


Quality of Life of Informal Caregivers of Cervical Cancer Patients: Analysis of Anxiety and Spirituality
[La calidad de vida de los cuidadores informales de las pacientes con cáncer de cuello uterino: análisis de la ansiedad y la espiritualidad]
Rosana Moysés1, B. Dainana Santos2, Adele Benzaken3, and M. Graça Pereira2
1Federal University of Amazonas, Manaus, Brazil; 2University of Minho, Braga, Portugal; 3Amazonas State University, Manaus, Brazil.
https://doi.org/10.5093/clysa2022a6
Received 13 March 2021, Accepted 20 October 2021
Abstract
This study analyzed the association and contribution of anxiety, spirituality, coping and burden to quality of life (QOL) in informal caregivers of patients with cervical cancer. The sample included 119 informal caregivers of patients undergoing treatment for cervical cancer at a reference hospital in the state of Amazonas, Brazil. The caregivers answered instruments that assessed sociodemographic variables, burden, coping, anxiety, spirituality, and QOL. Female caregivers used more spirituality (reflection and positive interpretation) than male caregivers. The number of hours of care dedicated by caregivers was positively correlated with their burden. Burden had a positive association with anxiety and was negatively associated with the caregivers’ mental QOL. Spirituality (reflection and positive interpretation) moderated the relationship between anxiety and caregiver’s mental QOL. The results showed the importance of interprofessional teams in oncology to intervene with caregivers, focusing on psychological morbidity to prevent burden and the spirituality as a coping strategy.
Resumen
Este estudio analiza la asociación y contribución de la ansiedad, espiritualidad, afrontamiento y sobrecarga con la calidad de vida (CV) en cuidadores informales de pacientes con cáncer de cuello uterino. La muestra fue de 119 cuidadores informales de pacientes en tratamiento de cáncer de cuello uterino en un hospital de referencia en el estado de Amazonas, Brasil. Los cuidadores cumplimentaron cuestionarios que evaluaban variables sociodemográficas, sobrecarga, afrontamiento, ansiedad, espiritualidad y calidad de vida. Las mujeres cuidadoras utilizaron más espiritualidad (reflexión e interpretación positiva) que los varones cuidadores. El número de horas de atención dedicadas por los cuidadores se correlacionaba positivamente con su sobrecarga. Esta tuvo una asociación positiva con la ansiedad, asociándose negativamente con la calidad de vida mental de los cuidadores. La espiritualidad (reflexión e interpretación positiva) moderaba la relación entre la ansiedad y la calidad de vida mental del cuidador. Los resultados mostraron la importancia de que los equipos interprofesionales de oncología intervengan con los cuidadores, centrándose en la morbilidad psicológica para prevenir la sobrecarga, así como en la espiritualidad como estrategia de afrontamiento.
Palabras clave
Cáncer de cuello uterino, Ansiedad, Espiritualidad, Cuidadores informales, Calidad de vidaKeywords
Cervical cancer, Anxiety, Spirituality, Informal caregivers, Quality of lifeCite this article as: Moysés, R., Santos, B. D., Benzaken, A., and Pereira, M. G. (2022). Quality of Life of Informal Caregivers of Cervical Cancer Patients: Analysis of Anxiety and Spirituality. ClĂnica y Salud, 33(2), 65 - 71. https://doi.org/10.5093/clysa2022a6
gracep@psi.uminho.pt Correspondence: gracep@psi.uminho.pt (M. Graça Pereira).According to the Pan American Health Organization, 56,000 new cases of cervical cancer (CC) are registered every year in Latin America, and 311,000 women died in 2018 from the disease. In 2017 in Brazil 6,385 deaths from CC were registered and the forecast for 2020 was 16,590 new cases of the disease in the country (Instituto Nacional do Cancer, 2020; Pan American Health Organization, 2019). In the Northern Region of Brazil cervical cancer is the second most incident type of cancer and 26.24 cases per 100,000 women were expected in 2020. The state of Amazonas is expected to have 580 new cases in the year 2020. There were 189 deaths from CC registered in the state in 2018, being an important public health problem (Foundation for Cancer Control of the State of Amazonas, 2017; Veiga et al., 2016). CC is a chronic disease with a long treatment and side effects inherent to antineoplastic therapy, which requires daily care for most patients and almost always the presence of formal or informal caregivers during their treatment (Veiga et al., 2016). Informal caregivers are defined as members of the family or the community (partners, friends, neighbors) who assume the role of providing care with guidance from a health care team, have no formal training, and do not receive any payment to provide this care (Sterling & Shaw, 2019). When analyzing the role of the caregiver in the Amazonian context, one has to consider that the only reference hospital for cancer treatment in the state is located in the capital, Manaus, while studies show that most patients with CC live in towns in the interior (Moysés et al., 2019). Therefore, due to the geographic characteristics of the state, patients are forced to remain in Manaus for the duration of the treatment, depending on caregivers and support homes (Moysés et al., 2019). In this scenario, caregivers dedicate long periods of the day to these patients and perform several tasks. In addition to providing care, they provide emotional support and act as relationship mediators between the patient and the health team. This dedication can generate physical burnout, burden, and have a psychological impact on quality of life (QOL) of caregivers (Figueiredo et al., 2017; Wakiuchi et al., 2017). Burden, defined as the physical, social, and psychological effects that result from the act of caring for a person who depends on the provision of continuous care, is associated with psychological morbidity (anxiety and depression) (Pereira & Carvalho, 2012). Studies show that factors such as being female, the duration of care and the patient’s level of dependence can increase caregiver burden (Lai et al., 2018; Surbone et al., 2010). The literature also reports that informal caregivers feel insecure due to the uncertain prognosis of the disease and the new roles and obligations, which are part of the act of caring; these factors are responsible for the feelings of vulnerability related to symptoms of psychological morbidity (Areia et al., 2019; Streck et al., 2020). Several studies suggest that psychological morbidity is an important predictor of the mental and physical quality of life of informal caregivers (Veiga et al., 2016; Wakiuchi et al., 2017). Coping includes cognitive and behavioral strategies used by individuals in an attempt to manage specific demands evaluated as stressors (Folkman et al., 1991). Caring for cancer patients may cause emotional discomfort requiring caregivers to resort to emotional and behavioral coping mechanisms (Botelho & Pereira, 2015). The literature describes that the way the caregiver adapts to the adversities imposed by the caregiving will depend on the power to react to the difficulties during the course of the illness and on the effectiveness of one’s coping strategies (Aydogan et al., 2016; Coppetti et al., 2019). Among caregivers of cancer patients, coping has been shown to moderate the relationship between psychological morbidity and QOL, i.e., caregivers with better coping strategies showed lesser symptoms of anxiety and better QOL (Coppetti et al., 2019; Teskereci & Kulakaç, 2018). In the Brazilian population, the differentiation between the concepts of spirituality and religiosity may be hard to make (Mesquita et al., 2019). However, the literature considers spirituality a subjective issue which brings harmony between oneself and others centered on three domains: connection, meaning of life, and transcendence that is not limited to having a religion (Paul Victor & Treschuk, 2020; Weathers et al. 2016). In a study with Brazilian caregivers, spirituality was perceived as providing comfort and peace, and the act of caring for a sick family member, a divine opportunity for personal and spiritual transformation (da Silva et al., 2018; Paiva et al., 2015). Spirituality among caregivers may be considered a way of dealing with the chronic illness, since it played a moderating role in the relationship between psychological morbidity and QOL of caregivers during the treatment period (Lalani et al., 2018). According to the literature, caregivers with more symptoms of psychological morbidity have lower QOL, but spirituality was a protective factor in that the negative relationship between morbidity and QOL was less intense when spirituality was high (Ochoa et al., 2020; Teskereci & Kulakaç, 2018). The importance of informal caregivers to CC patients and the complexity of the factors involved during the care process, especially due to the epidemiological demand in the Amazonas state, require specific research regarding the variables that contribute to QOL as well as the moderating variables in the relationship between psychological morbidity and QOL in informal caregivers of cancer patients. Study design and sample This cross-sectional study analyzed the associated and moderating variables regarding QOL, in informal caregivers of CC patients undergoing treatment at the reference hospital for cancer treatment in the State of Amazonas, the Oncology Control Center Foundation of Amazonas (FCECON), in the Manaus capital. The sample was non-probabilistic and calculated based on the estimated number of new cases of cervical cancer treated at FCECON in 2016, taking into consideration a confidence level of 95%, an anticipated effect size of 0.15 and a desired statistical power of .80, with nine variables, and the minimum required sample was 113. The participants were informal caregivers, 18 years old or over, of patients diagnosed with CC undergoing treatment (chemotherapy/radiotherapy) at FCECON. There were two indigenous patients and, consequently, their caregivers were excluded from the sample due to cultural and linguistic peculiarities. Instruments Sociodemographic questionnaire, assessing age, gender, race, location, marital status, education, occupation, income, family relation towards the patient, cancer stage (patient), and hours dedicated to care. Burden Interview Scale (BIS; Zarit & Zarit, 1987; Brazilian version by Scazufca, 2002): This instrument assesses the burden in informal caregivers of patients with chronic illnesses with 22 items that refer to concern areas for caregivers, namely health, social and personal life, financial situation, emotional well-being, and interpersonal relations. Questions 1 to 21 are scored as 0 (never), 1 (rarely), 2 (sometimes), 3 (frequently), 4 (always); and item 22 as 0 (not a little), 1 (a little), 2(moderately) 3(very), and 4 (extremely). This last question evaluates the intensity of burden in the caregiver. The total score ranges from 0 to 88 and higher scores indicate greater the caregiver burden. Cronbach’s alpha in the Brazilian version was .87. In this study, Cronbach’s alpha was .84. SF-36 - Short Form Health Survey (SF36; Ware & Sherbourne, 1992; Brazilian version by Ciconelli et al., 1999). The SF36 assesses physical and mental QOL. It is made up of 36 items in 8 scales or domains, namely functional ability, physical aspects, pain, general health status, vitality, social aspects, emotional aspects, and mental health. Scores are awarded to the 8 domains ranging from 0 to 100, where 0 = worst and 100 = best, for each domain. Thus, the higher the score the better the quality of life. Cronbach’s alpha in the Brazilian version for all items was over .90. The Physical component (general health, functional health, ability, body pain, physical function) showed a Cronbach’s alpha of .68 and the Mental component (vitality, emotional aspects, social conditions), a Cronbach’s alpha of .76. Career’s Assessment of Managing Index (CAMI; Nolan et al., 1995; Portuguese version by Brito, 2000): This instrument assesses coping strategies used by the caregivers and includes 38 items grouped into three subscales: 1, “dealing with situations/problem solving”, 2, “alternative perceptions of the situation”, and 3, “dealing with stress symptoms”. The 38 items are scored from 0 to 3: 0 (no use), 1 (use/no result), 2 (use/gives some result), and 3, (use/gives good result). High results indicate greater use of more effective coping strategies. In the original version, Cronbach’s alpha was .84, .80, and .37, respectively, for the three subscales, and .90 for the total scale. In the Portuguese version, Cronbach’s alpha for the total CAMI was .80 and for the subscales .75, .62, and .60. In this study, an exploratory factor analysis was performed for the Brazilian population. The Brazilian version has one less item (27) than the original version and has 2 domains: one with 25 items and another with 14 items, totalising 37 items. Both domains were renamed for semantic adequacy to the content. Cronbach’s alpha was .78 for Alternative’s perceptions/Dealing with situations in the domain with 25 items and .67 for the Problem Resolution domain. The alpha for the global scale was .82. Hospital Anxiety and Depression Scale (HADS; Zigmond & Snaith, 1983; Brazilian version by Botega et al., 1995). This instrument has 14 items grouped into two subscales, anxiety and depression, with seven items each to evaluate depression and anxiety. Each item can be scored from 0 to 3, adding up to a maximum score of 21 points for each scale (anxiety and depression). The cutoff points for HADS anxiety in the Brazilian version are 0 to 8 - no anxiety, and ≥ 9 anxiety and for HADS depression, the cutoff points are 0 to 8 no depression, and ≥ 9 for depression. In the Brazilian version, Cronbach’s alpha for depression subscale was .77 and for anxiety subscale was .68. In this study, the Cronbach’s alpha for the anxiety subscale was .70, for depression subscale .55, and the global scale was .73. In this study, only the global scale and the anxiety sub-scale were used. Spiritual and Religion Attitudes in Dealing with Illness (SpREUK; Bussing, 2010; Brazilian version by Pereira et al., 2019). This instrument has 15 items divided into three subscales: 1-Seeking support/access, 2-Confidence in a superior orientation/source, 3-Reflection and positive interpretation of the disease. SpREUK items are scored in five points scale from disagreement to agreement, 0 (not applicable at all), 1 (not really applicable), 2 (I do not know - neither yes nor no), 3 (little applicable), and 4 (applies a lot). Scores can be referred to a 100% level (transformed scale score). Scores > 50% indicate greater agreement (positive attitude), while scores < 50% indicate disagreement (negative attitude). Higher results indicate greater use of spirituality. The original version of this instrument showed Cronbach’s alphas ranging from .86 to .91. In the Portuguese version, Cronbach alphas vary between .81 and .86. This instrument was used for the first time with the Brazilian population and the Brazilian validation has one less item (4). The adapted Brazilian version differs from the original instrument and includes two subscales and 14 items. The two subscales have been renamed for semantic adaptation. The “spiritual support” subscale has 9 items and the “reflection and positive interpretation of the disease” subscale has 5 items (26). Confirmatory factor analysis showed the following results: χ2 = 103.82, df = 76, CFI = .976, TLI = .971, RMSEA = .056, RMSEA 90% CI = .081. In this instrument, Cronbach’s alpha for the spiritual support subscale was .72 and for the reflection and positive interpretation of the disease subscale it was .72. Cronbach’s alpha for the global instrument was .81. Data Collection Data collection took place from August 2017 to October 2018. Caregivers were interviewed separately in an office while they waited for patients’ consultations at the Chemotherapy and Radiotherapy Outpatient Clinic at FCECON. Participation in the study was voluntary and all participants signed an informed consent form before participating in the study. The study was approved by the ethical committee of the hospital. The consent form was read to the illiterate and fingerprints were collected upon agreement. Caregivers who met the inclusion criteria were randomly selected by patients’ medical records on alternate days of the week during radiotherapy/chemotherapy sessions. The study was approved by the FCECON Teaching and Research Committee and by the National Research Ethics Committee, Brazil (CAAE no.68816417.0.0000.5020). Data Analysis Data analysis was performed using IBM SPSS® (Statistical Package for the Social Sciences), version 26.0. Descriptive statistics were used to describe the sociodemographic characteristics of the sample (mean, standard deviation, frequencies, and percentages). The Pearson’s correlation test was used to assess the relationship between sociodemographic and psychological variables. Linear multiple regression was used to evaluate the contribution of the variables that best explained QOL: the dependent variable was QOL and the predictive variables were burden, coping, spirituality, anxiety, and the sociodemographic variables correlated with physical and mental QoL. Demographic variables were included in step 1, followed by psychological variables in step 2. Multicollinearity was tested in the two models, and VIF values were well below 10 and the tolerance statistics all well above 0.2 (Field, 2009). The variable gender was categorized as 1 for female and 0 for male. The moderating role of spirituality in the relationship between anxiety and mental/physical QOL was assessed using Macro Process command for SPSS version 26 and the Johnson-Neyman technique (JN), since all the assumptions for moderation were met. Sample Characteristics The sample consists of 119 caregivers of patient undergoing chemotherapy/radiotherapy for cervical cancer at FCECON. The average age of informal caregivers was 37.1 (SD ± 12.2); 70% of the caregivers were female, 78.2% declared to be grayish-brown, and 63% lived in the capital of the state of Amazonas, Manaus. Regarding marital status, 55.6% of caregivers were married. Most caregivers attended school for 9 years or more (58.8%) and 63.9% were unemployed. The family income of 69% of the caregivers was 2 Brazilian minimum wages ($368 USD monthly income). In this study, 68.9% of the caregivers were family members and 59.7% spent between 18 to 24 hours/day taking care of the patient (Table 1). Table 1 Sample Sociodemographic Characteristics ( N = 119) 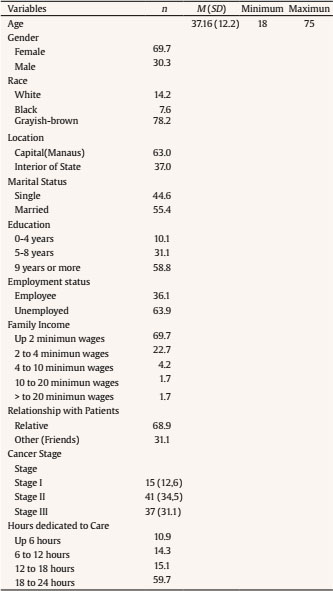 Relationship between Sociodemographic, Psychological Variables, and QOL The results showed an association between being a male caregiver and burden (negative association indicates male gender). There was also an association between being a female (positive association indicates female gender) and the use of spirituality (reflection and positive interpretation of the disease). There was an association between education (number of years) and coping strategies, in which caregivers with higher education reported better coping strategies. Caregivers’ family income was negatively associated with coping strategies, i.e., caregivers with higher family income showed worse coping strategies. Table 2 presents the sociodemographic and psychological variables and their association with mental and physical QOL. Table 2 Correlations between Sociodemographic and Psychological Variables (N =119) 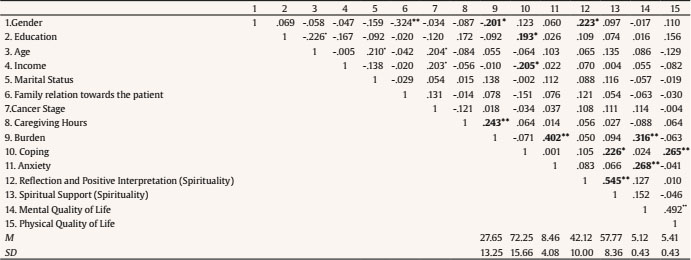 *p < .01, **p < .001. Number of caregiving hours showed a positive correlation with burden, indicating that the more time dedicated to care, the greater the burden. Burden had a positive association with anxiety and was negatively associated with the caregivers’ mental QOL, and so the higher the burden the greater the symptons of anxiety and worse the mental QOL (Table 2). The use of spirituality (reflection and positive interpretation of the disease) was associated with better coping strategies. Poor caregivers’ mental QOL showed a positive relationship with more symptoms of anxiety. Finally, better physical QOL was associated with better mental QOL and more effective coping strategies (Table 2). Variables that Contributed to QOL In the model that tested psychological variables that contributed to caregivers’ mental QOL, burden (r = -.316, p < .01) and anxiety (r = -.268, p < .01) were included as they were significantly correlated with mental QOL (Table 2). The results showed that the regression model was statistically significant and explained 12% of the variance, R2 = .12, F(2, 116) = 8.188, p < .01, but only burden (β = -.249, t = - 2.62, p < .00) was associated with mental QOL (Table 3). Since only coping contributed to physical QOL, regression analysis could not be performed. Table 3 Variables that contribute to Mental Quality of Life 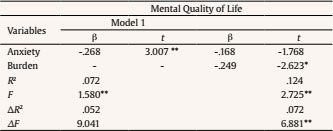 *p < .01, **p < .001. Regarding the moderating role of spirituality (reflection and positive interpretation of the disease) in the relationship between anxiety and caregiver’s mental QOL, the model was significant, F(3, 115) = 5.93, p < .00, β = -.23, 95% CI [ -.44, -. 03], t = .02, p < .05, explaining 11% of the variance. Thus, low spirituality (reflection and positive interpretation of the disease) had a negative relationship with anxiety and mental QOL, β = - 3.84, 95% CI [-.44, -. 03], t = 4.02, p < .01. The Johnson-Neyman technique (JN) revealed that anxiety was negatively correlated with mental QOL when the standardized value of spirituality (reflection and positive interpretation of the disease) was 40.98 below the mean (β = -1.98, p = .05) and this happened in 33% of the sample of caregivers (Figure 1) Figure 1 The Moderating effect of Spirituality (Reflection and Positive Interpretation of Disease and Spiritual Support) in the Relationship between Anxiety and Mental Quality of Life. 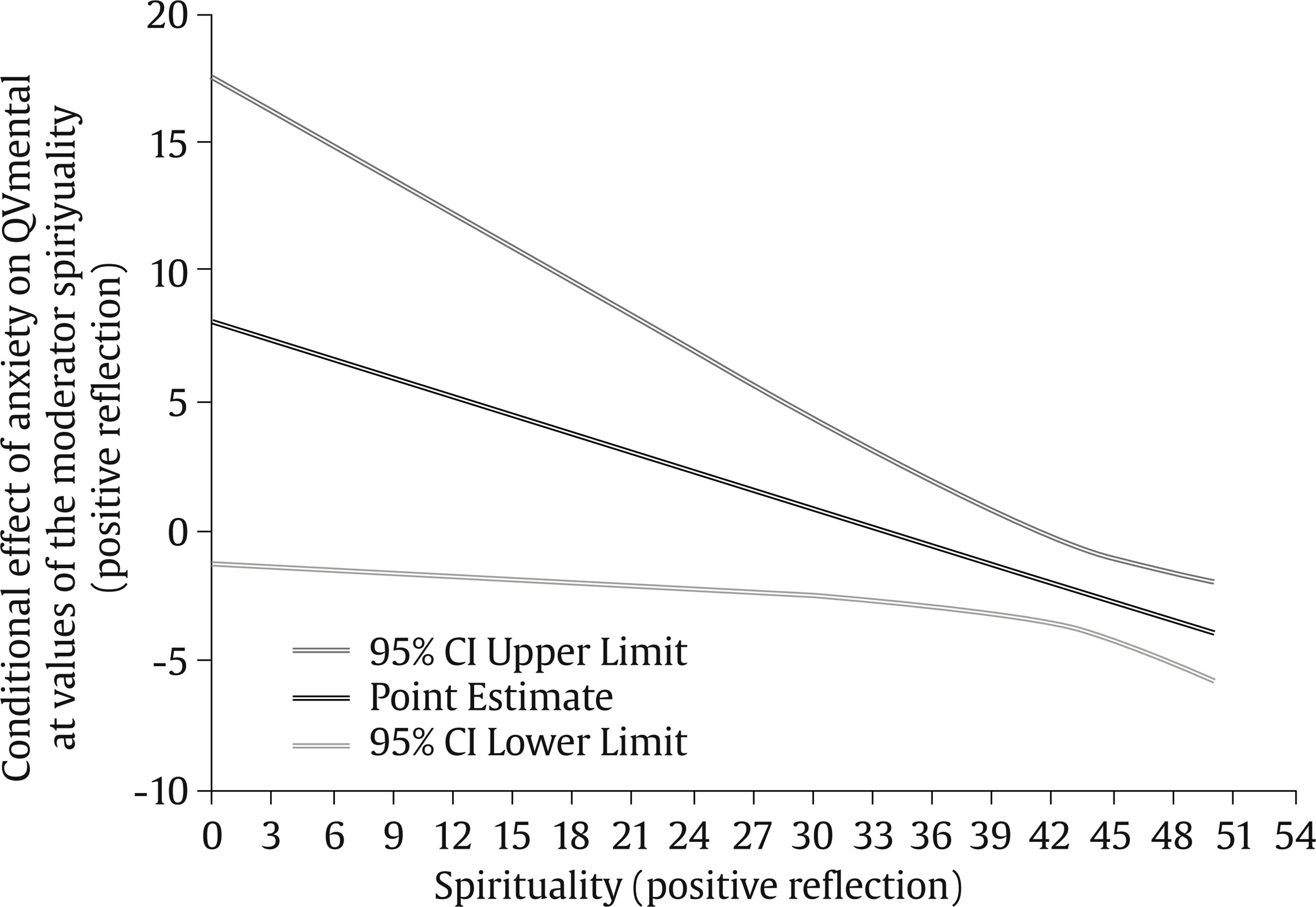 Finally, the moderating role of spirituality (spiritual support) in the relationship between anxiety and mental QOL (β = .41, p = .34) was not significant. The literature shows that caregivers of cancer patients are mostly female, a profile confirmed in the present study. The social role of women is almost a historical-cultural “pre-determination”, in which they assume the home and hospital care of a family member when they fall ill (Surbone et al., 2010; Swinkels et al., 2019; Ugalde et al., 2019). Other studies also reinforce that most informal caregivers in Brazil are married and have about nine years of education and a family income of 2 Brazilian minimum wages. Informal caregivers have jobs and patient care is considered a “second shift”, contrary to the findings in our study which shows that 63.9% were unemployed and 59.7% spent more than 18 hours on patient care (Coppetti et al., 2019; Gayoso et al., 2018). In this study, being a male was associated with more symptoms of burden compared to women. This result differs from the literature, which describes greater burden on female caregivers. A recent study reports that the burden of male caregivers may be directly influenced by the advanced stage of the patient’s disease, which is characterized by a decrease in a patient’s functionality and a greater demand for caregiving, in addition to the uncertainty of the duration of such caregiving (Govina et al.2019). However, the literature reinforces that the association between gender and burden cannot be analyzed in isolation, since the evaluation of burden is subjective and has to be analyzed with other underlying factors, such as financial and emotional issues, workload and hours dedicated to care (Coppetti et al., 2019; Swinkels et al., 2019). The resuts need to be replicated in future studies that include a similar number of male and female caregivers, and shoud therefore, be interpreted caustiously. In the present study, being a female caregiver was associated with greater use of spirituality (reflection and positive interpretation of the disease) than a male caregiver, corroborating the literature that describes the female gender as a variable strongly associated with greater spirituality in informal caregivers. This result is important because spirituality is considered a coping strategy with a great impact on reducing caregivers’ psychological symptoms, such as psychological morbidity (anxiety) and burden (Lai et al., 2018; Teskereci & Kulakaç, 2018). When analyzing caregiver education, the higher level of education and lower income were associated with the use of better coping strategies. This result corroborates the study by Coppetti et al (2019), which showed that caregivers with more education had better coping strategies, resulting in better caring skills. Studies with Brazilian samples that analyzed the relationship between low family income and coping strategies revealed that individuals from low-income families have a greater capacity to use coping strategies, since they already deal with poor socioeconomic conditions as the main stressor. Brazilian studies show that patients use more direct strategies, acting and seeking change with greater capacity to adapt to new situations and directly facing problems, as found in the present study (Albuquerque et al., 2008; Nepomuceno et al., 2016). Several studies have shown that more hours dedicated to patient care are associated with greater caregiver burden, and that caregivers with more symptoms of burden also have more psychological morbidity (anxiety) and, consequently, worse mental QOL, thus corroborating the results of this study (Muliira etal., 2019; Teskereci & Kulakaç, 2018; Ugalde et al., 2019). The results of the present study clearly show the challenge of the informal caregiver in the Amazonia state, whose routine, for the most part, is dedicated exclusively to patients reinforcing the need for programs to use an interprofessional approach to monitor and provide psychological support for caregivers. The effectiveness of several types of interventions (psychological, behavioral, informative) with caregivers of cancer patients are shown to have a positive impact in reducing psychological symptoms (Ugalde et al., 2019). The importance of coping strategies to deal with psychological symptoms and the association of spirituality as a strategy for strengthening coping are widely described in the literature (Teskereci & Kulakaç, 2018). Other studies also confirm that the new challenge is to educate and qualify interprofessional oncology teams in order to offer psychological assistance to informal caregivers, taking into account the “screening of the spiritual history” and adding this data to clinical practice (Lambert et al., 2017; Santos et al., 2019; Siler et al., 2019). Thus, the results of the present study reinforce that interprofessional education has to be integrated and interdisciplinary, seeking to qualify professionals to deal with the complexity of the psychological, social, and family context of chronic illness in order to strengthen the coping strategies of caregivers, such as spirituality. In this study, anxiety was related with worse mental QOL and burden was the psychological variable with the greatest impact on informal caregivers’ mental QOL. These results are similar to those found in the literature which show that better mental QOL is related to fewer psychological symptoms (Muliira et al. 2019; Teskereci & Kulakaç, 2018). However, the influence of burden on mental QOL suggests the need to conceive strategies to reduce the burden on informal caregivers. Studies have shown effective results of educational, psychosocial, and psychoeducational interventions to prevent and reduce caregiver burden (França et al., 2020). More effective coping strategies have been associated with greater physical QOL, as evidenced in the literature and in the present study (Albuquerque et al., 2008; Muliira et al., 2019). However, coping strategies did not contribute to physical QOL, suggesting their importance on caregives’ psychological rather than physical symptoms, impacting therefore mental QOL. Future studies should analyze the contribution of coping strategies to physical QOL, taking into consideration caregivers’ sociodemographic variables but also patient’s functionality. Caregivers’ spirituality (reflection and positive interpretation of the disease) moderated the relationship between anxiety and mental QOL, showing that caregivers that used more reflection and positive interpretation reported a reduction in anxiety symptoms and better mental QOL. Studies on spirituality and caregivers of cancer patients reiterate these results and show the importance of spirituality as a coping strategy in caring for the chronically ill (Lalani et al., 2018; Teskereci & Kulakaç, 2018). Given that the assessment of QOL, as well as of spirituality, are complex with subjective, individual and dynamic characteristics, further longitudinal studies are needed to assess these two variables, by monitoring the caregiver for a longer period of time during the evolution of cancer and patients’ care (Lambert et al., 2017; Muliira et al., 2019; Ugalde et al., 2019). Limitations This study used a cross-sectional design that does not allow causal inferences, a modest sample size and used only self-report questionnaires. Therefore, future studies should replicate the findings in bigger samples and use longitudinal designs to study the variables that contribute to caregivers’ QOL, over time, as patients’ disease progresses. The results show that coping strategies were associated with better physical and mental QOL. Burden was the psychological variable with the greatest impact on mental QOL showing the importance of interprofessional teams in to include also behavioral health professionals that help caregivers decrease their burden and psychological morbidity (anxiety) in order to improve QOL. Clinical Implications The findings of this study underline the need to develop intervention programs for informal caregivers of Amazonian women with cervical cancer, focusing on psychological morbidity in order to prevent and reduce burden as well as emphasizing the use of spirituality as a coping strategy. According to the results, there is a need for interprofessional teams in oncology settings to assess and intervene the patient-caregiver dyad, in order to decrease caregiver burden, and indirectly promote a patient’s adjustment to CC. Conflict of Interest The authors of this article declare no conflict of interest. Acknowledgements The authors would like to thank the study participants and all the collaborators who contributed to data collection the FCECON. Cite this article as: Moysés, R., Santos, B. D., Benzaken, A., & Pereira, M. G. (2022). Quality of life of informal caregivers of cervical cancer patients: Analysis of anxiety and spirituality. Clínica y Salud, 33(2), 65-71. https://doi.org/10.5093/clysa2022a6 References |
Cite this article as: Moysés, R., Santos, B. D., Benzaken, A., and Pereira, M. G. (2022). Quality of Life of Informal Caregivers of Cervical Cancer Patients: Analysis of Anxiety and Spirituality. ClĂnica y Salud, 33(2), 65 - 71. https://doi.org/10.5093/clysa2022a6
gracep@psi.uminho.pt Correspondence: gracep@psi.uminho.pt (M. Graça Pereira).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
Clinical and Health is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License








