


Exploring the Relationship between Contextual Performance and Burnout in Healthcare Professionals
[La exploración de la relación entre el desempeño contextual y el agotamiento emocional en los profesionales de la salud]
Patricia Palenzuela, Naira Delgado, and JosĂ© A. RodrĂguez
Universidad de La Laguna, España
https://doi.org/10.5093/jwop2019a13
Received 5 July 2018, Accepted 9 May 2019
Abstract
Contextual performance is assumed to be related to professionals’ quality of working life and health. This research aims to compare the levels of contextual performance at work in different hospital units, and to analyse the relationship between contextual performance and burnout syndrome. A total sample of 222 participants from a tertiary hospital took part in the study. Scores on contextual performance and burnout in five different hospital units were compared. The results showed that contextual performance is closely related with burnout. Also, results showed statistically significant differences in the degree of contextual performance at work by hospital unit. Overall, these results are significant for the development of health management strategies that promote contextual performance at work, thus improving the health and quality of work of health-care professionals.
Resumen
Se considera que el desempeño contextual puede estar relacionado con la calidad de la vida laboral y la salud de los profesionales. Esta investigación tiene como objetivo comparar los niveles de desempeño contextual en el trabajo en diferentes unidades hospitalarias y analizar la relación entre el desempeño contextual y el síndrome de burnout. Un total de 222 participantes de un hospital terciario participaron en el estudio. Se compararon las puntuaciones en el rendimiento contextual y el agotamiento en cinco unidades hospitalarias diferentes. Los resultados mostraron que el rendimiento contextual está estrechamente relacionado con el agotamiento. Además, mostraron diferencias estadísticamente significativas en el grado de desempeño contextual en el trabajo por unidad hospitalaria. En general, estos resultados son significativos para el desarrollo de estrategias de gestión de la salud que promueven el desempeño contextual en el trabajo, mejorando así la salud y la calidad del trabajo de los profesionales de la salud.
Palabras clave
Rendimiento contextual, Agotamiento, EnfermerĂa, Tratamiento de la salud.Keywords
Contextual performance, Burnout, Nursing, Health management.Cite this article as: Palenzuela, P. , Delgado, N. , & RodrĂguez, J. A. (2019). Exploring the Relationship between Contextual Performance and Burnout in Healthcare Professionals. Journal of Work and Organizational Psychology, 35, 115 - 121. https://doi.org/10.5093/jwop2019a13
Correspondence: ndelgado@ull.edu.es (N. Delgado).Exploring the Relationship between Contextual Performance and Burnout in Healthcare Professionals The objective of this research is to compare the levels of contextual performance at work in different hospital units and to analyse the relationship between contextual performance and one of the most important psychosocial risks in the healthcare context: the burnout syndrome. Contextual performance at work can be defined as the expression of benevolent and voluntary behaviour towards the organisation, which is beyond a worker’s formal obligations and which is not directly recognised by the organisation he or she works for (Organ, 1988). These acts are important because they form the organisational, social, and psychological context for task activities and procedures: individuals contribute to organisational effectiveness by doing things that are not defined within their main functions, but that are important because they shape the objectives of the organisation and the social context that supports the activities (Borman & Motowidlo, 1993). These activities have been labelled discretionary behaviours (Zeithaml, Parasuraman, & Berry, 1990), contextual performance (Borman & Motowidlo, 1993), or organisational citizenship behaviours (Bateman & Organ, 1983; Smith, Organ, & Near, 1983). This construct has undergone multiple variations in the last 20 years. Borman and Motowidlo (1993) focused on separating the constructs of task performance and contextual performance. Contextual performance includes activities such as helping others in their work, supporting the organisation, and voluntarily participating in additional work responsibilities, while task performance includes the way the set of tasks established for each job is carried out. There are other important differences between the two concepts as well. First, task-related behaviours vary among positions, while organisational citizenship behaviours are more similar. Second, tasks tend to be more explicitly and formally established than contextual performance in the requirements of the position. Finally, the antecedents of task performance seem to imply a greater degree of abilities and skills, while the antecedents of contextual performance are, to a greater degree, personality traits (Díaz-Vilela, Díaz-Cabrera, Isla-Díaz, Hernández-Fernaud, & Rosales-Fernández, 2012). The dimensions of contextual performance have been the object of study for different researchers. Some studies report on only one dimension (Hoffman, Blair, Meriac, & Woehr, 2007; Lepine, Erez, & Johnson, 2002), while others include up to five dimensions (Borman & Motowidlo, 1993). After reviewing the previous literature, Coleman and Borman (2000) developed a list of 27 behaviours associated with contextual performance (citizenship performance behaviours). They extracted four factors from a factor analysis of the collected data: help and cooperate with others, approve, support and defend organisational objectives, follow organisational rules and procedures, and persist with enthusiasm and extra effort to complete their tasks. Is There a Dark Side to Contextual Performance? Contextual performance is generally considered positive, the by-product of good employee-organisational relationships, and a reflection of employees’ perceptions of fair treatment and positive attitudes (Smith et al., 1983). However, in recent years, a research area has developed focusing on the negative effects of contextual performance at work (Bolino, Klotz, Turnley, & Harvey, 2013). The central idea of this novel theoretical approach is that contextual performance can result in some personal and professional costs for those who exercise it and can also conceal selfish motives linked to image management and counter-productive behaviour. Bolino, Turnley, and Niehoff (2004) challenged current opinions on contextual performance in three ways. First, they suggested that the behaviours that occur are not necessarily prosocial, since they can come from selfish motivations (good impressions, transgressions, and dissatisfaction with personal life). Second, they postulated that contextual performance could have insignificant or even negative effects on organisational performance, particularly when these behaviours are of low quality or are performed instead of the tasks that make up the professional role. Finally, they argued that employees who develop contextual behaviours may experience greater role ambiguity, work overload, stress at work, and conflicts between work and family, particularly if they feel pressured to participate in such behaviours. For all these reasons, these authors suggest that contextual performance could have negative consequences for employees when it occurs too frequently in the workplace. Although attractive, many of these ideas were based more on speculation than on evidence. However, in recent years, different researchers have published a series of conceptual documents and empirical studies that indicate that contextual performance does not always have positive consequences. To date, this research has not been systematically reviewed. Although the idea that contextual performance has many positive qualities is not discussed, in highlighting the more negative aspects of the concept, it is expected that a more balanced view of this type of behaviour will be offered (Fineman, 2006), encouraging future research that could consider the possibility that contextual performance may have potentially negative implications for individuals and organisations (Bolino et al., 2013). This perspective highlights the importance of incorporating measures related to professionals’ quality of working life and health into studies of contextual performance. In this way, it will be possible to identify which dimensions of contextual performance are associated with the worst health conditions, and under what circumstances. In a healthcare context, it is especially relevant to explore the possible relationship between contextual performance and burnout. The Relationship between Burnout and Contextual Performance The burnout syndrome can be defined as a prolonged response to chronic stressors at a personal and relational level at work, determined from the dimensions known as exhaustion, depersonalisation and cynicism, and professional inefficiency (Maslach, Schaufeli, & Leiter, 2001). More recent studies in occupational and pre-occupational samples reveal that burnout constitutes a syndrome characterised by: 1) exhaustion, related to crisis in the relationships between a person and work in general; 2) mental distance, which includes both cynicism—distant attitudes towards work in general—and depersonalisation—distant attitudes towards people for and with whom one works; and 3) professional inefficiency, the feeling of not doing tasks properly and being incompetent at work (Maslach & Jackson, 1981; Salanova, 2006). Schaufeli and Enzman (1998) estimated that 90% of all studies analysing the burnout syndrome had used the Maslach Burnout Inventory (MBI) as a measurement instrument. Burnout is a syndrome that causes severe problems for both professionals who suffer from it and recipients of their work. In general, research has indicated that there are negative consequences of a psychosomatic, behavioural, emotional, attitudinal, social, and organisational nature. Burnout involves problems such as anxiety, irritability, changes in mood, insomnia, depression, and drug use (Shanafelt, Bradley, Wipf, & Back, 2002). In addition, this syndrome is associated with a decrease in work performance and health problems linked to stress (Parker & Kulik, 1995). Empirical findings from different organisational settings support the negative association between burnout components and extra role behaviours, and the relationship between chronic exposure to stressful events, job stress, and contextual performance (Brown & Roloff, 2015; Chiu & Tsai, 2006; Cropanzano, Rupp, & Byrne, 2003; Hannam & Jimmieson, 2002; Kohan & Mazmanian, 2003; Wegge, Van Dick, Fisher, Wecking, & Moltzen, 2006). Contextual performance is considered one of the possible consequences of burnout. Particularly, some scholars suggest that employees’ sense of emotional and mental resource depletion prevents them from putting extra effort into or spending personal time on activities that exceed job requirements, are discretional, and are likely not rewarded (Cropanzano et al., 2003; Van Emmerick, Jawahar, & Stone, 2005). Research findings on the causal relationship between burnout and extra role behaviours are controversial, but most of the evidence demonstrates that they are negatively associated. Empirical support for this negative association was found in healthcare settings (Cropanzano et al., 2003), social services (Kohan & Mazmanian, 2003), education (Brown & Roloff, 2015; Hannam & Jimmieson, 2002), and production settings (Chiu & Tsai, 2006; Wegge et al., 2006). After an exhaustive review, Chiu and Tsai (2006) found that only one empirical study has shown that the emotional exhaustion component of burnout acts as an important predictor of contextual behaviour at work. Moreover, Cropanzano et al. (2003) found that emotional exhaustion only negatively affected the dimension of OCB-O (performance oriented to benefit the organisation). An explanation of this could be that employees who feel emotionally exhausted will inhibit citizenship behaviours directed specifically towards the organisation, but not those aimed at colleagues or the work team. Healthcare Units, Workload, and its Consequences Nursing may be categorised as a stressful occupation because nurses in their daily routines are exposed to direct and ongoing contact with patients and their relatives or friends, work overload, excessive administrative work, insufficient reaction intervals dealing with problematic users, direct contact with illness, pain and death, lack of specificity of functions and tasks, lack of autonomy, and authority at work to make decisions, etc. (Gil-Monte, 2001; Kar & Suar, 2014). Work overload is one of the work design characteristics that affect burnout. Specifically, Maslach and Leiter (2008) suggested that work overload contributes to emotional exhaustion by depleting the capacity to meet job demands (Leiter, Gascon, & Martínez-Jarreta, 2010). The literature of burnout among healthcare nurses concluded that burnout is reported when nurses lack adequate time to complete their day-to-day nursing activities or provide emotional support to their patients (Dickinson & Wright, 2008; Edward & Hercelinskyj, 2007). Shirom, Nirel, and Vinokur (2010), in their study of burnout among physicians, found that high workload levels predicted a physician’s level of burnout. These results highlight the importance of deepening the study of the relationship between contextual performance and burnout, while also including different healthcare services to better understand the role of job characteristics in the relationship between burnout dimensions and contextual performance. Although there are several classifications of medical services that consider work overload (for example, SIGNO project for Spanish hospitals; Cortés & Ortega, 1996), there is a lack of research that helps to differentiate between hospital units based on the degree of job control, task planning at work, and/or work overload. The purpose of this study is to incorporate information on the specific unit where healthcare professionals work into the analysis of the relationship between burnout and contextual performance. Particularly, we were interested in exploring the effect of units with different levels of job control and medical attention planning capacity on burnout and contextual performance. Specifically, two hypotheses are considered: H1: Participants that work in units with low levels of job control and planification (Emergency Ward, Internal Medicine Ward) will report more levels of burnout and fewer levels of contextual performance than participant from units with high levels of job control and planification (Specialized Outpatient Care, Operating Theatre). H2: Emotional exhaustion and hospital unit will predict contextual performance. Following Cropanzano et al. (2003), the effect will be higher for compliance than for altruism. Participants This study was carried out in a public hospital in the Canary Islands with a total population of 279 nurses and 230 nursing assistants in the following units: Emergency Ward, Intensive Care Unit, Operating Theatre, Internal Medicine Ward, and Specialized Outpatient Care. As an inclusion criterion, participants had to have worked in one of the aforementioned units for at least three months. After applying the inclusion criteria, 222 healthcare professionals participated in the study (43.61% of the nursing staff in the selected hospital units). Of the sample, 60.4% were nurses and 39.6% were nursing assistants. Mean age of participants was 38.58 years old (SD = 10.67). A total of 77% of the sample were women. The demographic characteristics of the sample are shown in Table 1. Table 1 Characteristics of the Sample (N = 222)  An a priori power analysis suggested that a sample size of 204 participants should provide 95% power to detect an alpha error of probability = .05 in the case of a medium effect size (d = 0.10), for multiple regression analyses. Instruments Participants received a questionnaire that included the following instruments: Contextual performance. The Spanish version of Coleman and Borman’s (2000) scale, extracted from Díaz-Vilela et al. (2012), was adapted for this study. This scale consists of 27 statements with a response method based on a 7-point Likert scale that ranges from totally disagree (1) to totally agree (7). For this study, a short version of the scale was applied, including only the items corresponding to the two main factors found in Díaz-Vilela et al. (2012). Specifically, the compliance dimension is made up of 9 items, and the altruism dimension is made up of 6 items. Burnout. The Maslach Burnout Inventory was selected, with 22 items measuring the three dimensions of the syndrome: emotional exhaustion, depersonalisation, and self-fulfilment. It consists of a 7-point Likert-type frequency scale ranging from never (0) to every day (6), with a maximum total score of 132 points. The maximum score is 54 points for the emotional exhustion dimension, 30 points for depersonalisation, and 48 points for self-fulfilment. Demographic variables. A demographic questionnaire was added to the survey to obtain descriptive information. Profession, gender, age, years of experience, time working in the specific unit, and work shift were included. Procedure Data was collected in a public hospital in the Canary Islands between 20 January 2016 and 30 July 2016. Previously, written consent was requested from the hospital management for the participation of their employees in the study. Once this authorisation had been granted, supervisors of units to be included in the survey were contacted to inform them of the study and ask for their collaboration regarding file deposit in a secure place where participants could easily access it. To collect data required for the study, the questionnaires described above were stapled together in a sealed envelope (one for each participant), and each participant returned their completed questionnaires in a sealed envelope so there would be no doubt of its anonymity and correct handling. A folder was left at each hospital unit where participants could hand in their completed surveys. During the six months of data collection the method adopted was to visit the different units several days in a row to reach as much of the staff as possible, and during those visits to explain to them the study and survey procedure and answer any questions. Data was analysed with the SPSS 21 and R. Before conducting the statistical tests, normality tests were performed, as well as the exploration of extreme cases. There were only a few missing data points (less than 2% of the scores collected), and we excluded those scores from those analyses. Because data was collected by means of a self-report survey that involved responding to all the instruments at the same time, we applied the Harman one-factor test to verify the common method variance effect (Podsakoff, Mackenzie, Lee, & Podsakoff, 2003). Since the result showed a factor explaining less than 50%, the effect of the common method variance does not seem to significantly affect the relationship of the variables from this study. Confirmatory Factor Analysis of Contextual Performance Scale To verify the empirical structure of the contextual performance scale, a confirmatory factor analysis was carried out. The fit indexes obtained showed an acceptable fit (TLI = .94, CFI = .95, RMSEA = .048, CI = .036-.059). The structure resulting from this model included the two original factors. Following Díaz-Vilela et al. (2012), we call the first factor Altruism and the second factor Compliance. Regarding the model obtained by Díaz-Vilela et al. (2012), all the items are adjusted to the two-factor structure obtained. Reliability of Dimensions and Correlations between Them Once the factor structure of the contextual performance scale was verified, the reliability of each dimension was checked. Table 2 shows the average scores and standard deviations obtained in contextual performance (global score), compliance, altruism, and burnout (emotional exhaustion, depersonalisation, and self-fulfilment) dimensions, for the total sample. Table 2 also shows the reliability scores (alpha and omega) for each dimension, and correlations between dimensions. Table 2 Mean Scores, Standard Deviations, Reliability, and Correlations between the Dimensions of the Study  *p < .05 (bilateral), **p < .01 (bilateral). First, it is observed that the compliance dimension has higher scores than the altruism dimension. Second, it is observed that both compliance and altruism dimensions have statistically significant correlations with the three burnout dimensions but are especially highly correlated with emotional exhaustion and self-fulfilment. Prevalence of Burnout To analyse the prevalence of the burnout syndrome in the healthcare personnel who participated in the study, data provided in the manual of the MBI Inventory in Spanish (Maslach & Jackson, 1997) was taken as a reference. Specifically, the scores corresponding to the sample of medical professionals were taken (N = 156). In response to these scores, the frequency of high levels of emotional exhaustion and depersonalisation and of low levels of self-fulfilment was calculated in the total sample, as well as the frequency of these dimensions within each hospital unit. The results are shown in Table 3. Of the total sample, 23.9% had high levels of emotional exhaustion, 28.4% had high levels of depersonalisation, and 21.2% had low levels of self-fulfilment. Table 3 Percentage of High Frequency of Emotional Exhaustion, Depersonalisation, and Low Self-fulfilment obtained in Total and in Each Hospital Unit  The analysis of the frequency of high levels of emotional exhaustion by hospital unit reveals that the Emergency Ward suffers the highest percentage of cases with high levels of emotional exhaustion, followed by Internal Medicine. For depersonalisation, Internal Medicine has the highest percentage of cases (38.9%), followed by the Emergency Ward (32.2%). There is a lower frequency (19.4%) in the Specialized Outpatient Care unit. Finally, in the case of low self-fulfilment, the Emergency Ward staff suffer the highest frequency in this dimension (27.1%), while the ICU has a much lower percentage of staff with low self-fulfilment than other units (8.3%). Comparison between Hospital Units To determine whether there were statistically significant differences between the different hospital units in each of the variables analysed, a series of ANOVAs was carried out. As a summary, Figure 1 shows the scores of the staff in each unit for each of the dimensions of contextual performance, and Figure 2 shows the scores for each of the dimensions of burnout. Figure 1 Means of Each Unit in Each of the Dimensions of Contextual Performance. 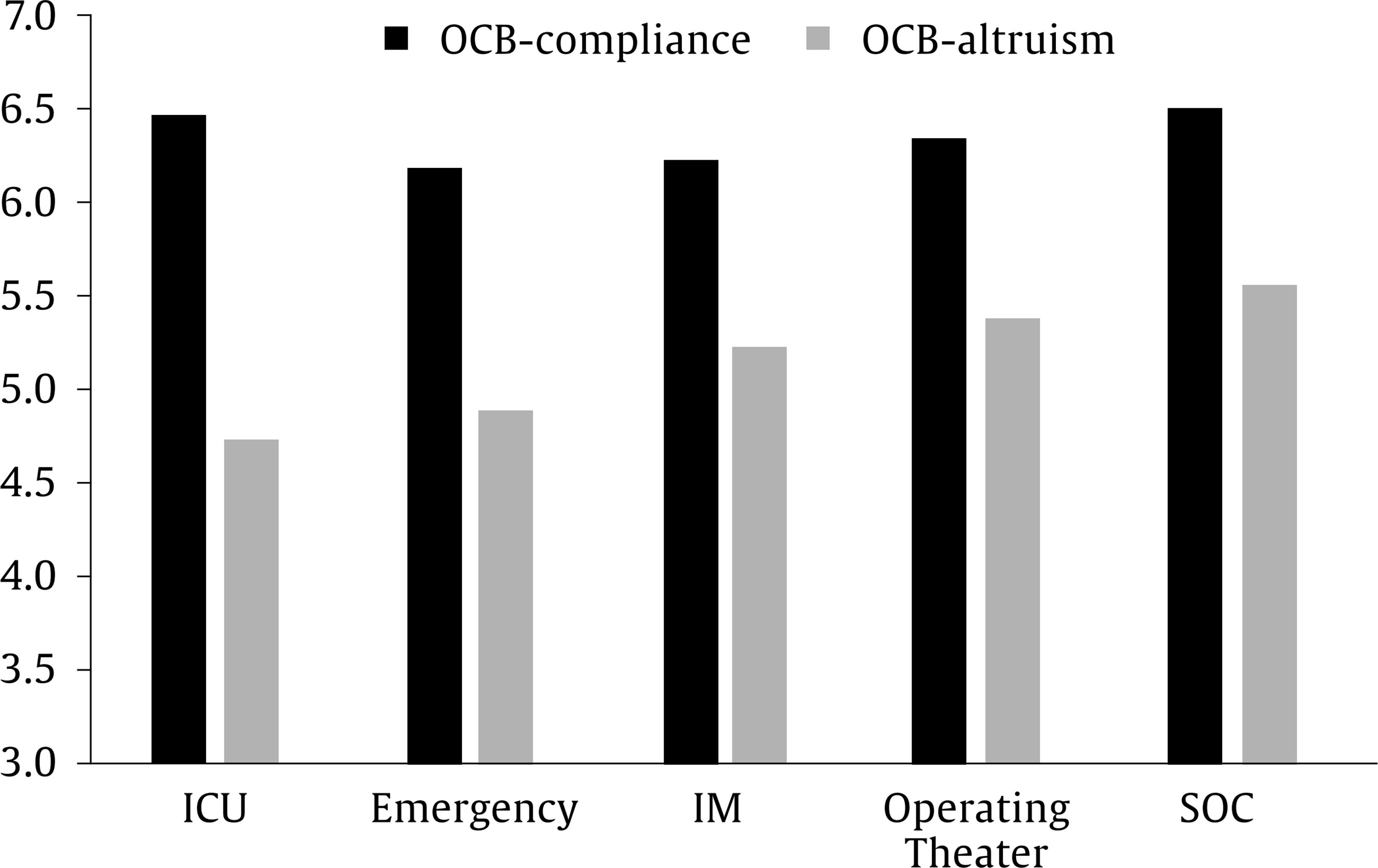 Note. ICU = Intensive Care Unit; IM = Internal Medicine; SOC = Specialized Outpatient Care. Figure 2 Means of Each Unit in Each of the Dimensions of Burnout 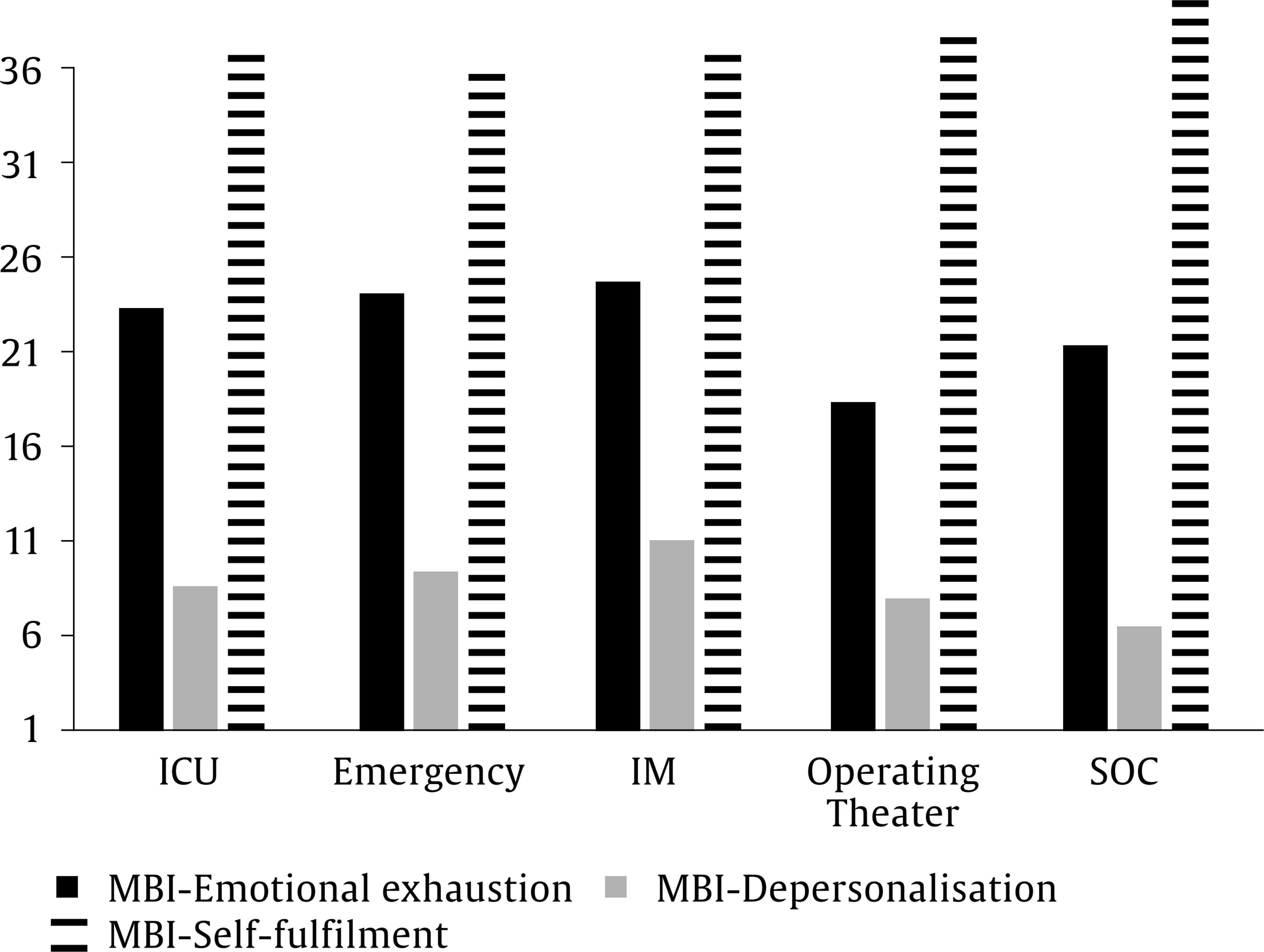 Note. ICU = Intensive Care Unit; IM = Internal Medicine; SOC = Specialized Outpatient Care. First, the scores obtained for contextual performance in each hospital unit were compared. The analysis of variance showed absence of statistically significant differences in the compliance dimension, F(4,216) = 1.54, p = .19. In the altruism dimension, the result of the ANOVA was statistically significant, F(4,216) = 3.39, p = .01. Paired comparisons showed statistical differences between Specialized Outpatient Care and ICU (p = .03), Specialized Outpatient Care and Internal Medicine (p = .038), and ICU and the Emergency Ward (p = .053). Statistical differences between Specialized Outpatient Care and the Emergency Ward (p = .07), and between ICU and Operating Theatre (p = .08) were marginally significant. With respect to burnout dimensions, the analysis of variance revealed marginally significant differences between the different units analysed in the emotional exhaustion dimension, F(4,215) = 2.345, p = .056. The analysis of paired comparisons in emotional exhaustion indicated that the Operating Theatre scores were statistically lower than those obtained in Internal Medicine (p = .014) and the Emergency Ward (p = .01) and marginally significant in ICU (p = .06). In the other two dimensions, the analysis showed no statistically significant differences by hospital unit, F(4,215) = 1.53, p = .195, for depersonalisation, and F(4,215) =1.471, p = .212, for self-fulfilment. Regression Analyses To test the hypothesis that burnout dimensions will predict contextual performance, and to explore the role of hospital unit in those relationships, two hierarchical regression analyses were performed. Specifically, each model included emotional exhaustion, depersonalization, self-fulfilment, and time (in years) working in the present job, and in the second level hospital unit. The model for compliance showed adjR2 = .15. Emotional exhaustion (B = -0.31, t = -4.09, p < .001) and self-fulfilment (B = 0.22, t = 3.35, p = .001) were the variables with statistical significance, with no effects for hospital unit. For altruism, the model showed adjR2 = .18. Emotional exhaustion (B = -0.30, t = -4.44, p < .001) and self-fulfilment (B = 0.25, t = 3.77, p < .001) were statistically significant in the model. Hospital unit was also statistically significant. Specifically, this variable was included as a categorical variable, and ICU was used as the comparison level with the rest of levels. Operating Theatre (B = 4.77, t = 1.99, p = .047) and Specialized Outpatient Care (B = 3.27, t = 2.26, p = .025) were statistically significant. The aim of this research was to compare the levels of contextual performance at work in different hospital units and to analyse the relationship between contextual performance and the burnout syndrome. The results obtained allow us to draw a series of relevant conclusions and serve as a guide for future research to develop management activities aimed at optimising work performance and quality of life in healthcare professionals. First, the results confirm that contextual performance is structured around two central dimensions, compliance and altruism. These two dimensions are consistent with previous literature, especially with the results obtained in the adaptation of the contextual performance scale by Coleman and Borman (2000) to Spanish, carried out by Díaz-Vilela, Díaz-Cabrera, Isla-Díaz, Hernández-Fernaud, and Rosales-Fernández (2012). In our study, a reduced version of this scale (15 items) was used, and the results obtained were very similar to those achieved with the full scale. The results are also consistent with those proposed by William and Anderson (1991). Specifically, the altruism dimension corresponds to OCB-I (behaviours mainly directed to colleagues), and compliance corresponds to OCB-O (behaviours mainly oriented to the organisation). Overall, the results obtained in this study support the findings obtained in previous studies with nurses, in which significant relationships were found between contextual performance and burnout. However, unlike previous results (Chiu & Tsai, 2006; Cropanzano et al., 2003), here the emotional exhaustion dimension is related not only to compliance, but also to altruism. In addition, self-fulfilment is also related with the two dimensions of contextual performance and, although at lower levels, a statistically significant correlation was found between depersonalisation and the two dimensions of contextual performance at work. Regarding the scores obtained in burnout dimensions, the average scores were slightly higher than those collected in the MBI Manual with the Spanish sample (Maslach & Jackson, 1997) for the total sample, and slightly lower than those obtained with medical professionals. The analysis comparing scores by hospital unit is more interesting. The Emergency Ward has the highest percentage of cases with high levels of emotional exhaustion, followed by Internal Medicine. The units with the lowest percentages were the Operating Theatre and ICU. One possible explanation is that there is often less communication with patients in these two units than in the other units, since most patients, given their pathologies and/or interventions, will be sedated. This lack of communication could reduce the emotional demands at work. With respect to depersonalisation, Internal Medicine has the highest percentage of cases, followed by the Emergency Ward. Looking at low self-fulfilment, Emergency Ward staff suffer higher levels more frequently, while the ICU has a much lower percentage of staff with low self-fulfilment than other units. These results suggest that the Emergency Ward is the unit where healthcare professionals are more susceptible to burnout as a syndrome. When comparing the different hospital units in terms of contextual performance, within the dimension of altruism, the units that have remarkably high scores are the Specialized Outpatient Care and Operating Theatre, while ICU has lower scores. However, in the compliance dimension, it is the Specialized Outpatient Care and ICU units that have the highest scores. It is possible that the structuring of work in each unit, together with the high task load and planning difficulties, lead to difficulties developing contextual performance at work. In ICU, the disparity in scores obtained between the dimensions of altruism and compliance may be related to the distribution of work. Each professional has certain patients assigned to them and deals with everything related to these patients, without having the opportunity to coordinate with other colleagues to have them perform certain functions. Studies comparing the levels of contextual performance in different hospital units are scarce; this study contributes to a better understanding of the relationship between contextual performance and burnout. The present research explores hospital units with different workloads, required levels of specialisation, degrees of interaction with patients, and volume of work. Taken together, results suggest that a hospital unit is more relevant to promote altruism than compliance. However, more research is needed to clarify the link between specific organisational conditions in each healthcare service and contextual performance. Future research should also incorporate the perceptions of medical personnel into the study. It is important to understand the extent to which aspects such as contextual performance and development of burnout are present in medical personnel, and if they occur to a greater or lesser extent than in the rest of the hospital staff. Also, future studies should focus on identifying background and consequent variables of contextual performance at work, using longitudinal studies with many participants. It would be interesting to carry out additional studies where different units are compared to those surveyed here. The present study has some limitations, which means that the conclusions should be taken with caution. In the first place, it is a cross-sectional study of a descriptive nature, which does not allow conclusions to be drawn from causality. In addition, given the voluntary nature of the response to the surveys, it is possible that those who decided to respond had a greater predisposition to collaborate and therefore are more likely to be professionals with higher levels of contextual performance. Another limitation is related to sample size, especially when comparisons are made within each hospital unit. For multilevel regression models, it is recommendable to work with more groups/units. The fact of having worked with a single hospital makes it difficult to generalise the results and limits the number of staff who could respond within each unit. Finally, all the responses collected were self-reported, and as such represent participants’ own opinions of themselves and how they behave. For future studies, it would be interesting to analyse, in addition to participants’ opinions, quality indicators for each unit, such as user satisfaction, as well as having contextual performance evaluated by peers and supervisors. This information could complement self-reports and offer a broader and more detailed view of contextual performance at work, and shed light on the possible impact on the organisation, healthcare professionals and patients, who, at the end, are the driving force behind hospital management. Cite this article as: Palenzuela, P., Delgado, N., & Rodríguez, J. A. (2019). Exploring the relationship between contextual performance and burnout in healthcare professionals. Journal of Work and Organizational Psychology, 35, 115-121. https://doi.org/10.5093/jwop2019a13 Financing: This article has been partially funded by the Official College of Nurses of Santa Cruz de Tenerife, Spain. References |
Cite this article as: Palenzuela, P. , Delgado, N. , & RodrĂguez, J. A. (2019). Exploring the Relationship between Contextual Performance and Burnout in Healthcare Professionals. Journal of Work and Organizational Psychology, 35, 115 - 121. https://doi.org/10.5093/jwop2019a13
Correspondence: ndelgado@ull.edu.es (N. Delgado).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print SEND
SEND






