


Profiles of Cognitive Emotion Regulation and their Association with Emotional Traits
[Los perfiles de la regulación cognitiva de las emociones y su asociación con los rasgos emocionales]
Amaia Lasa-Aristu, Begoña Delgado-Egido, Francisco P. Holgado-Tello, Pedro J. Amor, and Francisco J. Domínguez- Sánchez
Universidad Nacional de Educación a Distancia, Madrid, Spain
https://doi.org/10.5093/clysa2019a6
Recibido a 16 de Julio de 2018, Aceptado a 23 de Enero de 2019
Resumen
Existe un creciente interés en la investigación de las relaciones entre diferentes estrategias de regulación de la emoción y sus síntomas u otros rasgos emocionales. Este estudio considera estos tipos de estrategias como disposiciones personales en relación con otros factores, en un esfuerzo por identificar diferentes perfiles de regulación de la emoción cognitiva y analizar su capacidad para predecir el impacto positivo y negativo, rasgos emocionales (ansiedad e ira) y sintomatología depresiva. Los participantes fueron 350 individuos (50% hombres) con una edad media de 35.69 (SD = 7.5). Los métodos de análisis de datos empleados fueron cluster, análisis discriminante y comparación de medias. Encontramos aspectos idiosincrásicos que sugieren la existencia de diversos estilos cognitivos de regulación emocional. Estos estilos se diferencian por su mayor o menor frecuencia en el uso de estrategias consideradas en la literatura como “más adaptativa” o “menos adaptativa” (los perfiles “protector” y “vulnerable”), siendo la reevaluación positiva la estrategia que mejor distingue el perfil de regulación emocional de cada persona.
Abstract
There is increasing research interest in the relationships between different emotion regulation strategies and symptoms or other emotional traits. This study considers these types of strategies as personal dispositions in relation to other factors, in an effort to identify different cognitive emotion regulation profiles and analyze their predictive capacity for positive and negative affect, emotional traits (anxiety and anger), and depressive symptomatology. Participants were 350 individuals (50% men) with a mean age of 35.69 (SD = 7.5). The data analysis methods employed were cluster, discriminant analyses, and comparison of means. We found idiosyncratic aspects suggesting the existence of diverse cognitive styles of emotional regulation. These styles would be differentiated by greater or lesser frequency in the use of strategies considered in the literature as “more adaptive” or “less adaptive” (the “protector” and “vulnerable” profiles), positive reappraisal being the strategy that best distinguishes between individuals as regards their emotional regulation profile.
Palabras clave
Regulación de la emoción, Estrategias cognitivas, Perfiles, Rasgos emocionales, Sintomatología depresiva
Keywords
Emotion regulation, Cognitive strategies, Profiles, Emotional traits, Depressive symptomatology
Cite this article as: Lasa-Aristu, A., Delgado-Egido, B., Holgado-Tello, F. P., Amor, P. J., & Domínguez-Sánchez, F. J. (2019). Profiles of cognitive emotion regulation & their association with emotional traits. Clínica y Salud, 30, 33-39. https://doi.org/10.5093/clysa2019a6
Correspondence: alasa@psi.uned.es (A. Lasa-Aristu).
Introduction In general, emotional responses facilitate an individual’s functional adaptation to stressful or adverse circumstances. However, some people experience emotional difficulties that affect the efficacy of this regulation mechanism (Werner & Gross, 2010). Indeed, 75% of diagnostic categories of psychopathological disorders (DSM-IV-R) take into account problems of emotion or emotional regulation (MacLeod & Bucks, 2011). The growing number of studies published on emotional regulation indicates the extent of current interest in this phenomenon (Gross, 2015). Given its complexity, some experts argue for the need to distinguish empirically and theoretically between processes of emotional regulation and generation of emotion (Cole, Martin, & Dennis, 2004; Gross & Barrett, 2011). From a clinical point of view, this distinction would help us to better understand the involvement of emotional regulation in psychopathology; at the same time, the scientific study of emotion will benefit from the complementary use of different conceptual and methodological approaches (Barrett, 2017; Bloch, Moran, & Kring, 2009). Emotional regulation encompasses a set of competences that allow the person to supervise, appraise, and modify the processes involved in the genesis of emotion and modulate its manifestation (Gross, 1999; Thompson, 1994). Thus, over the course of their lives, people develop and put into practice a range of strategies that permit them to modulate and modify the intensity and type of emotional experience and the impact of emotional events (Diamond & Aspinwall, 2003; Gross, 1998). Moreover, the ability to regulate negative affect in an effective way is critical for one’s physical and emotional health, playing an important role in modulating the risk of depressive (Gotlib & Joormann, 2010) or anxiety disorders (Kashdan, Zvolensky, & McLeish, 2008; Mennin, Holoway, Fresco, Moore, & Heimberg, 2007). In either case, ineffectiveness or inadequacy of emotion regulation in response to stressful events can trigger pathological conditions (Compas et al., 2017; Denny, Silvers, & Ochsner, 2009; Gross & Thomson, 2007; Mennin et al., 2007). Since Lazarus and Folkman’s (1984) ground-breaking approach addressing the involvement of emotion regulation strategies in diverse psychopathological disorders, research has shown the importance of such mechanisms in the modulation of disorders other than anxiety and depression, among them those related to eating behaviour and the abuse of alcohol and other substances (see the meta-analysis by Aldao, Nolen-Hoeksema, & Schweizer, 2010). Findings from various studies and reviews lead to the conclusion that the use of strategies more closely associated with pathology, such as rumination, avoidance or suppression, together with the failure to employ protective strategies such as positive reappraisal or acceptance, can have a marked effect on affective disorders related to anxiety and depression (Aldao & Nolen-Hoeksema, 2010; Joormann & D’Avanzato, 2010). Therefore, despite the difficulties of categorization in the absence of knowledge about the context in which individuals regulate their emotional behaviour, strategies of the former type have been considered “less adaptive”, and strategies of the latter type have been deemed “adaptive” – though some authors advise caution with the rigid use of these terms; Aldao, for example, talks about putatively adaptive and maladaptive strategies. Studies that address the association between emotional regulation strategies and a range of psychopathologies have also done so within the context of cognitive strategies (Garnefski, Kraaij, & Spinhoven, 2001). The Cognitive Emotion Regulation Questionnaire (CERQ) is an instrument that provides information on the frequency of the conscious use of different cognitive emotion regulation strategies such as self-blame, acceptance, rumination, positive refocusing, refocus on planning, positive reappraisal, putting into perspective, catastrophizing, and blaming others. The results of the research focusing on cognitive emotion regulation strategies, taken together, reveal that emotional disorders (e.g., anxiety and depression) and emotional traits (e.g., trait anxiety, proneness to depression, negative affect, and trait anger) are related to types of strategies in unequal fashion. That is, strategies referred to as less adaptive (or maladaptive), including rumination and catastrophizing, are directly related to symptoms of depression and anxiety or to emotional traits; on the other hand, the so-called adaptive strategies, such as positive reappraisal or putting into perspective, are inversely related to such symptoms or traits. Findings like this have been obtained in a wide range of age groups, from pre-adolescents (age 9 to 12) to adults, and cultures (e.g., Garnefski et al., 2001; Jermann, Van der Linden, d’Acremont, & Zermatten, 2006; Martin & Dahlen, 2005; Potthoff et al., 2016). The majority of these studies focus on the relationship between cognitive emotion regulation strategies and symptoms or other emotional traits, but such strategies have also been studied as the expression of identifiable dispositions in individuals in relation to other factors (Doron, Thomas-Ollivier, Vachon, & Fortes-Bourbousson, 2013; Potthoff et al., 2016). Some authors, such as Hampson (2012), suggest that there are different cognitive styles of emotion regulation and argue that these can act either directly – moderating the relationship between threatening or unpleasant situations and proneness to various psychological symptoms – or indirectly, mediating this relationship. From another perspective, it is claimed that one of the functions of emotional regulation is to give coherence to the individual from a holistic point of view, that is, to provide us with a personality system (Koole, 2009; Kuhl, Quirin, & Koole, 2015). There is evidence that, based on the interaction between the traits related to emotional regulation (e.g., response tendencies that emerge in the secondary appraisal made by the individual) and those specific to emotional reactivity (e.g., personal characteristics or the nature of the triggering stimulus that influence a person’s initial response to the situation), it is possible to predict psychological functioning (Baumann, Kaschel, & Kuhl, 2007; Carver & Connor-Smith, 2010; Davidson, 1998, 2000; Skinner & Zimmer-Gembeck, 2007; Zimmer-Gembeck & Skinner, 2011). In the present study, taking the individual as the unit of measurement, as a person with idiosyncratic characteristics that distinguish him or her from others, we explore the possible existence of specific profiles, or participant groups defined by their cognitive coping profiles and their relationship with emotional symptoms. More specifically, the aim of this study is to identify different profiles of cognitive emotion regulation and analyze their predictive capacity in relation to positive and negative affect, different emotional traits (anxiety and anger), and depressive symptomatology. This objective founds the following working hypotheses: H1): participants, depending on the cognitive strategies of emotional regulation (adaptive strategies and less adaptive strategies), can be classified into different profiles or clusters; H2): from the nine cognitive coping strategies measured by CERQ, some of them will predict more probably the membership group; H3): emotional vulnerability to adverse events would depend on the cognitive profile of regulation. MethodSample Participants in this study were 350 people with a mean age of 35.6 years (SD = 7.6, range of 18 to 52). Men accounted for 50.3% of the sample (M = 35.69, SD = 7.5) and women 49.7% (M = 35.51, SD = 7.7). All were enrolled in courses at university, and as regards occupation, 61% were in regular employment, 11% were employed part-time, 12.6% were officially unemployed, 13.5% were exclusively studying, and 1.9% were pensioners. Participation was voluntary and there was no type of financial or academic reward. Procedure Selection of the sample was by means of a personal e-mail sent to students on various courses at a Spanish university. In this e-mail, potential participants were told that participation was voluntary and anonymous, and consisted in filling out a battery of questionnaires that could be found on an Internet website accessed by means of a username and a password. The final sample comprised equal numbers of men and women, matched by age and socio-economic status. Instruments Cognitive Emotion Regulation Questionnaire - Spanish version (CERQ-S; original version by Garnefski et al., 2001; Garnefski, Kraaij, & Spinhoven, 2002; Spanish adaptation by Domínguez-Sánchez, Lasa-Aristu, Amor, & Holgado-Tello, 2013). We used the shortened 27-item version (Holgado-Tello, Amor, Lasa-Aristu, Domínguez-Sánchez, & Delgado, 2018), which measures the cognitive emotion regulation strategies the person uses in response to a stressful life event. It comprises 9 conceptually distinct scales with 3 items each. Responses to the items were given in a Likert-type scale ranging from 1 (almost never) to 5 (almost always), and higher scores indicate greater use of the coping strategy assessed. The items are structured in accordance with a second-order factor model comprising two factors putative labelled Adaptive Strategies (acceptance, positive refocusing, refocus on planning, positive reappraisal, and putting into perspective) and Less Adaptive Strategies (self-blame, rumination, catastrophizing, and blaming others) (Domínguez et al., 2013; Garnefski et al., 2001; Jermann et al., 2006). In the sample used in the original study by Garnefski et al. (2001) the internal consistency (alpha) of the scales ranged from .72 to .88. In our study alpha values ranged from .75 to .85. Beck Depression Inventory (BDI; Beck, Rush, Shaw, & Emery, 1979; Spanish version by Vázquez & Sanz, 1997). This is a 21-item self-report (range: 0-63 points) that measures the intensity of depressive symptoms. The reliability coefficient obtained through the two-halves method is .93. As regards convergent validity, correlation with the clinical assessment of depression ranges from .62 to .66. In the sample used in this study the alpha is .88. State-Trait Anxiety Inventory (STAI; Spielberger, Gorsuch, & Lushene, 1970; Spanish version by TEA, 1982). This is a self-report instrument with 20 items related to trait anxiety and another 20 related to state anxiety; the score range is 0 to 60 points for each scale. In the present study we used the STAI-T, whose Spanish version has a test-retest reliability of .81 and an internal consistency ranging from .83 to .92 (.93 in sample used in this study). State-Trait Anger Expression Inventory-2 (STAXI-2; Spielberger, 1988; Spanish version by Miguel-Tobal, Casado, Cano-Vindel, & Spielberger, 2001). In this study we used the Trait Anger Scale (STAXI-2-T), which comprises 10 items (range of 0-40 points); it has a test-retest reliability of .71 and an internal consistency of .89 (.83 in sample used in this study). Positive and Negative Affect Schedule (PANAS; Watson, Clark, & Tellegen, 1988; Spanish version by Sandín et al., 1999). This is a 20-item instrument for the assessment of two independent dimensions: positive affect (PA) and negative affect (NA). The range for each scale is from 10 to 50 points (10 items in each scale). The internal consistency in the Sandín et al.’s (1999) study is in the range .87 to .91, and the remaining psychometric properties are quite satisfactory. In the sample used in this work the alphas are .64 (PANAS-NA) and .65 (PANAS-PA). Statistical Analyses The statistical analyses employed were: 1) k-means cluster analysis, to obtain homogenous groups of participants according to the score of the subjects in the second order factors (adaptive strategies and less adaptive strategies), that were the two clustering variables used in the analysis; 2) discriminant analysis, taking as predictor variables the different coping strategies and as criterion variable the membership group derived from the cluster analysis. This analysis makes it possible to identify the dimensions that best distinguish between the clusters found according to type of emotion regulation; 3) finally, we made comparisons of means between the coping profiles in the different cognitive emotion regulation strategies, and between these profiles and depressive symptoms, trait anxiety, trait anger, positive affect, and negative affect. To this end we used the Student’s t test and calculated the effect size by means of Hedges’ g and the confidence interval (95%) for non-centrality parameters, using the MBESS Package. We also used SPSS 15 and R (Kelley, 2010; Kelley & Lai, 2010) for the statistical analysis. ResultsCluster Analysis: Formation of Groups according to the Cognitive-Emotional Coping Style By means of the k-means cluster analysis of the scores obtained in the two second-order dimensions of the CERQ-S (adaptive and less adaptive strategies), we identified two groups of participants with different emotional-cognitive coping styles in response to stressful events. As shown in Table 1, we found statistically significant differences between the two groups as regards the frequency of use of cognitive emotion regulation strategies. Specifically, those in Group 2 were characterized by more frequent use of “adaptive” cognitive emotion regulation strategies, and less frequent use of “less adaptive” strategies than those in Group 1. Table 1 ANOVA of the Variables in the Clustering Process 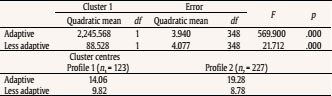 Note. k-means cluster solution. In the lower part of this table we indicate the centres of the final clusters. On the other hand, 35% of the participants were categorized in Profile 1, and no statistically significant differences were found between the two clusters by gender, ?2(1) = 0.001, p >.05. Figure 1 Groups (Profile 1 and Profile 2) Formed according to Mean Scores in Adaptive and Less-adaptive Strategies. 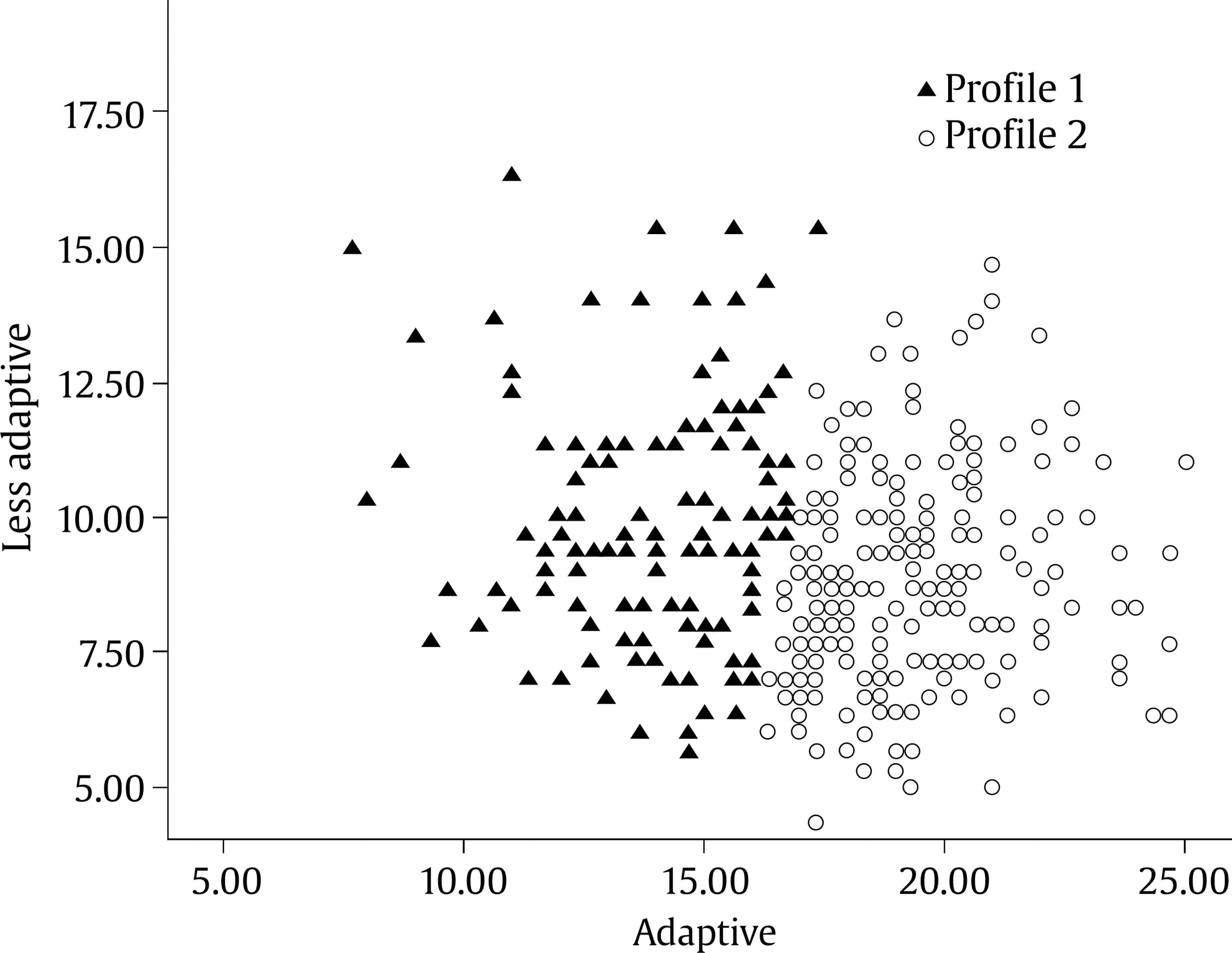 Figure 1 shows the differential distribution of the two groups according to their mean scores in the adaptive and less adaptive strategies of the CERQ-S. A more detailed analysis of these strategies suggests that, although there is a more homogeneous distribution regarding the use of less adaptive strategies in both groups, the participants in Group 1 (Profile 1) tends to be located in the left part of the graph, scoring lower on the adaptive strategies than Group 2 participants. In contrast, those in Group 2 (Profile 2) tend to be located on the right (greater use of adaptive strategies). The last profile faces the adverse events with a wider range of coping strategies than Profile 1. Profile 2 tends to use more frequently the putative labelled adaptive strategies. Statistically significant differences were found between the two groups in eight of the nine first-order dimensions of the CERQ-S (the exception being self-blame): participants in Profile 1 scored significantly higher in the strategies rumination, catastrophizing, and blaming others, with effect sizes ranging from small to moderate. On the other hand, those in Profile 2 obtained higher mean scores in the use of the five adaptive strategies of the CERQ-S – acceptance, positive refocusing, refocus on planning, positive reappraisal, and putting into perspective – with effect sizes ranging between large and very large. Table 2 shows the mean values obtained by each group in the nine cognitive emotion regulation strategies. Table 2 Descriptive Statistics and Comparisons between Average Scores in the Profiles for the CERQ Strategies 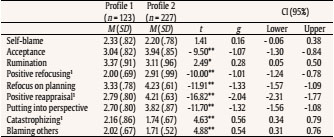 Note. 1Equal variances are not assumed; g = Hedges’ ; CI (95%) = confidence interval (95%); g = 0.20 (small), 0.50 (medium), and .80 (large). *p < .05, **p < .01. Discriminant Analysis: Formation of Profiles according to Emotion Regulation Strategies Next, we carried out a discriminant analysis, including as predictors the nine dimensions of the CERQ-S and as criterion variable the groups obtained previously by means of the cluster analysis (Table 3). The variables with the best capacity for predicting an individual’s emotional regulation profile are (beginning with the best): positive reappraisal, putting into perspective, and refocus on planning. Table 3 Main Results of the Discriminant Analysis 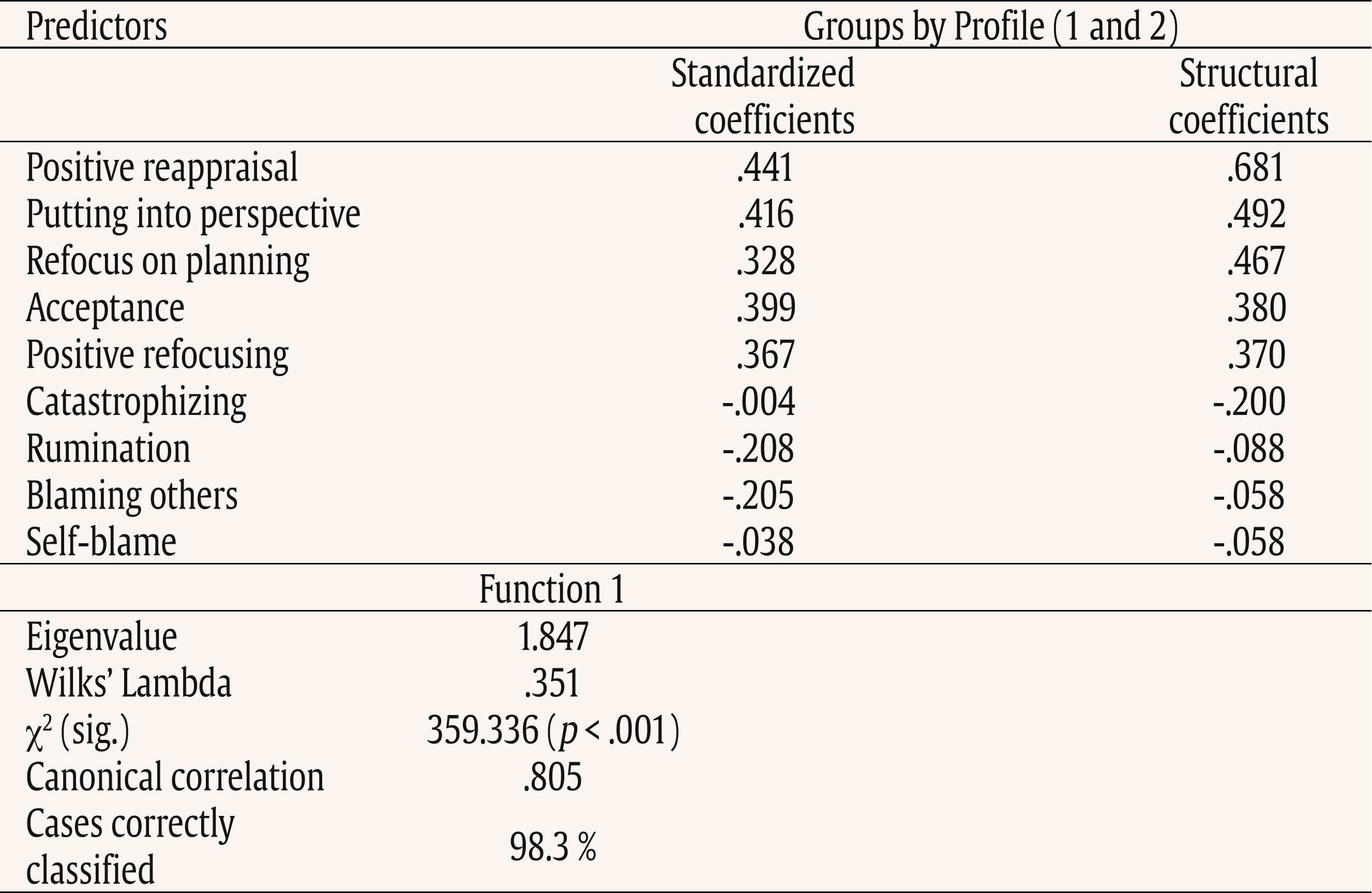 Comparison of Means between the two Cognitive Emotion Regulation Profiles in Trait Anxiety, Trait Anger, Depressive Symptomatology, and Positive and Negative Affect Finally, with the aim of defining the two profiles in those variables related to trait anxiety and anger, depressive symptoms, and positive and negative affect, we analyzed the differences of means between the two groups obtained in the cluster analysis, taking as dependent variables the scores on: a) trait anger (STAXI-T), b) trait anxiety (STAI-T), c) depressive symptoms (BDI), and d) positive affect (PANAS-PA) and negative affect (PANAS-NA). Table 4 shows the results obtained for each profile. Statistically significant differences were found in all the variables except negative affect, the effect sizes being high in trait anxiety and depressive symptomatology, moderate in positive affect, and small to moderate in trait anger. Those in Profile 1 scored significantly higher on depressive symptomatology, trait anxiety and trait anger, while those in Profile 2 scored significantly higher on positive affect. Table 4 Discussion Difference of Means between the two Profiles in Trait Anxiety, Trait Anger, Depressive Symptomatology, and Positive and Negative Affect  Note. 1Equal variances are not assumed; g = Hedges’ g; CI (95%) = confidence interval (95%); g = 0.20 (small), 0.50 (medium), 0.80 (large). *p < .05, **p < .01. Emotion regulation, a concept involving processes of a biological, social, behavioural, and cognitive nature, is itself an automatic or controlled, conscious or unconscious process in individuals that influences their own emotions, those of others, or both (Gross & Thompson, 2007). In the present study we explore in depth the relationship between cognitive disposition for emotional coping and depressive symptoms, anxiety, anger, positive affect, and negative affect. One of the novelties of this work is that it focuses both on the variables studied (the cognitive dimensions of emotion regulation) and on the individuals in whom these variables are measured. Thus, after having quantified the dimensions, two types of individual are identified, which form the basis for all the analyses, facilitating application of the results to clinical practice, insofar as the working unit is the individual him/herself. According to the hypotheses proposed, three main results emerge from our study. First, we identified two cognitive emotion regulation styles that differ as regards frequency of use of the regulation strategies considered as adaptive (acceptance, positive refocusing, refocus on planning, positive reappraisal, putting into perspective), and not by the frequency of use of the less adaptive strategies. Thus, those in the sample can be categorized according to their use of one set or the other of cognitive emotion regulation strategies. People situated in the “protector” profile (Profile 2) more frequently use strategies considered as adaptive, whilst such strategies are less likely to be used by those categorized in the “vulnerable” coping style group (Profile 1). These findings are in line with those suggesting a relationship between depressive symptoms and more frequent use of strategies such as rumination or suppression of emotion, as opposed to those that require more cognitive resources, such as positive reappraisal (Aldao & Nolen-Hoeksema, 2010; Campbell-Sills, Barlow, Brown, & Hofmann, 2006; Garnefski & Kraaij, 2007). Our results also appear to support the claim that psychological disorders are characterized by more rigid responses to the context (see Aldao, 2013; Aldao, Sheppes, & Gross, 2015; Bonanno & Burton, 2013), and this concordance constitutes further empirical evidence of the conceptual validity of the regulation profiles obtained. Second, of all the cognitive emotion regulation strategies studied, positive refocusing and, above all, positive reappraisal are those that best discriminate between Profiles 1 and 2 in this study. Identification of these profiles reveals that the criterion for distinguishing the two types of individual is based on the positive (adaptive) pole of cognitive emotion regulation. Thus, whilst the frequent use of less adaptive strategies does not permit the ascription of a person to one regulation profile or the other, the frequent use of so-called adaptive strategies is a sufficient condition for categorizing an individual in the “protector” profile. This result highlights the importance of promoting the use of adaptive strategies as a protective factor in the face of unpleasant situations or negative emotions such as sadness, fear or anger, as well as the importance of promoting and working on strategies more related to a healthy profile. The existence of different regulation profiles may derive from the fact that certain biases in information processing become chronic. Research focusing on individual differences in processes involving attention and memory has shown that these can affect the selection of strategies and the true effectiveness of emotional control in the context of affective disorders (Compas et al., 2017; Joormann & Gotlib, 2010; Nolen-Hoeksema, Wisco, & Lyubomirsky, 2008). At the same time, interest in fathoming out the explicit and implicit mechanisms of emotional regulation is helping researchers to improve their understanding of the different forms of such regulation and their consequences. Frequent use of a specific explicit strategy, during the process of emotional regulation, can feed or trigger a more implicit one, which, over time, may become more or less automatic – that is, become integrated into an individual’s habitual forms of response (Gross, 2015; Gyurak, Gross, & Etkin, 2011; Naragon-Gainey, McMahon, & Chacko, 2017). The level of automaticity of emotion regulation strategies, in addition to making it more difficult to separate processes of generation of emotions from those of regulation, highlights the importance of the degree of inflexibility of attentional and perceptual biases or unconscious appraisal – all sources of modulation of the various forms (more or less rigid) of response to potentially stressful situations. For example, in the types of scenario considered, a high internal, stable, and global attributional style, together with a high external, unstable, and specific attributional style for positive events constitute a more or less automatized form of interpreting situations that can result in depression (Fresco, Alloy, & Reilly-Harrington, 2006) and which, moreover, would make it difficult to use positive reappraisal. Such rigidity or inflexibility is common among patients encountered in clinical practice. Cognitive-behavioural therapy has been used for decades in interventions that directly address attentional biases or irrational interpretations in the face of situations that trigger a person’s emotional universe. In emotional disorders, such as depression and anxiety, these types of intervention in adults have shown themselves to be effective in both the short and long term (Dobson & Dobson, 2018; Hofmann, Asnaani, Vonk, Sawyer, & Fang, 2012). Thirdly and finally, the results of the present study suggest that the use or non-use of these forms of cognitive emotion regulation appears to be directly related to presenting higher or lower levels of depressive symptomatology and higher or lower scores on trait anxiety, and this could be taken into account on intervening in anxiety- or depression-based disorders. These results coincide, indeed, and from the perspective of the individual’s disposition, with those from other studies on depression and the use of emotion regulation strategies (Aldao et al., 2010; Kring & Sloan, 2010; Potthoff et al., 2016), which indicate that depression is associated with more frequent use of regulation strategies such as suppression or rumination, and less frequent use of other strategies, such as positive reappraisal. The differentiating role of the positive reappraisal strategy highlights the importance given to it in previous studies focusing on its nature and its relation to the experience of certain emotions. In this regard, research has confirmed the beneficial role of positive reappraisal given its association with positive affect, good interpersonal functioning, and higher levels of well-being (Gross & John, 2003). It has also been observed in experimental contexts that when those individuals who show greater use of this strategy are faced with an unpleasant task there is greater activation of the prefrontal brain regions involved in cognitive control (Drabant, McRae, Manuck, Hariri, & Gross, 2009) and in response to anger-inducing stimuli they present a healthier psychological profile (Mauss, Cook, Cheng, & Gross, 2007). The results of the present study, from a dispositional perspective of emotion regulation, would be in line with the conclusions of these previous works. To summarize, the results of the present study show that there are idiosyncratic aspects suggesting the existence of different cognitive emotion regulation styles. The two profiles identified are distinguished by higher frequency of so-called adaptive strategies (Profile 2) and lower frequency of use of such strategies (Profile 1). The category of adaptive strategies would include acceptance, positive refocusing, refocus on planning, positive reappraisal, and putting into perspective and, within this group, positive reappraisal is the strategy that best permits quantification of the differences. Membership of the “protector” group – less prone to presenting adverse psychological symptoms – would be determined by better disposition in stressful situations to reappraise the emotional valence of the situation, that is, to change the affective valence from negative to positive. In contrast, the “vulnerable” profile could be hindering the person’s optimal functioning by drastically reducing the range of strategies available in response to potentially stressful and unpleasant situations. In turn, it is essential to take into account an individual’s idiosyncrasies and personal cognitive style of regulating his or her emotions, in both prevention and intervention programmes. A limitation of this study is the methodology, which is based on the cluster analysis, so the results are tentative. We should stress, in concluding, the need for longitudinal research that would permit the study not only of how cognitive emotion regulation strategies work in different contexts (community, educational, clinical, etc.), but also of the extent to which the profiles identified are stable or subject to change. In terms of clinical implications, the differentiation of these two profiles of cognitive emotional regulation may be relevant for the study of the etiological factors of affective disorders and for their treatment. The results of this study suggest the convenience of including the coping styles most used by the patient in evaluation protocols. Also, it can be used as a tool in health promotion and prevention programs. In the first case, through the learning and implementation of adaptive regulation strategies; in the second case, it allows for the detection of people at risk, facilitating their monitoring and early intervention. Additionally, emotional regulation is presented as a key transdiagnostic factor that is common to different psychopathological syndromes (Aldao & Nolen-Hoeksema, 2010). This characteristic can play a relevant role in the most current mental health research frameworks (Fernandez, Jazaieri, & Gross, 2016). Future research related to the profiles of cognitive emotion regulation could include analysis of potential moderating and mediation factors – e.g., attachment styles (Malik, Wells, & Wittkowski, 2015) or the influence of social context (Marroquin & Nolen-Hoeksema, 2015) –, the study of the structure and dynamics of the regulatory profiles themselves – e.g., effects derived from the variability and flexibility in the use of different strategies (Aldao et al., 2015; Kuppens , Allen, & Sheeber, 2010)–, as well as the interaction of each of them with the context in which they are used (Dixon, Aldao, & De Reyes, 2015). Cite this article as: Lasa-Aristu, A., Delgado-Egido, B., Holgado-Tello, F. P., Amor, P. J., & Domínguez-Sánchez, F. J. (2019). Profiles of cognitive emotion regulation and their association with emotional traits. Clínica y Salud, 30, 33-39. https://doi.org/10.5093/clysa2019a6 References |
Cite this article as: Lasa-Aristu, A., Delgado-Egido, B., Holgado-Tello, F. P., Amor, P. J., & Domínguez-Sánchez, F. J. (2019). Profiles of cognitive emotion regulation & their association with emotional traits. Clínica y Salud, 30, 33-39. https://doi.org/10.5093/clysa2019a6
Correspondence: alasa@psi.uned.es (A. Lasa-Aristu).
Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
Clinical and Health is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License








