


Weight Control and Healthy Eating: Cross-cultural Invariance of Self-efficacy, Motivation, and Perceived Barriers
[El control del peso y la alimentaciĂłn saludable: la invarianza transcultural de la autoeficacia, la motivaciĂłn y las barreras percibidas]
María Marentes-Castillo, Isabel Castillo, Inés Tomás, & Octavio Álvarez
University of Valencia, Spain
https://doi.org/10.5093/clh2026a7
Received 16 December 2024, Accepted 7 October 2025
Abstract
Weight control and healthy eating can be assessed with instruments that measure constructs such as self-efficacy, motivation, and perceived barriers, contributing to a better understanding of the underlying psychosocial processes. This study examined the psychometric properties and cross-cultural invariance of three instruments: Healthy Eating and Weight Self-efficacy (HEWSE), Behavioral Regulation in Exercise Questionnaire (BREQ-3) adapted to weight control, and Barriers to Healthy Eating (BHE).
The sample included 1,045 Mexican and Spanish students (Mage = 16.67, SD = 1.37). Invariance, descriptive, and correlation analyses were conducted.
Structural, metric, scalar and strict invariance were supported for all three instruments. Significant cross-cultural differences emerged, with Mexican students showing stronger negative associations between HEWSE and both daily mechanism and social support perceived barriers, and between autonomous motivation and daily mechanism perceived barriers.
The Mexican and Spanish versions of the instruments demonstrated adequate psychometric properties, supporting their use in cross-cultural research.
Resumen
El control de peso y la alimentación saludable pueden evaluarse de manera eficaz mediante instrumentos psicosociales que tengan propiedades psicométricas adecuadas. Estas herramientas permiten una medición fiable de constructos clave, como la autoeficacia, la motivación y las barreras percibidas, lo que contribuye a un mejor conocimiento de los procesos psicosociales implicados. Este estudio tuvo como objetivo evaluar las propiedades psicométricas y la invarianza factorial transcultural de tres instrumentos: la Autoeficacia para una Alimentación Saludable y para el Control del Peso (HEWSE), el Cuestionario de Regulación Conductual para el Control del Peso (BREQ-3), y el Cuestionario sobre las Barreras para una Alimentación Saludable (BHE)).
La muestra incluyó 1,045 estudiantes mexicanos y españoles (Medad = 16.67, DT = 1.37). Se realizaron análisis de invarianza y análisis descriptivos y de correlación.
Se confirmó la invarianza estructural, métrica, escalar y estricta de los tres cuestionarios, encontrándose diferencias transculturales significativas, con asociaciones negativas más fuertes en la muestra mexicana entre la HEWSE tanto en los mecanismos diarios, como las barreras percibidas del apoyo social y entre la motivación autónoma y las barreras percibidas de los mecanismos diarios.
Las versiones mexicana y española de los tres instrumentos mostraron propiedades psicométricas adecuadas, lo que los hace idóneos para su uso en la investigación transcultural.
Palabras clave
Control de peso, AlimentaciĂłn saludable, Autoeficacia, MotivaciĂłn, Barreras percibidasKeywords
Weight control, Healthy eating, Self-efficacy, Motivation, Perceived barriersCite this article as: Marentes-Castillo, M., Castillo, I., Tomás, I., & Álvarez, O. (2026). Weight Control and Healthy Eating: Cross-cultural Invariance of Self-efficacy, Motivation, and Perceived Barriers. Clinical and Health, 37, Article e260721. https://doi.org/10.5093/clh2026a7
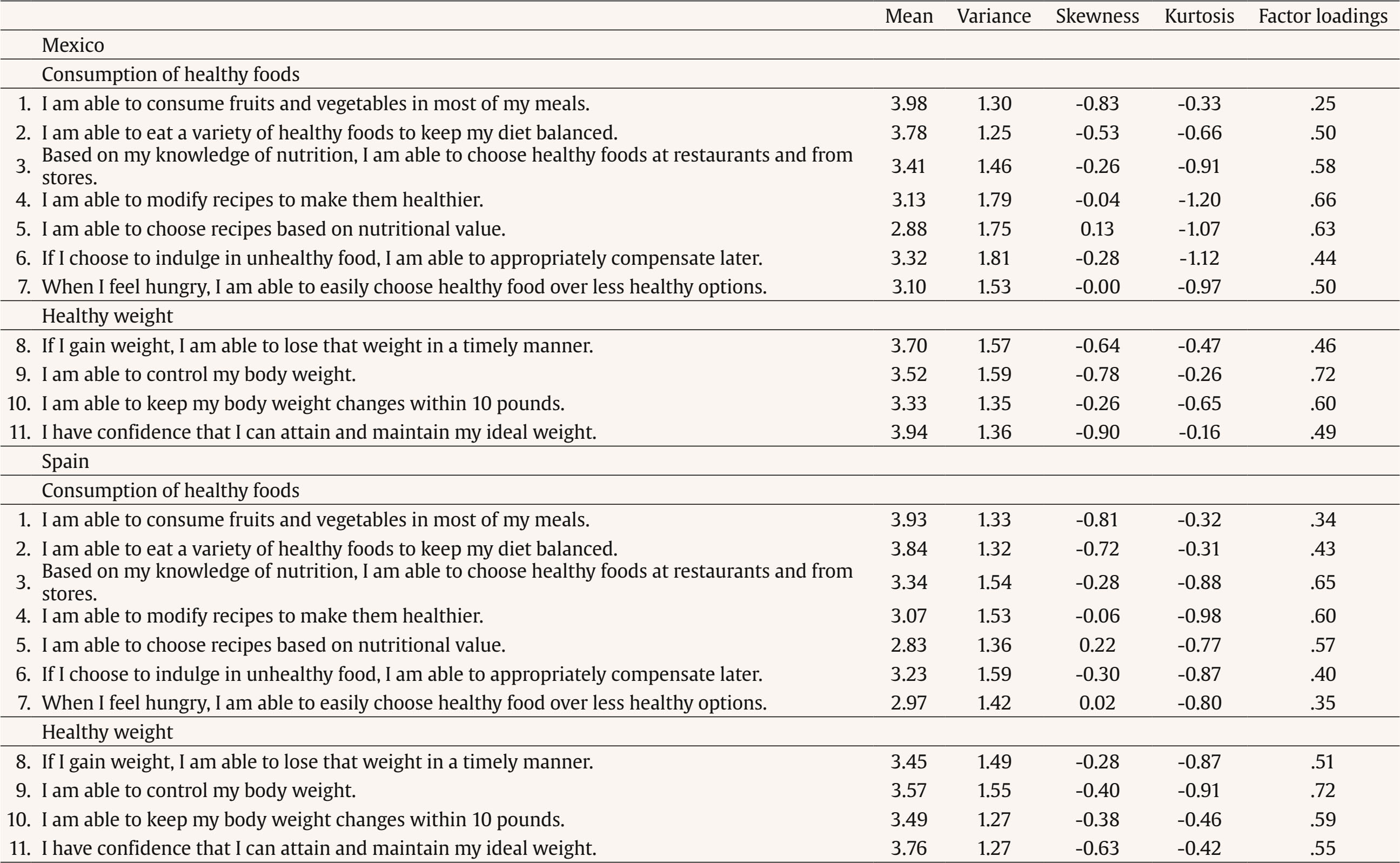
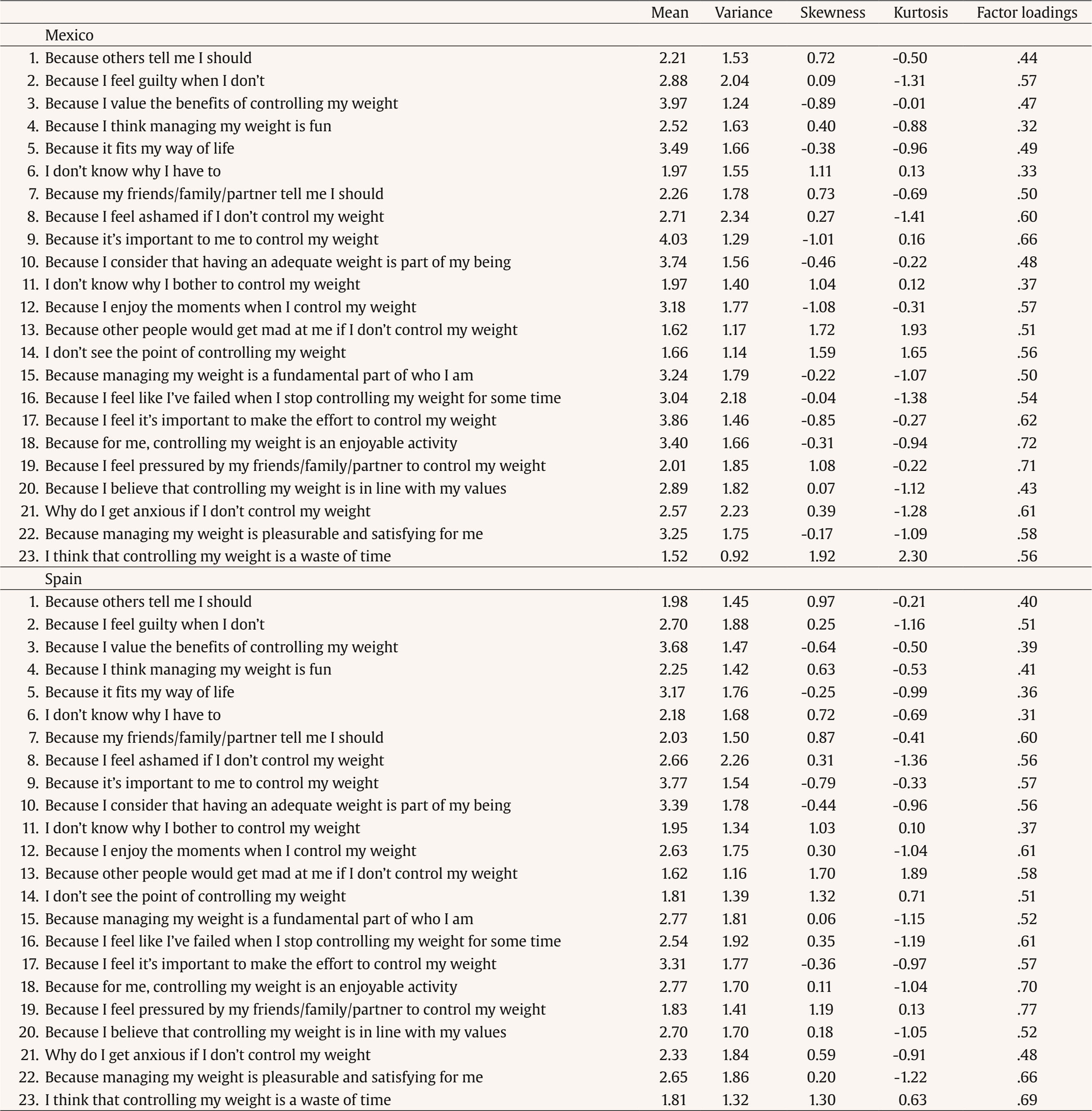
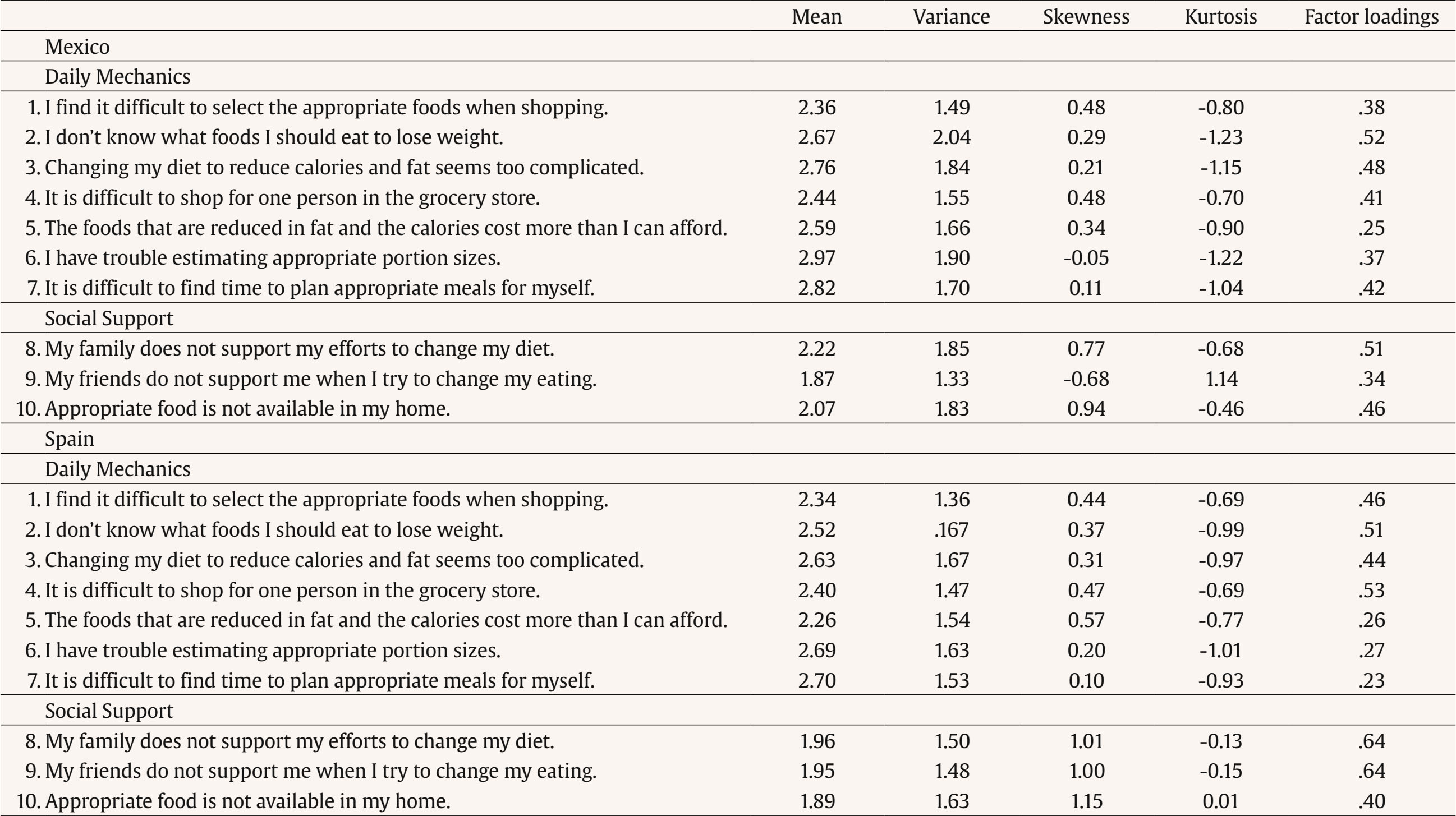
Correspondence: Ines.Tomas@uv.es (I. Tomás)., Correspondence: Ines.Tomas@uv.es (I. Tomás).Research has shown that successful weight loss maintainers have made significant changes in their lifestyles, despite being in obesogenic environments (Phelan et al., 2009; Teixeira et al., 2012). These improvements have been associated with new forms of lifestyle, new goals, motives, emotional responses, habits, etc. (e.g., Fuglestad et al., 2012; Silva et al., 2011), highlighting the need to focus research at an individual level to understand why, how, and under what conditions children, adolescents, and adults can remain overweight and obese (Teixeira et al., 2012). In 2022, 390 million children and adolescents aged 5-19 years were overweight (of these, 160 million were obese) (World Health Organization [WHO, 2024]). Recent studies continue to highlight the importance of psychosocial variables that directly and indirectly impact weight regulation and healthy eating behavior (see Marentes-Castillo et al., 2024; Marentes-Castillo et al., 2022a, 2022b). To this end, instruments have been constructed and adapted with the aim of exploring variables such as self-efficacy (e.g., Salado et al., 2022; Wilson-Barlow et al., 2014), motivation (e.g., Ryan & Connell, 1989; Wilson et al., 2006), and perceived barriers (e.g., Jeffery et al., 1993; Sun et al., 2019). Exploring their various associations requires valid measurement instruments that can ensure theoretical/practical congruence with reality (Goméz-Peresmitré et al., 2021). Additionally, the underlying concept reflected by the scales must be consistent across all groups (Norman et al. 2021). It is thus necessary to perform analyses to ascertain whether the various translated and adapted versions of the instruments in question measure the same underlying factors, as well as to determine the invariance of item parameters between cultural groups (Tomás et al., 2014). The performance of measurement invariance analyses is regarded as a crucial step in ensuring the validity of an instrument (Putnick & Bornstein, 2016; Vandenberg & Lance, 2000). Despite the development of numerous instruments designed to examine a range of variables associated with healthy behavior, few have been tested for consistent properties across different cultural groups. This observation motivates the primary objective of the present study, which is to analyze the measurement invariance of three instruments assessing psychosocial variables (self-efficacy, motivation, and perceived barriers) associated with healthy eating and weight control, between Mexican and Spanish cultures, where overweight and obesity represent significant public health concerns (Goméz-Peremistré et al., 2021; Marentes-Castillo et al., 2024). Self-efficacy in healthy behavior has been defined as an individual’s belief in one’s ability to engage in a specific behavior, for example, healthy consumption and weight regulation (Bandura, 1995; Wilson-Barlow et al., 2014). Given the association of self-efficacy with weight control and eating-related behaviors (e.g., Marentes et al., 2024), different instruments have been developed, such as the Eating Self-efficacy Scale (ESES; Glynn & Ruderman, 1986), Eating Self-efficacy, a brief parental self-efficacy scale (Norman et al., 2021), the Perceived Self-efficacy Scale for the prevention of obesity in pre-adolescents (SE-HEPA; Gómez-Peresmitré et al., 2021), a brief scale (Lombardo et al., 2021) and the Healthy Eating and Weight Self-efficacy for adolescents and adults (HEWSE; Wilson-Barlow et al., 2014). The latter scale is the one we will analyze in the present study. Similarly, motivational factors underlying healthy behavior may be critical in the prevention of overweight and obesity (Cohen, 2008; Morrison & Berthoud, 2007). The Self-determination Theory (Ryan & Deci, 2017) posits that the type of motivation (autonomous, controlled, and amotivated) can explain how a person may initiate, regulate, and sustain behaviors such as healthy eating (Marentes-Castillo et al., 2022a, 2022b; Silva et al., 2011; Teixeira et al., 2006). The proliferation of research to learn about the association between types of motivation and healthy behavior can be credited to the development of instruments that have made it possible to quantify these relationships (Guérin et al., 2012). To measure the types of motivation, several adaptations of Ryan and Connell’s (1989) Perceived Locus of Causality (PLOC) inventory have been used towards the context of diet treatment and exercise (Levesque et al., 2007; Marentes-Castillo et al., 2019; Mata et al., 2019), with the purpose of exploring the different regulations of motivation (intrinsic, integrated, identified, introjected, external, and non-motivational regulation). On the other hand, the Behavioral Regulation in Exercise Questionnaire (BREQ-3; Wilson et al., 2006) adapted to weight control has also been used (Marentes-Castillo et al., 2022, 2022b); as a matter of fact, the latter is the one we will analyse in this study. In addition to the study of self-efficacy and motivation, it is essential to identify and assess the barriers that may hinder adherence in maintaining healthy behavior (Sun et al., 2019). Jeffery et al. (1993) developed the Barriers to Healthy Eating scale (BHE), which assesses the emotional factor (individual barriers), daily mechanisms (external barriers), and social support (social barriers). This scale has been modified in recent years to propose shorter versions, such as Sun et al.’s (2019), though no invariance analyses have been performed for this scale. In this study, we will evaluate the daily mechanisms and social support subfactors of the BHE. To sum up, the general objective of this study was to evaluate the measurement invariance of three psychosocial instruments (the Healthy Eating and Weight Self-efficacy scale, the Behavioral Regulation to Weight Control questionnaire, and the Barriers to Healthy Eating scale) across country, using samples of adolescents from Mexico and Spain. Additionally, we sought to provide evidence of the validity of the theoretical associations between the subfactors of the variables studied and any potential differences between the Mexican and Spanish samples. Participants A total of 1,045 adolescents from Mexico (n = 719) and Spain (n = 326) participated in the study (60% were female). The participants ranged in age from 15 to 19 years (M = 16.67, SD = 1.37) and were selected through non-probability cluster sampling in different schools in Mexico and Spain. Following Kline’s (2016) recommendation that a minimum of 200 participants is generally required to obtain reliable and stable solutions in confirmatory factor analysis (CFA), our sample size was adequate, as both groups exceeded this recommend threshold. Instruments The Healthy Eating and Weight Self-efficacy (HEWSE; Wilson-Barlow et al., 2014) This was used in its Spanish version (Marentes-Castillo et al., 2024). This scale measures the belief about the abilities to engage in healthy eating with 11 items on a Likert-type scale from 1 (strongly disagree) to 5 (strongly agree). It measures two dimensions: self-efficacy toward healthy consumption (7 items; “I am usually able to eat fruits and vegetables at most of my meals”) and toward maintaining a healthy weight (4 items; “I am usually confident that I can reach and maintain my ideal weight”). The Behavioral Regulation in Exercise Questionnaire (BREQ-3) It is adapted to weight control (Wilson et al., 2006) was administered in its Spanish version (Marentes-Castillo et al., 2022a, 2022b). This questionnaire measures the type of motivation regulations towards weight control behavior with 23 items on a Likert-type scale from 0 (not at all true) to 4 (completely true). It measures three motivational regulations: autonomous motivation (11 items; e.g., “because controlling my weight is accord to my values”) including intrinsic, integrated, and identified subdimensiones; controlled motivation (8 items; e.g., “because others tell me I should do it”), including introjected and external regulation; and amotivation (4 items; e.g., “I find that controlling my weight is a waste of time”). The Barriers to Healthy Eating (BHE; Sun et al., 2019) Aadapted to the Spanish version (Marentes-Castillo et al., 2024), the BHE was used. This scale measures frequent perceived barriers to healthy eating and weight control with 22 items on a Likert-type scale from 1 (not a problem at all) to 5 (a very important problem). Of the 22 items we have used only 10 items which refer to the following two dimensions: Daily Mechanisms factor (7 items; e.g., “I find it difficult to select the right foods when shopping”), and Social Support (3 items; e.g., “my family does not support my efforts to change my diet/eating”). Statistical Analysis In order to evaluate the instruments’ measurement equivalence across countries, a series of multi-sample confirmatory factor analyses (CFA) was performed using MPlus 8.0. (Muthén & Muthén, 1998-2017). Since there was normality in the data, maximum likelihood estimation was used. The skewness and kurtosis values for all items were within the acceptable range (± 2) supporting the adequacy of the normality assumption (Bandalos & Finney, 2010). Before proceeding on to multi-sample analyses, the a priori factor structure was fitted separately in the Mexican (M0a) and Spanish (M0b) subsamples. Next, a set of four nested models tested different levels of restricted equivalence between the groups: the Structural Invariance model (M1) addressed the equality of the number and pattern of factor loadings between groups and was used as the base model for fit comparisons with the subsequent, more restricted models; the Metric Invariance model (M2) tested the invariance of factor loadings across groups; the Scalar Invariance model (M3) tested both factor loadings and intercepts invariance across groups; and finally, the Strict Invariance model (M4) tested the invariance of factor loadings, intercepts, and measurement errors (Byrne et al., 1989; Muthén & Muthén, 1998-2017). Model fit was evaluated using the χ2 statistic, the root mean square error of approximation (RMSEA), the normalized root mean square residual (SRMSR), the comparative fit index (CFI), and the Tucker-Lewis index (TLI). The interpretation of these indexes is as follows: for RMSEA and SRMSR, values below .05 indicate a close fit, while values below .08 indicate a reasonable fit (Browne & Cudeck, 1993; Hu & Bentler, 1999); for CFI and TLI, values above .90 and .95 are typically taken to indicate acceptable and excellent fit, respectively (Marsh et al., 2005). We considered an invariance hypothesis to be tenable if: (a) the model specifying the hypothesis demonstrated a practical fit and (b) the differences in RMSEA, CFI, and TLI values between this model and the unconstrained model were negligible (≤ .015 for RMSEA; Chen, 2007), and ≤ .01 for CFI and TLI (Cheung & Rensvold, 2002; Widaman, 1985). The percentage of missing data was found to be below 5% (Graham & Hofer, 2000), which is an acceptable level for the purposes of analysis. Descriptive analyses, Pearson’s correlation and Cronbach’s alpha were performed for all subscales. Furthermore, Fisher’s z-test was employed to examine the differences between the correlations observed in both countries. Procedure This study was conducted in accordance with the ethical guidelines established by the American Psychological Association and in alignment with the standards outlined in the Declaration of Helsinki. All procedures involving the participants in the research study were approved by the Commission on Ethics in Experimental Research of the University of Valencia (Ref. 1707311). A request was submitted to educational centers in Mexico and Spain asking for authorisation to collect data online from adolescents between the ages of 15 and 19 who were enrolled during the academic year. The data collection took place from March to June 2022 via online Google Forms. Prior to data collection, a real-time connection was established to provide participants with a detailed explanation of the procedure to be followed, accompanied by the presence of the teacher responsible for the school group. The questionnaire completion lasted around 15-20 minutes. Students were required to provide informed consent, and participation was voluntary and anonymous. Prior to the invariance analysis, CFAs were conducted separately for each group (Mexico, M0a; Spain; M0b; see Tables 1 to 3). All models showed adequate fit for the three scales when tested within each country. The baseline model (M1) was then specified to test structural invariance, followed by increasingly constrained models to evaluate metric (M2), scalar (M3) and strict (M4) invariance (see Tables 1 to 3). Table 1 Goodness of Fit Indices for Tested Invariance Models across Country for the HEWSE Scale  Note. HEWSE = healthy eating and weight self-efficacy; df = degrees of freedom; SB = Satorra-Bentler; RMSEA = root mean square error of approximation; 90% CI = 90% confidence interval for the RMSEA; SRMR = standardized root mean square residual; TLI = Tucker-Lewis index; CFI = comparative fit index; comparisons based on incremental fit indices (ΔRMSEA, ΔTLI, and ΔCFI) are made with respect to the structural model (M1). Table 2 Goodness of Fit indices for Tested Invariance Models across Country for the BREQ-3 Adapted to Weight Control  Note. BREQ = behavioral regulation in exercise questionnaire; df = degrees of freedom; SB = Satorra-Bentler; RMSEA = root mean square error of approximation; 90% CI = 90% confidence interval for the RMSEA; SRMR = standardized root mean square residual; TLI= Tucker-Lewis index; CFI = comparative fit index; comparisons based on incremental fit indices (ΔRMSEA, ΔTLI, and ΔCFI) are made with respect to the structural model (M1). Table 3 Goodness of Fit Indices for Tested Invariance Models across Country for the BHE Scale  Note. BHE = barriers to healthy eating; df = degrees of freedom; SB = Satorra-Bentler; RMSEA = root mean square error of approximation; 90% CI = 90% confidence interval for the RMSEA; SRMR = standardized root mean square residual; TLI= Tucker-Lewis index; CFI = comparative fit index; comparisons based on incremental fit indices (ΔRMSEA, ΔTLI, and ΔCFI) are made with respect to the structural model (M1). Measurement Invariance Results in Table 1 for the HEWSE scale indicate that structural (M1), metric (M2), scalar (M3), and strict (M4) invariance models showed acceptable practical fit. Moreover, using M1 as a baseline to evaluate the following more restrictive models, comparison of incremental RMSEA (ΔRMSEA), TLI (ΔTLI), and CFI (ΔCFI) values provided support for metric, scalar and strict invariance. Thus, invariance of factor loadings, intercepts, and measurement errors across countries was supported for the HEWSE. The invariance models for the BREQ-3 adapted to weight control (Table 2) showed non relevant differences in RMSEA (ΔRMSEA) and TLI (ΔTLI) values between the baseline model (M1) and the successive invariance models, supporting metric (M2), scalar (M3), and strict (M4) invariance across countries for this scale. Although ΔCFI supported only metric invariance across countries, the convergence of evidence from two out of the three criteria indicates that measurement invariance across countries can reasonable be assumed, even if the findings are not fully conclusive. For the BHE scale (Table 3), the invariance analyses indicated that differences in RMSEA and TLI values between the baseline model (M1) and the subsequent models were not relevant, thereby supporting metric (M2), scalar (M3), and strict (M4) invariance. These results suggest invariance of factor loadings, intercepts, and measurement errors across countries for this scale. In contrast, the ΔCFI criterion only supported metric invariance, as it showed negligible differences for M2, but relevant differences for M3 (scalar invariance) and M4 (strict invariance). Nevertheless, given that two of the three fit indices consistently favored invariance at all levels, we consider that the assumption of cross-country invariance for the BHE scale is reasonably sustained, even though the lack of CFI support prevents a fully conclusive statement. Descriptive Statistics and Reliability The descriptive statistics (mean, standard deviations, skewness, and kurtosis) and Cronbach’s alpha values for the subscales of the three tested questionnaires are presented in Table 4. All subscales showed adequate reliability in both countries. Table 4 Descriptive Statistics and Reliability of the Subscales of the Study Questionnaires in Mexico and Spain  Note. 1 = self-efficacy toward healthy consumption, 2 = self-efficacy toward maintaining a healthy weight, 3 = autonomous motivation, 4 = controlled motivation, 5 = amotivation, 6 = barriers to daily mechanism, 7 = barriers to social support; healthy eating and weight self-efficacy (HEWSE) include scales 1 and 2; behavioural regulation in exercise questionnaire (BREQ-3) adapted to weight control include scales 3 to 5; barriers to healthy eating (BHE) include scales 6 and 7. M = mean; SD = standard deviation; Sk = skewness; K = kurtosis; α = Cronbach’s alfa coefficient. Evidence of Validity Based on Relationship with other Variables Table 5 shows that all the significant associations between the study variables are in line with theoretical expectations. However, the results show significant differences across countries in the negative association between self-efficacy of healthy consumption and barriers to daily mechanisms, with a stronger relationship in the Mexican sample. In addition, significant differences were found in the relationship between self-efficacy toward maintaining a healthy weight and social support barriers, and between autonomous motivation and barriers to daily mechanism, with a negative and statistically significant relationship only in the Mexican sample. Table 5 Correlations among the Subscales and Differences across Country 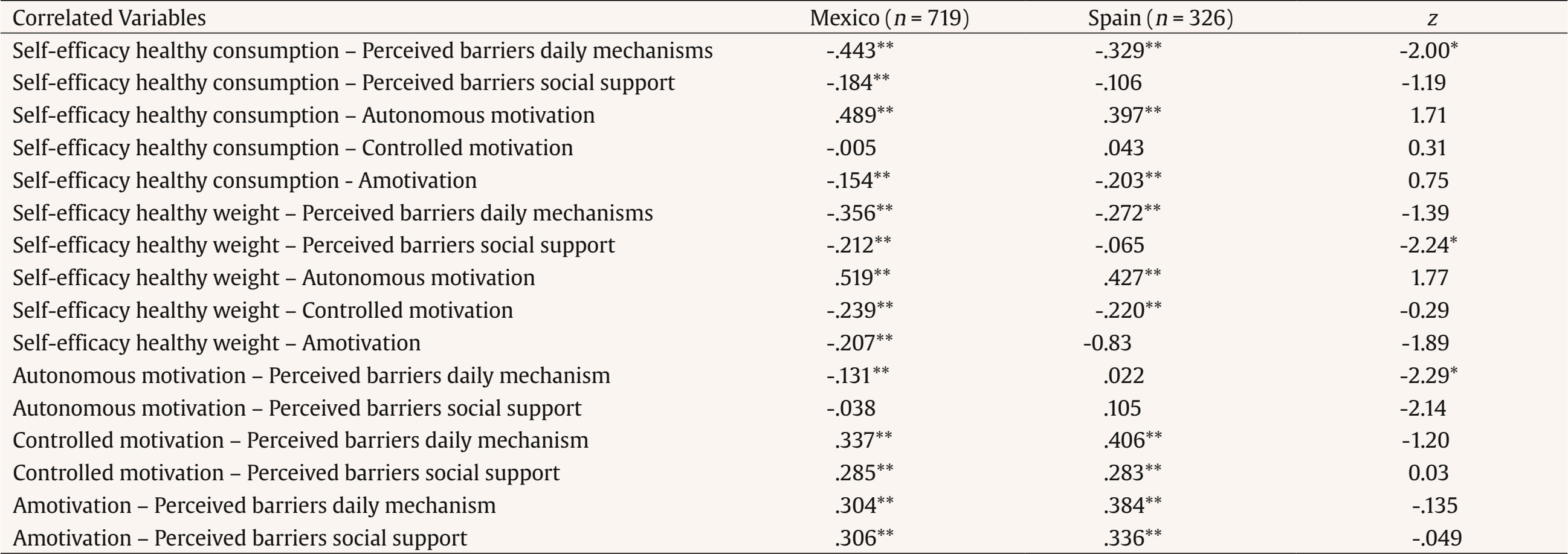 Note. Healthy eating and weight self-efficacy (HEWSE) include self-efficacy healthy consumption and self-efficacy healthy weight; behavioral regulation in exercise questionnaire (BREQ-3) adapted to weight control include autonomous motivation, controlled motivation and amotivation; barriers to healthy eating (BHE) include perceived barriers daily mechanism and perceibed barriers social support. *p < .05, **p < .01. The main objective of the current study was to evaluate the measurement invariance across country of three psychosocial instruments in adolescents from Mexico and Spain. In addition, the relationships between the subscales of the questionnaires were obtained as evidence of validity of the instruments studied and differences across countries were tested. Overall, the HEWSE scale, the BREQ-3 adapted to weight control, and the BHE questionnaire showed good psychometric properties in the Mexican and Spanish samples. Structural invariance was supported, showing that the factor structure of the questionnaires was invariant across the responses of the two groups of Mexican and Spanish adolescents. Metric invariance (invariance of factor loadings), strong or scalar factorial invariance (invariance of factor loadings and intercepts), and strict factorial invariance (invariance of factor loadings, intercepts, and measurement errors) across countries was also supported for the HEWSE scale. Our analysis of the BREQ-3 adapted to weight control and the BHE provided substantial support for measurement invariance across countries. While the DCFI criterion supported only metric invariance, both RMSEA and TLI indicated invariance at the metric, scalar, and strict levels. In line with recommendations to consider multiple criteria when evaluating invariance, we interpret these findings as reasonably strong evidence that both instruments function equivalently across cultural groups. Nonetheless, the lack of full support form CFI suggests some caution is warranted, and further research may be needed to confirm the robustness of scalar and strict invariance. These findings reinforce the cross-cultural validity of the variables self-efficacy toward healthy eating and weight regulation, motivation for weight control, and perceived barriers to healthy eating, and reinforces the potential usefulness of the three tested instruments (HEWSE, BREQ-3 adapted to weight control, and BHE) for the investigation of healthy eating behavior and weight regulation in Mexican and Spanish adolescent samples. The use of these questionnaires can help us to understand the “why” and “how” of unhealthy eating patterns and lack of body weight regulation in Mexican and Spanish youth, in turn confirming the relevance of psychosocial variables in healthy adolescent behavior (Marentes-Castillo et al., 2024; Marentes-Castillo et al., 2022a, 2022b). Furthermore, it is of great importance that those scales are useful for testing cultural differences in the measured variables across Spanish and Mexican adolescents (e.g., Norman et al., 2021; Tomás et al., 2014). The correlation analyses, as evidence of validity, indicate the theoretically expected associations between the study subscales. However, some differences were identified across countries in the relationship between healthy eating self-efficacy and perceived barriers of daily mechanisms, healthy weight self-efficacy, and social support barriers, and between autonomous motivation and perceived barriers of daily mechanisms. Mexican adolescents exhibited a higher negative association value compared to Spanish youth. In this case, self-efficacy for healthy eating and weight regulation is a pivotal variable in the adoption of healthy behaviours and weight regulation (see Marentes-Castillo et al., 2024). The findings of this study demonstrate the usefulness of the tested instruments for investigating healthy eating and weight regulation in adolescents. However, their applicability is currently limited to Mexican and Spanish youth and may not extend to other Spanish-speaking populations. Furthermore, the greater representation of Mexican participants relative to Spaniards may introduce a degree of sampling bias. In addition, cross-sectional design and reliance on self-report measures should be considered when interpreting the results, as they may influence the robustness and generalizability of the findings. Despite these limitations, the study provides a valuable foundation for future research in diverse cultural contexts. In conclusion, the current study offers preliminary support for the potential generalizability of the healthy eating and weight self-efficacy, motivation to weight control, and the barriers to healthy eating in Mexican and Spanish adolescents. This contributed to initial evidence supporting the validity of the interpretations and the cross-cultural comparability of the HEWSE scale, the BREQ-3 adapted for weight control, and the BHE scale across groups from Mexico and Spain. The development of valid instruments allows the quantification of relationships between the variables under study (Guérin et al., 2012). Consequently, more precise measurement facilitates the implementation of more effective psychosocial interventions for the promotion of healthy eating and weight regulation. Furthermore, this study emphasises the significant correlation between self-efficacy, motivation, and perceived barriers to change as psychosocial variables associated with healthy eating behaviour and weight regulation in adolescents.
Conflict of Interest The authors of this article declare no conflict of interest. Cite this article as: Marentes-Castillo, M., Castillo, I., Tomás, I., & Álvarez, O. (2026). Weight control and healthy eating: Cross-cultural invariance of self-efficacy, motivation, and perceived barriers. Clinical and Health 37, Article e260721. https://doi.org/10.5093/clh2026a7 References |
Cite this article as: Marentes-Castillo, M., Castillo, I., Tomás, I., & Álvarez, O. (2026). Weight Control and Healthy Eating: Cross-cultural Invariance of Self-efficacy, Motivation, and Perceived Barriers. Clinical and Health, 37, Article e260721. https://doi.org/10.5093/clh2026a7
Correspondence: Ines.Tomas@uv.es (I. Tomás)., Correspondence: Ines.Tomas@uv.es (I. Tomás).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
Clinical and Health is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License








