


Disconnecting to Detach: The Role of Impaired Recovery in Negative Consequences of Workplace Telepressure
[Desconectar para desvincularse: el papel de la mala recuperaciĂłn en las consecuencias negativas de la telepresiĂłn en el trabajo]
Xinyu Hu1, Alecia M. Santuzzi1, and Larissa K. Barber2
1Northern Illinois University, USA; 2San Diego State University, USA
https://doi.org/10.5093/jwop2019a2
Received 6 August 2018, Accepted 27 December 2019
Abstract
Information and communication technologies (ICT) afford benefits in staying connected and increasing work flexibility for employees; however, they also bring us negative behavioral and psychological outcomes. This research examines the potential consequences of workplace telepressure, referring to the preoccupation with and urge to respond quickly to work-related ICT messages, on employee physical and psychological outcomes and the intervening roles of psychological detachment and boundary-crossing behaviors. A sample of 233 full-time workers from an online survey panel completed an online questionnaire. We observed bivariate relationships between workplace telepressure and health outcomes (i.e., employee burnout, poor sleep quality), psychological detachment, and boundary crossing. Bootstrapped indirect effects analyses showed that only boundary crossing provided a viable pathway by which workplace telepressure was associated with physical fatigue, poor sleep quality, and low sleep quantity. Implications of the intervening role of boundary crossing and the relationships between workplace telepressure and negative health outcomes are discussed.
Resumen
Las tecnologĂas de informaciĂłn y comunicaciĂłn (TIC) ofrecen las ventajas de estar conectados y aumentar la flexibilidad laboral de los empleados, aunque tienen consecuencias conductuales y psicolĂłgicas negativas. Esta investigaciĂłn analiza las consecuencias que tiene la telepresiĂłn, referida a la preocupaciĂłn y urgencia en responder rápidamente a mensajes relativos al trabajo (utilizando las TIC), sobre el desempeño fĂsico y psicolĂłgico de los trabajadores y sobre el papel intermediario que juegan la desvinculaciĂłn psicolĂłgica y el cruzar los lĂmites del trabajo. Se pasĂł un cuestionario en lĂnea a 233 trabajadores a tiempo completo. Observamos las relaciones bivariadas de la telepresiĂłn y sus consecuencias en la salud (por ejemplo, agotamiento emocional o mala calidad del sueño), el desapego psicolĂłgico y el franqueo de los lĂmites del trabajo. Los análisis de bootstrap de los efectos indirectos mostraron que solo el franqueo de estos lĂmites constituye un camino válido para asociar la telepresiĂłn con la fatiga fĂsica, la mala calidad de sueño y dormir poco. Se discuten las implicaciones del papel interventor que tiene el cruzar los lĂmites del trabajo y sus relaciones entre la telepresiĂłn y las consecuencias negativas para la salud.
Palabras clave
TelepresiĂłn en el trabajo, Desapego psicolĂłgico, Franquear los lĂmites del lugar de trabajo, Agotamiento emocional, Presentismo, Sueño.Keywords
Workplace telepressure, Psychological detachment, Boundary crossing, Burnout, Presenteeism, Sleep.Cite this article as: Hu, X. , Santuzzi, A. M. , & Barber, L. K. (2019). Disconnecting to Detach: The Role of Impaired Recovery in Negative Consequences of Workplace Telepressure. Journal of Work and Organizational Psychology, 35, 9 - 15. https://doi.org/10.5093/jwop2019a2
Correspondence: hujudy12@gmail.com (X. Hu).Introduction Information and communication technologies (ICTs), such as portable technology devices (e.g., smartphones, tablets, and laptop computers) and software packages (e.g., virtual private network) have allowed employees to stay connected to their work teams both during and after work hours (Towers, Duxbury, Higgin, & Thomas, 2006). Despite the benefits of flexible work arrangements (Hill et al., 2008), engaging in work tasks beyond the boundaries of the workplace (e.g., at home) predicts negative behavioral and psychological outcomes, including work-family conflicts and impaired recovery experiences (Boswell & Olson-Buchanan, 2007; Derks, Duin, Tims, & Bakker, 2015; Park & Jex, 2011). Even within the workplace, electronic communication can increase interruption, referred to temporarily shifting one’s focus from a primary work task to either another work-related request or nonwork-related messages, which in turn leads to increased work exhaustion and negative affect (Kossek, Ruderman, Braddy, & Hannum, 2012; Sonnentag, Reinecke, Mata, & Vorderer, 2018; ten Brummelhuis, Bakker, Hetland, & Keulemans, 2012). The negative consequences of continuous connection to electronic devices may be driven by employees’ psychological responses to perceived demands to stay connected and respond quickly. Barber and Santuzzi (2015) introduced workplace telepressure, defined as a preoccupation with and an urge to respond quickly to work-related electronic messages. Conceptually distinct from other technology constructs (i.e., usage and demands; Day, Paquet, Scott, & Hambley, 2012), workplace telepressure represents psychological reaction to the expected and encouraged responses to work-related messages. Telepressure was shown to be linked to negative health-related outcomes, such as poor sleep quality and burnout in both worker and student samples (Barber & Santuzzi, 2015, 2017). This study aimed to further examine the effects of workplace telepressure on psychological and physical health outcomes and to uncover potential underlying mechanisms of those relationships. Workplace Telepressure and Health Outcomes According to the Job Demands-Resources Model (Bakker & Demerouti, 2007), extended physical and psychological efforts (demands) negatively affect both health-related outcomes and work-related outcomes (Schaufeli & Bakker, 2004). With the increase in using work technologies, expectations for quick responses, technical failures and disruptions, and other technology use challenges have emerged as common workplace demands (Day et al., 2012). Importantly, ICT demands have been shown to predict stress and strain outcomes above and beyond traditional job demands (Day et al., 2012; Stich, Tarafdar, Cooper, & Stacey, 2017). As such demands are associated with higher levels of telepressure among workers (Barber & Santuzzi, 2015), we expect people with high levels of workplace telepressure to suffer from impaired psychological health outcomes and reduced work productivity. Recent research has found associations between workplace telepressure and employee burnout and sleep outcomes, such as poor sleep quality and sleep quantity (Barber & Santuzzi, 2015; Santuzzi & Barber, 2018). Although it was a plausible expectation, past research has not shown a bivariate relationship between workplace telepressure and presenteeism, referring to engaging in work-related activities while being ill (Koopman et al., 2002). This was surprising because research has demonstrated that constant exposure to work-related tasks via technological devices may be linked to physical health problems in the long run (Arlinghaus & Nachreiner, 2014; Lanaj, Johnson, & Barnes, 2014). Therefore, this study aimed to replicate the bivariate relationships between workplace telepressure and physical and psychological health outcomes. We hypothesize that, Hypothesis 1: Workplace telepressure is positively associated with a) burnout, b) presenteeism, c) poor sleep quality, and (d) sleep inconsistency, and negatively associated with (e) sleep quantity. Psychological Detachment and Boundary Crossing as Intervening Variables Workplace telepressure not only relates to workers’ health outcomes, but also the recovery experiences aimed to preserve health and well-being in the long term (Barber & Santuzzi, 2015). Drawing from the Effort-Recovery Model (Meijman & Mulder, 1998), the effort required by work demands, including high workloads and meeting people’s expectations, causes temporary load reactions that manifest experientially as feelings of exhaustion. Sufficient recovery is needed in order to restore energy and return the loads level to the baseline. In particular, individuals can recover from work demands in various ways, such as psychological detachment, referred as mentally refrained from work-related tasks (Sonnentag & Fritz, 2007). However, individuals experiencing high workplace telepressure may be more likely to ruminate on work-related communication tasks, which interferes with one’s recovery experiences. Thus, we will examine how workplace telepressure may have an impact on recovery in two forms: psychological detachment and boundary-crossing behavior. Psychological Detachment A systematic review of the Stressor-Detachment Model suggested that low psychological detachment would lead to more burnout, sleep problems, health complaints, and other impaired well-being outcomes (Sonnentag & Fritz, 2015). More job stressors would lead to lower levels of psychological detachment, which in turn increase emotional exhaustion (Sonnentag, Kuttler, & Fritz, 2010). Additionally, Berset and colleagues have examined a similar model with rumination as a mediator, for which they found that rumination mediated the effect of job stressors on impaired sleep (Berset, Elfering, Lüthy, Lüthi, & Semmer, 2011). Recovery experiences were limited when work availability was extended, which led to impaired well-being (Dettmers, Vahle-Hinz, Bamberg, Friedrich, & Keller, 2016). Workplace telepressure may function similarly to being exposed to higher levels of job stressors by interfering with psychological detachment, and subsequently impairing various health outcomes. Santuzzi and Barber (2018) found some evidence supporting psychological detachment as an intervening variable in the relationship between workplace telepressure and physical exhaustion and sleep problems. Although they collected experiences across three measurement periods, the effects were only apparent at the between-person level of analysis. Thus, the findings should emerge using a cross-sectional survey design involving measures of workplace telepressure, psychological detachment, and health outcomes at the individual level. Similar to past findings, we expect that lower levels psychological detachment would at least partially explain the relationship between workplace telepressure and physical and psychological health outcomes. Specifically, we hypothesized that, Hypothesis 2: Workplace telepressure is negatively associated with psychological detachment. Hypothesis 3: Workplace telepressure has an indirect effect on (a) employee burnout, (b) presenteeism, and (c) sleep outcomes via psychological detachment. Boundary-crossing Behavior While psychological detachment captured the psychological piece of connectivity, boundary crossing is a behavioral manifestation of technological connectivity, such as some individuals may engage in work-related activities using technology devices while temporally or physically being in a nonwork domain (e.g., family time or at home; Allen, Cho, & Meier, 2014). Technology use during after-hours have been shown to lead to lack of recovery over time (e.g., Derks, van Mierlo, & Schmitz, 2014; Ohly & Latour, 2014). Individuals who experience high levels of telepressure may be more likely to perform work-related tasks (e.g., responding to work-related text messages) while at home or during other forms of recovery time (Barber & Santuzzi, 2015). Additionally, allowing work tasks to cross boundaries into non-work life has been commonly studied in relation to its negative impact on work-family conflicts, which in turn leads to stress-related outcomes (Allen et al., 2014). Given that workplace telepressure is conceptualized as an internal psychological state, it is important to examine how workplace telepressure is manifested behaviorally, and whether it serves as an alternative mediating role. By definition, workplace telepressure involves a preoccupation with responding to work messages. Logically, this suggests telepressure should interfere with competing demands, such as those outside of the workplace, and encourage ICT response behaviors during non-work time. Thus, we hypothesize that, Hypothesis 4: Workplace telepressure is positively associated with boundary crossing. Hypothesis 5: Workplace telepressure has an indirect effect on (a) employee burnout, (b) presenteeism, and (c) sleep outcomes via boundary crossing. MethodParticipants and Procedure Full-time workers were recruited through Survey Monkey Audience for a study on technology use and health-related outcomes. As an incentive to complete the survey, participants were allowed to assign a $0.50 donation to a charity of their choice. Out of the 313 who agreed to participate, 259 fully completed the survey. Of those, 22 were dropped for missing a quality control check item assessing whether respondents were currently using a computer. In addition, 5 participants were dropped for not reporting valid full-time work hours. Thus, the final sample included 233 cases1. The majority of completed respondents were female (n = 161, 69.15%). Respondents ranged from ages 18 to 29 (n = 19, 8.2%), 30 to 44 (n = 64, 27.6%), 45 to 60 (n = 106, 45.7%), and 60 and above (n = 43, 18.5%). One participant (0.4%) did not report age. The average hours worked per week was 44.56 (SD = 6.76) with a minimum of 32 hours and a maximum of 65 hours reported. Of those who reported telecommuting (n = 85, 36.5%), the average hours per week spent telecommuting was 11.40 (SD = 10.79) with a minimum of 1 hour and a maximum of 40 hours reported. They also spent an average of 2.82 days per week telecommuting (SD = 2.39) with a minimum of 0 day and a maximum of 7 days reported. Measures Workplace telepressure. Workplace telepressure was assessed using the 6-item validated measure (Barber & Santuzzi, 2015; α = .90). Participants were asked to think about situations when they use messaged-based technologies for work purposes. An example item is “I feel a strong need to respond to others immediately.” Response options ranged from 1 (strongly disagree) to 5 (strongly agree). Burnout. Burnout was assessed using the 14-item Shirom-Melamed Burnout Measure (Shirom & Melamed, 2006). This measure comprises three subdimensions: physical fatigue (e.g., “I feel fed up”; α = .94), cognitive weariness (e.g., “I have difficulty concentrating”; α = .97), and emotional exhaustion (e.g., “I feel I am not capable of investing emotionally in coworkers or customers”; α = .94). Responses ranged from 1 (never or almost never) to 7 (always or almost always). Presenteeism. Presenteeism was assessed using the 6-item Stanford Presenteeism Scale (Koopman et al., 2002; α = .95). Participants were asked to report the extent to which health problems interfered with their productivity over the last month. An example item is “I felt hopeless about finishing certain work tasks due to health problems.” Responses ranged from 1 (strongly disagree) to 7 (strongly agree). Sleep problems. We measured sleep in three ways: sleep quantity, sleep quality, and sleep consistency. Sleep quantity. Sleep quantity was measured using one item that asked participants, “over the past month, how many hours of sleep did you typically get during a work week?” Sleep quality. Sleep quality was measured using a 4-item insomnia scale (Jenkins, Stanton, Niemcryk, & Rose, 1988; α = .81). This scale asked participants to indicate how often they experienced sleep symptoms during the past month on a scale ranged from 0 (not at all) to 7 (every night). These symptoms included: trouble falling asleep, trouble staying asleep, waking up several times during the night, and waking up after one’s usual amount of sleep feeling tired and worn out. Higher scores indicated poorer sleep quality. Sleep consistency. Sleep consistency was measured using a 3-item subscale taken from the Sleep Hygiene Index (Mastin, Bryson, & Corwyn, 2006; α = .69). These items asked participants to indicate the extent to which they experienced the following: went to bed at different times from day to day, get out of bed at different times from day to day, and stay in bed longer than they should have two or three times a week. Responses ranged from 1 (never) to 5 (always) and higher scores indicated more sleep inconsistency. Psychological detachment. Psychological detachment was measured using a 4-item subscale from the Recovery Experience Questionnaire (Sonnentag & Fritz, 2007; α = .87). This scale asked participants to indicate specifically the extent to which they mentally detached from work related tasks during nonwork time. An example item is, “During my free evenings (or nonwork time), I forget about work.” Responses ranged from 1 (strongly disagree) to 5 (strongly agree). Boundary crossing. Boundary crossing was measured using 2 items used in Barber and Santuzzi (2015), which were adapted from an original scale (Olson-Buchanan & Boswell, 2006; Park & Jex, 2011). Both items asked how often one uses technology devices to perform work tasks and arrange work schedules at home and during nonwork hours. Responses ranged from 1 (never/almost never) to 5 (very often/almost always). The two items demonstrated good internal consistency (α = .80). ResultsDescriptive statistics, reliabilities, and bivariate correlations of all study variables are shown in Table 1. Table 1 Descriptive Statistics, Reliability, and Correlation Matrix of Study Variables  Note. Cronbach’s alpha is indicated in bold on the diagonal. M denotes average of variables; SD denotes standard deviation of variables. N = 233.*p < .05. Common Method Variance Given that our variables were measured based on self-reported experiences, we tested the presence and magnitude of common method variance in our data using a single unmeasured latent method factor technique recommended by Podsakoff, MacKenzie, Lee, and Podsakoff (2003). By using Mplus version 8.0 (Muthén & Muthén, 1998-2018), we compared three models, a nine-factor measurement model, a measurement model with an orthogonal method factor, and a revised method factor model by constraining correlations among the nine factors to the correlation obtained from the nine-factor only model. We used chi-square tests, comparative fit index (CFI), Tucker-Lewis Index (TLI), root mean square error of approximation (RMSEA), and standardized root mean-square residual (SRMR) to evaluate measurement models (Hu & Bentler, 1999). The nine-factor and an orthogonal method factor model, χ2(627) = 1415.457, p < .001, CFI = .889, TLI = .869, RMSEA = .073, 95% CI [0.068, 0.079], SRMR = .056, fitted better than the nine-factor only model, χ2(666) = 2055.093, p < .001, CFI = .805, TLI = .783, RMSEA = .095, 95% CI [0.090, 0.099], SRMR = .099; particularly, variance partitioning showed that 19.40% of variance was attributed to the method factor, which is smaller than a median amount of variance 25% from other self-reported studies (Williams, Cote, & Buckley, 1989). Additionally, the fit of a revised model, χ2(663) = 1457.204, p < .001, CFI = .889, TLI = .875, RMSEA = .072, 95% CI [0.067, 0.077], SRMR = .076, did not change significantly (Δχ2 = 41.747, Δdf = 36, p = .235), which showed little evidence for common method variance. Therefore, analyses for hypothesis testing were conducted without accounting for the method factor. Hypothesis Testing We found that workplace telepressure had significant positive associations with all three subdimensions of burnout (physical fatigue: r = .24, p < .01; cognitive weariness: r = .29, p < .01; emotional exhaustion: r = .16, p < .01) and poor sleep quality (r = .13, p < .05). We also found that higher levels of workplace telepressure were associated with lower levels of psychological detachment (r = -.22, p < .01), and higher levels of boundary crossing behaviors (r = .19, p < .01). Non-significant bivariate relationships were found between workplace telepressure and presenteeism, poor sleep inconsistency, and sleep quantity (r = .11, p = .10; r = .04, p = .59; r = -.11, p = .10, respectively). Thus, Hypothesis 1a, 1c, 2 and 4 were supported. To test Hypotheses 3 and 5, we conducted path analyses, using maximum likelihood and bootstrapping for bias-corrected indirect effects estimation. As shown in Table 1, neither psychological detachment nor boundary crossing was significantly correlated with emotional exhaustion, presenteeism, and poor sleep inconsistency; therefore, we did not include them in the indirect effects models. We conducted two indirect effects models, one with psychological detachment as an intervening variable and one with boundary crossing as an intervening variable. The models only included outcomes that were viable based on bivariate correlation results. For the model with psychological detachment (see Figure 1), we did not find significant results supporting the indirect effects of workplace telepressure on physical fatigue (ab = .06, SE = .03, p = .086), cognitive weariness (ab = .05, SE = .03, p = .118), poor sleep quality (ab = .08, SE = .04, p = .068) or sleep quantity (ab = -.02, SE = .09, p = .055) via psychological detachment. Thus, Hypothesis 3 was not supported. The direct effects of workplace telepressure on health outcomes were significant for physical fatigue (c’ = .32, SE = .10, p = .002) and cognitive weariness (c’ = .39, SE = .10, p < .001), but not for poor sleep quality (c’ = .18, SE = .12, p = .131) or sleep quantity (c’ = -.30, SE = .27, p = .274), after controlling for psychological detachment. Figure 1 Path Model of Psychological Detachment Linking Workplace Telepressure and Health Outcomes.  Note. Subscripts are used to differentiate parameter estimates for different outcome variables; ab estimates represent indirect effects; c’ estimates represent direct effects; *denotes significant parameter estimates. When testing boundary crossing as an intervening variable in the relation between telepressure and health outcomes, we found significant indirect effects of workplace telepressure on physical fatigue (ab = .08, SE = .04, p = .033), poor sleep quality (ab = .10, SE = .04, p = .022), and sleep quantity (ab = -.25, SE = .11, p = .017) via boundary crossing (see Figure 2). However, we did not find evidence that workplace telepressure was indirectly related to cognitive weariness via boundary crossing (ab = .06, SE = .04, p = .075). Thus, Hypothesis 5a and 5c were partially supported, suggesting that the relationship between workplace telepressure and burnout and sleep outcomes could be partially driven by boundary crossing behaviors. Figure 2 Path Model of Boundary Crossing Linking Workplace Telepressure and Health Outcomes. 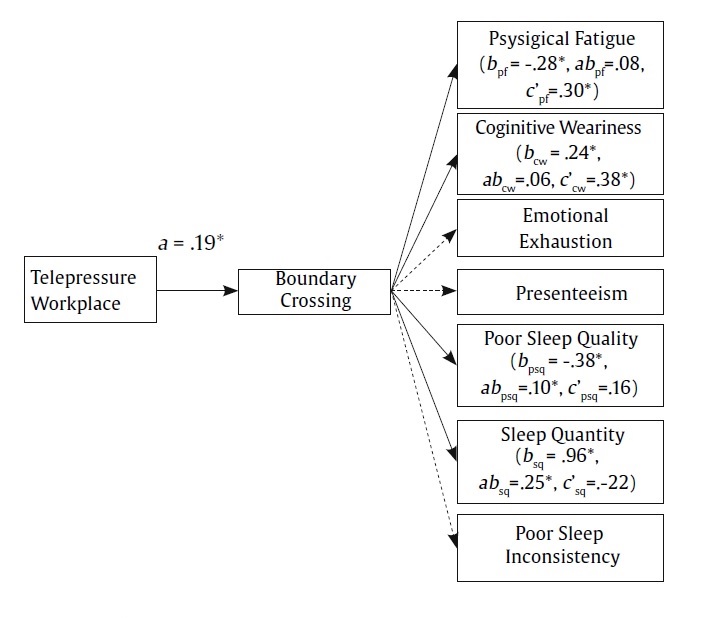 Note. Subscripts are used to differentiate parameter estimates for different outcome variables; ab estimates represent indirect effects; c’ estimates represent direct effects; *denotes significant parameter estimates. Additionally, we found that the direct effects of workplace telepressure on health outcomes were significant for physical fatigue (c’ = .30, SE = .10, p = .004) and cognitive weariness (c’ = .38, SE = .10, p < .001), but not for poor sleep quality (c’ = .18, SE = .12, p = .131) or sleep quantity (c’ = -.30, SE = .27, p = .274), after controlling for boundary crossing. DiscussionBuilding on the Effort-Recovery Model (Meijman & Mulder, 1998) and Stressor-Detachment Model (Sonnentag & Fritz, 2015), this study aimed to unpack the underlying mechanisms of the negative consequences of workplace telepressure on employee health outcomes. In addition to replicating the bivariate relationships found in past research (Barber & Santuzzi, 2015), psychological detachment and boundary crossing were examined as intervening variables for the negative consequences of workplace telepressure on physical and cognitive employee burnout, as well as sleep quality and quantity. This study established some evidence that workplace telepressure is positively associated with more burnout and poorer sleep quality, but not presenteeism and other sleep problems. These bivariate relationships are mostly consistent with the findings in Barber and Santuzzi (2015). Particularly, our study also found an additional significant positive correlation between workplace telepressure and emotional exhaustion. Findings regarding to three sleep indicators, such that only significant association was found with sleep quality, are not surprising given that the three sleep indicators are conceptually distinct aspects of sleep behaviors, which is reflected from the low correlations among the sleep indicators observed in this study. Though the magnitudes of correlations are relatively small in our study, the directions of the correlations are consistent with the literature (Barber, Munz, Bagsby, & Powell, 2010; Barber & Santuzzi, 2015; Litwiller, Snyder, Taylor, & Steele, 2017). Additionally, we found significant bivariate relationships between workplace telepressure and psychological detachment as well as boundary crossing. This shows that psychological reactions to technological demands not only influence one’s strain psychologically, but also change one’s behaviors by involving in work-related tasks in nonwork domains. Inconsistent with past literature (Santuzzi & Barber, 2018), the indirect effects through psychological detachment did not hold for workplace telepressure and employee burnout and sleep problems in this study. One alternative explanation is that workplace telepressure may function differently from other work demands, such that psychological detachment may not repair the exhaustion due to workplace telepressure. However, another plausible explanation is that the cross-sectional survey design did not allow for reliable measurement of detachment and health experiences. Past research showing the proposed indirect effect collected experiences across a two-month period. Although the effects emerged at the individual level of analysis, the individual level scores were informed by three measurements of each variable (and thus experiences during the two months of study; Santuzzi & Barber, 2018). A more inclusive collection of recovery and health experiences over time may be required for the impact of telepressure through poor recovery to be observed. However, we found evidence for significant indirect effects of workplace telepressure on physical fatigue and poor sleep quality and sleep quantity through boundary crossing. This provides initial evidence to workplace telepressure research, such that the experiences of workplace telepressure may very likely change one’s behaviors, which may subsequently negatively affect one’s cross-domain experiences. In particular, this contributes to the work- family literature such that workplace telepressure may have an impact on individual family role experiences, which could likely increase work-family conflicts (Amstad, Meier, Fasel, Elfering, & Semmer, 2011). Future research should explore this serial pattern using longitudinal measurement to reduce common measure correlations and test directional relationships among variables. Additionally, given the connections between workplace telepressure and boundary crossing behaviors, this practically implicates the potential of future behavioral intervention designs to alleviate the negative consequences of workplace telepressure. Limitations and Future Directions This study enriched the research on workplace telepressure and its relationship with other health outcomes; however, the results need to be interpreted by taking the cross-sectional design into account. Simultaneous measurement of multiple perceptual outcomes may limit the possibility to infer causal relationships. As suggested by previous research, there has been few cross-sectional and longitudinal studies that examined the mediating role of recovery between work-related factors and employee health; therefore, more diverse research using different designs and stressor factors (e.g., workplace telepressure) is needed (Sonnentag & Fritz, 2015). Thus, future research should consider adopting more rigorous methodology to uncover whether the impact of workplace telepressure on recovery experiences may last over time. In addition, the current study used self-reported subjective judgment of psychological experiences and behaviors, which may be susceptible to recall errors and biases due to current psychological states. Though common method variance was examined using a statistical remedy (Podsakoff et al., 2003), future research should consider other measurements to rule out potential biases arisen from subjective interpretation of psychological experiences of ICT behaviors. Some examples include using objective measures for behavioral concepts (i.e., monitoring amount of time spent using work-related ICT for work purpose during nonwork time as a way to capture boundary crossing), and physiological measurement to better represent the physical aspects of health outcomes (Semmer, Grebner, & Elfering, 2004). Using more rigorous research designs might encourage more precise estimates of effect sizes. This study extended current literature regarding the intervening roles of psychological detachment and boundary crossing behaviors in the relationship between workplace telepressure and health outcomes. Although receiving limited attention in the current literature, there are reasons to suspect a relationship between boundary crossing and psychological detachment, such that individuals who are inclined to engage in boundary crossing behaviors are less likely to feel psychologically detached from work-related tasks (Kinnunen et al., 2016, 2017). Barber and Jenkins (2014) suggested that creating boundary around using ICTs for work-related purposes could benefit one’s recovery experiences, lending some corroborating evidence that boundary management may protect worker recovery and, thus, health outcomes (i.e., sleep). We explored this pattern in our data by conducting post-hoc analyses to examine whether the effect of workplace telepressure can be transmitted through boundary crossing and psychological detachment in series. However, no significant serial indirect effects were found. This may be due to the relatively high correlation between boundary crossing and psychological detachment (r = .55) and the nature of cross-sectional design of current study. Future research could adopt a repeated-measure design to more appropriately test how behavioral and psychological aspects of recovery are related and collectively contribute to the negative consequences of workplace telepressure. Conclusion Telepressured employees may be more likely to exhaust and experience impaired well-being, such as employee burnout and poor sleep quality. Creating boundaries around work-related technology use is critical for reducing the negative effect of workplace telepressure on both physical and psychological outcomes. Occupational health is important in sustaining positive organizational outcomes (e.g., job performance; Wright & Cropanzano, 2000). Given that technologies have been prevalent in organizational communications, future research on interventions for ICT uses and experiences may be desired in order to prevent employees from experiencing work exhaustions and sleep problems, and to improve various positive organizational outcomes, such as work engagement and job performance. Cite this article as: Hu, X., Santuzzi, A. M., & K. Barber, L. K. (2019). Disconnecting to detach: The role of impaired recovery in negative consequences of workplace telepressure. Journal of Work and Organizational Psychology, 35, 9-15. https://doi.org/10.5093/jwop2019a2 Note 1A response was changed on an item assessing hours worked away from the office as a telecommuter as it appeared to be a typo. The initial response of 100 hours was changed to 10 hours, which better coincided with the participant’s answers on other items. References |
Cite this article as: Hu, X. , Santuzzi, A. M. , & Barber, L. K. (2019). Disconnecting to Detach: The Role of Impaired Recovery in Negative Consequences of Workplace Telepressure. Journal of Work and Organizational Psychology, 35, 9 - 15. https://doi.org/10.5093/jwop2019a2
Correspondence: hujudy12@gmail.com (X. Hu).Copyright © 2026. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print SEND
SEND






