


Restless Legs Syndrome and Mental Health Problems in Peripartum Women: A Prospective Study
[El sĂndrome de las piernas inquietas y los problemas de salud mental en las mujeres en el periparto: un estudio prospectivo]
Muhamed Lepuzanović1, Vildana Aziraj Smajić2, Sandra Nakić Radoš3, Osman Sinanović1, 4, 5, & 6
1University Sarajevo, School of Science and Technology, Sarajevo, Bosnia & Herzegovina; 2Cantonal Hospital Dr “Irfan Ljubijanki” of Biha, Biha, Bosnia & Herzegovina; 3Catholic University of Croatia, Zagreb, Croatia; 4University of Tuzla, Bosnia & Herzegovina; 5International Academy of Science and Arts of Bosnia & Herzegovina; 6Academy of Medical Sciences of Bosnia and Herzegovina, Sarajevo, Bosnia & Herzegovina
https://doi.org/10.5093/clh2026a3
Received 10 July 2024, Accepted 23 June 2025
Abstract
Background: Restless leg syndrome (RLS) affects about 25% of pregnant women and is associated with peripartum depression. However, other mental health problems were not investigated. The study aimed to examine differences between women with and without RLS in depression, anxiety, and stress over the peripartum period. Method: Pregnant women with and without RLS were followed from pregnancy (T1) to two months postpartum (T2) (N = 259). They completed the Depression, Anxiety, and Stress Scale-21 on each occasion and the Restless Legs Syndrome Scale. Results: Women with RLS (26.6%) diagnosed in pregnancy had significantly higher levels of depression, anxiety, and stress compared with women without RLS during pregnancy and two months postpartum. Conclusions: Women with RLS had significantly impaired mental health, not just during pregnancy but up to two months postpartum. Women with RLS should be given special attention, and the possible shared mechanisms underlying RLS and mental health should be investigated further.
Resumen
Antecedentes: El síndrome de piernas inquietas (SPI) afecta a un 25% aproximadamente de las mujeres gestantes y se asocia con la depresión perinatal. No se investigaron otros problemas de salud. El estudio se ha centrado en las diferencias en depresión, ansiedad y estrés en el periodo perinatal entre mujeres que padecían el síndrome y las que no. Método: Se hizo un seguimiento de las mujeres gestantes con el síndrome y sin el desde el embarazo (T1) hasta dos meses posparto (T2)(N = 259), las cuales cumplimentaron la Escala-21 de Depresión, Ansiedad y Estrés en ambas ocasiones, así como la Escala del Síndrome de Piernas Inquietas. Resultados: Las mujeres a quienes se había diagnosticado SPI (26.6%) en el embarazo tenían un mayor nivel significativo de depresión, ansiedad y estrés que las mujeres a las que en el embarazo y dos meses posparto no se había hecho tal diagnóstico. Conclusiones: Las mujeres con diagnóstico de SPI tenían problemas de salud mental, no solo durante el embarazo sino también dos meses después del parto. Debería prestarse una atención especial a las mujeres diagnosticadas de SPI y profundizar en la investigación de los posibles mecanismos compartidos que subyacen al SPI y a la salud mental.
Palabras clave
SĂndrome de piernas inquietas, Embarazo, Posparto, DepresiĂłn, Ansiedad, EstrĂ©sKeywords
Restless leg syndrome, Pregnancy, Postpartum, Depression, Anxiety, StressCite this article as: Lepuzanović, M., Aziraj Smajić, V., Nakić Radoš, S., & Sinanović, O. (2026). Restless Legs Syndrome and Mental Health Problems in Peripartum Women: A Prospective Study. Clinical and Health, 37, Article e260718. https://doi.org/10.5093/clh2026a3
Correspondence: muhamed.lepuzanovic@gmail.com (M. Lepuzanović).Restless legs syndrome (RLS) is a disease from the spectrum of movement disorders. In the description of the disease, patients most often state a feeling of growing restlessness in the lower extremities, accompanied by a feeling of pain, itching, and unpleasant sensations through them. It is characterised by an urgent need to move the legs. Symptoms appear in the evening and at rest and decrease or stop after moving the extremities (Allen et al., 2014; Holzknecht et al., 2020). As RLS occurs dominantly in the evening and night hours, it often makes it difficult for people with RLS to fall asleep, disrupting the quality and length of sleep (Chen et al., 2018), and also disrupting periods of rest, thus leading to functional disturbances in mood, cognition, daily energy, and disrupting other daily activities (Trenkwalder et al., 2018). Women suffer from RLS twice as often as men, and the overall frequency in the standard population is 1-10% (Japaridze et al., 2018; Seeman, 2020). The frequency of this syndrome increases in pregnant women, and a recent meta-analysis found a 23% prevalence rate in the third trimester of pregnancy, with a large discrepancy between countries, from 4% in Japan to 63% in Turkey (Darvishi et al., 2020). The sleep quality of pregnant women is the lowest in the third trimester of pregnancy when the prevalence of RLS is also at its highest level (Gossard et al., 2021; Nanayakkara et al., 2023). Pathophysiological mechanisms implicated in the RLS include dopaminergic and glutamatergic dysregulation, iron deficiency in brain regions, and hormonal fluctuations that influence neurotransmission and contribute to women’s increased vulnerability to RLS and other comorbid disorders, such as depression and anxiety (Seeman, 2020). Furthermore, a direct association of RLS symptoms with depression and anxiety was shown in a meta-analysis, which included 23 studies from the general population (An et al., 2024). Research has also shown that the association between RLS symptoms and depressive symptoms such as daytime fatigue, sleep disturbance, reduced concentration, and psychomotor agitation is overlapping and bidirectionally related (Becker & Novak, 2014). On the other hand, studies on the association between RLS and mental health in the peripartum are scarce. A systematic review found two Swedish studies showing the association of gestational RLS with depression both during pregnancy and postpartum (Steinweg et al., 2020). However, this should be examined further because of the scarcity of such studies in other countries. Also, what has been limited in previous research is the extent to which the RLS affects the appearance of symptoms of anxiety and stress both during pregnancy and postpartum. RLS, as a relatively common movement disorder with a prevalence which increases so much in the peripartum period that one in four suffers from it (Darvishi et al., 2020), is largely neglected by obstetricians, and can be suitable for screening for the expected development of mental disorders in pregnant and postpartum women. The goal of this study was to examine differences in mental health problems over the peripartum period between women with and without RLS. We hypothesised that women with RLS will have more depression symptoms both during pregnancy and after childbirth compared with women without RLS. However, regarding anxiety and stress, we did not have a firm hypothesis given the lack of studies on the association between RLS and anxiety and stress during peripartum, and especially not longitudinal studies. Participants and Procedure This correlational study with prospective design followed pregnant women from pregnancy to two months postpartum. Pregnant women could participate in the study if they were older than 18, without exclusion criteria. Ethical permission for the study was obtained from the Ethics Committee of the “Dr. Irfan Ljubijankić” Cantonal Hospital. All participants were informed about the study and signed the informed consent before entering the study. Women were recruited from the maternity ward of the “Dr. Irfan Ljubijankić” Cantonal Hospital (Bihać, Bosnia and Herzegovina) between the 35th and 40th week of pregnancy (T1) when they came for a regular check-up before the planned birth. The above was conducted by a medical doctor (neurologist and gynaecologist) and a psychologist from November 2020 to May 2021. In T1, 277 participants were included in the study, and 259 were followed up to two months after birth, specifically between 8 and 9 weeks postpartum (T2), with a drop-out rate of 6.5%. In T1, participants completed the scales with paper and pencil while a physician examined the RLS (while providing information to the patients about RLS symptoms and diagnosis); at T2, participants were contacted by phone by the same healthcare professional. Instruments The Depression, Anxiety, and Stress Scale (DASS-21; Lovibond & Lovibond, 1995) The DASS-21 is a self-report measure of depression, anxiety, and stress symptoms over the last week. The scale has 42 items, but in this study the short version with 21 items was used with seven items per subscale. Each item is rated on a four-point scale from 0 to 3, and the total sum for each subscale is multiplied by two to be comparable with the full scale. The scale has been previously translated into Croatian (Reić Ercegovac & Penezić, 2012). In the current study, the internal consistency of Cronbach α for Depression, Anxiety, and Stress subscale was .64, .78, and .85 during pregnancy, and .73, .75, and .74 at two months postpartum, respectively. Scale to Diagnose the Restless Legs Syndrome (International Restless Legs Syndrome Study Group - IRLSSG; Allen et al., 2014) The scale was developed and updated and consists of five items, and the diagnosis of restless legs syndrome is made in patients who answered positively to the first four items related to the symptoms of RLS and gave a negative answer to the 5th question, which is an exclusion criterion due to other conditions or diseases. The women filled out the survey orally in such a way that the examiner explained each question in detail. The Demographic Sheet This sheet included questions on age, education level, marital status, employment status, and parity. Health-related questions were about chronic disease and medication use. Statistical Analysis Differences between women with and without RLS in socio-demographic and health variables were examined with χ2 test, while differences in depression, anxiety, and stress scores over the peripartum period were examined with mixed-design ANOVA. Additional differences were inspected by t-test. G*Power software indicated that to detect two-tailed differences, with medium size effects of .50, a significance level of 5%, a power of 80%, and a .20 ratio of the RLS sample, it was necessary to have at least 38 RLS and 190 no-RLS participants (228 in total), which was exceeded. All analyses were set to p-value p < .05 and were done in SPSS Statistics 28.0 for Windows. Pregnant women (N = 259) were, on average, 28.79 years old (SD = 5.70, range = 18-45). Most participants graduated from high school (57.9%), were married (96.9%), and were unemployed (67.2%). Regarding parity, 44.8% were primiparous, and 55.2% were multiparous. Regarding health variables, 17.4% had some chronic diseases (most common were anaemia, arterial hypertension, thyroid disease, and diabetes mellitus), and 17.8% used medication. The group of women with RLS and the control group did not differ on any of the sociodemographic or health variables (Table 1) and, therefore, were not controlled for in subsequent analyses. Table 1 Structure of the Participants with and without Restless Leg Syndrome (RLS) according to Demographic and Health Characteristics (N = 259) 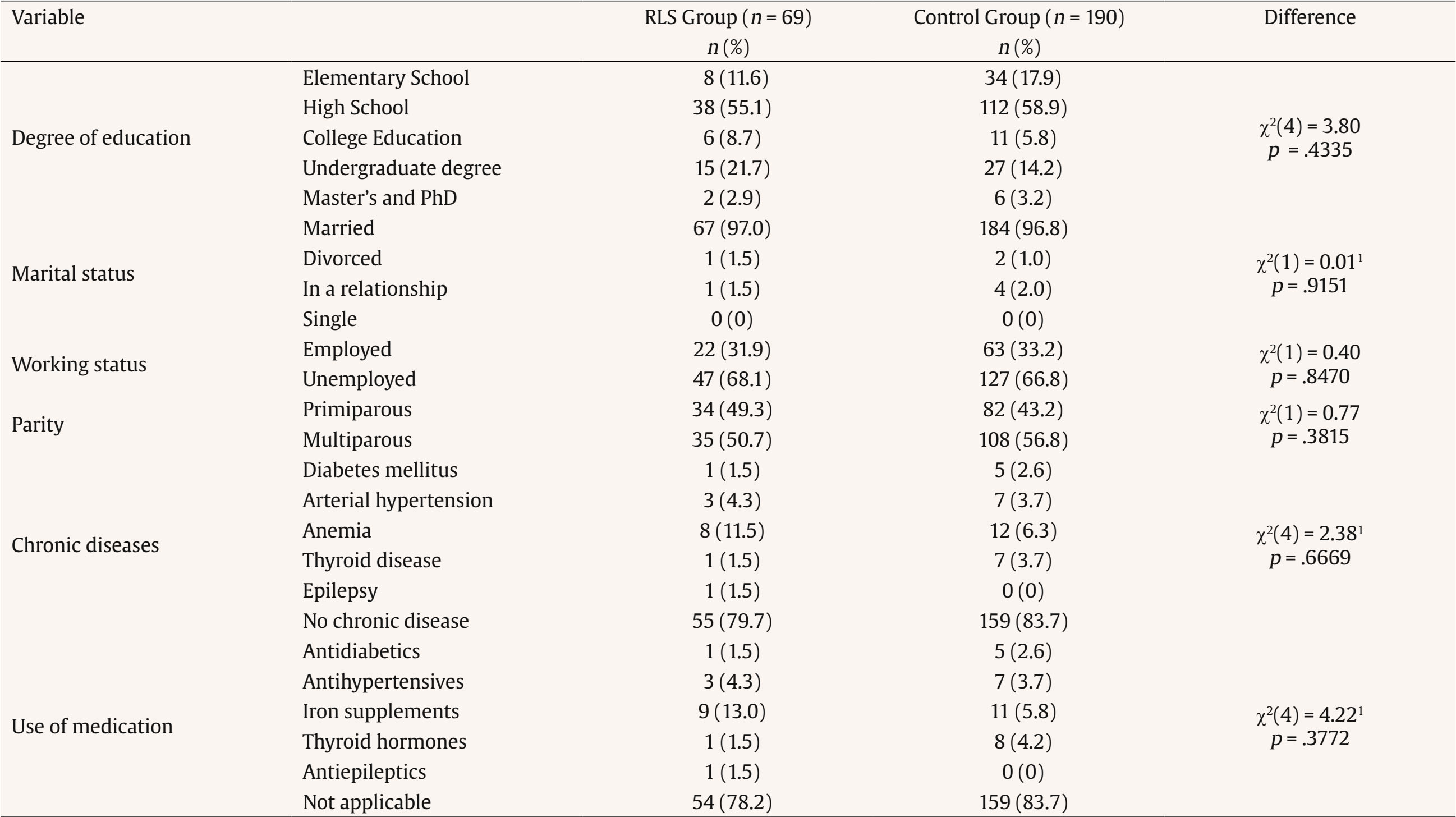 Note. 1Cells with 0 frequency were merged. RLS was present in 69 women (26.6%) in the 3rd trimester of pregnancy and 47 women (18.2%) two months postpartum, which was a significant decrease over time, χ2(1) = 4.90, p = .0269. Mixed-design ANOVAs showed that there was a significant effect of group (RLS vs. no-RLS) for depression, F(1, 257) = 27.43, p < .001, anxiety, F(1, 257) = 48.23, p < .001, and stress, F(1, 257) = 61.73, p < .001. For all comparisons, pregnant women who were diagnosed with RLS (n = 69) had higher levels of mental health problems both during pregnancy and two months postpartum (Figure 1). Figure 1 Depression, Anxiety, and Stress Scores over Peripartum Period in Women with (n = 69) and without (n = 190) Restless Leg Syndrome Diagnosed during Pregnancy. 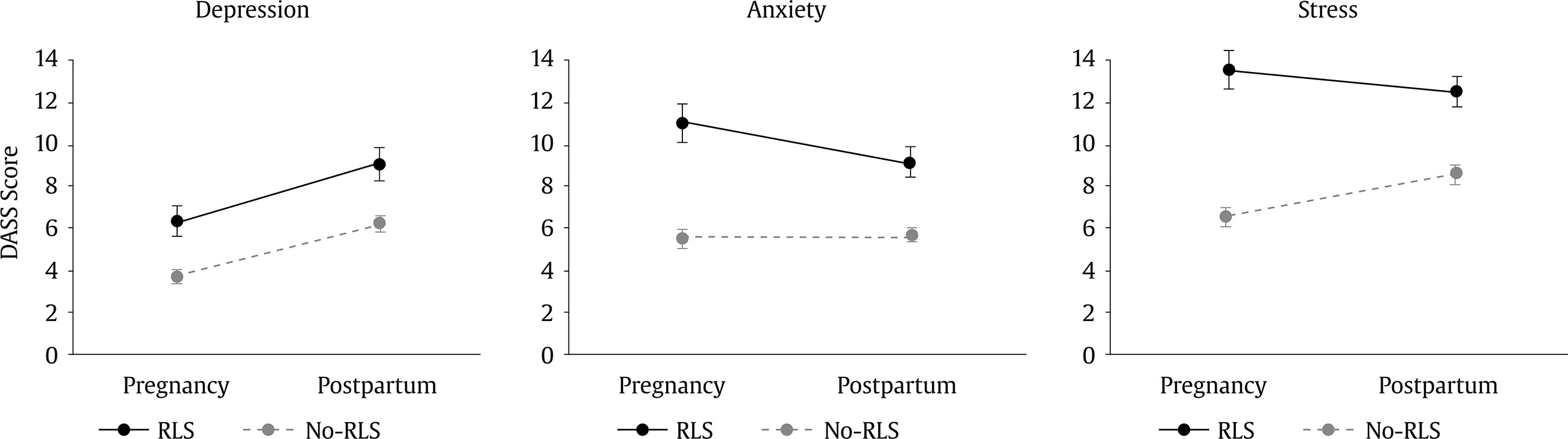 Note. Means and standard error of the means presented. Given that some women who had RLS during pregnancy did not have RLS after childbirth anymore, additional differences were analysed between women who still had RLS and those without RLS at two months postpartum. Women diagnosed with RLS at two months postpartum (n = 47) had significantly higher levels of depression, t(53.93) = 2.56, p = .013, anxiety, t(55.75) = 3.87, p < .001, and stress, t(257) = 5.02, p < .001, than women without RLS. Given that the association between RLS and different aspects of mental health over the peripartum period were under-investigated, this study aimed to examine whether women with RLS would have more depression, anxiety, and stress symptoms in pregnancy and two months postpartum, compared to the control group of women. The results indicated that women diagnosed with RLS during pregnancy reported higher levels of depression, anxiety, and stress both during pregnancy and two months postpartum. Also, our findings indicate that 26% of pregnant women is affected by the RLS in the third trimester of pregnancy, which is aligned with systematic review showing the 23% prevalence rate (Darvishi et al., 2020). In line with previous systematic reviews in general (An et al., 2024) and the peripartum population (Steinweg et al., 2020), our findings also showed that people with RLS have higher levels of depression symptoms. Although the review in the general population (An et al., 2024) was quite extensive, the review in peripartum samples (Steinweg et al., 2020) included only two studies, both coming from Sweden. Therefore, our findings are important to substantiate the literature in this respect. A bidirectional association between the RLS and depressive symptoms has been implicated (Becker & Novak, 2014), given that both include sleep disturbance, daytime fatigue, and psychomotor agitation. The low levels of iron and high levels of estrogen may be involved in dopaminergic and glutamatergic dysregulation, which explain women’s susceptibility to the RLS and comorbid mental disorders (Seeman, 2020). Regarding the association between RLS and anxiety, a systematic review of general samples (An et al., 2024) pointed out that people with RLS have higher levels of anxiety. However, systematic review in peripartum samples was not focused on other aspects of mental health apart from depression. Therefore, our findings that women with RLS have more adverse mental health, not just concerning depression but anxiety and stress, as well, are important contributions to the literature. This highlights the adverse effects of the RLS on sleep length and quality (Chen et al., 2018) and daily functioning (Trenkwalder et al., 2018), but also extends to adverse effects on different aspects of mental health in the peripartum period. Several limitations should be addressed. Mental health problems were examined by self-report measures, so future studies would benefit by administering the diagnostic interview. Follow-up after childbirth was only until two months postpartum, so it would be useful for future studies to include wider postpartum follow-up. To conclude, women with RLS, compared to the control group, had significantly impaired mental health concerning depression, anxiety, and stress, both during pregnancy and up to two months postpartum. Given the large prevalence, adverse effects on mental health, and the regular prenatal check-ups during pregnancy with plenty of opportunities to see pregnant women by health professionals, they should be screened and treated for RLS. Future studies should look more in depth into the possible shared mechanism underlying RLS and mental health, especially in the peripartum period. Conflict of Interest The authors of this article declare no conflict of interest. Cite this article as: Lepuzanović, M., Aziraj Smajić, V., Nakić Radoš, S., & Sinanović, O. (2025). Restless legs syndrome and mental health problems in peripartum women: A prospective study. Clinical and Health, 37, Article e260718. https://doi.org/10.5093/clh2026a3 References |
Cite this article as: Lepuzanović, M., Aziraj Smajić, V., Nakić Radoš, S., & Sinanović, O. (2026). Restless Legs Syndrome and Mental Health Problems in Peripartum Women: A Prospective Study. Clinical and Health, 37, Article e260718. https://doi.org/10.5093/clh2026a3
Correspondence: muhamed.lepuzanovic@gmail.com (M. Lepuzanović).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
Clinical and Health is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License








