


Mental Health, Well-being, and Sexual Health in Recurrent Pregnancy Loss: A Systematic Review
[La salud mental, el bienestar y la salud sexual en la pérdida recurrente del embarazo: una revisión sistemática]
Joan Vicent Sánchez-Ortí1, 2, Ascensión Bellver-Pérez1, 3, & Evelyn Moreno-Maldonado1
1Faculty of Psychology, University of Valencia, Valencia, Spain; 2INCLIVA - Health Research Institute, Valencia, Spain; 3University and Polytecnic La Fe Hospital, Valencia, Spain
https://doi.org/10.5093/clh2026a9
Received 20 September 2025, Accepted 23 February 2026
Abstract
Recurrent pregnancy loss (RPL) is associated with significant psychological burden in women and couples. This systematic review examines the impact of RPL on mental health, quality of life, sexual health, and sleep using evidence from observational studies. A total of 23 peer-reviewed studies using validated psychometric tools were included. Participants were mostly women (n = 12,759; aged 19-47) and some men (n = 1,419; aged 20-49). Of the women, 60.6% had RPL, while 31% had no RPL. Among men, 83.4% were partners of women with RPL. Results showed that women with RPL experienced significantly higher levels of anxiety, depression, and stress, as well as reduced sexual health, sleep quality, and overall well-being. Social support was identified as a key protective factor. However, variation in methods and measurement tools limited comparability across studies. The impact on couples, especially male partners, remains underexplored due to scarce data. Findings underscore the urgent need for integrated, multidisciplinary psychological support in healthcare settings to improve mental health and quality of life for individuals and couples affected by RPL.
Resumen
La pérdida recurrente del embarazo (PRE) o aborto recurrente se asocia con una carga psicológica significativa en las mujeres y las parejas. Esta revisión sistemática examina el impacto de la PRE en la salud mental, la calidad de vida, la salud sexual y el sueño utilizando pruebas procedentes de estudios observacionales. Se incluyeron 23 estudios revisados por pares que emplearon instrumentos psicométricos validados. La mayoría de los participantes fueron mujeres (n = 12,759; 19-47 años) y en menor medida hombres (n = 1,419; 20-49 años). Entre las mujeres, el 60.6% presentaba antecedentes de PRE, mientras que el 31% no los tenía; en el caso de los hombres, el 83.4% tenía como pareja una mujer con PRE. Los resultados indicaron que las mujeres con PRE experimentaban niveles significativamente más altos de ansiedad, depresión y estrés, así como una disminución en la salud sexual, la calidad del sueño y el bienestar general. Se encontró que el apoyo social era un factor protector clave. Sin embargo, la heterogeneidad de los métodos y de los instrumentos empleados limitó la comparabilidad de los estudios. El impacto en las parejas, en particular en los hombres, continúa siendo poco explorado debido a la escasez de datos. Los resultados destacan la necesidad urgente de integrar un apoyo psicológico desde un enfoque multidisciplinar en los servicios de salud con el fin de mejorar la salud mental y la calidad de vida de las personas y parejas afectadas por PRE.
Palabras clave
Aborto recurrente, Salud mental, Calidad de vida, Salud sexual, Sueño, ParejasKeywords
Recurrent pregnancy loss, Mental health, Quality of life, Sexual health, Sleep, CouplesCite this article as: Sánchez-Ortí, J. V., Bellver-Pérez, A., & Moreno-Maldonado, E. (2026). Mental Health, Well-being, and Sexual Health in Recurrent Pregnancy Loss: A Systematic Review. Clinical and Health, 37, Article e260723. https://doi.org/10.5093/clh2026a9
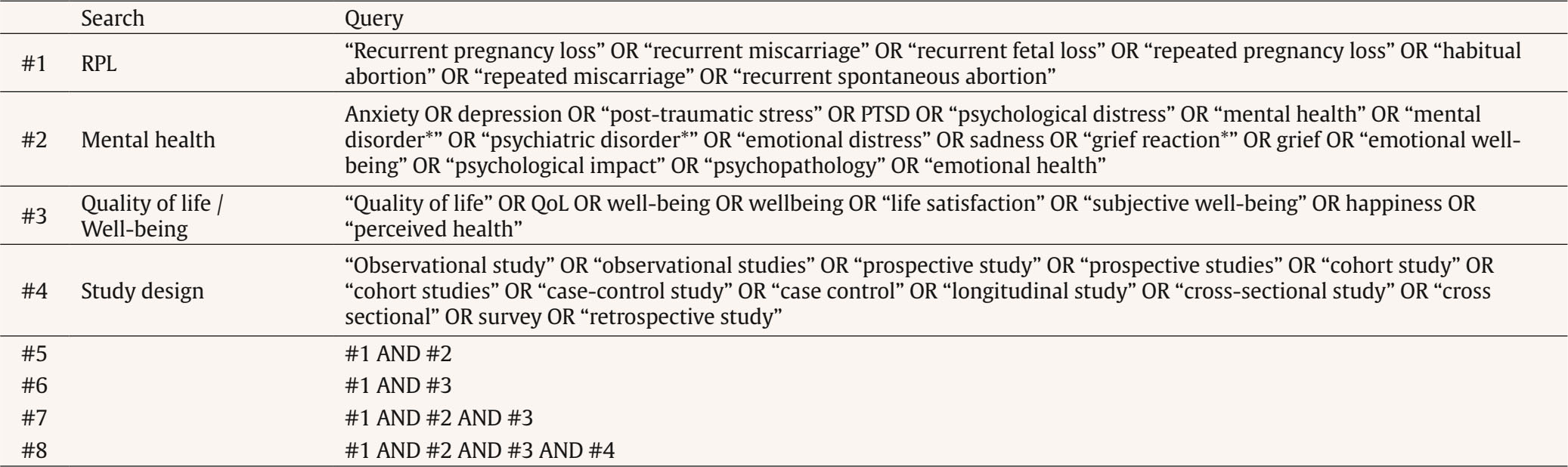
Correspondence: ascension.bellver@uv.es (A. Bellver-Pérez).Repeated pregnancy loss (RPL) is a growing common problem affecting about 25% of the female population of reproductive age (du Fossé et al., 2020). It is defined as the occurrence of two or more pregnancy losses before 20-24 weeks of gestation (Genovese & McQueen, 2023). RPL has a profound psychosocial impact that may affect the well-being of these women, couples and their babies during pregnancies subsequent of these losses (Hunter et al., 2017). However, it has historically been overlooked in healthcare settings (Bilardi & Temple-Smith, 2023). There are a multitude of psychosocial and environmental risk factors related to RPL. Recent literature showed that the key psychosocial risk factors are, first, social pressure to comply with traditional gender roles. There is an ingrained expectation that women must become mothers in order to feel fulfilled and thus meet social and family standard (Quenby et al., 2021). Second, gender stereotypes also play an important role. Pernicious judgments that associate women’s reproductive capacity with their personal worth have a negative impact on women’s self-esteem and self-image, exacerbating their emotional distress. Third, the social stigma associated with infertility increases feelings of isolation and loneliness that can lead women to feel excluded in different areas of personal development (e.g., social or occupational) (Fernández-Sola et al., 2020). Lastly, stress generated by the search for pregnancy is an important environmental risk factor for RPL. The perceived stress is higher when it is associated with difficulties in conceiving naturally and fertility treatments (e.g., artificial insemination and in vitro fertilization) are used (Aimagambetova et al., 2020). These experiences negatively impact emotional well-being, affecting quality of life and interpersonal relationships in this population (Bilardi et al., 2021) and can also have lasting negative effects on mental health (Cuenca, 2023). Recent studies suggest that women who have experienced RPL have an increased risk of developing anxiety and depression symptoms compared to those who have not experienced RPL (Inversetti et al., 2023). Likewise, post-traumatic stress is a psychological response that often develops as a result of RPL. Recent evidence reports that people with RPL may experience symptoms of re-experiencing, avoidance, and increased arousal more frequently than the general population (Shen et al., 2024). These findings have also been observed in close family members, especially partners of women who have suffered RPL. A recent study has shown that they may experience feelings of helplessness and frustration, which, in turn, may result in a worsening of their mental health and quality of life (Di Nallo, 2025; Inversetti et al., 2025). Understanding these circumstances is crucial to providing adequate support to those suffering from these painful experiences related to RPLs (Turesheva et al., 2023). However, the overall interpretation of the above results is hampered by methodological variability (e.g., recruitment methodologies, assessment tools, timing of assessments, and comparison groups), as well as variation across studies in terms of definitions of RPL, types of losses, and types of outcomes measured. This review expands on previous work by focusing exclusively on RPL using a strict definition, examining multiple psychosocial outcomes, and including both women and their partners using the most recent evidence. Our objective was to explore and synthesize current knowledge on the psychosocial impact of RPL on women and couples. We explored the frequency and intensity of mental health-related symptoms (e.g., anxiety, depression, stress), as well as the impact on well-being and quality of life. The present systematic review was conducted according to the guidelines of the latest version of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses, PRISMA 2020 (Page et al., 2021). Information Sources and Search Strategy The literature search was conducted between January 2014 and July 15, 2025, in MEDLINE through PubMed (National Library of Medicine, Bethesda, Maryland, USA), Science Direct and Scopus through the Elsevier platform (Elsevier B.V., Amsterdam, The Netherlands), and PsycINFO through the American Psychological Association (APA). Web of Science provided by Clarivate Analytics (Philadelphia, Pennsylvania, USA). This approach was considered because the field of study is constantly evolving and this time period ensures that the review includes studies that respond to recent sociocultural changes and current theoretical paradigms. The search terms used include those related to RPL (e.g., “recurrent pregnancy loss”, “recurrent miscarriage”, or “recurrent fetal loss”), constructs associated with mental health and well-being status (e.g., “anxiety”, “depression”, “stress”, “quality of life”, and “psychopathology”), and the study design (e.g., “observational”, “prospective”, and “case-control”) (see Supplementary Material in Appendix). Eligibility Criteria We included original studies that (i) assessed the impact of RPL on different constructs related to mental health (e.g., anxiety, depression, stress) and well-being status (e.g., psychopathology, quality of life) in women with RPL compared to women (or couples) without RPL, using standardized psychological assessment instruments; (ii) examined women or couples with RPL, defined as ≥ 2 gestational losses, unless subgroup analyses for RPL were reported separately; (iii) were published in English; and (iv) had an observational study design (e.g., case-control, cohort). In addition, only data from peer-reviewed articles were included, as defined on a journal’s website or based on the full text of the article. We excluded studies that (i) only explored biomedical aspects associated with RPL; (ii) evaluated RPL as a single miscarriage; (iii) did not include measurement of constructs related to mental health and/or well-being status; (iv) did not have a design that could be included in a systematic review such as review articles and meta-analyses, case series, opinion articles or dissertations; or (v) lacked a full-text version. Study Selection and Data Extraction Two researchers (EM-M and JVS-O) independently and masked proceeded to review the titles and abstracts of the non-duplicate articles, evaluating their eligibility according to the selection criteria. In the next step, the reviewers examined the full texts of the studies likely to be included in the review to identify eligible studies. In case of disagreement among the reviewers, discussion and consensus were reached with the third author (AB-P). Relevant data from included studies were extracted using Microsoft Excel 2010. The information extracted from the studies included: publication details (authors, year and country), study type (where possible timing of assessment), characteristics of the population and sample groups (sample age, age, and number of RPL), and study outcomes (levels of anxiety, depression, stress, quality of life, and well-being measured and method of measurement). Descriptive analyses were made by comparing population characteristics and outcomes of the included studies. Validity and reliability measures reported in the studies were estimated using Pearsons r and derived correlations (e.g., biserial-point correlation). Risk of Bias and Quality Assessment The risk of bias and quality assessment of the included case-controls and cohorts studies regardless of whether they were cross-sectional or longitudinal were assessed using the Newcastle Ottawa scale (NOS; Wells et al., 2008). For cohort studies, this scale assigns points for representativeness of the exposed and control groups, adequate ascertainment of exposure, clarity of the absence of outcomes at study start, comparability of groups based on study design and analysis, blinded assessment or record linkage to confirm study outcomes, the sufficiency of follow-up duration to observe the outcomes of interest and reporting of a sufficiently low withdrawal rate that would not threaten a significant risk of bias to the study. For case-control studies, this scale assigns points for adequate case definition, representativeness of the cases, adequate selection and definition of controls, comparability of cases and controls based on the design or analysis, adequate ascertainment of exposure, same method of ascertainment for cases and controls, and same (non-response) rate for both groups. A maximum of nine points can be assigned. The quality of the information included in the studies was assessed using the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) tool for observational cohort, case-control, and cross-sectional studies (von Elm et al., 2007). It consists of 22 items, and each item is rated as affirmative, negative, not available, or not applicable. The items cover various aspects of the articles, such as the title and abstract (point 1), the introduction (points 2 and 3), methodology (points 4-12), results (points 13-17), and discussion (points 18-21), as well as other relevant sections (point 22 on funding). Three categories were used to rate the quality of the studies: good, fair, and poor quality, according to criteria proposed by STROBE. In both assessments, disagreements were discussed until consensus was reached and, when needed, were resolved by a third author (AB-P). The STROBE checklist was used exclusively to assess the completeness of reports. The literature search yielded 2,967 results in total. Of these, 1,843 were duplicates with a further 1,118 articles as they (a) did not have full text in English, (b) were not objective assessment of mental health and well-being, (c) were not RPL sample, or (d) were not original articles, leaving 23 articles for full-text screening. The PRISMA flow diagram is presented in Figure 1. Figure 1 PRISMA 2020 Flow Diagram for New Systematic Reviews which Included Searches of Databases, Registers and Other Sources. 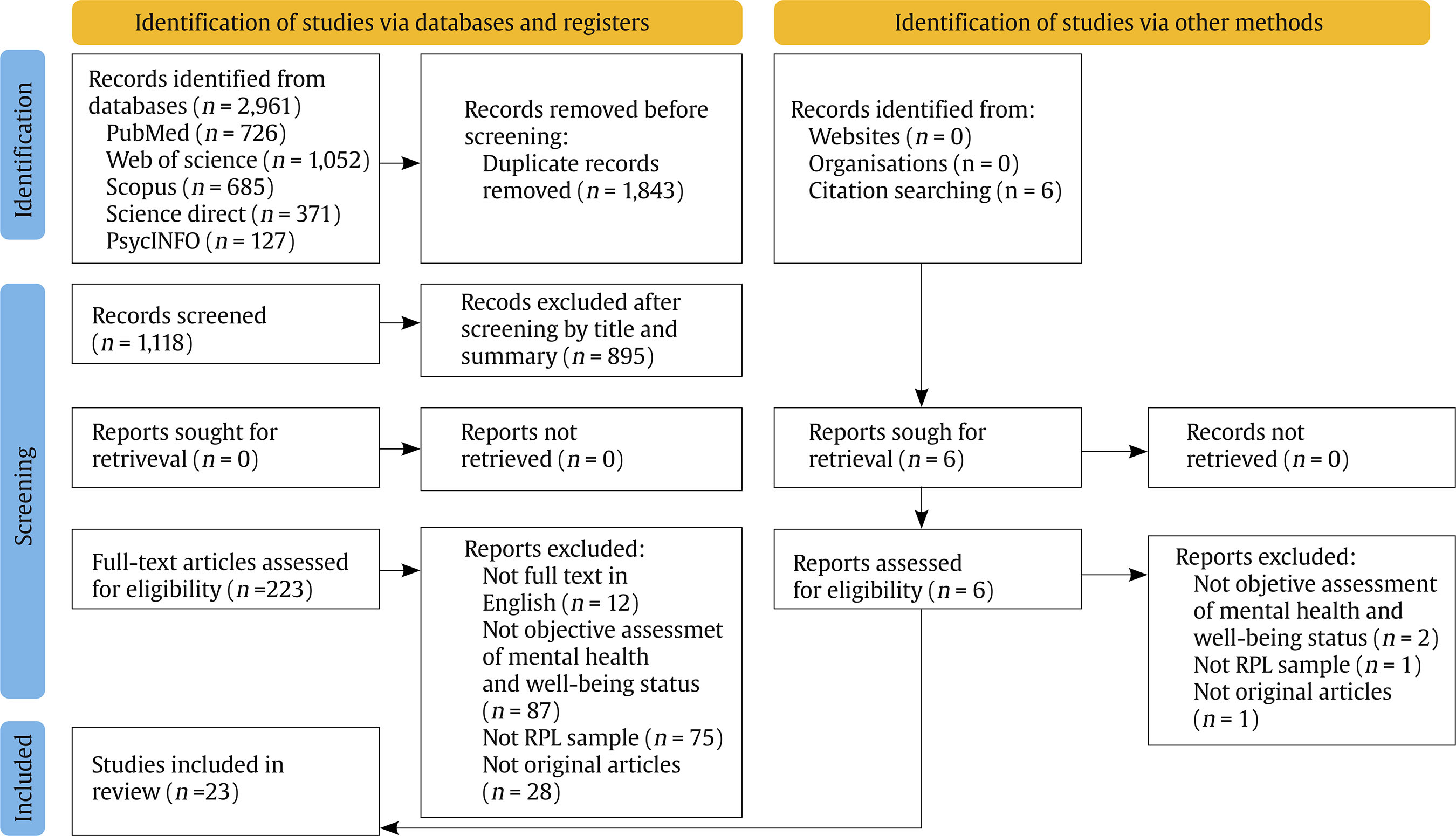 Source: Page et al. (2021). https://doi.org/10.1136/bmj.n71 This study is licensed under CC BY 4.0. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/ Characteristics of the Included Studies As detailed in Table 1, 30.4% (k = 7) of the studies were conducted in China, 17.3% (k = 4) in Iran, 13% (k = 3) in Denmark, 8.7% (k = 2) in Germany, whereas countries such as the Turkey, Kazakhstan, Lithuania, India, Romania, Nigeria, and USA contributed one study each (4.3%). Table 1 Overview of the Main Characteristics of the Included Studies  Edad (x ± σ), Sexo (% femenino). Abbreviations: 1PL = One Pregnancy Loss; BMI = Body Mass Index; CES-D = Center for Epidemiologic Studies Depression Scale; CI = Confidence Interval; CISS = Coping Inventory for Stressful Situations; DASS-21 = Depression Anxiety Stress Scales – 21; DSCS = Dyadic Sexual Communication Scale; EPDS = Edinburgh Postnatal Depression Scale; FQCI = Fertility Quality of Communication Inventory; FSFI = Female Sexual Function Index; GAD-7 = Generalized Anxiety Disorder – 7; HADS = Hospital Anxiety and Depression Scale; HSS = High Social Support; IES-R = Impact of Event Scale – Revised; IIEF-5 = International Index of Erectile Function – 5; IPV = Intimate Partner Violence; ISI = Insomnia Severity Index; ISS = Index of Sexual Satisfaction; IUS = Intolerance of Uncertainty Scale; L/MSS = Low/Moderate Social Support; MDI = Major Depression Inventory; MIQ = Marital Intimacy Questionnaire; MIF = Medical Infertility History; non-RPL = Women without Recurrent Pregnancy Loss; OR = Odds Ratio; PPP = Psychological Profile Parameters; PRAQ-2 = Pregnancy-Related Anxiety Questionnaire – Revised; PSS = Perceived Stress Scale; PSSS = Perceived Social Support Scale; PSQI = Pittsburgh Sleep Quality Index; RPL = Recurrent Pregnancy Loss; RR = Relative Risk; SAS = Self-Rating Anxiety Scale; SCL-25 = Symptom Checklist – 25; SCL-90 = Symptom Checklist – 90; SCL-90-R = Symptom Checklist - 90 – Revised; ScreenIVF = Screening Instrument for Subfertility Patients; SDS = Self-Rating Depression Scale; SF-36 = Short Form - 36 Health Survey; SII = Sexual Interaction Inventory; STAI = State-Trait Anxiety Inventory; VDAS = Visual Analogue Scale for Anxiety; x = arithmetic media. Most studies (k = 18) were cross-sectional, of which 61.1% (k = 11) (Abbaspoor et al., 2016; Gül & Kirka, 2021; He et al., 2019; Hedegaard et al., 2021; Kolte et al., 2015; Kulshreshtha et al., 2023; Liu et al., 2024; Van et al., 2023; Voss et al., 2020; T. Wang et al., 2023; Zhang et al., 2016) were comparative and correlational, the 27.8% were only comparative (k = 5) (R. Gao et al., 2022; Ghorbani et al., 2022; Kuhlmann et al., 2023; Nitu et al., 2023; Tavoli et al., 2018), and the other 11.1% were only correlational (k = 2) (L. Gao et al., 2020; Kukulskien & Žemaitien, 2022). The remaining studies were (k = 4) case-control studies, comparative, or correlational (Adib-Rad et al., 2019; Eleje et al., 2024; Issakhanova et al., 2023; Y. Wang et al., 2021), and another (k = 1) was a comparative prospective cohort study (Slot et al., 2022). Overall, 12.759 were women aged between 19 and 47 years (X = 32.9, SD = 4.8) were included, of which 60.6% had RPL, 3.2% had 1PL, 5.2% were women couples, and 31% did not had RPL. As for the men, a total of 1419 aged between 20 and 49 years (X = 34.2, SD = 3.7) were included, of whom 83.4% were female couples with RPL and 16.6% without RPL. Most of the studies assessed depressive symptoms (k = 12, 52.1%) (L. Gao et al., 2020, 2022; He et al., 2019; Hedegaard et al., 2021; Kolte et al., 2015; Kukulskien & Žemaitien, 2022; Kulshreshtha et al., 2023; Slot et al., 2022; Van et al., 2023; T. Wang et al., 2023; Y Wang et al., 2021; Zhang et al., 2016) using instruments such as the Edinburgh Postnatal Depression Scale (EPDS), Self-Rating Depression Scale (SDS), Major Depression Inventory (MDI), and Center for Epidemiologic Studies Depression Scale (CES-D). The 30.4% informed anxiety symptoms (k = 7) (L. Gao et al., 2020; Gül & Kirka, 2021; He et al., 2019; Kulshreshtha et al., 2023; T. Wang et al., 202; Y. Wang et al., 2021; Zhang et al., 2016) through the following tests Self-Rating Anxiety Scale (SAS), Visual Analogue Scale for Anxiety (VDAS), Generalized Anxiety Disorder-7 (GAD-7), and State-Trait Anxiety Inventory (STAI). Specifically, a study reported anxiety related to pregnancy (Kulshreshtha et al., 2023) measured with the Pregnancy-Related Anxiety Questionnaire – Revised (PRAQ-2), while another study informed mixed symptoms of anxiety and depression (Tavoli et al., 2018) through the Hospital Anxiety and Depression Scale (HADS). Regarding stress-related outcomes, the 21.7% reported symptoms related to perceived stress (k = 5) (Hedegaard et al., 2021; Kolte et al., 2015; Kulshreshtha et al., 2023; Slot et al., 2022; Van et al., 2023) using the questionnaire Perceived Stress Scale (PSS). Post-traumatic stress was measured (k = 2), using the Impact of Event Scale – Revised (IES-R) test, in the 8.7% of studies (Kuhlmann et al., 2023; Kukulskien & Žemaitiené, 2022). Two study showed mixed results for anxiety, depression, and stress measured with the following instruments Depression Anxiety Stress Scales-21 (DASS-21) (Eleje et al., 2024; Issakhanova et al., 2023). Moreover, the 8.7% informed on coping styles (k = 2) (Kuhlmann et al., 2023; Nitu et al., 2023), using the Fertility Quality of Communication Inventory (FQCI) and Coping Inventory for Stressful Situations (CISS). Approximately one-fifth (17.3%) of the studies reported general psychopathology (k = 4) (Abbaspoor et al., 2016; Adib-Rad et al., 2019; Nitu et al., 2023; T. Wang et al., 2023) using the following tests Symptom Checklist-25 (SCL-25), Symptom Checklist-90 (SCL-90), Symptom Checklist - 90 – Revised (SCL-90-R), and Psychological Profile Parameters (PPP). To a lesser extent, 13.4% of the studies (k = 3) reported on sleep quality (Gül & Kirka, 2021; Van et al., 2023; T. Wang et al., 2023) measured through Insomnia Severity Index (ISI) and Pittsburgh Sleep Quality Index (PSQI), 8.7% reported results related to quality of life assessed (k = 2) (Abbaspoor et al., 2016; Tavoli et al., 2018) using the Perceived Social Support Scale (PSSS) and another study (k = 1) (L. Gao et al., 2020) reported on perceived social support measured with Short Form - 36 Health Survey (SF-36). Moreover, the 8.7% of the studies reported mental health-related results (k = 2) (Kuhlmann et al., 2023; Voss et al., 2020) from a multidimensional perspective measured with the Screening Instrument for Subfertility Patients (ScreenIVF). Finally, sexual health outcomes were explored in 26% of studies (k = 6), of which 13% reported sexual satisfaction (k = 3) (Ghorbani et al., 2022; Liu et al., 2024; Nitu et al., 2023; Zhang et al., 2016) measured through the Female Sexual Function Index (FSFI), International Index of Erectile Function-5 (IIEF-5), Sexual Interaction Inventory (SII), Dyadic Sexual Communication Scale (DSCS), and Index of Sexual Satisfaction (ISS), 8.7% reported marital intimacy (k = 2) (Kulshreshtha et al., 2023; Nitu et al., 2023) using the Marital Intimacy Questionnaire (MIQ) and Intimate Partner Violence (IPV), and one reported infertility history (k = 1) (Gül & Kirka, 2021) measured with Medical Infertility History (MIF). Depressive and Anxiety Symptoms Fourteen cross-sectional studies have been conducted to assess depressive and anxiety symptoms in individuals with RPL across diverse countries (L. Gao et al., 2020; R. Gao et al., 2022; Gül & Kirka, 2021; He et al., 2019; Hedegaard et al., 2021; Kolte et al., 2015; Kukulskien & Žemaitiené, 2022; Kulshreshtha et al., 2023; Slot et al., 2022; Tavoli et al., 2018; Van et al., 2023; T. Wang et al., 202; Y. Wang et al., 2021; Zhang et al., 2016). Overall, women with RPL consistently showed significantly higher rates of depression and anxiety compared to women without RPL. In the Asian continent, specifically in China, L. Gao et al. (2020) reported anxiety in 45% and depressive symptoms in 37% of participants with RPL (p < .05). Perceived social support was inversely associated with anxiety (adjusted OR = 2.89, p < .001) and depression (adjusted OR = 2.56, p < .001) (L. Gao et al., 2020). A subsequent study confirmed the high prevalence of depression in women with RPL compared to those without (45% vs. 30%, p < .01) (R. Gao et al., 2022). Moreover, He et al. (2019) observed significantly higher levels of anxiety and depression among women with RPL and 1PL compared to women without RPL (p = .006), and low educational level was revealed as an independent risk factor (adjusted OR = 1.75-1.80, p < .01-.03) (He et al., 2019). Studies with larger samples corroborated these findings. Y. Wang et al. (2021) found a higher prevalence of depression (49%) and anxiety (29%) in women with RPL (p < .001), and a strong association between increased levels of depression and anxiety with an increased risk of RPL (adjusted OR = 4.23-5.95, p = .001-.05) (Y. Wang et al., 2021). Likewise, T. Wang et al. (2023) reported state anxiety in 60.3%, trait anxiety in 51.7%, and depression in 33.9% of participants, with ≥ 4 RPL, low income, and recent loss ( < 6 months) being the main predictive factors (adjusted OR = 1.98-5.52, p = .01) (T. Wang et al., 2023). Moreover, Zhang et al. (2016) revealed that men with partners experiencing RPL also experienced significantly higher rates of depression (26.3%), anxiety (39.1%), and reduced sexual satisfaction (p = .001) (Zhang et al., 2016). Similarly, we find converge results in other Eastern countries. In India, Kulshreshtha et al. (2023) reported higher rates of depression (27%) and generalized anxiety (15%) in women with RPL, along with elevated pregnancy-related anxiety (p = .01). RPL were identified as an independent risk factor for depressive symptoms (adjusted OR = 26.45, p = .01) (Kulshreshtha et al., 2023). Tavoli et al. (2018) found that Iranian women with RPL scored significantly higher on anxiety (p < .0001) and depression (p < .0001) symptoms and lower on emotional functioning (p = .0001-.05) (Tavoli et al., 2018), while, in Turkey, Gül and Kirka (2021) found increased dream anxiety in women with RPL compared to 1PL and non-RPL groups (p = .001) (Gül & Kirka, 2021). Likewise, similar results have also been found in Western countries, such as Denmark, Lithuania and USA. For example, in Danish population, Hedegaard et al. (2021) observed that women with RPL showed a significantly higher prevalence of depressive symptoms compared to men (p = .001), and a strong correlation between depressive symptoms and number of RPL was reported among affected couples (adjusted RR = 3.74, p = .001) (Hedegaard et al., 2021). In line with these findings, Kolte et al. (2015) found that individuals with RPL exhibited significantly higher levels of depression (8.6% vs. 2.2%) than those without RPL (p = .01), with symptom severity closely associated with both outcomes in the RPL group (adjusted OR = 5.53, p = .01) (Kolte et al., 2015). Moreover, Slot et al. (2022) demonstrated that primary RPL (32.1%) was associated with a greater psychological burden than secondary RPL (18.4%), including sadness, guilt, and low self-esteem (p = .007) (Slot et al., 2022). Similar findings were also observed in Nigerian women (Eleje et al., 2024). In Lithuanian population, Kukulskien and Žemaitiené (2022) indicate that 59.1% of women with RPL are at increased risk of postnatal depression, with 48.9% classified as being at high risk, while 44.7% were considered to be at increased risk for post-traumatic stress symptoms (adjusted OR = 2.45-2.45, p = .001-.01) (Kukulskien & Žemaitiené, 2022). Moreover, Van et al. (2023) observed poorer sleep quality in women with RPL, which was significantly associated with depressive symptoms among US individuals (adjusted OR = 2.03, p < .05) (Van et al., 2023). Stress and Coping Styles Several observational studies have examined psychological stress in women affected by RPL, revealing consistent evidence of elevated stress levels and their associations with sociodemographic, emotional, and reproductive factors (Hedegaard et al., 2021; Issakhanova et al., 2023; Kolte et al., 2015; Kuhlmann et al., 2023; Kukulskien and Žemaitiené, 2022; Kulshreshtha et al., 2023; Nitu et al., 2023; Slot et al., 2022; Van et al., 2023). On the European continent, specifically in Denmark, Hedegaard et al. (2021) found significantly higher emotional stress in women with RPL compared to their male partners (p = .02-.01). The number of RPL was positively associated with perceived stress (adjusted RR = 1.24; p = .02), while men showed a protective effect (adjusted RR = 0.67, p = .02) (Hedegaard et al., 2021). Another Danish study by Kolte et al. (2015) reported elevated stress levels in women with RPL (41.2%) compared to controls (23.2%), and the number of losses was positively correlated with stress severity (adjusted OR = 1.59, p = .01) (Kolte et al., 2015). Similarly, in a prospective cohort study, Slot et al. (2022) observed that women with primary RPL reported higher levels of stress (32.7%) compared to those with secondary RPL (19.9%), feelings of helplessness, guilt, and emotional exhaustion were more common in the primary RPL group (p = .01) (Slot et al., 2022). In Lithuania, Kukulskien and Žemaitiené (2022) found that 44.7% of women with RPL were at increased risk of post-traumatic stress symptoms, significantly associated with the number of RPL (OR = 2.45, p = .001) (Kukulskien & Žemaitien, 2022). Likewise, Nitu et al. (2023) observed significantly higher stress levels (61% vs. 47%) and maladaptive coping strategies (43% vs. 27%) in Romanian women with RPL. These included a greater tendency toward emotion-focused coping, lower self-esteem, and greater relationship dissatisfaction compared to individuals without RPL (p = .01). In addition, stress was related to sexual dissatisfaction and lower marital intimacy (p = .001) (Nitu et al., 2023). Similar findings were also observed in Nigerian women (Eleje et al., 2024). The psychological burden of RPL extends to partners. In Germany, Kuhlmann et al. (2023) reported that women (13.7%) showed significantly higher levels of post-traumatic stress compared to men (3.9% (p = .01) (Kuhlmann et al., 2023). Stress in women was closely related to limited social support and relationship strain, which in turn contributed to partner distress and sexual dissatisfaction. Moreover, in USA, Van et al. (2023) reported that no direct association was established between sleep and stress (Van et al., 2023). Similar findings have been observed in some countries on the Asian continent. Kulshreshtha et al. (2023) identified significantly higher levels of perceived stress (3%) in Indian women with RPL compared to people without RPL (0.8%), and RPL was found to be an independent predictor of psychological distress (adjusted OR = 26.45, p = .01) (Kulshreshtha et al., 2023). Likewise, Issakhanova et al. (2023) found that women with RPL in Kazakhstan had significantly higher stress scores compared to women without RPL (p < .001). The number of RPL was strongly associated with stress symptoms (adjusted OR = 3.67, p < .001) (Issakhanova et al., 2023). Psychopathology and Well-being Outcomes Several cross-sectional and case-control studies have reported consistent deficiencies in psychosocial areas such as psychopathology, sleep quality, perceived social support, and quality of life (Abbaspoor et al., 2016; Adib-Rad et al., 2019; L. Gao et al., 2020; Gül & Kirka, 2021; Kuhlmann et al., 2023; Nitu et al., 2023; Tavoli et al., 2018; Van et al., 2023; Voss et al., 2020; T. Wang et al., 2023). Psychopathology has been observed to be more prevalent and severe in populations with RPL. The great majority of evidence comes from Eastern countries, specifically Iran and China. In Iran population, Abbaspoor et al. (2016) reported significantly higher scores on multiple domains of the SCL-25 in women with RPL, including anxiety, depression, phobia, and obsession-compulsion, compared to women without RPL (p = .01-.0001). The number of previous RPL was positively associated with psychopathological symptoms (adjusted OR = 4.22, p = .001) (Abbaspoor et al., 2016). Similarly, Adib-Rad et al. (2019) found higher overall psychopathology and intolerance to uncertainty among women with RPL (p < .0001), with psychopathology being the strongest predictor of RPL recurrence (adjusted OR = 6.05, p ≤ .0001) (Adib-Rad et al., 2019). In Chinese individuals, Wang et al. (2023) provided comprehensive evidence that women with RPL experience high levels of depression, anxiety, and general psychopathology (p < .05-.0001). Mean scores were significantly higher in women with RPL compared to women with 1PL and without RPL in areas such as hostility, phobic anxiety, paranoid ideas, and obsessive-compulsive symptoms (p = .001). Depression was closely related to low family income, recent losses, and lack of sleep (adjusted OR = 1.98-5.52, p = .001) (T. Wang et al., 2023). Moreover, although to a lesser extent similar results have been found in Western populations. Nitu et al. (2023) found that women with RPL showed greater emotional stress (p = .02-.001). Emotion-focused coping was more common among women with RPL (p = .01), along with lower self-esteem and poorer psychological profiles (impairment relational and interpersonal) (p = .01-.001) (Nitu et al., 2023). Sleep quality was also revealed to be a major concern in Eastern countries, specifically Turkey and China. Gül and Kirka (2021) and T. Wang et al. (2023) found significantly worse insomnia and dream-related anxiety among women with RPL compared to the 1PL and non-RPL groups in Turkish population (p = .001) (Gül & Kirka, 2021) and only compared with non-RPL group (p = .01) (T. Wang et al., 2023). Likewise, in the USA, Van et al. (2023) reported significantly worse sleep in participants with RPL, which correlated with depressive symptoms (adjusted OR = 2.03, p = .04) (Van et al., 2023). Overall quality of life and well-being were also compromised in Eastern population. In Iran, Abbaspoor et al. (2016) and Tavoli et al. (2018) reported lower scores on multiple domains of the quality of life among participants with RPL, including physical functioning, vitality, emotional role, and mental health (p = .01-.001). These deficiencies were strongly related to increased psychological distress (adjusted OR = 4.22, p = .001) (Abbaspoor et al., 2016; Tavoli et al., 2018). In China, L. Gao et al. (2020) assessed perceived social support and found that women with RPL reported moderate levels of support (p = .01). Notably, low perceived support was associated with an increased risk of anxiety (OR = 2.8, p = .001) and depression (OR = 2.56, p = .001), suggesting a protective role for social relationships (Gao et al., 2020). It should be noted that the perspectives of the couple were addressed by Kuhlmann et al. (2023) and Voss et al. (2020) in Western population, who demonstrated that women with RPL had significantly higher levels of anxiety, depression, and post-traumatic symptoms compared to men (p = .01-.001) (Kuhlmann et al., 2023). Limited social support, maladaptive coping styles, and psychosocial risk were strongly associated with greater distress in both partners (r = .47-.62, p = .05-.001) (Voss et al., 2020). Sexual Health Sexual health is increasingly recognized as a fundamental dimension of well-being that is affected by RPL. Several studies reported alterations in various domains of sexual function, satisfaction, and intimacy in women with RPL and their partners (Ghorbani et al., 2022; Gül & Kirka, 2021; Kulshreshtha et al., 2023; Liu et al., 2024; Nitu et al., 2023; Zhang et al., 2016). Most of the findings are found in Eastern countries. In Iran, Ghorbani et al. (2022) found that women with RPL had reduced sexual function, showing significantly lower scores in desire, arousal, lubrication, orgasm, satisfaction and pain (p < .001), indicating a marked reduction in sexual well-being after RPL (Ghorbani et al., 2022). Likewise, Zhang et al. (2016) provided a gender perspective by examining the male partners of women with RPL in Chinese population. The study found a significantly higher prevalence of sexual dysfunction among men in the RPL group, with lower sexual satisfaction (p = .02) and higher rates of erectile dysfunction (p = .01). Psychological symptoms, such as depression and anxiety, were strongly associated with sexual dissatisfaction and performance problems, indicating a bidirectional relationship between emotional distress and sexual health (OR = 1.47-1.86, p < .001) (Zhang et al., 2016). Similar findings were also observed in women with RPL (Liu et al., 2024). Although not directly focusing on sexual function itself, Gül and Kirka (2021) observed higher levels of dream anxiety and insomnia among women with RPL in Turkey (p = .30), factors that have been linked to reduced sexual desire and relational tension (p = .001). These sleep-related symptoms may indirectly affect sexual health and intimacy (Gül and Kirka, 2021). Similar findings have been found in Western countries, although to a lesser extent. Specifically, in Romania, Nitu et al. (2023) highlighted that women with RPL reported significantly greater sexual dissatisfaction (p < .001) compared to women without RPL (p < .001), as well as decreased marital intimacy and reduced quality of sexual communication (p = .02-.008). These findings suggest that RPL affects not only the physiological aspects of sexuality, but also the relational and emotional components, especially in the context of marital dynamics (Nitu et al., 2023). Finally, Kulshreshtha et al. (2023) and Nitu et al. (2023) emphasized the interconnection between emotional distress and sexual health in women with RPL. Higher levels of depression, anxiety, and perceived stress in women with RPL were accompanied by lower satisfaction in intimate relationships, poor sexual communication, and less emotional connection with their partners (p = .03-.001). Emotion-focused coping styles and low self-esteem were also more prevalent, which could contribute to the observed decline in sexual quality of life. Table 2 Risk of Bias and Quality Assessment of the Included Case-Controls and Cohorts Study – NOS Scale 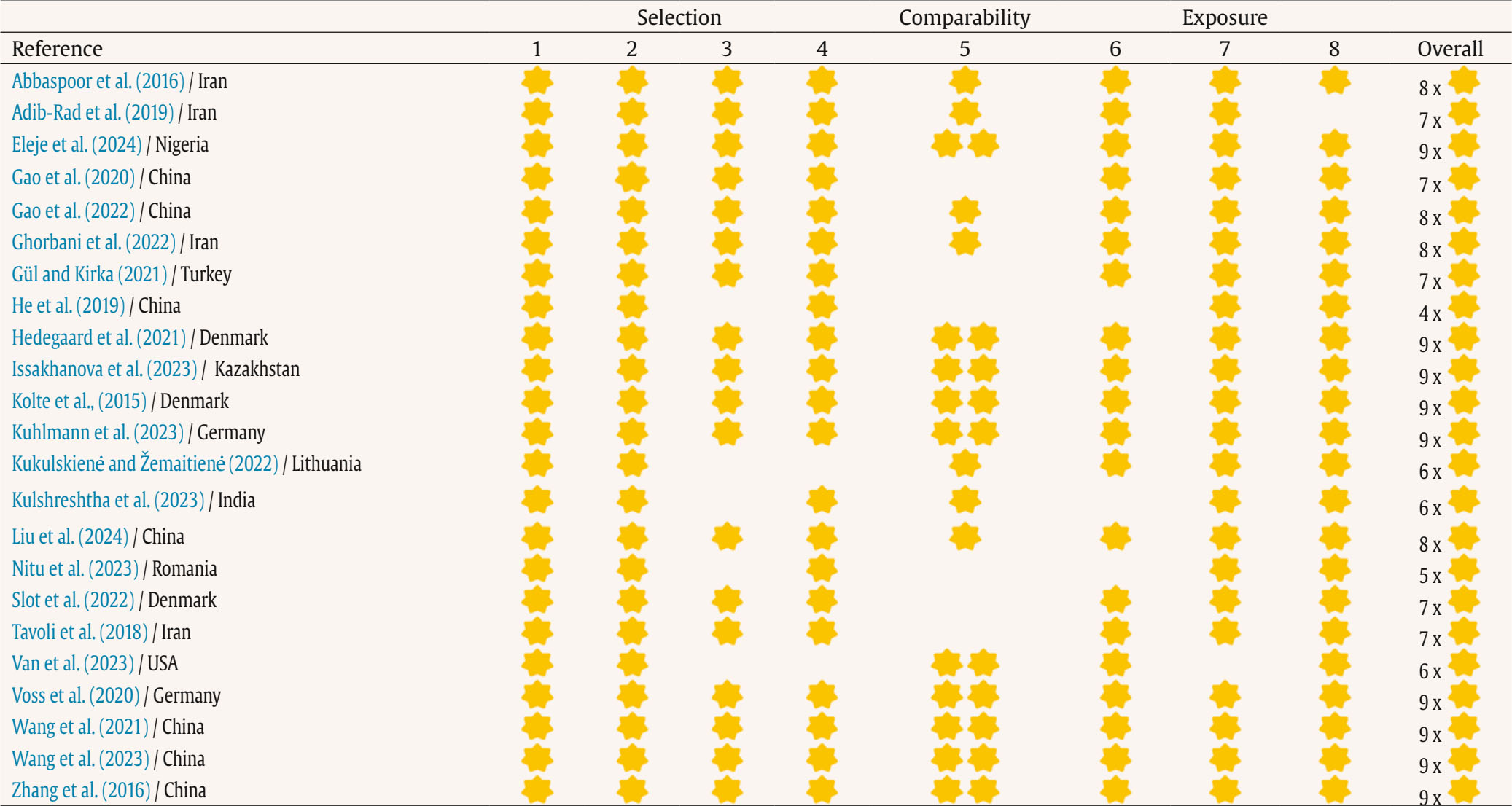 Case-control studies Selection 1. Is the case definition adequate? a) Yes, with independent validation / b) Yes, e.g., record linkage or self-reporting / c) No description 2. Representativeness of cases a) Consecutive or obviously representative series of cases / b) Potential for selection bias or not stated 3. Selection of controls a) Community controls / b) Hospital controls / c) No description 4. Definition of controls a) No history of disease (endpoint) / b) No description of source Comparability 5. Comparability of cases and controls based on the design or analysis a) Study controls for the most important factor / b) Study controls for an additional factor Exposure 6. Determination of exposure a) Secure recording (e.g., surgical records) / b) Structured interview blinded to case/control status / c) Interview not blinded to case/control status / d) Written self-report or medical history only / e) No description 7. Same method of determination for cases and controls a) Yes / b) No 8. Non-response rate a) Same rate for both groups / b) Non-response described / c) Different rates and no description Cohort studies Selection 1. Representativeness of the exposed cohort a) Truly representative of the mean of… in the community / b) Somewhat representative of the mean of… in the community / c) Selected group (e.g., nurses, volunteers) / d) No description of the derivation of the cohort. 2. Selection of unexposed cohort a) Coming from the same community as the exposed cohort / b) From a different source / c) No description of derivation 3. Determination of exposure a) Secure recording (e.g., surgical records) / b) Structured interview / c) Written self-report / d) No description 4. Demonstration that the outcome of interest was not present at baseline a) Yes / b) No Comparability 5. Comparability of cohorts based on design or analysis a) Study controls for the most important factor / b) The study controls for an additional factor Outcome 6. Outcome assessment a) Independent blinded assessment / b) Record linkage / c) Self-report / d) No description 7. Was the follow-up long enough for the outcomes to occur? a) Yes (an appropriate follow-up period must be specified) / b) No 8. Adequacy of follow-up of cohorts a) Complete follow-up - all subjects accounted for / b) Loss to follow-up is unlikely to introduce bias - small number lost or description provided / c) Follow-up rate < ___% and no description of those lost / d) No statement Table 3 Quality Score of the Information Included in the Studies - Strengthening the Reporting of Observational Studies (STROBE) 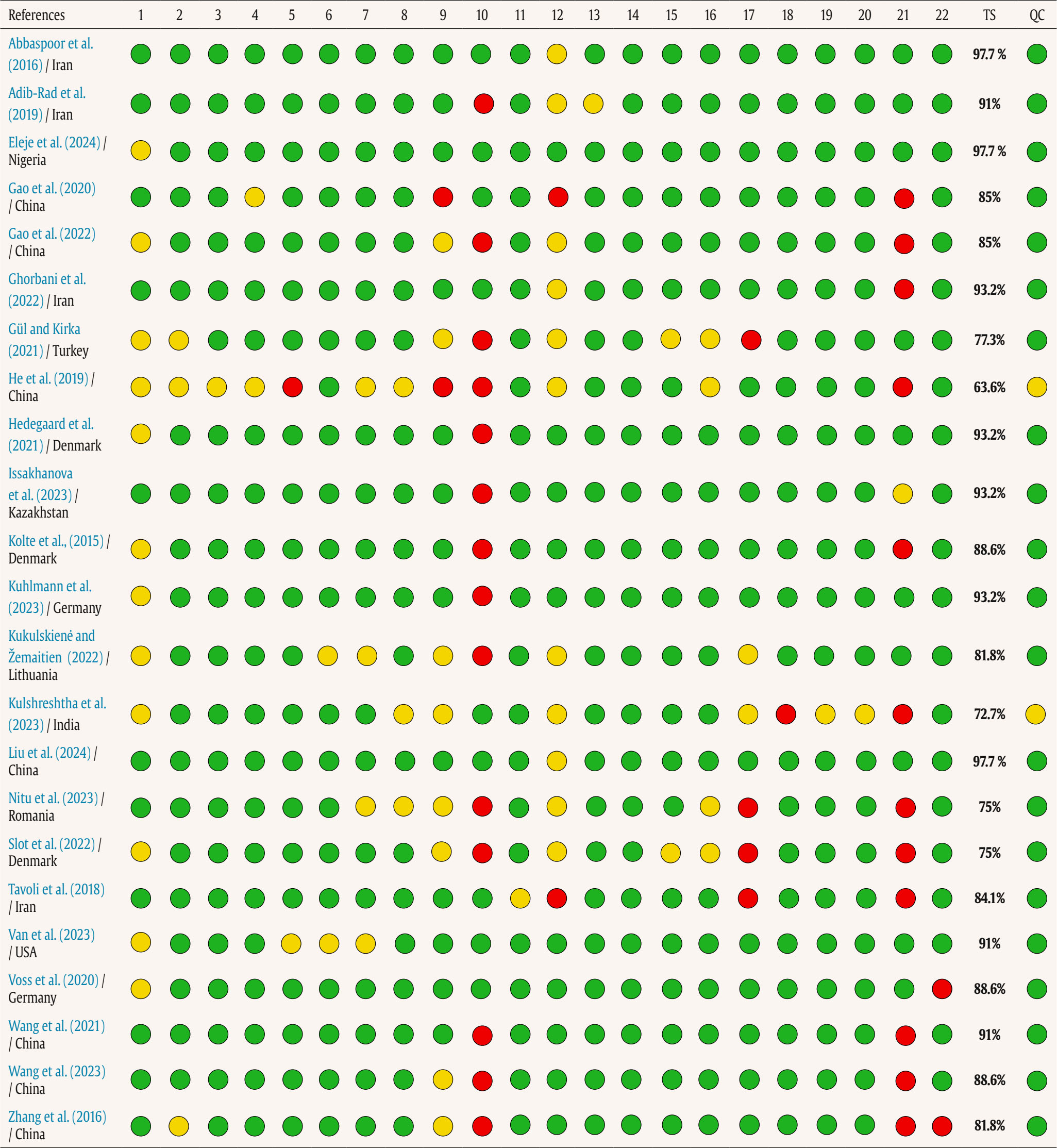 List of Items 1. Title and Abstract: a) Indicate, in the title or abstract, the study design using a commonly used term. b) Provide an informative and balanced synopsis in the abstract of what was done and what was found. 2. Introduction > Background/Rationale: Explain the scientific background and rationale for the investigation being reported. 3. Introduction > Objectives: State the specific objectives, including any pre-specified hypotheses. 4. Methods > Study Design: Present the key elements of the study design early in the paper. 5. Methods > Setting: Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data collection. 6. Methods > Participants: a) Cohort studies: Provide eligibility criteria, as well as sources and methods of selection of participants. Specify follow-up methods. a) Case-control studies: Provide eligibility criteria, as well as sources and diagnostic methods for cases and selection methods for controls. Provide reasons for the choice of cases and controls. a) Cross-sectional studies: Provide eligibility criteria and the sources and methods of selection of participants. b) Cohort studies (matched): Provide matching criteria and the number of exposed and unexposed participants. b) Case-control studies (matched): Provide matching criteria and the number of controls per case. 7. Methods > Variables: Clearly define all variables: outcomes, exposures, predictors, confounders, and effect modifiers. Provide diagnostic criteria if applicable. 8. Methods > Data Sources/Measurement: For each variable of interest, provide data sources and details of measurement methods. If there is more than one group, describe the comparability of assessment methods. 9. Methods > Bias: Describe any efforts to address potential sources of bias. 10. Methods > Study Size: Explain how the study size was determined. 11. Methods > Quantitative Variables: Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and why. 12. Methods > Statistical Methods: a) Specify all statistical methods, including those used to control for confounding. b) Specify any methods used to examine subgroups and interactions. c) Explain how missing data were addressed. Cohort studies: If applicable, explain how loss to follow-up was addressed. Case-control studies: If applicable, explain how matching of cases and controls was handled. Cross-sectional studies: If applicable, describe analytical methods that take account of the sampling strategy. d) Describe any sensitivity analyses. 13. Results > Participants: a) Report the numbers of individuals at each stage of the study; e.g., numbers potentially eligible, examined for eligibility, confirmed eligible, included in the study, completing follow-up, and analyzed. b) Give reasons for non-participation at each stage. c) Consider the use of a flow diagram. 14. Results > Descriptive Data: a) Give characteristics of study participants (e.g., demographic, clinical, social) and information on exposures and potential confounders. b) Indicate the number of participants with missing data for each variable of interest. c) Cohort studies: Summarize follow-up time (e.g., average and total amount). 15. Results > Outcome Data: Cohort studies: Report numbers of outcome events or summary measures over time. Case-control studies: Report numbers in each exposure category or summary measures of exposure. Cross-sectional studies: Report numbers of outcome events or summary measures. 16. Results > Main Results: a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (e.g., 95% confidence interval). Make clear which confounders were adjusted for and why. b) If continuous variables were categorized, report the category boundaries. c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period. 17. Results > Other Analyses: Report other analyses done (e.g., subgroup analyses, interactions, sensitivity analyses). 18. Discussion > Key Results: Summarize key results with reference to study objectives. 19. Discussion > Limitations: Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both the direction and magnitude of any potential bias. 20. Discussion > Interpretation: Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar studies, and other relevant evidence. 21. Discussion > Generalizability: Discuss the generalizability (external validity) of the study results. 22. Other Information > Funding: Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the present article is based.
* Total Score: Sum of items answered affirmatively (value = 1) / total number of items (total items = 22) x 100 Abbreviations: NA = not applicable; TS = total score; QG = qualitative grade Assessment of Risk of Bias and Quality Assessment The assessment of risk of bias and methodological quality was performed using the NOS (see Table 2). Overall, the included case-control and cohort studies had a low risk of bias and good methodological quality. The majority (k = 18) obtained scores ranging from 7 to 9, indicating low risk of bias in terms of selection, comparability and exposure or outcome assessment. However, some studies had specific methodological limitations, such as lack of clear information on exposure ascertainment, or potentially insufficient or undescribed follow-up, which could compromise the internal validity of the findings (k = 5) (He et al., 2019; Kukulskien & Žemaitien, 2022; Kulshreshtha et al., 2023; Nitu et al., 2023; Van et al., 2023). Despite these limitations, overall compliance with key quality criteria was observed, especially in studies such as those by Eleje et al. (2024), Hedegaard et al. (2021), Issakhanova et al. (2023), Kolte et al., (2015), Kuhlmann et al. (2023), Voss et al. (2020), Y. Wang et al. (2021), T. Wang et al. (2023), and Zhang et al. (2016) (k = 9), which achieved the maximum score, reflecting robust methodological execution. Overall, the included studies present an acceptable methodological level to support their conclusions. The assessment of the quality of information included using the STROBE tool showed the most articles had a good quality of information. Specifically, 91.3% (k = 21) of the studies had a score above 75%, indicating a good quality of information. The remaining 8.7% (k = 2) (He et al., 2019; Kulshreshtha et al., 2023) of articles showed “fair” quality of information, with scores between 50% and 75%, suggesting some concerns regarding to quality of information. No studies with low quality of information (score below 50%) were identified (see Table 3). To our knowledge, this is the first systematic review of available observational studies that has comprehensively evaluated mental health outcomes, including emotional well-being and quality of life, in individuals who have experienced RPL and their couples. Our results highlight a significant increase in psychopathology, especially symptoms of depression, anxiety, and stress in this population compared to women who have not experienced RPL. They also indicate that quality of life and sexual satisfaction are significantly reduced and, to a lesser extent, problems with sleeping habits in women who have suffered RPL. This systematic review also supports an association between RPL and deterioration in mental health and general well-being, specifically, with a marked loss of sexual satisfaction during subsequent pregnancies, regardless of the number of losses. Although the sample of men was small, similar findings were observed in the partners of women who had experienced RPL. It should be noted that these findings have been observed in several countries with different customs and cultures. Our findings support and extend previous reviews of the field. Our results converge with previous literature confirming elevated levels of anxiety, depression and stress in women who have suffered RPL and their partners (Daugirdait et al; Hunter et al., 2017), with profound consequences on quality of life and well-being (Quenby et al., 2021). Growing literature further demonstrate that mental health impairments, such as psychopathology and emotional distress, are not only outcomes but also potential contributors to poor reproductive outcomes, reinforcing the notion, reported in our results, that psychosocial vulnerability may serve as a risk factor for future pregnancy loss (Cuenca, 2023). Moreover, our study converges with previous findings confirming that the severity of psychopathology is directly related to more intense and unfavorable responses to RPL (Inversetti et al., 2023). Likewise, our results align with evidence indicating that poorer coping styles and lower social support are associated with higher psychological distress, making it more difficult for women to adapt to new pregnancies following loss (Balle et al., 2024). Similar findings have been found for other risk factors such as poor sexual health and inadequate sleep patterns, both of which were significantly worse in women with RPL compared to women without RPL, which also converges with our results (Allsop et al., 2024; Freeman et al., 2025). Additionally, our results indicate that psychological distress may be more pronounced in women with primary RPL compared to those with secondary RPL, suggesting that the absence of previous live births may increase vulnerability (Luo et al., 2023; Schliep et al., 2022). Sociodemographic variables also play a role, with low educational attainment being independently associated with increased anxiety and depression in RPL populations (Fernández-Basanta et al., 2023). It should be noted that the psychological impact extend to partners, our results showing that while women consistently report higher levels of depression and anxiety, men in couples experiencing RPL are also significantly affected, particularly in terms of stress and post-traumatic symptoms, which is consistent with previous findings (Inversetti et al., 2025). The psychological impact of RPL is influenced by personal and sociocultural factors (Tong et al., 2024). Regarding personal factors, a recurrent finding in the literature is the significant role of social support in modulating the negative mental health consequences of RPL. For example, women (or couples) who report having strong support networks tend to better manage the stress associated with RPL (Iwanowicz-Palus et al., 2021). Social support not only provides an emotional buffer, but can also offer pragmatic resources (e.g., advice on different fertility techniques or adaptive coping strategies) essential for coping with RPL during pregnancy (Tetruashvili et al., 2023). Another major factor involved is having a high capacity for resilience and self-awareness that provide a beneficial impact on how women and their partners cope with and process these stressful experiences. In addition, coping style also significantly influences mental health in this population, so while adaptive strategies (such as sense-making or emotional expression) are associated with better mental health, the use of maladaptive mechanisms (such as avoidance or denial) predicts higher levels of anxiety and depression (Turesheva et al., 2023). Overall, and consistent with our findings, these studies suggest that the development of adequate interpersonal skills along with adequate social support can play a crucial role in improving the quality of life and well-being of women and their partners who have experienced RPL. In addition to these personal factors, there are sociocultural elements that also influence the emotional experience of RPL. The stigma associated with infertility or RPL, especially in contexts where motherhood is strongly linked to female identity, can intensify psychosocial suffering and generate feelings of failure, shame, or isolation (Judge-Golden & Flink-Bochacki, 2021). Likewise, the social invisibility of RPL as a significant loss can hinder the grieving process, as the experience is not emotionally validated (Mu et al., 2024). Finally, unequal access to healthcare and mental health resources, conditioned by variables, such as socioeconomic status, cultural environment, or educational background, can limit the search for help and perpetuate emotional distress (Harnett et al., 2025). All of this underscores the need to understand the impact of RPL from an integrative perspective that considers both personal resources and the sociocultural context in which the experience of RPL unfolds. In this regard, the findings highlight the importance of implementing systematic psychological treatments for women and their partners throughout the pregnancy process and in the aftermath of a perinatal loss, including the assessment of psychopathology (symptoms of anxiety, depression, stress), quality of life, and general well-being (including sexual health and sleep habits). It is essential to consider that some people may require psychological care even before accessing specialized perinatal health services, which means that the initial presentation of emotional distress may occur in primary care settings. Therefore, it is necessary to increase awareness and training among primary care professionals regarding the emotional consequences of RPL and its implications for subsequent pregnancies (Donegan et al., 2023). Furthermore, our study highlights the need to offer continuous, person-centered care, including aspects such as continuity of the professional providing care, effective communication between teams, and easy access to both physical and psychological prenatal checkups. Recognizing that these women may experience another loss and providing empathetic and constant support can significantly improve their emotional well-being and that of their families. Strengths and Limitations This systematic review has several limitations that affect the interpretation and generalization of the findings. First, the predominance of cross-sectional studies prevents the establishment of causal relationships between RPL and the psychological effects observed. Second, the frequent use of self-reports as a source of data introduces recall and social desirability biases. Third, there is marked methodological heterogeneity among the studies, both in the scales used to measure psychopathology and quality of life and in the definitions of RPL, making it difficult to compare research. Fourth, the diverse sociodemographic characteristics of the samples, coupled with the low representation of vulnerable populations (adolescent women, women living in poverty, ethnic minorities, or women with multiple pregnancies), limit the generalizability of the results to other contexts. Fifth, there are gaps in the inclusion of important covariates such as the number of living children, the time elapsed since the loss, or the presence of previous psychological symptoms. Sixth, many studies did not differentiate between types of loss (miscarriage, stillbirth, neonatal death), which prevents an assessment of their specific impact. Furthermore, the limited availability of data on stress, on couples (including same-sex couples), and on specific experiences such as RPL restricts a comprehensive understanding of the phenomenon. These weaknesses reflect the need for more longitudinal, representative, and culturally diverse research that addresses the emotional impact of RPL in greater depth. Lastly, due to the predominance of cross-sectional designs, causal inferences cannot be made, and the results should be interpreted as associations. Despite its limitations, this review also has significant strengths that reinforce its validity and clinical utility. First, it highlights the exclusive use of validated psychological instruments and a systematic assessment of the quality of the included studies, which ensures greater reliability of the results. Second, relevant patterns were identified in levels of anxiety, depression, and stress, suggesting that psychopathology may serve as a risk indicator in this population. Third, it emphasizes the need to offer continuous psychological care throughout pregnancy and after RPL, and to adapt the health system to respond empathetically and appropriately to the emotional needs of these women and their partners. Fourth, it highlights the importance of effective communication between professionals, individualized follow-up, easy access to mental health services, and explicit recognition of experiences of loss. Finally, the report highlights the urgent need to develop specific psychosocial interventions aimed at reducing emotional distress during subsequent pregnancies, with the aim of improving the well-being of mothers, their partners, and future children. Future Lines of Research Future research should focus on examining the differential impact of different types of RPL on mental health during subsequent pregnancies, considering understudied variables such as attachment, post-traumatic stress disorder, number of living children, and the interval between the loss and the current pregnancy. It is essential to broaden the representativeness of samples, including women at higher risk of loss, same-sex couples, and different cultural and socioeconomic contexts. Likewise, definitions and methodologies need to be standardized to improve comparability between studies and analyze how levels of anxiety, depression, and stress vary in the different trimesters of pregnancy after loss. Another crucial line of research is the development and evaluation of specific psychosocial interventions, as well as the implementation of clinical care that ensures continuity, effective communication, and mental health monitoring in these cases. Finally, it is important to explore the long-term consequences for the mother, the couple, and the family, including the impact on attachment and emotional well-being, and to control for previous baseline variables to avoid bias in the results. This systematic review provides compelling evidence of the profound psychosocial impact of RPL on both women and their partners, manifesting in high levels of anxiety, depression, stress, decreased quality of life, sexual dissatisfaction, and sleep disturbances, regardless of cultural context. Furthermore, it highlights that this emotional distress is modulated by personal factors, such as social support, resilience, and coping styles, as well as by sociocultural determinants such as stigma, the invisibility of grief, and inequalities in access to mental health services. Despite the methodological limitations of the studies analyzed, the findings support the urgent need to implement systematic, comprehensive, and continuous psychological interventions, both in primary and specialized care, that include empathetic communication, individualized follow-up, and explicit recognition of the experience of loss, in order to improve the emotional well-being of those affected and prevent future complications during pregnancy.
Conflict of Interest The authors of this article declare no conflict of interest. Cite this article as: Sánchez-Ortí, J. V., Bellver-Pérez, A., & Moreno-Maldonado, E. (2026). Mental health, well-being, and sexual health in recurrent pregnancy loss: A systematic review. Clinical and Health, 37, Article e260723. https://doi.org/10.5093/clh2026a9 References References marked with an asterisk indicate studies included in the metaanalysis. |

Cite this article as: Sánchez-Ortí, J. V., Bellver-Pérez, A., & Moreno-Maldonado, E. (2026). Mental Health, Well-being, and Sexual Health in Recurrent Pregnancy Loss: A Systematic Review. Clinical and Health, 37, Article e260723. https://doi.org/10.5093/clh2026a9
Correspondence: ascension.bellver@uv.es (A. Bellver-Pérez).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
Clinical and Health is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License








