


The Mediator Role of Illness Representations in Patients with Obstructive Sleep Apnea: A Preliminary Study
[El papel mediador de las representaciones de la enfermedad en pacientes de apnea obstructiva del sueño: un estudio preliminar]
Rute Sampaio1, 2, João C. Winck1, and M. Graça Pereira3
1University of Porto, Porto, Portugal; 2CINTESIS - Center for Health Technology and Services Research, Porto, Portugal; 3University of Minho, Braga, Portugal
https://doi.org/10.5093/clysa2024a7
Received 20 July 2022, Accepted 15 December 2023
Abstract
Background: This preliminary study examined the mediating role of illness representations on health-related quality of life (HRQoL) between adherent and poorly adherent obstructive sleep apnea patients (OSA) to the automatic positive airway pressure (APAP) therapy. Method: A total of 185 patients were assessed on determinants of APAP treatment, illness representations, family coping, and self-efficacy, at T1 (prior to APAP treatment) and T2 (1 to 2 months with APAP treatment). Results: Regarding the determinants of APAP, adherent patients showed higher self-efficacy, outcome expectations, and decisional balance index, compared to poorly adherent patients. Adherent patients also showed higher family coping and HRQoL, but less threatening cognitive representations compared to poorly adherent patients. Illness cognitive and emotional representations mediated the relationship between self-efficacy/family coping and HRQoL, in adherent patients. Only illness cognitive representations mediated the relationship between self-efficacy and HRQoL in poorly adherent patients. Conclusions: The results highlight the importance of illness representations during OSA treatment in the promotion of adherence to APAP.
Resumen
Antecedentes: Este estudio preliminar examina el papel mediador de la representación de la enfermedad en la calidad de vida relacionada con la salud (CVRS) entre pacientes con apnea obstructiva del sueño (AOS) observantes y poco observantes de la terapia de presión positiva automática en las vías respiratorias (APAP). Método: Se evaluó a un total de 185 pacientes sobre los determinantes del tratamiento APAP, las representaciones de la enfermedad, el afrontamiento familiar y la autoeficacia en T1 (antes del tratamiento APAP) y T2 (1 a 2 meses con tratamiento APAP). Resultados: En cuanto a los determinantes de la APAP, los observantes mostraron mayor autoeficacia, expectativas de resultados e índice de equilibrio decisional en comparación con los poco observantes. Los observantes también mostraron un mayor afrontamiento familiar y CVRS pero menos representaciones cognitivas amenazantes en comparación con los observantes deficientes. Las representaciones cognitivas y emocionales de la enfermedad mediaron la relación entre la autoeficacia/afrontamiento familiar y la CVRS en pacientes observantes. Solo las representaciones cognitivas de enfermedad mediaron la relación entre la autoeficacia y la CVRS en pacientes de baja observancia. Conclusiones: Los resultados destacan la importancia de las representaciones de la enfermedad durante el tratamiento de la AOS en la promoción de la adherencia a la APAP.
Palabras clave
Apnea obstructiva del sueño, Patrones de adherencia a APAP, Calidad de vida relacionada con la salud, Representaciones de la enfermedadKeywords
Obstructive sleep apnea, Adherence patterns to APAP, p Health-related quality of life, Illness representationsCite this article as: Sampaio, R., Winck, J. C., & Pereira, M. G. (2024). The Mediator Role of Illness Representations in Patients with Obstructive Sleep Apnea: A Preliminary Study. ClĂnica y Salud, 35(1), 21 - 26. https://doi.org/10.5093/clysa2024a7
Within automatic positive airway pressure (APAP) therapy, continuous positive airway pressure (CPAP) has been the treatment of choice in obstructive sleep apnea (OSA) patients (Patil et al., 2019) since its introduction in 1981 (Sullivan et al., 1981). Despite all the technical improvements made on the PAP devices, such as humidification, noise reduction, and patient-specific auto titration, its effectiveness is limited by suboptimal adherence (Aloia et al., 2010; Alves et al., 2012). Higher rates of poor adherence or discontinued treatment usage continue to be a problem for clinicians and researchers in the OSA field (Arachchige & Steier, 2021; Weaver & Sawyer, 2010). Therefore, understanding adherence is of considerable clinical interest given the extensive evidence in the literature on the benefits of CPAP usage in reversing sleep apnea symptoms (D’Ambrosio et al., 1999; Zampogna et al., 2019) and improving Health Related Quality of Life (HRQoL) (Lynch et al., 2019; Sforza et al., 2003). As a subjective concept, HRQoL is the barometer outcome variable which encompasses the impairment caused by treatment and disease processes (Baldwing et al., 2001). HRQoL was a dependent variable in the present study since it is a major clinical factor for cost-benefit OSA treatment (Lee et al., 2016). A recent systematic review suggested an association between untreated OSA and worse HRQoL (Pauletto et al., 2021). Indeed, the way patients perceive disease symptoms and their impact on physical, emotional, and cognitive functioning are the main clinical predictors of HRQoL (Lynch et al., 2019; Wild et al., 2004). Previously, the authors have suggested that illness representations predict HRQoL, independently of PAP usage and that there was a relationship between threatening illness representations (OSA) and a decrease in HRQoL (Sampaio, 2013). Illness representations are considered self-assessments of one’s health, including symptom perception, interpretation, and reporting, central to illness-related self-regulatory behavior (Cameron & Leventhal, 2002). The emphasis on theory-driven psychological constructs to predict adherence has recognized their potential regarding treatment target interventions (Pinho & Sampaio, 2022). The literature is unanimous in identifying self-efficacy, decisional balance, outcome expectancies, and active coping strategies as main predictors of adherence (Aloia et al., 2005; Mehrtash et al., 2019). Self-efficacy is the belief in one’s ability to succeed in specific situations or accomplish a task (Bandura et al., 1999). Decisional balance is a method for analyzing the pros and cons of different choices, helping someone decide what to do in a particular circumstance (Prochaska et al., 2002). These constructs emerge during the initiation phase of adherence to PAP treatment and shape the determination to use it (Aloia et al., 2005; Weaver & Grunstein, 2008). Active coping strategies include initiating direct action, increasing one’s efforts, and trying to execute a coping attempt in a stepwise fashion and independently contributed to 16% of the variance in CPAP adherence (Stepnowsky, Bardwell, et al., 2002). The Leventhal Self-Regulation Model (Leventhal et al., 1997) is similar to the social cognitive models in sharing the assumption that individuals develop beliefs that influence the interpretation of information and one’s experience which guides behavior (Leventhal et al., 2008), though illness representations have not been consistently studied in OSA patients. A previous study found that illness representations and family coping predicted PAP adherence, over a six-month period (Sampaio, 2013). Olsen et al. (2008) emphasized the lack of research regarding mediating and moderating relationships between psychological factors and HRQoL outcomes (Olsen et al., 2008). For example, one randomized controlled trial conducted a cognitive-behavior intervention to improve CPAP adherence and conceptualized self-efficacy, social support, and expectancy as mediators of adherence (Richards et al., 2007). Another large randomized control trial, focusing on the efficacy of a telemedicine intervention on adherence to CPAP, identified self-efficacy and decisional balance index as factors that were influential on outcomes (Sparrow et al., 2010). Also, self-efficacy regarding the use of CPAP moderated the relationship between its usage and fatigue/sleepiness (Baron et al., 2011; Mehrtash et al., 2019). Moreover, in a previous study, an interaction between illness cognitive representations, self-efficacy and family coping with adherence patterns was found (Sampaio et al., 2014). In other medical illnesses such as cancer, Johansson et al. (2018) found that illness perceptions mediated the relationship between self-efficacy and HRQOL. The present study pursued the latter hypothesis and investigated the mediating effect of illness representations in the relationship between family coping/self-efficacy (coping strategies) and HRQoL in OSA patients. The purpose of this study was to test: 1) differences between poorly adherent and adherent patients, following APAP treatment, on socio-demographic, clinical, and psychological variables (family coping, self-efficacy, outcome expectations, decisional balance index and HRQoL), and 2) the mediator role of cognitive and emotional representations between psychological factors (family coping, self-efficacy) and HRQoL in adherent and poorly adherent patients receiving APAP treatment. Participants and Data Collection This study is based on a prospective cohort study, with two-time assessments at baseline T1 (prior to APAP treatment) and T2 (1 to 2 months with APAP treatment). A total of 185 patients participated in the study and underwent a standardized protocol (general clinical evaluation by a sleep specialist, home sleep study, and psychological evaluation).Of these, 106 were classified as adherents, based on the average number of hours used and total percentage usage. Poorly adherent patients were those who used APAP < 4h/night and < 70% total days of usage and adherent patients were those who used APAP > 4h/night and > 70% total days of usage (Engleman et al., 1994; Stepnowsky, Marler, et al., 2002). The study was conducted in a Sleep Disordered Breathing Clinic of a university hospital in northern Portugal and was approved by the research ethics committee of the hospital, of the hospital, with the code 21/08. Exclusion criteria included psychiatric disorders or other sleep disorders. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. All participants signed an informed consent form, participated voluntarily, and were assured anonymity along with the possibility of withdrawing at any time. Instruments Upon APAP prescription (T1), a number of baseline questionnaires were provided, during a face-to-face interview with a trained health psychologist and repeated in T2. Determinants of Nasal CPAP Compliance (Stepnowsky, Marler, et al., 2002; Portuguese version by Sampaio, 2014) This instrument has 6 scales: self-efficacy (4 items), outcome expectations (4 items), knowledge (11 items), social support (9 items), decisional balance index (12 items), and the process of change (20 items), using a five-point (1-5) response scale. Higher scores represent enhanced behavior engagement for CPAP compliance, enabling to understand these categories along a continuum of motivational readiness to change a specific behaviour (Stepnowsky, Marler, et al., 2002). An internal consistency reliability coefficient (Cronbach alpha) was adequate for five scales, self-efficacy (a = .87), outcome expectations (a = .75), social support (a = .94), decisional balance index (a = .86), and process of change (a = .88), indicating good reliability, with the exception of the knowledge scale (a = .53), which was not included. The process of change subscale was completed only after APAP use. Hospital Anxiety and Depression Scale (HADS; Zigmond & Snaith, 1983) HADS is a validated 14 item scale with two subscales, measuring anxiety and depression, in a four point (0-3) Likert scale. Scores range from 0 to 21, in both scales. A score above 11 (cutoff threshold) indicates a clinical diagnosis of anxiety and depression. In the current sample, internal consistency reliability coefficient was adequate for both anxiety (α = .72) and depression subscales (α = .82), indicating good reliability. Illness Perception Questionnaire-Brief (Broadbent et al., 2006) The Portuguese validated version (Figueiras et al., 2010) has eight items, combined in three scales, that assess illness perceptions: cognitive illness representations (consequences, timeline, personal control, treatment control, and identity), emotional representations (concern and emotions), and illness comprehensibility. All items are rated on a 10-point Likert scale. This instrument has also another item, assessing casual representations, which is answered with an open-ended response. High scores (sum of all items) reveal a more threatening perception of the illness. In the current sample, internal consistency reliability coefficients (Cronbach alpha) for cognitive and emotional representations subscales were both acceptable (a = .60 and a = .70, respectively). Family Crisis Oriented Evaluation Scales (F-Copes; (McCubbin, 1981) This instrument measures how families cope with problematic situations, such as a recent OSA diagnosis. The Portuguese version (Cunha, 2017) includes five subscales: acquiring social support (6 items), reframing (7 items), seeking spiritual support (3 items), mobilizing the family to acquire and accept help (8 items), and passive appraisal (6 items). The alpha for the total scale was .83. Responses were scored using a 5-Likert point scale (1 = lower use of the coping strategy and 5 = higher use of the coping strategy). Higher scores indicate more use of family coping strategies. SAQLI Sleep Apnea Quality of Life Index (Sampaio et al., 2012a) This validated scale evaluates four domains of quality of life (daily functioning, social interactions, emotional functioning, symptoms) and an additional domain (treatment related symptoms) that evaluates treatment effects (used in T2). Higher scores indicate better quality of life. Hence, SAQLI is a potentially useful instrument concerning treatment success and side effects, which can capture of pre-and post-treatment differences. SAQLI showed alpha coefficients of .84 to .89. Pearson correlation coefficients between SAQLI inter-domains before and after APAP treatment and clinical variables were highly correlated (Sampaio et al., 2012b). APAP Adherence APAP adherence was assessed at home by an overnight sleep study using a five-channel recording device (Sleep Screen, Viasys TM Healthcare) as described in a previous publication This device produces a computerized recording of variations in oronasal airflow (measured by nasal cannula), body position, wrist actimetry, pulse rate, and arterial oxygen saturation (measured by finger pulse oximetry). Sleep technicians carried out a manual analysis of the recordings, by counting apnea episodes of ≤ 10% of previous airflow (with at least 10 seconds of duration) and hypopnea episodes (episodes showing 20 to 50% of the previous airflow, with at least 10 seconds of duration together with a 4% dip in oxygen saturation) and dividing the total number of these episodes by sleep time in hours, obtaining a manual apnea hypopnea index according to established criteria. For a fuller description, please see Sampaio et al (2012). Data Analysis Descriptive analyses of socio-demographic variables (age and gender), clinical variables (AHI, mask leakage, P95cm percentile pressure – the level of APAP pressure exceeded only 5% of the time) and psychosocial variables (self-efficacy, outcome expectations, decisional balance index, illness representations, and family coping) were performed for adherent and poorly adherent patients. Categorical variables were described as absolute frequencies and relative frequencies; means and standard deviations were used for continuous variables; t-test and chi-squared tests were performed to describe differences between the two groups. Selected thresholds to define adherence were based on the average number of hours used and total percentage usage, downloaded from the APAP machine, as mentioned above in the section on participants. To test simple mediation Preacher and Hayes’ (2004) bootstrapping methodology was chosen for indirect effects based on 5,000 bootstrap resamples to describe the confidence intervals of indirect effects (Chen, 2010; Preacher & Hayes, 2004). Bootstrapping is a nonparametric procedure that generates an estimate of the indirect effect, including a 95% confidence interval assuming that the distribution of the measures approximates that of the population. This procedure avoids assuming that any indirect effect is normally distributed (Chen, 2010). The indirect effect is represented by the product of the coefficients. When zero is not in the 95% confidence interval, one can conclude that the indirect effect is significantly different from zero at p < .05 (two-tailed) and, thus, the effect of the independent variables (family coping and self-efficacy) on the dependent variable (HRQoL) will be mediated by OSA cognitive and emotional representations, after CPAP treatment (T2). Bootstrapping analysis was chosen since it provides reliable results even when the data deviates from normality assumption or with smaller sample sizes (N ≤ 100). In this case, the sample size of the poorly adherent group included 79 patients. Of the total of 185 OSA patients, 19.5% were female and 80.5% male, with a mean age of 52.3 years old. After APAP treatment usage, 57.3% were adherents and 42.7% were poorly adherent patients. Table 1 describes the sociodemographic and clinical characteristics of the sample. Differences on Socio-demographic, Clinical and Psychological Variables between Poorly Adherent and Adherent Patients at T2 Table 1 describes OSA patients at baseline (T1) and differentiates poorly adherent and adherent patients following APAP treatment (T2). The groups did not differ significantly on any of the sociodemographic or clinical variables (p > .05). Regarding psychological variables, adherents had significantly higher self-efficacy, t(95) = - 7.74, p < .001, outcome expectations, t(110) = - 4.26, p < .001, and higher decisional balance index. t(123) = - 6.45, p < .001, concerning the determinants of APAP treatment, compared to poorly adherents. A similar trend was observed for family coping, t(183) = -1.20, p < .05, and HRQoL, t(135) = - 5.36, p < .01, with adherents scoring significantly higher than poorly adherents. Finally, in terms of illness representations, adherents showed less threatening cognitive representations, t(161) = 2.07, p < .05, than poorly adherents. Table 1 Socio-demographic, Clinical and Psychological Characterization of Patients at Baseline - T1 (n = 185), and Differences between Adherents (n = 106), and Poorly Adherents (n = 79) after APAP Treatment - T2 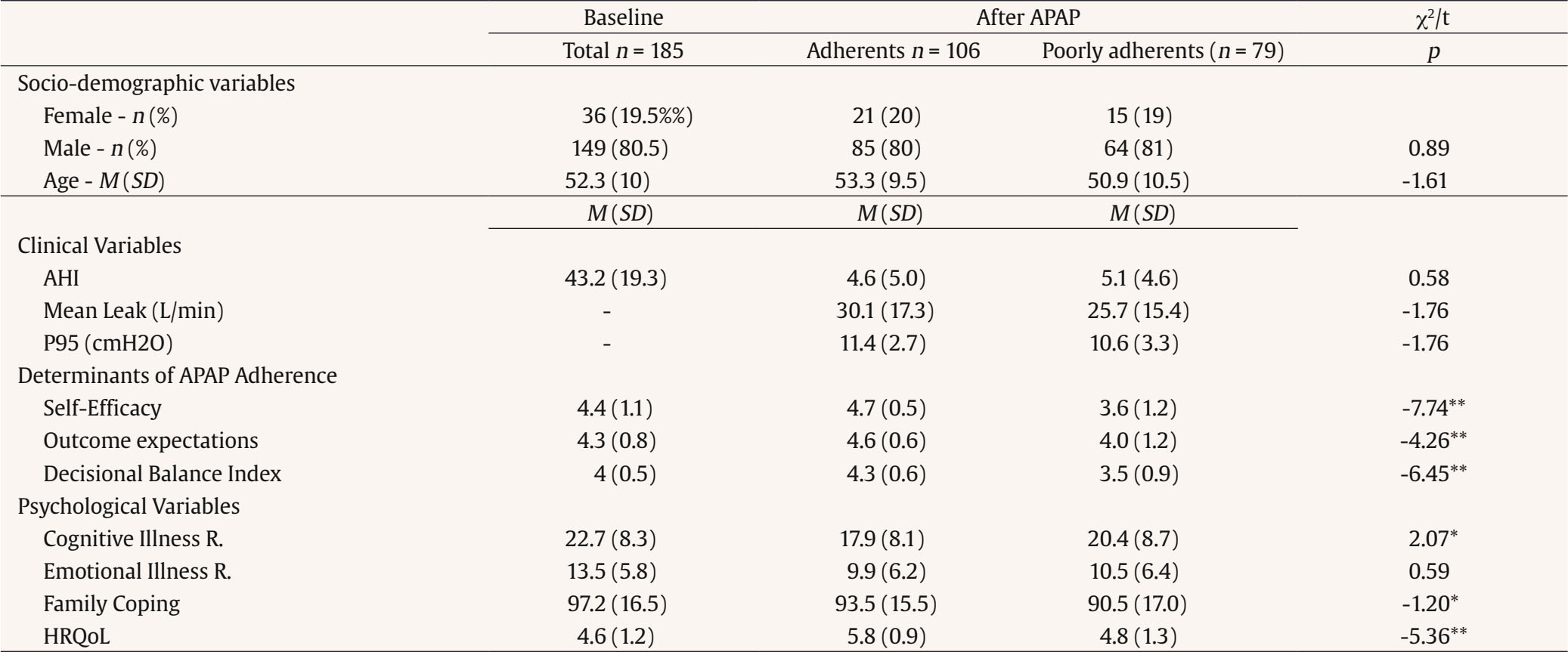 *p < .05, **p < .01. Illness Representations as Mediators between Family Coping/Self-Efficacy and Quality of Life in Adherent Patients at T2 The first analysis revealed that illness cognitive representations partially mediated the relationship between family coping, and HRQol as the indirect effects were estimated to lie between 95% CI [.005, .018]. In the second mediation analysis, illness cognitive representations partially mediated the relationship between self-efficacy, and HRQol as the indirect effects were estimated to lie between 95% CI [.0924, .4475]. The results of the final mediation analysis showed that emotional illness representations mediated the relationship between self-efficacy, and HRQol as indirect effects were estimated to lie between 95% CI [.0616, .4757] (see Table 2). Table 2 Illness Representations as Mediators between Family Coping/ Self-Efficacy and HRQol, in Adherent Patients at T2 (n = 106)  *p < .05, **p < .01. Illness Representations as Mediators between Family Coping/Self-Efficacy and Quality of Life in Poorly Adherent Patients at T2 The mediating effect of illness cognitive representations was discarded since bootstrap 95% CIs indicated that the indirect effect of family coping 95% CI [-.0032, .0136] was non-significant. The same was true regarding the mediating effect of emotional representations between self-efficacy and HRQol 95%CI [-.1496, .0710]. Interestingly, in this group, cognitive representations mediated the relationship between self-efficacy and HRQol since indirect effects lied between 95% CI [.1155, .3898] (Table 3). Table 3 Illness Representations as Mediators between Family Coping/ Self-Efficacy and HRQol in Poorly Adherent Pationes at T2 (n = 106)  Note. 1Family coping; 2self-efficacy. **p < .01 One critical psychological variable often neglected in research, pertaining to the perception of APAP adherence, is the way patients perceive their illness and treatment. The findings of the present study highlight the importance of illness representations in the conceptualization of the relationship between self-efficacy, family coping, and HRQoL (Cheng, Inder, et al., 2020; Cheng, Yang, et al., 2020). Not only did illness representations independently predicted adherence, but they also mediated the relationship between self-efficacy, family coping, and HRQoL in adherence patterns. Adherent patients, showing less threatening illness representations, could identify OSA signals and symptoms, had higher control of their health problem, perceived an intermittent course of the disease, and showed lower impairment due to OSA. Also, adherent patients evaluated their HRQoL as less impaired and employed more family coping strategies. The first mediation analysis revealed that adherent patients had higher engaged in a higher number of family coping strategies, reported higher HRQoL and that relationship was partially mediated by illness cognitive representations. In this group, illness cognitive representations mediated the relationship between adoption of family coping strategies and HRQoL. The same did not occur in the poorly adherent group, probably due to the threatening illness cognitive perceptions, which inhibited family coping strategies and HRQoL. Cognitive illness representations were also important in establishing a link between self-efficacy and HRQoL for both poorly adherent and adherent groups. Also, higher self-efficacy predicted better HRQoL but only when patients showed less threatening cognitive representations, as observed in a study with adults with multiple chronic conditions (Cheng, Yang, et al., 2020). In contrast, in poorly adherent patients, higher threatening emotional representations were associated with lower HRQoL. Interestingly, emotional representations were related to self-efficacy, which confirmed the previous assumption of a relationship between these two constructs at an information process level (Cameron, 2003; McAndrew et al., 2018; Sampaio et al., 2014). Regarding treatment, adherents perceived themselves as self-efficient and having good HRQOL. However, this relationship was only established when OSA was perceived as less emotionally threatening. In conclusion, this study provides more insights when explaining the interplay between illness representations, self-efficacy, family coping strategies, and HRQoL in adherence patterns after 1 to 2 months of APAP treatment. Limitations Limitations include the use of self-report instruments in psychological assessment, sample size, and the design that included only two assessment moments, with a short time between both assessments. Future studies should examine the role of illness representations in adherence to APAP over time, using longitudinal designs, and assess also partners’ illness representations in order to analyze their contribution to the patient’s adherence patterns. Conclusion In this preliminary study, the relationship between illness representations, self-efficacy, and HRQoL in adherence patterns for APAP treatment was confirmed, suggesting that relevant psychological factors, such as illness representations, should be targeted in future investigations. OSA is a chronic disease that implies permanent psychosocial adjustment during a long process that must be continually evaluated. Given the relationships between illness cognitive and emotional representations, self-efficacy, family coping, and HRQoL, health professionals should consider illness representations during OSA treatment, in order to help patients to develop less threatening illness representations and, therefore, promote adherence to APAP. Conflict of Interest The authors of this article declare no conflict of interest. Authors’ Contribution Rute Sampaio was responsible for data collection, data analysis, data interpretation and manuscript preparation; João C. Winck was responsible for data interpretation, manuscript review and editing, revising the paper critically for important intellectual content; and M. Graça Pereira was responsible for the study design, data interpretation, manuscript review, and for revising the paper critically for important intellectual content. Funding: This work was supported by a grant (SFRH/BD/ 38388/2007) from the Portuguese Foundation of Science and Technology. This study was conducted at the Psychology Research Centre (PSI/01662), School of Psychology, University of Minho, supported by the Foundation for Science and Technology (FCT) through the Portuguese State Budget (Ref.: UIDB/PSI/01662/2020). Cite this article as: Sampaio, R., Winck, J. C., & Pereira, M. G. (2024). The mediator role of illness representations in patients with obstructive sleep apnea: A preliminary study. Clínica y Salud, 35(1), 21-26. https://doi.org/10.5093/clysa2024a7 |
Cite this article as: Sampaio, R., Winck, J. C., & Pereira, M. G. (2024). The Mediator Role of Illness Representations in Patients with Obstructive Sleep Apnea: A Preliminary Study. ClĂnica y Salud, 35(1), 21 - 26. https://doi.org/10.5093/clysa2024a7
Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
Clinical and Health is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License








