


Predictors of Therapeutic Alliance: Patient Attachment and the Personal Style of the Therapist
[Los predictores de la alianza terapéutica: el apego del paciente y el estilo personal del terapeuta]
Nerea B. Bárez1, Luis A. Saúl2, & Sergi Corbella3
1Instituto Español de Psicoterapia Integradora (IEPI), Madrid, Spain; 2Universidad Nacional de Educación a Distancia (UNED), Madrid, Spain; 3Universidad Ramón Llull (URL), Madrid, Spain
https://doi.org/10.5093/clh2026a5
Received 3 March 2025, Accepted 3 September 2025
Abstract
Background: The therapeutic alliance is crucial for psychotherapy effectiveness. Research has examined patient attachment and therapist personal style, but their impact on different treatment phases and alliance subcomponents remains unclear. This study analyzes their predictive role in the alliance, distinguishing between initial and advanced stages. Method: 264 participants and 28 therapists from four private Madrid-based centers participated. Patient symptomatology, attachment, and therapeutic alliance were measured, along with therapist personal style. Two groups were formed: initial stage (≤5 sessions) and advanced stage (≥ 6 sessions). Results: Attachment avoidance and overall functioning predicted alliance in the initial phase, while therapist attentiveness was more relevant in the advanced phase. Expressive function influenced the therapeutic bond, and therapist age had a moderating effect. Conclusions: The therapeutic alliance varies by treatment stage. Patient attachment avoidance is a constant predictor, while therapist style modulates its impact. Tailoring interventions to patient profiles and treatment phases enhances alliance and clinical outcomes.
Resumen
Antecedentes: La alianza terapéutica es crucial para la eficacia de la psicoterapia. La investigación ha examinado el apego del paciente y el estilo personal del terapeuta, pero su influencia en las diferentes fases del tratamiento y los subcomponentes de la alianza sigue siendo incierta. El estudio analiza su papel predictivo en la alianza, distinguiendo entre las etapas iniciales y avanzadas. Método: La muestra está compuesta por 264 participantes y 28 terapeutas de cuatro centros privados madrileños. Se midió la sintomatología, el apego y la alianza terapéutica del paciente, así como el estilo personal del terapeuta. Se formaron dos grupos: etapa inicial (≤ 5 sesiones) y etapa avanzada (≥ 6 sesiones). Resultados: La evitación del apego y el funcionamiento general predijeron la alianza en la fase inicial, mientras que la atención del terapeuta fue más importante en la fase avanzada. La función expresiva influyó en el vínculo terapéutico y la edad del terapeuta tuvo un efecto moderador. Conclusiones: La alianza terapéutica varía según la etapa del tratamiento. La evitación del apego del paciente es un predictor constante, mientras que el estilo del terapeuta modula su impacto. Adaptar las intervenciones a los perfiles de los pacientes y las fases del tratamiento mejora la alianza y los resultados clínicos.
Palabras clave
Alianza terapéutica, Apego, Evitación, Estilo personal del terapeuta, Predictores, Proceso terapéutico
Keywords
Therapeutic alliance, Attachment, Avoidance, Personal style of the therapist, Predictors, Therapeutic process
Cite this article as: Bárez, N. B., Saúl, L. A., & Corbella, S. (2026). Predictors of Therapeutic Alliance: Patient Attachment and the Personal Style of the Therapist. Clinical and Health, 37, Article e260719. https://doi.org/10.5093/clh2026a5
Correspondence: nereabarez@nbpsicologia.es (N. B. Bárez).
The therapeutic alliance is one of the most influential factors in the effectiveness of psychotherapy, regardless of the theoretical model used (Flückiger et al., 2021). It has traditionally been defined as having three components: the emotional bond between patient and therapist, an agreement on goals, and a consensus with regard to tasks (Bordin, 1979). For operational assessment purposes, a number of subcomponents have been identified, including bonding, targets, tasks, and the client’s theory of change. These have been validated in a range of clinical contexts and are considered to be essential to therapeutic practice (Duncan et al., 2003; Gelso & Kanninen, 2017; Hunik et al., 2021; van Benthem et al., 2024). However, the lack of a unified definition has led to diverse conceptual and methodological approaches to studying the alliance (Krause et al., 2011). A wide range of variables have been studied as alliance predictors, including sociodemographic, clinical, and relational characteristics. A patient’s symptomatology has been identified as a key factor, as high levels of unease can impair the building of a solid alliance (Evans et al., 2022). Patients with a greater interpersonal adjustment and better emotional regulation tend to develop a stronger alliance (Chu et al., 2014; Lawson et al., 2020). One of the aspects that has attracted most research with regard to the therapeutic alliance is the impact of a patient’s attachment style. Attachment styles, initially conceptualized in Bowlby’s (1969, 1982) attachment theory, describe the way in which people establish and maintain interpersonal relations throughout their lives. It has been found that patients with secure attachments develop a more solid therapeutic alliance, while patients that employ avoidance or anxiety strategies can experience difficulties in generating confidence in their therapeutic relations (Bernecker et al., 2014; Mikulincer & Shaver, 2007; Zilcha-Mano & Fisher, 2022). Attachment avoidance has been particularly linked to a difficulty in establishing an emotional connection with the therapist, which may negatively affect the therapeutic process (Diener & Monroe, 2023; Dozier, 1990; Mallinckrodt & Jeong, 2015). Research highlights the importance of the patient’s attachment tendency and adjusting elements such as the therapist’s emotional distancing (Egozi et al., 2023). As well as the factors related to the patient, the therapist’s characteristics also play a crucial role in the building of the alliance (Flückiger et al., 2022; Folmo et al., 2021). The capacity of the therapist to express empathy and create a warm relationship has been identified as a key factor in the establishing of an emotional bond of the therapeutical alliance. This emotional connection, which reinforces a patient’s sense of security and confidence, has been widely studied as a crucial element in therapeutic success (Bar-El & Gil, 2022; Rossetti & Botella, 2017; Slade, 2008). The personal style of the therapist (PST) specifically refers to the personal and professional characteristics that the therapist brings to the therapeutic relationship, including their capacity to express empathy, their warmth, and their ability to connect emotionally with the patient (Corbella, 2020; Corbella et al., 2024; Fernández-Álvarez et al., 2003; Fernández-Álvarez et al., 1998). The expressive function of the therapist’s personal style indicates the preference for the use of emotions in therapy, as well as the level of proximity of the therapist to the patient (Corbella, 2020), while the role of attention offers information regarding openness and receptivity versus the therapist’s focused and concrete willingness with respect to the patient’s information. Research has shown that therapists with the most flexible personal and empathetic style tend to develop the strongest alliances with their patients, resulting in the best therapeutic results (Gelso & Kanninen, 2017; Wampold & Imel, 2021). It has been proven that variations in the personal style of the therapist could be related to changes in the alliance, highlighting the need for an adjustment between the therapist and the patient (Botella et al., 2008; Botella & Corbella, 2005; Malik et al., 2002). Recent research suggests that the interaction between the therapist’s personal style and the form of the patient’s attachment may be more complex than previously proposed, underlining the importance of adapting the therapeutic approach to the patient’s profile (Gillath et al., 2016; Talia et al., 2020). With regard to the temporal development of the therapeutic alliance, it has been seen that this is not a static variable, but rather one that evolves throughout the therapeutic process (Horvath et al., 2011). Research suggests that the first five sessions are particularly important in establishing a solid alliance, as this is an initial period in which the patient and the therapist work out an emotional bond and agree on the treatment goals and tasks (Coutinho et al., 2014). While the alliance tends to establish itself after this point, the first sessions represent a key period in which ruptures in the alliance might occur, but also where the necessary remedies can strengthen the relationship (Ardito & Rabellino, 2011; Eubanks et al., 2018; Safran & Muran, 2005). Recent literature supports the idea that a successful handling of ruptures in the alliance, often related to a confrontation of the patient’s dysfunctional patterns, is essential to long-term therapeutic progress (Høgenhaug et al., 2023; Muran & Eubanks, 2023). In such a context, the main aim of this study is to investigate the influence of variables such as the patient’s attachment style and the therapist’s personal style in the quality of the therapeutic alliance within a naturalistic clinical setting. It suggests that patients with attachment avoiding strategies will have greater difficulties in establishing a solid alliance, especially with respect to the emotional bond with the therapist (Mallinckrodt & Jeong, 2015). The study also proposes an assessment of the various aspects of the personal style of the therapist, such as how the expressive or attentional functions may be determining variables in the building of an alliance (Fernández-Álvarez et al., 1998; Corbella, 2020). This study also examines sociodemographic variables such as sex, age, the reason for seeking therapy, subjective discomfort, and the number of preceding sessions in order to determine their possible impact on the therapeutic alliance. Although these variables have shown inconsistent results in previous research (Barkham et al., 2021; Horvath et al., 2011), their inclusion offers a more complete analysis of the factors that have a bearing on the therapist-patient relationship. Finally, the study assesses the progress of the alliance before and after the fifth session, based on previous research which highlighted that this is the important turning point for the stability of the alliance and the long-term success of the treatment (Coutinho et al., 2014; Safran & Muran, 2005). Sample The study featured a total of 264 participants who underwent therapy at a private center in the Madrid region (average age = 32.4, DE = 11.5, range = 16-67 years of age), of which 67.8% were women. As far as the employment situation was concerned, 52.3% of those taking part were in full-time employment, 9.5% worked part-time and 28% were students. The most common reasons for seeking therapy were relationship problems (34.8%) and anxiety and stress (28%). The time that they had been affected by the problem that led them to seek therapy was very diverse; there was the same number of cases (28.4%) that had spent less than six months in therapy as those who attended regularly. Slightly over half of the group had been in therapy previously. Among those that had, it was more common that they had had more than a year since their last session. The vast majority were not taking medication (nearly 81%). Of the few that were, the most habitual were anxiolytics (6.4%), antidepressants (4.2%), or a combination of the two (6.4%). The sample was split into two groups: those who were in the initial phase of the alliance (having attended five therapy sessions or less) and those in the advanced phase of therapy (six or more sessions), the characteristics of which can be seen in Table 1. For participants in the initial phase (n = 157, average age = 31.7, SD = 11.1, range from 16 to 67, 66.2% women, 52.9% in full-time employment, 10.2% part-time, and 28% students) the most common reason for seeking therapy was relationship and interpersonal problems (35.7%), while the most time with this problem was under six months (30.6%). For participants in the advanced phase (n = 107, average age = 33.3, SD = 12, range from 18 to 60, 70.1% women, 51.4% in full-time employment, 8.4% part-time and 28% students) the most common reason for seeking therapy was also relationship and interpersonal problems (33.6%), while the most time with this problem was over one year (29%) and permanent or recurrent (29.0%). Table 1 Characteristics of the Series Patient Sample (N = 264) 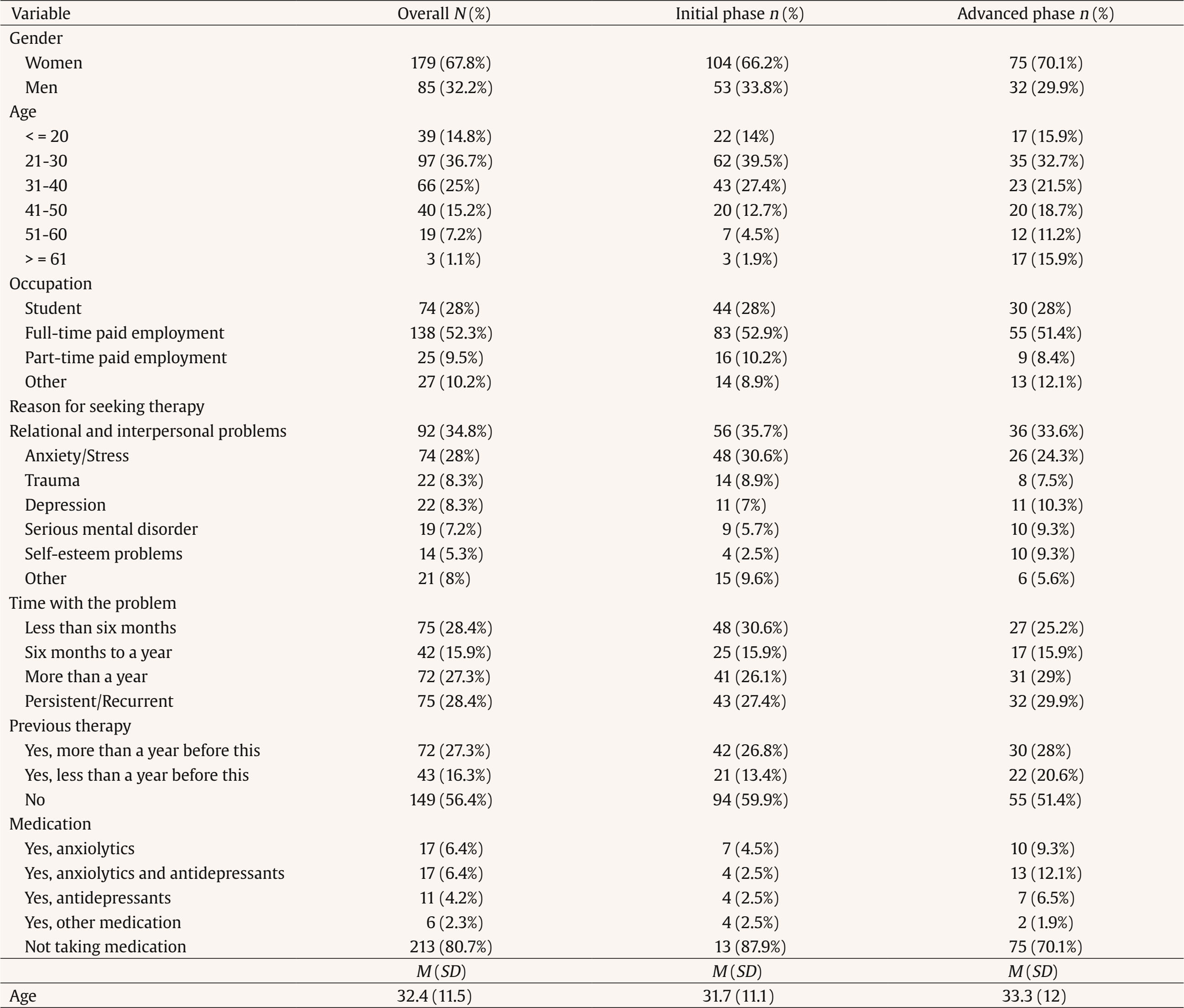 Note. M = mean, SD = standard deviation. The 264 patients were seen by 28 therapists who were working in the clinic during the research. The sample was mostly made up of women (n = 25, 89%) while the age of the therapists was between 24 and 46, with a median age of 29 and a mean age of 30.1 (CI 95% [29.6, 30.7], SD = 4.7). Their professional experience ranged from 1 to 26 years, with a median period of 4 years and a mean period of 5.3 years. All therapists reported an integrative theoretical orientation, mainly combining cognitive-behavioral, humanistic, and systemic approaches. The average number of sessions attended was 11.4 (DE = 17.4). The sample was also analyzed in terms of the treatment phase (Table 2). Table 2 Characteristics of the Series Therapist Sample. N = 28 / N = 264 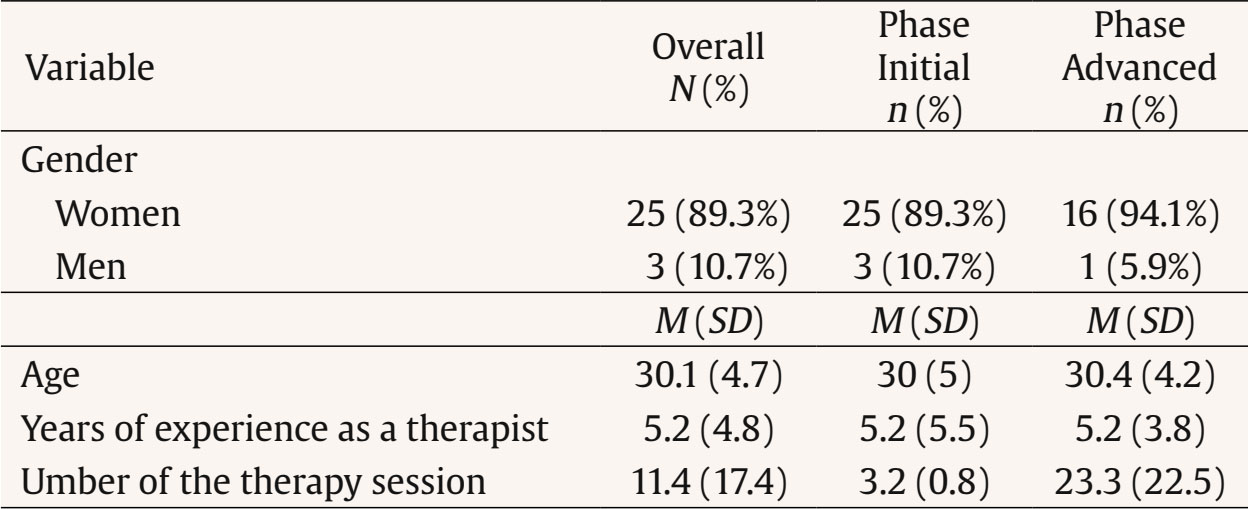 Note. M = mean, SD = standard deviation. Procedure Non-experimental quantitative research was undertaken through single group ex-post facto research. The procedure was approved by the ethics committee of the Universidad Nacional de Educación a Distancia [National University of Distance Learning] (UNED). The research was carried out over a two-year period in four private psychology centers in the Madrid region. All the participants were included, regardless of the phase of the therapeutic process or the number of sessions attended. Both therapists and patients participated voluntarily, having given their informed consent prior to the assessment. The questionnaires were filled out in person or online using Qualtrics (https://www.qualtrics.com) The therapeutic alliance, a variable depending on the study, was measured through WATOCI (Duncan & Miller, 1999), which offers an overall score with specific values for its subcomponents: goals, tasks, bonding, and theory of change (ToC). The independent variables included:
Instruments Assessment of Attachment: ECR Experiences in Close Relationships (ECR; Spanish version by Alonso Arbiol et al., 2007) was used with 36 items, in order to assess attachment in adults, with responses recorded on a 7-point Likert scale. It included a revised version (ECR-R) and an abridged version (ECR-S), although in this study the full version was used. ECR was used due to its psychometric properties and its relevance as an assessment of attachment instrument used with Spanish people (Bárez et al., 2024). It allows information to be extracted regarding the two attachment dimensions (Brennan et al., 1998): anxiety, related to the security of intimate relationships, and avoidance, which reflects an easiness with emotional intimacy. The ECR allowed variations to be identified in both dimensions, which were independent of each other. Satisfactory reliability indices were obtained – a Cronbach’s alpha above .83 – suggesting a solid internal consistency in the assessed dimensions. Assessment of Subjective Distress, Symptomatology, and Therapeutic Progress: CORE-OM Clinical Outcomes in Routine Assessment Outcome Measures (CORE-OM; Spanish version by Feixas et al., 2012) was used. It featured 34 items, producing a total score and four sub-domains: Subjective Wellbeing, Problems/Symptoms, General Functioning, and Risk. A high score indicated a more severe problem or symptom. This test was recorded as a total score, excluding risk items as they were more related to intervention than overall progress. The questionnaire provided psychometric indicators with a suitable initial reliability of between .75 and .90 and an index of .95 in the Spanish assessment (Trujillo et al., 2016). There was a good convergence, which correlated with other detection tests such as the SCL-90 (Derogatis, 1983) and the GHQ (Goldberg & Hilier, 1979). Assessment of the Therapeutic Alliance A Working Alliance Theory of Change Inventory (WATOCI; Duncan & Miller, 1999; Spanish version by Corbella & Botella, 2004) was carried out. This featured 17 items which were answered according to a 7-point Likert scale (from 1 = never to 7 = always). It was made up of four sub-domains: Goals, Tasks, Bond, and Theory of Change (ToC). This was the instrument that was chosen as it not only provided a total score of the overall alliance, but also an assessment of the Working Alliance Inventory (Hovarth & Greenberg, 1989), to which five items corresponding to the ToC domain were added due to their solid psychometric properties in both the original version and the one adapted for Spanish use. It also offered a measure of the reliability of the assessed instrument with a Cronbach’s alpha coefficient of .93 and equally high measurements (> .82) in each of the sub-domains. Assessment of Therapeutic Style An Assessment Questionnaire on the Personal Style of the Therapist PST-Q (Fernández-Álvarez et al., 1998) was used. This features 36 items which respond through a 7-point Likert scale. The questionnaire provided information on the dimensions of each therapist’s style: operational, instructional, expressive, attentional, and implicational. A version has also been constructed in Spanish (Argentinean and Spanish samples) and validated by various population groups, including a recent brief Spanish version of the PST (Prado-Abril et al., 2019). Analysis of Data and Planning Statistical analysis was undertaken using SPSS 28. First, exploratory and descriptive analyses were carried out on each of the variables, which were also segmented based on the study group. The internal consistency of each instrument and its sub-domains (Cronbach’s alpha) was then checked. Multivariate regression models with different variables to predict and predictor variables were then carried out. The regression models included variables that referred to both the patients and therapists, with the scores of the different measured instruments combined. Domain Results The WATOCI (perception of the therapeutic alliance) had a high internal consistency (α = .93, IC 95% [.92, .94]). Most responses were between 5 and 7, indicating a perception that was favorable to the alliance, with low variability in the responses. The Kolmogorov-Smirnov test showed a significant deviation from normal (p < .01), although the similarity between means and medians justified the use of parametric analysis. The ECR-QC (attachment questionnaire) showed a satisfactory level of reliability (α = .78). Average anxiety (M = 4.14) and avoidance (M = 2.83) scores were below the theoretical mean, reflecting a balance in distribution without marked biases. Both variables were adjusted to a normal distribution, allowing the use of parametric analysis. The CORE-OM (mental health) showed a very high level of reliability (α = .95), confirming its accuracy in the assessment of psychological health. Responses showed a variability among the items, with a wide range of perceptions concerning psychological wellbeing without dominant tendencies. Predictive Models Four main models were proposed: one for the total WATOCI score in the overall sample, a second for the initial phase (≤ 5 sessions), a third for the advanced phase (≥ 6 sessions), and a specific model for the bonding sub-domain in the overall sample. The selection of these models was based on the differences detected in the predictive relations, with the hypothesis that the treatment phase would influence the alliance and that there would be differences between the therapeutic bond and the other alliance components. Model 1. Total WATOCI Score of the Patient’s Significant Factors (CORE-OM and ECR-Attachment) and the Personal Style of the Therapist Factors A predictive model of the therapeutic alliance (total WATOCI score) in the overall sample was prepared, assessing the influence of patient and therapist variables. As can be seen in Table 3, the model was highly significant (p < .001) and explained 16.7% of the variance. Table 3 Predictive Multivariate Models 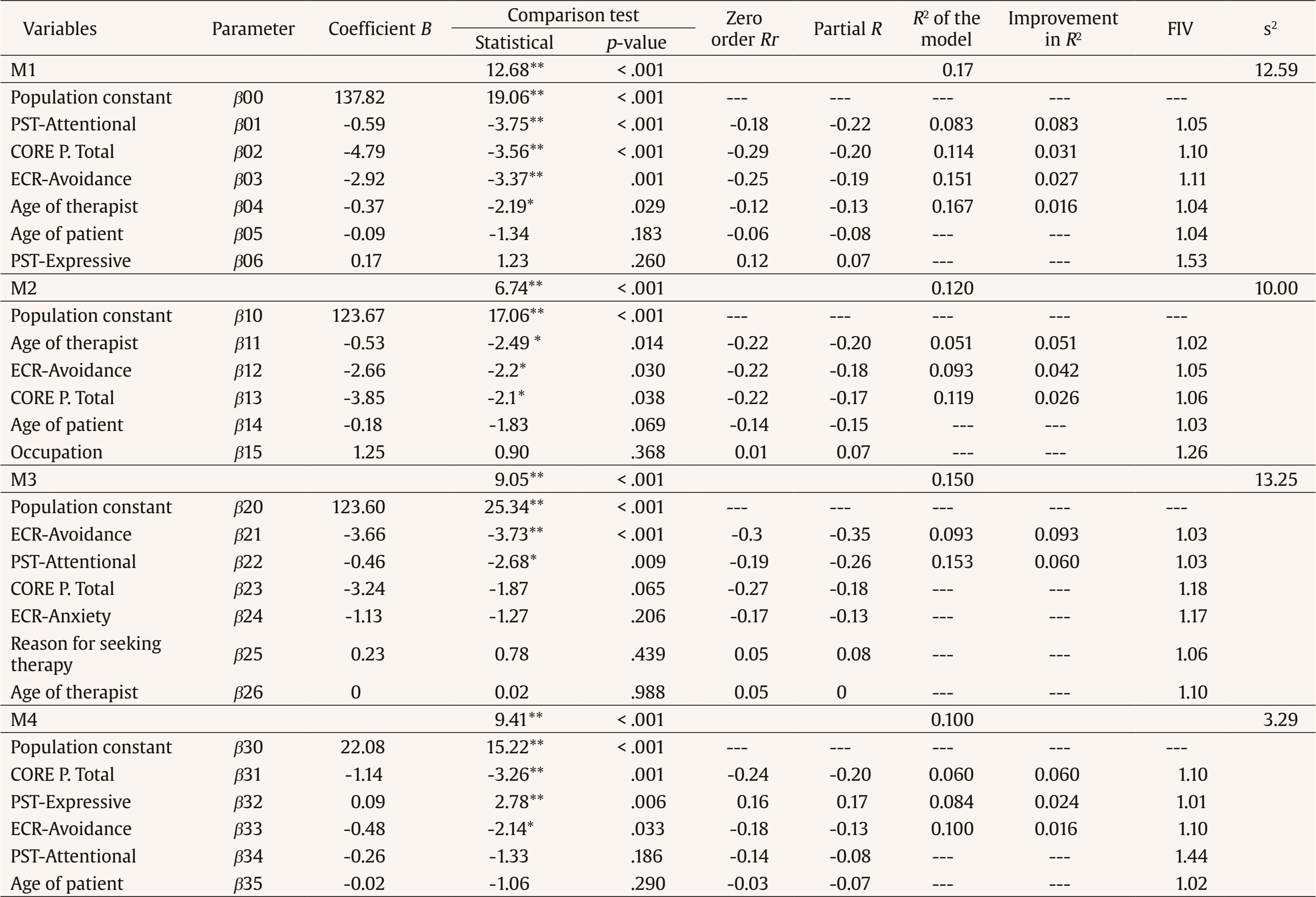 Note. M1 = total WATOCI score from the patient’s significant factors (CORE-OM and ECR-Attachment) and the Personal Style of the Therapist factors; M2 = total WATOCI score from the patient’s significant factors (CORE-OM and ECR-Attachment) and the Personal Style of the Therapist factors, cases in the initial phase of the alliance; M3 = WATOCI Theory of Change from the patient’s significant factors (CORE-OM y ECR-Attachment) from the patient’s significant factors (CORE-OM and ECR-Attachment) and the Personal Style of the Therapist factors, cases in the advanced phase of the alliance; M4 = predictive multivariate models of the WATOCI Bonding dimension from the patient’s significant factors (CORE-OM and ECR-Attachment) and the Personal Style of the Therapist factors; s2 = estimation error. *p < .05, **p < .01. Four key factors emerged as predictors. The PTS-Attentional was the most important (p < .001), providing 8.3% of the explained variance. The total CORE score (p < .001) contributed 3.1%, followed by attachment avoidance (ECR-Avoidance) (p < .01), which added 2.7%. Finally, the therapist’s age (p < .05) increased prediction by 1.6%. Model 2. Total WATOCI Score of the Patient’s Significant Factors (CORE-OM and ECR-Attachment) and the Personal Style of the Therapist Factors in the Initial Phase of the Alliance A model was carried out for each phase of the alliance, exploring to what extent the influential variables were determined by the stage of the therapeutic process. First, a model for the Total WATOCI score was prepared in those cases which were in an initial phase of alliance. A significant model (p < .001) was obtained with a total efficiency of 12%, comprising three main factors: the age of the therapist (this explains the 5.1% error reduction – older therapist, stronger alliance), followed by ECR-Avoidance, which added 4.2%, and CORE Total (the remaining 2.6%). Model 3. Total WATOCI Score of the Patient’s Significant Factors (CORE-OM and ECR-Attachment) and the Personal Style of the Therapist Factors in the Advanced Phase of the Alliance In this model of the Total WATOCI dimension with participants in the advanced phase of the alliance, the PTS-Attentional variable was included, which had a significant impact on the models. The CORE Total variable did not enter into the final model, although it was close to being significant. The final model, which was significant (15% efficacy), comprised two factors: ECR-Avoidance (9.3% error reduction) and PTS-Attentional (6%). If the CORE Total score had been significant, efficacy would have risen to 18.1%. Model 4. WATOCI Bonding Sub domain Score of the Patient’s Significant Factors (CORE-OM and ECR-Attachment) and the Personal Style of the Therapist Factors A model was prepared for each WATOCI sub-domain, including each of the bonding, tasks, goals, and ToC scores as a dependent variable in this case. Models very similar to those obtained in the total score were obtained, except in the case of the Bonding component, where clearly differential elements were found. The Bonding dimension model showed three predictive factors: the CORE Total score (6%), PST-Expressive (2.4%), and ECR-Avoidance (1.6%). The patient’s PTS-Attentional and age variables did not significantly improve prediction (p > .05). In line with previous findings (Flückiger et al., 2022; Horvath et al., 2011), the results of this study confirm the importance of the patient’s attachment style and the personal style of the therapist as key predictors of the therapeutic alliance. The design of the study, which differentiated between initial and advanced phases of treatment, allowed differences to be noted in the predictive capacity of these variables throughout the therapeutic process, offering a new and necessary perspective in this aspect of research. One of the most significant findings was the predictive capacity for avoidance in the patient’s attachment style. As previous research has suggested (Diener & Monroe, 2023; Mikulincer & Shaver, 2007), patients with an avoidant attachment style tend to avoid emotional intimacy which hinders the building of a solid alliance. In our study, avoidance manifested itself as a significant predictor of the quality of the alliance in both the initial and advanced phases of treatment. These results suggest that throughout the therapeutic process, patients with an avoidant attachment style continue to encounter difficulties in establishing and maintaining emotional bonding with the therapist, something that can negatively affect the development of the treatment. This finding coincides with literature that highlights the impact of avoidant attachment of therapeutic relations, where patients seek to minimize emotional dependency and maintain a defensive distance (Bernecker et al., 2014; Mallinckrodt & Jeong, 2015). In the initial phase of treatment, patient avoidance, general functioning, and therapist’s age were the key alliance predictors. Avoidance seems to act as an early obstacle to the building of a solid alliance, a factor that underlines the importance of therapists adjusting their focus in a way that respects the emotional limits of these patients. The general behavior of the patient, measured through CORE-OM, had a significant impact on the quality of the alliance, in line with research that links improved functioning with a greater ability to establish positive interpersonal relations (Horvath et al., 2011). Participants with the highest CORE-OM scores, indicative of more impaired general functioning and greater symptomatology, tended to form weaker alliances, especially in the initial phases of treatment, when their capacity to involve themselves in the therapeutic process was more compromised. These results underline the importance of comprehensively assessing the patient’s state, as poorer overall functioning hinders the creation of solid bonds, which is consistent with previous studies that pointed to alliance difficulties when interpersonal functioning is impaired (Chu et al., 2014; Evans et al., 2022; Lawson et al., 2020). With regard to the personal style of the therapist, the results show that in the advanced phase of the treatment, the attentional role acquired greater importance, suggesting that as the treatment progressed the therapist’s ability to be present, adjusted to the patient’s changing needs and maintaining a constant attention to the emotional details of the process, was key to the maintenance and consolidation of the alliance. This result reinforced the idea that therapists should be flexible and adaptable, especially when working with patients in the advanced stage of treatment, as this facilitates the adaptation of therapeutic goals and tasks to the patient’s emerging needs (Flückiger et al., 2022). Although it has not been explored in depth in earlier research, the therapist’s attentional role has been shown to be an influential factor in the building of the alliance, especially in terms of its technical components, such as goals and tasks (Botella & Corbella, 2005). In particular, recent studies suggest that open or floating attention on the part of the therapist may facilitate a greater consensus on treatment goals, especially late in the therapeutic process, where patient and therapist need to continually adjust to the changing demands of treatment (Corbella et al., 2024). Furthermore, the analysis of the specific components of the alliance revealed that the expressive role of the therapist has a significant impact on the bonding component, although not on treatment goals or tasks. This suggests that the therapist’s ability to express empathy and create a warm, understanding relationship is especially important to the development of an emotional bond with the patient, as proposed in previous studies (Fernández-Álvarez et al., 2003; Gelso & Kanninen, 2017). This finding underlines the importance of the expressive role as a crucial element in the creation of a strong therapeutic bond. This is less the case in other areas of the alliance, such as the setting of goals and tasks, which depend more on the therapist’s ability to adjust their attention and focus according to patient needs. In terms of the clinical implications of this, these results suggest that it is essential to adapt therapeutic interventions to the characteristics of the patient. In line with the previous study, it would seem to be crucial that the therapist adjusts their closeness to the patient depending on the attachment role that is present (Egozi et al., 2023). This is particularly clear in the case of patients with avoidant attachment, who may require a more gradual and less intrusive approach to emotional bonding in the early phases of treatment. Therapists should also be aware of how their own personal style, and in particular their attentional and expressive role, can influence an alliance throughout the therapeutic process. Finally, it is important that we recognize certain limitations in this study. Although the sample was taken from a natural clinical environment, which increased its external validity, the majority of the participants came from a private treatment context, a factor that might not accurately represent groups who were attended to in the public health system. Additionally, the use of self-reporting to measure the therapeutic alliance introduced a possible bias in the perception of patients and therapists, meaning that future research might benefit from the inclusion of observational methods or third-party assessment. The homogenous profile of the therapists (sex, therapeutic orientation, work context) may also be a limitation in this study, which does not allow more general conclusions to be drawn about the functioning of different therapists. In conclusion, this study highlights the importance of the patient’s attachment style and the personal style of the therapist as key predictors of the therapeutic alliance, with significant differences depending on the treatment phase. These findings contribute to a promising line of research that allows for the optimization of therapeutic interventions, adapting them to the individual characteristics of the patient and the therapist’s style, with the goal of improving long-term psychotherapeutic outcomes. Future research could expand on these findings by exploring how such variables influence more diverse samples of therapists, taking into account different theoretical orientations and working conditions. It would also be interesting to conduct longitudinal studies that analyze the evolution of therapeutic alliances over time and the possible adjustments in the therapist’s style as a function of this process. This would allow a better understanding of the alliance dynamic and its impact on the effectiveness of treatment.
Cite this article as: Bárez, N. B., Saúl, L. A., & Corbella S. (2026). Predictors of therapeutic alliance: Patient attachment and the personal style of the therapist. Clinical and Health, 37, Article e260719. https://doi.org/10.5093/clh2026a5 References |
Cite this article as: Bárez, N. B., Saúl, L. A., & Corbella, S. (2026). Predictors of Therapeutic Alliance: Patient Attachment and the Personal Style of the Therapist. Clinical and Health, 37, Article e260719. https://doi.org/10.5093/clh2026a5
Correspondence: nereabarez@nbpsicologia.es (N. B. Bárez).
Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
Clinical and Health is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License








