


Validation of Edinburgh Postnatal Depression Scale (EPDS) in Perinatal Women under War Conditions in Ukraine
[La validaciĂłn de la Escala Edimburgo de DepresiĂłn Posnatal en mujeres perinatales en condiciones de guerra en Ucrania]
Magdalena Chrzan-Dętkoś1, Iliana Liakea2, Natalia Murawska1, Raquel Costa3, Ana Uka4, Liudmyla Krupelnytska5, Alona Vavilova5, Helena S. García-López6, & Olha Morozova-Larina5
1Institute of Psychology, University of Gdask, Gdansk, Poland; 2Radboud University Nijmegen, Nijmegen, The Netherlands; 3Universidade LusĂłfona, Coimbra, Portugal; 4Western Balkans University, Tirana, Albania; 5Taras Shevchenko National University of Kyiv, Kyiv, Ukraine; 6University of Maryland Global Campus (Europe Site), Rota, Spain
https://doi.org/10.5093/clh2026a6
Received 9 October 2024, Accepted 11 December 2025
Abstract
Background: The present study aimed to assess the psychometric properties and the factor structure of the Ukrainian version of the Edinburgh Postnatal Depression Scale (EPDS) in the prenatal and postpartum women. Method: In a cross-sectional study, 625 participants, including 207 (33.2%) pregnant and 408 (66%) postpartum women, completed online questionnaires: Edinburgh Postnatal Depression Scale (EPDS), the City Birth Trauma Scale (City BiTS), Generalized Anxiety Disorder (GAD-7) and a sociodemographic questionnaire. Results: A 3-factor model (anhedonia, anxiety, and depression) is the best fit to the data, both for antepartum and postpartum samples. EPDS exhibits excellent internal consistency for the overall scale and good internal consistency for its subscales. The total sample’s Cronbach’s alpha has a value of .87 for antepartum women and .86 for postpartum women, similar to those of the original scale. Conclusions: The Ukrainian version of EPDS is reliable and can be used to screen in the perinatal period, during pregnancy, and in the postpartum period.
Resumen
Antecedentes: El estudio pretende analizar las propiedades psicométricas y la estructura factorial de la versión ucrania de la Escala Edimburgo de Depresión Perinatal (EPDS) en mujeres prenatales y posparto. Método: En un estudio transversal, 625 mujeres participantes, de ellas 207 (33.2%) embarazadas y 401 (66.8%) posparto rellenaron los siguientes cuestionarios online: la Escala Edimburgo de Depresión Posnatal EPDS), la Escala City de Traumas en el Nacimiento (City BiTS), Trastorno de Ansiedad Generalizada (GAD-7) y un cuestionario socidemográfico. Resultados: El que mejor se ajusta a los datos es un modelo trifactorial (anhedonia, ansiedad y depresión), tanto para las muestras anteparto como para las posparto. La escala de Edimburgo muestra una excelente consistencia interna para la escala global y una buena consistencia para sus subescalas. El alfa de Cronbach para la muestra total es de .87 para las mujeres anteparto y .86 para las posparto, como para las de la escala original. Conclusiones: La versión ucrania de la escala de Edimburgo es fiable y puede utilizarse como criba en el periodo perinatal, durante el embarazo y tras el parto.
Palabras clave
DepresiĂłn perinatal, EEDP, ValidaciĂłn, Ucrania, GuerraKeywords
Perinatal depression, EPDS, Validation, Ukraine, WarCite this article as: Chrzan-Dętkoś, M., Liakea, I., Murawska, N., Costa, R., Uka, A., Krupelnytska, L., Vavilova, A., García-López, H. S., & Morozova-Larina, O. (2026). Validation of Edinburgh Postnatal Depression Scale (EPDS) in Perinatal Women under War Conditions in Ukraine. Clinical and Health, 37, Article e260717. https://doi.org/10.5093/clh2026a6
Correspondence: Magdalena.chrzan-detkos@ug.edu.pl (M. Chrzan-D tko ).Depression is the most common mental health problem during pregnancy and postpartum period. The prevalence of perinatal depression (PD) varies between countries, but it is estimated that 17.2% of women experience PD worldwide (Wang et al., 2021). The World Health Organization (WHO, 2022) recommends a step-by-step approach to screen for PD to ensure accurate identification and effective intervention. The initial screening with the use of standardized screening tools like the Edinburgh Postnatal Depression Scale (EPDS) is recommended to identify symptoms of PD and as in other countries, the Ukrainian prenatal and postpartum women should have access to the validated screening tool. Russia’s invasion of Ukraine and a full scale war, which began on February 24, 2022, poses additional threat and burden for the Ukrainian population including mothers and their families in the perinatal period. Approximately one-third of all Ukrainians, including children, have been forced to flee their homes (Lutsenko et al., 2023). This population includes a significant number of mothers with infants and small children, who have had to adapt to life in new countries amidst the ongoing conflict. In March 2025, there were approximately 6.37 million Ukrainian refugees registered across Europe (UNHCR, 2025). Since the start of the war till August 2024, more than half a million babies were born and registered in Ukraine (Save the Children, 2024). War and armed conflicts rank among the most catastrophic human tragedies, with their impacts often hitting the most vulnerable groups hardest, particularly women in the perinatal period and their newborns (Rodríguez-Muñoz & Chrzan-Dętkoś, 2025). Safeguarding Health in Conflict Coalition and Insecurity Insight (2025) documented 1,279 incidents of violence against health care systems until the end of 2023 (De Vos et al., 2023). The war context has a detrimental impact on mental health, with rates of depression, anxiety, and post-traumatic stress disorder (PTSD) being two to three times higher among individuals exposed to armed conflict compared to those not exposed (Carpiniello, 2023; Lushchak et al., 2023). This may also apply to women in perinatal period as described in some studies (Korchinska et al., 2022; Savrun et al., 2024; Zhabchenko et al., 2018). Several studies have indicated that being in a combat zone, or even recalling such experiences, can be significant causes of depression or can greatly worsen the emotional state of pregnant and postpartum women (Keasley et al., 2017; Khalifa et al., 2015). Punamäki et al. (2018) found that pregnant and postpartum women living in the Gaza territory during the Gaza War experienced mental health problems, including increased symptoms of PTSD, anxiety, depression, and dissociative states, along with pregnancy complications. In the Klapper-Goldsten et al.’s (2024) study involving 502 women, with 230 delivering during the war and 272 delivering before the war, the rates of PD were higher in women delivering during the war compared to those delivering before war (26.6% vs. 12.4%). In Mohammad et al.’s (2018) study among postpartum women as war-affected refugees from Syria, almost half of them scored > 12 on EPDS. Also, another study conducted in war-affected Syria indicates a high percentage of women scoring higher on the PD scale (28.20%; Roumieh et al., 2019). Heer et al.’s (2024) meta-analysis and systematic review revealed that the prevalence of PD among refugee and asylum-seeking women from different cultural backgrounds was 22.5%, while the prevalence of non-refugee/asylum-seeking women with PD was 17.5%. Additionally, a meta-analysis of 40 studies, involving 10,123 participants, concluded that one-third of refugee women from low- and middle-income countries experienced PD (Fellmeth et al., 2018). Screening for depression is not currently part of routine perinatal care in Ukraine (Martsenkovsky et al., 2009). Also, there are no epidemiological data describing PD rates in the perinatal women population in Ukraine. Since the invasion on 24.02.2022, and even prior to the armed conflicts in Eastern regions of Ukraine, several studies have been conducted on specified groups of women. A survey conducted in 2020 by Gusak et al. (2024) among Ukrainian women of young children receiving services from non-governmental organizations showed a quite high prevalence: 39 percent of mothers scored > 13 on the EPDS. However, the participants were not only postpartum women, but mothers of children aged 0 to 5, and the study was conducted during the COVID-19 pandemic, which could have also influenced the results. Bailey et al. (2016) study focusing on the prevalence of the depressive symptoms among pregnant and postpartum HIV-positive women in Ukraine found that 27% antenatally and 25% postpartum participants screened positive for depressive symptoms. In Zhabchenko et al.’s (2018) study, in a group of 96 internally displaced pregnant women depressive symptoms were diagnosed in one fourth of women. These indicators exceeded the indicators of the control group (n = 34, Ukrainian women, not internally displaced) by 6 times. At the initial stage of a full-scale invasion in internally displaced pregnant women, depressive symptoms (measured with Beck Depression Inventory) were detected in 85.7% of them, 26.9% fulfilling criteria for mild depression; 36.5% for moderate depression; 17.5% for severe depression; and 4.8% for extremely severe depression (Korchinska et al., 2022). One third of women in the early stages of motherhood, from Vinnytsia (central Ukraine), had mental disorders in 2024, while before the beginning of the full-scale war in 2021, the proportion of such women was significantly lower (Savrun et al., 2024). At the same time, the frequency of women with an increased risk of postpartum depression and psychosis in the group with an unplanned pregnancy was higher. There is also data indicating an increased level of anxiety in those pregnant women in the second and third trimesters of pregnancy who are expecting a boy (Pelekh, 2023). Worldwide, there are several screening instruments for PD with the EPDS scale being the most commonly used (Cox, 2019). The EPDS was developed as a uni-dimensional measure of depression (Cox et al., 1987). In 2019, the EPDS was available in 60 languages (Cox, 2019). Previous research has supported different models, including one-, two-, and three-factor structures. This structure typically encompasses core depressive symptoms, anxiety, and anhedonia. In the present review, we identified five studies reporting a two-factor solution and seven studies supporting a three-factor solution. Most studies favored the three-factor model. Also for example Coates et al.’s (2017) study conducted on large community samples of women taking part in the Avon Longitudinal Study of Parents and Children (ALSPAC) has confirmed the three-factor structure model. The anxiety subscale (EPDS-3A) emerges consistently and has been linked to a maternal history of anxiety disorders (Lautarescu et al., 2022). The third subscale, anhedonia, represents a core feature of major depressive disorder (MDD), with up to 70% of individuals experiencing it (Cao et al., 2019). Anhedonic features in MDD have been associated with a worse course and outcome, and may predict nonresponse to treatment, as selective serotonin reuptake inhibitors (SSRIs) appear less effective in patients with the anhedonic subtype (Luca et al., 2024). Targeted interventions may therefore be particularly important for this group. Overall, the three-factor structure holds significant clinical relevance and has important implications for intervention design. Based on a brief literature review of 6 recent years presented in Table 1, it was observed that EPDS could be used as a multi-dimensional measure too. Few studies have examined the severity of PD symptoms using the EPDS during wars, but the available data suggests that the EPDS may serve as an important and reliable screening tool in situations of war and armed conflicts (Klapper-Goldsten et al., 2024; Mohammad et al., 2018). Table 1 Factor Structure of the Edinburgh Postnatal Depression Scale in Previous Recent Papers (between 2019 and 2024) 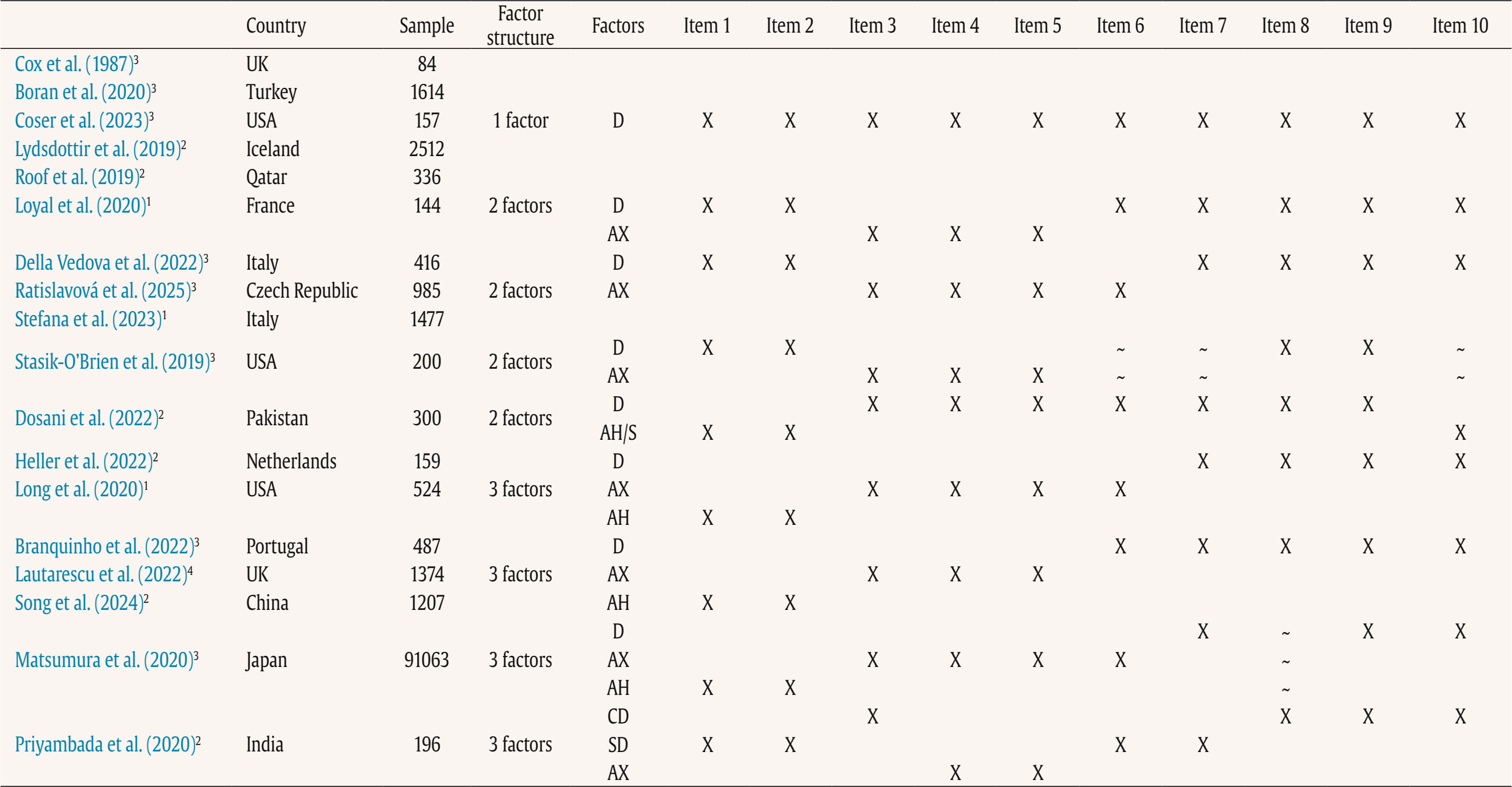 Note. D = depression; AX = anxiety; AH = anhedonia; S = suicide; CD = cognitive depression; SD = somatic depression; 1peripartum population; 2antepartum population; 3postpartum population, 4antepartum high risk population; Item 1: “I have been able to laugh and see the funny side of things”; Item 2: “I have looked forward with enjoyment to things”; Item 3: “I have blamed myself unnecessarily when things go wrong”; Item 4: “I have been anxious or worried for no good reason”; Item 5: “I have felt scared or panicky for no very good reason”; Item 6: “Things have been getting on top of me”; Item 7: “I have been so unhappy that I have had difficulty sleeping”; Item 8: “I have felt sad or miserable”; Item 9: “I have been so unhappy that I have been crying”; Item 10: “The thought of harming myself has occurred to me.” Based on these data, we can observe that the PD severity is high in Ukraine, especially now, during the full-scale war. As pregnant women, mothers, and families with infants (Chrzan-Dętkoś, et al., 2022) are especially vulnerable, there is an urgent need to ensure a valid and cost-effective method for the screening of depression so that mothers in need may be referred to mental health specialists. Effective screening is crucial for successfully implementing the stepped-care approach as recommended by the World Health Organization (WHO, 2022). Although some translation of PD screening questionnaires are available in Ukraine, to the best of our knowledge, they are not validated. Additionally, no validation of EPDS, the most commonly used screening tool, in the Ukrainian language exists. Pushkareva (2005) notes that the Cronbach’ alpha coefficient of the scale translated from English is .79. However, this version of the scale was not found in existing publications today. In Ukrainian-language publications, where EPDS is mentioned, (Danilchenko & Kanigina, 2023; Grygus, 2023; Romanenko & Yesip, 2022), the authors refer to the original EPDS, without specifying information about the adaptation. In the appendix of the Medical Care Standards, “Normal pregnancy” approved by the Order of the Ministry of Health of Ukraine No. 1437 of 09/08/2022 (Dubossarska et al., 2022), the text of EPDS is given in Ukrainian but no information about adaptation or psychometric properties is provided. According to Cox (2017), the validity of the scale for the population of mothers completing the EPDS should be calculated. As such, the validation of the Ukrainian version is crucial. The main objective of this study was to translate into the Ukrainian language and validate EPDS for the Ukrainian population of pregnant and postpartum women. Since the EPDS is widely used during both pregnancy and the postpartum period, including both groups provides a broader perspective on its applicability across the perinatal continuum. More specifically the study’s objectives were to:
This study used data from the prospective observational cohort study “Perinatal Mental Health for Refugee Women Study”, aimed at evaluating the psychological impact of the war on pregnant and postpartum women. This study received approval from the Ethics Committee of the principal institutions participating in the study: The Research Ethics Committee of Universidad Nacional de Educación a Distancia (21-PSI-2022) and the Research Ethics Committee of the Faculty of Psychology of Taras Shevchenko National University of Kyiv (Date: August of 2022, Decision No. 04, Protocol No. 01) and its designers. The study design has been registered in ClinicalTrials.gov (ref: NCT05654987) following the gold standards for cross-sectional studies, as outlined by STROBE (Vandenbroucke et al., 2007). To address potential emotional states’ affection and risk for participants, a list of up-to-date services and resources in Ukrainian language was provided at the survey webpage, offering information and assistance regarding free of charge mental health services and lactation advice. On the study website, there were also informational leaflets about postpartum depression symptoms in Ukrainian language, as well as methods for both self-help and treatment. Additionally, contact details for the lead research team in each nation was available for participants seeking further information. Data Collection Data collection is described comprehensively elsewhere (Rodríguez-Muñoz et al. 2023). To summarize, data were collected through an online questionnaire administered via the Qualtrics® XM survey platform from 01 December 2022 to 01 October 2023. Invitations for anonymous participation were disseminated through various platforms, including Facebook groups, Instagram, personal contacts, and Ukrainian support centers in European countries. The study was advertised on social media, information was sent to popular parenting social media groups in Ukraine, and the study information was published in Ukrainian media, such as ELLE. Flyers were distributed to help centers for Ukrainians in Poland. Co-authors from Ukraine actively promoted the project within the local community. Participants were asked to read an information sheet about the study, which explained the voluntary nature of participation and the option to withdraw at any stage, and sign an informed consent before completing the questionnaires. Participants Inclusion criteria for participation were: being (i) pregnant or a biological mother of an infant up to 12 months of age, (ii) 18 years or older, and (iii) a war refugee from Ukraine (entrance to European countries from 24 February 2022), or staying in Ukraine after 24 February 2022 during the war (being internally displaced or non-displaced). Only participants that had fully completed the EPDS and responded to whether they were pregnant or at postpartum period were included in the final sample. The final sample consisted of N = 625 women, 207 (33.2%) were pregnant and 418 (66.8%) were at the postpartum period. About three-quarters were living in Ukraine during the war at the same place as before (non-displaced women), around 10% women were internally displaced, and around 15% of women had moved to other/host countries (externally displaced). External refugees had residences in Poland, Germany, Portugal, Latvia, Estonia, Denmark, Spain, Romania, Hungary, France, Belgium, Netherlands, Lithuania, Austria - in various settlements (big urban area: 59%; small urban area: 22%; rural area: 9%). Descriptive statistics of the total sample and separately for the antepartum and postpartum women are detailed in Table 2. Table 2 Characteristics of the Participants 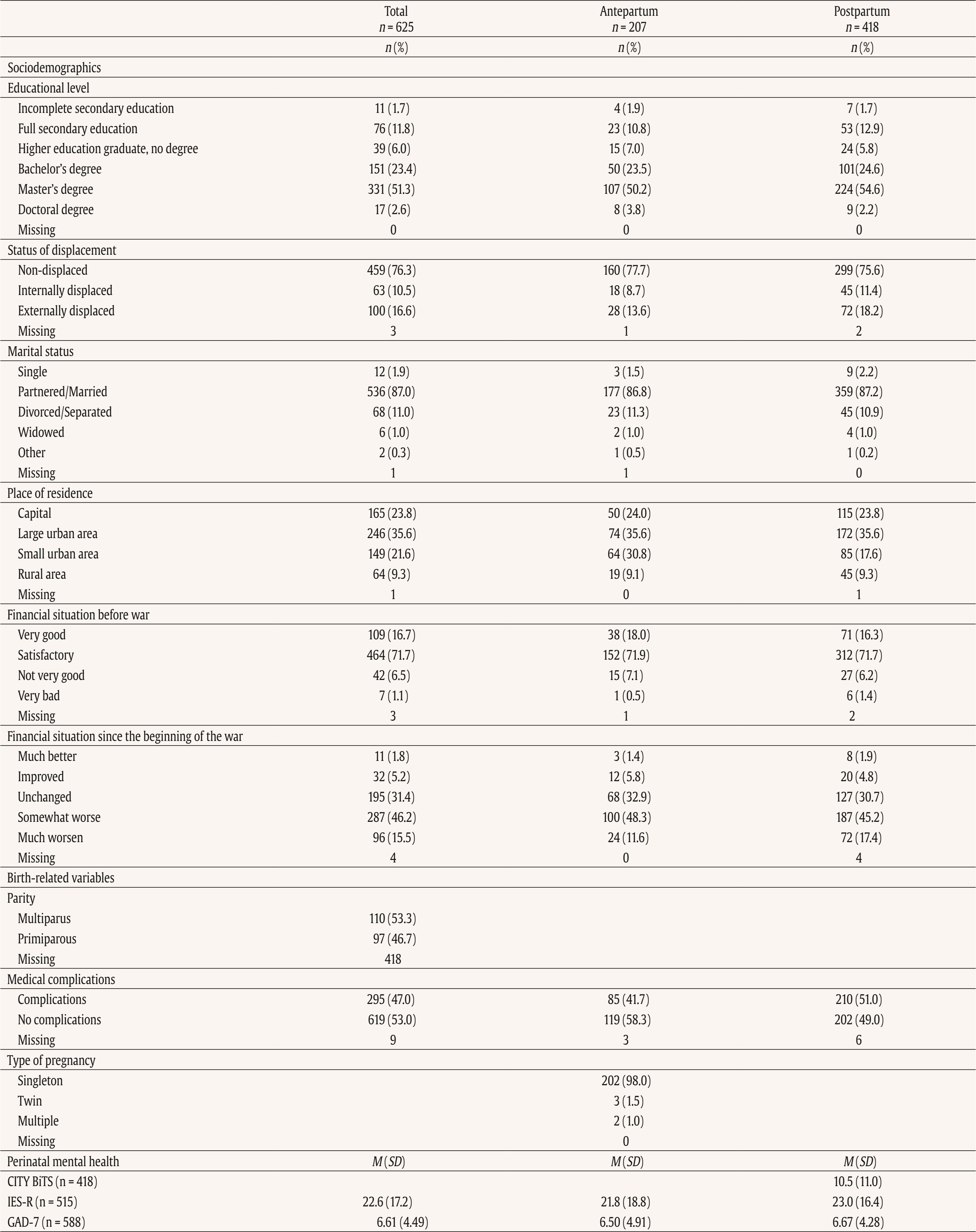 Note. CITY BiTS = City Birth Trauma Scale; IES-R = Impact of Event Scale-Revised; GAD-7 = General Anxiety Disorder. Instruments Assessment, Care, and Trust - Pregnant and New Mothers (ACT-PNM) This form was created by the authors (Blinded, 2022) for this study to collect sociodemographic data. The ACT-PNM includes questions about educational level, marital status, place of residence, the financial situation before the war and since the beginning of the war, medical complications during pregnancy and type of pregnancy. The questions are scored on a categorical scale depending on the covering issue. This form was completed by all participants. The Edinburgh Postnatal Depression Scale (EPDS; Cox et al., 1987) The EPDS is a self-reported questionnaire consisting of 10 items that are specifically designed to assess symptoms of depression in the perinatal period. The items are scored on a 4-point Likert scale ranging from 0 to 3. Thus, the total score of the scale ranges between 0 to 30. Systematic reviews and meta-analyses have shown that a score of 13 or more points provides higher specificity in identifying clinically significant depressive symptoms during both pregnancy and the postpartum period (Levis et al., 2020; O’Connor et al., 2016). Internal consistency shows a Cronbach É‘ of .87 in the original study (Cox et al., 1987). The positive predictive value equals 70% (Cox et al., 1987), or even 90% (Zelkowitz & Tamara, 1995). The Ukrainian version of EPDS underwent the standard translation and back-translation methodology, adhering to the translation principles outlined in the EPDS manual (Cox et al., 2014). This scale was completed by all participants. General Anxiety Disorder (GAD-7; Spitzer et al., 2006) The GAD7 is a self-reported measurement of 7 items that assesses symptoms of generalized anxiety disorder (GAD). The items are measured on a 4-point Likert scale ranging from 0 not at all to 3 nearly every day. The total score ranges from 0 to 21. The internal consistency of the original version of the GAD-7 was excellent with Cronbach’s α = .92 (Spitzer et al., 2006). In the current study, Cronbach’s α was .87, signifying a good internal consistency. The Ukrainian version of GAD-7 was validated for the purpose of the project this study is a part of, however, the results are not published yet (Chrzan-Dętkoś et al., 2026; Uka et al., 2025). This scale was completed by all participants. Impact of Event Scale-Revised (IES-R; Weiss & Marmar, 1997) The IES-R was used to measure the symptoms of post-traumatic stress disorder (PTSD). This is a self-reported tool that assesses symptoms of PTSD experienced within the last 7 days, especially in the response sets of intrusion, avoidance, and hyperarousal, as well as total subjective stress. It consists of 22 items rated on a 5-point Likert scale ranging from 0 not at all to 4 extremely. The total score ranges from 0 to 88, where a higher score indicates a higher level of PTSD symptoms. Internal consistency was excellent with Cronbach’s α = .95. The internal consistency calculated for our sample was identical. The Ukrainian version of IES-R was translated into Ukrainian by the study authors (Krupelnytska et al., 2025). This scale was completed by all participants. City Birth Trauma Scale (City BiTS; Ayers, 2018) The City BiTS was used to measure symptoms of PTSD related to childbirth. It consists of 29 items, with 20 items dedicated to measuring the four clusters of symptoms following the DSM-5 (APA, 2013) criteria: re-experiencing, avoidance, negative cognitions and mood, and hyperarousal during the preceding week. The questions that correspond to the stressors criteria (criterion A) have a binary response option (yes/no), whereas all the others are rated on a 4-point Likert scale ranging from 0 “not at all” to 3 “five or more times”. The total score ranges from 0 to 60 points, with a higher score indicative of elevated childbirth-related PTSD symptoms. The original version of the City BiTS showed excellent reliability with Cronbach’s α = .92 for the total scale (Ayers et al., 2018). We used the Ukrainian version of the scale, validated for the purpose of the project this study is a part of (Chrzan-Dętkoś et al., 2022). This scale was completed only by postpartum women. Statistical Analyses All analyses were conducted for two groups (antepartum and postpartum). Descriptive statistics were computed to report the socio-demographic and mental health-related characteristics of participants overall and according to the perinatal period. Eighteen confirmatory factor aAnalysis (CFA) were conducted to test the fit of different previously identified models to our samples (antepartum and postpartum), These included one-factor, two-factor and three-factor models. Model fit was assessed using the comparative fit index (CFI), the Tucker-Lewis Index (TLI), the root-mean-square error of approximation (RMSEA), and the standardized root-mean-square residual (SRMR). Adequate or good model fit were considered if CFI and TLI values ≥ .90 or ≥ .95, RMSEA values ≤ .08 or ≤ .06, and SRMR values ≤ .10 or ≤ .08, respectively (Browne & Cudeck, 1993; Hu & Bentler, 1999). The Akaike Information Criterion (AIC; Akaike, 1987) was used to compare models. Factor loadings over .40 are considered meaningful (Tabachnick & Fidell, 2007). The internal consistency was assessed using the CFA best-fitting model by computing item-total correlation, average inter-item correlation, McDonald’s omega and Cronbach’s alpha coefficients. Good internal consistency was considered when Cronbach’s alpha is over .70 and mean inter-item correlations exceed .15 (Nunnally & Bernstein, 1994) and item-total correlation is over .30 (Field, 2005). Convergent validity was analyzed using Pearson correlations (listwise deletion) between EPDS total score and subscales score, GAD-7, City BiTS, and IES-R total score. We opted for listwise deletion to handle missing data, as the pattern appeared to be random and likely related to the varying conditions under which participants completed the questionnaires. A t-test analysis was conducted to compare the postpartum and antepartum group. Confirmatory Factor Analyses The results of CFAs are detailed in Table 3 and 4. Table 3 Confirmatory Analysis of All the Factor Structures Found in Previous Papers for Antepartum Women 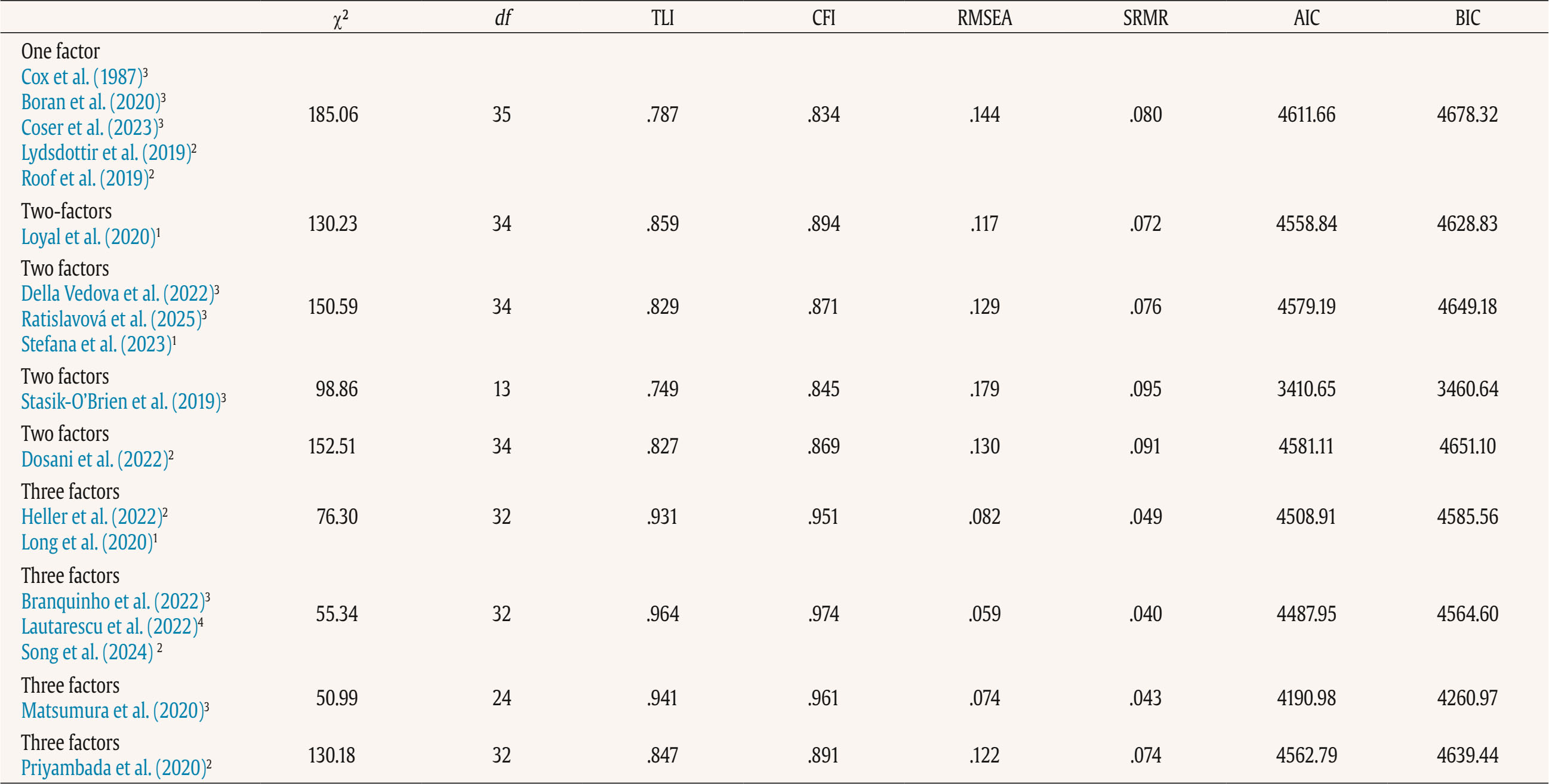 Note. 1Peripartum population; 2antepartum population; 3postpartum population; 4antepartum high risk population; The models tested align with all factor structures identified in the literature (the citation corresponds exactly with the tested model – see Table 1). ***p < .001. Table 4 Confirmatory Analysis of All the Factor Structures Found in Previous Papers for Postpartum Women 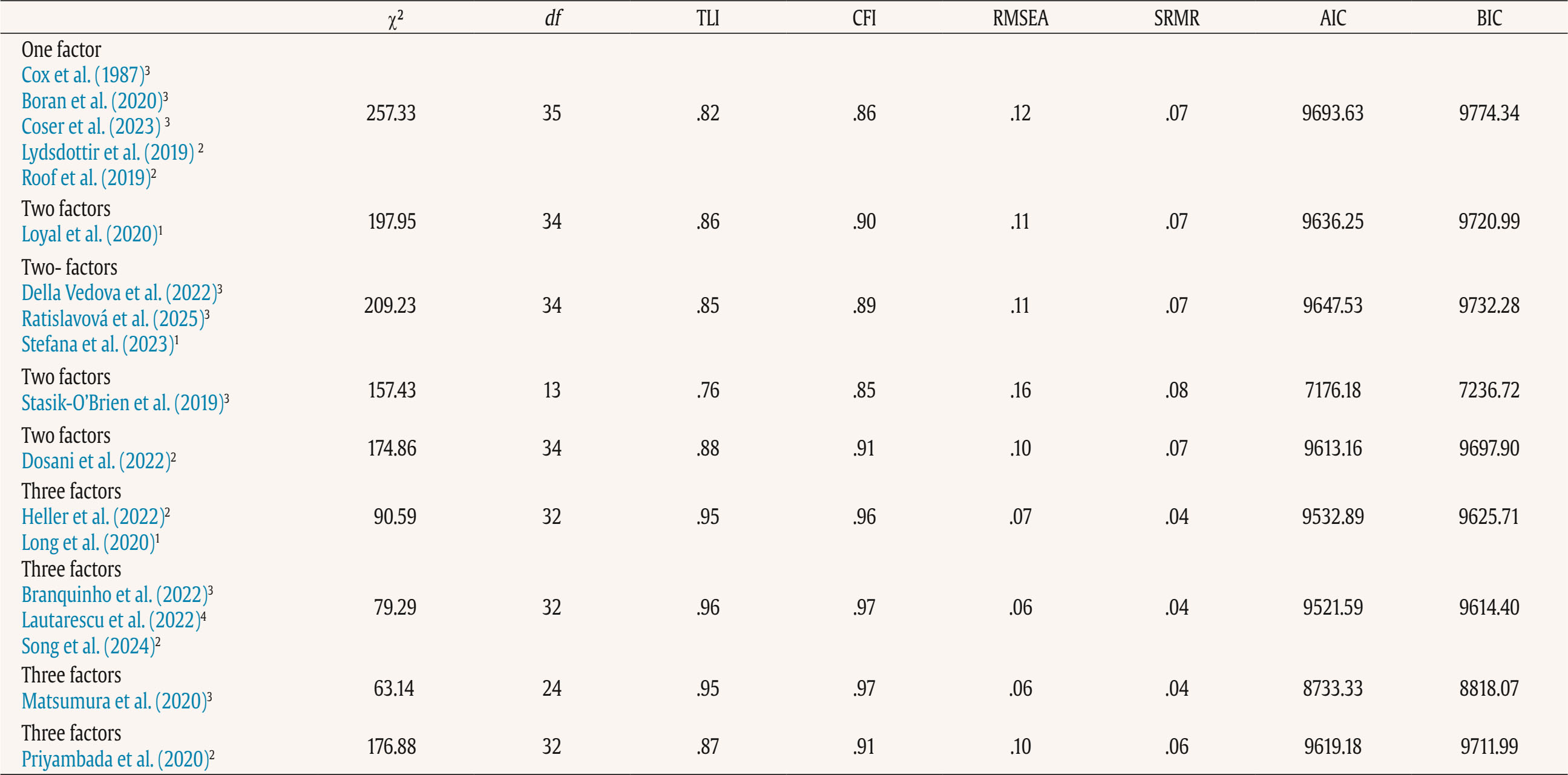 Note. 1Peripartum population; 2antepartum population; 3postpartum population; 4antepartum high risk population. The models tested align with all factor structures identified in the literature (the citation corresponds exactly with the tested model – see Table 1). ***p < .001. Table 3 shows fit indices for nine confirmatory factor models of the EPDS in the pregnant sample. Models 6-8 (three-factor structures) demonstrated substantially better fit (CFI ≥ .95, TLI ≥ .93, RMSEA ≤ .08, SRMR ≤ .05) compared with the one- and two-factor solutions. Model 7 showed the best overall fit, χ²(32) = 55.34, p > .05, CFI = .97, TLI = .96, RMSEA = .06, SRMR = .04, AIC = 4487.95, BIC = 4564.60. Table 4 shows fit indices for nine confirmatory factor models of the EPDS in the postpartum sample. Models 6-8 (three-factor structures) demonstrated substantially better fit (CFI ≥ .95, TLI ≥ .94, RMSEA ≤ .07, SRMR ≤ .04) compared with the one- and two-factor solutions. Model 7 showed the best overall fit, χ²(32) = 79.29, p > .05, CFI = .97, TLI = .96, RMSEA = .06, SRMR = .04, AIC = 9521.59, BIC = 9614.40. These results indicate that, among postpartum women, the EPDS is best represented by a three-factor structure comprising Anhedonia (items 1-2), Anxiety/Worry (items 3-5), and Depressive symptoms (items 6-10). This three-factor model provides a strong and parsimonious fit, supporting the multidimensional nature of depressive symptoms measured by the EPDS in the postpartum period. The best-fitting model is a three-factor model found in Branquinho et al. (2022), Lautarescu et al. (2022), and Song et al. (2024) studies. The factor loading of each EPDS item is depicted in Table 5. All factor loadings were above .40. Table 5 Standardized Factor Loadings - Best Model (M7: 1-2/3-5/6-10) 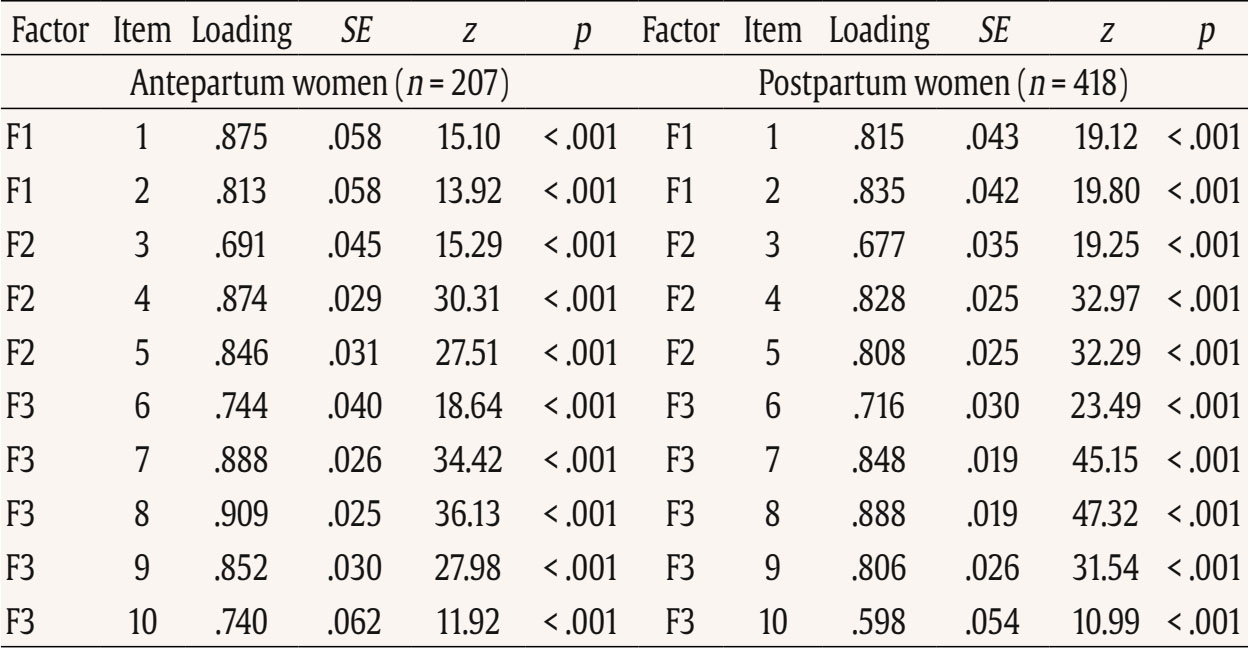 Note. Item 1: “I have been able to laugh and see the funny side of things”; Item 2: “I have looked forward with enjoyment to things”; Item 3: “I have blamed myself unnecessarily when things went wrong”; Item 4: “I have been anxious or worried for no good reason”; Item 5: “I have felt scared or panicky for no very good reason”; Item 6: “Things have been getting on top of me”; Item 7: “I have been so unhappy that I have had difficulty sleeping”; Item 8: “I have felt sad or miserable”; Item 9: “I have been so unhappy that I have been crying”; Item 10: “The thought of harming myself has occurred to me.” Descriptive Statistics A descriptive analysis was conducted on the 10 items of EPDS (see Table 6). The analysis included calculations of the mean, standard deviation, range, skewness, and kurtosis. The results indicated that all items demonstrated a complete range of values from 0 to 3, and none of the items exceeded the proposed cut-off of 3 for skewness (except item 10 for antepartum women) and 10 for kurtosis (Kline, 2011). Table 6 Descriptive Statistics of the EPDS Items 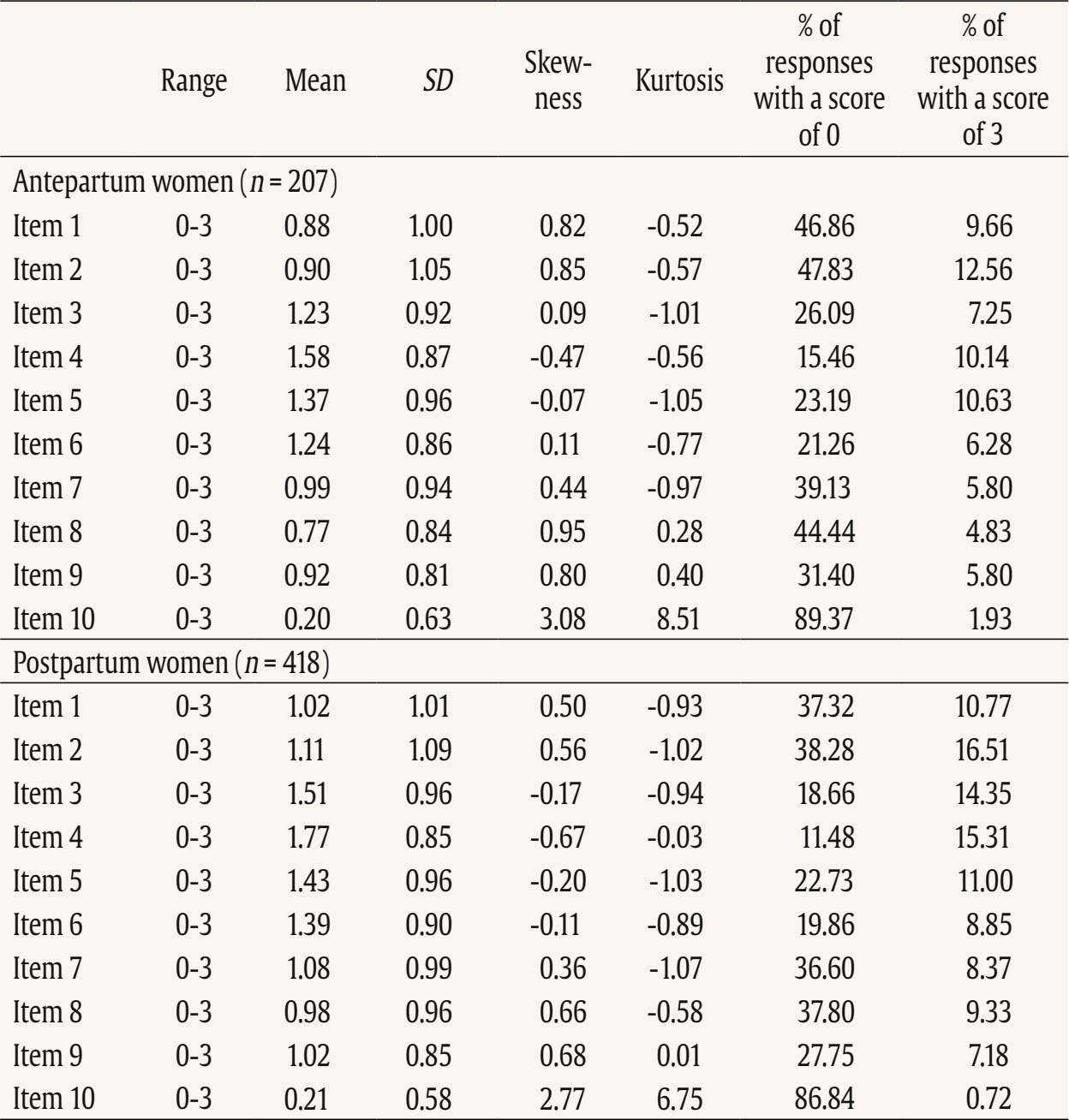 Note. Item 1: “I have been able to laugh and see the funny side of things”; Item 2: “I have looked forward with enjoyment to things”; Item 3: “I have blamed myself unnecessarily when things went wrong”; Item 4: “I have been anxious or worried for no good reason”; Item 5: “I have felt scared or panicky for no very good reason”; Item 6: “Things have been getting on top of me”; Item 7: “I have been so unhappy that I have had difficulty sleeping”; Item 8: I have felt sad or miserable”; Item 9: “I have been so unhappy that I have been crying”; Item 10: “The thought of harming myself has occurred to me.” A descriptive analysis was also calculated for the total score and subscales related to EPDS (see Table 7). The analysis included calculations of the range, mean, standard deviation, skewness, and kurtosis. None of them exceeded the proposed cut-off of 3 for skewness and 10 for kurtosis (Kline, 2011). Table 7 Descriptive Statistics of the EPDS and Subscales 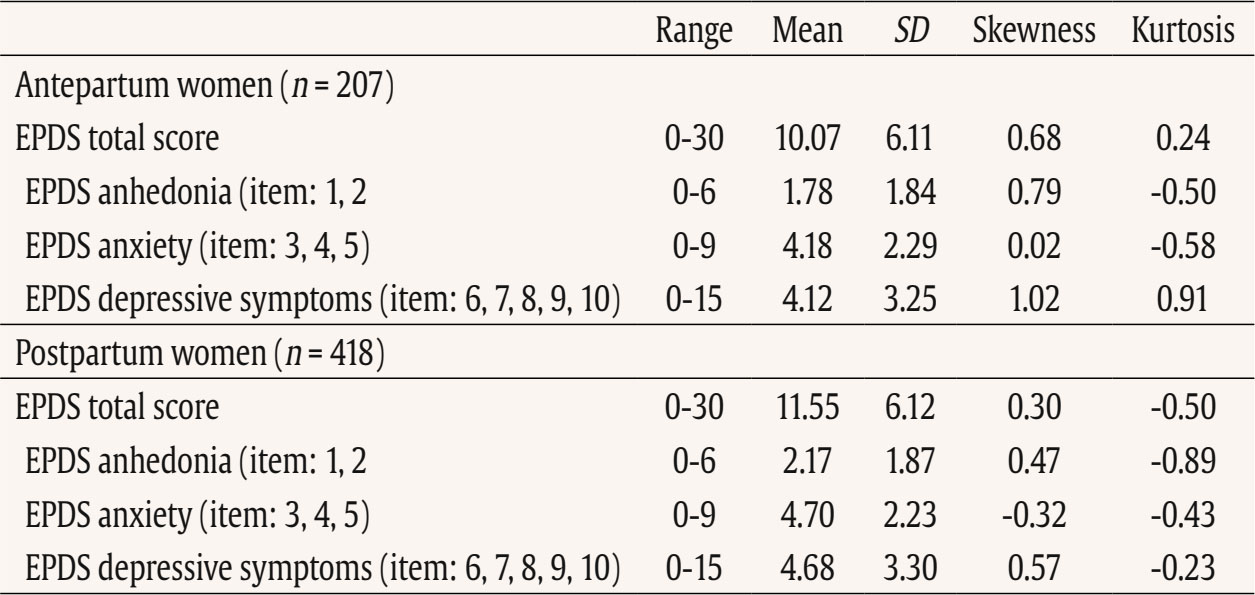 Table 8 shows the correlation between items. All items are positively and significantly correlated. The average inter-item correlation is r = .52 for pregnant women and r = .47 for postpartum women. Table 8 Inter-Item Correlation Matrix of EPDS Items 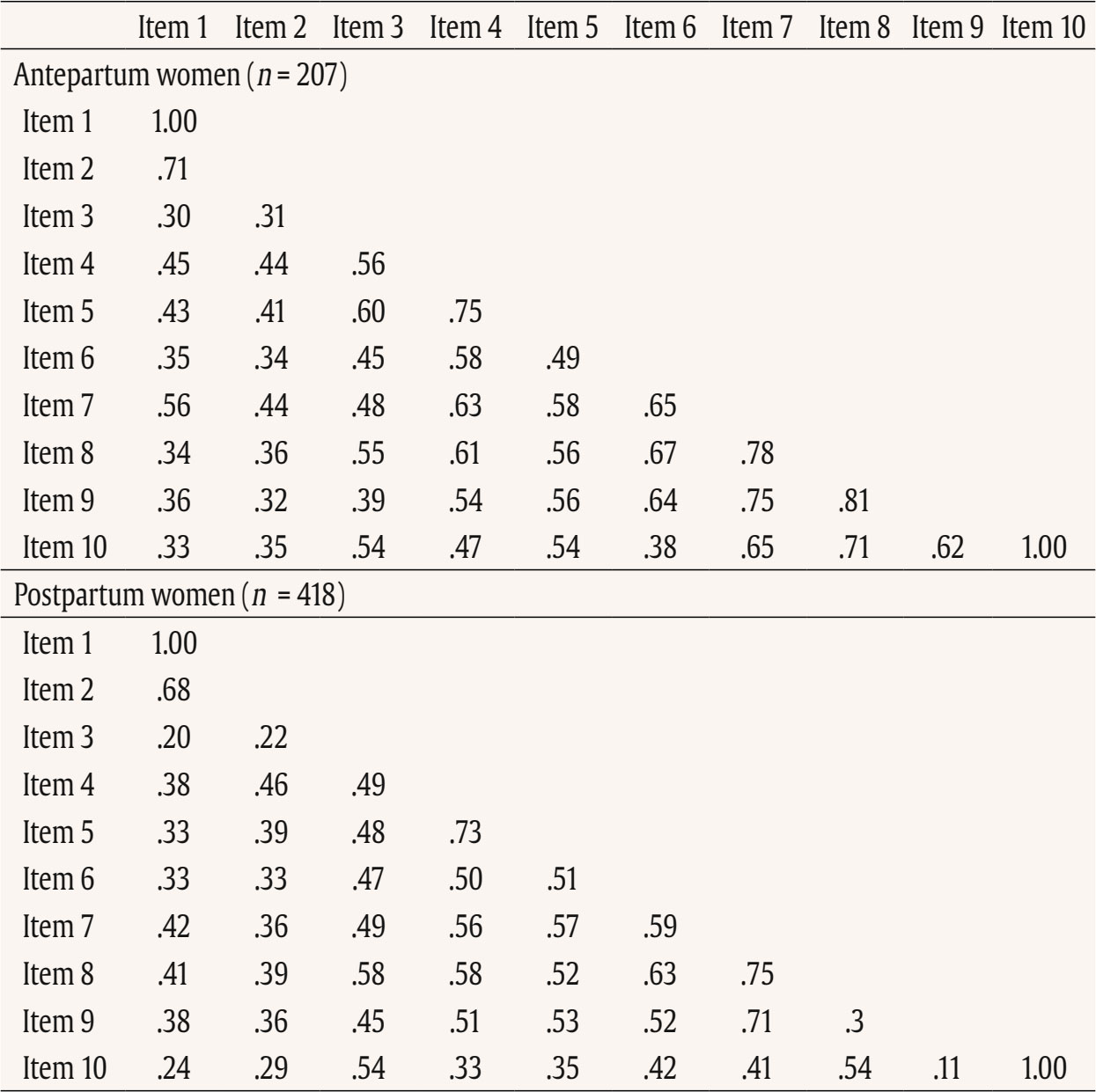 Note. Item 1: “I have been able to laugh and see the funny side of things”; Item 2. “I have looked forward with enjoyment to things”; Item 3: “I have blamed myself unnecessarily when things went wrong”; Item 4: “I have been anxious or worried for no good reason”; Item 5: “I have felt scared or panicky for no very good reason”; Item 6: “Things have been getting on top of me”; Item 7: “I have been so unhappy that I have had difficulty sleeping”; Item 8: “I have felt sad or miserable”; Item 9: “I have been so unhappy that I have been crying”; Item 10: “The thought of harming myself has occurred to me.” p < .001. Reliability Internal consistency demonstrated satisfactory reliability. The total sample Cronbach’s alpha coefficients confirmed a value of 0.87 for the EPDS total for antepartum women and .86 for the EPDS total for postpartum women. The item-total correlation (r) of the items ranged from .35 to .73. All item-total correlations are over .30. The deletion of any of the items would not increase Cronbach’s alpha. See details in Table 9. Internal consistency of the EPDS subscale also demonstrated satisfactory reliability (Table 10). Table 9 Cronbach’s α if Item Deleted and Item-Total Correlation of EPDS Items 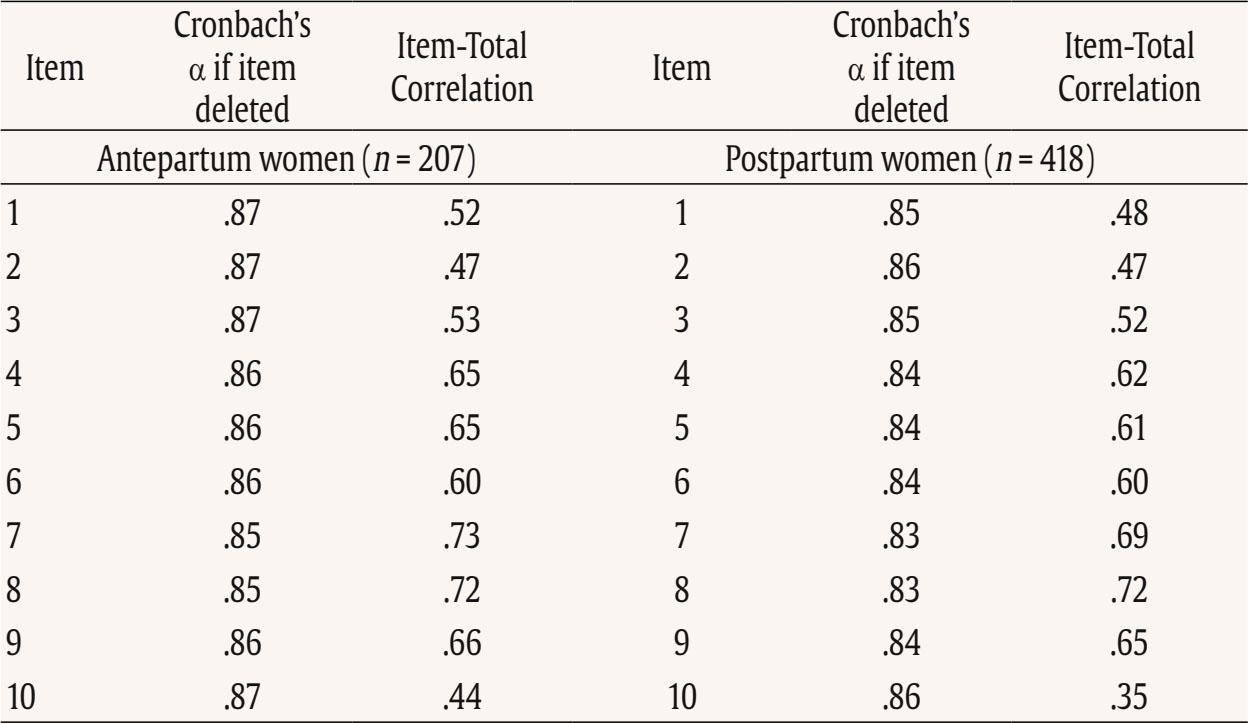 Note. Item 1: “I have been able to laugh and see the funny side of things”; Item 2: “I have looked forward with enjoyment to things”; Item 3: “I have blamed myself unnecessarily when things went wrong”; Item 4: “I have been anxious or worried for no good reason”; Item 5: “I have felt scared or panicky for no very good reason”; Item 6: “Things have been getting on top of me”; Item 7: “I have been so unhappy that I have had difficulty sleeping”; Item 8: “I have felt sad or miserable”; Item 9: “I have been so unhappy that I have been crying”; Item 10: “The thought of harming myself has occurred to me.” Table 10 Internal Consistency of the EPDS Subscales 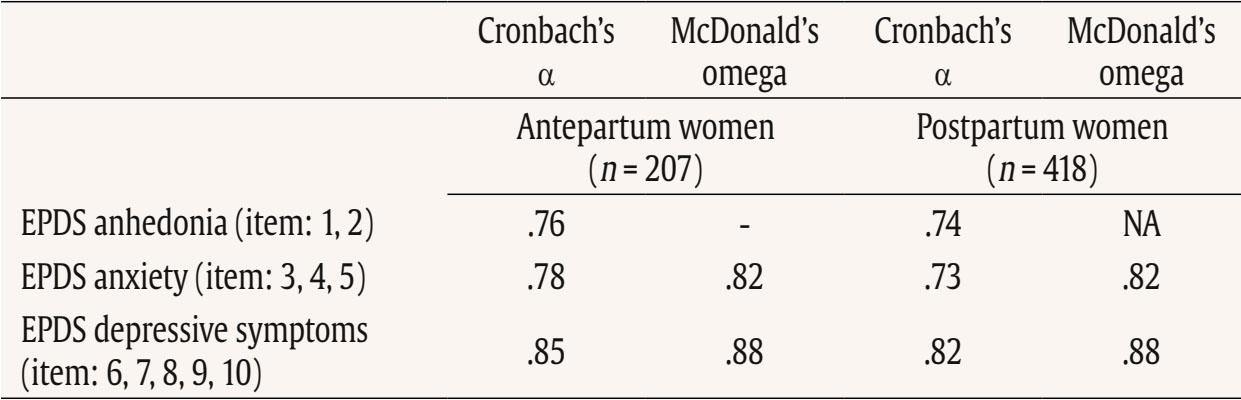 Note. NA = not applicable. Convergent Validity Convergent validity of the EPDS was tested via correlations with trauma symptoms (IES-R, CITY BiTS) and anxiety symptoms (GAD-7) as these constructs are conceptually and empirically related to perinatal depression and are known to co-occur. The EPDS total score and all subscales correlated significantly with trauma and anxiety symptoms (Table 11). Table 11 Divergent Validity of the EPDS 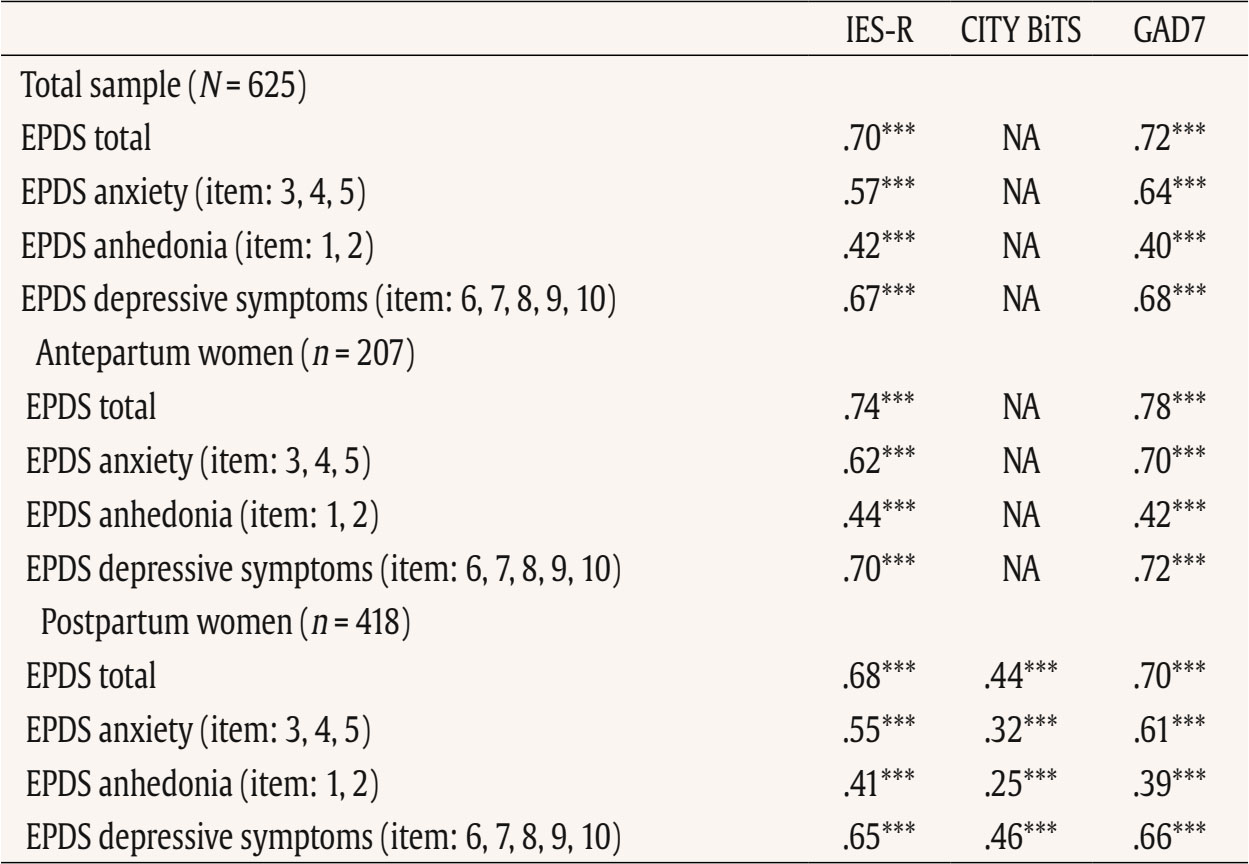 Note. NA = not applicable. ***p < .001. The Average Results in EPDS for Antepartum and Postpartum Women Postpartum women achieved statistically significantly higher average scores both in the overall EPDS result and in each dimension of the scale (see Table 12). Table 12 Analysis of the Differences between the Average Results in EPDS for Antepartum and Postpartum Women  This study details the validation of the Edinburgh Postnatal Depression Scale, specifically designed to measure PD, on a population of perinatal women (separately for antepartum and postpartum women) in Ukrainian language. Consistent with other language versions, the Ukrainian EPDS was found to be a reliable and valid instrument for both samples. Regarding the first hypothesis we found that the 3-factor structure model of the EPDS (anhedonia, anxiety, and depression) is the best-fitting model for both samples. Similar conclusion was found also in Branquinho et al. (2022), Lautarescu et al. (2022), and Song et al. (2024) studies as well as in earlier studies conducted by Tuohy and McVey (2008), Kubota et al. (2014), and Lau et al. (2010). Our results add to the growing evidence suggesting that the Edinburgh Postnatal Depression Scale (EPDS) is not a unidimensional measure of perinatal depression, but has a multifactor structure. This multifactor structure can more accurately identify different dimensions of postnatal depression, such as anxiety, anhedonia, and depression, what can allow a more nuanced understanding of a patient’s symptoms, which can lead to better-targeted interventions and treatments (Branquinho et al., 2022). Identifying profiles of women with PD symptoms according to the EPDS factors allows us to understand the distinct paths of development of postnatal depression. Additionally, as most psychological interventions are designed to decrease negative affect rather than increase positive affect (Sandman & Craske, 2022), and are largely ineffective for reducing anhedonia. The anhedonia subscale allows monitoring the severity of these symptoms and tracking the progress of interventions. Next, related to the second hypothesis, the results revealed that the Ukrainian validation of EPDS exhibits excellent internal consistency for the overall scale and good internal consistency for its subscales in both samples. As was stated in the third hypothesis, we found a strong correlation between the EPDS and CITY BiTS, IES-R and GAD-7 scales, indicating the appropriate convergent validity of the tool. These findings are in line with other studies that highlight the strong link and frequent co-occurrence of depression, anxiety and trauma experiences (Agius et al., 2016; Kurapov et al., 2023; Shevlin et al., 2018). The EPDS score in our sample was relatively high with the average results of 10 points for prenatal and 11.55 for postpartum women. These results are also in line with other studies observing high rates of depression in war-affected Ukraine among civilians (Kurapov et al., 2023; Seleznova et al., 2023; Shevlin et al., 2018) and perinatal mothers (Korchinska et al., 2022; Savrun et al., 2024; Zhabchenko et al., 2018). This finding is consistent with other research conducted during war (Klapper-Goldstein et al., 2024) among Israeli women, where the prevalence of PD symptoms doubled in comparison with before war conditions. Mohammed et al. (2018) and Roumieh et al.’s, (2019) studies among war-affected Syrian postpartum mothers showed also similar results. We hypothesize that the high scores of depressive symptoms could have been impacted by the real threats to women’s and their families’ well-being and daily war-related stressors, such as missile alarms, electricity shortages, and current or anticipated separation from loved ones, as well as challenges related to external or internal displacement and daily burden. Overall, the severity of depressive symptoms is higher in Ukrainian women compared to those living through other societal crises, such as the COVID-19 pandemic (Costa et al., 2023). Postpartum women scored significantly higher than pregnant women on total and subscale EPDS scores and our separate analyses suggest that these differences reflect variations in symptom intensity rather than differences in the underlying construct measured by the scale. This is in line with previous findings indicating that the percentage of women experiencing depression in the postpartum period is higher than during pregnancy (Mateus et al., 2022; Wang et al., 2021). Evidence shows that the war context changes the situation of mothers both during the prenatal and the postpartum period. Studies have elaborated on the challenges of new mothers during birth, for example as Shlemkevytch et al. (2024, p. 18) study described: “In cities where active hostilities are taking place or where there may be air strikes, or air alarms, hospitals are forced to use basements to protect mothers with newborns.” As the number of wars increases and the growing body of research highlights the importance of caregiver mental health in predicting the developmental outcomes of war-affected children (Betancourt & Khan, 2008; Meyer et al., 2017; Tol et al., 2013), the need for immediate support is vital. The first step is identification followed by the clarification of the results to the mother and referral. Although the Ukrainian validation of EPDS was done during the war, the psychometric properties are comparable to other countries indicating that it may be an important tool in helping to identify the affected mothers. We are aware that in war situations, fear, anger, sadness, and stress associated with constant mobilization may also play an important, adaptive role in being vigilant to possible threats and are also the natural part of the grief reaction. Additionally, Ukrainian families are not only exposed to war-related violence, but they also have to cope with many additional challenges such as lack of water supply, sanitation and hygiene in front-line cities, electricity shortages, financial restrictions, multiple losses and limited or diminished due to the constant stress, interpersonal resources in families. In case of refugee, war-affected mothers, we underscore the importance of advocating for mother-centered models that address their unique needs in the broader community, social, and cultural context. The possibility of screening in the native language seems important for war refugees. It would be worthwhile to include the Ukrainian version of the EPDS in countries where PD screening is mandatory. When screenings are not obligatorily performed by midwives, for example, during patronage visits or pregnancy, it is important to raise awareness among health professionals working with refugees about the increased risk of perinatal mental health problems. It is imperative for policymakers and healthcare professionals to recognize the risk and prevalence of depressive symptoms among pregnant women and mothers, and to investigate in more detail and understand its enduring consequences. The identification of affected mothers, now possible with the validation of the Ukrainian version of the Edinburgh Postnatal Depression Scale, is the first step toward recognizing and offering appropriate interventions in Ukraine as well as in host countries. Even though the war situation or language barriers in host countries may hinder access to psychological assistance, one way to obtain help is through programs like iFightDepression – self-help, online and cognitive-behavioral therapy based tool available also in Ukrainian language, which has proven effective in cases of mild to moderate depression (Varga et al., 2024). Limitations This study comes along with several strengths. The procedure followed the Standards for Educational and Psychological Testing (American Educational Research Association, American Psychological Association, & National Council on Measurement in Education, 2014). It includes a large sample of pregnant and postpartum Ukrainian women. The factor structure of the EPDS was examined in groups of postpartum and pregnant women. The results confirmed that the factor structure and reliability indices were highly comparable, supporting the use of the EPDS in both populations. Despite these strengths, the study has some limitations as well. The data collection occurred during the ongoing Ukrainian-Russian war, which may affect the generalizability of the results to the Ukrainian population of pregnant and postpartum women in no war periods. The online recruitment of participants limits the sample to those who use technology and social media (however, the selected social platforms are among the most popular worldwide), and the majority of respondents were well-educated and financially stable, which may not represent other social groups, groups at risk and vulnerable groups. We acknowledged that the underrepresentation of participants from less privileged social groups or rural areas, as well as the potential effects of socioeconomic status, geographic location, and internet accessibility may have significant importance for generalizability of our conclusions. On the other hand, Bowling (2005) reported that the difference in setting: online anonymous versus clinical environment may influence results, as the anonymity offered by the online environment could increase participants’ willingness to disclose sensitive or perceived as shameful information. A lot of efforts were made to promote the survey in refugee help centers and in different locations. Additionally, the participants were able to return to the survey in case of the electricity or wifi disconnection. A technical issue prevented recording the participants’ age which did not allow us to analyze age-related trends. Although the three-factor solution was supported by the data, the anhedonia subscale contains only two items, which may limit its psychometric robustness, but factor structure with 2-item subscale is similar to other studies and widely used (Lautarescu et al., 2022; Tuohy & McVey, 2008; Yang et al., 2025). No other depression-specific tool (e.g., BDI-II or CES-D) has been used which precludes a direct assessment of convergent validity with parallel measures, but the correlations with GAD-7, IES-R, and City BiTS already provide partial evidence of convergent validity within the broader domain of negative affect. The divergent validity was not evaluated, so it is recommended for future research to involve unrelated constructs to assess divergent validity more rigorously. Additionally, no clinical diagnostic interview was conducted to establish a diagnosis of major depression according to DSM-V or ICD-11 which made it impossible to establish sensitivity, specificity, positive predictive value and optimal cut-off points for clinical or research work. Due to the fact that across studies, and in particular across languages, the optimal cutoff scores of the EPDS have varied considerably, a clinical interview confirming the result of the screening test using the questionnaire is recommended. Our study was conducted in the first and early second year of the war, in a situation of frequent relocation and problems with electricity, organizing clinical interviews would have been very difficult to carry out. Since this study used self-reported data, it was not possible to rule out subjective bias and discrepancies between declarations and actual behavior, which may limit the generalizability of the conclusions. Social desirability bias may have influenced the results, as some women might have been reluctant to disclose socially unpopular feelings and psychological health issues. We highly recommend that future research conducted on the Ukrainian population of perinatal women include comprehensive diagnostic interviews and clinical assessments of mental health and psychiatric history, as well as quantitative screening measures for depression and anxiety. Potential differences in optimal cut-off points for pregnant and postpartum women should be further examined in future research, as this has clear implications for clinical practice. Moreover, future studies with larger and more balanced samples could formally test measurement invariance through multi-group CFA, which would provide a more rigorous evaluation of cross-group equivalence. The Ukrainian version of the EPDS demonstrates high reliability and can effectively screen for depression during pregnancy and the postpartum period. The identification of affected mothers, now possible with the validation of the Ukrainian version of the Edinburgh Postnatal Depression Scale, is the first step toward recognizing and offering appropriate interventions. Three factor structure has several advantages. It enables better diagnostics, greater accuracy taking into account the diversity of symptoms and their severity and individualized therapy. Especially in war zones with limited resources, we see the potential to use the EPDS to screen for both anxiety and depression. The EPDS screening carried out under war conditions should be followed by an in-depth clinical interview to understand the severity and prevalence of the symptoms as the result of war-related stress exposure or more clinical picture of depressive episodes. Under such conditions, however, proper support and interventions are recommended. Considering the fact that armed conflicts have severe and prolonged psychological impact on surviving citizens, it is imperative for policymakers and healthcare professionals to recognize the risk and prevalence of depressive symptoms among pregnant women and mothers affected by war and offer adequate intervention. The Ukrainian validation of the EPDS allows Ukraine to be included in European and global research focusing on the perinatal mental health. It is an important step in integrating Ukrainian scientists and practitioners with those from countries where the EPDS and its validation were previously available. European cooperation can help implement screening and intervention programs that are important in every country, but may have additional significance especially in a country affected by armed conflict. Conflict of Interest The authors of this article declare no conflict of interest. Acknowledgments We would like to thank to all Ukrainian women who have participated in the study and were eager to share their experience in this extremely difficult war situation which affected their lives and their country. Note According to the European Commission of Migration and Home Affairs: a person or groups of persons who has been forced or obliged to flee or to leave their homes or places of habitual residence, in particular as a result of or to avoid the effects of armed conflict, situations of generalised violence, violations of human rights or natural or human-made disasters, and who have not crossed an internationally recognised State border. This article has been promoted by COST ACTION: CA18138 - Research Innovation and Sustainable Pan-European Network in Peripartum Depression Disorder (Riseup-PPD). Cite this article as: Chrzan-Dtko, M., Liakea, I., Murawska, N., Costa, R., Uka, A., Krupelnytska, L., Vavilova, A., García-López, H. S. & Morozova-Larina, O. (2026). Validation of Edinburgh postnatal depression scale (EPDS) in perinatal women under war conditions in Ukraine. Clinical and Health, 37, Article e260717. https://doi.org/10.5093/clh2026a6 References |
Cite this article as: Chrzan-Dętkoś, M., Liakea, I., Murawska, N., Costa, R., Uka, A., Krupelnytska, L., Vavilova, A., García-López, H. S., & Morozova-Larina, O. (2026). Validation of Edinburgh Postnatal Depression Scale (EPDS) in Perinatal Women under War Conditions in Ukraine. Clinical and Health, 37, Article e260717. https://doi.org/10.5093/clh2026a6
Correspondence: Magdalena.chrzan-detkos@ug.edu.pl (M. Chrzan-D tko ).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
Clinical and Health is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License








