


Gender Influence on severe Mental Disorders: Relationship between Behavior Problems and Family Burden
[Influencia del g├ęnero en trastornos mentales graves: relaci├│n entre problemas de comportamiento y carga familiar]
Antonio Vázquez-Reyes1, Agustín Martín-Rodríguez2, María Ángeles Pérez-San-Gregorio2, Antonio J. Vázquez-Morejón1, and 2
1University Hospital Virgen del Roc├şo, Seville, Spain; 2University of Seville, Spain
https://doi.org/10.5093/clysa2021a3
Received 26 April 2020, Accepted 23 September 2020
Abstract
Gender differences in behavior problems and their relationship with family burden in severe mental disorders were analyzed. The Behavior Problems Inventory (BPI) and two items related to family burden (FB 1: “Do you feel able to endure the illness or disorder and the problems it causes?” and FB 2: “How often are you overwhelmed by these behavior/illness problems?”) were administered to 235 key informants under treatment in a community mental health unit. The results show that men presented more behavior problems and family burden, with significant differences in impulse dyscontrol and severe behavior problems. A positive correlation was found between behavior problems and family burden, where the inactivity/social withdrawal dimension was the best predictor of family load for men and women. We conclude that men have more behavior problems and that the inactivity/social withdrawal dimension has the most explanatory power for family burden in both men and women.
Resumen
Se analizan las diferencias de género en problemas de conducta y su relación con la carga familiar en trastornos mentales graves. El Inventario de Problemas de Conducta (BPI) y dos ítems relativos a la carga familiar (“¿Se siente usted capaz de sobrellevar la enfermedad o trastorno y los problemas que ocasiona?” y “¿Con qué frecuencia se ve usted desbordado/a por estos problemas de comportamiento/enfermedad?”) se administraron a 235 informantes clave de pacientes en tratamiento en una unidad de Salud Mental Comunitaria. Los hombres presentaban mayores problemas de conducta y carga familiar, existiendo diferencias significativas en descontrol de impulsos y en problemas de comportamiento graves. Se halla una correlación positiva entre problemas de comportamiento y carga familiar, siendo la dimensión inactividad/aislamiento social la mejor predictora de carga familiar. Respecto a la carga familiar, es la dimensión inactividad/aislamiento social la que posee mayor capacidad explicativa en hombres y mujeres.
Palabras clave
Problemas de comportamiento, Trastornos mentales graves, Carga familiar, Descontrol de impulsos, Aislamiento socialKeywords
Behavior problems, Severe mental disorders, Family burden, Impulse dyscontrol, Social withdrawalCite this article as: Vázquez-Reyes, A., Martín-Rodríguez, A., Pérez-San-Gregorio, M. Á., and Vázquez-Morejón, A. J. (2021). Gender Influence on severe Mental Disorders: Relationship between Behavior Problems and Family Burden. Cl├şnica y Salud, 32(2), 65 - 70. https://doi.org/10.5093/clysa2021a3
antvazrey90@gmail.com Correspondence: antvazrey90@gmail.com (A. V├ízquez-Reyes).The study of severe mental disorders has a very relevant place in mental health due to its psychopathological richness and variability, their transfer to behavioral problems (Wykes & Sturt, 1986), and their personal, family, social, and economic impact (Jin & Mosweu, 2017). In this context, gender is a variable which has been acquiring relevance in the study and understanding of severe mental disorders (Jiménez-García-Bóveda & Vázquez-Morejón, 2012; Ordóñez et al., 2016). Due to discrimination undergone by the female population insofar as research on their needs (Goldstein & Tsuang, 1990; Hosang & Bhui, 2018) and the influence which stereotyped roles of males appear to exert (assumption of more risk conduct, use of violence, dominance over others, etc.) on the psychopathology of men (Mahalik et al., 2003; Tager et al., 2010), in recent years a need has arisen to progress in understanding the impact of gender on severe mental disorders. From this perspective, the inclusion of a gender-sensitive focus is pertinent for early detection, evaluation, and clinical intervention adjusted to individual needs. Other studies focusing on gender differences have found more externalizing disorders in men and internalizing in women (Zahn-Waxler et al., 2008). Traditionally, study has concentrated on clinical variables (prodromal, duration of untreated psychosis, positive and negative symptoms, etc.), with inconstant, not very conclusive results (Koster et al., 2008; Morgan et al., 2008). The diversity of results underlines how these clinical variables can become unspecific, as patients with the same diagnosis have different symptoms (APA, 2013), which is the main reason studies focus on elements common to all, such as affectation in social functioning (Carpenter & Strauss, 1991), behavior problems (Vázquez-Morejón et al., 2018), and family burden (Awad & Voruganti, 2008; Möller-Leimkühler & Wiesheu, 2012). Research generally emphasizes better social functioning in women, both premorbid and over the course of the illness (Morgan et al., 2008; Thorup et al., 2007). Females specifically show better social functioning in the areas evaluating autonomy and employment, while there are no significant differences in gender in dimensions such as social integration, communication, or leisure (Jiménez-García-Bóveda et al., 2000). In social functioning, Brewin et al. (1987) described behavior problems as a construct that can interfere with adaptation and social functioning in such patients. From this perspective, behavior problems are understood as the behavioral expression of the characteristic psychopathology of psychosis and related disorders (Wykes & Sturt, 1986). Due to this conceptualization, its study is progressively acquiring more relevance in view of the need to include objective, observable approaches which enable the study of adaptation of these patients to their community context (Cella et al., 2014). Along these lines, several studies have attempted to delimit the main behavior problems in this clinical population. Harvey et al. (1996) found four behavior problem factors in schizophrenia (social isolation, altered thinking, antisocial behavior, and depression) which were later replicated and confirmed by Curson et al. (1999). Recently, Vázquez-Morejón et al. (2018) found three factors (inactivity or social isolation problems, active problems, and impulse dyscontrol) which included the main behavior problems in psychosis and related disorders. Previous studies have explored the relationship between behavior problems and levels of autonomy (Wykes, 1982), family burden (Othman & Salleh, 2008), and family’s capacity for coping (Vázquez-Morejón et al., 2013). However, there is little knowledge of the differences in behavior problems by gender and their relationship with family burden. Thus, in a scientific context in which interest in studying the factors common to functional affectation is gradually growing, the objective of our study was to explore the differences in behavior problems between men and women and their possible relationship with family burden. The study sample consisted of 235 key family members of patients diagnosed with a severe mental disorder: schizophrenia (ICD-10 F.20), other psychotic disorders (ICD-10 F.21-F.29), or bipolar disorder Type 1 (ICD-10 F.31). The mean age of the patients was 40.13 (SD = 11.67, range = 18-65); 152 were men (64.7%) and 83 women (35.3%). The distribution by marital status was: 178 single (75.7%), 38 married (16.2%), 13 separated (5.5%), and 6 widowed (2.6%). They were diagnosed with the following disorders: 132 with schizophrenia (56.2%), 60 with psychotic disorders (25.5%), and 43 with bipolar disorder Type 1. Informants were: 113 mothers (48.1%), 37 fathers (15.7%), 26 spouses (11.1%), 35 siblings (14.9%), and 24 other relatives (10.2%). There were 171 women (72.8%) and 64 men (27.2%). All the patients in treatment in a Community Mental Health Unit (CMHU) at the time the study was begun who met the following inclusion criteria: 1) of legal age, 2) had any of the diagnoses mentioned above, and 3) agreed to participate in the evaluation. Criteria for the inclusion of family members were that their participation in the study was voluntary and they had been selected by the patient as persons with the most knowledge of their condition. Thus, key family members were in charge of filling out the evaluation instruments. Behavior Problem Inventory (BPI). The BPI (Vázquez-Morejón et al., 2018) was designed as a rapid and efficient measure of the most representative behavior problems of individuals with psychosis and related disorders. It consists of 14 items and three dimensions (identified by factor analysis): inactivity/social withdrawal (points vary from 0 to 15), active problems (0 to 15 points), and impulse dyscontrol (0 to 12 points). Two other scores are also found: moderate behavior problems (MBP, number of items with score equal to or over 2, where scores are 0 to 14) and severe behavior problems (SBP, number of items with score equal to 3, where scores vary from 0 to 14). The higher the score, the greater the behavior problems. The answers refer to behavior observed during the last three months rated on a Likert-type scale where 0 = never, 1 = hardly ever, 2 = sometimes, and 3 = often. BPI psychometric properties support both validity and reliability, with excellent internal consistency (Cronbach’s alpha) for the 14 items (α = .85), for inactivity/social withdrawal (α = .76) and for active problems (α = .80), while for the impulse dyscontrol dimension the internal consistency is rather questionable (α = .56). Temporal reliability measured by the total score of behavior problems in 28 patients was satisfactory (r = .82, p < .001). Furthermore, empirical evidence shows significant correlations supporting both concurrent validity with the Social Behaviour Schedule (SBS) and construct validity with the Social Functioning Scale (SFS) (Vázquez-Morejón et al., 2018). Perceived family burden. Family burden was evaluated by asking a relative to respond to the following items: “Do you feel able to endure the illness or disorder and the problems it causes?” (FB 1) and “How often are you overwhelmed by these behavior/illness problems?” (FB 2). Both were answered on a Likert-type scale where 0 = not at all, 1 = a little, 2 = somewhat, 3 = quite often, and 4 = a lot. A score is also found for total family burden resulting from the mean of the scores on both items. The sample of 235 patients was chosen from a database of people with severe mental disorders at a Virgen del Rocío University Hospital CMHU. Patients who were under treatment and met criteria for inclusion at the start of the project were selected. The diagnosis had been made by a referral clinical psychologist or psychiatrist in each case based on the clinical history and psychopathological exploration. During the usual psychological evaluation of the patients being followed up, a member of the team (the one with the closest contact and/or confidence with family) requested the participation of key family members and told them that it was entirely voluntary and, if they accepted, they were given the evaluation instruments to fill in. Analyses were done using the SPSS v.24 statistical package. First, a descriptive analysis was carried out to study gender differences in behavior problems and perceived family burden (with the t-test for independent samples). Before the analysis, data were checked for non-normal distribution using the Kolmogorov-Smirnov test. However, the Levene test for equality of variances was not significant, so the homoscedasticity criterion was met. Cohen’s d was used to calculate the effect size (Cohen, 1988). Correlations between items and BPI dimensions and perceived family burden were also studied with Pearson’s correlation coefficient. Correlations are interpreted following Cohen’s (1988) guidelines, according to which the value of r classifies the correlation as small (r = .10 - .29), medium (r = .30 - .49) or large (r = .50 - 1.0). Finally, a stepwise multiple linear regression analysis was performed to predict the increase in family burden (criterion or dependent variable) using three predictor or independent variables that referred to the behavior problem dimensions (inactivity/social withdrawal, active problems, and impulse dyscontrol). Compliance with the statistical assumptions was confirmed before making the multiple linear regression analysis (linearity, independence of residuals, homoscedasticity, and no multicollinearity). Descriptive Analysis Table 1 shows the mean, median, Q1 and Q3, and the minimum and maximum scores on the 14 items, three dimensions (inactivity/social withdrawal, active problems, and impulse dyscontrol), MBP, and SBP. Table 1 Descriptive Analysis of Behavior Problems Found with the Behavior Problems Inventory (N = 235) 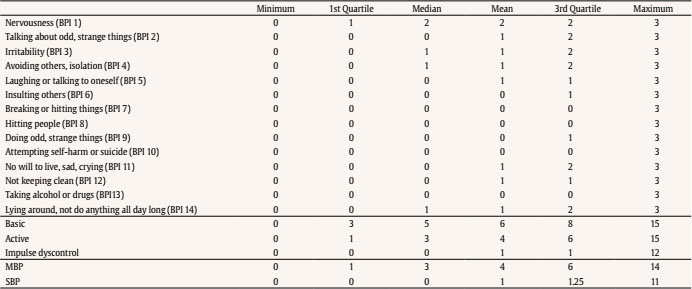 Note. Basic = Inactivity/social withdrawal dimension; Active = Active problems dimension; Impulse dyscontrol = Impulse dyscontrol dimension; MBP = Moderate behavior problems; SBP = Severe behavior problems. Item number 1 (“nervousness”) showed the highest mean, median, and Q1and Q3 scores, while the item with the lowest mean, median, and Q1and Q3 scores was number 13 (“Taking alcohol or drugs”). The inactivity/social withdrawal dimension had the highest mean, median, and Q1and Q3 scores, while the impulse dyscontrol dimension had the lowest scores. Figure 1 Impulse Dyscontrol in Other Psychotic Disorders by Gender. 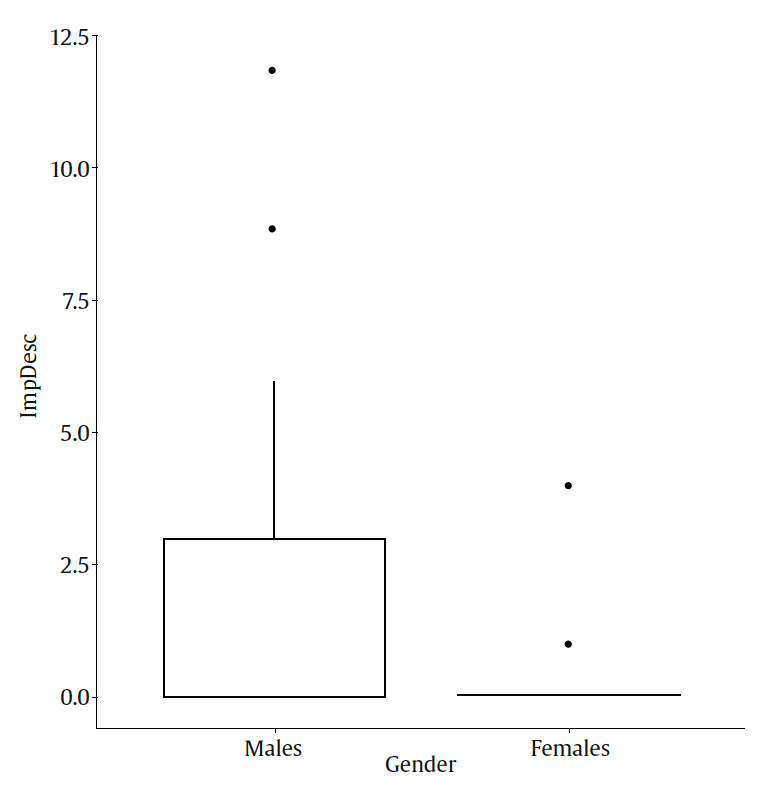 Gender Differences Significant gender differences were observed in the scores on behavior problems (Table 2). On items BPI 12 (“Not keeping clean”; p = .009, d = 0.346), BPI 13 (“Taking alcohol or drugs”; p = .001, d = 0.429) and BPI 14 (“Lying around, not do anything all day long”; p = .001, d = 0.432), there were more behavior problems among the men. Similarly, men also scored higher on the impulse dyscontrol dimension (p = .01, d = 0.339) and on SBP (p = .043, d = 0.269). Men scored higher on item FB 2 on family burden although it was not statistically significant. Table 2 Gender Differences in Behavior Problems and Family Burden 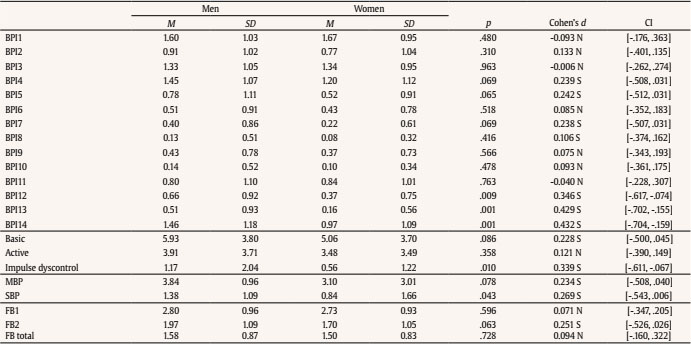 Note. BPI = Behavior Problems Inventory; basic = Inactivity/social withdrawal dimension; Active = Active problems dimension; Impulse dyscontrol = Impulse dyscontrol dimension; MBP = Moderate behavior problems; SBP = Severe behavior problems; FB = Family burden; CI = Confidence interval; N = Null effect size; S = Small effect size. Gender Differences in Behavior Problems by Diagnosis Figure 1 shows that men diagnosed with other psychotic disorders had significantly more behavior problems in the impulse dyscontrol dimension (p = .011, d = 0.744). No significant gender differences were found in the inactivity/social withdrawal, active problems or impulse dyscontrol dimensions among patients diagnosed with schizophrenia or bipolar disorder Type 1. Correlations between Behavior Problems and Family Burden The scores showed significant correlations between behavior problems and family burden (Table 3). Behavior problems most closely associated with family coping capacity (FB 1) were items BPI 3 (“Irritability”), BPI 11 (“No will to live, sad, crying”) and BPI 12 (“Not keeping clean”), all with small correlations. The most significant correlations regarding family perception of being overwhelmed (FB 2) pertained to items BPI 1 (“Nervousness”), BPI 2 (“Talking about odd, strange things”), BPI 3 (“Irritability”), BPI 4 (“Avoiding others, isolation”), BPI 6 (“Insulting others”), BPI 11 (“No will to live, sad, crying”), BPI 12 (“Not keeping clean”), and BPI 14 (“Lying around, not do anything all day long”), all with a medium correlation. Correlation with family burden was negative for FB 1 and positive for FB 2. Table 3 Correlations between Behavior Problems and Family Burden  Note. BPI = Behavior Problems Inventory; FB = Family burden; CI = Confidence interval. *< .01., **< .001. All of the dimensions were negatively correlated with coping with the illness (FB 1) and positive with perception of being overwhelmed (FB 2) (Table 4). The dimension which was the most strongly associated with family burden was inactivity/social withdrawal (FB 1, r = -.351, p = < .001; FB 2, r = .480, p = < .001), followed by active problems (FB 1, r = -.256, p = < .001; FB 2, r = .414, p = < .001), and in last place, impulse dyscontrol (FB 1, r = -.220, p < .01; FB 2, r = .275, p < .001). Table 4 Correlations between Behavior Problems Dimension and Family Burden 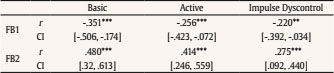 Note. Basic = Inactivity/social withdrawal dimension; Active = Active problems dimension; Impulse dyscontrol = Impulse dyscontrol dimension; FB = Family burden; CI = Confidence interval. **p < .01, ***p < .001. Family Burden Predictor The results of the multiple linear regression analysis with family burden as the dependent variable and the inactivity/social withdrawal, active problems, and impulse dyscontrol dimensions as predictors are shown in Table 5. The final model identified the inactivity/social withdrawal dimension as the only one able to predict family burden in men, F(3, 136) = 12.55, p < .001, and women, F(3, 69) = 12.56, p < .001. In the rest of the dimensions, neither active problems nor impulse dyscontrol were good gender predictors of family burden. This model explained 35.3% (R2 = .353) of the variance observed in family burden for women and 21.7% (R2 = .217) of family burden for men. Table 5 Behavior Problems Predicting Family Burden by Gender 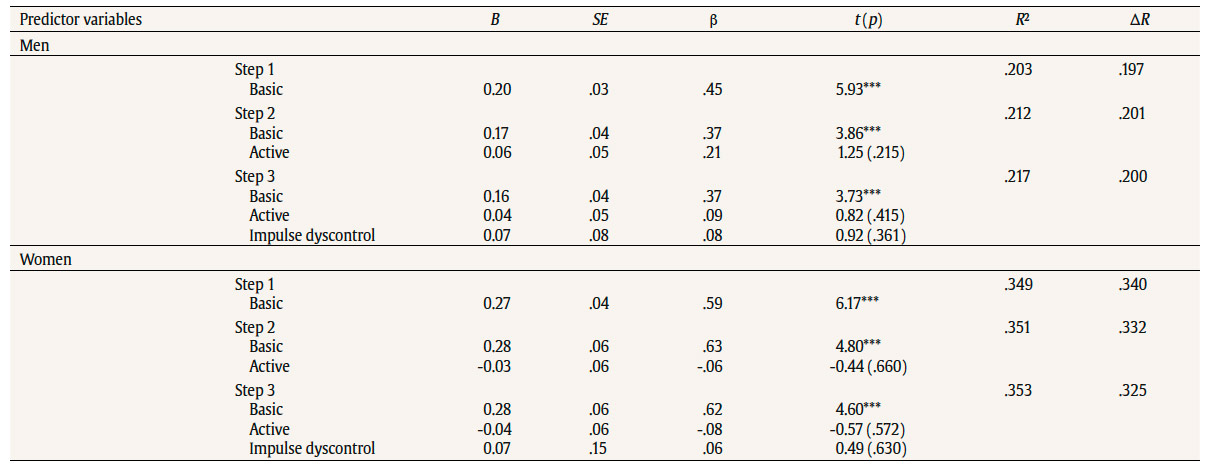 Note. basic = Inactivity/social withdrawal dimension; Active = Active problem dimension; Impulse dyscontrol = Impulse dyscontrol dimension. *p < .001 In general, the results show significant gender differences in behavior problems which were strongly related to the level of family burden perceived by family members who had frequent contact with the patients. Overall, men scored higher in behavior problems and in family perception of being overwhelmed by behavior problems. In agreement with previous research (Koster et al., 2008; Thorup et al., 2007), men had significantly greater impulse dyscontrol behavior problems than women while there were no significant differences in active problem dimensions or inactivity/social withdrawal. Men also showed significant differences in SBP, mainly explained by higher scores on the impulse dyscontrol behavior dimension. The results are in agreement with studies that emphasize the importance of socialization in men learning maladaptive emotional control strategies, associated with an increase in behavioral disinhibition, unhealthy behaviors, or acts of aggression by men (Gallagher et al., 2014; Panno et al., 2013). Men were found to score significantly higher on specific behavior problems in items BPI 12 (“Not keeping clean”), BPI 13 (“Taking alcohol or drugs”), and BPI 14 (“Lying around, not do anything all day long”), which evaluate behaviors in the inactivity/social withdrawal dimension. These results may be related to the fact that women show better social functioning in the areas of autonomy and competence (Jiménez-García-Bóveda et al., 2000). Results of the relationship between behavior problems and family burden were in line with Nordstroem et al. (2017) and Koutra et al. (2016), who suggested that family burden is greater when patients have a more severe and persistent psychopathology. Considering behavior problems as the expression of the underlying psychopathology (Wykes & Sturt, 1986), our study demonstrated that behavior problems are related to an increase in family burden, especially when such behavior is in the inactivity/social withdrawal dimension, and, to a lesser extent, behavior related to active problems and impulse dyscontrol. With regard to the evolution of the illness, emotion expressed has been shown to be a relevant construct in predicting relapse in patients with schizophrenia (Möller-Leimkühler & Wiesheu, 2012). Álvarez-Jiménez et al. (2012) emphasized the influence of critical and hostile comments of the main caregivers on relapse, which could be partially explained by the impact of behavior problems on family burden and its consequential effect on the increase in emotion expressed by main caregivers. Our results regarding the relationship between gender and family burden are in agreement with Mors et al. (1992), who suggested that the burden is heavier on the families of men. Although not statistically significant, it was observed that men’s families tended to be more intensely overwhelmed by the illness (FB 2). Coinciding with the study by Awad and Voruganti (2008), which related the increase in family burden with social impairment, our analysis found that the inactivity/social withdrawal dimension was the best predictor of family burden regardless of gender. Our findings seem to indicate that there are differential gender factors in the explanation for family burden. It is important to reflect on and study these differences to find out whether the roles culturally assigned to men and women (Goldstein & Tsuang, 1990), which have traditionally been more permissive with males, or the presence of psychosocial variables, may better explain male burden (social functioning, recovery time, treatment adherence, type of treatment received, quality of life, etc.). One of the limitations is the evaluation of behavior problems by a single family member who frequently interacted with the patient, and it might be recommendable to include other evaluation sources (other professionals, such as clinical psychologist, psychiatrist, or nurse) who could attribute behavior problems more objectivity and avoid possible bias (Sabbag et al., 2011). Another limitation is the procedure for measuring family burden, which is based on subjective evaluation with only two questions. This might have been more objective with an instrument with good psychometric properties such as the Involvement Evaluation Questionnaire (IEQ) (Schene & van Wijngaarden, 1992) or the Zarit Caregiver Burden Scale (Zarit et al., 1980). Finally, participants were selected from a single CMHU, so the inclusion of patients from other healthcare centers would have been more representative. Future studies could approach the relationship between behavior problems and gender in other functional dimensions affected by severe mental disorders, such as social functioning, recovery, quality of life, or attempted self-harm. More progress in identifying the differential factors that contribute to explaining family burden in men and women is still necessary. Finally, it would also be of interest to include a longitudinal perspective with which the relationship of these variables and their evolution over time may be studied. In conclusion, the results confirm the presence of more behavior problems in men in all three dimensions, inactivity/social withdrawal, active problems, and impulse dyscontrol. Inactivity/social withdrawal was the dimension with the most predictive power for burden in both men and women. Conflict of Interest The authors of this article declare no conflict of interest. Cite this article as: Vázquez-Reyes, A., Martín-Rodríguez, A., Pérez-San-Gregorio, M. Á., & Vázquez-Morejón, A. J. (2021). Gender influence in severe mental disorders: Relationship between behavior problems and family burden. Clínica y Salud, 32(2), 65-70. https://doi.org/10.5093/clysa2021a3 References |
Cite this article as: Vázquez-Reyes, A., Martín-Rodríguez, A., Pérez-San-Gregorio, M. Á., and Vázquez-Morejón, A. J. (2021). Gender Influence on severe Mental Disorders: Relationship between Behavior Problems and Family Burden. Cl├şnica y Salud, 32(2), 65 - 70. https://doi.org/10.5093/clysa2021a3
antvazrey90@gmail.com Correspondence: antvazrey90@gmail.com (A. V├ízquez-Reyes).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
Clinical and Health is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License








