


The Stress-Buffering Effect of Social Support on Socio-Economic Disparities in Mental Health among Cancer Survivors
Dafina Petrova1, 2, 3, 4, Daniel Redondo-Sánchez1, 2, 3, Blanca Madrid Pérez-Esparza1, 2, Pablo Fernández-Navarro3, 5, Mitti Blakoe6, Raquel Luque Caro1, 4, Maria-José Sánchez1, 2, 3
1Instituto de Investigación Biosanitaria ibs.GRANADA, Granada, Spain; 2Escuela Andaluza de Salud Pública, Granada, Spain; 3CIBER de Epidemiología y Salud Pública (CIBERESP), Madrid, Spain; 4Medical Oncology, Hospital Universitario Virgen de las Nieves, Granada, Spain; 5Cancer and Environmental Epidemiology Unit, National Center for Epidemiology, Carlos III Institute of Health, Madrid, Spain; 6Department of Anaesthesia and Intensive Care, Bispebjerg and Frederiksberg Hospital, University of Copenhagen, Copenhagen, Denmark
https://doi.org/10.5093/pi2026a9
Received 13 August 2025, Accepted 15 December 2025
Abstract
Background: Low socio-economic status (SES) is considered a major chronic stressor and is frequently associated with worse mental health among cancer survivors. We investigated the extent to which social support could mitigate the negative impact of low SES on the mental health of individuals with a history of cancer. Method: Participants were cancer survivors identified in two nationally representative surveys conducted in Spain in 2017 (n = 1,143) and 2023 (n = 980). SES was measured with the social class index of the Spanish Society of Epidemiology. Social support was measured with the Duke-UNC questionnaire and the Oslo Social Support Scale. Mental health outcomes included psychological distress (General Health Questionnaire-12), mental well-being (WHO-5 Index), and depression (Patient Health Questionnaire-8). The moderating role of social support was examined in a multiple regression framework, complemented by generalized additive models to capture potential non-linear effects. Results: Mental health vulnerability was highest among individuals with low levels of social support, where no SES-related differences were observed. Under medium social support, low SES was linked to higher psychological distress (B = 0.24, 95% confidence intervals, CI [0.05, 0.42]), lower mental well-being (B = -6.08 [-1.98, -10.18]), and higher rates of depression (OR = 2.78 [1.52, 5.00]). High social support buffered this effect, improving mental health among cancer survivors with low SES and reducing SES differences. Sub-group analyses revealed that this buffering effect was less evident among women, for whom inequalities persisted regardless of social support levels. Discussion: High social support consistently attenuated SES disparities across three different mental health outcomes, albeit less effectively among women.
Keywords
Cancer survival, Mental health, Psychological distress, Depression, Socio-economic status, Health disparities, Social support, Buffering effect
Cite this article as: Petrova, D., Redondo-Sánchez, D., Madrid Pérez-Esparza, B., Fernández-Navarro, P., Blakoe, M., Luque Caro, R., & Sánchez, M. (2026). The Stress-Buffering Effect of Social Support on Socio-Economic Disparities in Mental Health among Cancer Survivors. Psychosocial Intervention, 35, Article e260817. https://doi.org/10.5093/pi2026a9
Correspondence: Daniel.Redondo.easp@juntadeandalucia.es (D. Redondo-Sánchez).
Cancer does not affect everyone equally—there are pervasive socio-economic inequalities across the cancer continuum (Li et al., 2024). People with lower socio-economic status (SES), commonly identified by indicators such as education, income, or deprivation levels are at higher risk of developing several types of cancer (Li et al., 2024; Mihor et al., 2020). People with lower SES also have shorter survival, largely due to more advanced stage at diagnosis, more comorbidities, and less access to certain cancer treatments (Afshar et al., 2021; Li et al., 2024; Redondo-Sánchez et al., 2022). These socio-economic inequalities persist beyond the clinical treatment phase. Cancer survivors with low SES often report poorer quality of life (Ashing-Giwa & Lim, 2009; Kobayashi et al., 2008) and worse mental health outcomes (Chidobem et al., 2022). Studies with diverse cancer populations, including breast, colorectal, and prostate cancer survivors (Andrykowski et al., 2013; Simon & Wardle, 2008), consistently show that those with lower SES are more likely to report psychological distress, anxiety, or depression (Abdelhadi, 2023; Chidobem et al., 2022; Zeilinger et al., 2023). While socio-economic disparities in mental health are present in the general population (Kirkbride et al., 2024), they may be exacerbated among cancer survivors, who already are at higher risk of poor mental health due to their illness experience (Carreira et al., 2018; Forbes et al., 2024). The reasons behind these socio-economic inequalities are likely multiple, complex, and highly context-dependent. Low SES is considered a major chronic stressor (Baum et al., 1999), increasing exposure to stress-generating conditions such as unsafe neighborhoods, discrimination, work instability, financial difficulties, domestic problems, and interpersonal conflict (Baum et al., 1999; Turner et al., 1995). These challenges can be exacerbated after cancer diagnosis. Additionally, cancer survivors with lower SES may also experience more structural barriers to accessing healthcare, including mental health services (Arega et al., 2021), due to lack of insurance, transportation difficulties, or geographic inaccessibility, to name but a few. Individuals with lower SES might also have fewer psychosocial resources available to help diffuse the psychological burden of cancer (S. E. Taylor & Seeman, 1999). One such key resource is social support, broadly defined as the emotional, instrumental, or informational resources provided by others that may be useful for helping to cope with problems (Wills & Ainette, 2012). Social support is one of the strongest predictors of health and longevity, showing associations comparable in magnitude to those of well-established risk factors such as smoking and physical activity (Holt-Lunstad et al., 2010). The availability of social support is also one of the factors most consistently related to better mental health and quality of life outcomes in cancer survivors (Efficace et al., 2016; Eom et al., 2013; Petrova, Redondo-Sánchez et al., 2021), including longitudinally (Fong et al., 2017). Whereas the positive health effect of social support is well documented, fewer studies have addressed its ability to act as a stress buffer. The “stress-buffering” hypothesis, first introduced by Cohen and Wills (1985) proposes that social support specifically mitigates, or “buffers,” the negative effects of stress on health. It becomes most beneficial when individuals are exposed to high levels of stress and its protective effects become especially critical during stressful periods. Cancer survivorship is one such stressful period and social support may thus be able to at least partially buffer the negative effects of low SES on mental health among cancer survivors. This could happen through social support mitigating some of the objective SES-related stressors (e.g., work circumstances, income constraints…) or by reducing their subjective impact (e.g., improving coping strategies and emotional appraisal) (S. E. Taylor & Seeman, 1999; Uchino et al., 2025; Wills & Ainette, 2012). More broadly, this stress-buffering function of social support aligns with the Biopsychosocial Model of Engel (1977), which views health and illness as emerging from the dynamic interplay of biological, psychological, and social factors, and with the Stress Process Model (Pearlin et al., 1981), which posits that psychosocial resources such as social support can moderate or mediate the effects of structural stressors such as socio-economic deprivation. To the best of our knowledge, only two studies have tested the SES stress-buffering effect of social support in cancer populations, showing mixed results. In a small study of 52 gastric cancer patients, social support buffered the effect of SES on anxiety, but not depression (Jeong & An, 2017). In contrast, in a larger study of 487 women with ductal breast carcinoma in situ, social support did not buffer the effect of SES on either anxiety or depression (de Moor et al., 2010). To build upon this limited evidence, we conducted a study using two large, nationally representative samples of cancer survivors in Spain, with the aim of providing a more robust examination of the stress-buffering role of social support in the context of socio-economic inequalities in cancer. We assessed multiple dimensions of mental health and used validated instruments to measure SES and social support. Specifically, consistent with an interaction between SES and social support, we expected SES-related disparities in mental health to be more pronounced under low to moderate levels of support, and to diminish—or even disappear—under conditions of high support. Finally, we also examined to what extent this moderating effect varies as a function of gender, age, and time since diagnosis, to explore potential intersectionality effects (Kapilashrami & Hankivsky, 2018), that have rarely been examined in previous studies. We used data from two surveys —the Spanish National Health Survey (NAHES) in 2017 and the Health Survey of Spain (HESUS) in 2023—in order to test the effects of interest in two independent but comparable samples. Both are periodic, nationally representative, cross-sectional population surveys conducted by the Spanish Ministry of Health in collaboration with the National Institute of Statistics (Spanish Ministry of Health, National Statistical Institute of Spain, 2025, 2018). They are part of a periodic series that follows a similar methodology to create a continuous health monitoring system. A multistage stratified random sampling design is used to obtain a representative sample of the adult Spanish population (≥ 15 years old). Data were collected by trained interviewers through computer-assisted personal structured interviews (CATI) in NAHES 2017 and a combination of computer-assisted web interviewing (CAWI) and CATI in HESUS 2023. For each survey, a total of 37,500 households were initially selected across 2,500 census sections. These sections were grouped into six strata based on the population size of the municipalities they belonged to and were selected with a probability proportional to their size. Within each census section, 15 households were randomly chosen, and from each household, one adult was randomly selected to participate. Data collection was conducted between October 2016 and October 2017 for NAHES, and September 2023 and August 2024 for HESUS. The final samples included 23,090 respondents in NAHES (response rate of 72.2%) and 21,032 respondents in HESUS (response rate of 62.4%). The eligible study population for the current research included all participants in both surveys who self-reported having ever been diagnosed with cancer (malignant tumor) (n = 1,186 participants in NAHES and n = 1,100 in HESUS). This study was exempt from ethical committee review because it was based on anonymized secondary data analysis. Measures Socioeconomic status (SES), demographic characteristics, and clinical history variables were measured in a similar way across both surveys, whereas social support and mental health outcomes were measured with survey-specific instruments, as described below. Socio-economic Status This was assessed using the occupational social class classification of the Spanish Society of Epidemiology (Domingo-Salvany et al., 2013) in both surveys. Information about occupation and education is used to classify participants into one of six categories following a pre-established algorithm. For individuals who were retired, unemployed, students or homemakers, the occupation of the main income earner in the household is used for classification. For the current study, the highest three categories were assigned to the high SES group (including directors and managers, professionals with university degrees and other technical support professionals, sportsmen and artists, intermediate occupations, and self-employed workers), whereas the lowest three categories were assigned to the low SES group (supervisors and workers in qualified technical occupations, qualified workers from the agricultural and primary sector, other semi-skilled workers, and unskilled workers). Demographic and Clinical History Variables These included gender (male vs. female), age (in years and categorized as younger (< 65 years) vs. older (≥ 65 years), and civil status (married, separated/divorced, single, or widowed). Time since cancer diagnosis was recorded as recent (diagnosis within the past 12 months) vs. longer-term (diagnosed more than 12 months prior the survey). Consultation with a mental health care professional (MHCP) was assessed by asking participants whether they had seen a psychologist, psychiatrist, or psychotherapist within the previous 12 months preceding the survey (yes vs. no). History of mental health conditions was determined based on self-reported previous diagnosis of chronic anxiety or depression (yes vs. no). Additionally, a weighted physical comorbidity index was calculated as a measure of multimorbidity burden, based on self-reported information about history of 28 chronic somatic conditions, following a pre-established methodology (Petrova, Redondo-Sánchez, et al., 2021). Social Support In NAHES 2017, this was measured with the Spanish adaptation of the Duke-UNC Functional Social Support Questionnaire (Bellón Saameño et al., 1996). This instrument consists of 11 items that measure perceived social, emotional, and instrumental support (examples: “I receive help when I am sick in bed”, “I get useful advice about important things in life”, or “I get invitations to go out and do things with other people”). Responses are scored on a 5-point Likert scale, ranging from 1 (much less support than I want) to 5 (as much support as I want). Total score ranges from 11 to 55 (Cronbach’s alpha = .91), with higher scores reflecting greater perceived social support. In HESUS 2023, social support was measured using the Oslo Social Support Scale (OSS-3), a brief three-item instrument (Kocalevent et al., 2018). The items ask about the number of close confidants (from more than 5 to none), the sense of concern from other people (from a lot to none), and the ease of getting help from neighbors (very easy to very difficult), resulting in a final score from 3 to 14 (Cronbach’s alpha = .52), with higher scores reflecting greater levels of social support. Modest internal consistency is characteristic for this instrument, which is designed to measure three different aspects. Mental Health In NAHES 2017, the Spanish version of the 12-item General Health Questionnaire (GHQ-12) (Sánchez-López & Dresch, 2008) was used to measure psychological distress. This widely used screening tool identifies common mental health disorders in both the general population and clinical settings, assessing aspects such as perceived stress, coping ability, and self-esteem over the past few weeks. The questionnaire includes 12 items (Cronbach’s alpha = .93), each with four response options scored using a binary method (0-0-1-1), resulting in a total score ranging from 0 to 12. Higher scores indicate greater levels of psychological distress. In HESUS 2023, two validated instruments were used to assess mental health outcomes. The World Health Organization-Five Well-Being Index (WHO-5) (Topp et al., 2015) was used to measure mental well-being. It consists of five positively framed statements (e.g., “I have felt cheerful in good spirits”, “My daily life has been filled with things that interest me”) relating to the past two weeks. Each statement is rated on a 6-point Likert scale from 0 (at no time) to 5 (all of the time), and the final score is multiplied by 4 to obtain a percentage score from 0 to 100, where higher scores indicate better mental well-being (see Supplementary Material 1 for information on internal consistency). The Patient Health Questionnaire-8 (PHQ-8) (Kroenke et al., 2009; Muñoz-Navarro et al., 2017) was administered to screen for depression. PHQ-8 is a validated instrument composed of 8 items corresponding to diagnostic criteria for depressive disorders in the DSM-IV, each asking about the past two weeks and scored from 0 (not at all) to 3 (nearly every day), for a total possible score of 0-24 (see Supplementary Material 1 for information on internal consistency). Participants were classified as having significant depressive symptoms according to an established diagnostic algorithm for “major depression” (requiring either the first or second item (depressed mood or anhedonia) to be present more than half the days and at least 5 of the 8 symptoms to be present more than half the days) or “other depression” (two to four symptoms, including either depressed mood or anhedonia, are required to be present more than half the days). Final Sample Size and Minimum Detectable Effect Size From the eligible participants who self-reported a previous cancer diagnosis (1,186 in NAHES 2017 and 1,100 in HESUS 2023), only those with available data on the main measures of interest were retained for analysis (1,143 participants in NAHES and 980 in HESUS) (see Supplementary Material 2). We calculated the minimum detectable sample size for the hypothesized buffering effect by conducting simulations with the InteractionPoweR package (Baranger et al., 2023) particularly when variables are correlated and continuous. Moreover, although power is affected by main effects, their correlation, and variable reliability, it can be unclear how to incorporate these effects into a power analysis. The R package InteractionPoweR and associated Shiny apps allow researchers with minimal or no programming experience to perform analytic and simulation-based power analyses for interactions. At minimum, these analyses require the Pearson’s correlation between variables and sample size, and additional parameters, including reliability and the number of discrete levels that a variable takes (e.g., binary or Likert scale. Results based on 10,000 simulations for 11 different effect sizes showed that with the smallest available sample size (n = 980 in HESUS), interaction effects as small as 0.10 could be detected with excellent statistical power (≥ 88%) (see Supplementary Material 3 for detailed results). Statistical Analysis The social support scores were analyzed as a continuous variable and categorized into terciles (with the “medium” level as a reference), to be able to capture non-linear effects. In NAHES, the main outcome variable was the GHQ-12 score, which was analyzed as a continuous variable (log-transformed due to high skewness) and categorized into high (≥ 5) vs. low (< 5) psychological distress according to a cut-off identified for persons with history of cancer (Carlson et al., 2012; Vodermaier et al., 2009). Additionally, we created a variable identifying those participants with potentially unattended high psychological distress, characterized by GHQ12 scores ≥ 5 and reporting not having consulted a MHCP in the past year (vs. the rest of combinations). In HESUS, the main outcome variables were the WHO-5 mental well-being scores (analyzed as a continuous variable) and the PHQ-8 scores (categorized as depression vs. no depression). Similarly to NAHES, we created a variable identifying those participants with potentially unattended depression, characterized by depression identified with the PHQ-8 algorithm and reporting not having consulted a MHCP in the past year (vs. the rest of combinations). To address the main study objectives, we conducted moderation analyses using the PROCESS macro implemented in R (Hayes & Little, 2022). This was based on multiple linear regressions on the continuous outcomes (GHQ-12 and WHO-5 in NAHES and HESUS, respectively) and multiple logistic regressions on the categorical outcomes (significant psychological distress and depression in NAHES and HESUS, respectively). The models were adjusted for age, gender, time since cancer diagnosis, comorbidities, and previous mental health condition. In order to test the buffering effect of social support, an interaction term between SES and social support was tested (Model 1 in the PROCESS macro). In addition, conditional effects and 95% confidence intervals (CI) for the effect of SES at different levels of social support were estimated. For linear regression models, Johnson-Neyman intervals were calculated using the Interactions package in R to explore the values of social support at which SES had significant effects (Long, 2024). Table 1 Descriptive Statistics (n (%) for Categorical Variables and Mean ± Standard Deviation (median, interquartile range for continuous scores) for All Study Variables in the National Health Survey of Spain 2017 (NAHES: n = 1,143) and the Health Survey of Spain 2023 (HESUS: n = 980) 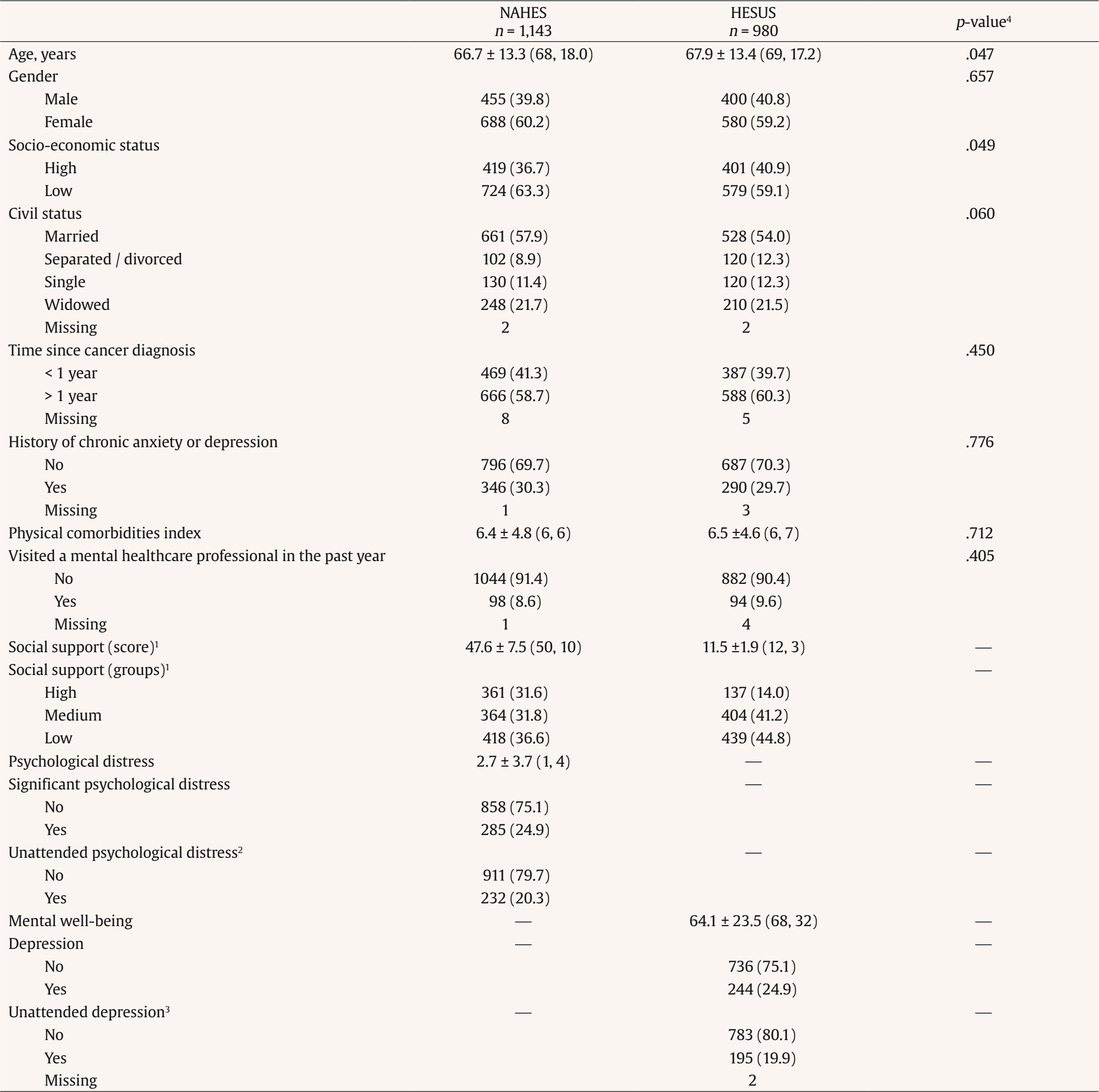 Note. 1Based on the Duke-UNC questionnaire for NAHES 2017 and the OSS-3 scale for HESUS 2023. 2GHQ12 ≥ 5 and not having consulted with a mental healthcare professional (MHCP) in the past year. 3Depression identified with the PHQ-8 algorithm and reporting not having consulted a MHCP in the past year. 4Based on Student’s t-test for continuous variables and Fischer’s exact test for categorical variables. To explore non-linear effects, the interaction between SES and social support was tested using generalized additive models (GAM) with restricted maximum likelihood estimation in the MGCV package in R (Wood, 2017). The models included separate smooth functions for social support by SES group. The effective degrees of freedom (edf) for each smooth term were used to assess non-linearity and the differences between SES groups were examined using the Marginaleffects R package (Arel-Bundock et al., 2024). Finally, we investigated if there were differences in the buffering effect as a function of gender (male vs. female), age (<65 vs, ≥ 65 years old) and time since diagnosis (< 1 years vs. > 1 year ago) by conducting stratified analyses in each group. Table 2 Results from Multiple Linear Regression Models with Outcomes Psychological Distress (NAHES, n = 1,143) and Mental Well-being (HESUS, n = 980) 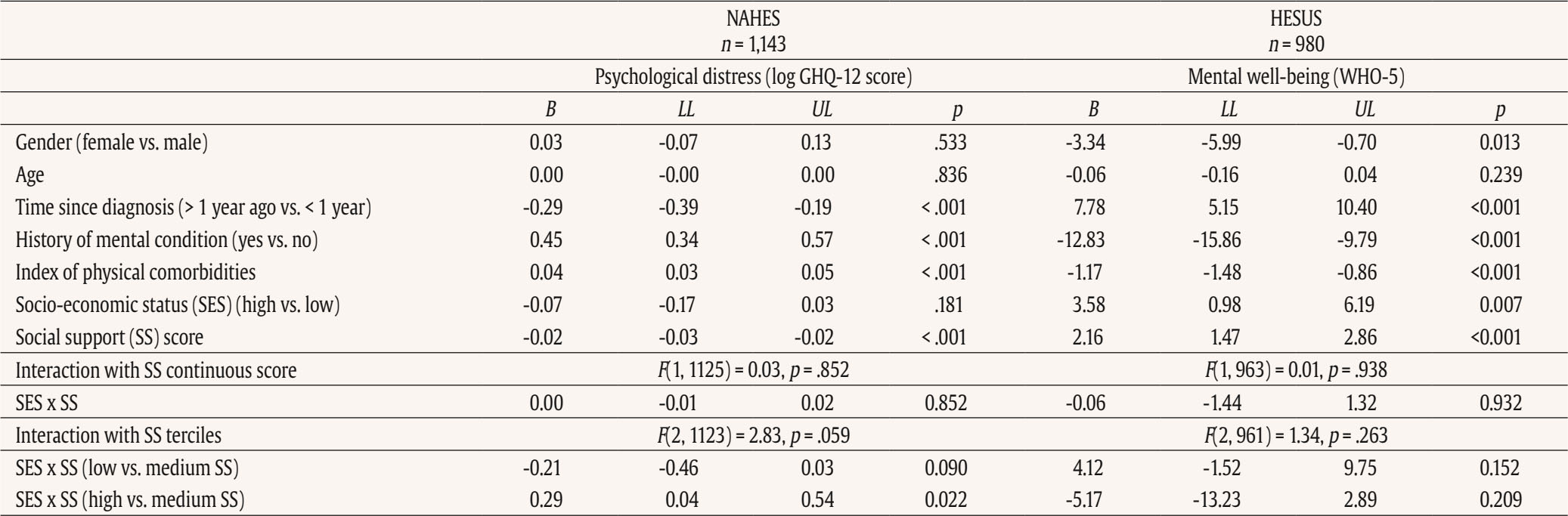 Table 3 Conditional Effects of Socio-economic Status (low vs. high) in the Different Social Support Terciles 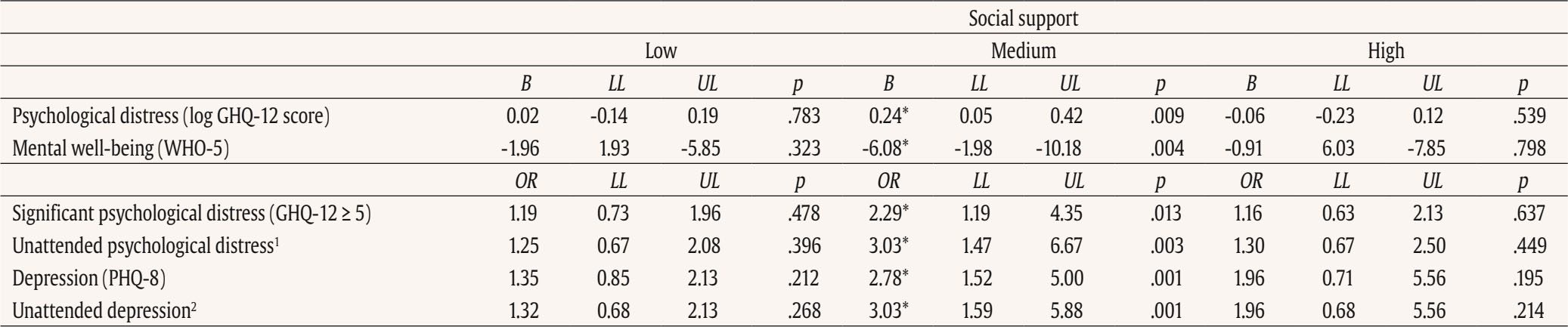 Note. Results are from models adjusted for age, gender, time since diagnosis, history of chronic anxiety or depression, and index of physical comorbidities. B =B unstandardized regression coefficient; OR = odds ratio; LL/UL = lower/upper level 95% confidence interval. 1GHQ12 ≥ 5 and not having consulted with a mental healthcare professional in the past year. 2Depression identified with the PHQ-8 algorithm and reporting not having consulted a MHCP in the past year. *p < .05. In both surveys, the majority of participants were female, married, and with low SES (see Table 1). There was a slightly higher proportion of participants with high SES in HESUS 2023. Participants in HESUS 2023 was also older, with median age 67 (range 19-96) in NAHES 2017 and 68 (range 20-97) in HESUS 2023. Regarding time since diagnosis, 41.0% and 39.7% were diagnosed in the preceding 12 months in NAHES and HESUS, respectively. Social support was high on average, with a median score of 50 (out of 55 maximum) in NAHES 2017 and 12 (out of 14) in HESUS 2023 (see Supplementary Materials, Figure S1). In NAHES 2017, the median score for the sample on the GHQ-12 questionnaire was 1 (range 0 to 12) and 24.9% were classified as having “significant mental distress” (GHQ score ≥ 5). In HESUS, the median well-being score was 68 out of 100, and 24.9% of participants were classified as positively screened for depression (14.2% with major depression and 10.7% with another depression). Psychological Distress (GHQ-12) in NAHES 2017 Lower social support was associated with higher psychological distress, but there was no effect of SES. There was no interaction between SES and the continuous social support score but there was evidence of an interaction with social support categorized into terciles (see Table 2). Stratified analyses showed that there was a significant effect of SES among participants with medium social support (B = 0.24, 95% CI [0.06, 0.42], p = .009), corresponding to exp(0.24) = 1.27, or 27% higher levels (ratio of geometric means) of mental distress among participants with low SES. However, there was no effect of SES among participants with low (B = -0.02 [-0.19, 0.15], p = .783) or high (B = 0.06 [-0.12, 0.23], p = .539) social support (see Table 3). Figure 1 displays this non-linear effect, such that psychological distress was highest among participants with low social support regardless of their SES; in contrast, under medium levels of social support participants with low SES reported significantly higher psychological distress than participants with high SES, a disadvantage that disappeared under high levels of social support. Figure 1 Psychological Distress in NAHES 2017 (n = 1,043) and Mental Well-being in HESUS (n = 980) as a Function of Socio-economic Status (SES) and Social Support Terciles. 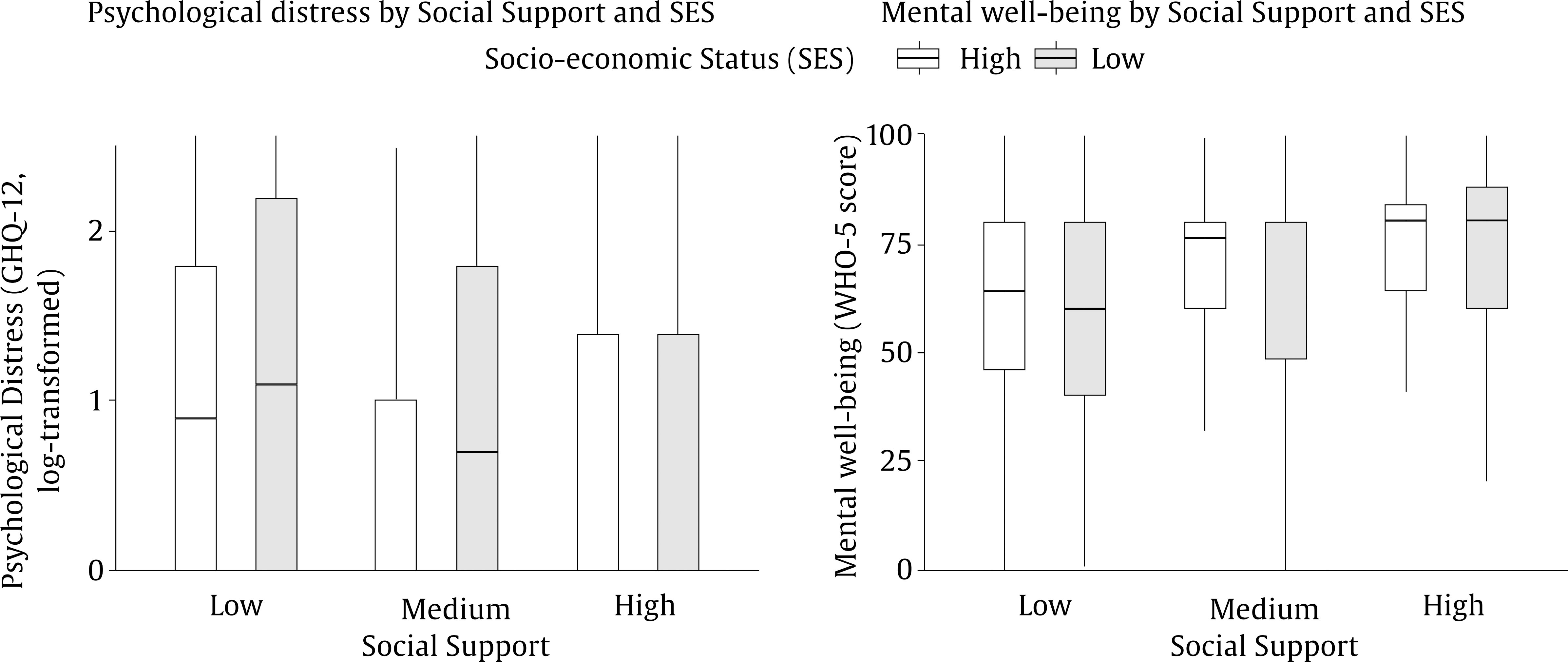 Note. The horizontal line inside the box represents the median and the box shows the interquartile range. The Johnson-Neyman analyses confirmed that an effect of SES (slope with p < .10) was observed for only medium levels of social support in the range between 38 and 47 on the 11-55 social support scale. The GAM models (see Supplementary Materials, Table S1) showed suggestive evidence for non-linearity of the social support effect in the low SES group (edf = 1.25, p < .001) and moderate evidence of non-linearity in the high SES group (edf = 1.78, p < .001). This translated into differences between SES groups only at medium levels of social support (Figure 2). Figure 2 Predicted Values of the Main Outcome Variables Shown as Smooth Functions of Social Support (Estimated Using Penalized Regression Splines), Separately for Each Level of Socio-economic Satus (SES). 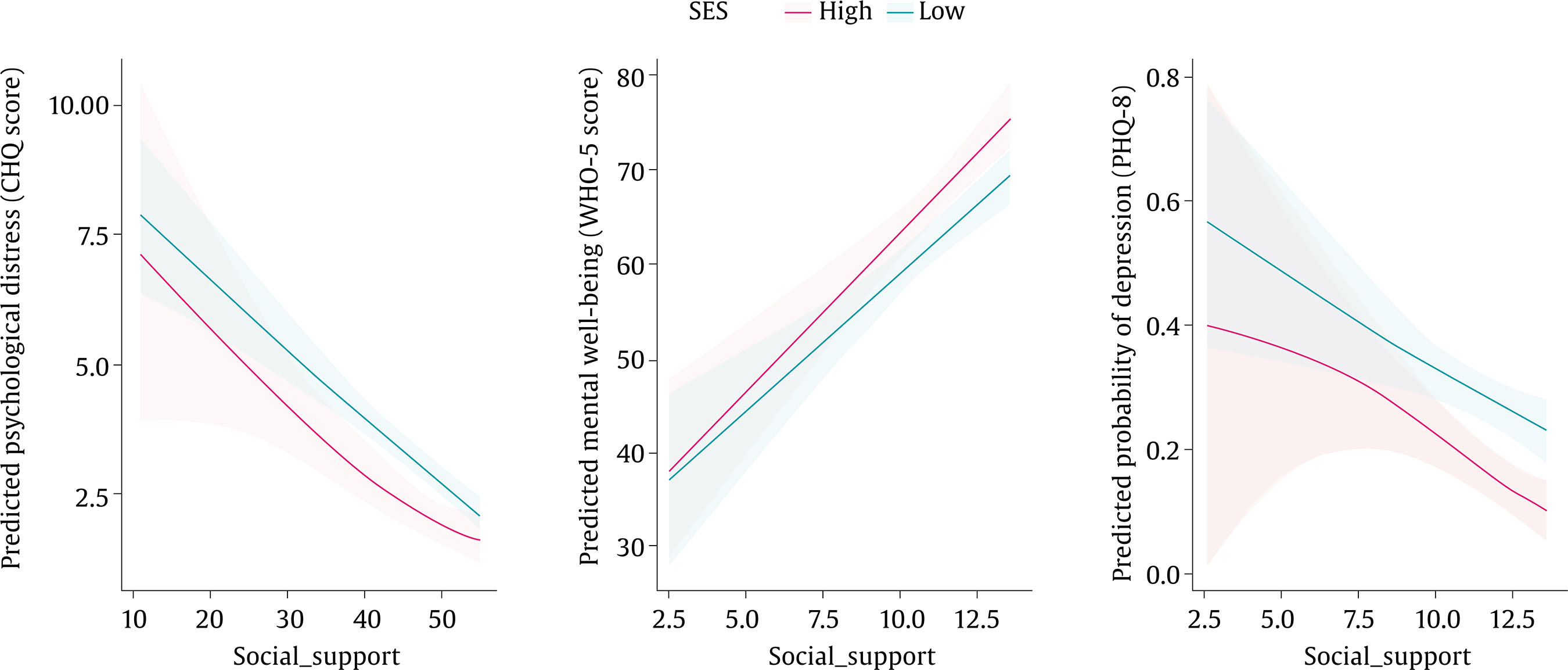 Note. Shaded areas are 95% confidence intervals. The results of multiple logistic regression models with outcomes significant psychological distress and unattended psychological distress showed a similar pattern (see Table 4 and see Supplementary Materials, Figure S2). There were significant differences among socio-economic groups only under medium levels of social support (Table 3), with participants with low SES having 2 to 3 times higher risk of significant (OR = 2.29 [1.19, 4.35]) or unattended (OR = 3.03 [1.47, 6.67]) psychological distress. In contrast, there were no significant SES differences under high levels of social support. In summary, the results from the different modeling approaches converge to indicate that SES differences in psychological distress were observed for medium levels of social support (values around the middle tercile) and disappeared under high levels of social support. Mental Well-being (WHO-5) in HESUS 2023 Higher SES and higher social support were associated with better mental well-being (Table 2). The interaction between SES and social support was not significant. However, the pattern of results was consistent with the previously observed. Mental well-being was lowest under low levels of social support, where no SES differences were observed. Socio-economic differences were present under medium levels of social support and disappeared with high social support (see Figure 2). Conditional effects analyses confirmed that there were significant SES differences only under medium levels of social support, such that participants with low SES had on average 6 points fewer on the WHO-5 well-being measure (B = -6.08 [-1.98, -10.18]), a difference that was not significant under high levels of social support. The Johnson-Neyman analyses confirmed that an effect of SES (slope with p < .01) was observed for only medium levels of social support in the range between 10 and 12 on the 3-14 social support scale. The GAM models (see Supplementary Materials, Table S1) were consistent with a linear association in both the low SES group (edf = 1.02, p < .001) and the high SES group (edf = 1.00, p < 0.001), which nevertheless translated into differences between SES groups at medium levels of social support (Figure 3). In summary, the results from the different modeling approaches converge to indicate that SES differences in mental well-being were observed for medium levels of social support (values around the middle tercile) and disappeared under high levels of social support. Table 4 Results from Multiple Logistic Regression Models with Outcomes Significant and Unattended Psychological Dstress (NAHES n = 1,143) and Depression and Unattended Depression (HESUS n = 980) 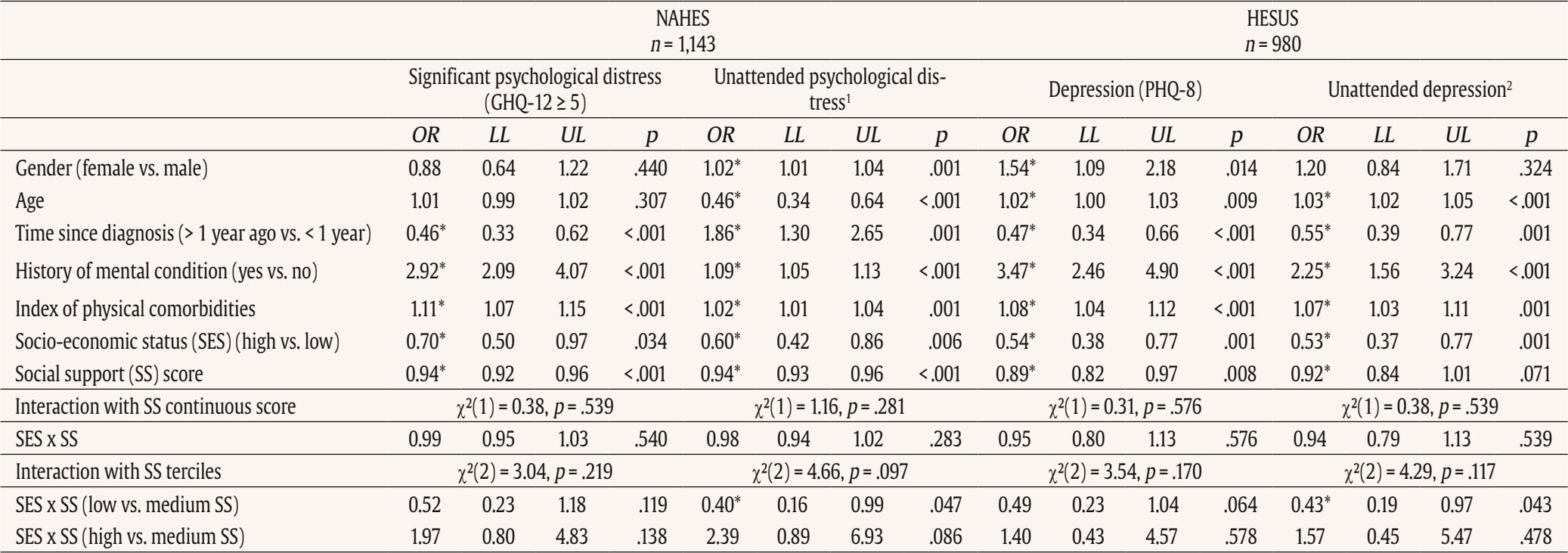 Note. OR = odds ratio; LL/UL = lower/upper level 95% confidence interval. 1GHQ-12 ≥ 5 and not having consulted with a mental healthcare professional in the past year. 2Depression identified with the PHQ-8 algorithm and reporting not having consulted a MHCP in the past year. *p < .05. Depression (PHQ-8) in HESUS 2023 Lower SES and lower social support were associated with higher odds of reporting depression (Table 4). The interaction between SES and social support was not significant. However, the results followed a similar pattern to the previously observed (see Supplementary Materials, Figure S2). Conditional effects analyses showed that under medium levels of social support, participants with low SES had 2 to 3 times higher risk of depression (OR = 2.78 [1.52, 5.00]) or unattended depression (OR = 3.03 [1.59, 5.88]) compared to participants with high SES. In contrast, there were no significant SES differences under high or low levels of social support (Table 3). The GAM models (see Supplementary Materials, Table S1) were consistent with a linear association in the low SES group (edf = 1.00, p = .006) and a non-linear association in the high SES group (edf = 1.67, p = .003). The most pronounced differences between SES groups were observed at medium levels of social support (Figure 3). Figure 3 Percentage of Participants with Depression (according to PHQ-8 algorithm) and Unattended Depression (depression identified with the PHQ-8 algorithm and reporting not having consulted a mental healthcare professional in the past year) according to Socio-economic Status and Social Support Tercile in HESUS 2023 (n = 980). 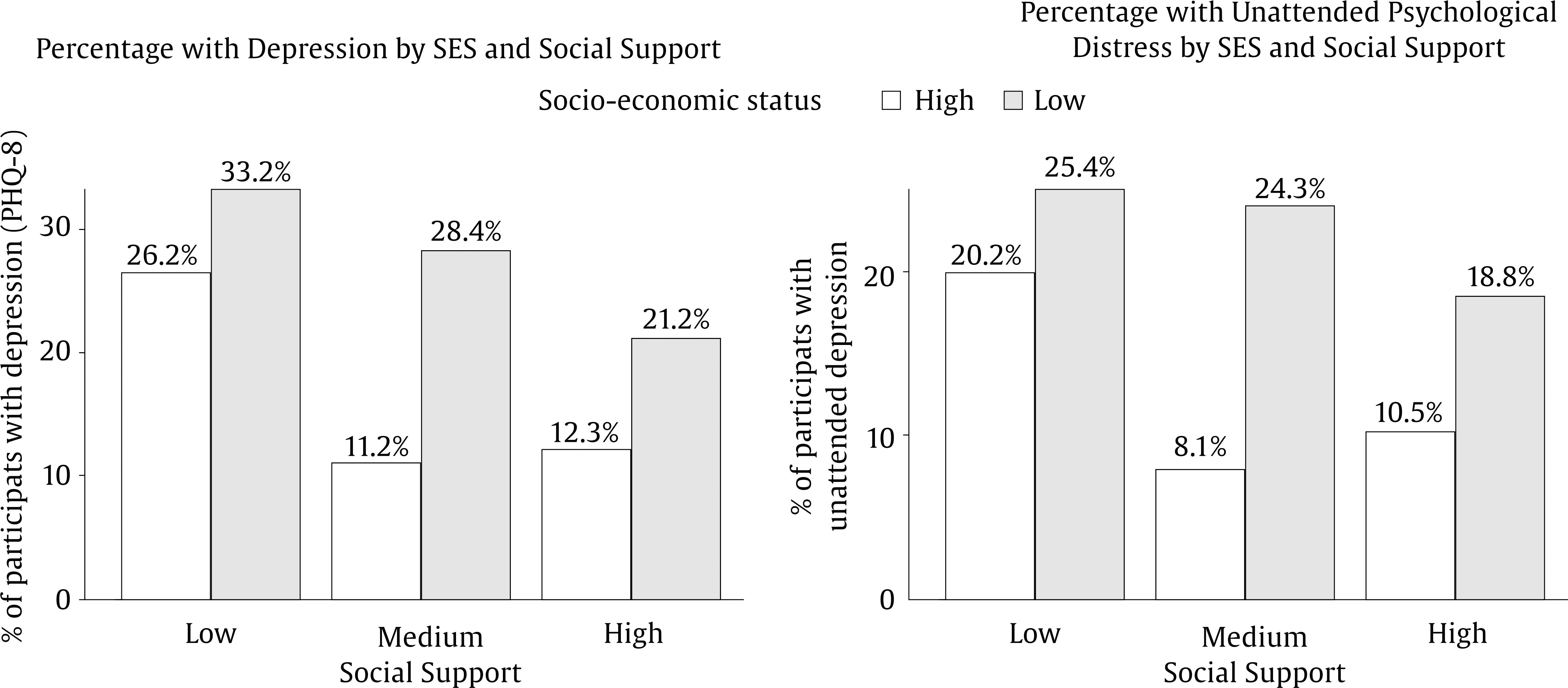 In summary, the results from the different modeling approaches converge to indicate that SES differences in depression prevalence were largest under medium levels of social support (values around the middle tercile) and smaller under high levels of social support. Socio-demographic and Clinical History Variables Overall, worse mental health outcomes were reported by women (in HESUS 2023), older individuals, individuals diagnosed within the past year, with previous history of a mental health condition, and with a higher physical comorbidity index (Tables 2 and 4). We next explored if the observed buffering pattern persisted for the main outcomes in different groups based on gender (male vs. female), age (< 65 vs. ≥ 65 years old), and time since diagnosis (< 1 vs. > 1 year ago). Gender Differences Both the PROCESS moderation analyses (see Supplementary Materials, Table S2) and the GAD non-linear models showed evidence for gender differences (see Supplementary Materials, Table S1). In particular, the buffering pattern was not observed for women neither on psychological distress in NAHES 2017, nor on mental well-being in HESUS 2023. In both cases, females with low SES reported worse mental health regardless of social support levels (see Supplementary Materials, Figures S3 and S4). Smaller gender differences were observed for depression in HESUS 2023 (see Supplementary Materials, Figure S4 and S5). Age Differences Results among younger survivors (< 65 years old) were more heterogenous and there was less consistent evidence for the buffering pattern in this group on psychological distress and mental well-being (see Supplementary Materials, Table S2, Figure S6 and S7). Because the younger group comprised survivors with very diverse ages, we further explored additional differences by fitting the GAM models separately for participants 18-49 years old and 50-64 years old (see Supplementary Materials, Figure S8). Overall, the pattern of results in the 50-64 age group was relatively similar to what was observed for 65+. However, results for survivors 18-49 years old more were heterogenous: mental health indicators were better among individuals with higher social support, however there was no consistent effect of SES (see Supplementary Materials, Figure S8). In the case of depression in HESUS 2023, differences between age groups were less pronounced and more heterogenous in nature (see Supplementary Materials, Figure S5, S7, and S8). Time since Diagnosis There was heterogeneity in the effects of SES and social support as a function of time since diagnosis (see Supplementary Materials, Table S2, Figures S9 and S10). However, there were no consistent interpretable differences in the pattern of results for the buffering effects across outcomes. We found partial support for the stress-buffering effect of social support in two large population-based samples of cancer survivors in Spain. In particular, we found that high levels of social support buffered the socio-economic inequalities in mental health observed under medium levels of social support. Among participants who reported some lack of social support, lower SES was consistently related to worse mental health outcomes, including higher psychological distress, lower mental well-being, and higher rates of depression, even after adjusting for key socio-demographic and clinical factors. However, among participants who reported high levels of social support, SES differences in mental health outcomes were either non-significant or substantially reduced. This suggests that social support may act as a protective factor, helping to neutralize the adverse mental health effects associated with low SES in the context of cancer survivorship. In contrast to our expectations, there were no SES-related differences among individuals under low levels of social support, who showed the highest mental health vulnerability regardless of SES. This finding suggests that the absence of social support may exert such a strong detrimental effect that it overrides the potential benefits of higher SES, highlighting the critical role of social support in shaping mental health outcomes after cancer. In addition to our main analysis, we adopted an intersectionality lens (Kapilashrami & Hankivsky, 2018), exploring socio-economic disadvantage dynamics as a function of gender, age, and time since diagnosis. The buffering effect of social support was observed in the whole study sample but in gender-stratified analyses it was mostly constrained to men. Among women, some extent of SES inequalities in psychological distress and mental well-being persisted across all levels of social support. This aligns with prior evidence showing gender differences in the availability, stability, and type of support cancer patients receive. For example, in a longitudinal study of patient-partner dyads, men consistently received high levels of partner support over time, whereas support to female patients declined; at the same time, female partners maintained high levels of support provision, while male partners’ support decreased (Luszczynska et al., 2007). Such asymmetry may disadvantage women during illness. More recently, J. Zhang et al. (2025) found that female cancer patients—particularly those with high psychological distress—reported substantially greater supportive care needs than men. In our context, this suggests that women, especially those with lower SES, may have additional needs not captured by the social support measures used or may experience forms of distress that social support alone cannot mitigate. More broadly, Belle (1982) argued that the stresses of low SES can constrain social networks, weaken marital relationships, limit neighborhood support, and turn social ties into sources of strain or dependency. These patterns may be especially pronounced for women with lower SES and may reduce the buffering potential of social support. Similar gender-specific effects of social support have been observed outside of oncology, in a study on cardiovascular prevention in Spain, where social support was found to be beneficial for men but not for women (Blakoe et al., 2023). Women are at higher risk of experiencing psychological distress and depression (Hyde & Mezulis, 2020)—in the general population and following a cancer diagnosis—something that was also confirmed in the current study. Women are also at a higher risk of financial toxicity following cancer treatment (Ginsburg et al., 2023), something that can be particularly exacerbated among those with lower SES. Our findings suggest that, although social support may help buffer some of the mental health vulnerability among female cancer survivors, it may not be sufficient to eliminate the socioeconomic inequalities they experience. These results underscore the need for targeted psychosocial interventions that explicitly consider the intersection of gender and socioeconomic disadvantage in cancer survivorship. Similarly, there was less evidence of the buffering effect among younger survivors, a population where cancer may have different social and economic impact (Islam et al., 2022). Our exploratory analyses showed a different pattern of results for the youngest survivors below 50 years old. In this group, social support showed a general beneficial association with mental health, yet no consistent socio-economic inequalities emerged. One possible explanation is that the SES index used in our study may not adequately capture the specific socio-economic circumstances—such as unemployment or unstable work—that have been linked to poorer mental health in younger cancer survivors (Dahl et al., 2019; Lane et al., 2021). Notably, for students and unemployed individuals, SES classification is based on the occupation of the main income earner, which may obscure key socio-economic circumstances. Overall, a more detailed and multidimensional SES assessment may be needed to detect inequalities and to more accurately examine the buffering role of social support, together with other important variables in this population, such as emotional regulation (Baziliansky & Cohen, 2021). Multiple mechanisms could explain how social support can buffer socio-economic inequalities in mental health (Thoits, 2011; Uchino, 2006). In particular, social support from others can provide structural, informational, or functional resources that help mitigate some of the financial, domestic, or employment problems associated with low SES that are likely to be exacerbated after cancer. Some supporting evidence for this is found in a recent large study of more than 9.500 cancer survivors, where social support buffered the negative effect of financial hardships experienced during the COVID19 pandemic on health-related quality of life and psychological distress (Noriega Esquives et al., 2024). Social support can also help moderate illness perceptions and the subjective impact of cancer. For instance, one study found that the perceived negative consequences of cancer predicted anxiety and depression over time but social support buffered this effect (Salafia et al., 2025). Similarly, the availability of social support can encourage the use of adaptive coping strategies, which can relieve psychological distress in the face of SES-related challenges. Supporting this idea, in a study of breast cancer patients, the protective effect of social support on depression symptoms was partially mediated by active coping, positive reframing, and acceptance (Zamanian et al., 2021). Emotional support, whereby individuals feel free and welcome to disclose stress-related thoughts, feelings, or concerns (called low “social constraint”), has also been found to be strongly related to general and cancer-specific distress and well-being (Rivera Rivera & Burris, 2020). Social support could also facilitate changes or maintenance of beneficial health practices (e.g., physical activity, sleep quality, healthy diet, refraining from smoking or drinking alcohol….) and medication adherence, which can have a positive influence on the mental health of cancer survivors (Uchino et al., 2025). In addition, social support can directly facilitate different biological mechanisms mediated through cardiovascular, endocrine, and immune parameters, that can help manage SES-related stress and adversity (Uchino et al., 2025). Two prominent biological mechanisms include a dampened hypothalamic pituitary-adrenocortical (HPA) axis stress response to challenges or threats (Hostinar et al., 2014) and reduced inflammation (Uchino et al., 2018) with the availability of social support. A crucial next step would be to seek better comprehension of the reasons behind the observed socio-economic inequalities and of the types of social support that can be effective for different socio-demographic groups. Our aim was to investigate the role of social support more generally. However, it would be of high theoretical and practical relevance to understand the role of different types of social support in buffering socio-economic inequalities. To illustrate, prior literature indicates that instrumental support can be particularly useful for facilitating health-protective behaviors (DiMatteo, 2004), whereas emotional support could help reduce psychological distress (Thoits, 2011; Uchino, 2006). However, the social support instruments used in the current research provide a global index of perceived support and do not differentiate between emotional, instrumental, and informational components as described in theoretical models (Wills & Ainette, 2012). This limits our ability to explore variation by support type, even though prior research indicates that different types of social support can have different effects on the mental health and well-being of cancer patients (Alfonsdóttir et al., 2025; Escalera et al., 2019; Ruiz-Rodríguez et al., 2021). For instance, in a recent study with cancer patients in Spain, emotional and information support were strongly related to patients’ quality of life and perceived stress, whereas instrumental support and support from health professionals were not (Ruiz-Rodríguez et al., 2021). Future studies could benefit from using multidimensional instruments that assess specific support functions to clarify these differential effects. Notable strengths of the research included the use of cancer survivor samples drawn from nationally representative population surveys and the opportunity to replicate the findings across different mental health measures and samples. Limitations include the lack of detailed information regarding the type of cancer, treatment status, and the exact time since diagnosis for participants diagnosed more than one year prior to the survey. This prevented us from examining how the buffering effect of social support varies across different cancer types or stages of survivorship. Previous research has shown that quality of life and mental health among cancer survivors depends on both cancer type and time since cancer diagnosis (Gao et al., 2023; Harrington et al., 2010; Petrova, Catena, et al., 2021; Wang et al., 2016). For instance, the prevalence of depression is generally higher during the first year after diagnosis and among survivors of gynecological, digestive, and breast tumors (Krebber et al., 2014; Petrova, Catena, et al., 2021). There is less research in long-term survivors (i.e., more than 5 years after diagnosis), but studies indicate that physical and psychological symptoms can persist well beyond 10 years after diagnosis (Harrington et al., 2010; Petrova, Catena, et al., 2021), reinforcing the importance of research on survivors’ mental health regardless of time since diagnosis. We used the Spanish occupational social class index adopted by the Spanish Society of Epidemiology (Domingo-Salvany et al., 2013) as a measure of SES due to its known effects on health outcomes (Blasco-Palau et al., 2023). Future studies should address the stress-buffering effect of social support using other socio-economic indicators such as education level, income, or employment status, that can have slightly different implications for mental health (Arias-de la Torre et al., 2019). The sample size limitations also prevented us from analyzing the socio-economic gradient in more detail (divided into smaller SES groups). The sample was also predominantly female. This imbalance reflects the underlying structure of the cancer survivor population (i.e., a larger number of female survivors in the Spanish population; Cancer Epidemiology Information System in Spain, 2025) and has been addressed by conducting gender-stratified analyses. Despite these limitations, the current study adds to emerging evidence showing socio-economic disparities in mental health among Spanish cancer survivors (Portero de la Cruz & Cebrino, 2022) and underscores the potential of social support as a modifiable protective factor in mitigating these disparities. There was heterogeneity in the results, which is to be expected with instruments measuring different aspects of mental health. To illustrate, the results for the more general measures of psychological distress and mental well-being were more similar compared to the results of the PHQ-8 questionnaire, which is designed to specifically screen for depression. Despite excellent statistical power, the interaction effects in the traditional moderation analyses were non-significant. However, the observed buffering effects were highly consistent across outcomes, and were further confirmed using GAMs. In our opinion, the current results offer convincing cross-sectional evidence to further explore the buffering effects of social support longitudinally and in interventions. The current results suggest that interventions providing social support may be successful at reducing socio-economic inequalities in mental health among cancer survivors. From a theoretical perspective (Engel, 1977; Pearlin et al., 1981; S. E. Taylor & Seeman, 1999; Uchino et al., 2025; Wills & Ainette, 2012), our findings reinforce stress-buffering models by showing that high levels of support could meaningfully attenuate SES-related disparities, offering a clearer understanding of when and for whom support is most protective. Our gender-stratified findings also allude to Belle’s (1982) support-gap model, which suggests that the stresses of low SES can constrain women’s social networks, weakening marital support, limiting community resources, and turning social ties into additional sources of strain, thereby reducing the extent to which social support can buffer socioeconomic disadvantage. Practically, they highlight social support as a modifiable resource that can be strengthened at the interpersonal, clinical, community, and policy level. The majority of previous interventions specifically targeting socio-economic disparities in cancer have mostly focused on addressing disparities in other aspects such as improving access to screening, treatment, and follow-up care (Ruiz-Pérez et al., 2019; Safari et al., 2025), with far less attention paid to the psychosocial consequences of cancer across socio-economic groups. Psychosocial interventions that include social support from peers (i.e., individuals with the same disease) have shown to be successful at improving quality of life and psychological outcomes in cancer survivors (Aizpurua-Perez et al., 2024; S. Zhang et al., 2022). However, it is not clear to what extent these or similar psychosocial interventions containing social support components are effective at reducing the negative effects associated with low SES (Kalter et al., 2018). For instance, an 8-week multi-component support group intervention for women with breast cancer was found to be more effective for participants with lower income, suggesting that social support components may be particularly impactful for disadvantaged populations (K. L. Taylor et al., 2003). Social support is usually integrated as part of broader multi-component interventions, in combination with other approaches such as cognitive-behavioral therapy, psychotherapy, or mindfulness-based meditation, making it challenging to sort out its unique effects (Kalter et al., 2018). Future research should aim to disentangle these effects and evaluate whether tailored, support-focused interventions can effectively reduce mental health disparities rooted in socio-economic disadvantage. In summary, we documented pervasive socio-economic inequalities in mental health among cancer survivors in Spain. Individuals with lower SES generally had worse mental health outcomes than survivors with high SES. Notably, these socio-economic disadvantages were concentrated under medium levels of social support and were successfully buffered by high levels of social support, more effectively so among men than among women. In contrast, participants with low social support exhibited the highest levels of psychological vulnerability, regardless of SES, suggesting that the absence of supportive resources may override the protective effects typically conferred by socioeconomic advantage. Together, these findings underscore the importance of strengthening social support systems as a feasible and scalable strategy that could be integrated into survivorship care pathways and psychosocial services to improve equity in cancer survivorship. Conflict of Interest The authors of this article declare no conflict of interest. Cite this article as: Petrova, D., Redondo-Sánchez, D., Madrid Pérez-Esparza, B., Fernández-Navarro, P., Blakoe, M., Luque Caro, R., & Sánchez, M. J. (2026). The stress-buffering effect of social support on socio-economic disparities in mental health among cancer survivors. Psychosocial Intervention, 35, Article e260817. https://doi.org/10.5093/pi2026a9 Funding: Cancer Epidemiological Surveillance Subprogram of the CIBER of Epidemiology and Public Health and the Health Institute Carlos III (VICA). DP is supported by a Miguel Servet Fellowship (CP23/00024) from the Health Institute Carlos III. The data and code for the analyses are available on the website of the Ministry of Health (https://www.sanidad.gob.es/estadEstudios/estadisticas/bancoDatos.htm) and the Open Science Framework (OSF), respectively: https://doi.org/10.17605/OSF.IO/69BRM Supplementary materials are available at https://doi.org/10.5093/pi2026a9 |
Cite this article as: Petrova, D., Redondo-Sánchez, D., Madrid Pérez-Esparza, B., Fernández-Navarro, P., Blakoe, M., Luque Caro, R., & Sánchez, M. (2026). The Stress-Buffering Effect of Social Support on Socio-Economic Disparities in Mental Health among Cancer Survivors. Psychosocial Intervention, 35, Article e260817. https://doi.org/10.5093/pi2026a9
Correspondence: Daniel.Redondo.easp@juntadeandalucia.es (D. Redondo-Sánchez).
Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB Supplementary files
Supplementary files CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
Psychosocial Intervention is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License







