as those of Beilby et al. (2012) and Palasik and Hannan (2013), show that acceptance of disfluencies and associated thoughts reduces the negative judgments and allows the individual to acquire a pattern of more flexible thinking. All in all, the relevance of this work lies in the originality of using third-generation therapy for the treatment of fluency disorder. Furthermore, empirical evidence is needed in this field to demonstrate Boyle’s (2011) theoretical proposal. We believe that MBI can help in the treatment of stuttering cases, specifically by reducing anxiety symptoms and the disfluencies in speech. In addition, on a general level, it is necessary to broaden and deepen the knowledge about the clinical management of fluency cases such as stuttering, in an effort to identify new possibilities on top of what has already been established. The goals of the present study are to a) reduce the disfluencies in speech, b) reduce anxiety symptoms, and c) increase the development of mindfulness attentional skills. Therefore, we hypothesized that the MBI program will reduce participants’ speech disfluencies in the different tasks, the anxiety symptoms associated, by the time that increases the mindfulness skills after the intervention. Participants Participants were two males, one adolescent who stuttered and one young adult who stuttered, selected due to their wish to voluntarily participate. None inclusion nor exclusion criteria were considered as they were the only two people available for taking part in the intervention. A written informed consent and information were given to each participant. Parental consent was obtained for video recording and consent for the use of data for academic purposes in the case of participant 1 was also obtained. Neither participant 1 nor participant 2 had been previously enrolled in any stuttering or psychological treatment. Participants presentation. The first participant was a 15-year-old student in his third year of compulsory secondary education in a public school in Spain. Participant 1 refers to being stuttering since he was a child, being conscious of the problem but not generating as much anxiety as he was used to dealing with it. He refers to stutter more in those situations in which he has to read in front of a big public, especially if he has not enough confidence (something that does not occur with friends) and those situations interacting with new people. The initial assessment with the Stuttering Severity Index revealed a severe degree of stuttering in the pretreatment. The second participant was a 20-year-old student in the second year of a history degree at a public university in Spain. He refers to have lived with this issue for a long time, since he has memory, and to find it quite difficult in his daily routine. Although he tried to do almost everything related to his studies (e.g. he is aware that avoiding public presentation will worsen the problem), he refers to feel anxious and worried about his future, feeling unable to pass a work interview or working in the social media sector in which he wants to. The initial assessment with the Stuttering Severity Index revealed that the degree of stutter observed in the pretreatment was moderate. Measures Video recording of speech sample. Fernández-Zúñiga and Caja’s (2008) work revealed that the most reliable measure of speech disfluency is a video of spontaneous speech and reading. In this study, we deployed video recording in which the participants spoke about a daily event, spoke about a recently watched film, and read a short part of a book. The video samples were given to three judges to calculate their level of agreement about the observed stuttering. Stuttering Severity Instrument. The Stuttering Severity Instrument (Todd et al., 2014) is a reliable and validated mechanism to evaluate the degree of stuttering severity. This instrument includes both spontaneous speech and reading, and provide us with data in four categories: frequency, which is the number of syllables stuttered (i.e., number of repetitions, blockages, sounds prolongation, word partitions); duration, in terms of average length in seconds of the longest stuttering events; physical concomitants, referring to distracting sounds, facial grimace, head movements, and movements of extremities (i.e., associated movements); and naturalness of an individual’s speech (tension and strain), counting the percentage of disfluencies and severity of the stuttering. In this sense, we could find four levels of stuttering severity: very light (2 % of total disfluencies), mild (2-15 % of total disfluencies); severe (15-25 % of total disfluencies), and very severe (> 25 % of total disfluencies). State and Trait Anxiety Inventory (STAI). The STAI scale (Spielberger et al., 2002) consists of 40 items, of which the first 20 relate to state anxiety, referred to a temporal anxiety more related to specific situations (e.g., “Now, I feel nervous”), and the last 20 to trait anxiety, referred to the general disposition of being anxious (e.g., “In general, I feel worried”). Responses follow a Likert scale ranging from 0 (nothing) to 3 (a lot). Reliability indices are good, ranging from .90 to .93 for state anxiety and from .84 to .87 for trait anxiety. Mean scores for males in the general population are 20.54 for state anxiety and 20.19 for trait anxiety. A score up to this mean score is considered as high. Five Facets Mindfulness Questionnaire (FFMQ). The FFMQ questionnaire (Baer et al., 2006) consists of 39 items that assess different facets of mindfulness: observation, based on the attention paid to both internal and external events, thoughts, and emotions; description, based on the labeling of inner experiences into words; acting with consciousness or ability, focused on an activity of the moment; not judging, based on the nonevaluative relationship with our thoughts and feelings; and nonreactivity, which allows the flow of thoughts and feelings in our mind without intending to eliminate them. Cronbach’s alpha coefficients were .81 for the observation dimension, .91 for description and not judging, .89 for acting with conscience, and .80 for nonreaction. Responses follow a Likert scale ranging from 1 (never or almost never true) to 5 (very often or almost always true). Mean scores for each dimension in the general population are 23.6 for observing, 28.7 for description, 27 for acting with consciousness, 26.8 for not judging, and 20.6 for nonreactivity. Scores up to these means scores are considered as high. Toronto Mindfulness Scale (TMS). The TMS scale (Lau et al., 2006) gives us information about the consciousness we have about our experience of the present moment, through the scale of curiosity, and the ability to disidentify us with thoughts and feelings through a decentering scale. Cronbach’s alpha coefficients were .93 and .91, respectively. The scale consists of 13 items with a Likert response format ranging from 1 (not at all) to 5 (a lot). Mean scores in the general population are 16.42 for curiosity and 23.29 for decentering. Data Analysis Firstly, videos in the first and fifth session were used to calculate the severity of stuttering using the Stuttering Severity Index. Secondly, the same videos were judged by three individuals who examined the time and type of disfluency of the participants. The observers of the videos were clinicians who had had different stuttering cases in their careers and each had had at least 6 years of expertise in assessment. Their analysis and assessment of the videos was done under blind conditions, without knowing whether the videos reflected pre- or post-treatment. A Fleiss kappa coefficient was calculated to assess the degree of concordance in the stuttering severity of our participants (Torres-Gordillo & Perera-Rodríguez, 2009). Lastly, to check whether there was a significant clinical change between pre- and post-measures, we used the reliable change index (RCI), which gauges how much change has occurred during a therapy (Atkins et al., 2005). We obtain a significant change whether this RCI is bigger than the difference between the pre- and post-measures. Procedure First we carried out a search for potential participants by contacting a national stuttering association in our country, on the basis of which we identified two volunteer participants. We planned a regimen of five weekly 2-hour sessions. The sessions were individually held in a private room in which the expert therapist used to work as a clinical psychologist. The intervention was carried out during the months of March and April, establishing the follow-up the next year in April in the same context, being the participants personally contacted. The participants come to the intervention sessions on different days, previously fixed, and being the same weekday throughout the intervention. In sessions 1 (pre-treatment) and 5 (post-treatment), measures of the speech characteristics, anxiety, and mindfulness skills were taken. Furthermore, these sessions were informative: in session 1, we explained what mindfulness is and what we mean by full consciousness, and session 5 was a review of training and the development of a plan of action. Sessions 2, 3, and 4 consisted of mindfulness skill training; each session began and ended with participants’ responses to the TMS scale. The clinical professional responsible for carrying out the intervention was an expert with more than 10 years of experience in clinical intervention and MBI programs. MBI intervention. The intervention program consisted of five weekly 2-hour sessions that were individualized for each clinical case. The programmatic development is explained below. Session 1 began with taking pretreatment measurements, followed by the practice of exercises to achieve full consciousness in daily activities and exit the “autopilot” mode (i.e., the tendency of the mind to disconnect from what the body does, called “mind wandering”). For example, different exercises related to either walking while paying attention to the muscles, feet, and limbs, or eating a nut while paying attention to the sensations in the mouth. It was shown that fully attending to something in a direct way changes the experience itself. This could be useful for the treatment of stuttering, allowing the person to tune into the physical sensations of speech production. As an informal mindfulness practice, the participants were asked to focus attention on one daily activity in their routine (i.e., participant 1 was suggested to pay attention to his sport practice and participant 2 was suggested to pay attention when he was walking to the faculty), at least for one hour per day. They were asked about this experience in the next session to assess (1) whether they had accomplished the informal practice and (2) the possible difficulties found. In session 2, the participants were taught to focus on a specific part of the body (“body scan”), based on the physical sensations in that region, and then to move the attentional focus to other body regions, i.e., starting paying attention to our feet and then moving our focused attention toward our limbs, stomach, and breast. At the end of the session, participants were taught to be aware of breathing (i.e., instructed to be fully aware of inhalation and exhalation in the stomach), allowing the flow of thoughts, emotions, and feelings without judging, without reacting to them, and then refocusing attention on the breath. As an informal practice, they were invited to continue practicing audio-guided body scan at home at least twice during the week. After the session, participants completed a self-report on fearful situations that occurred during the week related to public speaking, including how they acted and how they thought they should have acted. Session 3 started with mindfulness of breathing, as previously practiced. In addition, participants worked on exposure through imagining the situations listed in the self-report, i.e., situations related to the avoidance of feared situations (participant 1: “I was unable to speak in English during the class because everybody was staring at me”; participant 2: “I was invited to give an oral communication in a congress but I am absolutely scared of doing wrong”). Participants were then trained in a new relationship of oneself with one’s thoughts, that is, the interpretation of thoughts as mental acts and not absolute truths that need to be carried out. The instructions given were as follows (Segal et al., 2002): a) observe how thoughts come and go without following them, b) understand that these thoughts are mental acts that need not be carried out at the time, c) write out the thoughts on paper so that the emotional reaction is less intense and may be a more thoughtful response, and d) analyze how the idea comes about and whether or not it fits the current situation. They were asked to continue practicing this observation of thoughts as not absolute truths using the self-report of anxious situations previously taught when they appeared. Session 4 consisted of training the attention on the flow of feelings and thoughts using exposure through imagination of the feared situations. An alternative response was trained through the SOBER exercise (Stop, Observe, Breathing, Expand, Respond; Bowen et al., 2013). This exercise is meant to teach acting consciously, focusing on the process, not the outcome. With this exercise, the participants were exposed through imagination to their feared situations, and a 3-minute space was intercalated to allow them to act in the way they would like to, trying to diminish the avoidance response that automatically appeared. After the session, participants were asked to practice this SOBER exercise at home as an informal practice and write possible difficulties found at least for an hour per day. The difficulties found during this informal practice allowed us to determine the degree of accomplishment of this task. In session 5, a plan of action was developed in case of a possible relapse. The main goal is the early recognition of a possible relapse to act in time, so the inclusion of family or friends in identifying possible signs could be helpful. It is also useful to recognize inappropriate strategies in the past that prevented the detection of signals. The point is not to avoid any possible regression and relapse but to know how to act when it happens. Specifically, participants 1 was asked to continue practicing their body attention to be aware of his muscle tension and make use of the audio-guided practice of body scan. The goal of this plan was to continue increasing his awareness in the body parts that make him feel relax so that he stutters less. Participant 2 was asked to work on his anticipatory anxiety, placing emphasis on the importance of writing down any negative situation that makes him feel anxious and to intercalate a space which allows him to act with consciousness, diminishing the avoidance behaviors. Participants were asked to continue practicing all the exercises taught, including in their daily routine at least 1 hour of paying attention (e.g., to the breath, to a daily routine exercise), writing down all situations in which they anticipate the anxiety related to public speech, and including the SOBER exercise when they feel anxiety. Table 1 Participants’ Speech Frequency 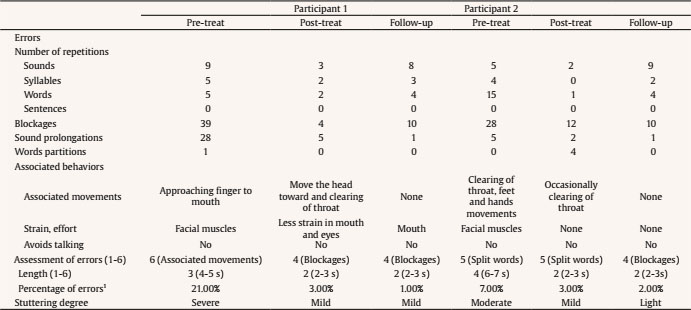 Note. 1Disfluencies/total of words = percentage; < 2% = very light; 2%-15% = mild; 15%-25% = severe; > 25% = very severe. Quantitative and qualitative analyses were completed of the pretreatment and post-treatment speech transcripts from each participant (Fernández-Zúñiga & Caja, 2008). The speech of participant 1 had 420 words in pretreatment and 502 words in post-treatment. Participant 2 had 663 words in pretreatment and 606 words in post-treatment. The results are summarized in Table 1. Stuttering Speech Frequency Fleiss kappa coefficient. Attending to the disfluencies types, three judges watched the videos and assessed the stuttering degree of the participants. Thus, the total number of observed disfluencies and the number of agreements were calculated, obtaining a total Fleiss kappa coefficient of .70 over 1, indicating a good concordance strength (Torres-Gordillo & Perera-Rodríguez, 2009). Participant 1. As shown in Table 1, we found a decrease in error rate of 18%, indicating a significantly diminished number of blockages and sound prolongations. In addition, there was a significant decrease post-treatment in associated movements and strain, showing fewer blockages and reducing the duration of these movements from four to two seconds. These changes occurred during the performance of the three exercises (i.e., speaking about a daily event, a recently watched film and reading a short part of a book). Similar results were obtained on the Stuttering Severity Index, for which there was a severe degree of stuttering in the pre-treatment condition (89-95%) and a decrease to mild stuttering post-treatment. Participant 2. The quantitative analysis of the speech sample (Table 1) indicates a decrease of language disfluencies of 4%, with a significant reduction in word repetition and number of blockages. The associated movements were smaller as well as the duration of these blockages, initially being of six seconds and at the end around two seconds. The Stuttering Severity Index supports these results, ranging from a moderate degree of stuttering before treatment to a mild degree after treatment. Overall measures of anxiety and mindfulness. These measures for each participant are summarized in Tables 2 and 3. Participant 1. As seen in Table 2, a nonsignificant clinical change was obtained in anxiety measured through the STAI questionnaire. However, the FFMQ questionnaire indicated a significant clinical change in “observation” and “act with awareness.” The “description” scale was close to reaching significance. The variables assessed through the TMS scale showed a significant clinical change between sessions 3 and 4 in the “decentering” dimension (see Table 3). Participant 2. As shown in Table 2, a significant clinical change was obtained in both scales of anxiety, trait and state. Also, in the FMMQ questionnaire a significant clinical change was obtained in the “not judge” dimension, and “description” was close to reaching significance. In regard to the TMS scale, significant clinical changes were found in session 2 in “decentering” and in sessions 3 and 4 in both “curiosity” and “decentering” (see Table 3). Follow-up measures Stuttering speech frequency. Follow-up measures of speech fluency taken one year after treatment are summarized in Table 1, showing that both participants maintained a low percentage of errors in speech. Participant 1 spoke 1,494 words and decreased his percentage from 3% to 1.74%, whereas participant 2, with 1,210 words of speech, maintained a similar percentage of post-treatment disfluencies. One year after treatment, both participants not only maintained the achievements they had gained after MBI training, but also exhibited longer speech and more words spoken. Overall measures of anxiety and mindfulness skills. Other measures taken one year post-treatment are summarized in Table 2. Participant 1 maintained his low anxiety measures from post-treatment and experienced a significant and positive clinical change in “observation,” experiencing a significant increase, and in the “not react” dimension, having diminished compared with a year before. Participant 2 obtained similar results, with a comparably low rate of anxiety symptoms as obtained after MBI, maintaining low trait and state anxiety levels, as well as a significant and positive clinical change in “not react” and “not judge,” with even higher scores than a year before, and a decrease in “act with awareness.” Table 2 Summary of Pre-treatment, Post-treatmen and Follow-up Measures in Both Participants, Including Reliable Change Index (RCI) 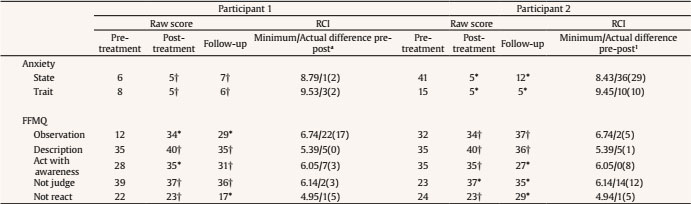 Note. FFMQ = Five Facets Mindfulness Questionnaire; 1minimum difference pre-post and pre-follow-up raw scores to become clinically significant/actual difference pre-post and (pre-follow-up) raw scores. *p < .05; †tendency non-significant. Table 3 Summary of TMS Measures in both Participants per Session, Including Reliable Change Index (RCI) 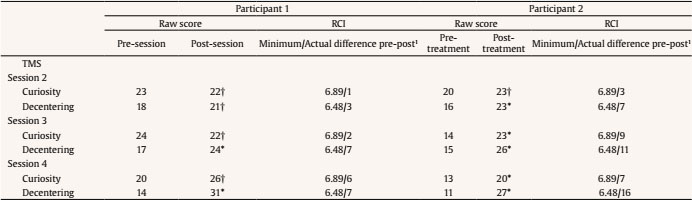 Note. TMS = Toronto Mindfulness Scale; 1minimum difference pre-post session raw scores to become clinically significant/actual difference pre-post raw scores. *p < .05; †tendency non-significant. Findings showed a reduction of language disfluencies in both participants, with a more significant decrease of disfluencies in Participant 1, from a severe to a mild degree after MBI. Moreover, in both cases a similar reduction occurred in terms of fluency characteristics of speech: a significant reduction in blockages and duration, in word repetition and prolongation of sounds, and the stress related to blockages. Regarding anxiety symptoms, only participant 2 achieved a significant clinical change. We hypothesize that the state/trait anxiety levels obtained by participant 1 were very low (10th percentile), so it was difficult to get a significant clinical change. Probably the stuttering in participant 1 may be caused or maintained by factors other than anxiety and emotional issues (Kefalianos et al., 2012). However, in participant 2, anxiety symptoms were significantly reduced, both state and trait, which could be related to the decrease in the degree of stuttering from moderate to mild after training. Highlighting the mindfulness skills, on the one hand, participant 1 had significant clinical changes in the dimensions of “observation” of internal and external events, “description” of inner experiences with words (close to a clinically significant change), and “act with awareness,” producing in this case the development of these skills that are beneficial in speech management. Moreover, regarding the TMS skills, we observed significant changes in the dimension of “decentering” in sessions 3 and 4. We may conclude that the progressive training in each session was useful to develop the ability to disidentify with their emotions and thoughts, being associated with the behavioral exposure (Plexico et al., 2009) and emotion regulation (Ramel et al., 2004) trained in those sessions. One explanation could be what Segal et al. (2002) argued that to develop techniques for speech, it is beneficial to let the process unfold naturally, because if one is focused on the end result, valuable attentional resources are used to compare what is happening with what one wants, so it detracts from one’s ability to process. We also know that PWS have difficulties in implementing their strategies of speaking, so that the greater the effort they exert, the greater the disfluency they have (Plexico et al., 2009). In this regard, stutterers show excessive attention to the speech disfluencies committed and have very strict criteria for what would be acceptable speech, so training focusing on the process and not the outcomes can supplement speech therapy. In this sense, it is important to highlight some difficulties found in the attention skills in this participant, especially in the two first sessions. Participant 1 found quite it difficult to focus his attention on his bodily sensation in the body scan practice, so we had to adapt the time of this exercise, starting with a brief period and then make it longer. Thus, this individualized intervention specifically for stuttering makes us more aware of individual difficulties and adaptation of the formal practice, increasing the likelihood of good learning. These difficulties could be related to being the first time practicing this kind of attention skills, which could explain the significant changes produced in this participant in the dimensions of observation and act with awareness as the effect of the practice. Participant 2 obtained a significant clinical change in the dimension of “not judge” and close to a significant clinical change in the dimension of “description”; there were already high scores for the dimensions of “observation” and “act with awareness”. In this case, it seems that this participant was more used to pay attention to their daily routines, as well as to be more aware of his bodily sensation related to stuttering. This fact could explain his higher scores in observation and act with awareness, in comparison with participant 1, and the facility to get significant clinical change in the latter. In contrast, participant 2 seems to beneficiate from the change in his relationship with thoughts through the mindfulness practice, being more aware of his judging attitude and trying to training this skill. This evidence may suggest that the presence of some attentional skills (i.e., observation and act with awareness) without the capability to handle them could be related to anxiety, whereas these attentional skills with the proper attitude of not judging could be useful in managing these emotional issues. On the other hand, the sensitivity of the TMS scale showed a good achievement of each session for the “curiosity” and “decentering” dimensions, showing significant clinical changes in the three sessions for both, except for session 2 that were changes only in the decentering dimension. It seems that the behavioral exposure linked to the emotion regulation trained in the two last sessions might be useful for this participant, as occurred with participant 1. Moreover, the attentional control trained from session 2 resulted in being useful to increase his level of curiosity. Boyle (2011) suggested that this technique would increase awareness of the tension that can occur in stuttering, for example in the neck and facial muscles. Moreover, Boyle’s study also showed that an increased awareness in bodily sensations can improve self-control of muscles used in speech and probably facilitate speech production. Thus, for participant 2, the development of attentional skills in thoughts, feelings, and sensations of the present moment, misidentifying with them and being able not to judge the experience, produced benefits in reducing anxiety symptoms and linguistic disfluencies. Furthermore, each session included training in the skills of describing feelings and emotions in words, which may have been beneficial as well. Therefore, we can say that MBI training may be an effective strategy for reducing symptoms of stuttering, although future studies with larger samples should deepen to establish firm conclusions. In addition, a reduction in anxiety symptoms was obtained for participant 2. Regarding the increase of mindfulness skills, we can say that participant 1 developed observation skills of feelings and thoughts, describing them and acting with awareness to leave the “autopilot” mode and gaining the ability to distance himself from these thoughts and feelings without being carried away by them (decentering). Participant 2 developed description skills of physical sensations, emotional feelings, and thoughts, without judging them, and also increased his capacity for curiosity and decentering about his experience. Regarding follow-up measures, we obtained promising results. One year post-treatment, both participants maintained a low rate of disfluencies comparable to that immediately post-treatment, and this was even lower for participant 1. These results may suggest that including emotional and attentional factors through the MBI program, as proposed in our study, i.e., training skills such as “not judge,” “description,” “act with awareness,” and “curiosity,” decreases the likelihood of relapse, as confirmed previously (Hancock & Craig, 2002). Furthermore, both participants maintained a low rate of anxiety symptoms even a year after MBI, suggesting that participants are able to communicate in an effective way with fewer syllables stuttered, and to feel less anxious. Thus, mindfulness practice may change the relationship between the person and his/her emotions and thoughts, a fact that is an important component for long-term stuttering management (Baer, 2003). Examining mindfulness skills in the follow-up measure, participant 1 showed a diminishment in his “not react” skill, a result that is compatible with our previous hypothesis about his low level of anxiety: the “not react” skill is not as necessary for participant 1 as for participant 2 due to his lower anxiety levels. He could manage stuttering without the “not react” skill in regard to his bodily sensations. In contrast, for participant 2, whose anxiety levels were higher, the “not react” skill increased in the follow-up measure, so for this participant a “not react” skill may be necessary for effective stuttering management, to decouple anxiety and stuttering. Plexico (2009) argued that a decrease in avoidance and fear responses is important to guarantee successful long-term stuttering management. Based on Boyle’s (2011) conclusions and our findings, mindfulness may be a valuable way to accomplish exposure to feared situations and to generalize them to a variety of contexts, empowering stutterers and providing a sense of control (Boyle, 2011), which has been related to successful long-term stuttering management (Mongia et al., 2019). The limitations of this study lie in the type of design used, as well as the sample characteristics and the dimensions evaluated. Firstly, in this study, the intervention was performed with only two willing participants. Future research in this field should involve projects with larger samples to establish control groups. In addition, one participant was a teenager, which may limit the development of mindfulness skills compared to an adult. The metacognitive abilities of participant 2, who is 20 years old, allowed a better understanding of the different skills. This age differential may also help to explain why the pretreatment anxiety levels were lower in the younger participant. In this regard, it should be recalled that the literature has found that the more situations and the longer the time period in which the person is exposed to a lack of fluency, the more negative the self-evaluation and anticipatory anxiety that may have been generated (Plexico et al., 2009). Moreover, our two participants were males, which limits the generalization of the results as previous studies found gender differences in the effectiveness of mindfulness practices, being females more likely to develop these skills (Kang et al., 2018). At the same time, other dimensions such as stress or quality of life could have been evaluated to see whether mindfulness skills training involves changes in these variables and the relationship with speech fluency. In this sense, we assessed the mindfulness skills that we were interested in training, and negative variables to provoke changes (i.e., trait and state anxiety). Positive variables, such as their self-efficacy in speech situations, locus of control, self-steam or satisfaction with the intervention, could be valuable to understand the long-term effects of this kind of interventions. Despite the timing for this MBI program, the five sessions scheduled cover the skills that have to be trained. Other recommendations for future projects could be to extend the period of informal practice of these exercises in order to achieve a more homogeneous and optimal development for the different facets of mindfulness. All in all, this pilot study allows us to deepen the applicability of mindfulness practices applying an individualized MBI to two participants, assessing pre and post-intervention as well as the changes in mindfulness skills during sessions. Therefore, this is a first step to continue growing the body of literature in this line. The aim of this study was to show descriptively the benefits of a MBI program in fluency disorders. The results of the intervention program showed that significant differences may occur in both clinical symptoms and behavioral problems associated with stuttering. Taking into account Boyle’s proposal (Boyle, 2011), as well as the scientific literature about the topic and our results, we suggest that mindfulness training may be worthwhile as a stuttering treatment and more research in this line is needed to contribute to our knowledge of its applicability. To conclude, our findings may address the potential incorporation of MBI programs into classical treatments to improve long-term success in therapy. Conflict of Interest The authors of this article declare no conflict of interest. Acknowledgements The authors thank the two volunteer participants who allowed us to boost this project and carry out the proposal. Cite this article as: Moreno-Jiménez, J. E., Rodríguez-Carvajal, R., García-Rubio, C., Castillo-Gualda, R., & Montero, I. (2021). Long-term effectiveness of a Mindfulness-based Intervention (MBI) program for stuttering: A case study. Clínica y Salud, 32(2), 55-63. https://doi.org/10.5093/clysa2021a1 Funding: Jennifer E. Moreno-Jiménez was granted a predoctoral fellowship, FPI-UAM 2017 of the Universidad Autónoma de Madrid. References |
Cite this article as: Moreno-Jiménez, J. E., Rodríguez-Carvajal, R., Garcia-Rubio, C., Castillo-Gualda, R., and Montero, I. (2021). Long-Term Effectiveness of a Mindfulness Based Intervention (MBI) Program for Stuttering: A Case Study. ClĂnica y Salud, 32(2), 55 - 63. https://doi.org/10.5093/clysa2021a1
raquel.rodrĂguez@uam.es Correspondence: raquel.rodrĂguez@uam.es (R. RodrĂguez-Carvajal).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
Clinical and Health is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License








