


Barriers to the Uptake of a Psychoeducational Intervention to Prevent Postpartum Depression: An Exploratory Study
[Las barreras para la adopciĂłn de una intervenciĂłn psicoeducativa para prevenir la depresiĂłn posparto: un estudio exploratorio]
Mª Asunción Lara, Laura Navarrete, Erica Medina, Eunice Ruiz, Marcela Tiburcio, & Patricia Fuentes
DirecciĂłn de Investigaciones EpidemiolĂłgicas y Psicosociales, Instituto Nacional de PsiquiatrĂa RamĂłn de la Fuente Muñiz, Ciudad de MĂ©xico, Mexico.
https://doi.org/10.5093/clh2026a10
Abstract
Background: The study aimed to evaluate the assessment of usefulness, barriers, and adaptations (among other variables) made by professionals caring for perinatal women during the implementation of an evidence-based intervention (EBI) for preventing postpartum depression. Method: From 2016 to 2022, 120 professionals participated in a guided online course to implement the Postpartum Depression Prevention Intervention (PPD-PI). Socio-demographic data, achievement of objectives, and knowledge acquired to implement the intervention were retrieved from the Application for Registration. A purposely designed follow-up questionnaire with sixteen open and closed questions evaluated the intervention’s implementation including its usefulness, barriers, and adaptations made. Data was analyzed using descriptive statistics and thematic categorization of open-ended responses. Results: Participants, including psychologists, physicians, psychiatrists, social workers, and nurses, reported high satisfaction with the course and significant skill development. Most professionals adapted the intervention to their work settings by altering the order of the topics, number of sessions, and activities. Key barriers included lack of time, resources, and institutional support. The training and materials were seen as effective for disseminating the PPD-PI. Conclusions: Professionals expressed satisfaction with the implementation, although they found the assessment measurements too general. These findings constitute an initial approach to EBI dissemination and implementation in Mexico.
Resumen
Antecedentes: El estudio tuvo como objetivo evaluar la valoración de la utilidad, las barreras y la adaptación (entre otras variables) observadas por profesionales que atienden a mujeres perinatales durante la implementación de una intervención basada en la evidencia (EBI) para la prevención de la depresión posparto. Método: Entre 2016 y 2022, 120 profesionales participaron en un curso dirigido online para implementar la Intervención para la Prevención de la Depresión Posparto (PPD-PI). Los datos sociodemográficos, el logro de los objetivos y los conocimientos adquiridos para aplicar la intervención se obtuvieron de la solicitud de registro. Un cuestionario de seguimiento diseñado específicamente, con dieciséis preguntas abiertas y cerradas, evaluó la implementación de la intervención, incluyendo su utilidad, las barreras y las adaptaciones realizadas. Los datos se analizaron mediante estadística descriptiva y categorización temática de las respuestas abiertas. Resultados: Los participantes, psicólogos, médicos, psiquiatras, trabajadores sociales y profesionales de enfermería, mostraron una gran satisfacción con respecto al curso y un desarrollo significativo de habilidades. La mayoría de los profesionales adaptaron la intervención a su entorno laboral modificando el orden de los temas, el número de sesiones y las actividades. Las principales barreras fueron la falta de tiempo, de recursos y de apoyo institucional. Se consideró que la capacitación y los materiales eran eficaces para la difusión del PPD-PI. Conclusiones: Los profesionales expresaron su satisfacción con la implementación, aunque consideraron que las medidas de evaluación eran demasiado generales. Los resultados constituyen un primer acercamiento a la difusión e implementación de la EBI en México.
Palabras clave
PrevenciĂłn, DepresiĂłn pospartoKeywords
Prevention, Postpartum depressionCite this article as: Lara, M. A., Navarrete, L., Medina, E., Ruiz, E., Tiburcio, M., & Fuentes, P. (2026). Barriers to the Uptake of a Psychoeducational Intervention to Prevent Postpartum Depression: An Exploratory Study. Clinical and Health, 37, Article e260724. https://doi.org/10.5093/clh2026a10
Correspondence: laracan@imp.edu.mx ((Mª. A. Lara).Perinatal depression is a significant public health problem occurring at a crucial point in the lives of mothers, increasing the risk of adverse consequences for their health and emotional well-being and those of their babies. Between 13% and 15% of mothers suffer from postpartum depression (Woody et al., 2017) worldwide, with a similar prevalence among Mexican women (Lara et al., 2015). The onset of depression during pregnancy is also common, with rates ranging from 9.2% to 19.2% (Lara et al., 2015; Woody et al., 2017). This prevalence is significantly higher in women in low- and middle-income countries than in high-income countries (Woody et al., 2017). The consequences of untreated maternal depression are of particular concern. During pregnancy, it increases the risk of preterm birth, small-for-gestational-age newborns, and low birth weight, as well as maternal perinatal complications and the risk of postpartum depression (PPD) (Jahan et al., 2021). Untreated PPD is known to be a key risk factor for the quality of mother-infant interactions and child development (Slomian et al., 2019; Stein et al., 2014), even if depression symptoms are only subclinical (Tronick & Reck, 2009). Randomized controlled trials (RCTs) of psychological interventions show that PPD can be prevented by reducing depression symptoms (Branquinho et al., 2021; Morrell et al., 2016; Muñoz et al., 2021). In Mexico, an RCT of a PPD preventive intervention implemented during pregnancy in a sample of women at risk of depression showed that the incidence of depression can be reduced (Lara et al., 2010). Results of the effectiveness of evidence-based interventions (EBIs) are often not translated into care protocols that can easily1 be adopted, and are therefore not disseminated or implemented in everyday practice (Battaglia & Glasgow, 2018), despite being urgently needed given the prevalence of PPD. In this respect, it has been documented that between 50% and 70% of women with perinatal depression are not identified timely, approximately 85% do not receive treatment, 91%-93% do not receive adequate treatment and 95%-97% continue to suffer symptoms without remission (Cox et al., 2016). Implementation science emerged to address the gap between research and clinical and community contexts. Implementation involves the processes and factors associated with successfully incorporating proven interventions into a particular setting and the process and factors leading to the target population’s widespread use of these interventions (Shelton et al., 2020). The implementation of an intervention by professionals at an institution constitutes a significant step towards fine-tuning as it informs on their perspective on aspects such as barriers, compatibility with work schedules, additional training needs of professionals, and workflow (Mol et al., 2019). A systematic review on the barriers and facilitators to implementing perinatal mental health care in health and social care settings showed that barriers to PPD screening, referral, and treatment measures included professionals’ lack of self-confidence in carrying them out and the sense that they lack sufficient training (Webb et al., 2021). Facilitators stressed the need for health-care professionals to have an open, non-critical attitude towards patients and a genuine interest in women’s needs (Webb et al., 2021). Al-abril et al. (2023) explore the experiences of a wide range of healthcare professionals, including nurses, midwives, and general practitioners, with varying years of experience in primary antenatal, peri- and postnatal care. Challenges professionals encountered with their patients included the need or desire for effective support from the health system in terms of training and providing clear protocols and guidelines for the detection and management of prenatal, peri and postnatal depression. Health systems in certain countries, particularly higher-income countries (HICs), have incorporated perinatal mental health care into pregnancy care services (Buist et al., 2008; Milgrom & Gemmill, 2014), which is conducive to implementing evidence-based strategies. In low- and middle-income countries (LMICs), such as Mexico, though perinatal mental health has not been given enough importance, and although there are official standards in this country specifying its care, its application is not mandatory, the mechanisms for its implementation are not specified, and it fails to provide health services with the required specialized mental health personnel (Navarrete et al., 2022). The authors document the absence of systematic implementation of evidence-based interventions designed to detect, prevent, and treat perinatal depression. As already noted, PPD has negative consequences on the emotional well-being and health of the mother, the unborn baby, and the infant, and without proper care, mothers may continue to suffer from it for months or years (Jahan et al., 2021; Slomian et al., 2019). The process of making the Postpartum Depression Intervention (PPD-PI) available to others was initiated through training courses for professionals in contact with perinatal women to provide them with the tools to identify and attend to women with PPD symptoms. Objective The study aimed to evaluate the Postpartum Depression Prevention Intervention (PPD-PI) implementation process among professionals caring for perinatal women in various contexts. As part of the implementation process, satisfaction with the training course to conduct the PPD-PI was measured. Implementation was evaluated through how each professional perceived the uptake of the intervention in their work environment, including usefulness, barriers, adaptation, perceived benefits for perinatal women. The question was also raised as to whether there were differences in these aspects depending on the institutions to which they were affiliated. Evidence shows how norms, expectations, and work climate can affect the uptake of evidence-based practices (Aarons et al., 2011). It should be noted that although implementation is generally understood as an institutional decision (Rabin et al., 2008), in this case, the trained professionals made the decision. The study data will enhance understanding of both the barriers and enablers in implementing evidence-based interventions in various perinatal healthcare contexts (such as public and private institutions and NGOs). Design This is a descriptive, exploratory study. Participants The sample comprises one hundred twenty professionals who passed the PPD-PI course between 2016 and 2022. Entry requirements include holding a professional degree and working with perinatal women (such as psychologists, general practitioners, psychiatrists, social workers, and nurses) in the public and private sectors, nongovernmental organizations (NGOs), or the private practice. Completion of 90% of the activities is an accreditation requirement. Measurements Sociodemographic Characteristics This information was retrieved from the Application for Registration in the online2 PPD-PI Course obtained from all applicants to courses taught by the Directorate of Epidemiological and Psychosocial Research (DIEP) of the Ramón de la Fuente Muñiz National Institute of Psychiatry (INPRFM), which collects data on age, educational attainment, profession, workplace, and reasons for applying for the course. Course Completion Questionnaire At the end of the training course, participants answered a satisfaction questionnaire on the same platform3. Four questions were used to explore the achievement of objectives, the acquisition of knowledge necessary for the implementation of the intervention, and the perceived importance of complementary activities, such as forums. Follow-up Questionnaire A questionnaire with sixteen open and closed questions was designed to evaluate the intervention’s uptake. It explores whether the intervention was implemented, whether it was delivered in a group or individual setting, its usefulness to participants’ professional work, barriers encountered in its uptake, adaptations made to meet the demands of their population, and benefits perceived by users. Procedure At the end of each course, participants shared their experiences in providing the intervention and their observations through a questionnaire sent by email. Administration of the Follow-up Questionnaire There were two questionnaire administration waves: one in January 2019 to professionals who had completed the PPD-PI course between 2016 and 2019 and the second in January 2023 to those trained between 2020 and 2022. The invitation to complete the questionnaire, the informed consent form, and the questionnaire were sent to the email registered for the course. Postpartum Depression Prevention Intervention (PPD-PI) Next, we will discuss the background of the psychoeducational intervention in which health professionals are trained. The intervention is organized and described in a set of books designed for participants (Lara & García-Hubard, 2024), and for the facilitator (Lara et al., 2022) including the information, checklists, and worksheets required for its implementation. Based on the results of a previous study (Lara et al., 2003), an individual system was devised whereby each participant receives information on how to use the self-help manual (Lara & García-Hubard, 2024), and provide follow-up for feedback and support (Lara et al., 2022), The PPD-PI implemented during pregnancy in a sample of women at risk of depression had proved capable of reducing the incidence of depression (SCID, BDI-II) and was evaluated by those who received it as having a “moderate” to “major” influence on their well-being, depression, current problems, role as mothers and relationship with their babies (Lara et al., 2010). The course content, questionnaires, assignments, feedback and forums are presented on a Moodle platform. An expert PPD facilitator guides the course, provides feedback, support and information through forums and remote sessions, monitors individual performance and evaluates each participant’s achievement of the goals. Data Analysis Comparisons were made between those who did and did not answer the follow-up questionnaire on sociodemographic characteristics: t-tests for age and chi-square for the rest. To determine differences about course satisfaction among the professional’s workplace, test Kruskall-Wallis was used. All analyses were performed using SPSS 21 for Windows. Answers to the open questions about the usefulness of the information, adaptations made to the intervention, barriers to implementation, and perceived benefits in women who received the intervention were analyzed by constructing categories using the “categorization of meanings” technique proposed by Kvale and Brinkmann, 2009, which enables one to identify common themes and shared experiences. The categories established deductively were a) adaptations made, b) barriers to implementation, and c) perceived benefits in women receiving the intervention. We adhered to the ethical principles suggested by the Council of International Organizations of Medical Sciences (Council of International Organizations of Medical Sciences [CIOMS, 2016]). This is a minimal-risk study since participants were adults with a bachelor’s or graduate degree or a specialization who decided to collaborate as evaluators or reviewers. They were not subordinate to the study researchers and were not obliged to disclose personal information. Regarding data protection, the application form for entry to the course states that the Directorate of Epidemiological and Psychosocial Studies of the INPRFM is the obligated subject responsible for processing personal data collected following the Personal Data Protection Act.4 In the registration form, applicants must check the box labeled “I have read and accepted the privacy notice.” They are informed that the institution will use the data solely for reports, scientific publications, and statistical analysis, which will not include the names of participants. Follow-up of participants was an extension of the exchanges that had taken place during the course. The informed consent letter was emailed with the invitation, stating that agreement to participate would be provided by completing and returning the questionnaire. The procedure for presenting the informed consent form to the participant is based on the recommendation of CIOMS Guideline Nine, obtaining informed consent. Essential information for potential research subjects: objective, methods, expected benefits, and being informed about the general outcome and results of the research. Demographic Characteristics One hundred and twenty professionals received training. The mean age was 35.7, and 93.5% were women. The majority held bachelor’s degrees (49.2%) or higher (50.8%), mainly in psychology (70.8%), and most worked in public institutions (60.0%) and lived in the capital, Mexico City (77.5%). Comparisons between the characteristics of respondents to the follow-up questionnaire (n = 71) and non-respondents (n = 49) yielded no significant differences in any of the categories (Table 1). Table 1 Demographic Characteristics of Trained Professionals 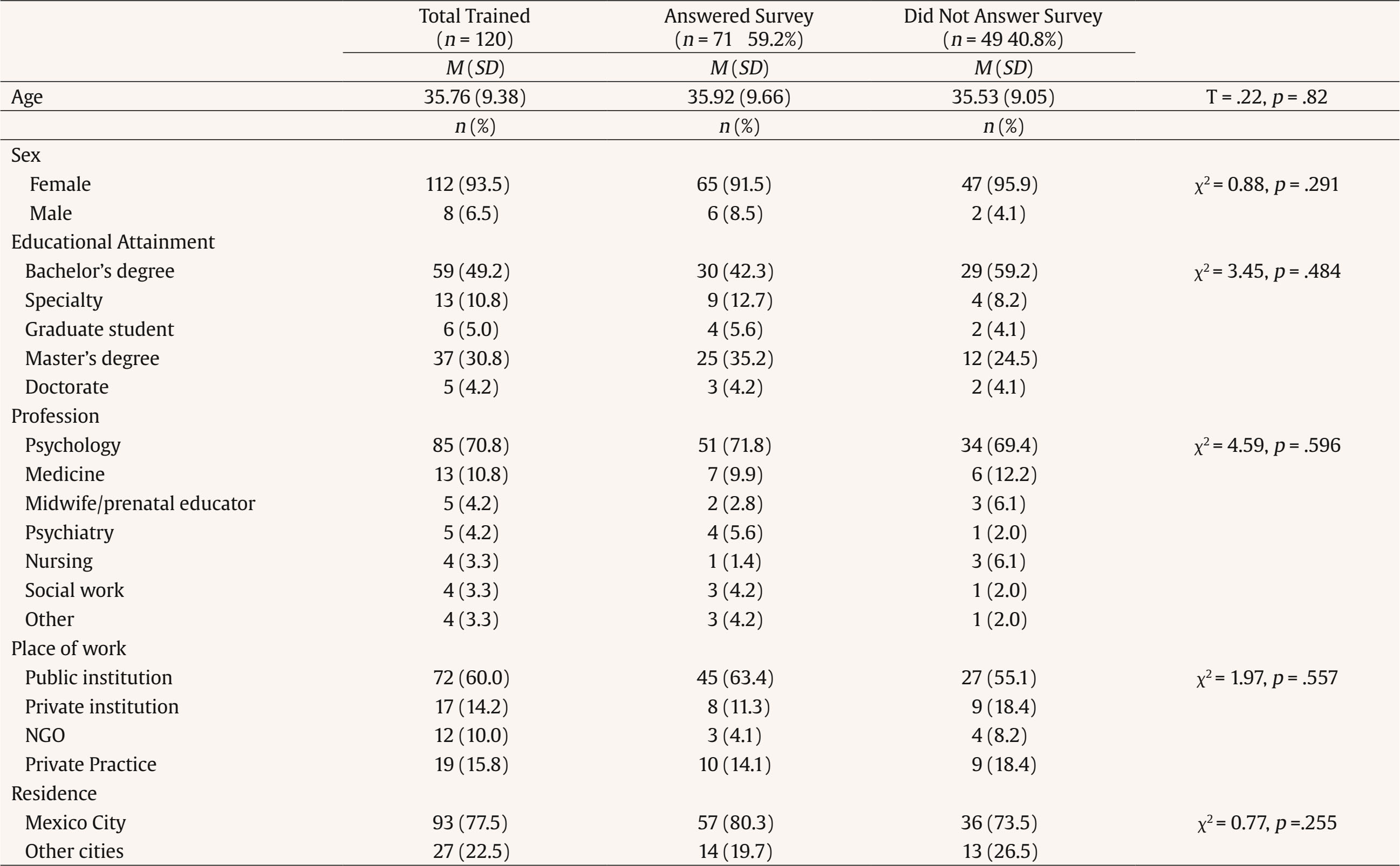 Satisfaction with the Training Course Participants generally gave scores of five or close to this maximum value to the four aspects evaluating satisfaction with the course: achievement of objectives, knowledge acquisition, skill development, and group activities. No statistical differences were observed between professionals from different workplaces, whether public and private institutions, NGOs, or private practice (Table 2). Table 2 Satisfaction with Training Course (N = 71)  Implementation of the Intervention In the follow-up questionnaire, 56.7% of the professionals reported implementing the intervention at least once. The highest percentage of those who had done so were professionals from public institutions (66.7%), followed by those in private practice (60%). As to whether learning the interventions was useful in their everyday work, the majority, between 87.5%and 100% of those who had a job, answered affirmatively Eleven implemented it in groups and twenty-nine individually. In all, they estimated that 318 women had participated in the intervention in groups while 139 had received it individually. Usefulness of Information As to why it had been useful to them, the main categories of responses were: 1) they acquired the knowledge and tools to support women during the perinatal period, 2) they developed greater empathy towards the conditions women undergo during this period, and 3) they carried out other actions related to perinatal depression, such as giving courses or promoting research on the issue (Table 3). Some participants said that the training had not been helpful because they needed more time to get involved with the women they cared for, either because they were focused on their training or did not work with it. Table 3 Usefulness of Course Information 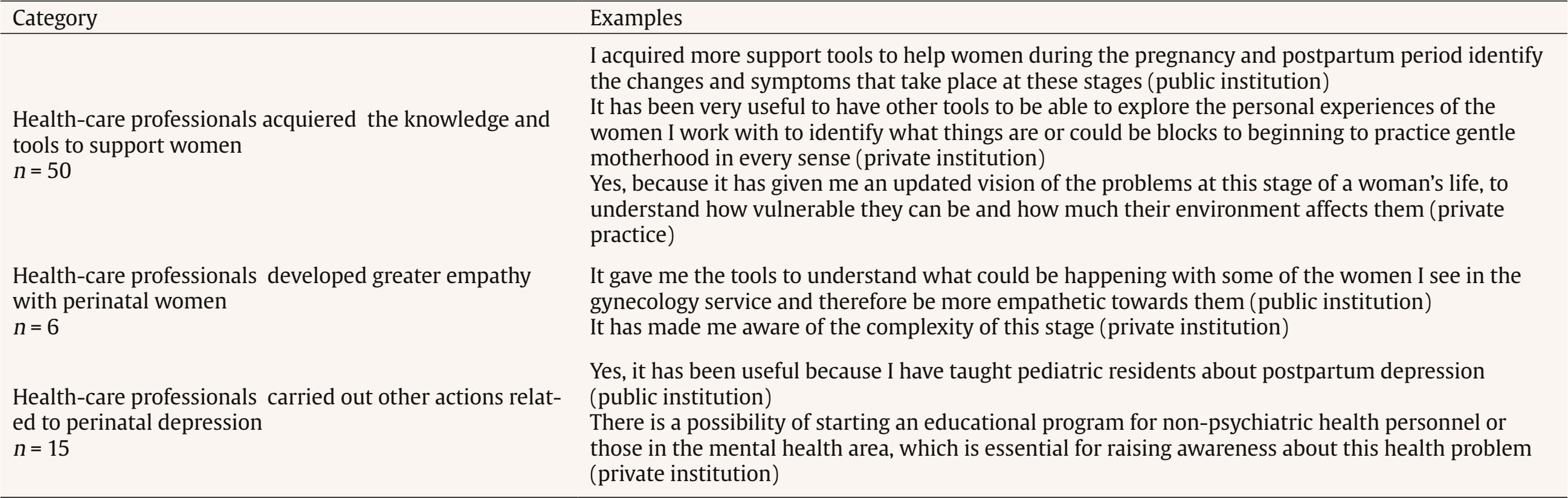 Adaptations Most (90.5%) made some adaptations when implementing the intervention. The main adaptations mentioned were: 1) only selecting content relevant to the case, 2) reducing the number of sessions, and 3) including other therapeutic components, such as pharmacotherapy and family therapy; incorporating other family members and adding content (such as breastfeeding, life history, and couple relationship issues) (Table 4). Table 4 Adaptations Made to the Intervention 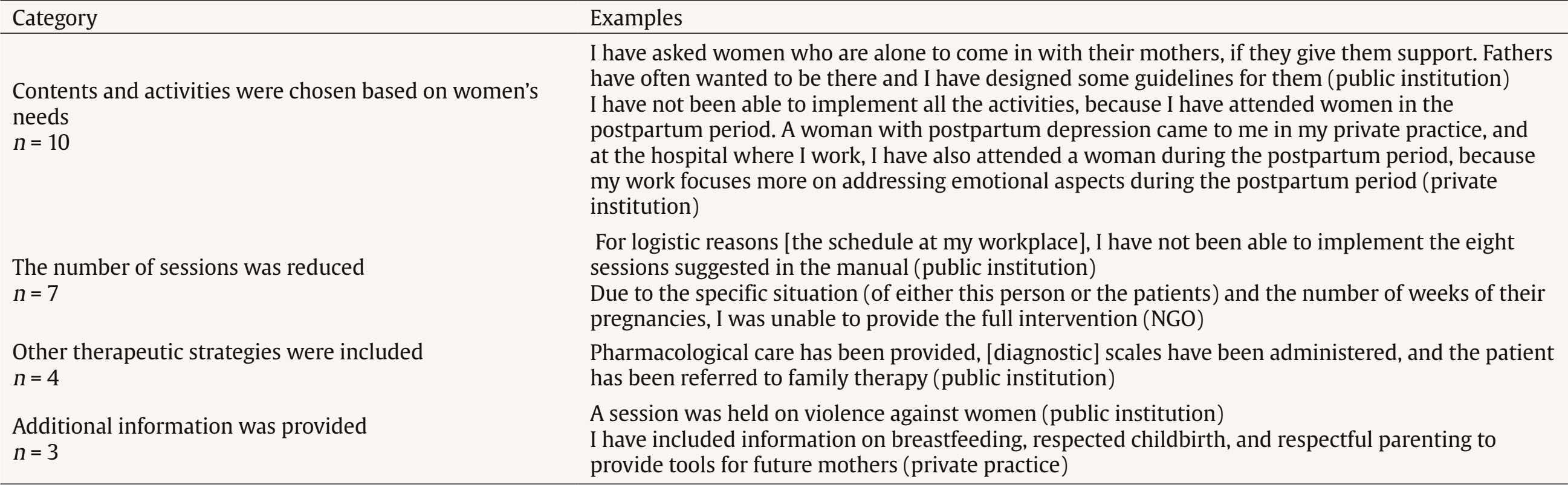 Barriers to Implementation The challenges faced in initiating the implementation of the PPD-PI included a lack of time and resources, such as needing a designated space. Additionally, due to administrative changes, their institutions provided insufficient support. Furthermore, some of the women attending the institution demonstrated reluctance to seek help (Table 5). Table 5 Barriers to Implementation 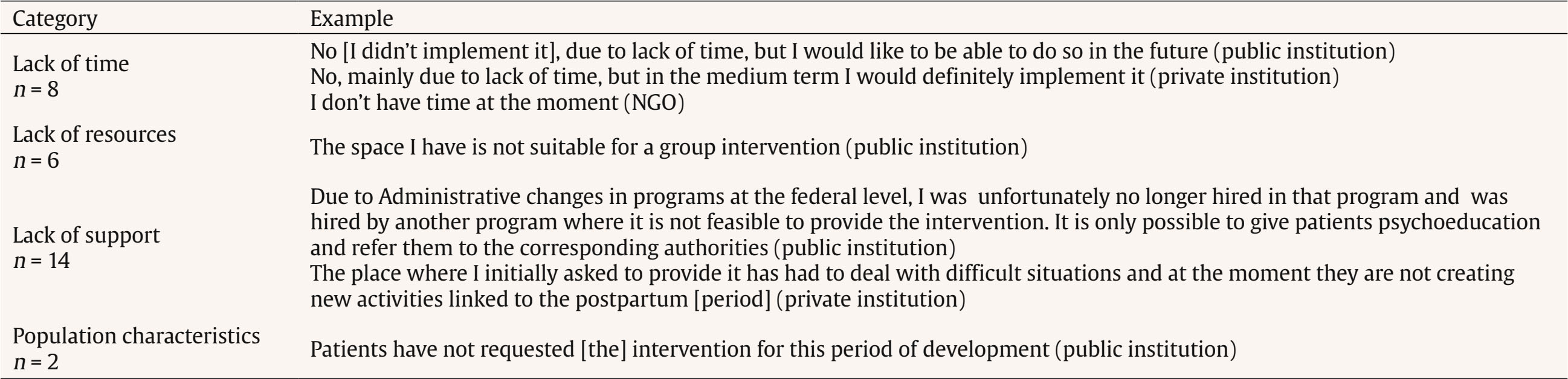 Benefits Perceived in Women Receiving the Intervention The professionals who reported that they had implemented the intervention perceived the following benefits in these women: they felt more empowered, their mood improved, they developed more positive feelings towards their role as mothers, engaged in better self-care, and achieved better family relationships (Table 6). Table 6 Benefits Perceived by Professionals in Women who Received the Intervention 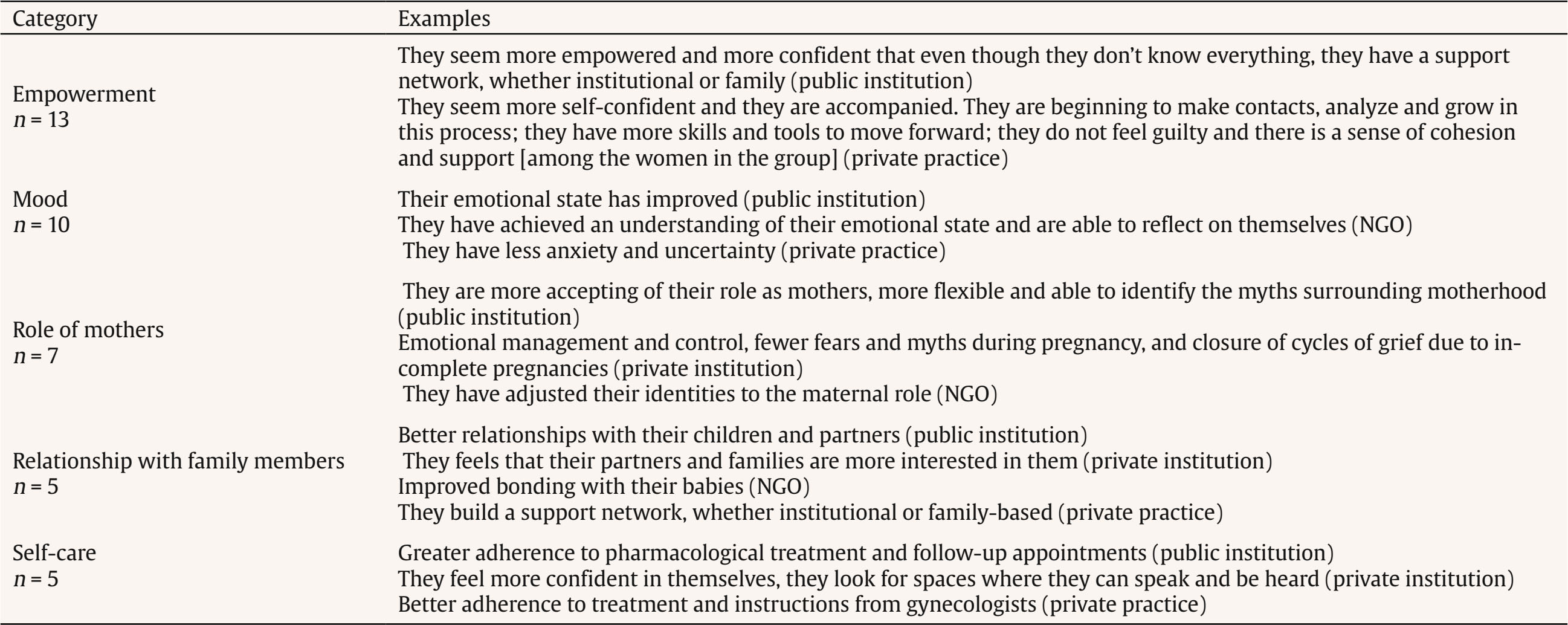 Perinatal depression, the most frequent complication of pregnancy and the postpartum period is associated with adverse obstetric, maternal, and neonatal effects (Woody et al., 2017). Nevertheless, in many countries, including Mexico, PPD is neither systematically addressed nor treated as a health priority (Navarrete et al., 2022). Furthermore, while evidence-based interventions (EBIs) are poorly implemented in the health systems and professional practice of High-Income Countries (HICs) (Battaglia & Glasgow, 2018), the challenges are significantly compounded in Low- and Middle-Income Countries (Martínez et al., 2016). In this context, the objective of the study was to evaluate the implementation of the PPD-PI in professionals attending perinatal women in various contexts (public and private sectors, NGOs and private practice), regarding satisfaction with the course, its usefulness, barriers and adaptations to its uptake in their work environment. The professionals who received the training expressed satisfaction with the course in achieving objectives, acquiring knowledge, developing skills, and group activities, with no significant differences between work environments. Overall, training provided healthcare professionals with the tools to support women during pregnancy and postpartum and to address their mental health, while the training course and the accompanying educational materials constituted a useful strategy for disseminating PPD-PI among the target population. Developing educational materials and conducting educational sessions is a common implementation strategy to support women during the perinatal period (Taple et al., 2022). The professionals who received the training consider that improving the knowledge and skills required to identify perinatal depression in obstetric service providers is a fundamental part of any intervention to ensure that perinatal women receive better care (Byatt et al., 2021). Half (56.7%) of the professionals reported having implemented the intervention. In the literature, implementation refers to an organization or community’s decision to commit to or begin adopting an evidence-based intervention (EBI) (Rabin et al., 2008). In this case, the professionals decided to implement it in addition to their professional and institutional responsibilities. These data indicate a clear need for tools to support the perinatal women they serve. However, the uptake of the PPD-PI was evaluated very generally without requesting specific information on the situations in which it was implemented, or the characteristics of the population to which it was provided. Despite this shortcoming, what is important about these data is that at least some elements of the course proved useful for the professional’s attending women whom they thought had symptoms of depression or other emotional problems in a range of contexts. Having been trained in the PPD-PI was useful in their everyday work for the majority (87.5%-100%) of those who were employed. The first reason it was useful for them has to do with the first barriers to perinatal mental health care: lack of knowledge (Tabb et al., 2015). In this respect, the trained professionals thought it was useful because they acquired the knowledge and tools to support the women they attended during this period. The second reason was that they developed greater empathy towards the women they attended. This result is a pivotal finding given the lack of empathy, disinterest, and prejudice perinatal women perceive regarding their mental health in prenatal care (Lara et al., 2014; Navarrete et al., 2022). Most participants (90.5%) adapted certain aspects of the PPD-PI to implement it effectively within their work context. The main changes involved the sequence of topics, the number of sessions, and the choice of activities suited to their specific situation. Bina et al. (2018) noted that the rigidity often associated with EBIs hinders their implementation in primary care services. This is especially apparent in the number of sessions needed and the topics to be covered. The latter indicates that it is essential to tailor EBIs to the specific needs of the context for effective implementation in everyday practice. This adaptation allows researchers to advance to the next stage, which involves disseminating the intervention, implementing it, and continuing its development (Wampold & Imel, 2015). The next step in the implementation process is to evaluate the modified interventions to reduce the risk of postpartum depression and compare them with the original design (Lara et al., 2010). The need for adaptations raises essential questions about fidelity and the effectiveness of interventions aimed at preventing depression. This issue is significant not only for the beneficiaries but also for the professionals responsible for making adaptations. These individuals must determine which changes to implement while adhering to the original intervention (von Thiele Schwarz et al., 2020). The authors highlight the challenge of balancing fidelity and adaptation when applying EBIs to ensure they are suitable for specific contexts while achieving results comparable to the original version. In the case of PPD-PI, the initiative was initiated by professionals working with perinatal women rather than by the institutions they are affiliated with. To have the support of their institution to implement the program, health professionals must adjust the intervention to meet their pre-established daily activities. Barriers to implementation are widely recognized, as much evidence-based interventions (EBIs) have not been designed for a single perinatal context (Overbeck et al., 2016). The practitioners in our study identified a lack of time, resources, and institutional support as the most significant limitations. Other studies have also noted an excessive institutional workload as a barrier to the implementation of health programs (Al-Abri et al., 2023). Implementing the intervention is not only an institutional decision, which creates barriers for professionals who wish to provide it. This highlights the need to advocate for decision-makers to acknowledge the importance of this type of intervention. Additionally, there is a need for a regulatory framework that supports its adoption and implementation. The professionals observed improvements in the women who received the intervention, although this assessment is subjective and not based on the evaluation of depressive symptoms, health professionals observe that PPD-IP benefits the expression of positive emotions in perinatal women. The professionals perceive the women as feeling more empowered, experiencing improved moods, having more positive feelings towards their roles as mothers, and engaging in more self-care behaviors. These findings are consistent with the subjective evaluations reported by the women who participated in the controlled study in which the PPD-IP was evaluated (Lara et al., 2010). The health-care professionals found the content to be useful, as it equipped them with the knowledge and strategies necessary for working with perinatal women who may be experiencing depression. Most of these professionals needed to make changes to adapt the intervention to their specific work environments and to overcome barriers, mainly due to a lack of institutional support. They noted improvements in the women they served, aligning with the program’s objectives. These findings constitute an initial approach to implementing EBIs in Mexico, but they have several limitations. The most significant limitation is the general nature of the questions in the questionnaire, which need to address how PPD-PI was applied. Additionally, the study did not measure the participants’ levels of depression or any potential changes in those levels. On an international scale, there is growing concern regarding the need for rigorous qualitative evaluations of the implementation of EBIs (Toews et al., 2016). This paper makes a modest contribution to the limited research on the and implementation of EBIs, particularly concerning the phenomenon of PPD and its detection, prevention, and treatment within health systems. The aim is to show what is achievable and use these findings as a foundation for improving strategies to address this issue. Highlights
Conflict of Interest The authors of this article declare no conflict of interest. Notes Cite this article as: Lara, Mª. A., Navarrete, L., Medina, E., Ruiz, E., Tiburcio, M., & Fuentes, P. (2026). Barriers to the uptake of a psychoeducational intervention to prevent postpartum depression: An exploratory study. Clinical and Health, 37, Article e260724. https://doi.org/10.5093/clh2026a10 1 Translating in this context means condensing information about innovations and converting it into userfriendly formats (Wandersman et al., 2008). 2 From Research Project EP09 4294.0: Training of Counselor Networks Based on Successful Community Intervention Models. Principal Investigator: Dr. Patricia Fuentes. 3 Final Evaluation Card for the Courses for the Dissemination of Community Intervention Models of the DIEP. Principal Investigator: Dr. Patricia Fuentes. 4 General Law on the Protection of Personal Data Held by Obligated Subjects. Official Gazette of the Federation, January 26, 2017. https://www.diputados.gob.mx/LeyesBiblio/pdf/LGPDPPSO.pdf References |
Cite this article as: Lara, M. A., Navarrete, L., Medina, E., Ruiz, E., Tiburcio, M., & Fuentes, P. (2026). Barriers to the Uptake of a Psychoeducational Intervention to Prevent Postpartum Depression: An Exploratory Study. Clinical and Health, 37, Article e260724. https://doi.org/10.5093/clh2026a10
Correspondence: laracan@imp.edu.mx ((Mª. A. Lara).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Imprimir
Imprimir Enviar
EnviarALERTA POR E-MAIL
La Revista de Clínica y Salud está distribuida bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObra Derivada 4.0 Internacional.com








