


Mental Health Shame of UK Construction Workers: Relationship with Masculinity, Work Motivation, and Self-Compassion
[La vergüenza relativa a problemas de salud mental en trabajadores de la construcción británicos: su relación con la masculinidad, la motivación en el trabajo y la autocompasión]
Yasuhiro Kotera, Pauline Green, and David Sheffield
University of Derby, United Kingdom
https://doi.org/10.5093/jwop2019a15
Received 5 June 2018, Accepted 9 May 2019
Abstract
Despite their poor mental health, many UK construction workers do not seek out help, because of shame for mental health problems relating to masculinity. The purposes of this study were to investigate relationships among mental health shame, mental health problems, masculinity, self-compassion, and motivation, and examine whether self-compassion would mediate the relationship between mental health shame and mental health problems. Construction workers (N = 155) completed measures for those five constructs. The five constructs were adequately correlated with each other, but masculinity and motivation were not related to shame. Self-compassion partially mediated the relationship between mental health shame and mental health problems. Findings may help construction workers understand the importance of mental health shame with mental health problems, and identify better solutions for poor mental health. Brief online self-compassion training was recommended to reduce shame and enhance self-compassion, and may be accessible for construction workers who work at diverse sites and hours.
Resumen
A pesar de su estado de salud mental, muchos trabajadores de la construcción del Reino Unido no buscan ayuda debido a la vergüenza que provocan los problemas de salud mental relacionados con la masculinidad. Los propósitos de este estudio fueron investigar las relaciones entre esta vergüenza, los problemas de salud mental, la masculinidad, la autocompasión y la motivación y examinar si la autocompasión mediaría la relación entre la vergüenza por su estado de salud mental y los problemas de salud mental en sí. Trabajadores de la construcción (N = 155) cumplimentaron medidas para esos cinco componentes. Estos se correlacionaban adecuadamente entre sí, pero la masculinidad y la motivación no se relacionaban con la vergüenza. La autocompasión medió parcialmente la relación entre la vergüenza y la salud mental y los problemas de salud mental. Los resultados pueden ayudar a los trabajadores de la construcción a entender la importancia de la vergüenza para los problemas de salud mental e identificar mejores soluciones para estos problemas de salud mental. Se recomendó una breve capacitación online en autocompasión para reducir esta vergüenza y mejorar la autocompasión, que pueda ser accesible a los trabajadores de la construcción que trabajan en diversos lugares y diferentes jornadas.
Palabras clave
Vergüenza con respecto a la salud mental, Masculinidad, Autocompasión, Trabajadores de la construcción, Motivación.
Keywords
Mental health shame, Masculinity, Self-compassion, Construction workers, Motivation.
Cite this article as: Kotera, Y. , Green, P. , & Sheffield, D. (2019). Mental Health Shame of UK Construction Workers: Relationship with Masculinity, Work Motivation, and Self-Compassion. Journal of Work and Organizational Psychology, 35, 135 - 143. https://doi.org/10.5093/jwop2019a15
Correspondence: Yasuhiro Kotera (y.kotera@derby.ac.uk)
Poor Mental Health of UK Construction Workers Workers in the construction industry engage with various activities for buildings and public engineering works, relating to repair, additions, and modifications (Office for National Statistics, 2015). They frequently work for a contractor who manages and supervises the entire process of construction work. Examples of construction workers include plumbers, electricians, scaffolders, as well as supervisors such as foremen and chargehands (Health and Safety Executives, 2015). The construction industry in the UK has grown to yield £150 billion annually (6% of the economy) and employ 2.7 million people (8% of the national workforce; Statista, 2018). Despite its significance, the mental health of UK construction workers is challenging. Fifty-five percent of them have experienced mental health problems (i.e., depression, anxiety, and stress) in their lives, and 42% of them have suffered from mental health problems at their current workplace: both figures are more than twice of the national average (25% for lifetime occurrence and 17% for at-work occurrence; Alderson, 2017). Unsurprisingly, the number of suicides is also relatively high in this population. Whilst the deaths due to accidents on site have reduced from 200 to 40 in the past 60 years, the number of suicides, supposedly caused by mental health issues, such as depression, anxiety, and stress, has been static at about 280 per annum (Sanderson, 2017). Male construction workers are four times more likely to commit suicide than the national average (Office for National Statistics, 2017). These figures illustrate the seriousness of this problem. Despite the seriousness of mental health, however, UK construction workers are often reluctant to tell others about their problems or seek out help. The Mind Matters campaign (N = 1,139) launched in 2017 by Construction News, a major news informer of the industry, reported that 30% of construction workers have taken time-off from work due to mental health problems, but 60% did not tell their boss that the reason for absence was due to those mental health problems (Alderson, 2017). A quarter of the construction workers have considered suicide; 90% of the construction workers who have considered suicide or have known someone who committed suicide, did not ask for support (Alderson, 2017). Further, the majority reported the reason for not turning to their employer was shame (Alderson, 2017). Indeed, mental health shame has been reported as a barrier for help-seeking in various populations including university students (Gilbert et al., 2007; Kotera, Green, & Sheffield, 2019) and adult workers (Kotera, Adhikari, & Van Gordon, 2018), and it has been positively associated with mental health problems (Gilbert et al., 2007; Kotera, Adhicari et al., 2018; Kotera et al., 2019). Though low self-stigma about mental health was found in male Australian construction workers (Milner et al., 2017), no study to date has explored the relationships between mental health problems and mental health shame in UK construction workers. Accordingly, the present study aimed to explore these relationships. H1a: Mental health shame will be positively associated with mental health problems. Masculinity and Shame The Construction Industry Helpline, a supporting agency for UK construction workers, noted that poor mental health of construction workers and their low help-seeking were due to the masculine culture of this industry (Sanderson, 2017). While the definition of masculinity is still debated (Clay, 2012), commonly it is considered as a set of qualities that are traditionally associated with being male, and is different from the biological sex (i.e., some women and girls have a high level of masculinity; Ferrante, 2008). Though it can differ by culture (Kimmel & Bridges, 2011), masculinity, in general, emphasises toughness, stoicism, acquisitiveness and self-reliance, and is related to shame (Lomas, 2014). For example, Australian farmers also suffer from poor mental health because of shame (Alston 2011; King, Lane, MacDougall, & Greenhill, 2009): their desire to succeed as farmers fosters their masculinity, which then makes it difficult to ask for help for mental health problems, which may contribute to the high suicide rate in this population (Bryant & Garnham, 2015). Though masculinity is different from biological sex, males and highly-positioned UK hospitality workers had higher levels of shame and mental health problems (Kotera, Adhikari, & Van Gordon, 2017). Masculinity can prevent people from seeking for help on their mental health problems, as illustrated in the common phrase “boys don’t cry”, which can exacerbate the clinical outcomes (Galdas, Cheater, & Marshall, 2005; Lomas, 2014). Unsurprisingly, men’s help-seeking for psychological distress has been reported as substantially lower than women’s help-seeking cross-culturally and throughout the lifespan (Addis & Mahalik, 2003; Judd, Komiti, & Jackson, 2008; Levant, Wimer, & Williams, 2011), and lower than men’s help-seeking for physical problems (O’Brien, Hart, & Hunt, 2007). A systematic review of 37 studies of mostly non-clinical participants about masculinity in men’s help-seeking supported the contention that there was low help-seeking behaviour among men due to stoicism and self-stigma. Behavioural interventions focusing on men’s strengths, providing problem-solving tools for long-term behavioural changes, and reframing help-seeking as a courageous and masculine behaviour were suggested as useful approaches to encourage help-seeking (Seidler, Dawes, Rice, Oliffe, & Dhillon, 2016). However, to date, the relationship between masculinity and shame about mental health has not been explored in UK construction workers, traditionally perceived as a male occupational group (Francis, 2017). H1b: Mental health shame will be positively associated with masculinity. Work Motivation Work motivation refers to the psychological factors that prompt workers to attend to work-related activities (Pinder, 1998). Work motivation has been researched in depth by organisational researchers because a highly motivated workforce is a key asset to organisations (Kanfer, Chen, & Pritchard, 2008). Similarly, low levels of occupational health and motivation are detrimental to organisations and cost £6 billion per year to the UK economy, amounting to 0.4% of UK GDP in 2012 (Centre for Economics and Business Research, 2013). Work motivation was related with mental health shame in hospitality workers (Kotera, Adhicari et al., 2018) and business students (Kotera, Conway, & Van Gordon, 2018). Extrinsic motivation (a type of motivation that is driven by external rewards such as money and fame) was more strongly related to mental health problems and mental health shame than intrinsic motivation (a type of motivation that is derived from inherent pleasure in doing what one is passionate about; Kotera, Adhicari et al., 2018; Kotera, Conway et al., 2018). One of the most established theories about work motivation is Self-Determination Theory (SDT), asserting that human beings have a natural tendency to integrate their psychic energy into a sense of self and larger social structures (Deci & Ryan, 1985). SDT categorises work motivation into three types: intrinsic motivation occurs when you do an activity for inherent joy and satisfaction, extrinsic motivation occurs when you do an activity for an external incentive such as money and/or status, and amotivation occurs when you lack intention to act or act passively. Extrinsic motivation can be further categorised into four subtypes: external regulation (i.e., engaging in work only to receive a reward), introjected regulation (i.e., work motivation based on self-worth contingencies, such as colleagues’ reputation), identified regulation (i.e., acknowledging the importance of work), and integrated regulation (i.e., the value of the work activity is integrated into an employee’s sense of self, such as ‘I work because I am a construction worker’). Expectancy Theory (Vroom, 1964) attributes the different types of motivation to the locus of control: intrinsic motivation is based on an individual’s autonomous decision, while extrinsic motivation is based on an incentive, which can be manipulated by the organisation, and behaviours will cease as the incentive ceases (Mathibe, 2008). Each type of motivation is related to different outcomes. Intrinsic motivation is associated with positive organisational outcomes (Gagne & Forest, 2011), such as active information gathering (Koestner & Losier, 2002), goal achievement (Sheldon & Elliot, 1999), increased work performance (Baard, Deci, & Ryan, 2004; Miller, 2002), well-being (Ilardi, Leone, Kasser, & Ryan, 1993), job and life satisfaction (Locke & Latham, 2004), and prosocial behaviour (Gagne, 2003). At an interpersonal level, intrinsic motivation is related to better perceptions from subordinates (e.g., feeling safer and more supported), and job satisfactions including personal autonomy, job security, and work atmosphere (Deci, Connell, & Ryan, 1989; Zuckerman, Porac, Lathin, & Deci, 1978). On the other hand, extrinsic motivation and amotivation are related to negative outcomes (Vallerand & Ratelle, 2002), such as emotional exhaustion, physical and mental health problems (Houkes, Jassen, de Jonge, & Bakker, 2003), depression (Blais, Lachance, Vallerand, Brière, & Riddle, 1993), turnover intentions (Quast & Kleinbeck, 1990), unstable goal striving (Koestner, Losier, Vallerand, & Carducci, 1996), susceptibility to persuasion (Koestner & Losier, 2002), and compromised performance due to low concentration and memory (Vallerand, 1997). Unsurprisingly, compared to extrinsic motivation and amotivation, intrinsic motivation is three times more strongly related to work engagement (Cho & Perry, 2012) – a positive affective-cognitive state of mind characterised by vigour, dedication, and absorption (Schaufeli, Salanova, González-Romá, & Bakker, 2002). The cost of low work engagement is estimated to be about $370 billion annually in America, equating to 2% of GDP ($16 trillion; Gallup, 2013). Intrinsic motivation can be augmented by an autonomy-supportive work climate (Gagne & Deci, 2005), which can satisfy the three psychological needs of competence, autonomy, and relatedness (Ryan & Deci, 2000). A recent study identified that extrinsic motivation was more strongly positively related with mental health problems and mental health shame than intrinsic motivation among UK hospitality workers (Kotera, Adhicari et al., 2018); therefore, we hypothesised: H1c: Motivation will be positively associated with mental health problems (extrinsic motivation > intrinsic motivation). H1d: Motivation will be positively associated with mental health shame (extrinsic motivation > intrinsic motivation). Self-Compassion Compassion has been reported to be particularly important to mental health (Chu, 2017; Sommers-Spijkerman, Trompetter, Schreurs, & Bohlmeijer, 2018), and self-compassion is also related to lower levels of mental health problems (H1e), mental health shame (H1f), and more intrinsic motivation (H1g) in UK hospitality workers (Kotera, Adhicari et al., 2018) and Belgium students (Raes, 2011). Self-compassion is the self-directed version of compassion, and entails being kind to oneself during times of suffering, aiming to ease one’s suffering (Neff, 2003). A substantial amount of recent research reported that good mental health is positively associated with self-compassion, and that strong self-compassion may reduce the risk of mental health problems (Barnard & Curry, 2011; Ehret, Joormann, & Berking, 2015; Hofmann, Sawyer, Fang, & Asnaani, 2012; MacBeth & Gumley, 2012; Muris, Meesters, Pierik, & de Kock, 2016). Compassion-based psychotherapeutic interventions reduced mental health problems and shame (Braehler et al., 2013; Gilbert & Procter, 2006; Kelly, Zuroff, & Shapira, 2009). Self-compassion mediated the relationship between shame and depression in an adult clinical population (Zhang et al., 2018), and self-reassurance (a similar construct to self-compassion) mediated the relationship between mental health shame and mental health problems in workers (Kotera, Gilbert, Asano, Ishimura, & Sheffield, 2018). In these mediation relationships, shame negatively predicted self-compassion/self-reassurance, which negatively predicted mental health problems (H2). Despite these significant relationships between motivation, self-compassion, mental health problems and mental health shame, to date, no study explored these relationships in UK construction workers. H1e: Self-compassion will be negatively associated with mental health problems. H1f: Self-compassion will be negatively associated with mental health shame. H1g: Self-compassion will be positively associated with intrinsic motivation. H2: Self-compassion will mediate the relationship between mental health shame and mental health problems: Mental Health Shame → (negative) Self-Compassion → (negative) Mental Health Problems. Aims and Hypotheses In this study, therefore, we aimed to investigate relationships between mental health shame, mental health problems, masculinity, motivation, and self-compassion in UK construction workers (H1). In addition, path analysis is used to elucidate the mechanism of how their self-compassion impacts on mental health shame and problems (H2). Findings based on testing these hypotheses would help to identify potential shame-based approaches for alleviating poor mental health of UK construction workers. Participants The participating UK construction company was engaged in roadway (rock, sand, gravel, and cement), managing about 300 sites in the country, and 3,500 employees. About 1,000 workers were notified of this study from their managers or announcements. Eligible participants were 18 years old or older and had more than one year of work experience in this field. One hundred and sixty full-time workers agreed to participate, and 155 (138 male and 17 female; RNGage = 21-67, Mage = 40.28, SDage = 11.05 years) completed self-report measures about mental health shame, mental health problems, masculinity, motivation, and self-compassion, satisfying the required sample size (n = 114; Faul, Erdfelder, Buchner, & Lang, 2009). They had 15.44 years of work experience in construction on average (SD = 11.06 years), and their reported average weekly working hour was 49.35 hours (SD = 9.55 hours). For their workplace, 50% of them worked in transient workplaces (i.e., site-based), 39% worked at office, and the remaining 11% worked at other places such as highways. Thirty-four percent of them worked routinely in the day with some irregular night shifts, 26% worked during the day time only, 18% worked mixture of day and night times, 12% worked only at night, and the remaining 10% worked routinely at night with irregular day time working. Thirty-five percent of them were managers, 23% were foremen/supervisors, 20% were operatives/workers, 12% were technical professionals, the remaining 10% included directors, health and safety, trainees, and administrative staff. Fifteen percent of them had some sort of mental health training and 14% of them had previously received mental health support. Instruments Mental health shame was measured using the Attitudes Towards Mental Health Problems (ATMHP), a 35-item on a four-point Likert scale (from 0 = do not agree at all to 3 = completely agree; a higher score indicates stronger shame). This scale consists of four sections: (i) community and family attitudes consider their perception of how their community and family perceive mental health problems, (ii) external shame assesses their perception of how their community and family would perceive them if they had a mental health problem, respectively, (iii) internal shame relates to how they perceive themselves if they had a mental health problem, and (iv) reflected shame evaluates how their family would be perceived if they had a mental health problem (family-reflected shame), and fears of reflected shame on themselves, associated with a close relative having a mental health problem (self-reflected shame). All of the subscales had good internal consistency (α = .85-.97; Gilbert et al., 2007). Table 1 Descriptive Statistics: Attitudes Towards Mental Health Problems (Mental Health Shame), Depression Anxiety Stress Scale 21 (Mental Health Problems), Masculinity Behavior Scale (Masculinity), Self-Compassion Scale (Self-Compassion), and Work Extrinsic and Intrinsic Motivation Scale (Work Motivation) in UK Construction Workers (N = 155) 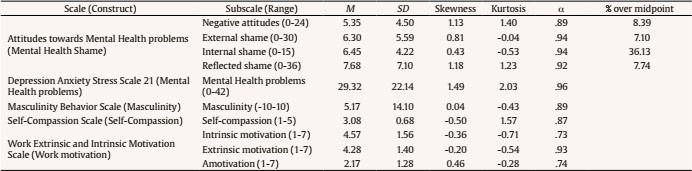 Level of their mental health problems was evaluated using the Depression Anxiety and Stress Scale (DASS21), 21-item on four-point Likert scale (from 0 = did not apply to me at all to 3 = applied to me very much or most of the time). DASS21 is a short-form version of the DASS42 (Lovibond & Lovibond, 1995) consisting of three seven-item subscales: depression (e.g., ‘I felt that I had nothing to look forward to’), anxiety (e.g., ‘I felt I was close to panic’), and stress (e.g., ‘I found it difficult to relax’), measuring the level of mental health problems in total (Lovibond & Lovibond, 1995). DASS21 had good reliability (α = .87-.94; Antony, Bieling, Cox, Enns, & Swinson, 1998). Masculine Behavior Scale (MBS) is a 20-item self-report instrument measuring the degree of one’s engagement with masculine behaviours (e.g., ‘I spend a great deal of my time pursuing a highly successful career’; Snell, 1989). Each item is rated on a five-point Likert scale (from +2 = agree to -2 = disagree). The four components of masculinity demonstrated meaningful correlations with one another (inhibited affection and restrictive emotionality, and success dedication and exaggerated self-reliance), and the criteria validity was confirmed with a relevant scale. This scale has adequate internal consistency (α = .84; Snell, 1989). Work Extrinsic and Intrinsic Motivation Scale (WEIMS) entails 18 items measuring levels of different types of work motivation, following SDT (Tremblay, Blanchard, Taylor, Pelletier, & Villeneuve, 2009). Three items are allocated to six types of motivation: amotivation, external regulation, introjected regulation, identified regulation, integrated regulation, and intrinsic motivation. Each item is responded on a seven-point Likert scale (from 1 = does not correspond at all to 7 = corresponds exactly). The six subscales of WEIMS demonstrated meaningful correlations with one another and were correlated with relevant scales. All of the subscales have adequate internal consistency (α = .70-.83; Tremblay et al. 2009), with the exception of identified regulation (α = .67) and amotivation (α = .64). Though Cronbach’s alphas of these two subscales were low in the original validation paper (Tremblay et al. 2009), in our sample none of the subscales had Cronbach’s alpha lower than .70, therefore deemed to be acceptable (see Table 1). For the purpose of this study, the mean score of external regulation, introjected regulation, identified regulation, and integrated regulation was used to calculate extrinsic motivation (Tremblay et al., 2009). Self-Compassion Scale (SCS) comprises 26 five-point Likert scale items (1 = almost never to 5 = almost always; e.g., ‘I try to be understanding and patient towards those aspects of my personality I don’t like’), measuring the level of one’s self-compassion (Neff, 2003). SCS has high internal consistency (α = .92; Neff, 2003). Procedure Managers at a construction company in the UK had an introduction meeting with the researchers in order to understand the purposes and procedure of the study. They then distributed the study information and consent to their team members. After consenting to participate to the study, the participants were sent links to the online scales. Once they had completed all questions, a debrief was sent to them, which included information about available mental health support. Ethics approval was obtained from the University Research Ethics Committee. A cross-sectional design was employed. First, the collected data were screened for outliers, and the ratios of construction workers who scored over the midpoint in each ATMHP subscale were identified. Second, the data were screened for the assumptions of parametric tests. Third, in order to achieve the second aim of investigating relationships between mental health shame, mental health problems, masculinity, motivation, and self-compassion, correlations were completed (H1). Fourth, path analysis was used in order to examine whether self-compassion would mediate the relationship mental health shame and problems (H2). The correlation analyses were conducted using IBM SPSS 24. The Process macro 3 for SPSS (Hayes, 2017) was used for path analysis, with 5,000 bootstrapping re-samples and bias-corrected 95% confidence intervals (CIs) for indirect effects. Descriptive Statistics One score in family attitudes, six scores in family external shame, two scores in depression, and five scores in anxiety were identified as outliers using the outlier labelling rule (Hoaglin & Iglewicz, 1987), and so were winsorised (Tukey, 1962). Skewness values (0.04 to 1.18), and Kurtosis values (-0.04 to -2.03) were of no concern. Internal consistencies for all of the scales and subscales were high (α ≥;. 73). Table 1 summarises the descriptive statistics. The rates of construction workers who scored above the midpoint in each type of mental health shame were low: 8.39% for negative attitudes, 7.10% for external shame, 36.13% for internal shame, and 7.74% for reflected shame. The mean score of mental health problems (29.32) was in the ‘normal’ level, yet close to the ‘mild’ level (30; Lovibond & Lovibond, 1995). Though comparable data available were limited, the mean score of the masculinity (5.17 of -10 to 10) was significantly higher than 394 American psychology students (290 females and 104 males; M = -.85, SD = 4.86, p < .0001; Snell, 1989), and not significantly different from 69 American male veterans (M = 8.33, SD = 10.86, p = .10; Garcia, Finley, Lorber, & Jakupcak, 2011) through t-tests. The mean score of self-compassion (3.08 of 1-5) was not significantly different from 328 individuals (181 females and 147 males; Mage = 57, SDage = 15.2 years) in the general public (M = 3.07, SD =. 63, p = .87; López, Sanderman, Ranchor, & Schroevers, 2018). The mean scores of intrinsic (4.57 of 1-7, SD = 1.56), extrinsic motivation (4.28 of 1-7, SD = 1.40), and amotivation (2.17 of 1-7, SD = 1.28) were significantly lower than 103 hospitality workers (56 females and 47 males; Mage = 28.2, SDage = 8.6 years; intrinsic M = 5.79, SD =. 95, p < .0001; extrinsic M = 5.70, SD = .99 , p < .0001; amotivation M = 5.25, SD =1.82 , p < .0001; Kotera, Adhicari et al., 2018). Table 2 One-way MANOVA: Difference in the Mean Mental Health Shame, Mental Health Problems, Masculinity, Self-compassion, and Motivation Scores betweenDifferent Roles  Note. *Significant differences among the groups (p < .001). Same superscripts indicate a significant difference between the two groups on that measure (p < .05). Further, a one-way multivariate analysis of variance (MANOVA) was conducted to appraise whether there were differences in mental health shame, mental health problems, masculinity, self-compassion, and motivation between different job roles (Table 2). There was a multivariate effect (p < .001); univariate analyses revealed there were only differences in intrinsic and extrinsic motivation. Managers and technical professionals had higher intrinsic motivation than operators/workers and foremen/supervisors, based on t-tests. Also, managers and technical professionals had higher extrinsic motivation than operators/workers. Relationships between Mental Health Shame, Problems, Masculinity, Motivation, and Self-Compassion (H1) The subscales of ATMHP were summed to calculate the ‘mental health shame’ score (Gilbert et al., 2007). The mental health shame score was not normally distributed (Shapiro-Wilk’s test, p < .05), thus all the variables were square-root-transformed to satisfy the assumption of normality (Field, 2018). Mental health shame was positively associated with mental health problems (H1a), while mental health shame was not associated with masculinity (H1b). Amotivation was positively associated with mental health problems (H1c), though none of the three types of motivation was related to mental health shame (H1d). Self-compassion was negatively associated with mental health problems (H1e), shame (H1f), and amotivation (H1g). H1 was accepted in the main (Table 3). Previous treatment experience was associated with higher mental health problems and lower self-compassion. Table 3 Correlations among Mental Health Shame, Mental Health Problems, Masculinity, Self-compassion, and Work Motivation in UK Construction Workers (N = 155)  Note. All variables are square-route transformed. 10. Whether they have attended mental health training in the past. 11. Whether they have received mental health treatment inthe past *p < .05, **p < .01. Self-Compassion as a Mediator between Mental Health Shame and Problems (H2) Finally, path analysis was conducted, using model 4 in the Process macro (parallel mediation model; Hayes, 2012), in order to examine whether self-compassion (mediator variable) mediated the relationship between mental health shame (predictor variable) and mental health problems (outcome variable). Figure 1 Parallel Mediation Model: Mental Health Shame as a Predictor of Mental Health Problems, Mediated by Self-compassion. 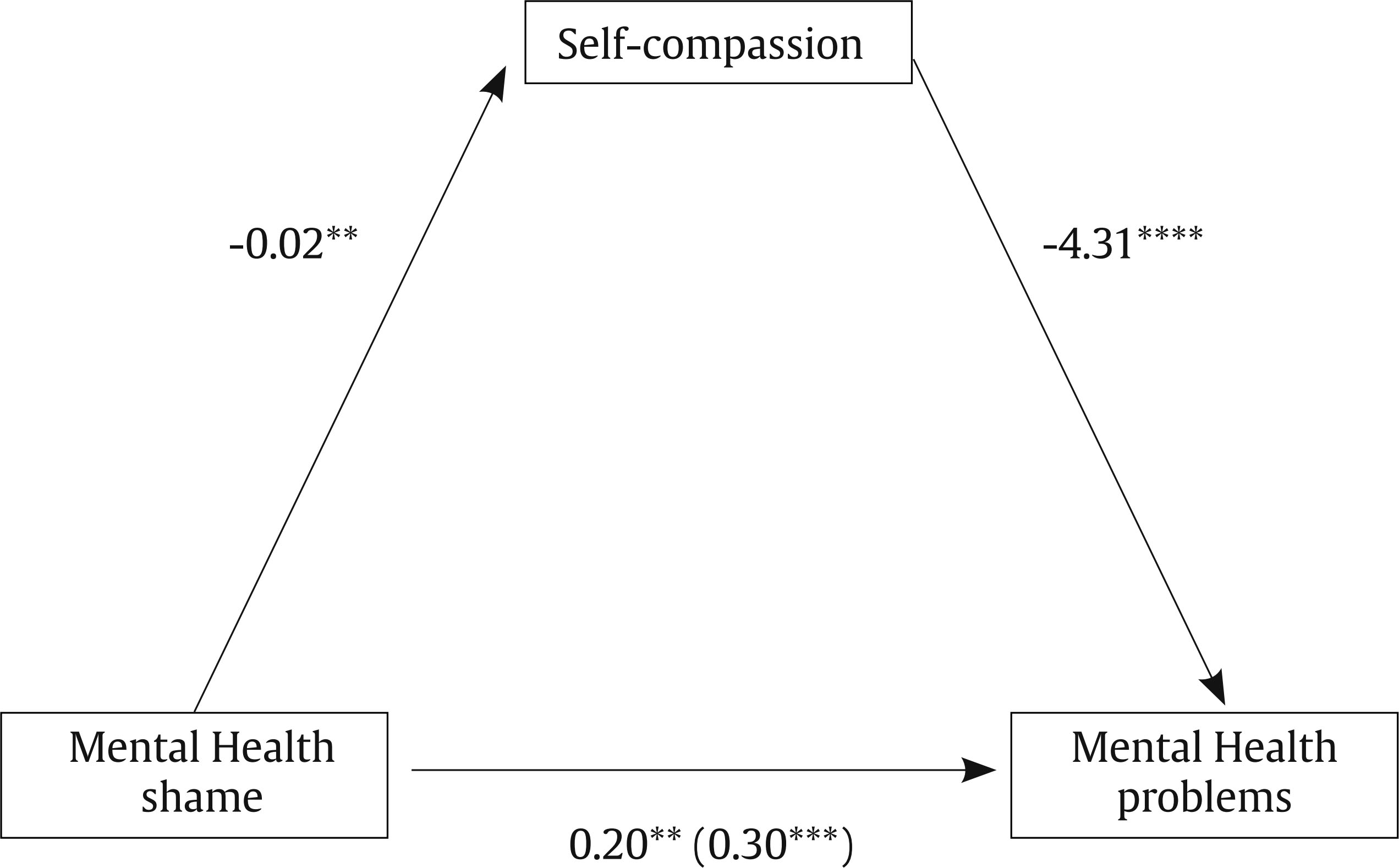 The confidence interval for the indirect effect is a BCa bootstrapped CI based on 5,000 samples. Direct effect (total effect). Values attached to arrows are coefficients indicating impacts. *p < .05, **p < .01, ***p < .001, ****p < .0001. There was a significant indirect effect of mental health shame on mental health problems through self-compassion, b = 0.10, BCa CI [.04, .18], which explained 15% of the variance in mental health problems, and accounted for 33% of the total effect, indicating a medium effect. The direct effect of mental health shame on mental health problems, controlling for the self-compassion, was still significant, b = 0.20, t(152) = 2.71, p = .008, implying that mental health shame could directly predict the variance in mental health problems. The total effect of mental health shame on mental health problems, including self-compassion, was also significant, b = 0.30, t(152) = 3.78, p = .00002. Because both of the paths from shame to self-compassion (negative prediction; higher shame predicting lower self-compassion), and from self-compassion to mental health problems (negative prediction; higher self-compassion predicting lower mental health problems) were significant, while the path from shame and mental health problems (positive prediction; higher shame predicting higher mental health problems) was also significant, self-compassion partially mediated the relationship between mental health shame and mental health problems. Mental health shame directly predicted mental health problems along with indirect effects through self-compassion on mental health problems. The full model of mental health shame as a predictor of mental health problems mediated through self-compassion is outlined in Figure 1 and summarised in Table 4. H2 was accepted. Table 4 Summary of the Path Analyses (Figures 1) (5,000 Bootstrap Samples)  Note. 1Significant point estimates (p < .05) using 95% bootstrapping confidence interval p < .05, **p < .01, ***p < .001. This study investigated the relationships between mental health shame, mental health problems, masculinity, self-compassion, and motivation. The rates of construction workers who scored over the midpoint were low, the highest being 36.13% for internal shame. Mental health shame, mental health problems, masculinity, self-compassion, and motivation were adequately related to each other (H1a, c, e-g), except for mental health shame and masculinity (H1b), and mental health shame and motivation (H1d). Finally, self-compassion partially mediated the relationship between mental health shame and mental health problems (H2). Each finding is discussed in turn below. The rates of construction workers who scored over the midpoint in each type of mental health shame were low, with internal shame being the highest (Table 1). Contrary to our hypothesis and previous findings (Alderson, 2017), construction workers in this study did not report high shame about mental health problems. This may imply that because mental health shame has been highlighted in the UK construction industry, some groups of construction workers already have good awareness of mental health problems: a recent study reported a low level of self-stigma in male Australian construction workers (Milner et al., 2017). Though not substantial, as many as 15% of participants in this study had mental health training, and 14% received mental health support. A relatively high level of internal shame suggests their strict self-evaluation about mental health problems: when they have mental health problems, they may feel shameful about themselves, seeing themselves as weak or incompetent. This contrasts with low rates in other types of mental health shame. Whilst they have a rather compassionate perspective towards other colleagues’ mental health problems, they would not see themselves in a similar way when they have a mental health problem. Self-criticism, related to strict self-evaluation, may help interpret this difference. Self-criticism was most strongly related with internal shame among all types of mental health shame in Japanese workers (Kotera, Gilbert et al., 2018). Future research should explore the effects of mental health training on mental health shame in construction workers and examine how positive attitudes about mental health (i.e., low mental health shame) can be transmitted in work settings. Further evaluating their self-criticism may offer insights into the mechanism of mental health shame in construction workers. Because managers have been highlighted as key players for mental health in a workplace (Kline & Sussman, 2000) and had high work motivation in general (Table 2), mental health training for managers may be an effective first step towards improvement of organisational mental health attitudes. In our correlation analysis (Table 3), mental health problems were positively related to mental health shame (i.e., negative attitudes, external shame, internal shame, and reflected shame), and amotivation, while they were negatively related to self-compassion. This echoed previous findings (e.g., Houkes et al., 2003; Kotera, Conway et al., 2018; Kotera et al., 2019; Raes, 2011), suggesting broad negative implications of poor mental health. Contrary to previous findings (Bryant & Garnham, 2015; Lomas, 2014) and our hypothesis, masculinity was not related to mental health shame. This suggests that there were relatively many construction workers who had low shame about mental health problems and high masculinity, or vice versa. Indeed, masculinity scores were high. So, it is possible that these workers use their masculinity to counter the feelings of shame. For example, some highly success-dedicated workers (one factor of masculinity; Snell, 1989) may ignore shame about mental health problems, as it could hinder their success. Additionally, a high level of emotional restriction (another factor of masculinity; Snell, 1989) may, at least temporarily, help them cope with shame. Repressive coping, in which negative emotions are denied without conscious recognition in order to secure one’s positive self-image (Garssen, 2007) may help explain these non-significant relationships between masculinity and mental health shame. Repressors tend to report their problems as less problematic than they actually are, in order to protect their self-worth (Wiltink, Subic-Wrana, Tuin, Weidner, & Beutel, 2010). The mechanisms underpinning these relationships should be explored in the future. Finally, self-compassion was a significant mediator in the relationship between mental health shame and mental health problems. In our path analysis, the importance of self-compassion was highlighted: the total effect (of mental health shame on mental health problems, including self-compassion) and the effect of self-compassion on mental health problems were stronger than the direct effect (of mental health shame on mental health problems). While previous studies separately explored the relationships between self-compassion, mental health shame, and mental health problems (Gilbert, 2009; Kotera et al., 2018; Sommers-Spijkerman et al., 2018), the present study elucidated the structure of how those three may be interrelated. Compassion training to cultivate self-compassion may be effective for improving mental health among construction workers (Braehler et al., 2013; Gilbert & Procter, 2006; Kelly et al., 2009). It is noteworthy to highlight that training ought to focus on self-compassion (rather than compassion for others) because self-compassion was not related to compassion for others: further, compassion for others was not related to mental health (López et al., 2018). Considering their long, various working hours, brief online self-compassion training may be useful. For example, three-hour online training about self-compassion increased gratitude, well-being, and self-compassion in health professionals, who also work long, irregular hours (Rao & Kemper, 2017). Additionally, as many construction workers work at diverse sites, the accessible nature of online training may be suited to this group of workers. Research into this type of intervention would need to be careful of information sharing between the intervention and passive control groups, as that could reduce mental health shame in the control group (Milner et al., 2017). There were some limitations to this study. Firstly, the participants were collected through opportunity sampling, which limits the generalisability of the findings of this study. Secondly, the participants were recruited from one organisation albeit a large one, thus organisational biases might have been present such as low recruitment of women. Thirdly, while there was no correlation between shame and perceived risk of disclosing personal information in UK samples (Gilbert et al., 2007), measuring shame and masculinity using self-report scales might limit their accuracy (Fan et al., 2006). Fourthly, the total score of the Self-Compassion Scale (Neff, 2003) needs to be interpreted with caution because the negatively worded items in this scale captured self-criticism, which was independent from self-compassion (thus should not be measured together; López et al., 2015). Nevertheless, we decided to use this scale, as it was the only scale exclusively measuring the degree of self-compassion at the time of the study. Lastly, the causal direction of these effects has not been analysed. In the future, longitudinal data would help appraise the temporal patterning of the observed relationships and may help develop interventions that would refine our understanding of causality. Despite the challenging mental health of construction workers and the importance of the industry to the UK economy, research into mental health and shame toward it among UK construction workers has been sparse. Findings from this study suggest that shame about mental health problems were related to mental health, self-compassion, and motivation in UK construction workers. Self-compassion and mental health shame were key constructs influencing the mental health of this workforce, although the direction of these effects could not be determined in this cross-sectional study. If self-compassion and mental health shame play key roles in their mental health problems, future research should determine whether the provision of the training focusing on mental health shame and brief self-compassion training leads to improvements in mental health among UK construction workers. Cite this article as: Kotera, Y., Green, P., & Sheffield, D. (2019). Mental health shame of UK construction workers: Relationship with masculinity, work motivation, and self-compassion. Journal of Work and Organizational Psychology, 35, 135-143. https://doi.org/10.5093/jwop2019a15 References |
Cite this article as: Kotera, Y. , Green, P. , & Sheffield, D. (2019). Mental Health Shame of UK Construction Workers: Relationship with Masculinity, Work Motivation, and Self-Compassion. Journal of Work and Organizational Psychology, 35, 135 - 143. https://doi.org/10.5093/jwop2019a15
Correspondence: Yasuhiro Kotera (y.kotera@derby.ac.uk)
Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print SEND
SEND






