


Variables Associated with Abandonment, Permanence, or Clinical Discharge from a Suicide Risk Attention Program
[Las variables asociadas con el abandono, la permanencia o el alta clínica en un programa de atención al riesgo de suicidio]
Laura T. Rodríguez Hernández1, María del C. Caballero Guzmán2, Mike Murphy3, Raquel Tierno Patiño2, and Juan José Fernández Muñoz1
1Rey Juan Carlos University, Alcorcón, Madrid, Spain; 2University Hospital José Germain, Leganés, Madrid; 3University College Cork, Ireland
https://doi.org/10.5093/clysa2024a15
Received 29 January 2024, Accepted 6 May 2024
Abstract
Background: Suicidal behavior is a public health problem whose incidence has increased recently. The Suicide Risk Attention Program (ARSUIC) is developed for the detection and prevention of suicidal behavior. The data obtained allow us to study suicidal behavior. The aim of this study is to analyze predictive variables of clinical outcomes. MethodA quantitative and associate design with a retrospective viewpoint was carried out. Data from 459 adults, children, and adolescents referred to the ARSUIC program from 2018 to 2022 were collected. The analysis was conducted using SPSS and R. ResultsThe number of appointments, social support, and attempted suicide explain the abandonment of the program; the number of appointments, psychiatric history, and suicide attempts the permanence in the program; and finally, clinical discharge was explained by the number of appointments, a psychiatric personal history, social support, and past psychological violence. ConclusionsThis is the first study analyzing predictive variables of outcomes in the ARSUIC program. Increasing our knowledge about this is necessary to improve clinical interventions and reduce dropouts.
Resumen
IntroducciónEl comportamiento suicida es un problema de salud pública cuya incidencia ha aumentado recientemente. El Programa de Atención al Riesgo de Suicidio (ARSUIC) ha sido desarrollado para la detección y prevención del comportamiento suicida. Los datos obtenidos permiten estudiar el comportamiento suicida. El objetivo de este estudio es analizar las variables predictoras de los resultados clínicos del programa. MétodoSe realizó un diseño cuantitativo y asociativo con una perspectiva retrospectiva. Se recopilaron datos de 459 adultos, niños y adolescentes referidos al programa ARSUIC desde 2018 hasta 2022. El análisis se llevó a cabo utilizando SPSS y R. ResultadosEl número de sesiones, el apoyo social y el intento de suicidio explican el abandono del programa; el número de sesiones, el historial psiquiátrico y los intentos de suicidio la permanencia en el programa; finalmente, el alta clínica fue explicado por el número de sesiones, un historial psiquiátrico personal, apoyo social y violencia psicológica pasada. ConclusionesEste es el primer trabajo que trata de analizar variables predictoras de resultados en el programa ARSUIC. Aumentar nuestro conocimiento sobre este tema es necesario para mejorar las intervenciones clínicas y disminuir el abandono del programa.
Palabras clave
Suicidio, Violencia, Programa de atención al riesgo de suicidio, Prevención, Alta clínica
Keywords
Suicide, Violence, Suicide risk attention program, Prevention, Clinical discharge
Cite this article as: Hernández, L. T. R., Guzmán, M. D. C. C., Murphy, M., Patiño, R. T., & Muñoz, J. J. F. (2024). Variables Associated with Abandonment, Permanence, or Clinical Discharge from a Suicide Risk Attention Program. Clínica y Salud, 35(3), 111 - 118. https://doi.org/10.5093/clysa2024a15
Funding: This study was supported by the following research grant from the Spanish Ministry of Science and Innovation: XMIDAS (ref. PID2021-122640OB-I00).
Correspondence: lt.rodriguezh@alumnos.urjc.es (L. T. Rodríguez Hernández).
Suicidal behavior is a public health problem of great importance nowadays, with a lot of associated direct and indirect costs, as well as a progressively increasing incidence worldwide (Turecki et al., 2019). It is considered a highly complex phenomenon, with difficulties in reaching a consensus regarding its definition in current literature (Al-Halabí & Fonseca, 2023). It is defined as “a variety of manifestations, ranging from ideation and planning, through suicidal communication to suicidal attempts and completed suicide” (Al-Halabí & Fonseca, 2021). Also, the term “deliberate self-harm behavior (DSH)” covers suicidal behavior, non-suicidal self-injury (NSSI), and other self-harm behaviors of ambiguous intentionality (Al-Halabí & Fonseca, 2023). The World Health Organization (WHO, 2019) estimates around 700,000 deaths by suicide per year globally. In Spain, the suicide rate has increased progressively in recent years. Eight out of every 100,000 inhabitants died by suicide in 2020, making a total of 3,941 deaths (7.3% more than in 2019) (Ministerio de Sanidad, 2020). In 2021 this figure increased by 1.6%, with 4,003 deaths (2,982 men and 1,021 women), considered the leading non-physical-illness-related cause of death in Spain. In 2022, statistics mention an increase of 5.6% compared to 2021, with 4,227 deaths by suicide (3,126 males and 1,101 females). Data from the first half of 2023 point out that suicide continues to be the leading cause of external death with 1,967 deaths (75.2% males and 24.8% females) (INE, 2023). It is estimated that these figures are even higher, since in the statistics there are inaccuracies regarding the cause of death as the motivation of the person is not objectively known, so there could be deaths considered accidental where there was a desire to die (Snowdon & Choi, 2020). According to Huertas-Maestre (2022), non-lethal suicidal behavior prevalence in Europe is around 3.96% (1.53% wish of death, 5.28% suicidal ideation and 0.63% suicide attempt). Meanwhile, in Spain the prevalence in 2019 was 7.7 per 100,000 persons (WHO, 2019). Suicidal behavior is considered a complex, multifactorial, and multidimensional phenomenon involving a mix of sociocultural, biological, and psychological factors (Al-Halabí & Fonseca, 2021). In this line, O’Connor and Nock (2014) point out personality and individual differences, social and cognitive factors, and negative life events as key factors that contribute to its appearance. In fact, in a meta-analysis of 50 years of research about risk factors of suicidal thoughts and behaviors (Franklin et al., 2017) there were no risk factors found that allow them to predict suicidal behavior. From 2010-2014, a Suicide Risk Attention Program (ARSUIC) was set up in Madrid Region, with the aim of guaranteeing continuity of care for patients at risk of suicide, ensuring an outpatient follow-up appointment at the Mental Health Center of their district (Consejería de Sanidad, 2023). The program focuses on reducing the risk of new suicide attempts as much as possible in a period considered to be of maximum vulnerability for patients (Jiménez-Sola et al., 2019). The ARSUIC Program is considered an individualized treatment that fits a patient’s needs. Once patients come to the emergency room at the hospital due to suicidal behavior they are treated by psychiatrists who prescribe medicines or hospital admission in Psychiatry if necessary. After their stabilization, they are referred to the Mental Health Center through the ARSUIC Program, with an appointment in a maximum of 7 days. After that appointment, the professional together with the patient decides which intervention may be the most beneficial: pharmacological and/or psychotherapeutic interventions, individual or group therapy, or socio-family approaches, in collaboration with a multidisciplinary team that works in the Unit (psychiatrists, clinical psychologists, nurses, and social workers). Even though the ARSUIC suicide prevention program was implemented in Madrid Region between 2010 and 2014, there is hardly any literature about it. The profile of patients attended, its results regarding prevention rates of suicide ideation or attempts, possible risk factors, or those associated with clinical discharge due to improvement or discontinuation of follow-up have not been studied in depth. There are variables associated with clinical discharge, dropout, or permanence in treatment in people with suicidal behaviors. According to Hom and Joiner (2016), overall functioning and substance use disorder are factors associated with dropouts in outpatients with clinically significant suicidal ideation, as well as depressive symptoms, comorbid diagnosis, and severe suicidal symptoms. Other studies have focused on aspects that professionals could improve in order to increase treatment adherence, observing that developing brief interventions in the emergency room as well as implementing group interventions for adolescents would help the patient keep a long-term follow-up (Lizardi & Stanley, 2010). Promoting greater flexibility and commitment of the therapist, generating a good therapeutic adherence, makes it easier for the patient to maintain treatment (Gibbons et al., 2010). The therapeutic alliance, as well as the emotional validation and active engagement of the patient in the treatment, have been noticed to be significant factors associated with therapeutic success in persons with suicidal behaviors (Michel, 2021). A robust therapeutic alliance reported since the beginning of psychotherapy is associated with a significant reduction of suicidal behaviors in the future (Huggett et al., 2022). Likewise, it is considered an important factor for clinical success, impacting positively on the treatment and being related to a decrease in suicidal ideation in at risk patients (Fartacek et al., 2023). There is a high probability of a new onset of suicidal behavior after hospital discharge, which makes it important the care on an outpatient bias (Forte et al., 2019). However, low compliance is frequent in this population. This fact increases the possibility of new episodes and long-term comorbidity with other psychiatric disorders, making it difficult to address and requiring more psychiatric interventions in the future (Groholt & Ekeberg, 2009). The complexity and heterogeneity associated with this population make further research necessary to increase our knowledge about the factors related to therapeutic effectiveness in order to optimize interventions in patients at risk (Michel, 2021). The data obtained through the ARSUIC program allow us to learn more about the variables associated with suicidal behavior, increasing the understanding of this phenomenon and the implementation of prevention strategies that may reduce current mortality rates in this population. The present study aimed initially to explore the relationship between suicidal ideation and suicide attempts. Our secondary aim was to analyze if suicide attempt, number of appointments, social support, presence of psychiatric personal history, and psychological violence are associated with clinical discharge, dropout, or permanence in the ARSUIC program. These objectives have been operationalized through the following research hypotheses: H1: There will be a significant relationship between suicide attempts and suicidal ideation. H2: Suicide attempt, number of appointments, social support, presence of psychiatric personal history, and psychological violence are variables that will be associated with abandonment, permanence, or clinical discharge from the ARSUIC program. Participants A total of 459 people were recruited from an initial sample of 519 referred from a Mental Health Center in Madrid Region through the ARSUIC program during the last four years (2018-2022). The patients were treated by the psychiatry service of the reference hospital due to suicide ideation and/or suicide attempt within a maximum period of 7 days after discharge. The following exclusion criteria were established: population referred from the reference hospital not been included in the ARSUIC program and population referred to the Mental Health Center through Primary Care. Taking this into account, as well as repeated data in the reviewed records, 60 people were excluded, with 459 included in the final sample. All the patients recruited in this sample were clinical population that presented suicidal ideation and/or suicide attempt when they were attended by the service of psychiatry in the emergency room. Some patients required psychiatric hospitalization and subsequently were referred to the Mental Health Center, while other patients were discharged after the hospital visit with a similar referral appointment. Instruments Clinical records of patients referred to the ARSUIC program were collected using Selene, a software used by clinicians for specialized attention in hospitals and medical centers. It is a widely used tool for mental health professionals in Spain to manage care processes (Vigueras-Paredes & Hernández-Contreras, 2017). Patients’ health assessment was carried out through a semi-structured clinical interview. The reason for consultation, current illness, relevant biographical factors, personal and family medical and psychiatric history, current and historical substance use, and current treatment are collected in the adult population. In the case of children and adolescents, in addition to the above, it also includes academic and family member information. During the follow-ups, the progress of the patient is assessed through an unstructured clinical interview. The following sociodemographic variables were collected: participants’ age, whether the patient was an adult or a child/adolescent, year of referral, social support, number of appointments after referral to the Mental Health Center, and outcome (abandonment, permanence, or clinical discharge). Regarding clinical variables, the following were measured: presence of suicide ideation, suicide attempt, psychological violence in the past, and personal psychiatric history. Procedure Permission from the José Germain University Hospital Research Unit was requested to access the clinical data. Subsequently, this information was sought from the Admission, Information and Patient Care Service of this hospital, giving the researchers data on patients treated in the ARSUIC program between 2018 and 2022. The collection and elaboration of data took place from institutional computers through VPN (Virtual Private Network) access. The data were pseudonymized. Exemption from the requirement to obtain patient consent was granted since the researchers worked with retrospective data collected from clinical engagement and never with the patients themselves. This study was approved by the Ethics Committee of the Severo Ochoa University Hospital on May 31th 2023, Acta 05/23. The study complied with the provisions of the General Data Protection Regulation (EU Regulation 2016/679, of 27th April 2016 of the European Parliament and of the Council, about the protection of natural persons with regard to the treatment of personal data and the free circulation of them) and Organic Law 3/2018, of December 5th, on Protection of Personal Data and Guarantee of Digital Rights, as well as the concordant European and Spanish regulations. Information was gathered from the clinical histories and records from appointments to the Mental Health Center during those years. A retrospective descriptive and exploratory analysis was carried out using clinical records from Selene. To extract all the necessary data, two researchers (MCGC and LTRH) accessed the clinical data. Data Analysis To achieve the proposed objectives several statistical procedures were conducted through the software SPSS 27.0 (IBM Corp. 2020) and R (R Development Core Team, 2008): descriptive and frequency analysis of clinical and sociodemographic variables previously mentioned and crosstab tables analysis and chi-square contrast to look into the relationship between suicide attempt and suicidal ideation. The predictive models were developed with three binary logistic models, known also as “logit” (Long, 1997). In this regard, the authors made use of the “glm” function, in which the binomial particularity of the dependent variables is specified as a parameter (family = “binomial”). The main purpose was to determine if clinical history variables could explain ARSUIC program abandonment, permanence, or clinical discharge. Before that, the polytomous variables called “outcome” were divided into three dichotomous variables: abandonment, permanence, and medical discharge. In such a model, the probability of success is given by P(Y = 1) whereas the probability of fail P(Y = 0) equals 1-P(Y = 1). In the case at hand, the hypothesis is that X1, X2, and Xn (suicidal attempt, suicidal ideation, or clinical history) are variables influencing the dependent variable (Y); therefore, the logistic regression model performs the ratio of success of fail for each dependent variables through its natural logarithm: Logit P = α + β1X1 + β2X2 + β3X3 + βnXn. Of the 459 participants, 38 (8.3%) did not attend the first appointment and 109 (23.7%) attended only the evaluation interview. Of the 459 people recruited, 410 (89.3%) were adults and 49 (10.7%) were children or adolescents (M = 41.06, SD =18.86, age range = 10-93). Regarding gender, 262 (57.1%) were females and 197 (42.9%) were males. Table 1 describes the number of patients by year who participated in the ARSUIC program, describing age and sex variables. Table 1 Descriptive Information about Age and Sex of Patients by Year in the ARSUIC Program 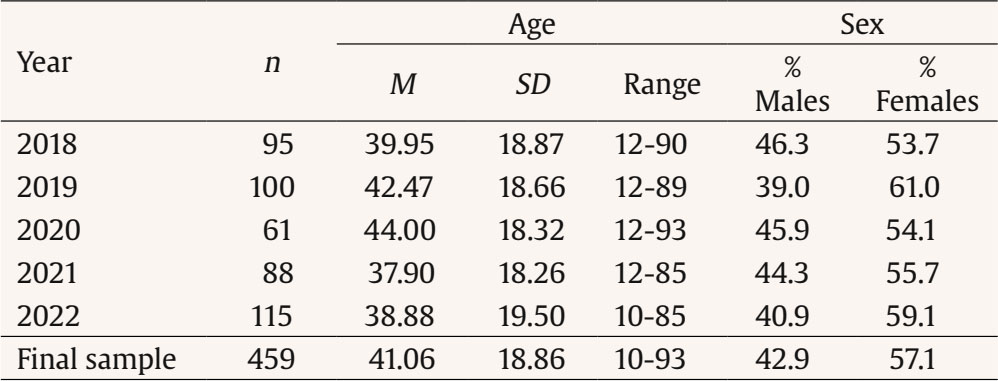 As it can be observed in Table 2, of the 459 participants 344 (74.9%) present suicide ideation and 265 (57.7%) suicide attempts, 284 (61.9%) psychiatric personal history, and 160 (34.9%) a history of psychological violence in the past. Regarding the outcomes in the ARSUIC program, 287 (62.5%) patients dropped out treatment, 73 (15.9%) maintained it, and 99 (21.6%) were clinically discharged. Table 2 Descriptive Information about Suicidal Behaviors, Psychiatric and Violence Histories, and Outcome  Table 3 Relationship between Suicidal Ideation and Suicide Attempt  Table 4 Logit Regression for Abandonment, Permanence, and Medical Discharge in the ARSUIC Program 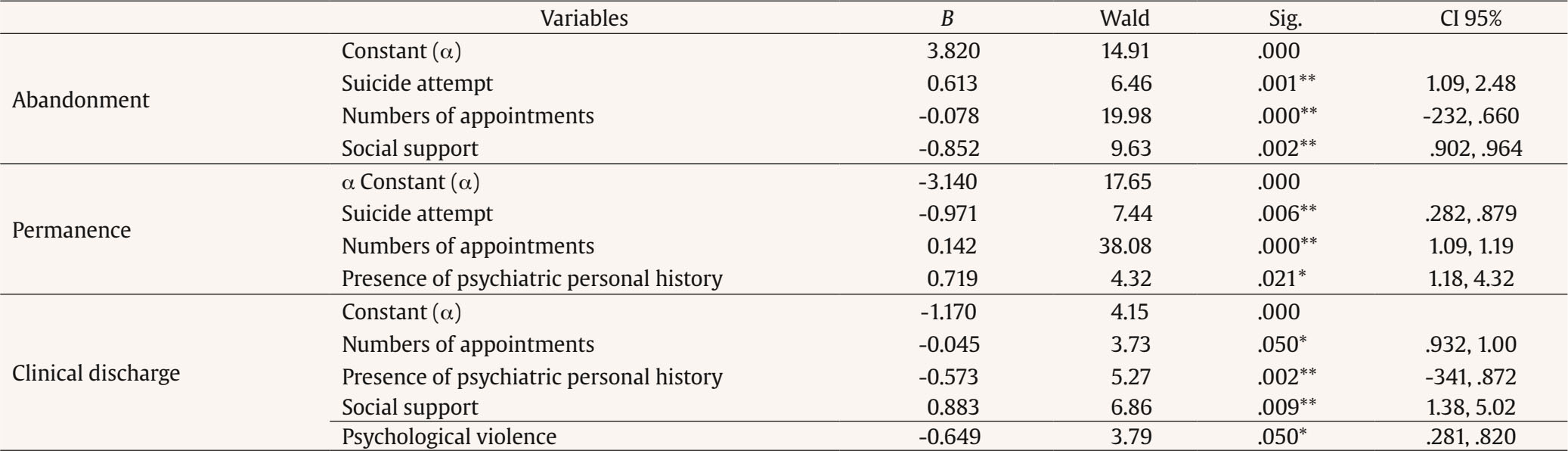 Note. Nagelkerke R2 for abandonment = .169; Nagelkerke R2 for permanence = .294; Nagelkerke R2 for medical discharge = .146. * p < .05, ** p < .01. Table 3 shows a significant relationship between suicidal ideation and suicide attempt (χ2 = 79.59, p < .01; C = .395, p < .01). On the one hand, from the total of patients without a previous suicide attempt, 99.4% had developed suicidal ideation; on the other hand, from the total of patients with a suicide attempt (262), 63.7% had developed suicidal ideation and 36.3% had not developed suicidal ideation. Table 4 describes the output of the logistic regression for the three dependent variables (abandonment, permanence, and clinical discharge). For the first dependent variable (abandonment), suicide attempt (B = 0.613, W = 6.46, p < .01) was positive and significantly different from zero meanwhile number of appointments (B = -0.078, W = 19.98, p < .01) and social support (B = -0.852, W = 9.63, p < .01) were negative and significantly different from zero. This means that these variables have a positive and negative impact on the probability of leaving (abandonment) the ARSUIC program. Nagelkerke’s R2 index was .169. For the second dependent variable (permanence), suicide attempt (B = -0.971, W = 7.44, p < .01) was negative and significantly different from zero; number of appointments (B = 0.142, W = 38.08, p < .01) and presence of psychiatric previous history (B = 0.719, W = 4.32, p< .05) were positive and significantly different from zero. Suicide attempt (-), number of appointments (+), and presence of psychiatric personal history (+) have an impact on the probability of continuing with the treatment in the ARSUIC program. Nagelkerke’s R2 index was .294. Finally, for the third variable, the number of appointments (B = -0.045, W = 3.73, p < .05) and presence of psychiatric personal history (B = -0.573, W = 5.27, p < .01) and psychological violence in the past (^ = -0.649, W = 3.79, ^ < .05) were negative and significantly different from zero; and social support (B = 0.883, W = 6.86, p < .01) was positive and statistically significant. Nagelkerke’s R2 index was .146. The main objective of this research was to explore the relationship between suicidal ideation and suicidal attempt. There is a significant positive association between these phenomena, something already observed in the literature in different populations (Klonsky et al., 2016). As Rubio et al. (2020) showed, suicide ideation works as a mediator between negative affect and suicide attempts in adolescents. According to Turecki et al. (2019), the risk of suicide attempts is greater depending on the content and frequency of suicidal ideation (hopelessness, ambivalence, structured plan, among others). Mental disorders are commonly related to self-injury and suicide phenomena. Clinical conditions related to distress and disrupted impulsive control promote the transition from suicidal ideation to suicidal behavior, while mood disorders are more related only to suicidal ideation (Turecki et al., 2019). Klonsky et al. (2016) indicate that previous research has focused on suicidal ideation but that it is important to consider the difference between this and suicide attempts due to the higher risk of suicide in this group. In fact, in this study 36.3% of the sample had suicide attempts without recognizing previous suicide ideation. The ideation-to-action framework suggests that these cases could be explained by such mental disorders as post-traumatic stress disorder, impulsivity, access to lethal means, knowledge of lethal means, and non-suicidal self-injury (Klonsky et al., 2016). The secondary aim of this study was to analyze the association between suicide attempt, number of appointments, social support, presence of psychiatric personal history, and psychological violence in the past with abandonment, permanence, or clinical discharge in the ARSUIC program. A smaller number of appointments and a lack of social support are associated with the abandonment of treatment. There is little literature about the influence of social support on interventions for suicidal behavior. Social isolation increases vulnerability in patients with suicidal behavior, increasing the possibility of suicide (Hou et al., 2022). Also, according to LeCloux et al. (2017), family support predicts less depression in cases of suicidal behaviors. Lutz et al. (2018) observed that lower perceived social support is an important variable related to treatment dropouts in persons with suicidal behaviors. In other populations, it is also a valuable variable. In patients with obsessive-compulsive disorder, it has been seen that the bond with significant others plays an important role in maintaining long-term profits from interventions (Steketee, 1993). Something similar occurs in the case of patients with alcoholism, where social support from significant people is related to overcoming their addiction. This is because positive relationships with others improve self-esteem and self-image, positively impacting their coping strategies (Booth et al., 2009), a mechanism that could be extrapolated to persons with suicidal behavior. It is noteworthy that a large proportion of withdrawals occurred at the beginning of therapy. In fact, 8.3% did not attend even the first appointment and 23.7% attended only once. A reduced number of appointments is linked to dropouts in mental health services, so this occurs especially at the beginning of treatment (Saxon et al., 2017). The discontinuance of treatment could be related to the limited engagement, due to incongruent patient-therapist expectations about the treatment received and a poor therapeutic alliance (Anderson et al., 2018; Hardy et al., 2017). Suicide attempts are also related to treatment dropout, in comparison with suicide ideation, as considered by Hom and Joiner (2016). Suicide thoughts and behaviors can be differentiated based on suicidal intent. There are suicide plans or attempts that aim to cause death and there are suicide threats or gestures that do not have that final intention (called Non-suicidal self-injuries - NSSI; Fox et al., 2015; Robinson et al., 2022). In this latter case, these gestures serve to indicate distress to others, possibly with a view to mobilizing support for the person’s struggles (Kreitman et al., 1970). The appearance of NSSI predicts the future existence of behaviors with suicidal intentions (Voss et al., 2019), so it is important to take it into account regarding clinical interventions. Patients with NSSI may not have either the intention to die or a mental illness that requires clinical intervention. In this case, dropout may be mainly due to those whose reactive stressors cause them great anxiety, leading to NSSI as a mobilizing and communicating agent. Once the objective pursued has been achieved, the treatment would no longer make sense, leading to abandonment. When talking about the permanence of treatment, a large number of appointments, the presence of personal psychiatric history, and suicidal ideation without suicide attempts are variables that can be associated with it. On the one hand, the greater number of appointments favors a better therapeutic alliance that promotes treatment adherence. This allows to meet the therapeutic objectives, leading to clinical success and positive treatment outcomes (Baier et al., 2020; Nahum et al., 2018). Having a history of psychiatric symptoms in the past as an associated variable with maintaining treatment is something not studied nowadays, although it appears to have a certain influence on dropouts according to previous literature (Hom & Joiner, 2016). No literature was found either about the association between the continuation of treatment and having suicide ideation with no suicide attempts. Psychiatric antecedents may indicate that these persons have more signs of mental disorder. This could make clinicians more careful with them, having more appointments to ensure their wellness before deciding on clinical discharge. Also, they are more accustomed to engaging with mental health services and this facilitates maintaining follow-up appointments. On the other hand, the absence of suicide attempts may be because the patient has lower impulsive traits, and this facilitates a more reflective and structured approach to life and treatment. In addition, a previous experience in mental health service could provide either an increase or decrease in the likelihood of continuing treatment depending on how this experience was. In this case, it is important that having a history of mental illness can increase the possibility of engaging with and continuing treatment. Finally, the absence of previous personal psychiatric history, fewer appointments, adequate perceived social support, and no previous psychological violence are variables that are associated with clinical discharge from the ARSUIC program. The absence of previous mental disorders and antecedents of psychological violence might indicate a relatively minor vulnerability, increasing the chance of recovery and clinical discharge (Rivara et al., 2019; Wang et al., 2018). In addition, this would protect against possible psychopathological problems also in the future. The literature indicates the therapeutic alliance as an important variable for maintaining treatment in patients with suicidal behavior (Gibbons et al., 2010), something that could also be related to our study since more appointments favor an alliance with the therapist that promotes adherence and treatment maintenance. These aspects that concern the patient-therapist relationship are also considered important for clinical discharge (Michel, 2021). This study has the following limitations. Firstly, statistical analyses have an exploratory scope given the nature of the variables, which makes it difficult to establish cause-and-effect relationships between suicide attempt and/or suicidal ideation and the rest of the variables measured. Secondly, the sample is unbalanced in terms of the age of participants: the subset of adults is much larger than the subset of children and adolescents (89.60% vs. 10.40%). This could imply a significant bias in terms of the findings and significance of some variables included in the model. Thirdly, a significant limitation is that participants who have committed suicide are not identified, so there is no information about prevalence or its predictors and correlates, and it is also not possible to distinguish suicide completion vs. discharge or dropout. Fourthly, this program requires an appointment with mental health services within at least 7 days of urgent hospital attendance, but the time between follow-up appointments is crucial during treatment, and it has not been collected for this study. It is widely reported in the literature that a decreased frequency of appointments could be an important variable for dropouts and low therapeutic adherence. Roos and Werbart (2013) observed that a low frequency of appointments and a scant number of them were related to higher rates of dropouts. It has been shown that longer times between sessions (≥ 30 days) are connected to early dropouts in psychotherapy (Bugatti et al., 2023). Instead, fewer days between appointments lead to a greater reduction in symptoms (Sciarrino et al., 2020). Finally, data was collected before carrying out this research. An absence of information on different variables relevant to this study is possible, due to the inability of researchers to ensure that data are as complete as possible. This is the first study that tries to analyze associated variables with outcomes in the ARSUIC Suicide Risk Attention Program, currently carried out in Madrid Region. Suicidal behavior is a global public health concern, being considered the leading external cause of death in Spanish people (INE, 2022), as mentioned above. Given the increasing incidence of suicidal behavior worldwide, as well as its complexity and heterogeneity, it is of great importance to direct both interventional and research resources toward prevention strategies that impact the different areas involved in this phenomenon. In this way, it is necessary to join different strategies of universal prevention (involving the general population), selective prevention (for those with risk factors for suicidal behavior), and indicated prevention (for specific people at risk of suicidal behavior) (Al-Halabí & Fonseca, 2023). Paying attention to the existing programs for patients with suicidal behavior is necessary. Standardizing the interventions using a robust theoretical framework is crucial, as the current ones rely on the subjectivity of the healthcare professional, making it difficult to generalize the results across all hospitals that implement these programs. The role of psychotherapy is of special relevance and the need for a multidisciplinary approach in the Emergency room, with psychiatrists, clinical psychologists, and specialist nurses. Thus, a brief intervention can be carried out at the hospital in the acute moment, allowing patients to be linked to outpatient services, facilitating their long-term permanence in treatment, and reducing the risk of suicidal behaviors. Finally, it is necessary to carefully study the referral criteria for specific suicide prevention programs, as well as to structure those programs in a differentiated way based on other clinical criteria that commonly coexist with ideas of death, and that predict a greater risk of death and need for therapeutic interventions. The aim would be then to achieve an efficient use of mental health resources, reaching those who can really benefit from these interventions and reducing the risk of dropouts. Likewise, avoiding intensive interventions in populations at lower risk is an equally important objective given the risk of iatrogenicity that all treatment entails. Conflict of Interest The authors of this article declare no conflict of interest. Acknowledgments The authors thank the management of participating organizations (Rey Juan Carlos University and Mental Health Hospital José Germain) for the opportunity to carry out this study and also to acknowledge the use of their facilities and support. Cite this article as: Rodríguez Hernández, L. T., Caballero Guzmán, M. C., Murphy, M., Tierno Patiño, R., & Fernández Muñoz, J. J. (2024). Variables associated with abandonment, permanence, or clinical discharge from a suicide risk attention program. Clínica y Salud, 35(3), 111-118. https://doi.org/10.5093/clysa2024a Funding: This study was supported by the following research grant from the Spanish Ministry of Science and Innovation: XMIDAS (ref. PID2021-122640OB-I00). Highlights - There was a relationship between suicide attempt and suicidal ideation. - There have been different predictors between abandonment, permanence, or clinical discharge. - ARSUIC program should be reviewed to improve the number of clinical discharges. References |
Cite this article as: Hernández, L. T. R., Guzmán, M. D. C. C., Murphy, M., Patiño, R. T., & Muñoz, J. J. F. (2024). Variables Associated with Abandonment, Permanence, or Clinical Discharge from a Suicide Risk Attention Program. Clínica y Salud, 35(3), 111 - 118. https://doi.org/10.5093/clysa2024a15
Funding: This study was supported by the following research grant from the Spanish Ministry of Science and Innovation: XMIDAS (ref. PID2021-122640OB-I00).
Correspondence: lt.rodriguezh@alumnos.urjc.es (L. T. Rodríguez Hernández).
Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
Clinical and Health is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License








