


Quality of Life and Positive and Negative Affect in the Personality Disorder
[La calidad de vida y el afecto positivo y negativo en el trastorno de personalidad]
Juan M. Ramos, Paula M. Marco, Aintzane Sánchez, and Aurora Doll
Unidad de Trastornos de Personalidad del Hospital Dr. R. Lafora, Madrid, España
https://doi.org/10.5093/clysa2024a16
Received 19 March 2022, Accepted 24 May 2024
Abstract
Background: Recovery from psychopathology in patients with personality disorder (PD) after the therapeutic intervention is not necessarily accompanied by an increase in their quality of life. This phenomenon can be understood from a bifactorial model of affect and challenges our therapeutic design to focus on recovery. Method: In a sample of severe PD, we evaluate emotional and clinical variables before (N = 414) and after (N = 247) a 6-month intervention program. Results: The level of emotion intensity influences the association between positive and negative affect (PA and NA; p < .0001). Patients with a “self-constructive” affective profile improve more in PA than in NA ( p = .008). Conclusions: The specific promotion of PA, applied in a phase in which the person experiences less negative emotional reactivity, could improve satisfaction with life and psychosocial functioning of PD patients.
Resumen
Antecedentes: La mejoría de la psicopatología lograda tras la intervención terapéutica en pacientes con diagnóstico de trastorno de la personalidad (TP) no va acompañada necesariamente de una mejora de la calidad de vida, fenómeno que puede entenderse desde un modelo bifactorial del afecto y supone un reto a la hora de diseñar el abordaje terapéutico centrado en la recuperación. Método: En un grupo de TP grave (N = 414) evaluamos variables emocionales y clínicas antes (N = 414) y después (N = 247) de una intervención hospitalaria de 6 meses. Resultados: El nivel de intensidad emocional refuerza la asociación entre afecto positivo y negativo (AN y AP; p < .0001). Los pacientes con un perfil afectivo “autoconstructivo”mejoran más en AP que en AN (p = .008). Conclusiones: Fomentar expresamente el AP en la fase de tratamiento en la que la persona experimente una menor reactividad emocional negativa puede ayudar a aumentar la satisfacción en la vida y el funcionamiento psicosocial de los pacientes con TP.
Palabras clave
Calidad de vida, Afecto positivo, Afecto negativo, Trastorno de personalidad, Resultado del tratamiento, RecuperaciĂłn, Funcionamiento psicosocial, SatisfacciĂłn con la vidaKeywords
Quality of life, Positive affect, Negative affect, Personality disorder, Treatment outcome, Recovery, Psychosocial functioning, Satisfaction with lifeCite this article as: Ramos, J. M., Marco, P. M., Sánchez, A., & Doll, A. (2024). Quality of Life and Positive and Negative Affect in the Personality Disorder. ClĂnica y Salud, 35(3), 119 - 126. https://doi.org/10.5093/clysa2024a16
Correspondence: jmramos@cop.es (Juan M. Ramos).Symptom mitigation or recovery from psychopathological processes documented in a lot of relatively successful interventions in the field of personality disorders (Stoffers-Winterling et al., 2022) is not accompanied by a significant increase in personal satisfaction, psychosocial functioning, or quality of life (Javaras et al., 2017). This dislocation implies that harm reduction and wellness promotion are different processes. The therapeutic challenge of helping to achieve a quality life worth living continues to be pressing for clinicians, aware that symptom removal is not enough to meet patients’ needs (Grambal et al., 2017). Quality of life (QoL), a multidimensional construct that embodies subjective evaluation and objective features of wellness, is a marker of disease burden, a measure of intervention effectiveness and the touchstone for an effective, recovery-focused treatment of personality disorder (Grenyer et al., 2022; Katsakou et al., 2012). Independent living, vocational attainment, satisfying relationships, social inclusion, and a meaningful life are particularly lacking in people with personality disorder (Álvarez-Tomás et al., 2019; IsHak et al., 2013). Efforts to know the determinants of QoL in personality disorder have been made (Stefanatou et al., 2022; Thadani et al., 2022), but it still remains a matter of research and a goal for promotion (Guillén et al., 2021). Changes in affective processes are typically found in personality disorders, with alexithymia, inhibition, anxiety, stress, sensation seeking, impulsivity, anger, or depression being taken either as diagnostic criteria or as comorbid entities (Shah & Zanarini, 2018). High sensitivity to rejection and emotional self-regulation difficulties are possibly related to traumatic experiences of early attachment and increase interpersonal ineffectiveness (Chapman, 2019). Most articles published on PD select participants according to the traditional approach of discrete, categorical classifications, borderline personality disorder (BPD) being the privileged category investigated (Bateman Gunderson & Mulder, 2015). Nonetheless, a dimensional description based on the severity of the of the disturbed functioning rather than on the type of clinical presentation has been rising up, first appearing in the DSM 5 as an alternative for future development and recently claiming its full status in the ICD 11 classification, where a specification of prominent trait dimensions particularizes the general diagnosis. The complex experience of emotions, feelings, and moods constitutes a basic aspect of personality that the psychological tradition has tried to organize and systematize with different models that support and expand a dimensional perspective. Personality traits develop from the emotional profile of the infant (Plutchik, 1980). Emotions generate health and illness through the psychophysiological processes concerned, the belief systems that accompany them, and the lifestyles that they promote (Moreno, 2007). The theory of constructed emotion (Barret & Russell, 2014), which emphasizes the core experience of affect, characterized by the dimensions of valence and intensity underlying the discrete emotional states, is the frame to understand our work. We will focus on some aspects of affect related to the promotion of quality of life in personality disorder. There has been a rapid increase of intervention studies that include QoL and psychological well-being as an outcome measure, such as Well-being Therapy, Acceptance and Commitment Therapy, Life-review Therapy, and Positive Psychological Interventions (Weiss et al., 2016). Their aim is to explicitly enhance positive psychological functioning, but research so far show only small effect sizes in clinical samples (Chakhssi et al., 2018). In her manual for borderline (BPD) patients, Linehan (1993) proposed the promotion of positive affect in the Emotion Regulation Skills module, with instructions to (1) build up positive emotions (exposure to, and awareness of, pleasurable experiences or activities causes pleasurable events to occur more often); (2) build mastery learning to face the future (carry out activities or live experiences that make one feel competent, confident, self-efficacious, feel that one is good at something or that one is learning something); and (3) take care of one’s body (healthy eating, balanced sleep, physical exercise). For its part, Acceptance and Commitment Therapy also promotes the cultivation of personal values so that the fight against symptoms does not maintain a pathological experiential avoidance (Hayes et al., 2013). The available evidence on BPD reviews indicates that treatments improve QoL to some extent, but it remains unclear whether current treatments are able to restore QoL to community norms (Chakhssi et al., 2021; IsHak et al., 2013). Despite the relevance of positive affect (PA) in emotional disorders, few studies investigate the effect of its specific promotion (Díaz-García et al., 2017). López-Gómez et al. (2017) compared the effect of cognitive-behavioural intervention with positive psychology intervention in a group of 128 women diagnosed with major depression or dysthymia. Although they found no differences between them, they observed a more immediate pattern of change in depressive symptoms and a more gradual one in well-being. They concluded that it was necessary to evaluate both aspects separately. For their part, Gili et al. (2020) observed that a PA promotion program seemed ineffective in reducing depressive symptoms, but promoted quality of life and well-being in patients with depression. Recently, Díaz-García et al. (2021) implemented a treatment protocol (TIBP) for people with emotional disorders to contrast the additional therapeutic potential of promoting PA versus the more classic intervention aimed solely at reducing NA. The effect on PA was higher in the TIBP+PA condition (d = 1.27) than in the TIBP condition (d = 0.69), a result consistent with the fact that TIBP+PA includes a specific component to promote PA, emphasizing positive experiences. Evidence so far shows that positive mental states play an independent role in health outcomes (Huppert & Whittington, 2003); psychological well-being is a protective factor against mental illness and psychopathology (Weiss et al., 2016); there is a bidirectional relation between positive mental health and psychopathology (Lamers et al., 2015); personality disorders are associated with an inferior quality of life, poor health, and premature mortality (Ekselius, 2018); the severity of personality disorder determines the quality of life better than the specific category of personality disorder (Soeteman et al., 2008); interventions for patients with personality disorder seems to fail in achieving a normative QoL (IsHak et al., 2013); and research founds severity (Stefanatou et al., 2022), interoception (Löffler et al., 2018), resilience (Guillén et al., 2021), and perceived social support (Thadani et al., 2022) as determinants of quality of life for patients with personality disorder. One of the most productive models of affect is Watson et al.’s (1988) two-dimensional model . They proposed a bifactorial model of affect (positive affect [PA] and negative affect [NA]) and developed an instrument for its evaluation (Positive and Negative Affect Schedule [PANAS]), whose psychometric quality and simplicity of use have favoured its broad intercultural and interdisciplinary dissemination. The model takes for granted that positively valenced affective states (such as enthusiasm, interest, determination, or pride) are independent of negatively valenced states (fear, guilt, shame, or anger), a hypothesis supported by empirical research: the correlation between PA and NA is usually low and factor analysis studies frequently confirm a latent structure of two independent dimensions (Díaz-García et al., 2020; López-Gómez et al., 2015). Not by chance, NA is a construct close to neuroticism and PA is close to extraversion (Morán et al., 2017), two different dimensions of personality traits structure. Empirical studies with the PANAS usually corroborate the independence of PA with respect to NA. But results have also been found that seem to contradict such bidimensionality, showing significant correlations between PA and NA. These inconsistencies can be put down to: interculturality and language, temporal instructions (which can differentiate emotional state/trait), cross-sectional/longitudinal analysis methodology (Rush & Hoffer, 2014), level of stress, or even the age of the participants. In a previous study (Ramos et al., 2021), the opportunity to make positive affect a focus of research and a key to intervention for personality disorder was emphasized (p. 15), taking up what was already suggested by Meehan et al. (2018). But a high correlation was also noted between PA and NA (r = -.51, p < .001), which would go against the two-dimensionality of the construct and, therefore, the need to specifically enhance PA for personality disorder patients. In the validation of the PANAS carried out by López-Gómez et al. (2015) with a sample of the general Spanish population (N = 1,071), an association (notably smaller, but significant) was also found between PA and NA (r = -.19, p < .001). These authors explain that “when stress levels are high, the magnitude of the association between both subscales tends to increase considerably (…), which may be one of the causes of the divergence found in different studies” (p. 542). In this regard, Flores and Medrano (2016) suggest to study the role played by the intensity of the affective state in the interaction between PA and NA, echoing what was previously indicated by Watson et al. (1988). For their part, Norlander et al. (2002) devised a classification of “affective personality” from the data obtained with the PANAS scales. Combining emotional intensity and affective valence, four types are obtained: self-constructive (high PA and low NA), self-destructive (low PA and high NA), high affective (high PA and NA), and low affective (low PA and NA). This typology has proven to make out the well-being of university students (Morán et al., 2017). The first objective of our research with personality disorder is to determine if emotional intensity actually influences the interaction detected between the two dimensions of affect and if both dimensions of affect are differentially associated with clinical/negative variables (symptoms, disturbance, suicidal ideation) and constructive/positive variables (self-esteem, self-efficacy, social skills). The second objective is to check differential changes in PA and NA after 6-month therapeutic intervention for personality disorder patients, and if that eventual difference could be accounted for by their affective personality (Norlander et al., 2002). Verifying that two different affective processes are taking place even in patients with severe pathology expands the possibilities of intervention in order to improve QoL and reduce psychoiatrogenia. We hypothesized that (1) the correlation between positive and negative affect is related to the emotional intensity level; (2) both dimensions of affect are differentially associated with clinical/negative variables (symptoms, disturbance, suicidal ideation) and constructive/positive variables (self-esteem, self-efficacy, social skills); (3) they change differently after treatment; and (4) self-constructive type of affect (characterised by low NA and high PA) presents a predominant change in PA over the rest of types after treatment. Participants Adults successively admitted between 2008 and 2021 in a specific hospital unit for personality disorder in-patients (N = 414) participated in this study. All met criteria for severe personality disorder, diagnosed by the psychiatrists responsible for its outpatient treatment in community mental health centres, corroborated through clinical interviews in the unit itself. Exclusion criteria were brain damage, intellectual disability, compliance with a legal sentence, severe drug dependence, and severe anorexia. Age ranged from 18 to 58 (M = 35.7, SD = 8.6); the majority were women (79.6%), single (66.2%), living with a relative (80%), without their own home (55.5%). Their employment status was unemployed (61.6%), with a temporary (24.4%) or permanent disability (14%). Only 13.1% had university studies, and 38.4% had a recognized degree of disability (between 33% and 81%); 59.7% had received a diagnosis of BPD; the rest had an unspecified (20.6%) or mixed personality disorder (17.1%). After signing a therapeutic contract, they voluntarily get involved in a 6-month intervention program inspired by the therapeutic community model (Campling, 2001). The activities are framed in a space of coexistence that promotes the values of voluntariness, respect, participation, and mutual learning. Patients assume responsibility for their decisions, interpersonal experience takes on a central role, and the person goes through a process of reconceptualizing their problems, validating their limitations, and facing more effectively the challenges of their specific socio-family environment. The program integrates in a daily schedule individual interventions (medication, psychotherapy, counselling), family sessions, and broad-spectrum group activities (psychoeducational, assembly, promotion of acceptance, integration, mentalization, self-direction, and skills training) in an integrated multi-professional effort (psychiatry, psychology, nursing, occupational therapy, and social work) based on an individual therapeutic plan designed as a team, developed through continuous evaluation, and inserted into the network of mental health resources of the Madrid Region. The program included psychometric evaluation based on a battery of self-report questionnaires, for the use of which for research purposes the patient gave his/her consent. The data of participants who did not fully and adequately complete the instruments were excluded. Measures and Procedure Positive and Negative Affect Schedule (PANAS; Watson et al., 1988; Spanish version by Joiner et al., 1997) The subject is asked to assess the magnitude with which s/he has experienced each of the 20 adjectives (10 positive and 10 negative) presented in a specified time (that day, the previous week, etc.) in reference to a 5-point scale (not at all, a little, moderately, quite a lot, very much), with scores ranging between 10 and 50 for each of the two scales. Their reliability is adequate, with Cronbach’s α = .89 for the positive affect scale (PA) and .85 for the negative affect (NA) scale, as well as their construct validity and factor structure. In our sample, α = .93 for PA and α = .92 for NA. Symptom Checklist 90 Revised (SCL90-R; Derogatis, 2002). The SCL90-R evaluates a wide range of psychopathological characteristics (somatization, anxiety, depression, obsession-compulsion, interpersonal sensitivity, hostility, paranoid ideation, psychoticism). Participants evaluate how upset they felt in the last few weeks for each of 90 symptoms on a Likert scale (0 to 4). It has 10 scales and three global indices. Reliability is acceptable, with high internal consistency coefficients (α > .81) and test-retest values higher than .78. For this study, only the Global Severity Index (GSI) was used, which is a generalized and indiscriminate measure of the intensity of symptom distress. In our sample, Cronbach’s alpha was .97. Beck Depression Inventory (BDI; Beck et al., 1979; Spanish version by Sanz & Vázquez, 1998) The BDI rates the intensity of depressive symptoms. Its reliability coefficient, with the two halves method, is .93. In our sample, a Cronbach’s alpha of .91 was obtained. Three-Dimensional Depression Questionnaire (CTD; Jiménez-García & Miguel-Tobal, 2003) With 34 items, the CTD evaluates the three response systems (cognitive-subjective, physiological-somatic and motor-observable) in which depression occurs. It also includes a scale that assesses the potential risk of suicide (“suicidal tendency” [ST], which will be used in this work) and a total score. It has a high reliability, with test-retest correlations after 6 weeks ranging between .63 and .85 and good internal consistency (α = .88 and .96). Moreover, it shows adequate convergent validity, high capacity to distinguish between clinical and control populations and a solid factor structure. In our sample, the TS scale obtained a Cronbach’s alpha of .88. Social Skills Scale (EHS; Gismero, 2000) The EHS evaluates perceived assertiveness and social skills through 33 sentences rated from 1 to 4 and structured in 6 scales. We use the overall score in this sstudy, with a Cronbach’s alpha reliability of .90. Rosenberg Self-esteem Scale (RSS; Rosenberg, 1989; Spanish version by Martín-Albo et al., 2007) The RSS evaluates the sense of own worth with 10 sentences rated from 1 to 5. It shows adequate levels of reliability and validity. In the present sample, the Cronbach’s alpha obtained was .76 Generalized Self-Efficacy Scale (GSE; Baessler & Schwarzer, 1996) The GSE evaluates a general sense of personal agency with 10 sentences rated from 1 to 4. Reliability is acceptable and internal consistency coefficients range from .79 to .93. In our sample, α = .88. From the PANAS, which the participants complete daily, the following variables were constructed:
Participants completed the rest of the instruments during the first weekend (pre-measurement) and the last fortnight before the scheduled discharge (post-measurement). They make it possible to operationalize the concept of negative and positive variables, the former being the ones that give a measure of pathology (SCL90-R, BDI, TS) and the latter the ones that offer a measurement of qualities/capabilities (EAG, RSS, EHS). The scores are processed in a split database to preserve anonymity. The work complied with the ethical and regulatory guidelines for publication and was approved by the Hospital Research Commission (9th of June 2022, code 2022-1). Data Analysis Pearson’s r correlations between PA and NA are obtained according to the level of emotional intensity (EI) and to negative (GSI, BDI, TS) and positive (EHS, EAG, RSS) variables. Fisher transformation of z statistic is used to contrast the difference in correlations. The large sample size of the distribution according EI categories, (low: n = 181; high: n = 227) and the asymmetry (< 1) and kurtosis (< 5) values allow normality to be assumed, so Student’s t-test is used to compare differences, without assuming equal variances (Levene: p < .01). Student’s t-tests are conducted to examine pre-post change in PA and NA, and ANOVA tests to check differences in positive (PAC), negative (NAC), and predominant affect change (PC) between the four affective personality types (APT) after the intervention, with Hochberg’s GT2 post hoc contrasts because of unequal subgroups sizes and similar variance (Levene test for PAC: F(3, 410) = 0.140, p = .936); for PC: F(3, 410) = 1.408, p = .240); and Games-Howell post hoc contrast when different variance is assumed (NAC: F(3, 410) = 3.535, p = .015). The analyses are performed using the package IBM SPSS Statistics v. 26 (IBM Corp., 2019). Table 1 Differences in Negative and Positive Affect as a Function of Emotional Intensity 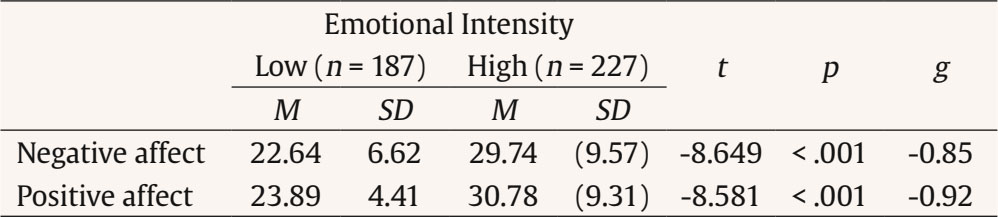 Table 2 Correlation Matrix of Negative and Positive Affect with the Rest of Variables (n = 414)  Note. 1 Scales from the Symptom Checklist-90-Revised (SCL-90-R). 2 For these variables, correlations with negative affect are different from correlations with positive affect (Fisher’s Z, p < .01). ** p < .01. Table 3 Pre-post Differences within Participants Who Completed the Intervention Program 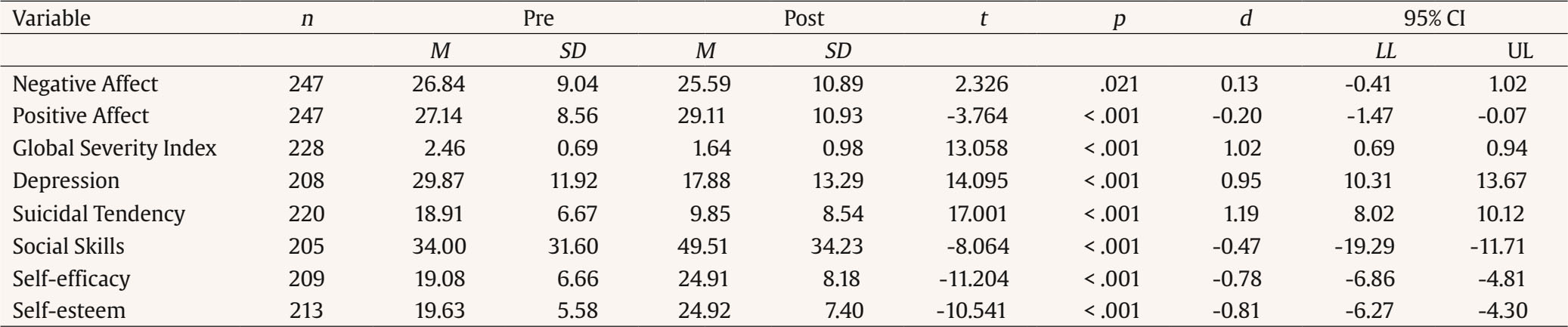 Note. CI = confidence interval; LL = lower limit; UL = upper limit. Table 1 shows the differences in NA and PA as a function of EI. The correlation between negative and positive affect from participants with low emotional intensity (r = -.580, p < .001) and from high emotional intensity (r = -.897, p < .001) are different (Fisher’s Z = 7.982, p < .001). Table 2 shows the correlations between PA and NA with the different subscales of the SCL90-R and with the rest of the questionnaires. One hundred seventy seven participants (40%) left the program before its completion. Pre-post differences among participants adhering to the program (n = 247, 60%) are shown in Table 3. They managed to reduce NA, M = -1.25, SD = 8.4; t(246) = -2.326, p = .021; 95% CI [-2.3, -0.2], and increase PA, M =1.97, SD = 8.2; t(246) = 3.764, p < .001; 95% CI [0.9, 3]. Taking the absolute values of both means, the difference between the magnitude of change in NA and PA is not significant, M = 0.72, SD = 7.9; t(246) = -1.432, p = .153; 95% CI [-1.7, 0.3]. However, when dividing the group according to emotional intensity level (low: n = 111, high: n = 136), the change in PA is higher than the change in NA in the subgroup of patients with high emotional intensity, NAC, t(241.2) = -0.653, p = .514, 95% CI [-2.7, 1.3]; PAC: t(241.9) = -2.363, p = .019; 95% CI [-4.4, -0.4]. Figure 1 shows the difference between pre and post intervention means in NA and PA by level of emotional intensity. Figure 1 Pre- and Post-Intervention Mean Raw Scores in Negative and Positive Affect in Function of Level of Emotional Intensity (low vs. high). 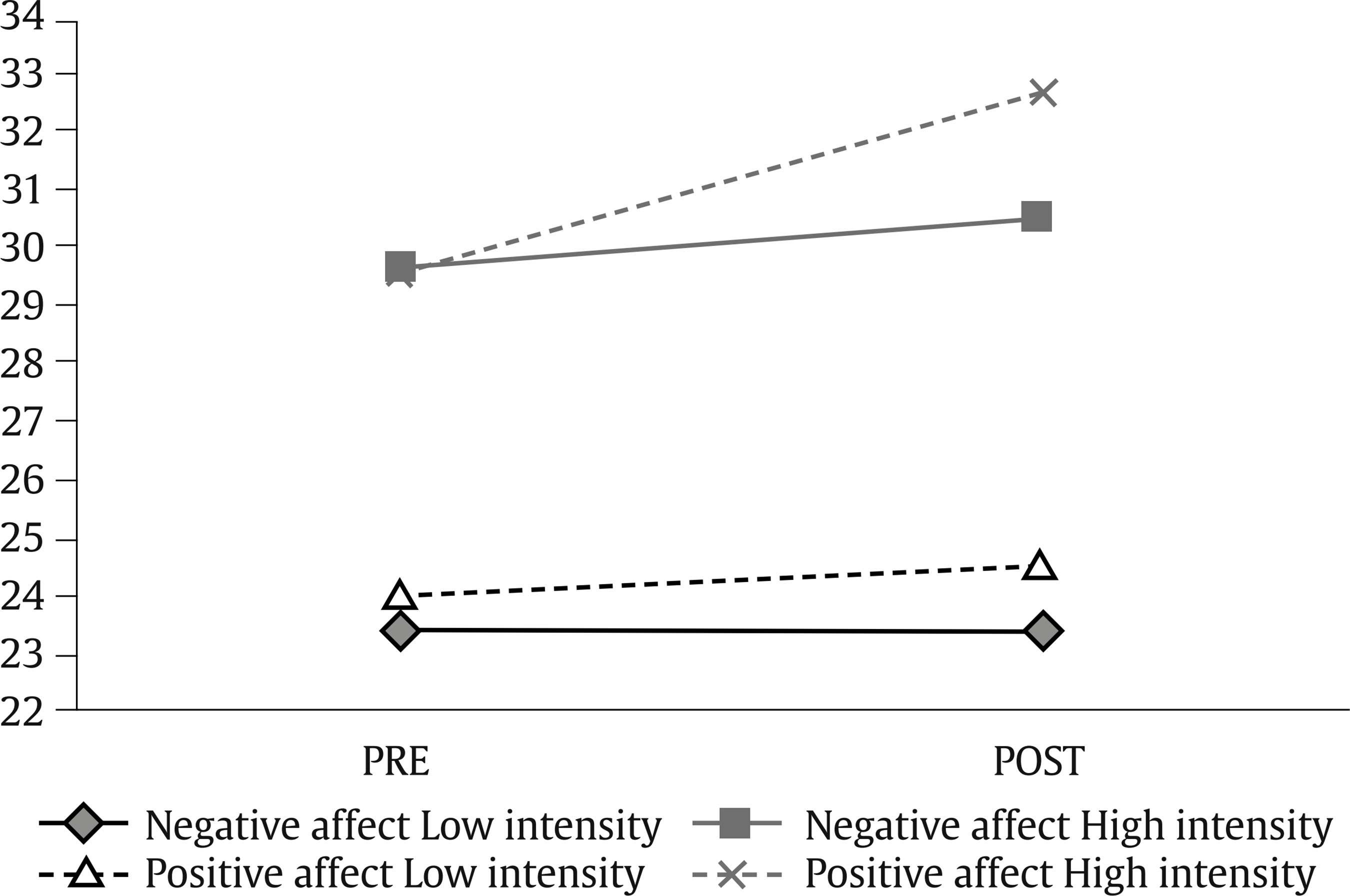 The ANOVA test indicates a significant low-size effect of affect personality type (APT) on negative affect change, F(3, 410) = 5.388, p = .001; η2 = .038, and on positive affect change: F(3, 410) = 2.906, p = .035; η2 = .021. The self-constructive patients (CON) reduce NA less than do self-destructive patients (DES), mean difference = -2.70 (0.93), p = .021; 95% IC [-5.1, -0.3], and high-affect patients (HA), mean difference = -3.73 (1.21), p = .013; 95% IC [-6.9, -0.6]. Post hoc contrasts show no significance for positive affect change. Table 4 Predominant Affect Change by Affect Personality Tpe and Hochberg’s GT2 Post-hoc Contrast of Group Differences 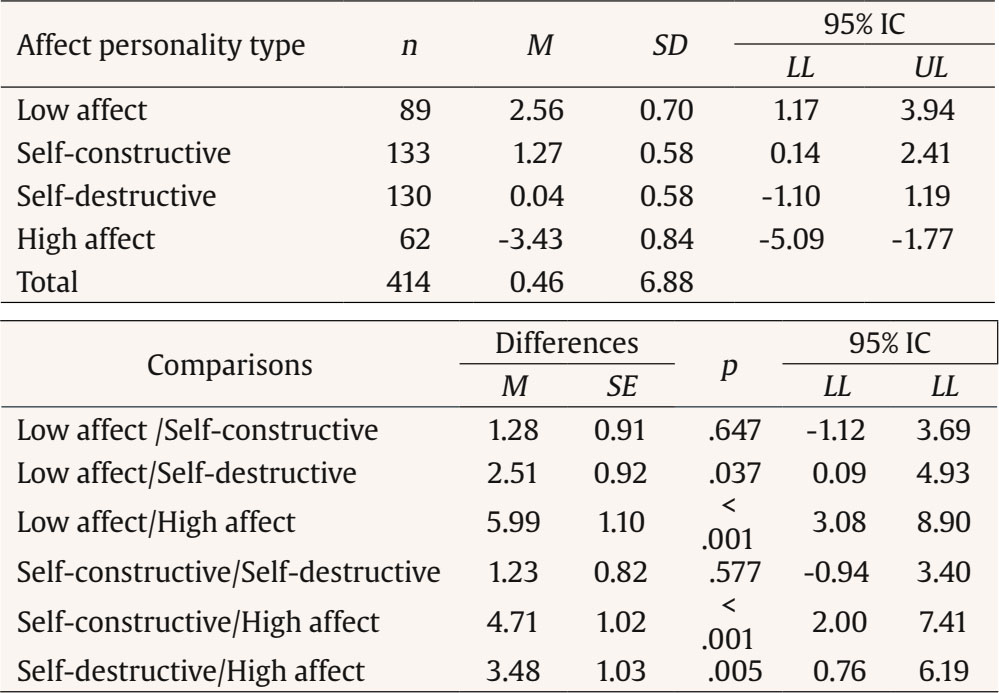 Note. CI = confidence interval; LL = lower limit; UL = upper limit. Figure 2 Predominant Affect Change (mean raw scores) in Function of Affective Personality Type (low affect, self-destructive, self-constructive, high affect).  There is a significant medium-size effect of APT on predominant change (PC), F(3, 410) = 10.870, p < .000; η2 = .074. Table 4 and Figure 2 show the magnitude of predominant affect change in each group according to their affective personality typology, and the significance of post hoc contrasts. High-affect patients increase PA less than do low-affect patients, self-constructive patients, and self-destructive patients. Psychopathology reduction and the conquest of a satisfactory quality of life seem to be different processes. The bifactorial theory of affect can help understand that dislocation. But data reported in various studies on high correlations between positive and negative affect appear to contradict the two-dimensionality of affect. Our work supports the suggestion that the association between both dimensions of affect is related to emotional intensity (Flores & Medrano, 2016; López-Gómez et al., 2015). Patients with higher EI present higher PAxNA correlations. Additionally, we observe that NA correlates to a greater extent with the variables of pathology (SCL90-R, BDI, and TS) and PA exhibits a high correlation with depression, which is consistent with the prediction of the Clark and Watson tripartite anxiety-depression model. PA correlation seems to be (p = .055) higher than NA correlation with only one of the positive variables: self-efficacy (GSE). This finding deserves to be cautiously highlighted. Not only could it corroborate data from other studies (Grimaldo Muchotrigo et al., 2021), but its implications are valuable: perceived self-efficacy is a general construct that accounts for variance in multiple domains of human functioning (Luszczynska et al., 2005), also in the specific field of PD (Ramos et al., 2018) and its enhancement seems more direct by promoting PA than by reducing NA. Our study also tried to examine whether there was a differential change between the two dimensions of affect among the participants who completed the program (n = 247) throughout the 6 months of intervention. Since it combined diverse approaches, varied activities, and different professionals, it is not possible to determine which elements were particularly responsible for the results. Research on the effectiveness of interventions for personality disorders suggests that various treatment packages produce similar results (Katakis et al., 2023; Levy et al., 2018). For this reason, investigating processes or mechanisms rather than results has been suggested to determine what really serves to promote change (Clarkin & Levy, 2006). Some common mechanisms identified in effective interventions for personality disorders are an accepted structure that clarifies roles and procedures, a validation of the experience and a support that builds interpersonal trust (Fonagy et al., 2015; Gunderson et al., 2013). Therapeutic communities particularly promote two specific factors (Pearce & Pickard, 2013): growth of the sense of belonging and enhancement of agency or personal responsibility. It is reasonable to think that these mechanisms have contributed to the change in affect of the participants in our study. Although there are no differences in magnitude (absolute scores) between the change in PA and the change in NA in the sample of adherents to the program, the differences do appear when emotional intensity is considered: PA change is higher than NA change in the subgroup of patients with high EI; furthermore, PA change in this subgroup is higher than in the subgroup of patients with low emotional intensity, while NA change is similar in both subgroups. The correlation of changes in positive and negative affect (PACxNAC) is also higher in patients with high emotional intensity. In line with the theory of Barret and Russel (2014), we consider that emotional intensity and quality (valence) of affect are independent variables that do not occur in the abstract but within persons, and therefore they are entwined in each patient (Kuppens et al., 2010; Ramos et al., 2017). Classifying the patients according to the typology of affective personality by Norlander et al. (2002) at the beginning of the intervention has allowed us to find differential change in positive and negative affect at the end. The high-affect type of personality gets to decrease NA more than to raise PA (predominance of NA change), just the opposite of what happens with the rest of profiles. Predominance of PA change in the subgroup of low-affect patients is higher than in the self-destructive type. Self-constructive patients get to reduce negative affect less than self-destructive and high-affect types. The emotional change observed after the intervention is not equivalent for positive and negative dimensions of affect when the patients are classified according to their core affect (Kuppens et al., 2010), which combines intensity and emotional valence. The patients who exhibit higher emotional intensity both in positive and negative emotions at the beginning of the intervention obtain better results mostly in the negative affect dimension. The opposite occurs in patients with lower emotional intensity in positive and negative emotions whose predominant gain come about in the positive affect dimension. In sum, when a patient scores high in the dimension of negative affect, s/he will probably score low in the dimension of positive affect (because of the observed raised correlation of both dimensions associated to high intensity), resulting in a worse experience of suffering and hopeless. When the patient gets to reduce the severity of negative affect, s/he will be able to increase positive affect. A progressive pattern emerges through the affect personality types, from low-affect to high-affect passing through self-constructive and self-destructive profiles (Figure 2): the lower the intensity of negative affect, the higher the prevalence of positive affect change after the therapeutic intervention. Understood as stages of change, these profiles could serve as a guide when designing a specific intervention to boost positive affect in order to enhance QoL. Positive emotions provide broader and richer behaviour scripts than those that foster negative emotions (Fernández-Abascal, 2009), so they must be cultivated strategically, at the moment of the therapeutic process in which their promotion will be more effective. Affective personality (Norlander et al., 2002) influences the predisposition for health or illness and is related to neuroticism and extraversion, the components of resilient or vulnerable personality (Morán et al., 2017). Extraversion predicts problem-solving and cognitive restructuring coping; neuroticism predicts problematic strategies like wishful thinking, withdrawal and emotion-focused coping strategies (Connor-Smith & Flachsbart, 2007). The differentiation of affective profiles, that turned out to be predictive of subjective well-being among university students (Morán et al., 2017), has also exhibited its ability to differentiate the change in PA and NA in our PD patients sample, and can be raised as a useful source of knowledge to better hit the expedient therapeutic design. Limitations of this work are the fact that it is based only on data from self-report, has a correlational nature and a static view: the fluctuation of affect, which uses to occur in short periods of time, has not been taken into account. That would imply an examination of the intra-personal variance (Rush & Hoffer, 2014). However, we have chosen a measure of the affective trait, not the affective state, which is one of the important sources of variability in research with the PANAS (Flores & Medrano, 2016). A limitation related with the generalization of results comes from the fact that only 60% of the initial sample adhered to the treatment program, something not uncommon in the intervention with PD patients. Besides, we have not examined which concrete aspects of the intervention program could be specifically attributed to the reduction of NA or to the promotion of PA, something that remains for future research. This paper shows that there is a dislocated behaviour between the two dimensions of affect, supporting the bifactorial model and thus the possibility of a differentiated therapeutic approach. The PA/NA dislocation and the verification of the effect that emotional intensity exerts on their association in patients with PD allow us to deduce practical implications for the design of intervention programs. A differentiated promotion of PA may be more effective when the emotional intensity and the affective valence of the patient are taken into consideration. The identification of relevant personal variables in health-disease processes contributes to the design of more personalized interventions. Affective states present co-activation in certain situations, so this contextual influence must be examined when designing the intervention, trying to “define more precisely those situations in which these constructs may be more related, both positively and negatively” (Flores & Medrano, 2016, page 182). The promotion of PA seems to be linked to obtaining good health (Chida & Steptoe, 2008). Studies such as Gili et al.’s (2020), Diaz-Garcia et al.’s (2021), or López-Gómez et al.’s (2017) seem to support its favourable effect in improving quality of life and well-being in patients with depression and emotional disorders. Future studies would test whether this statement is extensible to patients with PD, selecting the appropriate time and addressing the crucial processes to establish such a PA promotion program with guarantees of efficacy. Clinicians should not settle for the goal of a mere reduction of discomfort in a chronic revolving door. Conflict of Interest The authors of this article declare no conflict of interest. Cite this article as: Ramos, J. M., Marco, P. M., Sánchez, A., & Doll, A. (2024). Quality of life and positive and negative affect in the personality disorder. Clínica y Salud, 35(3), 119-126. https://doi.org/10.5093/clysa2024a16 References |
Cite this article as: Ramos, J. M., Marco, P. M., Sánchez, A., & Doll, A. (2024). Quality of Life and Positive and Negative Affect in the Personality Disorder. ClĂnica y Salud, 35(3), 119 - 126. https://doi.org/10.5093/clysa2024a16
Correspondence: jmramos@cop.es (Juan M. Ramos).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
Clinical and Health is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License








